Back to Journals » Infection and Drug Resistance » Volume 16
Risk Factor for Superimposed Nosocomial Bloodstream Infections in Hospitalized Patients with COVID-19
Authors Sathaporn N ![]() , Khwannimit B
, Khwannimit B
Received 9 March 2023
Accepted for publication 6 June 2023
Published 13 June 2023 Volume 2023:16 Pages 3751—3759
DOI https://doi.org/10.2147/IDR.S411830
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Natthaka Sathaporn, Bodin Khwannimit
Division of Critical Care Medicine, Department of Internal Medicine, Faculty of Medicine, Prince of Songkla University, Hat Yai, Songkhla, 90110, Thailand
Correspondence: Natthaka Sathaporn, Division of Critical Care Medicine, Department of Internal Medicine, Faculty of Medicine, Prince of Songkla University, 15 Kanchanavanich Road, Hat Yai, Songkhla, 90110, Thailand, Tel +66-887907414, Fax +66-74281457, Email [email protected]
Introduction: Corticosteroids are a component of the standard therapy for patients with coronavirus disease 2019 (COVID-19) because of the immunological dysregulation and hyperinflammation associated with the condition. This study aimed to evaluate the potential risk factors for nosocomial bloodstream infections in hospitalized patients with COVID-19, including the exploration of corticosteroid dosage and treatment duration.
Materials and Methods: A retrospective cohort study of hospitalized patients with COVID-19 was conducted in a tertiary care hospital. We performed univariate and multivariate analyses of various parameters to identify risk factors for nosocomial bloodstream infection.
Results: Of 252 patients, 19% had nosocomial bloodstream infections. The mortality rate of nosocomial bloodstream infections was 62.5%. Multivariate analysis revealed that male sex (odds ratio [OR] 3.43; 95% confidence interval [CI]: 1.60– 7.33), receiving methylprednisolone (OR: 3.01; 95% CI: 1.24– 7.31), receiving an equivalent dexamethasone dose of 6– 12 mg/day (OR: 7.49; 95% CI: 2.08– 26.94), and leukocytosis on admission (OR: 4.13; 95% CI: 1.89-9.01) were significant predictors of nosocomial bloodstream infections.
Conclusion: Unmodified risk variables for nosocomial bloodstream infections included male sex and leukocytosis at admission. Using methylprednisolone and obtaining a cumulative dosage of dexamethasone were adjusted risk variables associated with superimposed nosocomial bloodstream infections in hospitalized patients with COVID-19.
Keywords: bloodstream infection, risk factor, COVID-19, methylprednisolone, corticosteroid
Introduction
The severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) pandemic was an unprecedented global health obstacle that was first developed in 2019.1 Three clinical phases are commonly involved in adult coronavirus disease 2019 (COVID-19) models. First, there is an initial viral response phase, during which most patients experience only minor constitutional symptoms. Next is the pulmonary phase, during which the consequences of the host inflammatory response and viral replication coincide. Finally, a hyperinflammatory phase occurs, where the host immune reaction dominates pathogenesis.2 Because of immune dysregulation and hyperinflammation associated with COVID-19, the use of systemic corticosteroids has been a part of standard care since the Recovery trial3 was published in 2021 and has demonstrated a 28-day mortality benefit in hospitalized patients with COVID-19 requiring oxygen supplement.3 Moreover, anti-inflammatory agents such as interleukin-6, and Janus kinase (JAK) 1/2 inhibitors contribute to decreased hyperimmune response in the case of cytokine release syndrome.4–6 However, corticosteroids and immunosuppressive agents might increase the risk of secondary infection particularly nosocomial bloodstream infection (BSI) which increases morbidity and mortality.7–10 According to a previous study, patients with COVID-19 experience more BSIs during their intensive care unit (ICU) stay than patients without the virus.11 In real-world practice, corticosteroid dose and treatment duration depend on the physician’s pragmatics. Despite, various data from previous studies investigating the risk factors for BSI in patients with COVID-19, there are limited data on corticosteroid doses. Therefore, this study aimed to assess the risk factors of superimposed nosocomial BSI in patients with COVID-19, including exploration of corticosteroid dose and treatment duration.
Materials and Methods
This retrospective cohort study was conducted in a tertiary care referral center in Southern Thailand between February 2020 (when the first COVID-19 patient was admitted) and January 2022. This study was approved by the Human Research Ethics Committee of the Faculty of Medicine, Prince of Songkla University (REC.64-613-14-1) and was conducted under the ethical principles of the Declaration of Helsinki with a waiver of informed consent. This research is a retrospective study and presents no more than minimal risk of harm to subjects and involves no procedures for which written consent is normally required. A statement that covers the privacy of the participants, such as confirmation that the data was anonymized or maintained with confidentiality.
All hospitalized adult patients aged ≥ 18 years who were diagnosed with COVID-19 infection by a positive reverse transcription-polymerase chain reaction using the throat or nasopharyngeal swab or sputum aspirate and hemoculture performed during admission were included. Nosocomial BSIs were defined as the presence of microorganisms in one or more blood cultures at least 48 h after admission. For skin bacterial contamination such as Coagulase-negative staphylococci (CoNS), at least two in-sequence blood cultures for the same pathogen were diagnosed BSIs.12 The exclusion criteria were as follows: (1) patients who were diagnosed with community BSI, defined as positive blood culture < 48 h after admission, (2) patients who were transferred to other hospitals within 24 h, and (3) patients who were determined to receive the best supportive care and died within 24 h after admission. After enrollment, the patients were divided into the following two groups for analysis: nosocomial BSI and non-nosocomial BSI groups. Polymicrobial BSI was defined as the isolation of two or more different species from the same blood culture or two or more separate blood cultures.13 The primary outcome was the risk factor for nosocomial BSI in hospitalized patients with COVID-19. The secondary outcome was common nosocomial BSI pathogens.
This study recorded data on demographics, comorbidities, basic and inflammatory laboratory parameters, and pharmacologic and interventional treatments, including the duration of treatment. Treatment of corticosteroids was reported by receiving pulse methylprednisolone and cumulative dose of corticosteroids during hospitalization presented by equivalent dexamethasone dose calculated by 0.75 mg of dexamethasone equal to 5 mg of prednisolone and 20 mg of hydrocortisone.14 Severity scores, such as The Acute Physiology and Chronic Health Evaluation II (APACHE II),15 Sequential Organ Failure Assessment (SOFA),16 and Coronavirus Clinical Characterization Consortium (4C) Score17 were calculated by evaluating the worst parameters within 24 h after admission.
Continuous variables were presented as mean with standard deviation or median with interquartile range, and categorical variables were reported as numbers and percentages. Chi-square and Wilcoxon rank-sum tests were used to compare the categorical and continuous variables, respectively. The Kruskal–Wallis test was used to determine if there were statistically significant differences between two or more groups of independent variables continuously. Multivariate logistic regression was used to determine the variables that were significantly related to nosocomial BSI. Variables found to be significant at p < 0.1 on univariate analysis were entered into multivariate analysis. The multicollinearity was assessed by using the variance inflation factor (VIF), and any variable with a VIF greater than 2.5 was rejected from the model. All statistical analyses were performed using Stata version 15. A two-sided p < 0.05 was considered statistically significant.
Result
Two hundred and fifty-nine patients were screened during the study period of 2 years. Seven patients were excluded because of community BSIs (4 cases), referral within 24 h (2 cases), and need for end-of-life care with death within 24 h (1 case). Overall, 252 patients were included in the analysis, and 48 patients (19%) developed nosocomial BSIs. Most patients in this study (81.4%) were admitted to the ICU. Duration of ICU and hospital length of stay were significantly longer in the nosocomial BSI group. In addition, mortality in the nosocomial BSI group was significantly higher than that in the non-BSI group (62.5% vs 18.6%, p < 0.001). However, the overall mortality rate was 27%.
The demographic data and clinical characteristics of all patients are shown in Table 1. Age and pre-existing conditions were not significantly different between the groups. The three most prevalent comorbidities were hypertension (44.8%), type 2 diabetes (28.6%), and stages 4–5 of chronic renal disease18 (12.3%). Meanwhile, sex was significantly different between groups; the percentage of males was higher in the nosocomial BSI group (68.8%) than in the non-BSI group (45.6%). The median duration from symptom onset to hospital admission was 3 days in the nosocomial BSI group and 4 days in the negative blood culture group.
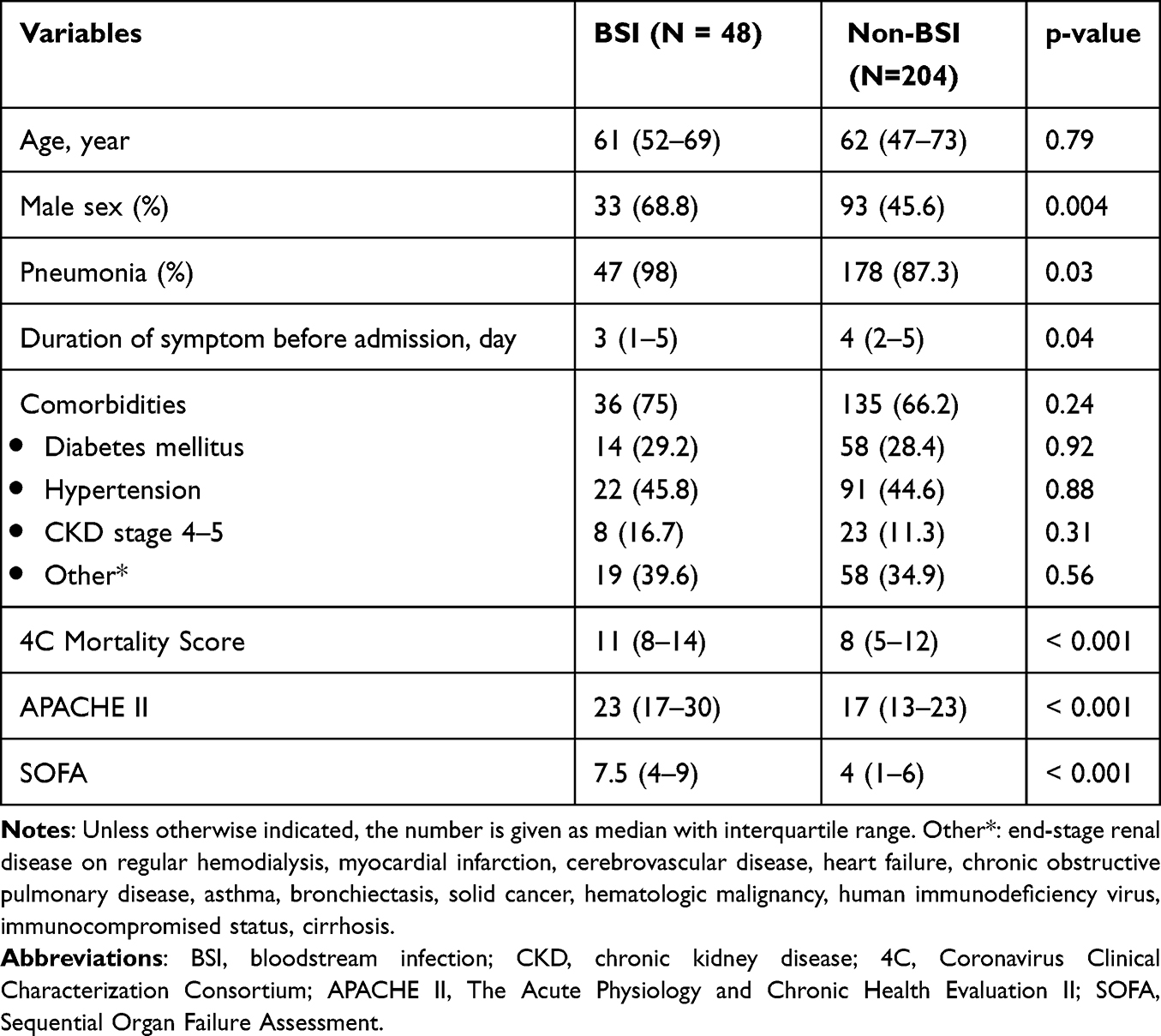 |
Table 1 Comparison of Demographics and Clinical Conditions Among COVID-19 Patients with Nosocomial BSIs and Non-BSIs |
Of the patients diagnosed with COVID-19 pneumonia, 97.9% were in the nosocomial BSI group, and 87.3% were in the non-BSI group. Corticosteroids were administered to all patients in the nosocomial BSI group. Meanwhile, 81.4% of the patients in the negative blood culture group used corticosteroids. Furthermore, the duration of corticosteroid use was significantly higher in the nosocomial BSI group than in the non-BSI group (21.5 days vs 13 days). The rate of receiving methylprednisolone was significantly higher in the nosocomial BSI group than in the non-BSI group (35.4% vs 10.8%). The median cumulative equivalent dexamethasone dose was higher in the nosocomial BSI group than in the non-BSI group (11.1 mg/day vs 9.8 mg/day). Moreover, the median durations from admission and corticosteroid administration to the first episode of BSIs were 12 days and 11.5 days, respectively. The median equivalent dexamethasone dose until the first episode of BSIs was 14.1 mg/day (interquartile range, 10.4–17.7). Sixty percent of the patients in the nosocomial BSI group received mechanical ventilation. The duration between the intubation day and the first episode of BSIs was 9 days. In the nosocomial BSI group, all severity scores determined by the APACHE II, SOFA, and 4C Mortality Score were considerably high.
Other pharmacological treatments and interventions, such as receiving antiviral therapy, did not differ between groups. The use of tocilizumab, baricitinib, and tofacitinib was not associated with nosocomial BSI. Moreover, antibiotic administration within the first 48 hours of admission did not decrease the risk of nosocomial BSI; 39.6% and 51.5% in BSI and non-BSI groups, respectively, p=0.13. In contrast, receiving of hemoperfusion, both triple and double-lumen insertions and urinary catheter insertions were associated with nosocomial BSI (Table 2).
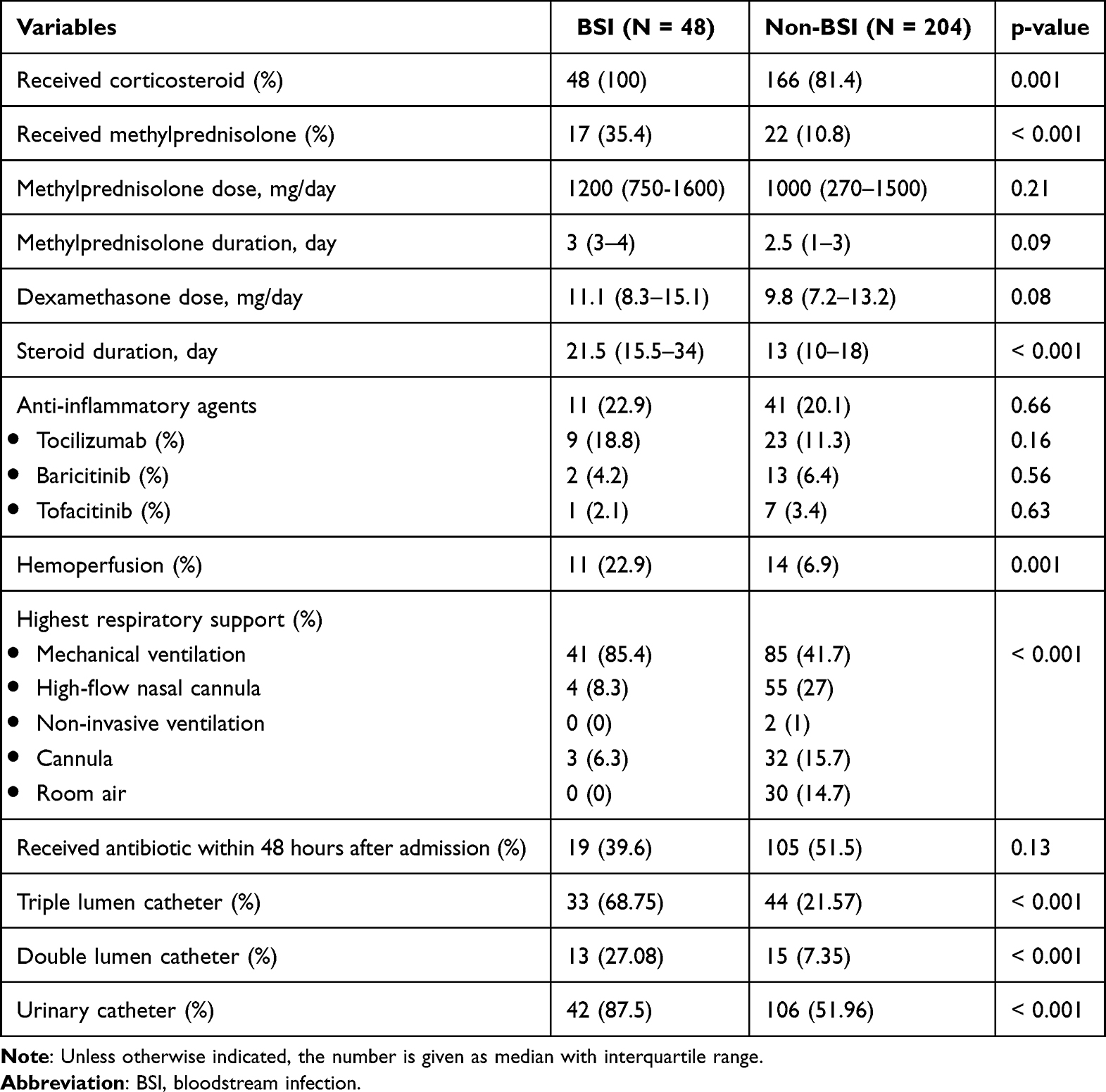 |
Table 2 Comparison of Treatment Among COVID-19 Patients with Nosocomial BSIs and Non- BSIs |
Inflammatory markers and white blood cell count on admission were significantly higher in the nosocomial BSI group. However, lower absolute lymphocyte counts were observed in the nosocomial BSI group (Table 3). Other characteristics of the nosocomial BSI group are shown in Table 4.
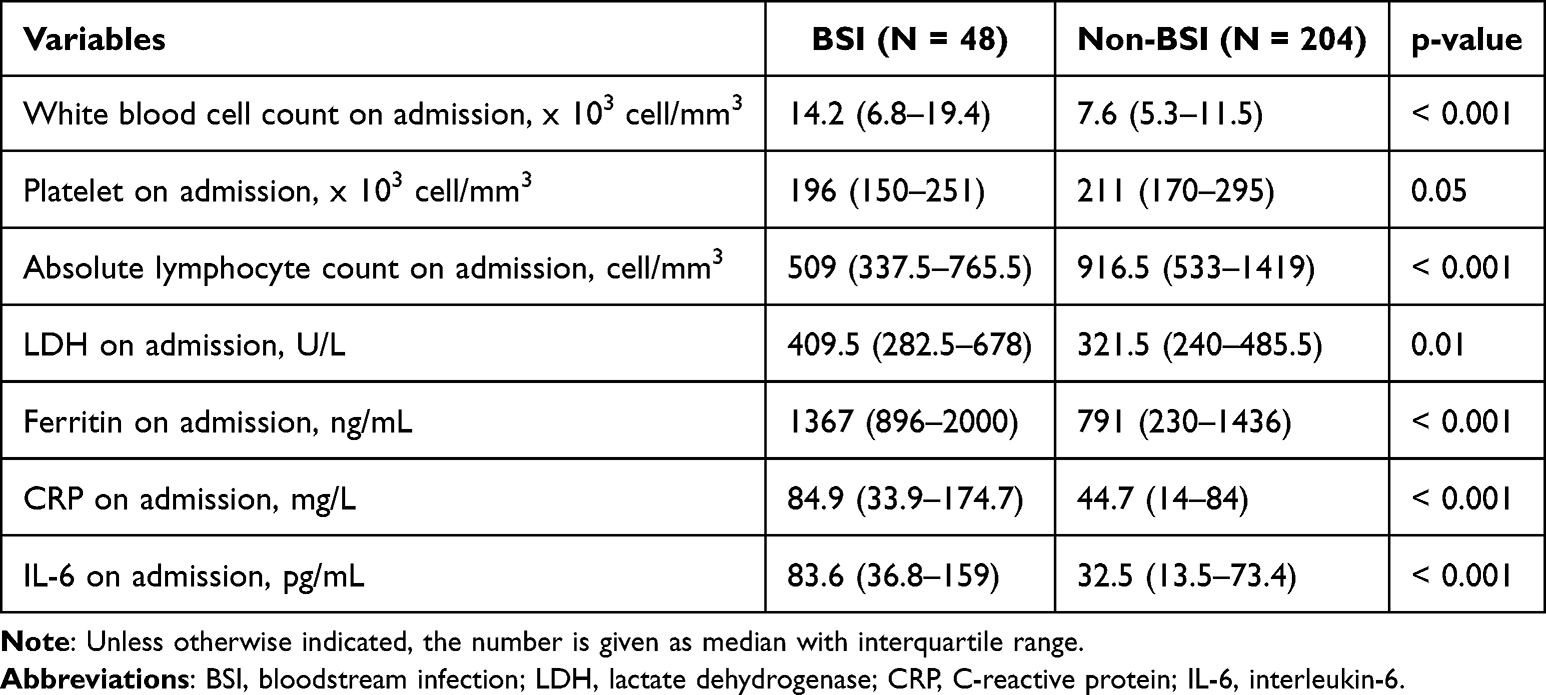 |
Table 3 Comparison of Investigation Among COVID-19 Patients with Nosocomial BSIs and Non-BSIs |
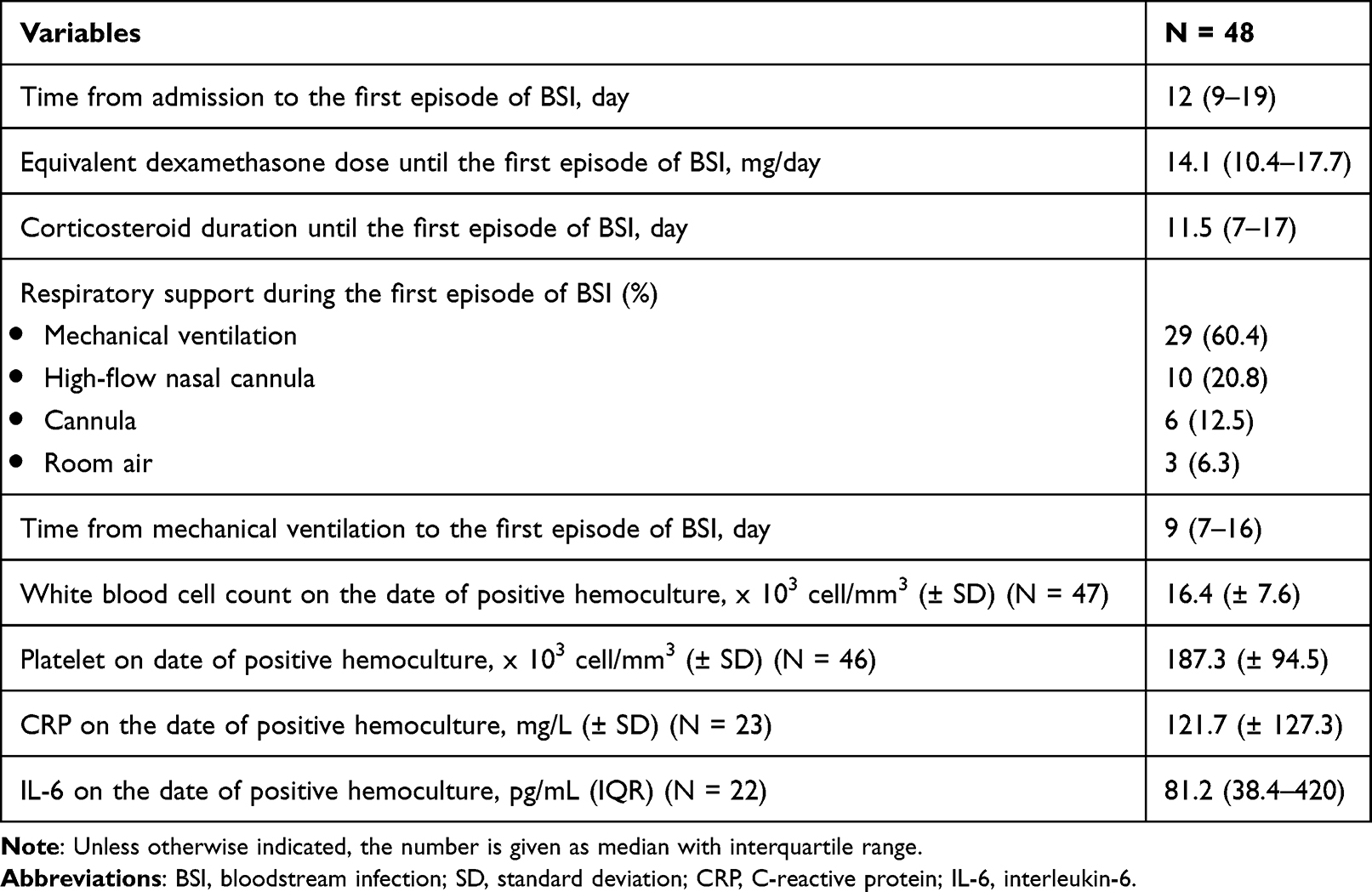 |
Table 4 Characteristics of the Nosocomial BSI Group |
According to univariate analysis, sex, COVID pneumonia diagnosis, SOFA, APACHE II, dexamethasone dosage, use of methylprednisolone, use of mechanical ventilation, receiving of hemoperfusion, white blood cell count, absolute lymphocyte count, and platelet count on admission were associated with nosocomial BSI. We chose APACHE II for the multivariate analysis after the multicollinearity test revealed that SOFA and APACHE II both had variance inflation factors larger than 2.5. In a multivariate analysis, the presence of leukocytosis is defined as white cell count ≥ 12×103 cell/mm3 on admission, being male, using methylprednisolone, taking a dose of dexamethasone equivalent to 6–12 mg/day were found to be significant predictors of nosocomial BSIs (Table 5).
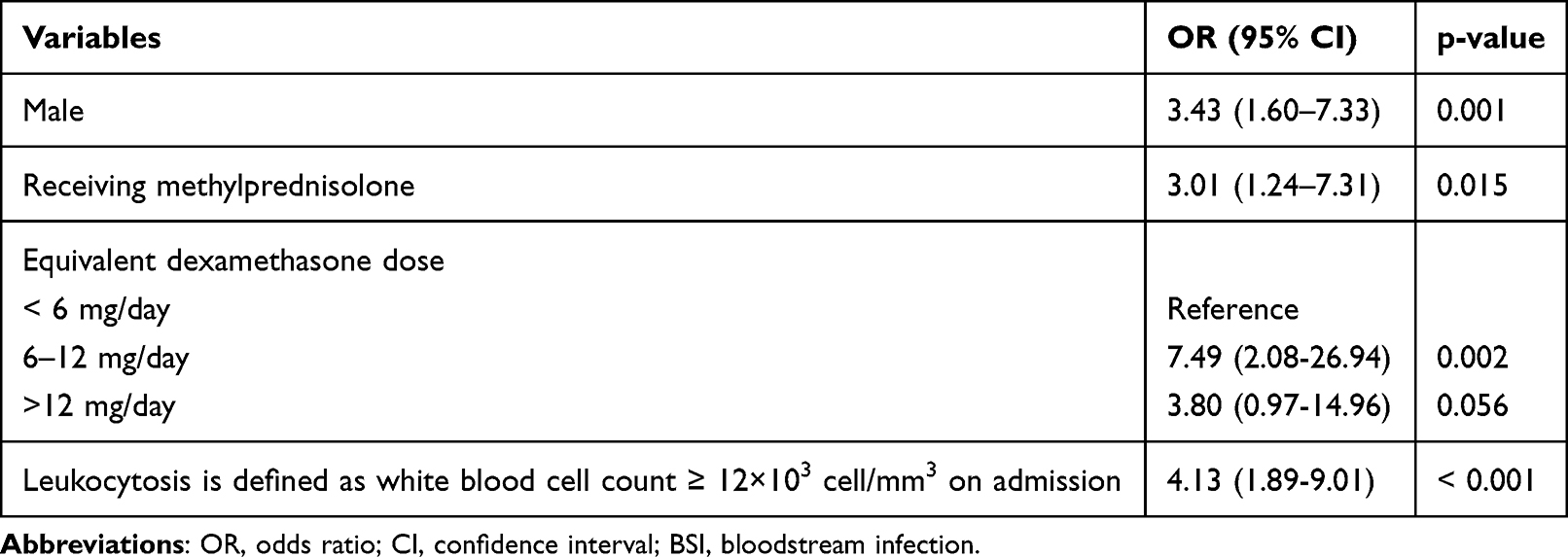 |
Table 5 Different Variables Associated with Nosocomial BSIs in Hospitalized Patients with COVID-19 in the Multivariate Analysis |
Patients who received a cumulative dose of > 12 mg/day had higher fatality rates than those who received 6–12 mg of dexamethasone per day (57.9% vs 15.2%). Moreover, patients who received a cumulative dose of > 12 mg of dexamethasone per day had a shorter median ICU stay than those who received a dose of 6–12 mg/day (13.5 days vs 17 days).
Forty-three patients (89.6%) experienced one episode of nosocomial BSI. The maximum number of episodes of nosocomial BSIs (five) occurred in one patient who underwent extracorporeal membrane oxygenation (ECMO); nonetheless, other patients (4 [8.3%]) experienced second episodes of nosocomial BSIs. Pneumonia (46.6%) was the most common source of infection, followed by primary BSI (20.7%), catheter-related BSI (10.3%), urinary tract infection (8.6%), intra-abdominal infection (8.6%), and skin and soft tissue infections (5.2%).
The five most common pathogens in this study were extended-spectrum beta-lactamase-producing Klebsiella pneumoniae (12.3%), methicillin-sensitive Staphylococcus aureus (12.3%), multidrug-resistant Acinetobacter baumannii (10.8%), Pseudomonas aeruginosa (9.2%), and Stenotrophomonas maltophilia (9.2%). Other pathogens of nosocomial BSI are shown in Table 6. The majority of nosocomial BSIs were monomicrobial (81.3%).
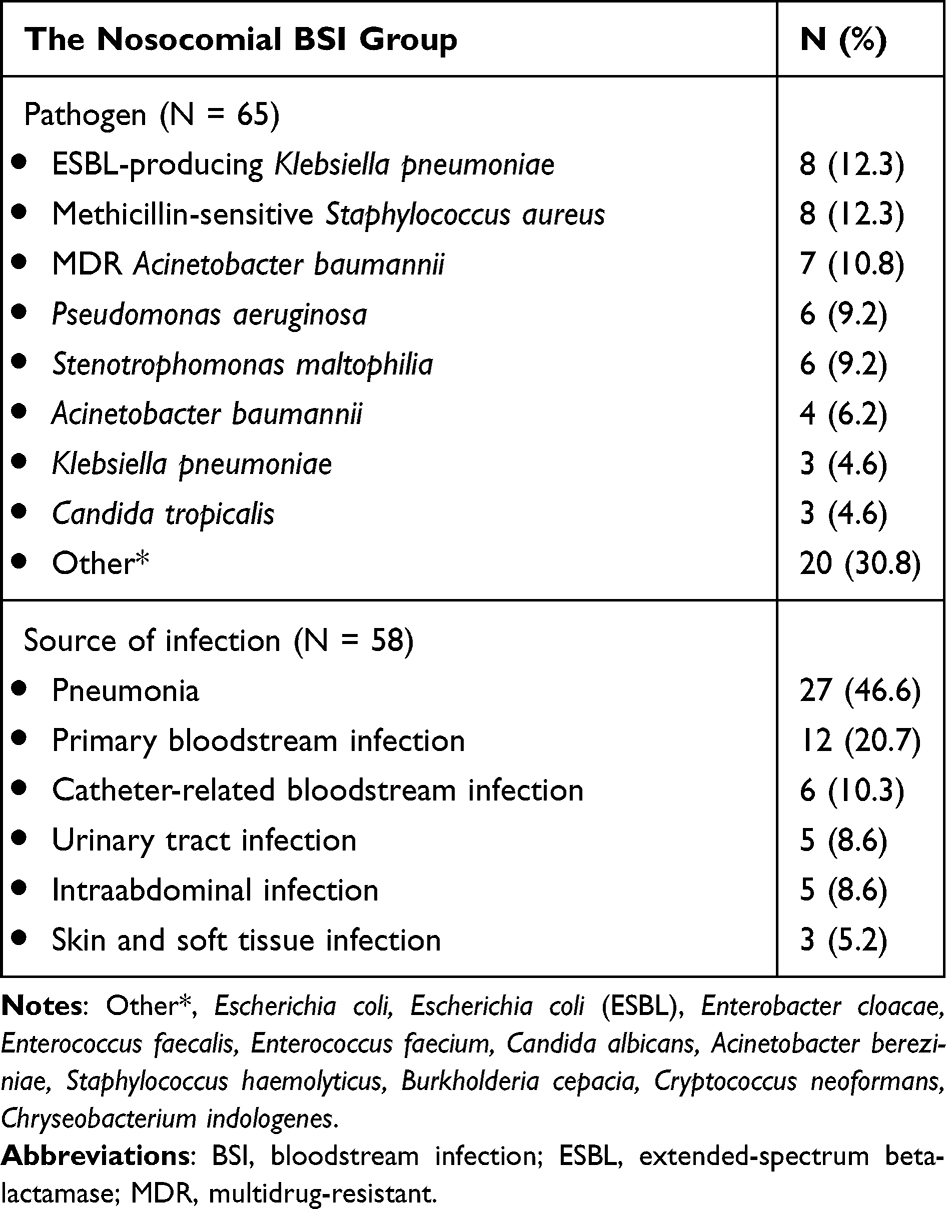 |
Table 6 Pathogen and Source of Infection |
Discussion
In our study, the male sex, receiving methylprednisolone, receiving an equal dexamethasone dose of 6–12 mg/day, and leukocytosis on admission were risk variables related to nosocomial BSIs. Notably, the median duration of nosocomial BSI occurred during the second week of corticosteroid therapy, duration from corticosteroid administration to the diagnosis of nosocomial BSIs was 11.5 days. This study determined that 6 mg per day of dexamethasone given over a maximum of 10 days was the safe dosage for COVID-19 patients.
Male sex is an unmodified risk variable for nosocomial BSI in our study. Similar findings from many studies indicated a male predominance in BSI.19–21 There are notable sex-specific differences in both the immunological and endocrine systems. The primary sex steroid hormones have effects on immune system cells in both the innate and adaptive immune systems.22 The theory suggests that the risk of BSI differs by sex because sex hormone levels in men and women change with aging. Men experience a progressive decline beginning in their second decade of life, but women experience a sudden decline during menopause.22
Patients receiving cumulative doses of > 12 mg of dexamethasone per day exhibited higher mortality rates and shorter ICU stays than those receiving doses of 6–12 mg/day. This may explain why cumulative dosages of > 12 mg of dexamethasone per day did not significantly increase the risk of superimposed nosocomial BSI. Patients who received > 12 mg of dexamethasone daily were at risk of severe pneumonia with multi-organ failure, which could result in death before BSI.
A recent systematic review and meta-analysis in 2021 by Ippolito et al23 revealed that the estimated incidence of BSIs in 46 studies was 7.3% with a mortality rate of 41%. The incidence of BSIs in the subgroup analysis of ICU patients was 29.6%. Meanwhile, our study revealed 19% of BSIs in all hospitalized patients with COVID-19, and the majority (81.4%) of the study population were admitted to the ICU. The mortality rate of nosocomial BSIs in our study was 62.5% higher than that reported in the systematic review.
Between 2020 and 2021, three randomized control trials including the Recovery trial,3 the CoDEX trial,24 and the COVID STEROID 2 trial25 that examined the therapeutic efficacy of corticosteroids in hospitalized COVID-19 patients were published. None of these trials found evidence of an elevated risk of nosocomial BSI. The duration of dexamethasone treatment in the previous three randomized control trials was not longer than 10 days, in contrast to our study, where patients in the nosocomial BSI group had a longer duration of 11.5 days from corticosteroid administration to the diagnosis of nosocomial BSIs and a total of 21.5 days of corticosteroid treatment. However, based on these three important trials, the dexamethasone dosing regimen was altered to 6, 10, 12, and 20 mg/day. As a result, in our study, the attending physicians determine the dexamethasone dose for hospitalized COVID-19 patients. Additionally, the doctor may have prescribed dexamethasone for a longer duration due to the severity of our patient’s conditions and the constantly high levels of inflammatory markers.
A case-cohort study of a multicentric OUTCOMEREA network by Buetti et al11 revealed that patients with COVID-19 admitted to six ICUs in France between January and October 2020 had a higher risk of developing ICU-BSI (14.9%) than those without COVID-19 (3.4%). Moreover, ICU-BSIs in patients with COVID-19 occurred within a median of 12 days, which is similar to the period for BSI occurrence in our study. The previous study revealed that patients who received tocilizumab had a noticeably higher probability of developing an ICU-BSI. In contrast, tocilizumab was not associated with nosocomial BSI in our study. This difference may be due to the prior study’s methodology, which compared the COVID-19 and non-COVID-19 groups, whereas our analysis focused exclusively on patients with COVID-19. Additionally, < 20% of patients with COVID-19 in our trial who were in the BSI and non-BSI groups used tocilizumab. In contrast to our investigation, a previous study discovered that the risk of ICU-BSI was not significantly increased by the use of corticosteroids over a shorter length of the initial two ICU days. Additionally, this study did not indicate the corticosteroid dosage.
The BSI incidence rate was found to be 50.2 per 1000 patient-days in a study conducted by Kurt et al.26 ECMO, methylprednisolone, tocilizumab, and continuous renal replacement therapy (CRRT) were independent risk factors for BSI in ICU patients. In comparison with our study, which performed CRRT at a rate of 4% and used tocilizumab at a rate of 12.7%, this study exhibited higher treatment rates for CRRT 31.9% and the use of tocilizumab 33%.
A study by Palanisamy et al27 conducted in a tertiary care COVID-ICU referral center in India revealed that 8.5% of 750 patients with severe COVID-19 admitted to the ICU developed secondary BSIs, indicating a lower incidence of BSI than that in our study. The factors significantly associated with BSIs in the multivariate analysis were increased total leukocyte count, mechanical ventilation, and the presence of comorbidities. A result similar to that of our study was that leukocytosis was significantly associated with BSIs, whereas tocilizumab use was not associated with BSI incidence. In a study by Palanisamy et al, corticosteroids were administered to all patients as part of the standard treatment regimen for severe COVID-19. However, their study did not evaluate corticosteroid doses related to BSIs. Our study revealed that an equivalent dexamethasone dose of 6–12 mg per day was associated with nosocomial BSI.
To the best of our knowledge, none of the previous studies have explored the association between the dose of corticosteroids used for the treatment of COVID-19 and the emergence of secondary nosocomial BSI; hence, our study is the first to investigate this association. Additionally, there were no missing data regarding the administration of methylprednisolone or corticosteroid dosage, which represented good accuracy of the primary outcome.
Moreover, good hospital infection control is of paramount importance to ensure patient safety and prevent the spread of healthcare-associated infections. Numerous pathogens, such as Acinetobacter baumannii and Stenotrophomonas maltophilia, can be acquired within the hospital environment or during medical interventions, leading to BSI and other serious complications. Therefore, infection control protocols are essential to provide high-quality care and maintain the integrity of healthcare systems.
This study had certain limitations. First, because the data were gathered at a single center, the management of the protocol may be different from that of other centers. Second, the ICU standard of care and healthcare experience may change depending on the study period. Lastly, we focused only on nosocomial BSI; therefore, our results did not reflect other hospital-acquired infections such as hospital-acquired pneumonia.
Conclusion
Unmodified risk variables for nosocomial BSIs included male sex and leukocytosis at admission. Using methylprednisolone and obtaining a cumulative dosage of dexamethasone were adjusted risk variables associated with superimposed nosocomial BSI in hospitalized patients with COVID-19. Therefore, the cornerstone of treatment is to choose the correct corticosteroid dose. Furthermore, because nosocomial BSIs contribute to increasing hospital mortality, physicians should carefully consider the administration of methylprednisolone if there is no clear indication.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lu H, Stratton CW, Tang YW. Outbreak of pneumonia of unknown etiology in Wuhan, China: the mystery and the miracle. J Med Virol. 2020;92(4):401–402. doi:10.1002/jmv.25678
2. Costela-Ruiz VJ, Illescas-Montes R, Puerta-Puerta JM, Ruiz C, Melguizo-Rodriguez L. SARS-CoV-2 infection: the role of cytokines in COVID-19 disease. Cytokine Growth Factor Rev. 2020;54:62–75. doi:10.1016/j.cytogfr.2020.06.001
3. Group RC, Horby P, Lim WS, et al. Dexamethasone in Hospitalized Patients with Covid-19. N Engl J Med. 2021;384(8):693–704.
4. Guimaraes PO, Quirk D, Furtado RH, et al. Tofacitinib in patients hospitalized with Covid-19 pneumonia. N Engl J Med. 2021;385(5):406–415. doi:10.1056/NEJMoa2101643
5. Rosas IO, Brau N, Waters M, et al. Tocilizumab in hospitalized patients with severe Covid-19 pneumonia. N Engl J Med. 2021;384(16):1503–1516. doi:10.1056/NEJMoa2028700
6. Selvaraj V, Finn A, Lal A, Khan MS, Dapaah-Afriyie K, Carino GP. Baricitinib in hospitalised patients with COVID-19: a meta-analysis of randomised controlled trials. EClinicalMedicine. 2022;49:101489. doi:10.1016/j.eclinm.2022.101489
7. McNamara JF, Righi E, Wright H, Hartel GF, Harris PNA, Paterson DL. Long-term morbidity and mortality following bloodstream infection: a systematic literature review. J Infect. 2018;77(1):1–8. doi:10.1016/j.jinf.2018.03.005
8. Santoro A, Franceschini E, Meschiari M, et al. Epidemiology and risk factors associated with mortality in consecutive patients with bacterial bloodstream Infection: impact of MDR and XDR bacteria. Open Forum Infect Dis. 2020;7(11):ofaa461. doi:10.1093/ofid/ofaa461
9. Garrouste-Orgeas M, Timsit JF, Tafflet M, et al. Excess risk of death from intensive care unit-acquired nosocomial bloodstream infections: a reappraisal. Clin Infect Dis. 2006;42(8):1118–1126. doi:10.1086/500318
10. Tabah A, Koulenti D, Laupland K, et al. Characteristics and determinants of outcome of hospital-acquired bloodstream infections in intensive care units: the EUROBACT International Cohort Study. Intensive Care Med. 2012;38(12):1930–1945. doi:10.1007/s00134-012-2695-9
11. Buetti N, Ruckly S, de Montmollin E, et al. COVID-19 increased the risk of ICU-acquired bloodstream infections: a case-cohort study from the multicentric OUTCOMEREA network. Intensive Care Med. 2021;47(2):180–187. doi:10.1007/s00134-021-06346-w
12. Osaki S, Kikuchi K, Moritoki Y, et al. Distinguishing coagulase-negative Staphylococcus bacteremia from contamination using blood-culture positive bottle detection pattern and time to positivity. J Infect Chemother. 2020;26(7):672–675. doi:10.1016/j.jiac.2020.02.004
13. Roberts FJ. Definition of polymicrobial bacteremia. Rev Infect Dis. 1989;11(6):1029–1030. doi:10.1093/clinids/11.6.1029
14. Liu D, Ahmet A, Ward L, et al. A practical guide to the monitoring and management of the complications of systemic corticosteroid therapy. Allergy Asthma Clin Immunol. 2013;9(1):30. doi:10.1186/1710-1492-9-30
15. Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity of disease classification system. Crit Care Med. 1985;13(10):818–829. doi:10.1097/00003246-198510000-00009
16. Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (sepsis-3). JAMA. 2016;315(8):801–810. doi:10.1001/jama.2016.0287
17. Gupta RK, Harrison EM, Ho A, et al. Development and validation of the ISARIC 4C Deterioration model for adults hospitalised with COVID-19: a prospective cohort study. Lancet Respir Med. 2021;9(4):349–359. doi:10.1016/S2213-2600(20)30559-2
18. Kidney Disease: Improving Global Outcomes Blood Pressure Work G. KDIGO 2021 clinical practice guideline for the management of blood pressure in chronic kidney disease. Kidney Int. 2021;99(3S):S1–S87. doi:10.1016/j.kint.2020.11.003
19. Esper AM, Moss M, Lewis CA, Nisbet R, Mannino DM, Martin GS. The role of infection and comorbidity: factors that influence disparities in sepsis. Crit Care Med. 2006;34(10):2576–2582. doi:10.1097/01.CCM.0000239114.50519.0E
20. Laupland KB, Gregson DB, Zygun DA, Doig CJ, Mortis G, Church DL. Severe bloodstream infections: a population-based assessment. Crit Care Med. 2004;32(4):992–997. doi:10.1097/01.CCM.0000119424.31648.1E
21. Mohus RM, Gustad LT, Furberg AS, et al. Explaining sex differences in risk of bloodstream infections using mediation analysis in the population-based HUNT study in Norway. Sci Rep. 2022;12(1):8436. doi:10.1038/s41598-022-12569-8
22. Giefing-Kroll C, Berger P, Lepperdinger G, Grubeck-Loebenstein B. How sex and age affect immune responses, susceptibility to infections, and response to vaccination. Aging Cell. 2015;14(3):309–321. doi:10.1111/acel.12326
23. Ippolito M, Simone B, Filisina C, et al. Bloodstream infections in hospitalized patients with COVID-19: a systematic review and meta-analysis. Microorganisms. 2021;9(10):2016. doi:10.3390/microorganisms9102016
24. Tomazini BM, Maia IS, Cavalcanti AB, et al. Effect of dexamethasone on days alive and ventilator-free in patients with moderate or severe acute respiratory distress syndrome and COVID-19: the CoDEX randomized clinical trial. JAMA. 2020;324(13):1307–1316. doi:10.1001/jama.2020.17021
25. Group CST, Munch MW, Myatra SN, et al. Effect of 12 mg vs 6 mg of dexamethasone on the number of days alive without life support in adults with COVID-19 and severe hypoxemia: the COVID STEROID 2 randomized trial. JAMA. 2021;326(18):1807–1817. doi:10.1001/jama.2021.18295
26. Kurt AF, Mete B, Urkmez S, et al. Incidence, risk factors, and prognosis of bloodstream infections in COVID-19 patients in intensive care: a single-center observational study. J Intensive Care Med. 2022;37(10):1353–1362. doi:10.1177/08850666221103495
27. Palanisamy N, Vihari N, Meena DS, et al. Clinical profile of bloodstream infections in COVID-19 patients: a retrospective cohort study. BMC Infect Dis. 2021;21(1):933. doi:10.1186/s12879-021-06647-x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Risk Factors for Mortality and Outcomes in Hematological Malignancy Patients with Carbapenem-Resistant Klebsiella pneumoniae Bloodstream Infections
Meng H, Han L, Niu M, Xu L, Xu M, An Q, Lu J
Infection and Drug Resistance 2022, 15:4241-4251
Published Date: 4 August 2022
Increased Incidence and Risk Factors of Infections by Extended-Spectrum β-Lactamase-Producing Enterobacterales During the COVID-19 Pandemic: A Retrospective Case-Control Study
Geng Y, Li F, Chen C, Liu Z, Ma X, Su X, Meng H, Lu W, Wang X, Pan D, Liang P
Infection and Drug Resistance 2023, 16:4707-4716
Published Date: 20 July 2023
Internet Addiction and COVID-19 Misbeliefs Among Hungarian Online Gamers: A Cross-Sectional Study
Nemes A, Szok D, Tibold A, Kosa G, Kapus K, Berke G, Banko Z, Feher G
Journal of Multidisciplinary Healthcare 2024, 17:2351-2358
Published Date: 15 May 2024
Development and Validation of Nomograms for Predicting Pneumonia in Patients with COVID-19 and Lung Cancer
Xu Y, Li H, Wang X, Li B, Gao A, Zhao Q, Yang L, Qin W, Wang L
Journal of Inflammation Research 2024, 17:3671-3683
Published Date: 7 June 2024
Risk Factors for Secondary Organizing Pneumonia and Acute Fibrinous and Organizing Pneumonia in Patients with COVID-19 Pneumonia
Aikwanich A, Eksombatchai D, Petnak T, Tassaneeyasin T, Boonsarngsuk V
Infection and Drug Resistance 2024, 17:5017-5026
Published Date: 11 November 2024