Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Development and Preliminary Validation of an Oral Health Multidisciplinary Team Nurse Competency Scale
Authors Jiang Y, Wu S, Dong Y, Zhong K, Cao L
Received 9 March 2026
Accepted for publication 5 May 2026
Published 30 May 2026 Volume 2026:19 605940
DOI https://doi.org/10.2147/JMDH.S605940
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Veronica Swallow
Yan Jiang,1,* Shan Wu,2,* Yinyin Dong,2 Kun Zhong,3 Liu Cao4
1Multidisciplinary Dental Clinic, Stomatological Hospital of Guizhou Medical University, Guiyang, Guizhou, 550004, People’s Republic of China; 2Department of Nursing, Stomatological Hospital of Guizhou Medical University, Guiyang, Guizhou, 550004, People’s Republic of China; 3Comprehensive Oral Emergency Department, Stomatological Hospital of Guizhou Medical University, Guiyang, Guizhou, 550004, People’s Republic of China; 4Periodontal and Mucosal Diseases Department, Stomatological Hospital of Guizhou Medical University, Guiyang, Guizhou, 550004, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Shan Wu, Department of Nursing, Stomatological Hospital of Guizhou Medical University, No. 9 Beijing Road, Yunyan District, Guiyang, Guizhou, 550004, People’s Republic of China, Email [email protected]
Background: Oral health multidisciplinary team (OHMDT) care places nurses in a coordinating role across specialties, but the absence of a context-specific assessment tool limits training evaluation, competency benchmarking, and quality improvement. This study aimed to develop and preliminarily validate an OHMDT nurse competency scale.
Methods: We conducted a mixed-methods instrument-development study with two phases. First, an item pool derived from a systematic literature review was refined through two Delphi rounds with a multidisciplinary expert panel (n = 16). Second, a cross-sectional survey was administered to OHMDT nurses from three hospitals of different levels in Guizhou, China (September-December 2025). The final analytic sample included 120 nurses, and 25 completed a 2-week retest. Psychometric evaluation included content validity, item analysis, exploratory factor analysis using principal axis factoring with promax rotation, internal consistency, test-retest reliability, floor and ceiling effects, and known-groups validity.
Results: The final scale contained 23 items. Content validity was high (S-CVI/Ave = 0.93). Exploratory factor analysis supported a four-factor structure (KMO = 0.87; Bartlett’s χ2 [253] = 824.63, p < 0.001) explaining 47.3% of total variance. The total scale showed high internal consistency (Cronbach’s alpha = 0.895) and good 2-week stability (ICC[3,1] = 0.884; 95% CI: 0.756– 0.947). No floor or ceiling effects were observed. Total scores were higher among nurses with longer OHMDT experience (t[69] = − 9.59, p < 0.001, Cohen’s d = 2.32) and differed significantly across professional titles (F[3,116] = 41.01, p < 0.001, η2= 0.515).
Conclusion: The OHMDT Nurse Competency Scale showed promising reliability and preliminary validity in this single-province sample. At the current stage, it is best used for research, baseline assessment, or preliminary clinical screening rather than high-stakes standalone decisions. Larger multicenter studies with confirmatory factor analysis and criterion validation are needed.
Keywords: oral health multidisciplinary team, nurse competency, scale development, psychometric validation, reliability, validity, factor analysis
Introduction
Oral health multidisciplinary team (OHMDT) care is increasingly used in the management of complex oral and maxillofacial conditions that require coordinated input from multiple specialties, including oral cancer, maxillofacial trauma, advanced periodontal disease, and complex reconstructive care.1–5 In Chinese tertiary hospitals and stomatology specialty centers, these cases are often concentrated in settings where multiple disciplines participate in diagnosis, treatment planning, intervention, rehabilitation, and follow-up. Under this care model, nurses do more than provide routine peri-treatment care; they also support cross-specialty coordination, patient education, psychosocial communication, and implementation of team decisions.6–8
These practice demands are not fully captured by generic nursing competency instruments. Established tools such as the Nurse Competence Scale and related professional self-assessment instruments were developed for broad nursing settings rather than the specific workflow of multidisciplinary oral healthcare.9–14 They provide valuable general benchmarks, but they do not directly operationalize competencies such as cross-specialty scheduling, oral-treatment pathway coordination, multidisciplinary communication, and continuity management across OHMDT encounters. As a result, the lack of a context-specific instrument limits objective evaluation of nurse performance, identification of training priorities, and generation of evidence linking OHMDT nursing competence to care processes and outcomes.
In this study, we use the more explicit term oral health multidisciplinary team (OHMDT) for structured collaboration among oral and maxillofacial surgery, periodontics, endodontics, prosthodontics, orthodontics, radiology, pathology, oncology, reconstructive surgery, and specialized nursing. The participating centers often referred to this model locally as OMDT, but the present manuscript uses OHMDT to make the setting clearer to an international readership. The participating centers applied this model mainly to complex conditions that required concurrent specialist input rather than sequential referral. Within these teams, nurses commonly functioned as operational coordinators who supported case preparation, information transfer, patient counseling, peri-treatment management, and follow-up implementation.
We conceptualized OHMDT nurse competency as an integrated construct that includes knowledge, skills, attitudes, and professional behaviors needed to coordinate and deliver safe multidisciplinary oral healthcare.15,16 Because this construct had not been translated into a psychometrically evaluated instrument for OHMDT practice, we developed an OHMDT Nurse Competency Scale and conducted a preliminary psychometric evaluation. Specifically, we aimed to (1) generate and refine competency items through literature review and expert consensus, (2) examine the exploratory factor structure, (3) assess reliability, and (4) evaluate known-groups validity.
Methods
Study Design
We conducted a mixed-methods instrument-development and preliminary validation study with two sequential phases: (1) item generation and content refinement through a two-round Delphi process and (2) cross-sectional psychometric testing through a questionnaire survey. The study was designed with reference to the COnsensus-based Standards for the selection of health Measurement INstruments (COSMIN) framework for instrument development and psychometric evaluation.17
Setting and Participants
The validation phase was performed in three hospitals in Guizhou Province, China, between September and December 2025, including one Grade II hospital and two Grade III hospitals. Eligible participants were registered nurses who had participated in OHMDT-related clinical work, such as multidisciplinary case discussion support, peri-treatment coordination, or implementation of coordinated care plans. Nurses on extended leave during the study period and questionnaires with substantial missing data that prevented scoring were excluded.
Paper questionnaires were distributed by trained research staff after permission was obtained from participating departments. Participants completed the questionnaires independently, without supervisors present, and were informed that the survey was anonymous, voluntary, and had no right or wrong answers. These procedures were used to reduce social desirability pressure and duplicate submission risk. Because recruitment depended on department-facilitated access and nurse availability during the survey window rather than random sampling, nurses who were more engaged in OHMDT work, more available on duty days, or more willing to participate may have been overrepresented. A total of 130 questionnaires were distributed, 125 were returned, and 5 were excluded because of excessive missing data, yielding a final analytic sample of 120 nurses.
Because this study was exploratory and focused on scale development rather than confirmatory model testing, no separate hypothesis-testing power calculation was performed. Sample planning instead followed commonly used subject-to-item guidance for exploratory factor analysis. For a 23-item scale, the minimum 5:1 ratio suggested a target of at least 115 participants.18,19 We therefore aimed for 120 completed questionnaires to accommodate incomplete responses. We recognize that this sample size is sufficient for preliminary exploratory work but remains below what is generally preferred for stable confirmatory factor analysis.
For test-retest reliability, a convenience subsample of 25 participants completed the same instrument again after 2 weeks. Participants were not shown their earlier responses.
Development of the OHMDT Nurse Competency Scale
Item Pool Construction
An initial item pool was generated from (1) a systematic review of competency-related literature in oral nursing, multidisciplinary care, and interprofessional practice and (2) research-team discussion of competencies commonly required in OHMDT workflows. Searches were conducted in PubMed, CINAHL, Web of Science, CNKI, and Wanfang using combinations of the terms “multidisciplinary team”, “oral nursing”, “nursing competency”, “competency scale”, and “interprofessional care”. The search window covered publications from 2000 to 2023 in English and Chinese. A total of 94 articles were reviewed, yielding an initial pool of 45 items across five candidate dimensions. Item wording was behavior-oriented to favor observable practice over abstract trait endorsement.20–22
Delphi Expert Consultation and Content Refinement
Content validation and item refinement were conducted with a multidisciplinary Delphi panel (n = 16). Experts were eligible if they had at least 10 years of relevant clinical or academic experience, held a senior professional title, and were familiar with OHMDT practice or nursing competency assessment. The panel comprised 9 head nurses, 4 nursing specialists, 2 nursing directors, and 1 oral department director. Expert authority was quantified using the authority coefficient (Cr), calculated as the mean of the familiarity coefficient and the judgment coefficient; the mean Cr was 0.695 (range: 0.550–0.850). Although this value was close to the conventional 0.70 benchmark, we treated it as a modest limitation rather than over-interpreting it as unequivocally high authority.
Consensus was defined a priori as an item importance mean of at least 3.5 on a 5-point scale together with a coefficient of variation of 0.25 or less. In Round 1, experts rated the 45 candidate items and provided written comments on wording, redundancy, and missing content. After consolidating feedback, deleting redundant items, and revising clinically unclear phrasing, 28 items were retained for Round 2. In Round 2, experts re-evaluated the revised pool for relevance and comprehensiveness. After Round 2, five additional items were removed because of redundancy, insufficient consensus, or limited conceptual distinctiveness, yielding a 23-item field-test version for psychometric evaluation. Item-level content validity indices (I-CVI) and the average scale-level content validity index (S-CVI/Ave) were calculated, and Kendall’s coefficient of concordance (W) was used to describe inter-expert agreement in each round.
Data Collection Procedures
The survey package included participant characteristics and the draft OHMDT Nurse Competency Scale. Questionnaires with more than 20% missing items were excluded. To reduce socially desirable responding, items were phrased as competency-related behaviors rather than moralized self-judgments, participants completed the survey anonymously, and no supervisor was present during completion. These steps do not eliminate self-report bias, but they provide practical procedural controls for a paper-based field survey.
Psychometric Evaluation
Item Analysis
Item performance was examined using critical-ratio comparisons between higher- and lower-scoring groups, corrected item-total correlations, and alpha-if-deleted statistics. Items with corrected item-total correlations below 0.30 would have been considered for removal if their deletion improved internal consistency without sacrificing content coverage.23
Exploratory Factor Analysis
Sampling adequacy was evaluated using the Kaiser-Meyer-Olkin measure and Bartlett’s test of sphericity. Factors were extracted by principal axis factoring with promax oblique rotation because competency domains were expected to correlate in practice.23–25 The number of factors was judged by the Kaiser criterion, scree-plot inspection, and theoretical interpretability.26 For field-testing decisions, items were considered retainable when the primary loading was at least 0.40 and the difference between the primary and highest secondary loading was greater than 0.20.27 Items that approached but did not fully satisfy these thresholds were reviewed against the Delphi framework and retained only when their content was non-redundant and item-level performance remained acceptable The 23-item field-test version was entered into EFA. No additional items were deleted after EFA; therefore, the 23-item field-tested version was retained as the final preliminary instrument.
Reliability
Internal consistency was assessed using Cronbach’s alpha for the total scale and subscales.28–30 Test-retest reliability was estimated using a two-way mixed-effects intraclass correlation coefficient for absolute agreement, single measures, that is, ICC(3,1).31
Known-groups validity. Known-groups validity was examined by comparing total scores across groups expected to differ in OHMDT competence: nurses with less than 2 years versus at least 5 years of OHMDT experience, and nurses grouped by professional title. To maximize contrast for the primary t test, the experience comparison focused on the two end groups, whereas the 2–4 year group was retained for descriptive reporting in the Results section.32
Statistical Analysis
Continuous variables were summarized as mean ± standard deviation and categorical variables as n (%). Normality was assessed using the Shapiro–Wilk test together with skewness and kurtosis. Floor and ceiling effects were defined as the percentage of participants scoring at the minimum or maximum possible total score, with values above 15% considered substantial.33 All tests were two-sided with a significance threshold of p <0.05.
Results
Participant Characteristics
The final analytic sample included 120 OHMDT nurses. Participants were predominantly female and represented a range of educational and professional backgrounds. Mean age was 36.8 ± 8.3 years, mean oral nursing experience was 10.3 ± 5.7 years, and mean OHMDT work experience was 2.7 ± 2.1 years. Most participants held junior-college or bachelor’s degrees and were concentrated at the charge-nurse level. Detailed characteristics are shown in Table 1. Figure 1 summarizes the demographic distributions.
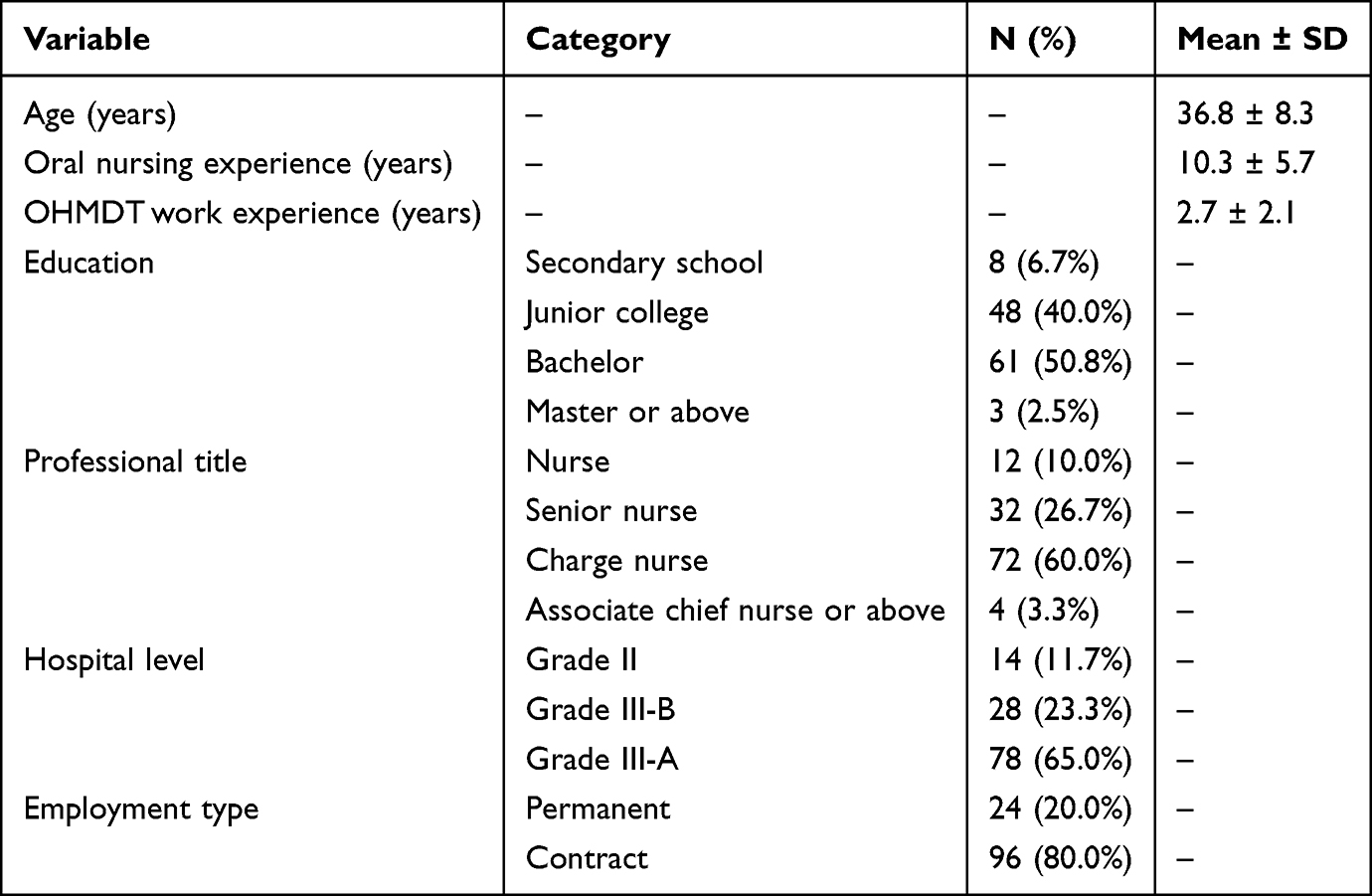 |
Table 1 Demographics and Professional Characteristics of OHMDT Nurses (N = 120) |
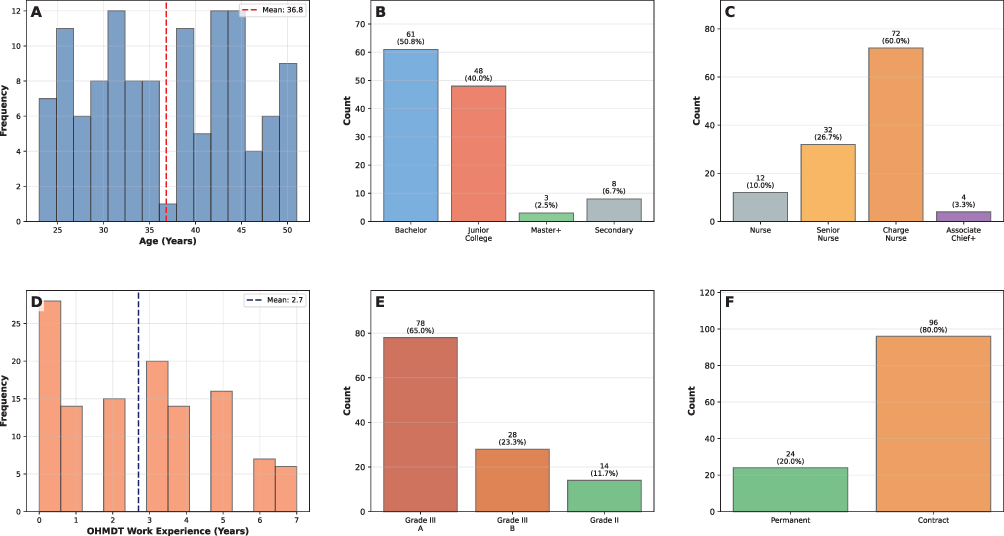 |
Figure 1 Demographics of OHMDT Nurses. (A) Shows age distribution, with the dashed line indicating the mean age of 36.8 years. (B) Shows education level distribution. (C) Shows professional-title categories. (D) Shows OHMDT work experience, with the dashed line indicating the mean value of 2.7 years. (E) Shows hospital level distribution, and (F) Shows employment type distribution. |
Delphi Consultation Results
Expert response rates were 100% in both Delphi rounds. Authority coefficients ranged from 0.55 to 0.85 (mean Cr = 0.695). In Round 1, Kendall’s W was 0.082 (χ2[44] = 58.05, p =0.076). After Round 1, the initial 45-item pool was reduced to 28 items for Round 2. Round 2 yielded Kendall’s W = 0.057 (χ2[27] = 24.44, p =0.606). Following Round 2, five further items were removed, resulting in a 23-item field-test version. These 23 items showed I-CVI values of 0.75–1.00, and the S-CVI/Ave was 0.93. These findings supported content relevance while also indicating that rank-order agreement among experts was limited in this emerging competency domain.
Item Analysis
All 23 items demonstrated acceptable discrimination between high- and low-scoring groups, and corrected item-total correlations ranged from 0.356 to 0.700 (Table 2). Deleting any single item did not materially improve the total-scale alpha. Q10 showed the lowest corrected item-total correlation (r = 0.356) but was retained because its discrimination remained significant and its content was judged central to cross-department coordination.
 |
Table 2 Item Analysis Results (N = 120) |
Exploratory Factor Analysis
The data were suitable for factor analysis (KMO = 0.87; Bartlett’s χ2[253] = 824.63, p <0.001). Harman’s single-factor test showed that the first unrotated component explained 30.9% of total variance, below the 50% threshold commonly used as a rough screen for severe common-method bias.33
Initial eigenvalues from the full correlation matrix were lambda-1 = 7.098, lambda-2 = 1.333, lambda-3 = 1.213, lambda-4 = 1.161, lambda-5 = 1.092, and lambda-6 = 1.023. Although the Kaiser criterion alone would have retained 6 factors, the scree plot showed a marked elbow after the first component and a smaller break after the fourth component. On balance, and in conjunction with the Delphi-derived conceptual framework, a 4-factor solution was retained. The 4 retained factors explained 47.3% of total variance (Table 3; Figure 2).
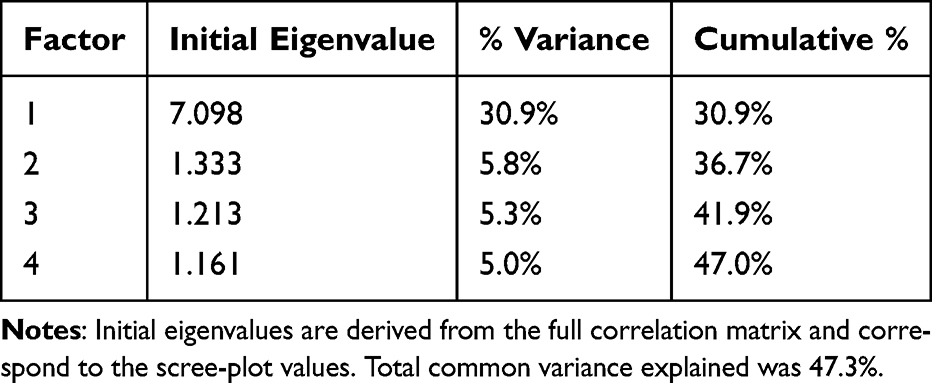 |
Table 3 Eigenvalues and Variance Explained by Retained Factors |
 |
Figure 2 Scree Plot for Factor Number Determination. Observed eigenvalues are plotted against factor order. The first four components exceeded the Kaiser criterion of lambda = 1.0, while the visual elbow supported a more conservative interpretation than the raw Kaiser count alone. |
After promax rotation, most items showed their highest loading on conceptually coherent factors (Table 4). Several items displayed secondary cross-loadings, and a small number of communalities were low. Rather than treating these findings as contradictory, we interpreted them as evidence that OHMDT nursing competencies overlap in actual practice. Importantly, the 23 field-tested items were all retained after EFA because their item-level performance remained acceptable and several low-communality items represented non-redundant competencies endorsed by the expert panel. Figure 3 visualizes the loading pattern. The final 23-item English scale is provided in Appendix 1.
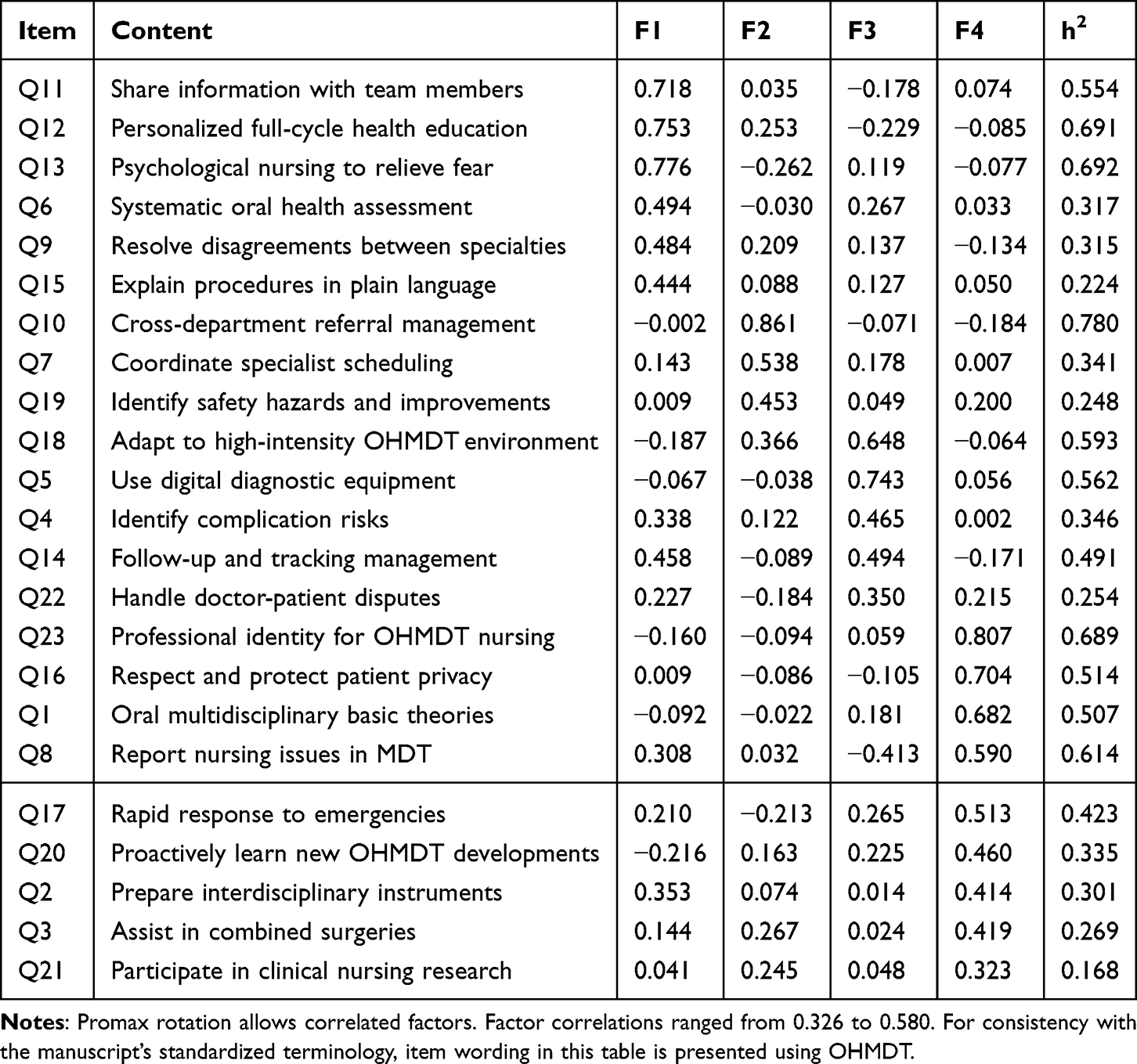 |
Table 4 Pattern Matrix After Promax Rotation (N = 120) |
 |
Figure 3 Pattern Matrix Heatmap After Promax Rotation. The heatmap displays the factor-loading pattern of the 23 items under the 4-factor exploratory solution. Warmer colors represent stronger positive loadings and cooler colors represent negative loadings. |
Reliability
The total scale demonstrated high internal consistency (alpha = 0.895). Subscale alpha values were 0.780, 0.614, 0.659, and 0.658, indicating that the total score was more robust than several subscale scores. The 2-week test-retest reliability in the 25-participant subsample was good (ICC[3,1] = 0.884; 95% CI: 0.756–0.947). Reliability results are presented in Table 5.
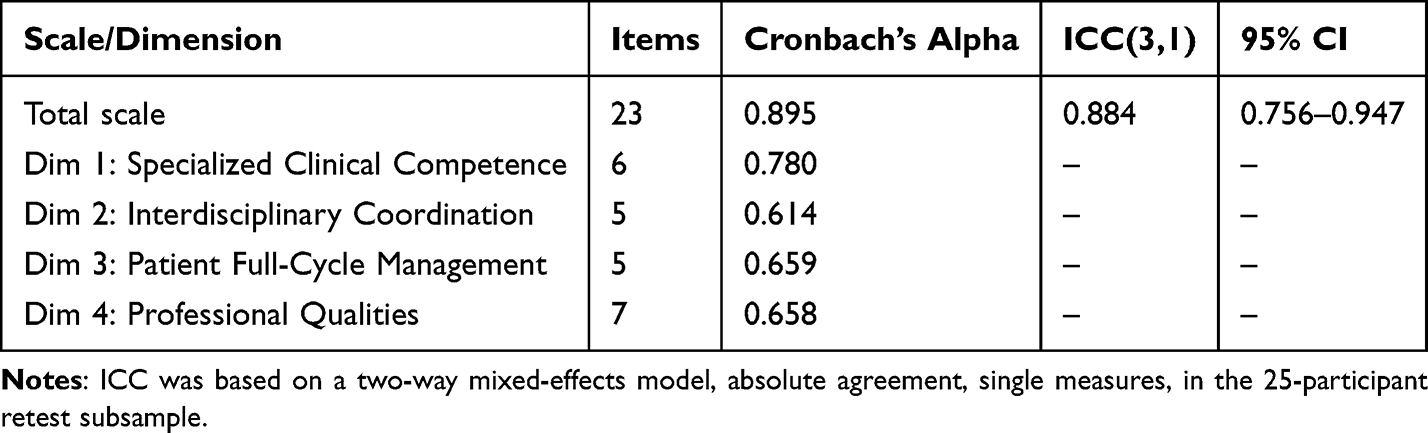 |
Table 5 Reliability Analysis Results |
Known-Groups Validity
Known-groups comparisons supported the expected direction of validity. Nurses with at least 5 years of OHMDT experience scored significantly higher than those with less than 2 years of experience (t[69] = −9.59, p <0.001, Cohen’s d = 2.32). Differences across professional-title groups were also significant (F[3,116] = 41.01, p <0.001, η2= 0.515). The intermediate 2–4 year experience group showed descriptive values between the two extreme groups. These findings are summarized in Table 6 and illustrated in Figure 4.
 |
Table 6 Known-Groups Validity Analysis |
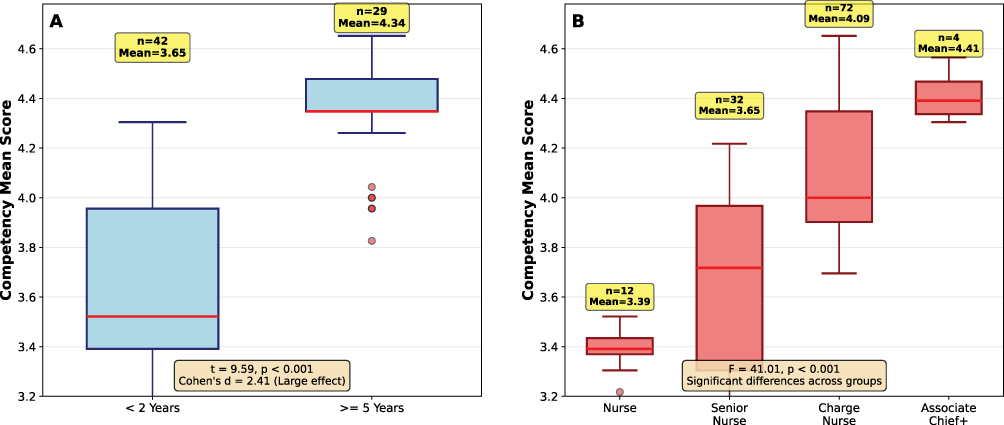 |
Figure 4 Known-Groups Validity Analysis. (A) Compares competency scores by OHMDT work-experience group. (B) Compares scores across professional-title groups. The figure illustrates the expected gradient of higher scores with greater experience and higher title. |
Discussion
This study describes the development and preliminary validation of a 23-item OHMDT Nurse Competency Scale for multidisciplinary oral healthcare settings. In the present sample, the instrument showed strong total-scale reliability and supportive evidence of validity from content review, item analysis, exploratory factor analysis, and known-groups comparisons. Taken together, these findings suggest that the scale captures a meaningful general competency construct while still requiring further structural confirmation.
A major contribution of the study is that it addresses a gap left by broader nursing competency instruments. Existing scales such as the Nurse Competence Scale and related professional self-assessment tools are useful for general nursing evaluation, but they do not directly target the cross-specialty workflow of oral multidisciplinary care.9,12,13 The current scale was built around this context, incorporating competencies such as referral coordination, multidisciplinary communication, patient full-cycle management, and adaptation to the OHMDT environment. In that sense, its value lies not in replacing generic competency tools, but in complementing them with content that is specific to multidisciplinary oral practice.
The Delphi process supported content validity, although it also revealed a degree of expert heterogeneity. The high S-CVI/Ave and acceptable I-CVI range suggest that experts broadly agreed on the relevance of the retained items. At the same time, the modest Kendall’s W values and mean Cr below 0.70 indicate that the panel did not yield uniformly strong rank-order consensus. We therefore interpret the Delphi findings cautiously: they support the relevance of the item pool, but they do not eliminate the need for further refinement and external validation.
The exploratory factor solution requires similarly careful interpretation. The empirically derived factors only partially matched the original theoretical dimensions, and this mismatch should not be treated as a failure of the scale. In multidisciplinary clinical work, domains such as communication, coordination, technical skill, ethics, and professional identity are intertwined. Items such as foundational theory, privacy protection, and patient communication may cluster differently in practice than they do in a conceptual outline. Our approach therefore prioritized transparent reporting over forced purity: we retained the 4-factor exploratory solution, acknowledged the overlap, and emphasized that the total score currently provides the clearest summary measure. This also explains why a total-score interpretation can coexist with an exploratory multidimensional structure. The first eigenvalue was substantially larger than the subsequent ones, suggesting an overarching general competency factor across items.
Several additional psychometric features deserve attention. A small number of items had lower communalities, and three subscales had alpha values below 0.70. These findings suggest that some domain scores are not yet stable enough for standalone interpretive use. By contrast, the total-scale alpha and the retest ICC indicate that the overall instrument performs better than its narrower components. For the current stage of development, this supports use of the total score as the primary metric and more cautious use of subscale scores.
The study also attempted to address expected bias mechanisms. Because the scale uses self-report items and all items are positively phrased, some inflation from social desirability or common response style remains possible. We used several procedural controls, including anonymous completion, no supervisor presence during administration, behavior-focused item wording, and explicit instructions that there were no correct or incorrect answers. These steps likely reduced pressure toward favorable responding, but they cannot fully eliminate self-report bias. The Harman single-factor result argues against severe common-method bias, yet that test is only a rough screening tool and should not be over-interpreted.
Clinical Applications
At its current stage, the scale may be useful in three practical ways. First, it can support baseline competency assessment in OHMDT services to identify broad strengths and weaknesses at the team or department level. Second, it may help guide training-program design by highlighting domains such as multidisciplinary communication, coordination, or patient full-cycle management that warrant targeted development. Third, it may serve quality-improvement work by offering a structured outcome for before-and-after educational initiatives. However, because several subscales remain only moderately reliable and criterion validity has not yet been established, the instrument should not be used in isolation for certification, promotion, or other high-stakes personnel decisions.
Limitations
Several limitations should be acknowledged. First, the sample size of 120 yields only a modest subject-to-item ratio for exploratory factor analysis and is insufficient for stable confirmatory factor analysis. Second, participants were recruited from three hospitals in a single province using department-facilitated, non-random sampling. Nurses who were more accessible during the survey window, more engaged in OHMDT practice, or more willing to complete a paper questionnaire may therefore have been more likely to participate, introducing potential selection bias in addition to limiting generalizability. Third, the instrument is self-reported and positively worded, leaving residual social desirability bias possible despite procedural precautions. Fourth, three subscales showed alpha values below 0.70, limiting their independent interpretability. Fifth, validity evidence in this study was limited to content, internal structure, and known-groups comparisons; convergent, discriminant, criterion, and predictive validity were not assessed. Finally, the highest professional-title group was small, which limits the stability of that comparison.
Future Directions
Future work should prioritize multicenter recruitment with larger samples, formal confirmatory factor analysis, and external validation against relevant outcomes. Additional studies should examine convergent validity with broader nursing competency measures, criterion validity with clinical-process or patient indicators, and responsiveness to training interventions. Refinement or expansion of lower-performing subscales may also improve the interpretability of domain-level scores.
Conclusions
We developed and preliminarily validated a 23-item OHMDT Nurse Competency Scale for multidisciplinary oral healthcare settings. The scale showed strong total-scale reliability and supportive preliminary validity in this single-province sample. At present, the total score is the most defensible interpretation target, whereas subscale scores should be used cautiously. The instrument is best viewed as suitable for research, baseline assessment, and preliminary clinical screening. Further multicenter validation, including confirmatory factor analysis and criterion-related testing, is needed before broader high-stakes application.
Data Sharing Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The study protocol was submitted to the Medical Ethics Management Committee of the Stomatological Hospital of Guizhou Medical University (Guiyang, China). Through expedited review, the committee concluded that this anonymous nurse questionnaire study did not involve medical ethical issues requiring formal ethics approval and issued a waiver notice. No formal ethics approval number was assigned. This study was conducted in accordance with the Declaration of Helsinki.
Consent to Participate
All participants were informed about the study purpose, voluntariness, anonymity, and confidentiality. Completion and return of the questionnaire were taken as implied informed consent to participate.
Acknowledgments
The authors thank the participating nurses and the Delphi experts for their time and contributions.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Guizhou Provincial Health Commission Science and Technology Fund Project (No. gzwkj2025-567); 2025 Guizhou Province Science and Technology Achievement Transformation and Industrialization Program (Clinical Special Project) Project: Qiankehe Achievement LC (2025) General 097.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Broom A, Kirby E, Good P. The geography of the clinical ethics industry: perspectives on multidisciplinary teams in Australian hospitals. Soc Sci Med. 2015;126:123–13.
2. Coulter A, Roberts S, Dixon A. Delivering Better Services for People with Long-Term Conditions: Building the House of Care. King’s Fund; 2013.
3. Oandasan I, Reeves S. Key elements of interprofessional education. Part 2: factors, processes and outcomes. J Interprof Care. 2005;19(Suppl 1):39–48. doi:10.1080/13561820500081703
4. Sargeant J, Loney E, Murphy G. Effective interprofessional teams: “Contact is not enough” to build a team. J Contin Educ Health Prof. 2008;28(4):228–234. doi:10.1002/chp.189
5. Nancarrow SA, Booth A, Ariss S, et al. Ten principles of good interdisciplinary team work. Hum Resour Health. 2013;11:19. doi:10.1186/1478-4491-11-19
6. Mitchell PH, Belza B, Schaad DC. From interdisciplinary to transdisciplinary: an elaboration of the nursing perspective on collaboration. J Prof Nurs. 2017;33(6):456–462.
7. Hall P. Interprofessional teamwork: professional cultures as barriers. J Interprof Care. 2005;19(Suppl 1):188–196. doi:10.1080/13561820500081745
8. Meretoja R, Isoaho H, Leino-Kilpi H. Nurse competence scale: development and psychometric testing. J Nurs Manag. 2004;12(1):9–22.
9. Cowan DT, Norman IJ, Coopamah VP. Competence in nursing practice: a controversial concept - A focused review of literature. Nurse Educ Today. 2005;25(5):355–362. doi:10.1016/j.nedt.2005.03.002
10. Costello AB, Osborne JW. Best practices in exploratory factor analysis: four recommendations for getting the most from your analysis. Pract Assess Res Eval. 2005;10(7):1–9.
11. Epstein RM, Hundert EM. Defining and assessing professional competence. JAMA. 2002;287(2):226–235. doi:10.1001/jama.287.2.226
12. Frank JR, Snell LS, Cate OT, et al. Competency-based medical education: theory to practice. Med Teach. 2010;32(8):638–645. doi:10.3109/0142159X.2010.501190
13. Liu Y, Zhang Y, Zhang J, et al. Development and psychometric testing of a nurse professional competence scale in China. J Adv Nurs. 2021;77(12):3325–3336.
14. Wang S, Li J, Zhang Y, et al. Development and validation of the Interprofessional Collaborative Competency Scale for Chinese nurses. Nurse Educ Today. 2022;114:105367.
15. Floyd FJ, Widaman KF. Factor analysis in the development and refinement of clinical assessment instruments. Psychol Assess. 1995;7(3):286–299. doi:10.1037/1040-3590.7.3.286
16. Nunnally JC, Bernstein IR. Psychometric Theory.
17. Meretoja R, Leino-Kilpi H, Kaira AM. Comparison of nurse competence in different hospital fields. J Nurs Manag. 2004;12(2):131–136. doi:10.1111/j.1365-2834.2004.00422.x
18. Wangensteen S, Johansson IS, Bjorkstrom ME. The nurse professional competence scale: development and psychometric testing in nurses. J Adv Nurs. 2018;74(11):2505–2517.
19. Goudarzian L, Bagheri F, Shafipour V. Challenges and recommendations of exploratory and confirmatory factor analysis: a narrative review from a nursing perspective. J Nurs Res Pract. 2023;7(1):184–260.
20. Lorenzo-Seva U, Ferrando PJ, Vigil-Colet A. Determining sample size requirements in EFA solutions: a trade-off between accuracy and efficiency. Psychol Methods. 2024;29(3):456–473.
21. Mokkink LB, Terwee CB, Patrick DL, et al. The COSMIN checklist for assessing the methodological quality of studies on measurement properties of health status measurement instruments: an international Delphi study. Qual Life Res. 2010;19(4):539–549. doi:10.1007/s11136-010-9606-8
22. MacCallum RC, Widaman KF, Zhang S, Hong S. Sample size in factor analysis. Psychol Methods. 1999;4(1):84–99. doi:10.1037/1082-989X.4.1.84
23. Tavakol S, Wetzel A, Dennick R. Factor analysis: a means for theory and instrument development in health care research. BMC Med Res Methodol. 2020;20:177. doi:10.1186/s12874-020-01059-y
24. Hair JF, Black WC, Babin BJ, Anderson RE. Multivariate Data Analysis.
25. Nunnally JC. Psychometric Theory.
26. Koo TK, Mae MY. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med. 2016;15(2):155–163. doi:10.1016/j.jcm.2016.02.012
27. Cohen J. Statistical Power Analysis for the Behavioral Sciences.
28. Podsakoff PM, MacKenzie SB, Lee JY, Podsakoff NP. Common method biases in behavioral research: a critical review of the literature and recommended remedies. J Appl Psychol. 2003;88(5):879–903. doi:10.1037/0021-9010.88.5.879
29. Cortina JM. What is coefficient alpha? An examination of theory and applications. J Appl Psychol. 1993;78(1):98–104. doi:10.1037/0021-9010.78.1.98
30. Mangone A, Rossi F, Bianchi M. Multidisciplinary approach in oncology: current perspectives and future directions. Ann Res Oncol. 2024;8(2):145–158.
31. Li M, Chen X, Wang Y. Construction of the competency index system for nursing staff in tertiary hospitals. BMC Nurs. 2025;24:158. doi:10.1186/s12912-025-02789-4
32. Ma M, Liu J, Zhang R. Development and psychometric testing of the nursing students’ career intentions towards dementia care scale. Nurse Educ Today. 2025;128:106542.
33. Catak T, Demir Y, Kaya H. Development and validation of the professional fit scale in nursing. J Nurs Manag. 2025;33(2):e7001.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Psychometric Properties of the Montreal Cognitive Assessment (MoCA) to Detect Major Neurocognitive Disorder Among Older People in Ethiopia: A Validation Study
Daniel B, Agenagnew L, Workicho A, Abera M
Neuropsychiatric Disease and Treatment 2022, 18:1789-1798
Published Date: 22 August 2022
Psychometric Evaluation of the Grit Psychological Resources Scale (GPRS)
Schimschal SE, Cleary M, Kornhaber RA, Barnett T, Visentin DC
Journal of Multidisciplinary Healthcare 2023, 16:913-925
Published Date: 5 April 2023
Research and Evaluation of a Cyberchondria Severity Scale in a Chinese Context
Wang D, Sun L, Shao Y, Zhang X, Maguire P, Hu Y
Psychology Research and Behavior Management 2023, 16:4417-4429
Published Date: 1 November 2023
Reliability and Validity Testing of the Occupational Exposure Risk Awareness Scale (OERAS) for Medical Personnel in Disinfection Supply Centers
Mu Y, Qian X
Risk Management and Healthcare Policy 2025, 18:3911-3919
Published Date: 19 December 2025
Development and Validation of a Health-Related Social Capital Instrument for Older People

Tan F, Song S, Feng Z
Clinical Interventions in Aging 2026, 21:568696
Published Date: 11 February 2026