Back to Journals » Psychology Research and Behavior Management » Volume 16
Research and Evaluation of a Cyberchondria Severity Scale in a Chinese Context
Authors Wang D, Sun L, Shao Y, Zhang X, Maguire P, Hu Y ![]()
Received 19 July 2023
Accepted for publication 14 October 2023
Published 1 November 2023 Volume 2023:16 Pages 4417—4429
DOI https://doi.org/10.2147/PRBM.S431470
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mei-Chun Cheung
Dawei Wang,1 Lingchao Sun,1 Yunru Shao,1 Xiaoyan Zhang,1 Phil Maguire,2 Yixin Hu1
1School of Psychology, Shandong Normal University, Ji’nan, Shandong, People’s Republic of China; 2Department of Computer Science, National University of Ireland, Galway, Ireland
Correspondence: Yixin Hu, School of Psychology, Shandong Normal University, Jinan, Shandong Province, 250358, People’s Republic of China, Email [email protected]
Purpose: Cyberchondria is a problematic or unhelpful behavior pattern that describes excessive or repetitive online health-related information searching related to an enhanced level of health anxiety. Such internet-derived medical anxiety can manifest itself in different ways across cultures. This study explores the unique nature of cyberchondria in the context of Chinese culture, identifying the risk factors for the condition and the possible negative outcomes.
Methods: An exploratory factor analysis (EFA) was used to explore whether the structure of the Chinese version of the Cyberchondria Severity Scale (C-CSS) is different from that in western context. Subsequently, a confirmatory factor analysis (CFA) was used to verify the model fit of the C-CSS. Finally, a series of regression analysis were used to test the relationship between cyberchondria and its antecedent variables and consequence variables in Chinese context.
Results: Retained 18 items and revised to 3 dimensions (Negative Effects, Excessiveness and Reassurance Seeking), the Chinese version of the Cyberchondria Severity Scale (C-CSS) was developed. In the context of China, the three antecedents were also effective predictors of cyberchondria, and C-CSS is also related to theoretically relevant outcomes.
Conclusion: This study initially demonstrated the validity, reliability and applicability of C-CSS to assess the severity of cyberchondria among Chinese undergraduates.
Keywords: cyberchondria severity scale, medical anxiety, Chinese health system, validity, reliability
Introduction
With rapid improvements in internet connectivity, it is becoming increasingly common for people to access health-related information online. A 2010 poll revealed that 60% of internet users in China had searched for health-related information online and 56% of them had self-diagnosed using such information.1,2 Nonetheless, these health-related information obtained online is likely to be inaccurate. For example, White and Horvitz3 found “Amyotrophic Lateral Sclerosis” to be the most common condition returned based on online searches for “muscle twitching”, despite the fact that the incidence of this serious disease is extremely low. Research available shows that excessive searching for health-related information online can lead to increased health anxiety. Rather than having their fears eased, users can end up being panicked into carrying out further medical information searches, resulting in a behavior pattern known as “Cyberchondria”.4
Cyberchondria is a problematic behavior pattern characterized by excessive or repetitive seeking of health-related information online, often connected with underlying health anxiety.5–7 Given the capacity of such information to exacerbate distress or anxiety, cyberchondria has been referred to as “the new frontier in illness anxiety”.8 According to models of pathological worry, cyberchondria can be described as a vicious cycle in which those who experience increased anxiety when accessing health-related information attempt to seek reassurance through further online searches.9 The short-term decrease in anxiety which these searches can provide may lead sufferers to search more and more, thus maintaining a long-term negative cycle.8 Those individuals with endogenous characteristics of “vulnerability”, such as perfectionism, high levels of anxiety sensitivity (AS) and intolerance of uncertainty (IU), are more likely to be trapped in the vicious circle of increased physical health concerns and online medical information seeking.10 This unique anxiety-amplifying effect of cyberchondria sets it apart.9,11 In addition to subjecting individuals to anxiety and distress, cyberhypochondria can also lead to inefficient use of medical resources, adding an unnecessary burden on the public health system.9,12,13
To date, several measures have been extensively relied on to assess cyberchondria. Some studies have evaluated cyberchondria indirectly based on reports of cyberchondria-related symptoms, such as the Short Health Anxiety Inventory (SHAI) and the Positive and Negative Affect Schedule (PANAS).5 Moreover, a questionnaire has been developed to assess cyberchondria directly, which includes three dimensions, namely escalation of concerns, persistence of concerns and judgment biases.14 This instrument omits some characteristics of cyberchondria, such as compulsion and reassurance seeking, and its psychometric characteristics have been inadequately reported. Semi-structured interviews have also been used to assess cyberchondria, though the questions used are not sufficiently detailed to shed light on the multidimensional structure of cyberchondria (eg “Why did you choose to look up this information on the Internet?”, “How accurate do you think the health information you found online is?”).15 In response, McElroy and Shevlin13 specified a multi-dimensional construct for cyberchondria and developed the Cyberchondria Severity Scale (CSS) to assess the severity of cyberchondria directly.
The CSS was found to be reliable in terms of internal consistency and test-retest stability.13 The convergent and divergent validity of CSS was also supported, as demonstrated by moderate correlations with established measures of depression, anxiety and stress. Additionally, a series of studies have indicated that the CSS supports the psychometric properties of validity and reliability, based on adult samples obtained in Turkey, Germany and America.12,16,17 Overall, this work supports the usefulness of the CSS as a reliable and valid instrument for assessing cyberchondria in adolescents and adults. However, Norr et al18 questioned the mistrust subscale its inclusion in the CSS, based on the small correlations found between Mistrust factor and other factors and the superior fit of their cyberhypochondria model when the Mistrust factor were excluded. As suggested by Fergus,12 the current study attempts to further illuminate the unique role these dimensions play in the development of cyberchondria.
Although the CSS has been studied in multiple cultures, it has not yet been evaluated empirically in a Chinese sample. In fact, there are no studies of cyberchondria or widely recognized evaluation tools for cyberchondria in China. Manifestations of cyberchondria are, to some extent, determined by cultural factors associated with socialization practices. It is therefore necessary to verify the applicability of CSS in China, given the marked differences in Chinese social institutions, medical systems, beliefs and values in comparison with predominantly individualistic cultures such as the United States and Germany. For example, in terms of the medical system, there are large regional differences in medical resources across China, and offline medical resources are relatively insufficient in some areas.19 It can be inconvenient for some rural Chinese to seek medical treatment; this may make them more likely to explore health-related information online. In terms of values, Chinese people tend to be conservative. Many patients are afraid to seek medical treatment due to their prejudice against diseases and a desire to preserve their self-respect.20 Accordingly, they may adopt more covert ways to alleviate their worries about diseases. By exploring the psychometric properties and construct of CSS in China, we hope to gain insight into its nature as manifested in a Chinese context.
Finally, although significant associations between cyberchondria, health anxiety and intolerance of uncertainty have been established,10 further research is required to understand the causal relationship between these factors. A better understanding of the nature of cyberchondria could lead to the identification of effective treatments.
In summary, this study sets out several goals. First, we aim to verify the validity and reliability of the CSS in a Chinese sample. Second, our objective is to explore the risk factors and potential adverse effects of cyberchondria by utilizing regression and calibration of antecedent and outcome variables, with the aim of enhancing the adaptability of CSS to the context of China’s 800 million internet users. Finally, we aim to provide a solid conceptual foundation for future studies investigating the prevalence and mitigation of cyberchondria in China.
Study 1 the Psychometric Properties of C-CSS
To explore the psychometric properties and construct of Cyberchondria Severity Scale in China, two substudies were conducted. In Study 1a, an exploratory factor analysis was conducted to preliminarily determine the underlying structure of the Chinese version of the Cyberchondria Severity Scale (C-CSS). Subsequently, in Study 1b, a confirmatory factor analysis (CFA) was used to verify the model fit of the C-CSS and a series of reliability and validity tests were carried out.
Study 1a EFA Analysis
Sample 1
The first sample consisted of 385 healthy Chinese undergraduates. These students were recruited from a university in the city of Jinan, located in Shandong Province, Eastern China. Their cyberchondria was measured using a paper and pencil test. After the exclusion of the questionnaires with substantial missing information or unreliable response patterns, 380 valid responses were identified. The sample was primarily female (52.6% female) with ages ranging from 17 to 23 (M = 19.549, SD = 1.064). All of the procedures involved in this study are consistent with the ethical standards of the Academic Board of Shandong Normal University and the 1964 Helsinki Declaration and subsequent revised ethical standards. The participants provided written, informed consent voluntarily and anonymously and had the right to withdraw from the research program at any time.
Measure
Cyberchondria Severity Scale (CSS)
The CSS is a self-report measure of the severity of cyberchondria, initially developed with United Kingdom samples.13 This scale consists of 33 items and 5 dimensions: Compulsion (8 items), Distress (8 items), Excessiveness (8 items), Reassurance Seeking (6 items) and Mistrust of Medical Professional (3 items) (see Appendix). Each item is rated using a five-point Likert scale indicating frequency (1=Never, 2=Rarely, 3=Sometimes, 4=Often, 5=Always). The whole CSS score demonstrated adequate internal consistency in previous studies (Cronbach’s alpha = 0.94).13
In this study, a Chinese back translated version of the CSS was used. The following procedures were applied. First of all, each item of the English version of the scale was translated into Chinese by the researchers. Second, researchers examined each item of the translated version of the scale in terms of meaning, accuracy, wording, spelling, and grammar. Third, the Chinese version of CSS was translated back to English in order to ensure the exact meaning of each item.
Results
Reliability Statistics
The internal consistency of the whole scale was α = 0.909, with the consistency increasing to α = 0.935 given removal of “Mistrust of Medical Professional” (including items 9, 28, 33).
EFA
The significance of Bartlett’s test of sphericity ( (528) = 6472.880, p < 0.001) and the size of the Kaiser-Meyer-Olkin measure of sampling adequacy (KMO = 0.930) showed that the 33 items had adequate common variance for factor analysis.21 EFA using principal axis factoring method was conducted to examine the internal structure of the 33-item CSS (the principal axis factoring method was applied). We rotated factors using an oblique rotation with kappa value of 4 based on our assumption that the factors would be correlated. Item selection was based on the following criteria: (1) items with loadings less than 0.50 on a factor were deleted, and (2) items with loadings at 0.50 or greater on a factor, but with cross-loadings at 0.32 or higher on the other factor, were deleted.21 To ensure minimal ambiguity among factors, the criteria for an acceptable factor were as follows: (1) the minimum eigenvalue was 1, and (2) the minimum loading on each factor was three items.22 As a result, three factors and 18 items were retained for the final version of the scale, and the internal consistency reliability was 0.921. Then, the EFA was rerun with 18 items. Three factors with eigenvalues over 1 were retained. And the rotated three‐factor solution explained 62.179% of the total variance. The results of the EFA are presented in Table 1.
(528) = 6472.880, p < 0.001) and the size of the Kaiser-Meyer-Olkin measure of sampling adequacy (KMO = 0.930) showed that the 33 items had adequate common variance for factor analysis.21 EFA using principal axis factoring method was conducted to examine the internal structure of the 33-item CSS (the principal axis factoring method was applied). We rotated factors using an oblique rotation with kappa value of 4 based on our assumption that the factors would be correlated. Item selection was based on the following criteria: (1) items with loadings less than 0.50 on a factor were deleted, and (2) items with loadings at 0.50 or greater on a factor, but with cross-loadings at 0.32 or higher on the other factor, were deleted.21 To ensure minimal ambiguity among factors, the criteria for an acceptable factor were as follows: (1) the minimum eigenvalue was 1, and (2) the minimum loading on each factor was three items.22 As a result, three factors and 18 items were retained for the final version of the scale, and the internal consistency reliability was 0.921. Then, the EFA was rerun with 18 items. Three factors with eigenvalues over 1 were retained. And the rotated three‐factor solution explained 62.179% of the total variance. The results of the EFA are presented in Table 1.
 |
Table 1 EFA |
Study 1b CFA and Scale Validation
Sample 2
Data in this study was collected from 221 healthy Chinese undergraduates with the paper-pencil method. These students were recruited from a university in the city of Jinan, located in Shandong Province, Eastern China. After the exclusion of questionnaires with substantial missing information or unreliable response patterns, 220 valid responses were identified. The sample was primarily female (56.8% female), with ages ranging from 16 to 22 (M = 18.500, SD = 0.852). All of the procedures involved in this study are consistent with the ethical standards of the Academic Board of Shandong Normal University and the 1964 Helsinki Declaration and subsequent revised ethical standards. The participants provided written, informed consent voluntarily and anonymously and had the right to withdraw from the research program at any time.
Measure
Chinese Version of Cyberchondria Severity Scale (C-CSS)
The 18-item Chinese version of CSS consists of 3 dimensions: Negative Effects (12 items), Excessiveness (3 items) and Reassurance Seeking (3 items). Each item is rated using a five-point Likert scale indicating frequency (1=Never, 2=Rarely, 3=Sometimes, 4=Often, 5=Always). A total C-CSS score can be calculated by summing scores on relevant items. In this study, a revised Chinese version of C-CSS was used (α = 0.901).
Short Health Anxiety Inventory (SHAI)
The SHAI is a self-report measure of health anxiety initially developed by Salkovskis et al.23 This scale comprises of 18 items, with each item rated using a four-point Likert scale (ranging from 0 to 3); the scale has demonstrated acceptable reliability and validity in Chinese samples.24 In this study, a Chinese version of SHAI (α = 0.880) was used to assess convergent validity of the CSS.
Padua Inventory (PI)
The 60-item PI was originally developed to assess the number and severity of obsessive-compulsive disorder (OCD) symptoms in clinical and non-clinical participants. Items are scored on a five-point Likert scale ranging from 0 (not at all) to 5 (very much) based on the degree of disturbance. The PI demonstrated good psychometric properties in Chinese samples.25 In this study, a Chinese version of PI (α = 0.879) was used to assess convergent validity of the CSS.
Results
CFA
A confirmatory factor analysis (CFA) was performed using Analysis of Moment Structure (AMOS) 21.0 statistical software to confirm the overall fit and acceptability of the three-factor structure of C-CSS derived from study 1. Previous studies have suggested the removal of the “mistrust of medical professional” subscale from the C-CSS. Consequently, the CFA was performed in a structure including three dimensions, and items were allowed to correlate with each other in each dimension. The robust maximum likelihood (MLR) estimator was used.26 Following Barke et al,17 the model fit of two competing measurement models were tested. Model 1 was a unidimensional model with all items loaded onto a single factor. Model 2 consisted of the hypothesized three‐factor structure derived from the EFA.
There are multiple approximate fit tests that can be used to evaluate the model’s fit to the data; the model specification and the parameter estimates are illustrated in Table 2. In this study, Normed Fit Index (NFI),27 Comparative Fit Index (CFI),27 Standardized Root Mean Square Residual (SRMR) and Root Mean Square Error Approximation (RMSEA)28 were employed to evaluate model fit. Despite widespread use of chi-square statistics in the literature, authors have criticized it due to its high sensitivity to sample size. This is because chi-square statistics tend to be conservative and detect trivial differences between hypothetical and observed models when the sample size is large.29 For that reason, instead of chi-square statistics, the aforementioned indices were considered. We viewed  /df < 3, TLI > 0.90, CFI > 0.95, RMSEA < 0.06 (N > 250) and SRMR < 0.11 as cut-off values representing good fit.30 The three-factor model was found to fit the observed data well (
/df < 3, TLI > 0.90, CFI > 0.95, RMSEA < 0.06 (N > 250) and SRMR < 0.11 as cut-off values representing good fit.30 The three-factor model was found to fit the observed data well ( /df = 1.719, TLI = 0.937, CFI = 0.949, RMSEA = 0.057, SRMR = 0.059), in comparison with the one-factor model (
/df = 1.719, TLI = 0.937, CFI = 0.949, RMSEA = 0.057, SRMR = 0.059), in comparison with the one-factor model ( /df = 3.082, TLI = 0.819, CFI = 0.848, RMSEA = 0.098, SRMR = 0.090). As illustrated in Figure 1, the standardized factor loadings of the three-factor model surpassed 0.5 and ranged from 0.50 to 0.87, indicating a moderate to high level of correlation between the latent variable (factor) and the explicit variables (analysis items).
/df = 3.082, TLI = 0.819, CFI = 0.848, RMSEA = 0.098, SRMR = 0.090). As illustrated in Figure 1, the standardized factor loadings of the three-factor model surpassed 0.5 and ranged from 0.50 to 0.87, indicating a moderate to high level of correlation between the latent variable (factor) and the explicit variables (analysis items).
 |
Table 2 CFA of Chinese Version of Cyberchondria Severity Scale (C-CSS) |
 |
Figure 1 Three-factor model. |
Intercorrelations and Reliability Statistics
Descriptive statistics (including means and standard deviations) and intercorrelations for the C-CSS total and three subscale scores were examined in order to investigate the construct validity of C-CSS, as shown in Table 3. The total scale demonstrated strong and positive correlations (p < 0.01) to the reassurance subscale (0.624), excessiveness subscale (0.683) as well as to the negative results subscale (0.939). The intercorrelations for the three cyberchondria dimensions were significant. In addition, the Cronbach’s alpha for the total, and that for the subscales used to evaluate the internal consistency of C-CSS, ranged from 0.752 to 0.903, thus exceeding the minimum requirement of 0.70.31
 |
Table 3 Descriptive Statistics for the Cyberchondria Severity Scale, the Short Health Anxiety Inventory and the Padua Inventory |
Convergent and Discriminant Validity
According to the Fornell-Larcker testing system, an AVE value for each construct larger than 0.5 indicates acceptable convergent validity at the level of scale construct. If the level of AVE for each attribute is higher than the square of inter-construct correlations involving the construct, this indicates discriminant validity at the construct level.32 The square root of AVE of each dimension was 0.661, 0.667, 0.741, thus being higher than 0.5 and also higher than the largest correlation coefficients among the dimensions (Table 3). This indicates that our constructs exhibited adequate convergent validity and discriminant validity.
Criterion-Related Validity
As presented in Table 3, the total scale and subscales of C-CSS were moderately correlated with HA total score and PI total score (p < 0.001).
Study 2 Antecedents and Outcomes
Anxiety sensitivity (AS) and intolerance of uncertainty (IU) are considered to be the cognitive factors underlying anxiety disorders.33,34 Several studies have examined the transdiagnostic vulnerability in individuals with a high level of AS, who, due to the characteristics of “vulnerability”, are at increased risk of developing cyberchondria.10,35,36 For individuals with a high level of AS, anxiety symptoms, such as increased heart rate, are likely to be interpreted as a signal of physical illness and psychological incapacitation, which might lead to further online health-related searching. There is substantial evidence that reducing uncertainty is a core motive in searching for health-related information on the Internet.34 It has been further proved that IU is positively associated with cyberchondria, and even can predict cyberchondria.10,36,37 In another study, comparable medium-strength correlations were found between cyberchondria and self-reported somatic complaints, suggesting the possibility that somatic complaints are one of the starting points of cyberchondria.17 Hence, following the important antecedents identified by Zheng et al,7 we regarded Anxiety sensitivity (AS), intolerance of uncertainty (IU), and somatic complaints as three antecedents of cyberchondria to verify their relationship with cyberchondria in the context of China.
For the outcomes of cyberchondria, previous studies have demonstrated that cyberchondria can be associated with a variety of psychosocial problems.7 As pointed out by recent studies, cyberchondria can contribute to impairment of one’s psychosocial functioning, and is associated with increased symptoms of depression and increased functional impairment.9,38 Furthermore, problematic internet use (PIU) as a form of maladaptive behavior may also be a result of cyberchondria, given that its constructs reflect an uncontrollability of internet use, which has been confirmed by many studies.39–41 The goal of the following investigation was thus to examine whether depression, functional impairment and PIU are outcomes of cyberchondria in the context of China.
Sample 3
Data in this study were collected from 199 healthy Chinese undergraduates. These students were recruited from a university in the city of Jinan, located in Shandong Province, Eastern China. All questionnaires were administered using paper and pencil. After exclusion of questionnaires with substantial missing information or unreliable response patterns, 198 valid responses were identified. The sample was primarily female (57.1% female), with ages ranging from 17 to 22 (M = 18.929, SD = 0.790). All of the procedures involved in this study are consistent with the ethical standards of the Academic Board of Shandong Normal University and the 1964 Helsinki Declaration and subsequent revised ethical standards. The participants provided written, informed consent voluntarily and anonymously and had the right to withdraw from the research program at any time.
Measure
The Patient Health Questionnaire-15 (PHQ-15)
The symptoms inquired about in the PHQ-15 include 14 of the 15 most prevalent DSM-IV somatic symptom disorders.42 In determining the PHQ-15 score, each individual symptom is coded as 0, 1, or 2, and the total score ranges from 0 to 30. The application of the Chinese version of PHQ-15 in a general population has shown good reliability and validity,43 and α = 0.718 in this study.
Sheehan Disability Scale (SDS)
The SDS is a 3-item self-report measure that assesses mental health-related impairment in three domains: (1) work/school; (2) social life/leisure; and (3) family life/home responsibilities. Participants were asked to respond on a 10-point Likert scale ranging from 0 (no impairment) to 10 (extreme). Previous research has shown the SDS to have strong psychometrics in Chinese samples,44 and α = 0.879 in this study.
Chinese-Internet Addiction Test (CIAT)
The CIAT measures internet addiction in five domains: (1) compulsion; (2) withdrawal behaviors; (3) tolerance; (4) interpersonal relationship and health; and (5) time management. Participants use a 4-point Likert scale to indicate the extent to which they experience internet addiction. The CIAT assessment has demonstrated strong psychometrics in previous studies,45 and α = 0.940 in this study.
Intolerance of Uncertainty Scale-12 (IUS-12)
The IUS-27 was originally developed with French samples to assess reactions to uncertainty, ambiguous situations, and the future.46 The IUS-12 is a short version of the 27-item IUS, which assesses prospective and inhibitory IU.47 IUS-12 assesses IU on a Likert scale ranging from 1 (not at all characteristic of me) to 5 (entirely characteristic of me), and demonstrated good internal consistency among Chinese participants,48 and α = 0.860 in this study.
Anxiety Sensitivity Index-3 (ASI-3)
The ASI-3 is an 18-item version of the original ASI49 intended to assess cognitive, physical and social anxiety sensitivities. The ASI-3 consists of 18 items, with each item rated using a five-point Likert scale indicating frequency (from 0 to 4). The Chinese version of ASI-3 has shown good validity and reliability in a clinical Chinese sample,50 and α = 0.894 in this study.
Beck Depression Inventory-II (BDI-II)
The 21-item BDI-II is a commonly used self-report measure of the severity of depression. Each item is rated on a four-point scale (ranging from 0 to 3), reflecting the degree of depression symptoms. The BDI-II was validated in Chinese clinical and nonclinical samples, and demonstrated adequate reliability and validity,51 and α = 0.812 in this study.
Results
The relationship between C-CSS and the three antecedents is shown in Table 4. Specifically, anxiety sensitivity, patient health, and intolerance of uncertainty all positively predicted negative effects, excessiveness, and total C-CSS (p < 0.001). In general, the high level of anxiety sensitivity, patient health, and intolerance of uncertainty can be viewed as three antecedents of cyberchondria measured by C-CSS. However, it should be noted that patient health and intolerance of uncertainty did not significantly predict reassurance (p > 0.05).
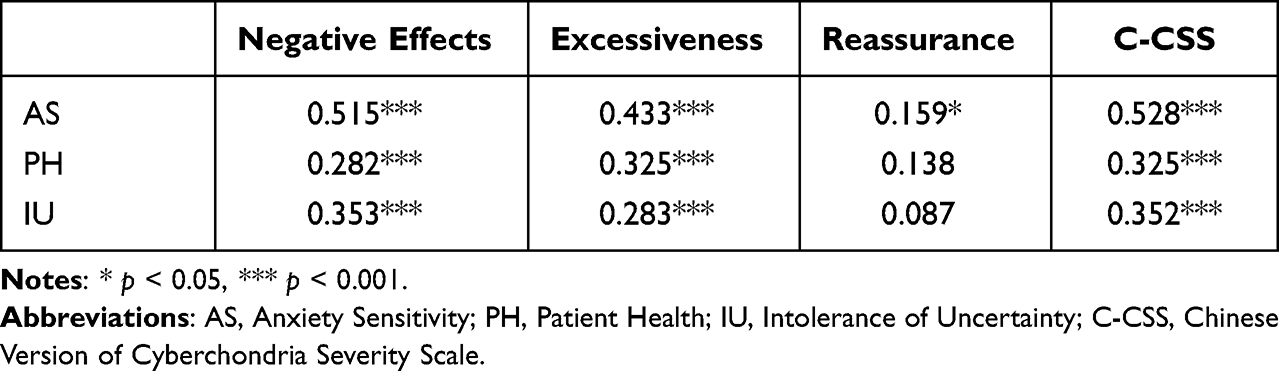 |
Table 4 Antecedents of Cyberchondria Measured by C-CSS |
The correlations between cyberchondria and the three outcomes are provided in Table 5. Cyberchondria measured by C-CSS had significant predictive effects on depression (p < 0.001), functional impairment (p < 0.001), and internet addiction (p < 0.01). However, reassurance exerted a nonsignificant predictive effect on functional impairment, depression and internet addiction (ps > 0.05). In sum, the new multidimensional C-CSS was related to theoretically relevant outcomes.
 |
Table 5 Outcomes of Cyberchondria Measured by C-CSS |
Discussion
As the first assessment tool founded on a multidimensional structure of cyberchondria, CSS has been translated into many languages, and has shown good psychometric characteristics across different cultures.13 In this study, we translated the CSS, and evaluated its reliability and validity in Chinese samples. Due to the differences in system and culture between Chinese and foreign countries, we merged the corresponding dimensions and removed some items, finally ending up with a version featuring 18 items and 3 dimensions, which demonstrated good psychometric properties.
In Study 1a, the factor structure of CSS was explored in a Chinese context. The results of EFA analysis indicated that the new three-factor measurement structure was successfully obtained from the modified 18-item C-CSS. 15 items were deleted due to not being in line with the acceptable criteria, or not being suitable for the unique cultural Chinese background. First, following the advice of Fergus12 and Norr et al18 the “mistrust” dimension (items 9, 28, 33) was deleted due to decreasing the reliability of the scale, its theoretical ambiguity, low correlations with the other four factors, as well as may not be relevant to a Chinese social context. Considering the imperfect basic medical care (eg, long queues) and unbalanced economic income in China, it is often more convenient for people to diagnose themselves online instead of going to hospital; this motivation to seek information online, however, is less likely to be attributed to the mistrust of medical professionals. Notably, Barke et al17 suggested that a shortened version of CSS is worth taking into consideration, due to its increased response rates, as well as its good internal consistency and validity. Accordingly, 7 items (10, 11, 18, 21, 27, 30, 32) were deleted due to the low-loading (< 0.50).
Afterwards, results showed that 3 items (3, 4, 5) had been allocated to a different factor for various reasons, and needed to be deleted. Item 3 (‘Researching symptoms or perceived medical conditions online interrupts my time spent on Facebook/Twitter/other social networks’) was reallocated from “Compulsion” to Excessiveness’. A possible explanation could be that people in different cultures have different attitudes towards social networks. Research has shown that online social networks are an important way to maintain interpersonal relationships for Chinese teenagers growing up in the subculture of the Internet.52 Thus, it is ‘excessive’ for individuals online search for health-related information to occupy more time than that spent on social networks.
The reason why item 4 (“Researching symptoms or perceived medical conditions online leads me to consult with my GP”) was reallocated from “reassurance” to “excessiveness” may be that from the perspective of China’s health system, family doctors are not popular. Going to the hospital is the most common way to consult doctors, which inevitably causes some problems, such as queuing and higher economic costs. In addition, the increasingly difficult doctor-patient relationship and the lack of trust in professional doctors have deterred patients from consulting doctors in recent years.53 Therefore, choosing to consult doctors can be regarded as an “excessive” choice for Chinese people when not feeling extremely ill.
In the exploratory factor analysis results, item 5 (“I have trouble relaxing after researching symptoms or perceived medical conditions online”) was reallocated from “Distress”, and had a cross loading between the negative effects and excessiveness dimensions, as difficulty in relaxing can be a result of “excessive” searching. Moreover, since items 19 and 20 were insufficient for forming a new dimension, we deleted them. Item 19 (“When I search a symptom online, I feel the ranking of the web search results reflects how common an illness is, with more likely medical conditions appearing higher up on the results page”) reflects an upgrade of search behavior, and was excluded from the “excessive” dimension. Under the background of the “collectivist” orientation in China, people are accustomed to visiting higher clicked websites, so viewing websites with higher page views as more reliable is a typical way for people to engage in self-diagnosis, rather than being an “excessive” behavior. Item 20 (“I think I am fine until I read about a serious condition online”) was excluded from the “distress” dimension, as it expresses changes in patients’ cognition instead of negative emotions. Finally, the distress and compulsion dimensions were combined according to the results of the EFA, which is consistent with the consideration that both “distress” and “compulsion” reflect the negative consequences caused by cyberchondria. Specifically, “distress” reflects internalizing problems, whereas “compulsion” reflects externalizing problems. Both were combined as one dimension named “negative effects”.
Confirmatory factor analysis (Study 1b) was used to test the psychometric properties of C-CSS. Concerning the construct validity, all items loaded on the corresponding dimensions, along with adequate concurrent and convergent validity. In addition, the scale demonstrated good criterion-related validity, which was confirmed by the strong correlation between cyberchondria and health anxiety and compulsion. Internal consistency was high for both the total scale and the subscales. These results provide support for the applicability of the 18-item C-CSS for the present Chinese sample. In sum, the results of the CFA support the measurement model, with three correlated but distinct subscales, namely negative effects, excessiveness and reassurance.
Understanding the antecedents of cyberchondria may be helpful for future studies investigating the condition. We explored the association between cyberchondria and three possible antecedents in Study 2, finding that AS, IU and PH are significant predictors of cyberchondria, as measured by C-CSS. Anxiety sensitivity (AS) refers to the fear of anxiety-related sensations which is caused by the belief that these sensations could lead to harmful consequences.54 A series of studies have supported the influence of both environmental factors and a genetic basis in child AS.55,56 For instance, Intrieri and Margentina55 demonstrated that individuals with insecure attachment show higher AS. According to the integrated model,57 insecure attachment offers an environment which could promote and maintain trait anxiety over time. Notably, these findings support a widespread comorbidity between cyberchondria and anxiety disorders, which in turn suggests that effective psychological intervention could reduce anxiety sensitivity and lower the risk of anxiety disorders such as cyberchondria. From the perspective of developmental contextualism and ecological systems theory, cyberchondria should be viewed as the result of the interaction of multiple factors. In order to comprehensively understand cyberchondria, it is valuable to further explore its antecedents.
We also examined associations between cyberchondria and outcomes. While cyberchondria has been portrayed as an anxiety-amplifying effect, our findings suggest that cyberchondria can also lead to other negative outcomes. We found that those who exhibited the highest scores on C-CSS were significantly more likely to experience depression, internet addiction and functional impairment. In line with existing evidence, negative moods which accompany cyberchondria, such as depression, might aggravate anxiety and even provoke mental disorders.3 This relationship between cyberchondria and functional impairment provides further support for the negative impact that cyberchondria can have on individuals’ normal life, potentially leading to overuse of medical services and posing a significant public health burden.9 Due to the relatively inelastic health care consumption, especially for rural dwellers, consumption inequality remains at a high level in China.58 Hence, in the context of a “healthy China” strategy, equalization of medical resources is an important issue. Addressing cyberchondria is not only conducive to individuals’ mental health, but also to alleviating the burden on stretched medical resources.
Limitations and Strengths
Although this study serves as a basis for future studies on cyberchondria in China, it has several limitations. First, the accuracy of the self-report data heavily depends on participant honesty, which may affect the experimental results to some extent. In addition, the cross-sectional design of this study prevents us from exploring the longitudinal stability of C-CSS subscales, and limits our ability to elucidate the strength and direction of causal relationships with other variables. Some outcomes, such as depression and problematic internet use, might plausibly act as antecedents. Furthermore, with the development of cyberchondria, the use of non-clinical samples does not allow us to draw conclusions about the relationship between C-CSS factor structure and health anxiety in clinical samples. Most cyberchondria study samples concentrate on teenagers, without understanding or distinguishing the profile of cyberchondria for other age groups (eg, teenagers and the elderly).
In spite of these limitations, the first psychometric evaluation of the C-CSS in a large sample of Chinese undergraduates has yielded encouraging results. Our findings support the argument that cross-cultural validation is necessary when seeking to apply CSS in different cultural settings. While C-CSS can be readily employed as an instrument for assessing cyberchondria, further research is needed to provide a better understanding of cyberchondria and its measurement in China.
The current study has identified several possible negative outcomes of cyberchondria, and has emphasized the importance of timely interventions. Future longitudinal studies would be valuable in order to confirm the causal relationship between cyberchondria and these variables.
Conclusion
Our results support the three-factor structure of cyberchondria in a Chinese context. The C-CSS demonstrated high internal consistency, along with adequate concurrent and convergent validity, and the criterion-related validity of C-CSS was supported by significant correlations between cyberchondria and health anxiety and compulsion. The current study determined the structure of C-CSS, and clarified the relationship between cyberchondria, as assessed by C-CSS, and the antecedent and outcome variables, thus laying the foundation for the application of C-CSS. Meanwhile, this study initially demonstrated the applicability of C-CSS to assess the severity of cyberchondria among Chinese undergraduates.
Data Sharing Statement
Research data are not shared.
Acknowledgments
This work was supported by General Project of Education in 2020 for the 13th Five-Year Plan of the National Social Science Fund of China: A longitudinal study on the development of overparenting and its impact on the psychosocial adjustment of early adolescents (grant no. BBA200036).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ding JL, Yang ZH. Cyberchondria: definition, Influencing Factors and Intervention Methods. Chine General Practice. 2015;18(16):134–138.
2. Mcdaid D, Park AL. Online Health: Untangling the Web. Bupa; 2010.
3. White RW, Horvitz E. Cyberchondria. ACM Transactions on Information Systems.Int J Med. 2009;27(4):1–37.
4. Norr AM, Oglesby ME, Raines AM, Macatee RJ, Allan NP, Schmidt NB. Relationships between cyberchondria and obsessive-compulsive symptom dimensions. Psychiatry Res. 2015;230(2):441–446. doi:10.1016/j.psychres.2015.09.034
5. Fergus TA. Cyberchondria and Intolerance of Uncertainty: examining When Individuals Experience Health Anxiety in Response to Internet Searches for Medical Information. Cyberpsychol Behav Soc Netw. 2013;16(10):735–739. doi:10.1089/cyber.2012.0671
6. Harding KJ, Skritskaya N, Doherty E, Fallon BA. Advances in understanding illness anxiety. Curr Psychiatry Rep. 2008;10(4):311–317. doi:10.1007/s11920-008-0050-1
7. Zheng H, Sin SCJ, Kim HK, Theng YL. Cyberchondria: a systematic review. Internet Res. 2020;31(2):677–698. doi:10.1108/INTR-03-2020-0148
8. Starcevic V, Berle D. Cyberchondria: towards a better understanding of excessive health-related Internet use. Expert Rev Neurother. 2013;13(2):205–213. doi:10.1586/ern.12.162
9. Mathes BM, Norr AM, Allan NP, Albanese BJ, Schmidt NB. Cyberchondria: overlap with health anxiety and unique relations with impairment, quality of life, and service utilization. Psychiatry Res. 2018;261:204–211. doi:10.1016/j.psychres.2018.01.002
10. Norr AM, Albanese BJ, Oglesby ME, Allan NP, Schmidt NB. Anxiety sensitivity and intolerance of uncertainty as potential risk factors for cyberchondria. J Affect Disord. 2015;174(174C):64–69. doi:10.1016/j.jad.2014.11.023
11. Starcevic V. Cyberchondria: challenges of Problematic Online Searches for Health-Related Information. Psychother Psychosom. 2017;86(3):129–133. doi:10.1159/000465525
12. Fergus TA. The Cyberchondria Severity Scale (CSS): an examination of structure and relations with health anxiety in a community sample. J Anxiety Disord. 2014;28(6):504–510. doi:10.1016/j.janxdis.2014.05.006
13. McElroy E, Shevlin M. The development and initial validation of the cyberchondria severity scale (CSS). J Anxiety Disord. 2014;28(2):259–265. doi:10.1016/j.janxdis.2013.12.007
14. Ivanova SKE. Elaborating on internet addiction and cyberchondria – relationships, direct and mediated effects. J Education Culture Society. 2014;1:17.
15. McManus F, Leung C, Muse K, Williams JMG. Understanding “cyberchondria”: an interpretive phenomenological analysis of the purpose, methods and impact of seeking health information online for those with health anxiety. Cognitive Behav Therapist. 2014;7(21):1–13. doi:10.1017/S1754470X14000270
16. Uzun SU, Zencir M. Reliability and validity study of the Turkish version of cyberchondria severity scale. Curr Psychol. 2018.
17. Barke A, Bleichhardt G, Rief W, Doering BK. The Cyberchondria Severity Scale (CSS): German Validation and Development of a Short Form. Int J Behav Med. 2016;23(5):595–605. doi:10.1007/s12529-016-9549-8
18. Norr AM, Allan NP, Boffa JW, Raines AM, Schmidt NB. Validation of the cyberchondria severity scale (CSS): replication and extension with bifactor modeling. J Anxiety Disord. 2015;31:58–64. doi:10.1016/j.janxdis.2015.02.001
19. Yan WN. How to ensure that rural areas have quality medical resources. Money China. 2014;19:281–282.
20. Wang JC. Eliminate prejudice against mental illness. Fam Med. 1996;17:26.
21. Tabachnick BG, Fidell LS. Using Multivariate Statistics.
22. Costello AB, Osborne JW. Exploratory Factor Analysis: four recommendations for getting the most from your analysis. Practical Assessment Res Evaluation. 2005;10(7):1–9.
23. Salkovskis PM, Rimes KA, Warwick HMC, Clark DM. The Health Anxiety Inventory: development and validation of scales for the measurement of health anxiety and hypochondriasis. Psychol Med. 2002;32(05):843–853. doi:10.1017/S0033291702005822
24. Yuan Y, Zhang Y, Liu R, Li G, Mao S, The reliability and validity of a Chinese-version Short Health Anxiety Inventory: an investigation of university students. Neuropsychiatr Dis Treat. 2015;11:1739–1747. doi:10.2147/NDT.S83501
25. Zhong J, Tan JQ, Kuang HY. Difference of Words Recognition in High and Low Obsessive Compulsive Symptom individuals. Acta Psychologica Sinica. 2005;37(6):753–759.
26. Yuan KH, Bentler PM. Three likelihood-based methods for mean and covariance structure analysis with nonnormal missing data. Sociol Methodol. 2010;30(1):165–200. doi:10.1111/0081-1750.00078
27. Bentler PM. Comparative fit indexes in structural models. Psychol Bull. 1990;107(2):238–246. doi:10.1037/0033-2909.107.2.238
28. Browne MW, Cudeck R. Alternative ways of assessing model fit. Sociol Methods Res. 1992;21(2):230–258. doi:10.1177/0049124192021002005
29. Bollen KA. Overall fit in covariance structure models: two types of sample size effects. Psychol Bull. 1990;107(2):256–259. doi:10.1037/0033-2909.107.2.256
30. Hu LT, Bentler PM. Fit indices in covariance structure modeling: sensitivity to underparameterized model misspecification. Psychol Methods. 1998;3(4):424–453. doi:10.1037/1082-989X.3.4.424
31. Nunnally JC. An Overview of Psychological Measurement. Clinical Diagnosis of Mental Disorders. Springer US; 1978.
32. Fornell C, Larcker DF. Evaluating structural equation models with unobservable variables and measurement error. J Marketing Res. 1981;18(1):39–50. doi:10.1177/002224378101800104
33. McLaughlin EN, Stewart SH, Taylor S. Childhood anxiety sensitivity index factors predict unique variance in DSM‐IV anxiety disorder symptoms. Cogn Behav Ther. 2007;36(4):210–219. doi:10.1080/16506070701499988
34. Wright KD, Lebell MANA, Carleton RN. Intolerance of uncertainty, anxiety sensitivity, health anxiety, and anxiety disorder symptoms in youth. J Anxiety Disord. 2016;41:35–42. doi:10.1016/j.janxdis.2016.04.011
35. Dixon LJ, Lee AA, Gratz KL, Tull MT. Anxiety sensitivity and sleep disturbance: investigating associations among patients with co-occurring anxiety and substance use disorders. J Anxiety Disord. 2018;53:9–15. doi:10.1016/j.janxdis.2017.10.009
36. Fergus TA. Anxiety sensitivity and intolerance of uncertainty as potential risk factors for cyberchondria: a replication and extension examining dimensions of each construct. J Affect Disord. 2015;184:305–309. doi:10.1016/j.jad.2015.06.017
37. Jokić-Begić N, Mikac U, Čuržik D, Jokić CS. The development and validation of the short cyberchondria scale (SCS). J Psychopathol Behav Assess. 2019;41(4):662–676. doi:10.1007/s10862-019-09744-z
38. Doherty-Torstrick ER, Walton KE, Fallon BA. Cyberchondria: parsing health anxiety from online behavior. Psychosomatics. 2016;57(4):390–400. doi:10.1016/j.psym.2016.02.002
39. Fergus TA, Dolan SL. Problematic internet use and internet searches for medical information: the role of health anxiety. Cyberpsychol Behav Soc Netw. 2014;17(12):761–765. doi:10.1089/cyber.2014.0169
40. Fergus TA, Spada MM. Cyberchondria: examining relations with problematic internet use and metacognitive beliefs. Clin Psychol Psychother. 2017;24(6):1322–1330. doi:10.1002/cpp.2102
41. Starcevic V, Baggio S, Berle D, Khazaal Y, Viswasam K. Cyberchondria and its relationships with related constructs: a network analysis. Psychiatr Q. 2019;90(3):491–505. doi:10.1007/s11126-019-09640-5
42. Liu G, Clark MR, Eaton WW. Structural factor analyses for medically unexplained somatic symptoms of somatization disorder in the Epidemiologic Catchment Area Study. J Psychosom Res. 1997;42:245–252. doi:10.1016/s0022-3999(96)00292-9
43. Lee S, Ma YL, Tsang A. Psychometric properties of the Chinese 15-item patient health questionnaire in the general population of Hong Kong. J Psychosom Res. 2011;71(2):69–73. doi:10.1016/j.jpsychores.2011.01.016
44. Leu SH, Chou JY, Lee PC, et al. Validity and reliability of the Chinese version of the Sheehan disability scale (SDS-C). Asia Pacific Psychiatry. 2015;7(2):215–222. doi:10.1111/appy.12182
45. Chen AH, Weng LZ, Su YR. Research of establishment and psychometric characteristics of Chinese Internet Addiction Scale. Chine J Psychol. 2003;45(3):279–294.
46. Freeston MH, Rhéaume J, Letarte H, Dugas MJ, Ladouceur R. Why do people worry? Pers Individ Dif. 1994;17(6):791–802. doi:10.1016/0191-8869(94)90048-5
47. Carleton RN, Norton MAPJ, Asmundson GJG. Fearing the unknown: a short version of the intolerance of uncertainty scale. J Anxiety Disord. 2007;21(1):105–117. doi:10.1016/j.janxdis.2006.03.014
48. Yang ZH. Psychometric properties of the intolerance of uncertainty scale (IUS) in a Chinese-speaking population. Behav Cogn Psychother. 2013;41(4):500–504. doi:10.1017/S1352465812000975
49. Maller RG, Reiss S. A behavioral validation of the anxiety sensitivity index. J Anxiety Disord. 1987;1(3):265–272. doi:10.1016/0887-6185(87)90031-4
50. Wang L, Liu WT, Zhu XZ, Wang YP, Li LY, Yang YL. Validity and reliability of the Chinese Version of the Anxiety Sensitivity Index-3 in healthy adult women. Chine j Mental Health. 2014;28(10):767–771.
51. Yang WH, Liu SL, Zhou T, et al. Reliability and Validity of Chinese Version of the Beck Depression Inventory-II; in Chinese Adolescents. Chine j Clin Psychol. 2014;22(2):240–245.
52. Yang ZR. The influence of social media on the interpersonal relationship of Chinese youth groups —— a case study of WeChat “thumb up”. New Media Res. 2019;15:39–40.
53. Wang H, Liu JL. Relational Hospitalization and Relational Trust: a Cognitive Shortcut for Chinese Doctor-Patient Initial Trust Judgments. Rev Chine Social Psychol. 2018;14:161–171.
54. McNally RJ, Reiss S. The preparedness theory of phobias and human safety-signal conditioning. Behav Res Ther. 1982;20(2):153–159. doi:10.1016/0005-7967(82)90114-0
55. Intrieri RC, Margentina SJ. Attachment and its relationship to anxiety sensitivity. Curr Psychol. 2017;5:1–15.
56. Stassart C, Dardenne B, Etienne AM. Specificity of gender role orientation, biological sex and trait emotional intelligence in child anxiety sensitivity. Pers Individ Dif. 2014;71:165–170. doi:10.1016/j.paid.2014.07.040
57. Manassis K, Bradley SJ. The development of childhood anxiety disorders: toward an integrated model. J Appl Dev Psychol. 1994;15(3):345–366. doi:10.1016/0193-3973(94)90037-X
58. Zhao GC, Ma C. The influence of rural residents’ income on the inequality of medical care consumption in China. Consumption Economy. 2019;35(5):14–21.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Validation of the Connor-Davidson Resilience Scale-10 in South Africa: Item Response Theory and Classical Test Theory
Pretorius TB, Padmanabhanunni A
Psychology Research and Behavior Management 2022, 15:1235-1245
Published Date: 16 May 2022
Validity and Reliability of the Thai Version of the 19-Item Compliance-Questionnaire-Rheumatology
Panichaporn S, Chanapai W, Srisomnuek A, Thaweeratthakul P, Katchamart W
Patient Preference and Adherence 2022, 16:2149-2158
Published Date: 17 August 2022
Psychometric Properties of the Montreal Cognitive Assessment (MoCA) to Detect Major Neurocognitive Disorder Among Older People in Ethiopia: A Validation Study
Daniel B, Agenagnew L, Workicho A, Abera M
Neuropsychiatric Disease and Treatment 2022, 18:1789-1798
Published Date: 22 August 2022
Development and Initial Validity of the Patients’ Literacy Scale Among Outpatients in Hangzhou City, China
Jiang D, Sang T, Xiao X, Wu Z, Wang H, Yang Q
Patient Preference and Adherence 2022, 16:2483-2496
Published Date: 7 September 2022
Development and Validation of the Patient/Caregiver Reported Hydroxyurea Evaluation of Adherence for Life (HEAL) Scale
Janson IA, Bloom EM, Hampton KC, Meier ER, Rampersad AG, Kronenberger WG
Patient Preference and Adherence 2022, 16:3229-3239
Published Date: 10 December 2022