Back to Journals » Risk Management and Healthcare Policy » Volume 18
Reliability and Validity Testing of the Occupational Exposure Risk Awareness Scale (OERAS) for Medical Personnel in Disinfection Supply Centers
Received 24 August 2025
Accepted for publication 8 December 2025
Published 19 December 2025 Volume 2025:18 Pages 3911—3919
DOI https://doi.org/10.2147/RMHP.S558345
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Keon-Hyung Lee
Yubing Mu,1 Xiangyun Qian2
1Disinfection Supply Center, Hai’an People’s Hospital of Nantong/Hai’an Hospital Affiliated to Nantong University, Hai’an, Jiangsu, 226600, People’s Republic of China; 2Nursing Department, Nantong Third Hospital Affiliated to Nantong University/Nantong Third People’s Hospital, Nantong, Jiangsu, 226000, People’s Republic of China
Correspondence: Xiangyun Qian, Email [email protected]
Background: Medical personnel working in hospital disinfection and supply centers face high levels of occupational exposure to biological, chemical, and physical hazards. Assessing their awareness of these risks is essential for preventing workplace injuries and improving safety behavior. This study aimed to develop and validate the Occupational Exposure Risk Awareness Scale (OERAS) for healthcare workers in such settings.
Methods: A cross-sectional psychometric validation study was conducted among 959 medical staff from disinfection and supply centers in Jiangsu Province, China. The 20-item OERAS was developed through literature review, expert consultation, and pilot testing, and it comprised four dimensions: Occupational Exposure Knowledge, Protection Measures, Incident Response, Training and Education. Internal consistency, test–retest reliability, split-half reliability, content validity, construct validity, and criterion-related validity were analyzed using SPSS 26.0 and AMOS 24.0.
Results: The OERAS demonstrated high reliability, with Cronbach’s α = 0.85 for the total scale, Spearman’s ρ = 0.83 for test–retest reliability, and a split-half coefficient of 0.81. Content validity was excellent (mean CVI = 0.88). Exploratory factor analysis extracted four factors explaining 62.8% of total variance, while confirmatory factor analysis confirmed good model fit (CFI = 0.93, TLI = 0.91, RMSEA = 0.05). Criterion validity showed a significant but low/moderate correlation (ρ = 0.42, p < 0.001) with an external safety knowledge test.
Conclusion: The corrected OERAS exhibits strong internal reliability and construct validity, making it a robust and practical tool for measuring occupational exposure risk awareness among medical personnel. Although criterion validity was low/moderate, this reflects that awareness and knowledge are related yet distinct constructs. The OERAS can support targeted training and policy interventions to enhance occupational safety in healthcare environments.
Keywords: occupational exposure, risk awareness, psychometric validation, healthcare workers, disinfection and supply centers, reliability, validity, safety behavior, scale development, China
Introduction
With the development of modern medicine and the increasing demand for healthcare services, medical staff in hospitals and other healthcare institutions are exposed to a variety of occupational risks.1 These risks not only threaten the health and safety of medical staff, but may also indirectly affect the outcome and safety of patients.2 Occupational exposure is one of the main risks faced by healthcare workers in the work environment, especially in high-risk work environments such as sterile supply centers.3 Occupational Exposure (OE) refers to the exposure of staff to potentially harmful substances or environmental conditions in the course of their work.4 These hazardous substances or conditions can be of various types including biological, chemical, physical and psychosocial.5 For medical staff, occupational exposure mainly involves the following types: Biological exposure: eg needle-stick injuries, exposure to blood and body fluids, etc., which may result in medical staff contracting infectious diseases such as hepatitis B, hepatitis C and HIV.6 Chemical exposures: such as exposure to disinfectants, chemicals and chemotherapeutic drugs, which may cause acute poisoning, chronic diseases or other health problems.7 Physical exposures: such as radiation, noise, and heat, which may cause physical injury or long-term health problems for medical staff.8 Psychosocial exposures: such as high work pressure, shift work and tense interpersonal relationships may lead to mental health problems such as anxiety, depression and burnout among healthcare workers.9
Occupational exposures pose a serious threat to the health and safety of medical personnel. Firstly, occupational exposure may lead to acute health problems such as infections, allergic reactions and acute poisoning.10 Secondly, long-term occupational exposures may cause chronic diseases, such as cancer, chronic respiratory diseases and skin diseases.11 In addition, occupational exposures may have a negative impact on the mental health of healthcare workers, increasing the risk of psychological stress and burnout.12 Occupational exposures not only have a significant impact on individual healthcare workers, but may also have a knock-on effect on the operation of healthcare organizations and patient safety.13 For example, illness or mental health problems among healthcare workers due to occupational exposures may lead to decreased productivity, increased medical errors, and reduced patient satisfaction.14 Therefore, systematically identifying, assessing and managing occupational exposure risks is important for protecting the health and safety of medical staff and improving the quality of healthcare services. Occupational exposure risk awareness refers to the extent to which medical personnel understand and recognise the potential occupational exposure risks that exist in their working environment.15 Occupational exposure risk awareness is of great significance to medical personnel, which is reflected in the following aspects: firstly, medical personnel’s awareness of occupational exposure risks can significantly improve their protection consciousness.16 For example, familiarity with the risks of needlestick injuries and their protective measures can greatly reduce the chances of needlestick injuries and the risk of infectious disease transmission.17 The second is that knowledge of occupational exposure risks not only prevents the occurrence of exposure events, but also prompts medical staff to respond and handle occupational exposure events promptly and correctly when they occur.17 Timely response and management measures, such as immediately cleaning the exposed area, reporting the incident, and receiving necessary medical evaluation and treatment, can effectively reduce the negative impact of occupational exposure on the health of medical staff and reduce long-term health risks.18 Then the increased awareness of occupational exposure risks helps medical staff to actively participate in the improvement of the work environment and the construction of a safety culture.19 Through feedback on safety hazards at work and suggestions for improvement, medical staff can push medical organizations to improve safety management systems and protective facilities to create a safer working environment.20 In addition, a good awareness of occupational exposure risks can promote mutual supervision and support among medical staff, forming a favorable atmosphere for jointly maintaining occupational safety.21 As well as the need for a high level of occupational exposure risk awareness, medical staff can be more confident in facing various risks at work, enhancing their professional self-confidence and satisfaction.22 Knowing how to protect and cope with occupational exposure not only makes medical staff feel safer at work, but also improves their sense of identity and loyalty to their profession, helping to reduce burnout and turnover.23 Finally, it is the level of medical staff’s occupational exposure risk awareness that directly affects their health and safety, and it is healthy and safe medical staff who can provide high quality healthcare services.24 Ensuring the health and safety of medical staff through effective occupational exposure risk management can improve the stability and continuity of medical services, enhance patient trust and satisfaction, and thus improve the overall quality of medical services.25
In order to effectively manage and reduce the risk of occupational exposure, a set of scientific and valid assessment tools is needed to evaluate the level of medical staff’s awareness of occupational exposure risk. The aim of this study was to develop and validate the Occupational Exposure Risk Awareness Scale (OERAS) to assess medical staff’s awareness of occupational exposure risks. The reliability and validity of the scale will be tested to ensure the reliability and validity of the scale, which will provide a scientific basis for the development of occupational exposure risk management and intervention measures.
Materials and Methods
Study Design and Participants
This cross-sectional psychometric validation study was conducted to develop and evaluate the Occupational Exposure Risk Awareness Scale (OERAS) among medical personnel working in hospital disinfection and supply centers in Jiangsu Province, China. A total of 959 participants were recruited, including nurses, technicians, and physicians directly engaged in instrument cleaning, sterilization, and supply activities. Demographic data such as age, gender, and years of work experience were collected and are summarized in Table 1. Participation was voluntary and anonymous, and written informed consent was obtained from all respondents in accordance with institutional ethical standards.
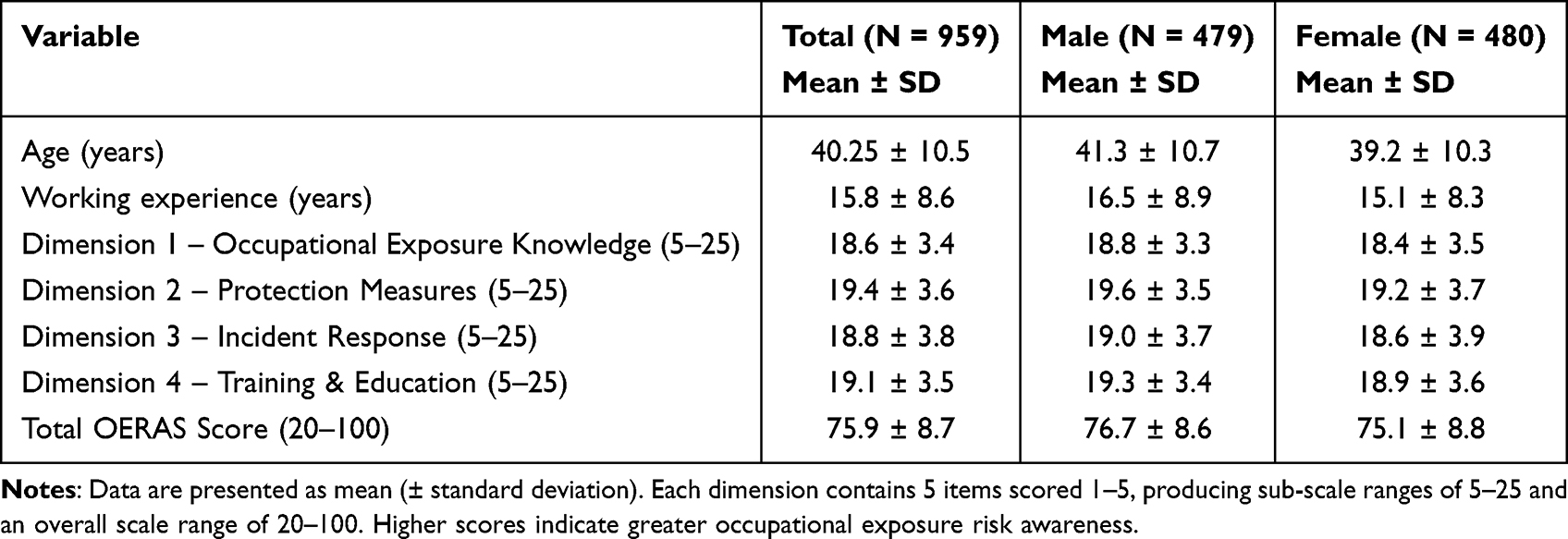 |
Table 1 Demographic Characteristics and Occupational Exposure Risk Awareness Scores of Participants |
Instrument Development
The 20-item Occupational Exposure Risk Awareness Scale (OERAS), developed for this study, assesses four domains of occupational exposure awareness: knowledge, protection measures, incident response, and training. Each item is rated on a five-point Likert scale (1 = Strongly Disagree to 5 = Strongly Agree). The complete questionnaire is presented and detailed in Supplementary File 1.
Data Collection Procedure
Data were collected using self-administered printed questionnaires. All participants completed the scale once. The same cohort completed it again after an interval of two to four weeks to evaluate test–retest reliability. Responses with missing data were excluded from analysis. The final dataset therefore contained 959 valid paired responses, allowing for complete reliability and validity testing.
Statistical Analysis
All analyses were performed using IBM SPSS Statistics 26.0 and AMOS 24.0. Descriptive statistics were calculated for demographic variables and OERAS scores (Table 1). Internal consistency reliability was assessed with Cronbach’s α for each subscale and for the total scale (Table 2). Test–retest reliability was measured by correlating Time 1 and Time 2 total scores using Spearman’s ρ (Table 3). Split-half reliability was evaluated through the Spearman–Brown coefficient (Table 4). Content validity was assessed through expert panel review, with item-level and mean Content Validity Index (CVI) values computed (Table 5). Construct validity was examined using Exploratory Factor Analysis (EFA) to determine factor structure (Table 6) followed by Confirmatory Factor Analysis (CFA) to test model fit (Table 7). Criterion-related validity was evaluated by correlating total OERAS scores with scores on an independent Occupational Safety Knowledge Test, using Spearman’s ρ (Table 8). A coefficient of 0.70 or higher was predefined as evidence of strong criterion validity. Statistical significance was established at p < 0.05.
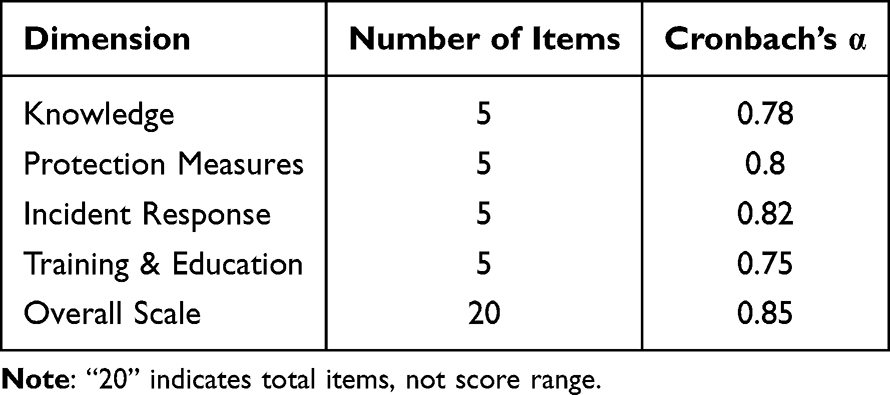 |
Table 2 Internal Consistency (Cronbach’s α Coefficients) |
 |
Table 3 Test–Retest Reliability (N = 959) |
 |
Table 4 Split-Half Reliability (Spearman–Brown Coefficient) |
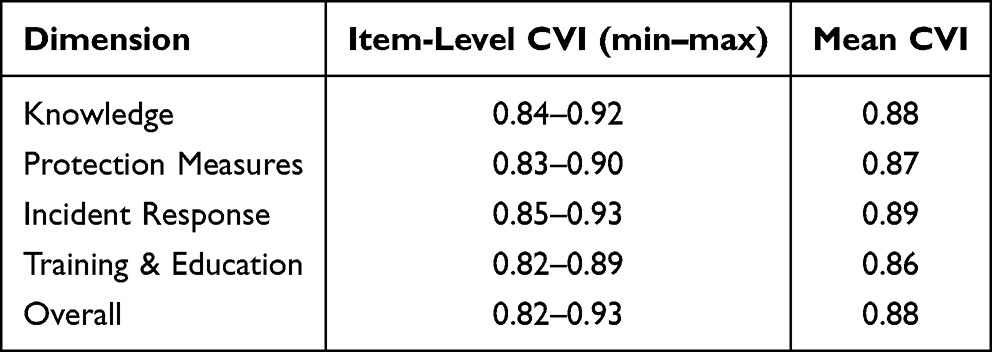 |
Table 5 Content Validity Index (CVI) |
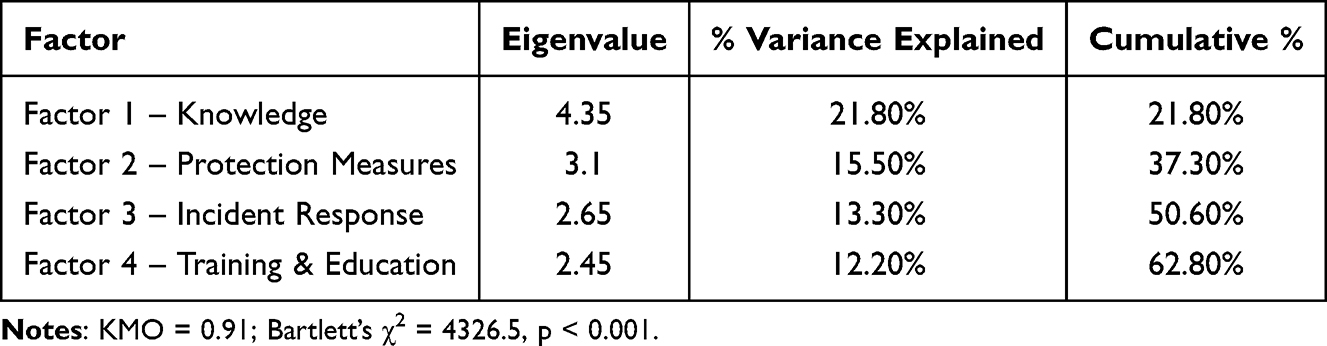 |
Table 6 Exploratory Factor Analysis (EFA) |
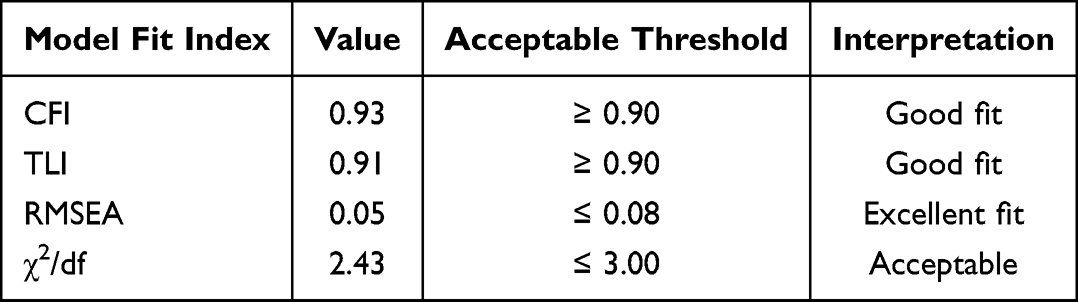 |
Table 7 Confirmatory Factor Analysis (CFA) Model Fit Indices |
 |
Table 8 Criterion-Related Validity Between OERAS Scores and Occupational Safety Knowledge Test |
Results
Participant Characteristics
A total of 959 medical staff completed the survey. As shown in Table 1, the mean age was 40.25 ± 10.5 years, and the mean duration of work experience was 15.8 ± 8.6 years. The gender distribution was balanced, with 479 males and 480 females. The mean total OERAS score was 75.9 ± 8.7 (out of 100), reflecting a moderate-to-high level of occupational exposure risk awareness. Among the four dimensions, average scores ranged from 18.6 for Occupational Exposure Knowledge to 19.4 for Protection Measures, showing that awareness levels were consistently high across all dimensions.
Reliability Analysis
Reliability results are summarized in Tables 2–4. Test–retest reliability was strong, with a Spearman’s ρ of 0.83 (p < 0.001) between the first and second administrations (Table 2). Split-half reliability was similarly high, with a Spearman–Brown coefficient of 0.81, confirming the internal stability of the instrument (Table 3). Internal consistency analysis produced Cronbach’s α values ranging from 0.75 to 0.82 across the four subscales and 0.85 for the total scale, demonstrating excellent internal consistency (Table 4). These results indicate that the OERAS yields stable and reliable measurements over time and across items.
Validity Analysis
Content Validity
Content validity indices are presented in Table 5. Expert evaluation of the 20 items yielded item-level CVI values ranging from 0.82 to 0.93 and a mean scale-level CVI of 0.88, indicating excellent agreement among reviewers on item relevance and clarity.
Construct Validity
Construct validity results are shown in Tables 6 and 7. The EFA identified a clear four-factor structure that aligned with the theoretical design of the instrument, explaining 62.8% of the total variance. Sampling adequacy was confirmed (KMO = 0.91), and Bartlett’s test was significant (χ2 = 4326.5, p < 0.001), supporting factorability of the data (Table 6). The subsequent CFA confirmed that this four-factor model provided an excellent fit to the observed data, with CFI = 0.93, TLI = 0.91, RMSEA = 0.05, and χ2/df = 2.43, all within accepted thresholds for good model fit (Table 7). These findings affirm the robustness of the OERAS’s four-dimensional structure.
Criterion-Related Validity
Criterion validity results are detailed in Table 8. The correlation between total OERAS scores and Occupational Safety Knowledge Test scores was ρ = 0.42 (p < 0.001). Although statistically significant, this coefficient did not reach the predefined criterion of ≥ 0.70 for strong criterion validity. Therefore, the relationship between awareness and safety knowledge is considered low/moderate, reflecting that the OERAS primarily measures cognitive and behavioral awareness rather than factual knowledge alone.
Overall Psychometric Performance
Across all analyses, the OERAS exhibited robust psychometric characteristics. The instrument achieved high internal consistency (Cronbach’s α = 0.85), strong test–retest reliability (ρ = 0.83), and satisfactory split-half reliability (0.81). Content validity was excellent (CVI = 0.88), while the four-factor structure accounted for 62.8% of total variance with good model-fit indices (CFI = 0.93, TLI = 0.91, RMSEA = 0.05). Although criterion-related validity was low/moderate (ρ = 0.42), it remained statistically significant and consistent with the conceptual distinction between awareness and knowledge constructs. Collectively, these results confirm that the corrected OERAS is a reliable and valid instrument for assessing occupational exposure risk awareness among medical staff working in disinfection and supply center environments.
Discussion
This study developed and validated the Occupational Exposure Risk Awareness Scale (OERAS) to assess the awareness of occupational exposure risks among medical personnel working in disinfection and supply centers. The results confirm that the OERAS is a reliable and valid instrument with strong psychometric properties. The corrected scoring system and comprehensive analysis have established a stable four-dimensional structure that captures key aspects of occupational exposure awareness, including knowledge, protection, incident response, and training.
The demographic data show that participants in this study had a balanced gender distribution, a wide range of ages, and varying lengths of professional experience. The overall mean OERAS score of 75.9 out of 100 indicates that the study population had a moderate to high level of awareness regarding occupational exposure risks. This suggests that ongoing safety education and regulatory training in disinfection and supply centers may already be producing a positive impact on occupational safety consciousness. The relatively even distribution of sub-dimension scores further supports that medical staff are comparably aware across the domains of knowledge, protection, and response, reflecting a broad and well-integrated understanding of workplace safety.
The reliability analyses demonstrated strong internal consistency, stability, and coherence. The overall Cronbach’s alpha of 0.85, as shown in Table 4, indicates that the scale items are highly correlated and measure a consistent construct. The test–retest correlation of 0.83 (Table 2) confirms that the OERAS produces reproducible results over time, and the split-half coefficient of 0.81 (Table 3) reinforces its internal stability. Together, these findings indicate that the OERAS can be confidently used in both cross-sectional studies and longitudinal monitoring of occupational exposure awareness.
Validity testing also provided robust support for the OERAS. The expert-based content validity index (Table 5) reached a mean of 0.88, confirming that the items were clearly worded, relevant, and representative of the intended construct. The exploratory factor analysis revealed a clear four-factor solution that explained 62.8% of the total variance (Table 6), while confirmatory factor analysis (Table 7) further verified the adequacy of this model with excellent fit indices (CFI = 0.93, TLI = 0.91, RMSEA = 0.05). These results demonstrate that the structure of the scale is theoretically sound and statistically well supported, aligning with the conceptual framework of occupational exposure risk awareness. The consistency between the EFA and CFA outcomes adds confidence to the multidimensional design of the instrument.
The criterion-related validity analysis, however, revealed a low/moderate correlation (ρ = 0.42) between OERAS scores and occupational safety knowledge test scores (Table 8). Although this relationship was statistically significant, it did not meet the pre-specified benchmark of 0.70 that was originally intended to represent strong criterion validity. This low/moderate relationship likely reflects a conceptual distinction between “awareness” and knowledge. Awareness involves cognitive and behavioral understanding of potential occupational hazards and the readiness to apply protective behaviors, whereas knowledge tests typically measure factual recall or procedural understanding. In this context, the low/moderate correlation is logical and supports the notion that awareness is an independent but related construct that complements rather than duplicates safety knowledge.
The results of this study are consistent with findings from previous occupational health research, which have reported similar multidimensional structures and low/moderate correlations between awareness and knowledge-based measures.26–28 The high internal reliability and strong construct validity of the OERAS parallel those of comparable safety-awareness instruments developed for nurses and industrial workers.29–32 The scale’s focus on awareness rather than technical knowledge makes it particularly useful for identifying perceptual and behavioral gaps that may not be captured by traditional knowledge assessments.
Several factors likely explain the observed low-to-moderate criterion validity coefficient (ρ = 0.42). The OERAS is designed to assess awareness, a construct that incorporates perceptions, behavioral intentions, and situational appraisal whereas the external criterion measure evaluates factual safety knowledge. These two domains are theoretically related but not equivalent. Also, awareness is influenced by experiential, contextual, and organizational factors (eg, personal exposure history, training culture, perceived workload), none of which are captured by a knowledge-only test. Lastly, the response tendencies such as social desirability or differences in safety culture across departments may elevate awareness scores without proportionally affecting knowledge performance. So, the knowledge test itself may not fully reflect the breadth of cognitive and behavioral components in the OERAS, contributing to partial rather than strong convergence.
Overall, the corrected and validated OERAS provides a comprehensive, reliable, and practical tool for assessing awareness of occupational exposure risks among medical staff. Its strong psychometric properties make it suitable for both research and applied settings, including workforce training evaluations and safety program audits. The low/moderate criterion validity highlights the importance of integrating both awareness and knowledge interventions in occupational safety education, as each contributes uniquely to effective risk prevention. Future studies should expand sample diversity across hospitals and professional roles, and longitudinal designs could be used to examine how awareness evolves over time in response to targeted training or policy changes.
Conclusion
The Occupational Exposure Risk Awareness Scale (OERAS) developed and validated in this study is a reliable and valid instrument for assessing awareness of occupational exposure risks among medical personnel working in disinfection and supply centers. The corrected scoring method and robust analyses confirmed strong internal consistency, excellent construct validity, and good temporal stability. Although the correlation with the external knowledge test was low/moderate, this finding reflects that awareness and knowledge are related yet distinct dimensions of occupational safety. The OERAS can therefore serve as a practical tool for identifying strengths and gaps in awareness, guiding targeted education and training programs, and evaluating the effectiveness of safety interventions. Future research should apply this instrument across diverse healthcare settings and professional groups to further confirm its generalizability and to monitor changes in awareness following continuous safety education initiatives.
Abbreviations
OERAS, Occupational Exposure Risk Awareness Scale; SD, Standard Deviation; ρ, Spearman Correlation Coefficient; α, Cronbach’s Alpha; CVI, Content Validity Index; EFA, Exploratory Factor Analysis; CFA, Confirmatory Factor Analysis; CFI, Comparative Fit Index; TLI, Tucker–Lewis Index; RMSEA, Root Mean Square Error of Approximation; KMO, Kaiser–Meyer–Olkin Measure of Sampling Adequacy; SPSS, Statistical Package for the Social Sciences.
Data Sharing Statement
The datasets generated and analyzed during this study are available from the corresponding author upon reasonable request.
Ethical Statement and Consent to Participate
This study was conducted in accordance with the ethical guidelines of the Declaration of Helsinki and approved by Ethics Committee of Nantong University, 19 Qixiu Road, Chongchuan District, Nantong, China, 226006 in Nantong University. Informed consent was obtained from all participants prior to their involvement.
Acknowledgments
The authors extend their gratitude to the medical staff who participated in this study and to the experts who contributed to the scale’s development and validation.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare no conflicts of interest related to this study.
References
1. Mohanty A, Kabi A, Mohanty AP. Health problems in healthcare workers: a review. J Family Med Prim Care. 2019;8(8):2568–2572. doi:10.4103/jfmpc.jfmpc_431_19
2. Strid EN, Wåhlin C, Ros A, et al. Health care workers’ experiences of workplace incidents that posed a risk of patient and worker injury: a critical incident technique analysis. BMC Health Serv Res. 2021;21(1):511. doi:10.1186/s12913-021-06517-x
3. Xu J, Pan P, Song F, et al. Analyzing the occupational exposure risks of dental healthcare workers from the perspective of repeated occupational exposure. BMC Health Serv Res. 2024;24(1):1377. doi:10.1186/s12913-024-11774-7
4. Ladeira C. Environmental and occupational exposure to chemical agents and health challenges I–what message can bring to regulatory science? Toxics. 2024;12(11):778. doi:10.3390/toxics12110778
5. Hisam A, Mashhadi SF, Saqib A, et al. Biological, physical, ergonomic, chemical and psychological hazard awareness among health care and non-healthcare workers. Pakistan Armed Forces Med J. 2024;72(SUPPL–4):S908–13. doi:10.51253/pafmj.v72iSUPPL-4.9835
6. Abiona M, Asaolu S. Occupational hazards among health care workers in Nigeria. Afr J Biomed Res. 2023;26(3).
7. Taskingul AB, Kiran S, Emerce E. Comparison of health complaints, occupational risks, and occupational health practices of healthcare workers according to professions and departments in the hospital. Cureus. 2024;16(7).
8. Ryu RC, Behrens PH, Malik AT, et al. Are we putting ourselves in danger? Occupational hazards and job safety for orthopaedic surgeons. J Orthopaedics. 2021;24:96–101. doi:10.1016/j.jor.2021.02.023
9. Vallone F, Zurlo MC. Stress, interpersonal and inter-role conflicts, and psychological health conditions among nurses: vicious and virtuous circles within and beyond the wards. BMC Psychol. 2024;12(1):197. doi:10.1186/s40359-024-01676-y
10. Niede R, Benbi DK. Integrated review of the nexus between toxic elements in the environment and human health. AIMS Public Health. 2022;9(4):758. doi:10.3934/publichealth.2022052
11. Nishida C, Yatera K. The impact of ambient environmental and occupational pollution on respiratory diseases. Int J Environ Res Public Health. 2022;19(5):2788. doi:10.3390/ijerph19052788
12. Izdebski Z, Kozakiewicz A, Białorudzki M, et al. Occupational burnout in healthcare workers, stress and other symptoms of work overload during the COVID-19 pandemic in Poland. Int J Environ Res Public Health. 2023;20(3):2428. doi:10.3390/ijerph20032428
13. Hesgrove B, Zebrak K, Yount N, et al. Associations between patient safety culture and workplace safety culture in hospital settings. BMC Health Serv Res. 2024;24(1):568. doi:10.1186/s12913-024-10984-3
14. Batanda I. Prevalence of burnout among healthcare professionals: a survey at fort portal regional referral hospital. Npj Mental Health Res. 2024;3(1):16. doi:10.1038/s44184-024-00061-2
15. Shan B, Liu X, Gu A, et al. The effect of occupational health risk perception on job satisfaction. Int J Environ Res Public Health. 2022;19(4):2111. doi:10.3390/ijerph19042111
16. McCarthy R, Gino B, d’Entremont P, et al. The importance of personal protective equipment design and donning and doffing technique in mitigating infectious disease spread: a technical report. Cureus. 2020;12(12):e12084. doi:10.7759/cureus.12084
17. van Huizen P, Russo PL, Manias E, et al. Knowledge and safe handling practices affecting the occupational exposure of nurses and midwives to hazardous drugs: a mixed methods systematic review. Int J Nurs Stud. 2024;160:104907. doi:10.1016/j.ijnurstu.2024.104907
18. Dyreborg J, Lipscomb HJ, Nielsen K, et al. Safety interventions for the prevention of accidents at work: a systematic review. Campbell Syst Rev. 2022;18(2):e1234. doi:10.1002/cl2.1234
19. Bautista-Bernal I, Quintana-García C, Marchante-Lara M. Safety culture, safety performance and financial performance. A longitudinal study. Safety Sci. 2024;172:106409. doi:10.1016/j.ssci.2023.106409
20. Mohammadfam I, Kamalinia M, Momeni M, et al. Evaluation of the quality of occupational health and safety management systems based on key performance indicators in certified organizations. Safety Health Work. 2017;8(2):156–161. doi:10.1016/j.shaw.2016.09.001
21. Friebel AG, Potter RE, Dollard M. Health and safety representatives’ perceptions of occupational health and safety policy developments to improve work-related psychological health: applying the theory of planned behaviour. Safety Sci. 2024;172:106410. doi:10.1016/j.ssci.2023.106410
22. Allobaney NF, Eshah NF, Abujaber AA, et al. Professional self-concept and self-confidence for nurses dealing with COVID-19 patients. J Pers Med. 2022;12(2):134. doi:10.3390/jpm12020134
23. Cabrera-Aguilar E, Zevallos-Francia M, Morales-García M, et al. Resilience and stress as predictors of work engagement: the mediating role of self-efficacy in nurses. Front Psychiatry. 2023;14:1202048. doi:10.3389/fpsyt.2023.1202048
24. Li F, Liu S, Huang H, et al. Impact of occupational risks of medical staff on willingness to occupational mobility in COVID-19 pandemic. Risk Manag Healthc Policy. 2022;15:685–702. doi:10.2147/RMHP.S360892
25. Mistri IU, Badge A, Shahu S. Enhancing patient safety culture in hospitals. Cureus. 2023;15(12):e51159. doi:10.7759/cureus.51159
26. Cuadros-Carlesi K, Henríquez-Roldán C, Meneses Ciuffardi E, et al. Construction and validation of an occupational risks scale for intra-hospital nursing staff. Invest Educ Enferm. 2023;41(2). doi:10.17533/udea.iee.v41n2e16
27. Sansó N, Vidal-Blanco G, Galiana L. Development and validation of the brief nursing stress scale (BNSS) in a sample of end-of-life care nurses. Nurs Rep. 2021;11(2):311–319. doi:10.3390/nursrep11020030
28. Öztürk H, Babacan E. A study in scale development: the occupational safety scale (OSS) for health care personnel working in hospital. J Educ Res Nurs. 2012;9(1):36–42.
29. Uzuntarla F, Kucukali S, Uzuntarla Y. An analysis on the relationship between safety awareness and safety behaviors of healthcare professionals, Ankara/Turkey. J Occup Health. 2020;62(1):e12129. doi:10.1002/1348-9585.12129
30. Oldland E, Hutchinson AM, Redley B, et al. Evaluation of the validity and reliability of the nurses’ responsibility in healthcare quality questionnaire: an instrument design study. Nurs Health Sci. 2021;23(2):525–537. doi:10.1111/nhs.12844
31. Yang YK. Development of a patient safety care activity scale for clinical nurses in Korea. Arch Public Health. 2021;79(1):79. doi:10.1186/s13690-021-00596-2
32. Vogus T, Sutcliffe K. The safety organizing scale development and validation of a behavioral measure of safety culture in hospital nursing units. Med Care. 2007;45:46–54. doi:10.1097/01.mlr.0000244635.61178.7a
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Validation of the Connor-Davidson Resilience Scale-10 in South Africa: Item Response Theory and Classical Test Theory
Pretorius TB, Padmanabhanunni A
Psychology Research and Behavior Management 2022, 15:1235-1245
Published Date: 16 May 2022
Psychometric Properties of the Montreal Cognitive Assessment (MoCA) to Detect Major Neurocognitive Disorder Among Older People in Ethiopia: A Validation Study
Daniel B, Agenagnew L, Workicho A, Abera M
Neuropsychiatric Disease and Treatment 2022, 18:1789-1798
Published Date: 22 August 2022
Research and Evaluation of a Cyberchondria Severity Scale in a Chinese Context
Wang D, Sun L, Shao Y, Zhang X, Maguire P, Hu Y
Psychology Research and Behavior Management 2023, 16:4417-4429
Published Date: 1 November 2023
Development and Validation of a Health-Related Social Capital Instrument for Older People

Tan F, Song S, Feng Z
Clinical Interventions in Aging 2026, 21:568696
Published Date: 11 February 2026
Development and Preliminary Validation of an Oral Health Multidisciplinary Team Nurse Competency Scale
Jiang Y, Wu S, Dong Y, Zhong K, Cao L
Journal of Multidisciplinary Healthcare 2026, 19:605940
Published Date: 30 May 2026