Back to Journals » Journal of Pain Research » Volume 19
Comparison of Quadratus Lumborum Plus Modified Erector Spinae Plane Block versus Pericapsular Nerve Group Block Plus Lateral Femoral Cutaneous Block on Postoperative Analgesia and Functional Recovery in Total Hip Arthroplasty: A Retrospective Propensity Score-Matched Study
Authors Wu X, Wang M, Du M, Wang Y, Chen X, Zhang D, Xu Y
Received 15 September 2025
Accepted for publication 7 January 2026
Published 13 January 2026 Volume 2026:19 567827
DOI https://doi.org/10.2147/JPR.S567827
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Rushna Ali
Xi Wu,1– 3,* Meiying Wang,1– 3,* Mengqi Du,1– 3 Yu Wang,1– 3 Xiangdong Chen,1– 3 Dingyu Zhang,4 Younian Xu1
1Department of Anesthesiology, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430022, People’s Republic of China; 2Institute of Anesthesia and Critical Care Medicine, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430022, People’s Republic of China; 3Key Laboratory of Anesthesiology and Resuscitation (Huazhong University of Science and Technology), Ministry of Education, Wuhan, People’s Republic of China; 4Department of Critical Care Medicine, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Dingyu Zhang, Department of Critical Care Medicine, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China, Email [email protected] Younian Xu, Department of Anesthesiology, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430022, People’s Republic of China, Email [email protected]
Purpose: Ultrasound-guided quadratus lumborum plus modified erector spinae plane (QLESP) block and pericapsular nerve group (PENG) plus lateral femoral cutaneous nerve (LFC) block are novel regional analgesia techniques for total hip arthroplasty (THA). This retrospective study aimed to compare the analgesic efficacy and opioid-related outcomes of the QLESP block and the PENG + LFC block following THA.
Methods: This retrospective study included 2180 patients who underwent THA between January 2022 and December 2024. In this study, 272 patients received the QLESP block (QLESP group) and 420 patients accepted the PENG + LFC block (PELF group). Propensity score matching (PSM) was performed to match patients in a 1:1 ratio.
Results: Of 2180 patients identified, 256 pairs between QLESP group and PELF group were successfully matched. In the match cohort, the QLESP group demonstrated significantly lower cumulative sufentanil consumption (QLESP: 13.0 ± 1.3 μg; PELF: 14.6 ± 3.3 μg; p < 0.001) and patient-controlled intravenous analgesia (PCIA) frequency (QLESP: 1 (0– 3); PELF: 2 (0– 4); P < 0.001) at 6 hours postoperatively compared to the PELF group. Additionally, the QLESP group was associated with a lower incidence of rescue analgesia (QLESP: 9.0%; PELF: 15.2%; P = 0.030) and a shorter postoperative length of stay (QLESP: 10.6 ± 6.0 days; PELF: 11.7 ± 6.2 days; P = 0.038). No significant differences were found in visual analogue scale (VAS) or time to first walk.
Conclusion: This observational study suggested that the QLESP block was associated with a modest reduction in early postoperative sufentanil consumption, PCIA frequency at 6 hours, and postoperative length of stay for total hip arthroplasty, compared to PENG + LFC block. Given the inherent limitations of the retrospective PSM design, the routine incorporation of these blocks into enhanced recovery pathways for total hip arthroplasty in clinical practice warrants further large randomized controlled trials.
Keywords: erector spinae plane block, lateral femoral cutaneous nerve, pericapsular nerve group block, postoperative analgesia, quadratus lumborum block, total hip arthroplasty
Introduction
Total hip arthroplasty (THA) is a painful surgical procedure performed to improve mobility and quality of life in patients with severe hip joint pathology.1 Inadequate analgesia may cause postoperative adverse effects, such as hindered recovery, hypercoagulable thrombosis, and delayed hospital discharge.2,3 Peripheral nerve blocks (PNBs), including fascia iliaca block, lumbar plexus block, and femoral nerve block, are commonly applied to multimodal analgesia in THA.4,5 However, these techniques are associated with the inherent risks of quadriceps femoris weakness, which can increase the risk of postoperative falls.6,7 Given the growing emphasis on enhanced recovery after surgery, the optimal regional technique for THA should balance analgesic benefits with motor function preservation.8,9
The pericapsular nerve group block (PENG), first described by Giron-Arango et al in 2018, targets articular branches of the femoral, obturator, and para-obturator nerves.10 Theoretically, this technique could reserve a pure sensory block without motor disability.11 A recent educational article suggested that undesirable spread of local anesthetics and quadriceps weakness could occur after PENG block, which might be related to injectate spreading to the femoral nerve from several routes.12 Furthermore, the PENG block does not cover the skin incision of posterolateral approach innervated by lateral femoral cutaneous nerve (LFC), potentially resulting in inadequate analgesia.13 Thus, the PENG block could be combined with the LFC block in THA operation.14–16 Previously, our team reported a novel QLESP block described as performing transmuscular quadratus lumborum and modified erector spinae plane block with a single-puncture technique.17,18 This technique is characterized by simplicity, high efficiency, and adequate dermatomal sensory block coverage. It is not clear whether the QLESP block was superior to PELF block for managing postoperative pain management and early mobilization in patients undergoing THA.
Although a few prior trials have compared PENG with quadratus lumborum block for hip surgery, our investigation features essential differences. Several studies adopted the lateral quadratus lumborum block which was different from the trans-muscular approach in our study.19,20 Several trials performed PENG block alone without the combination of LFC block.21–23 Additionally, some reported similar effectiveness of analgesic effects and functional recovery using PENG and quadratus lumborum block.20,22 However, some studies have reported contradictory conclusions for postoperative analgesia and motor function with the two blocks.19,21,23
In this retrospective trial, we aimed to compare the analgesic effects of the ultrasound-guided QLESP block versus PENG + LFC block as part of a non-opioid analgesia regimen for THA patients. The primary outcome was cumulative sufentanil consumption, frequency of PCIA and VAS pain scores within the initial 24 h postoperative period. The secondary objectives were the incidence of rescue analgesia, time to first walk after THA, opioid-related adverse effects, block-related side-effects, intra-operative intravenous fluid and blood loss, urine output, and postoperative length of stay between the two groups. We hypothesized that the QLESP block might offer superior analgesia and facilitate earlier mobilization for total hip arthroplasty in comparison with the PENG + LFC block.
Materials and Methods
Patients
The study complied with the principles underlying the Declaration of Helsinki and received approval from the Ethics Committee of Union Hospital, Tongji Medical College, Huazhong University of Science and Technology (No. 863). Given the retrospective design and anonymous selection, written informed consent was waived.
For this retrospective study, the perioperative data of patients undergoing unilateral elective THA at the Union Hospital, Tongji Medical College, Huazhong University of Science and Technology from January 2022 to December 2024 were retrospectively reviewed and extracted from the anesthesia information management system. The database was maintained and updated by a specialized quality control team within our department, with the objective of ensuring the accuracy and comprehensiveness of medical records. Inclusion criteria were: (1) Patients received elective and unilateral total hip arthroplasty in a lateral-posterior approach; (2) aged 18–65 years; (3) ASA physical status 1 to 3. Exclusion criteria were: (1) An unconventional approach to total hip arthroplasty (THA); (2) patients with chronic pain caused by malignant tumors or other conditions; (3) patients with polytrauma; (4) patients underwent neither QLESP block nor PENG+LFC block; (5) lack of medical record. Finally, a total of 2180 patients were enrolled in the retrospective observational study. Comparisons between PELF group and QLESP group were adjusted by the propensity score matching (PSM) and a cohort of 256 matched patients were obtained.
Techniques
All patients with elective and unilateral total hip arthroplasty in a lateral-posterior approach received standardized general anesthesia and postoperative rehabilitation protocols according to our institutional ERAS guidelines. Upon arrival in the operating room, continuous electrocardiogram, non-invasive blood pressure, heart rate, pulse oximetry, and bispectral index (BIS) was established. After patients received the pre-oxygenation with 100% oxygen for 3 minutes, intravenous induction was performed with etomidate (0.2–0.5 mg/kg) and sufentanil (0.5 µg/kg). Endotracheal intubation was facilitated with cisatracurium (0.15–0.2 mg/kg). Anesthesia was maintained with a continuous infusion of remifentanil (0.1–0.2 μg/kg/min) and propofol (4–6 mg/kg/h) to maintain the bispectral index reading between 40 and 60 and to keep the mean arterial blood pressure and heart rate within ±20% of baseline.
For QLESP block, patients were placed in the lateral decubitus position. The QLESP block was performed according to the established technique, as previously described by our group. With sterile aseptic condition, a low-frequency ultrasound probe ((SonoSite M-Turbo; SonoSite Inc, Bothell, WA, USA)) was placed on the flank cranially to the iliac crest to identify the transverse process of L4, quadratus lumborum muscle, erector spinae muscle, and psoas muscle on the sonogram.24 An 18-gauge, 10-cm needle (SonoPlex Nanoline; Pajunk Inc., Geisingen, Germany) was inserted and 15 mL of 0.4% ropivacaine was delivered slowly between the erector spinae muscle and the transverse process. With the needle repositioning, the remaining 15 mL of 0.4% ropivacaine was injected into the interfascial plane between the quadratus lumborum and the psoas major muscles with negative aspiration (Figure 1A).
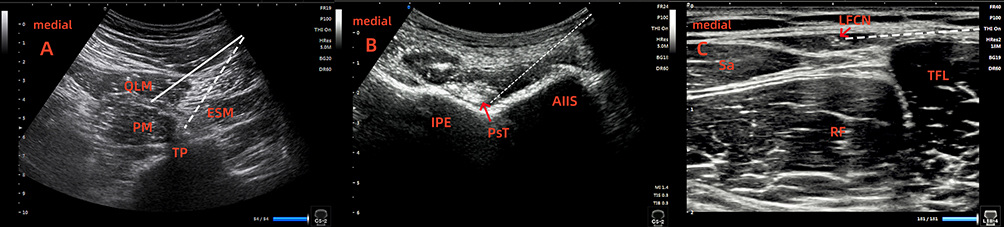 |
Figure 1 Ultrasound images for (A) quadratus lumborum and modified erector spinae plane (QLESP) block, (B) pericapsular nerve group (PENG) block, (C) lateral femoral cutaneous nerve (LFC) block. White dotted and solid lines indicate directions of needle. Red arrow in 1 (B) indicate PsT. Red arrow pointing to the target in 1 (C) indicate LFCN. Abbreviations: AIIS, anterior inferior iliac spine; ESM, erector spinae muscle; IPE, iliopubic eminence; LFCN, lateral femoral cutaneous nerve; PM, psoas muscle; PsT, psoas muscle tendon; QLM, quadratus lumborum muscle; RF, rectus femoris muscle; Sa, sartorius muscle; TFL, tensor fasciae latae muscle; TP, transverse process. |
For PENG block, patients were placed in the supine position. The low-frequency transducer was placed in a transverse orientation over the anterosuperior iliac, and the iliopsoas muscle and tendon, the anteroinferior iliac spine, and the iliopubic eminence were identified by rotating the probe counterclockwise approximately 45 degrees.10 After negative aspiration, 20 mL of 0.4% ropivacaine was injected between the psoas tendon and the pubic ramus with in-plane technique (Figure 1B). For LFC block, a high-frequency probe was placed on inguinal crease and scan proximally until the lateral end of probe lies over the anterior superior iliac spine to identify the fat-filled flat tunnel between the sartorius and the tensor fasciae latae muscle.25 With in-plane approach, the needle was inserted toward the flat tunnel in a lateral-to-medial direction and 10 mL of 0.4% ropivacaine was given following negative aspiration (Figure 1C).
All patients were transferred to the post-anesthesia care unit (PACU) for recovery after surgery. Postoperative PCIA pump was initiated for all patients upon arrival at the PACU, which was prepared by diluting sufentanil (100 µg) and tropisetron (5 mg) with 100 mL saline and set to deliver at a rate of 2 mL/h continuously with a 2 mL bolus injection with a 15-min lockout interval for 48 h. Tramadol (50 mg) was administered as rescue pain medications when patients reported VAS > 4. To ensure the accuracy of data collected from the computer cloud, education on the use of the analgesia pump was provided by a specialized nurse. All patients were managed under a standardized, multidisciplinary ERAS pathway for THA, adapted from established guidelines.26,27 Discharge readiness was determined by a multidisciplinary team using objective, functional criteria aligned with modern fast-track arthroplasty principles.2 Patients were approved for discharge only upon meeting all of the following criteria: functional milestones, adequate pain control, surgical stability, and patient readiness.28
Data Collection
The perioperative data were extracted from the anesthesia information management system. Demographics including age, sex, height, weight, ASA class, diagnosis, duration of the surgery, intraoperative sufentanil consumption, and waiting time to operation. The primary outcome included cumulative sufentanil consumption, frequency of PCIA, and VAS pain scores. The secondary outcomes included the incidence of rescue analgesia, time to first walk, operative blood loss, intraoperative intravenous fluid, urine output, opioid-related side-effects (postoperative nausea and vomiting, dizziness, respiratory depression), block-related side-effects (vascular puncture, local anesthetic systemic toxicity), length of PACU stay and postoperative length of stay. Time to first walk was defined as the interval between the end of surgery and the patients’ first postoperative ambulation (≥3 steps) with physical assistance.
The cumulative sufentanil consumption were calculated by PCIA which were systematically archived in a centralized cloud-based database at our institution. As part of the clinical pathway, VAS scores are recorded every 6 hours after entering the PACU by a PCIA nursing staff. Details of VAS scores at rest or on movement are not recorded. The opioid-related side-effects and puncture complications were documented by an investigator not involved with patient care during postoperative follow-up.
Statistics
Statistical analyses and the propensity score matching were conducted using SPSS 22.0 (IBM Corp., New York, USA), while graphical representations were generated with Prism 6.01 (Graph Pad Software, San Diego, CA, USA). Continuous variables are reported as mean ± standard deviation (SD) or median (range), while categorical variables are described as numbers (percentages). Group comparisons for normally distributed continuous variables were performed using the independent samples t-test, whereas the Mann–Whitney U-test was applied for non-normally distributed variables. Intragroup differences across time points were evaluated with a two-sided paired t-test. Categorical variables were compared via Chi-square test or Fisher’s exact test, as appropriate. A p-value <0.05 was considered to indicate statistical significance. To address potential selection bias, a propensity score matched analysis was employed to balance baseline characteristics between the PENG and PELF groups. Multivariate logistic regression model was constructed according to preoperatively known covariates including age, gender, height, weight, ASA class, diagnosis, duration of surgery, intra-operative sufentanil consumption, and pre-operative hospital stay. The propensity score was calculated via logistic regression analysis, and the nearest-neighbor algorithm was used with a caliper of 0.01. Patients in the PENG group were matched 1:1 to patients in the PELF group. After matching, standardized differences were calculated to confirm balance in baseline variables between the groups. The matched cohort was subsequently used to evaluate the association between treatment factors and the outcome. Supplementary Table S1 showed standardized mean differences (SMD) before and after propensity score matching. Supplementary Figure S1 illustrated Love plot visualizing the SMDs for each covariate before and after matching. After matching, 8 of 9 covariates achieved SMD below the 0.1 threshold (indicating good balance), with only “Weight” remaining slightly above at SMD = 0.165 (still within acceptable range of SMD < 0.2). The mean SMD decreased from 0.161 before matching to 0.061 after matching, representing an overall balance improvement of 62.3%. The percentage of discharged patients over time were visualized using Kaplan–Meier curves and compared using the Log rank test.
Results
Patient Characteristics
An initial retrieval identified 2180 records of elective and unilateral total hip arthroplasty between 1 January 2022 and 30 December 2024. Of these, 1488 records were excluded based on the inclusion and exclusion criteria. Finally, 512 records (256 patients per group) were finally matched out and included in the study (Figure 2). Several baseline characteristics showed significant differences before matching, including: patients who underwent QLESP tended to be younger, have a higher weight. Additionally, there was significant difference in preoperative diagnosis and ASA classification. After propensity score matching, all baseline characteristics were well balanced (Table 1).
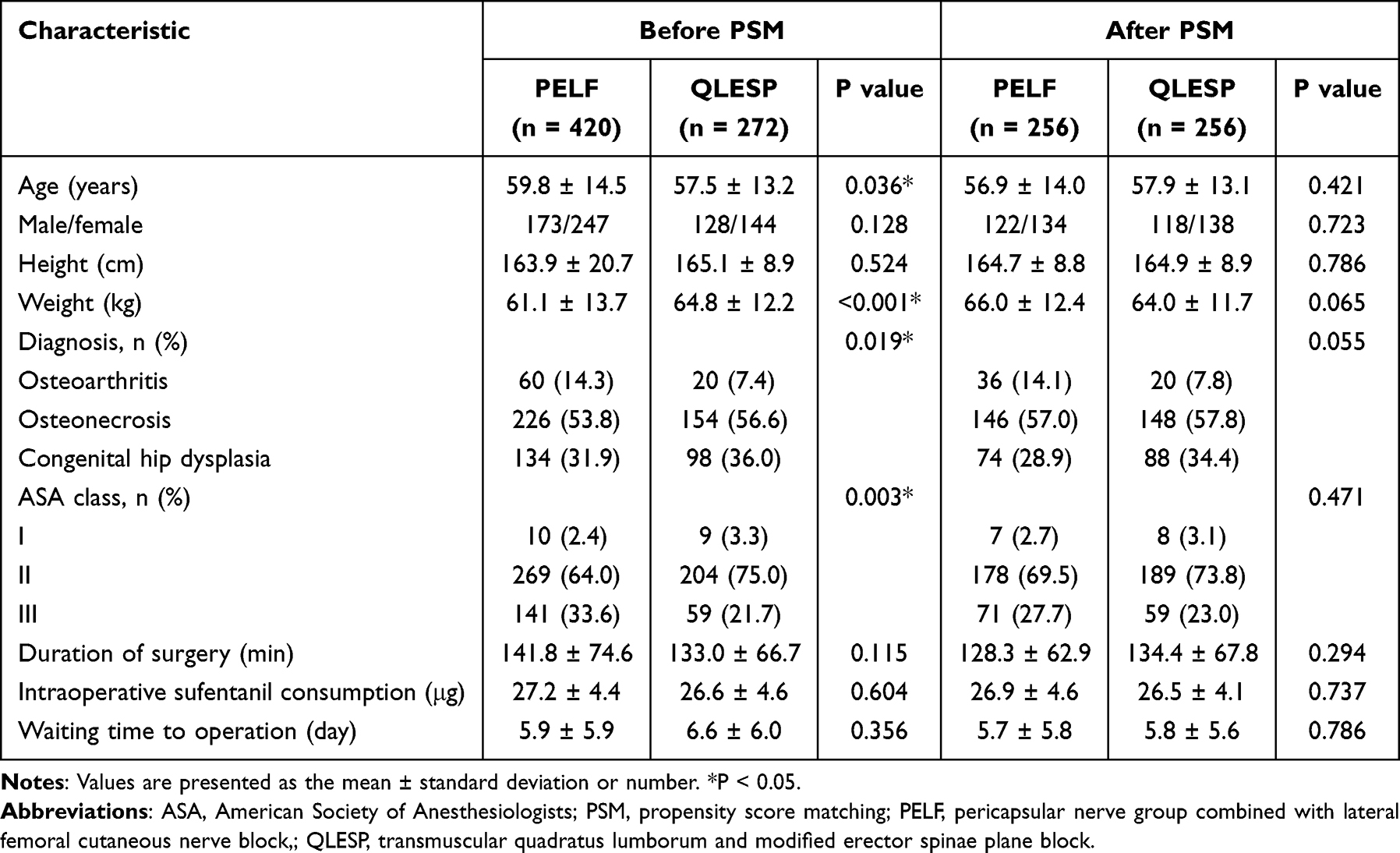 |
Table 1 Baseline Characteristics of Patients Before and After Propensity Score Matching |
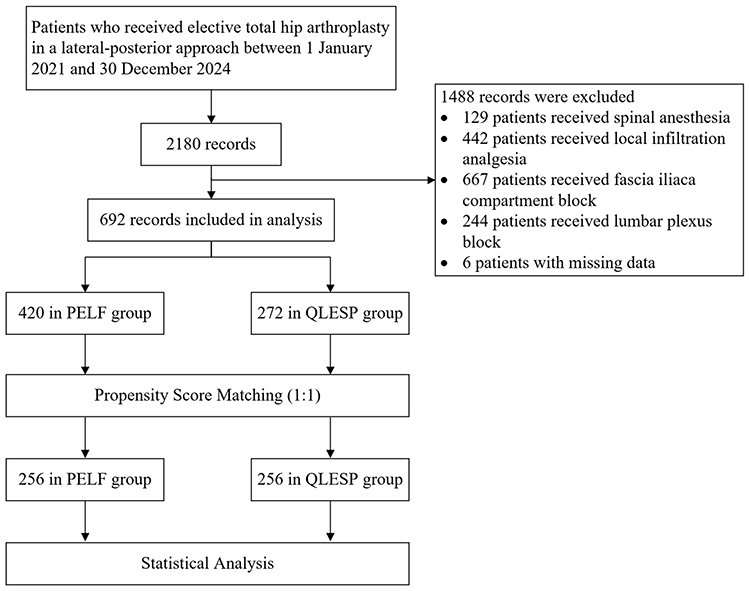 |
Figure 2 Flow diagram of selection, exclusion, and analysis. |
Primary Outcomes
Cumulative sufentanil consumption (QLESP: 13.0 ± 1.3 μg; PELF: 14.6 ± 3.3 μg; P < 0.001) was significantly lower in the QLESP group compared to the PELF group, after PSM. However, there was no significantly difference in cumulative sufentanil consumption between the groups at 12 hours postoperatively (QLESP: 28.6 ± 3.4 μg; PELF: 29.0 ± 4.0 μg; P = 0.317) and 24 hours postoperatively (QLESP: 56.6 ± 3.5 μg; PELF: 56.9 ± 4.1 μg; P = 0.379) (Table 2).
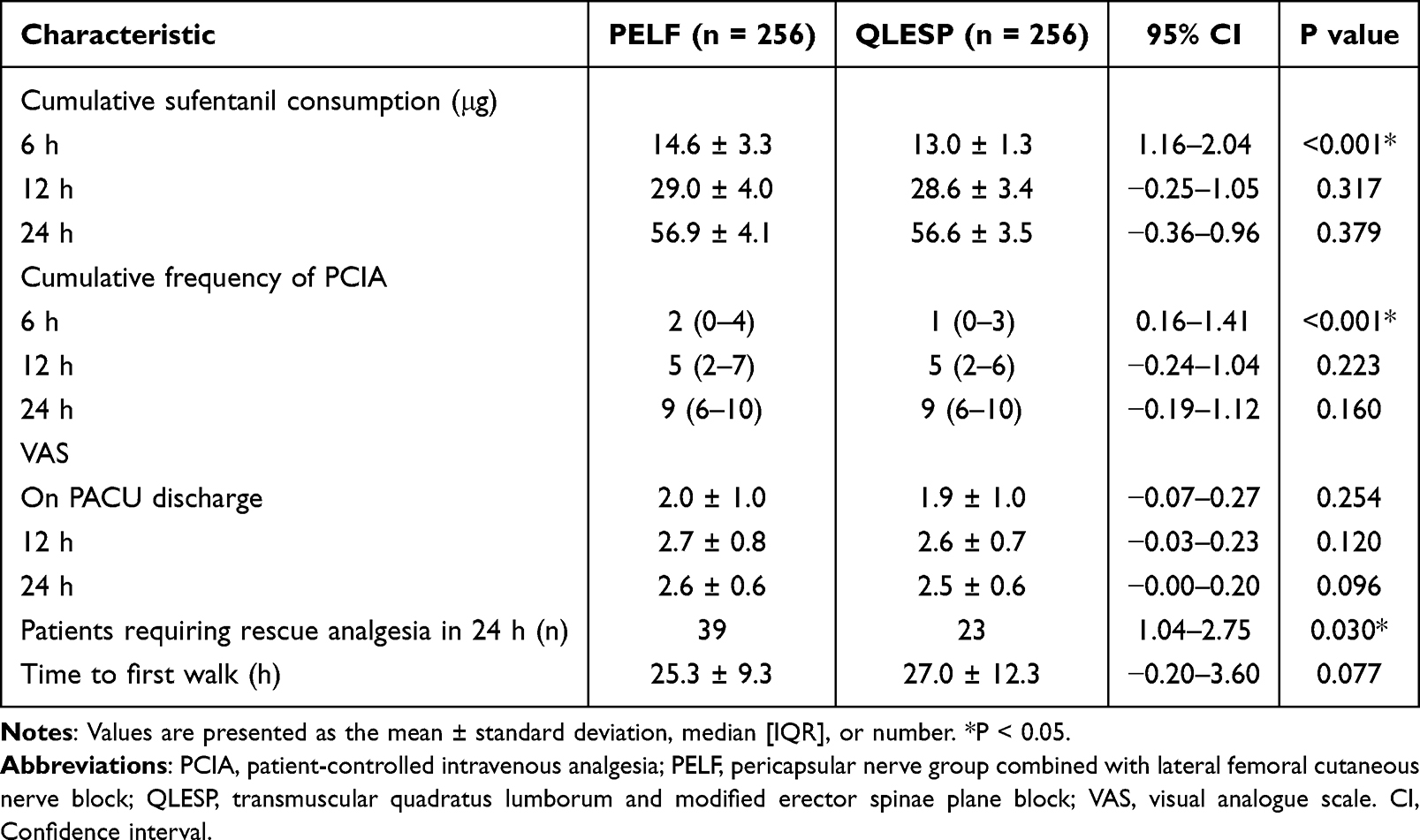 |
Table 2 Cumulative Sufentanil Consumption, Frequency of PCIA, VAS Scores and Motor Recovery Outcomes in the Matched Cohort |
In the matched cohort, the PCIA frequency (QLESP: 1 (0–3); PELF: 2 (0–4); P < 0.001) at 6 hours postoperatively was statistically significantly lower in the QLESP group. However, there was also no significantly difference in the cumulative frequency of PCIA at 12 hours postoperatively (QLESP: 5 (2–6); PELF: 5 (2–7); P = 0.223) and 24 hours postoperatively (QLESP: 9 (6–10); PELF: 9 (6–10); P = 0.160) (Table 2).
After PSM, the two groups had a similar VAS on PACU discharge (QLESP: 1.9 ± 1.0; PL: 2.0 ± 1.0; P = 0.254), postoperative 12 hours (QLESP: 2.6 ± 0.7; PELF: 2.7 ± 0.8; P = 0.120) and postoperative 24 hours (Q: 2.5 ± 0.6; PELF: 2.6 ± 0.6; P = 0.096) (Table 2).
Secondary Outcomes
After propensity score matching, the QLESP group demonstrated a significantly lower incidence of rescue analgesia within 24 hours postoperatively than the PELF group (9.0% vs 15.2%, P = 0.030) (Table 2).
No significant difference was found in time to first walk between the two groups (QLESP: 27.0 ± 12.3; PELF: 25.3 ± 9.3; P = 0.077) (Table 2). The postoperative length of stay was significantly shorter in the QLESP group than in the PELF group (QLESP: 10.6 ± 6.0 days; PELF: 11.7 ± 6.2 days; P = 0.038) (Table 3; Figure 3). However, no significant difference in PACU stay was found between the groups (QLESP: 34.6 ± 7.3 min; PELF: 33.4 ± 8.6 min; P = 0.625) (Table 3).
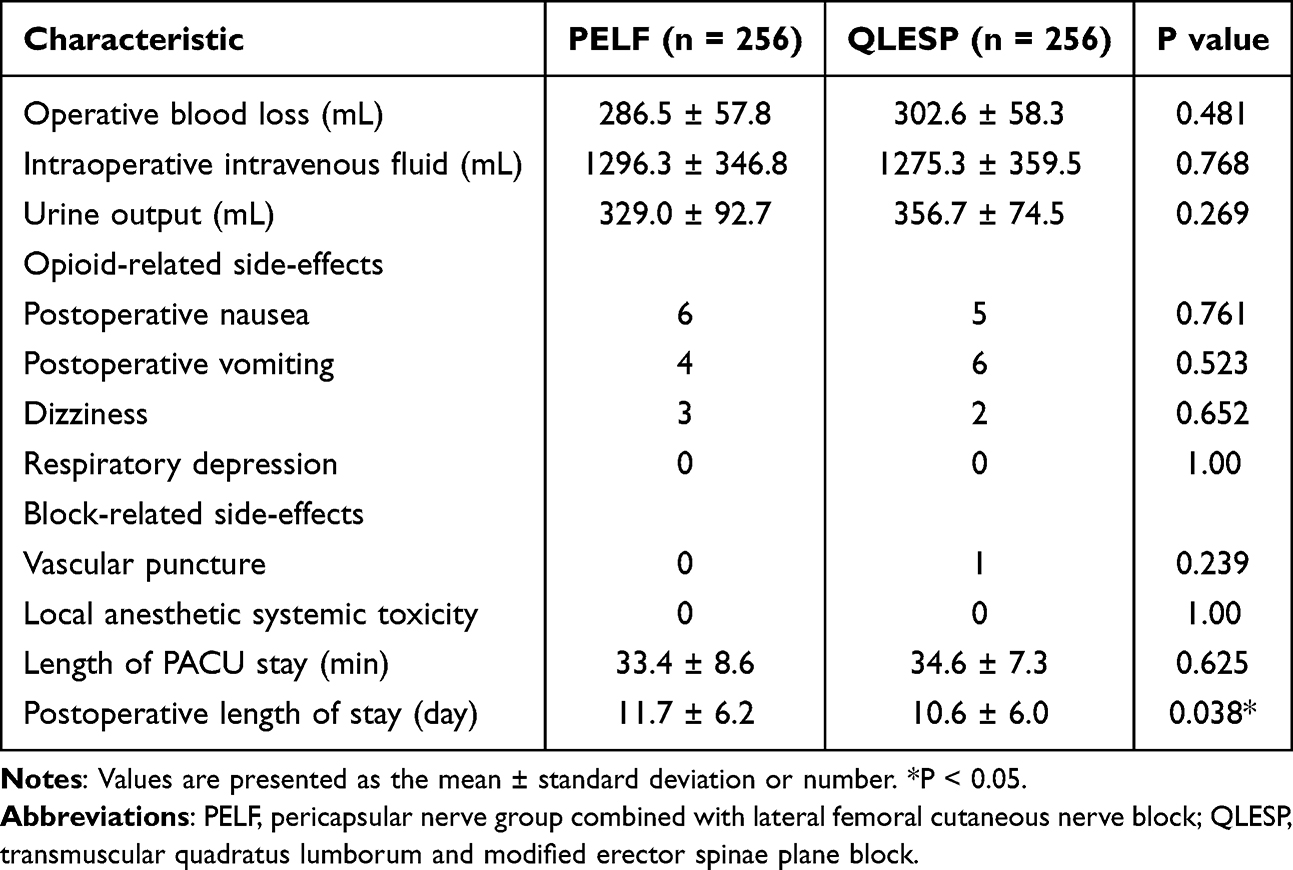 |
Table 3 Intra- and Postoperative Outcomes in the Matched Cohort |
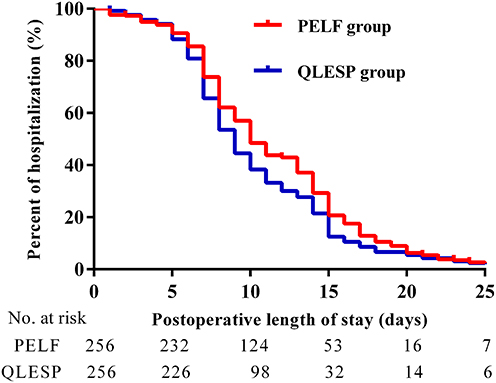 |
Figure 3 Kaplan‑Meier curves illustrating the post-operative length of hospital stay in the QLESP group and PELF group. Abbreviation: SMDs, standardized mean differences. |
In addition, patients in the QLESP group showed similar operative blood loss (QLESP: 302.6 ± 58.3 mL; PELF: 286.5 ± 57.8 mL; P = 0.481), intraoperative intravenous fluid (QLESP: 1275.3 ± 359.5 mL; PELF: 1296.3 ± 346.8 mL; P = 0.768), and urine output (QLESP: 356.7 ± 74.5 mL; PELF: 329.0 ± 92.7 mL; P = 0.269) as compared with the PELF group.
No significant differences were found in the incidences of postoperative nausea, vomiting, dizziness, respiratory depression, vascular puncture, or local anesthetic systemic toxicity between the two groups (Table 3).
Discussion
This retrospective propensity score-matched analysis indicated that QLESP block was correlated with reductions in the use of postoperative sufentanil consumption, 6-hour PCIA frequency, and postoperative length of stay for total hip arthroplasty, compared to PENG + LFC block.
Due to the complex nerve innervation of the hip surgery, the emphasis on regional block techniques to provide adequate analgesia in THA has been increased.29 The PENG block inhibits sensory innervation to the anterior hip capsule of the hip joint, primarily targeting the articular branches of the femoral, obturator, and accessory obturator nerves.12 Histologically, the anterior hip capsule consists mainly of nociceptive fibers and deposition of local anesthetic in anterior hip can produce analgesic effects without causing motor block. The rationale for combining LFC with PENG block is that the PENG block only targets the articular branches innervating anterior hip capsule without providing analgesia for surgical incision in posterior-lateral approach THA. Trans-muscular quadratus lumborum block (TQLB) is a myofascial plane technique that targets between the quadratus lumborum muscle and the psoas major muscle.30 Recent cadaver studies demonstrated that the TQLB could spread to the lumbar plexus and paravertebral space.31 TQLB combined with lumbar erector spinae plane block was reported to provide reliable surgical analgesia in high-risk patients undergoing hemiarthroplasty where general or spinal anesthesia was not possible.17,32 Blocking multiple nerves was superior to blocking any single nerve in the field of joint arthroplasty for optimal outcomes.33 A recent review suggested that QLB alone may not provide significantly clinical benefits for THA and was recommended to be combined with additional motor-sparing techniques for superior analgesia.34 To facilitate better analgesia, our team developed the QLESP technique, a single-puncture approach combining TQLB and lumbar erector spinae plane block, which enhances both work efficiency and patient satisfaction.17 In this PSM study, we observed an 11.0% decrease in cumulative sufentanil consumption within the first 6-h postoperative period after total hip arthroplasty in patients who underwent QLESP block compared with those who underwent PENG + LFC block. According to the anatomy of innervation, the wider block coverage of the QLESP block versus PENG + LFC block might explain for the opioid-sparing outcome.
A recent study described the pain trajectory after THA, highlighting that acute postoperative pain peaks between 0 and 2 hours, with pain intensity gradually decreasing at 4 and 8 hours after surgery.35 Interestingly, our results showed that the cumulative sufentanil consumption and pressing frequency of PCIA at 6 hours were lower in the QLESP group compared to the PELF group. Consistent with our findings, several studies aimed to explore superior analgesic strategies after THA have reported no significant difference in oral morphine equivalent (OME) at 12 and 24 hours postoperatively.36,37 These results suggested that the QLESP block might offer a short-term analgesic advantage within the early postoperative window, which corresponds to the period of peak pain intensity after THA. However, it should be noted that the observed reductions in opioid use within the first 6 hours, while statistically significant, were modest in magnitude. The clinical relevance of this early opioid-sparing effect requires further investigation. Moreover, the differences in opioid consumption did not persist beyond the early postoperative period, and no significant long-term benefits in pain scores or functional outcomes were demonstrated between the two groups. Future studies with larger sample sizes and longer follow-up are needed to determine whether this short-term analgesic advantage translates into meaningful improvements in recovery quality, patient satisfaction, or long-term functional outcomes. Our study also noted a significantly decreased postoperative hospital length of stay in the QLESP group compared to the PELF group. Similarly, a retrospective study of 210 patients found trans-muscular QLB combined with LFC block significantly decrease hospital of stay in total hip arthroplasty.38 Conversely, a recent randomized controlled study of 101 patients undergoing total hip arthroplasty randomized to the lateral QLB (n = 51) and PENG + LFC (n = 50), length of hospital stay did not differ between groups.19 Our study differentiated between preoperative and postoperative hospital stay instead of total hospital stay in prior publications. Length of hospital stay for primary hip arthroplasty is multifactorial and could be reduced by implementation of enhanced recovery program encompassing each stage.39
No significant difference was found between the QLESP group and PELF group. This observation is consistent with a prospective study of 89 patients receiving a PENG (n = 30), QLB (n = 30), or intra-articular local anesthetic injection (n = 29), the NRS scores over the first 48 h postoperatively were similar between the PENG and QLB groups.22 Another recent study demonstrated that lateral QLB only decreased VAS pain scores with movement compared with PENG + LFC block, yet no significant differences in VAS pain scores at rest was found between groups.19 Our study reported that the QLESP and PELF group did not differ in VAS scores. Due to the retrospective design, it was regrettable that specific details of VAS scores at resting versus movement were not recorded in this study. A further aspect is that the block techniques and approach in this study are not fully identical to the earlier studies, which might account for the lack of clinically significant differences on pain scores.
In clinical practice, QLESP technique could be performed in a single-puncture approach which allows subsequent quadratus lumborum blocks after redirection of the needle. This could be time-consuming and avoid the discomfort of multi-site puncture in patients. Compared to the QLESP block, the advantages of PELF block is allowing patients in supine position and useful for patients who are unsuitable for the lateral position. In the future study, the performance time, and the learning curve for capturing sonograms and identifying significant anatomical structures of the QLESP and PELF block are needed to be investigated.
This study has several limitations. Firstly, this was a retrospective design study. Although propensity score matching analysis was conducted to mitigate the confounding bias and minimize baseline differences between the two groups, some biases still could not be avoided. Secondly, we did not assess the sensory dermatomal levels with the pinprick test. It would be better to assess the area of the sensory blockade and establish the distribution and regression patterns of dermatomal anesthesia after the two blocks. Due to the retrospective design, differentiation of VAS scores between rest and movement was lacking. We will optimize the pain assessment in future studies. Thirdly, our study only recorded the time to first walk without assessing the lower limb muscle strength at several time points due to lack of clinical data. Well-designed randomized clinical trials are required in future work to evaluate the quadriceps muscle strength at multiple time points postoperatively. Furthermore, we used a total of 30 mL of 0.4% ropivacaine separately for QLESP and PELF block. The optimal concentration and volume of local anesthetics for performing ultrasound-guided QLESP and PELF blocks with effective postoperative pain relief and better functional recovery in total hip arthroplasty remain unknown.40
Conclusion
This retrospective observational study suggested that QLESP block was associated with a modest reduction in opioid consumption, PCIA frequency at 6 hours postoperatively, and postoperative length of stay for total hip arthroplasty, compared to PENG + LFC block. Despite statistically significant, the minor reductions and limited clinical improvement might not provide compelling evidence to warrant the routine use of QLESP to enhanced recovery protocols for total hip arthroplasty. Large multi-center prospective randomized control trials are warranted to validate these results in future studies.
Funding
This work was supported by the grants from the B. Braun Anesthesia Scientific Research Foundation (Funding Number: bnmr-2021-003).
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Shan L, Shan B, Graham D, et al. Total hip replacement: a systematic review and meta-analysis on mid-term quality of life. Osteoarthritis Cartilage. 2014;22(3):389–10. doi:10.1016/j.joca.2013.12.006
2. Guerra ML, Singh PJ, Taylor NF. Early mobilization of patients who have had a hip or knee joint replacement reduces length of stay in hospital: a systematic review. Clin rehabilitat. 2015;29(9):844–854. doi:10.1177/0269215514558641
3. Robin F, Newman N, Garneau S, et al. PROSPECT guidelines for total hip arthroplasty: a systematic review and procedure-specific postoperative pain management recommendations. Anaesthesia. 2021;76(10):1424. doi:10.1111/anae.15541
4. Fillingham YA, Hannon CP, Kopp SL, et al. The efficacy and safety of regional nerve blocks in total hip arthroplasty: systematic review and direct meta-analysis. J Arthroplasty. 2022;37(10):1922–1927.e1922. doi:10.1016/j.arth.2022.04.035
5. Memtsoudis SG, Cozowicz C, Bekeris J, et al. Peripheral nerve block anesthesia/analgesia for patients undergoing primary hip and knee arthroplasty: recommendations from the International Consensus on Anesthesia-Related Outcomes after Surgery (ICAROS) group based on a systematic review and meta-analysis of current literature. Reg Anesth Pain Med. 2021;46(11):971–985. doi:10.1136/rapm-2021-102750
6. Behrends M, Yap EN, Zhang AL, et al. Preoperative fascia iliaca block does not improve analgesia after arthroscopic hip surgery, but causes quadriceps muscles weakness: a randomized, double-blind trial. Anesthesiology. 2018;129(3):536–543. doi:10.1097/aln.0000000000002321
7. Eshag MME, Hasan LOM, Elshenawy S, et al. Fascia iliaca compartment block for postoperative pain after total Hip arthroplasty: a systematic review and meta-analysis of randomized controlled trials. BMC Anesthesiol. 2024;24(1):95. doi:10.1186/s12871-024-02476-y
8. Ripollés-Melchor J, Abad-Motos A, Díez-Remesal Y, et al. Association between use of enhanced recovery after surgery protocol and postoperative complications in total hip and knee arthroplasty in the postoperative outcomes within enhanced recovery after surgery protocol in elective total hip and knee arthroplasty study (POWER2). JAMA Surg. 2020;155(4):e196024. doi:10.1001/jamasurg.2019.6024
9. Aliste J, Layera S, Bravo D, et al. Randomized comparison between pericapsular nerve group (PENG) block and suprainguinal fascia iliaca block for total hip arthroplasty. Reg Anesth Pain Med. 2021;46(10):874–878. doi:10.1136/rapm-2021-102997
10. Girón-Arango L, Peng PWH, Chin KJ, et al. Pericapsular Nerve Group (PENG) block for hip fracture. Reg Anesth Pain Med. 2018;43(8):859–863. doi:10.1097/aap.0000000000000847
11. Del Buono R, Padua E, Pascarella G, et al. Pericapsular nerve group block: an overview. Minerva Anestesiol. 2021;87(4):458–466. doi:10.23736/s0375-9393.20.14798-9
12. Girón-Arango L, Peng P. Pericapsular nerve group (PENG) block: what have we learned in the last 5 years? Reg Anesth Pain Med. 2025;50(5):402–409. doi:10.1136/rapm-2024-105427
13. Girombelli A, Vetrone F, Saglietti F, et al. Pericapsular nerve group block and lateral femoral cutaneous nerve block versus fascia iliaca block for multimodal analgesia after total Hip replacement surgery: a retrospective analysis. Saudi J Anaesth. 2024;18(2):218–223. doi:10.4103/sja.sja_881_23
14. Liang L, Zhang C, Dai W, et al. Comparison between pericapsular nerve group (PENG) block with lateral femoral cutaneous nerve block and supra-inguinal fascia iliaca compartment block (S-FICB) for total hip arthroplasty: a randomized controlled trial. J Anesth. 2023;37(4):503–510. doi:10.1007/s00540-023-03192-6
15. Vetrone F, Saglietti F, Galimberti A, et al. Pericapsular Nerve Group Block Plus Lateral Femoral Cutaneous Nerve Block vs. Fascia iliaca compartment block in hip replacement surgery. J Clin Med. 2025;14(3). doi:10.3390/jcm14030984
16. Kim DH, Hong G, Lin E, et al. Combined pericapsular nerve group block and intrapelvic lateral femoral cutaneous nerve block is associated with decreased opioid consumption after hip arthroscopy: a retrospective cohort study. HSS j. 2024;20(4):530–538. doi:10.1177/15563316231201335
17. Wu X, Yang L. Quadratus Lumborum and modified Erector Spinae Plane (QLESP) block: a single-puncture technique for total hip arthroplasty. J Clin Anesth. 2020;61:109643. doi:10.1016/j.jclinane.2019.109643
18. An N, Yang K, Wang Q, et al. Ultrasound-guided QLESP block: a promising technique for postoperative analgesia in pediatric patients undergoing hip surgery. J Clin Anesth. 2023;90:111234. doi:10.1016/j.jclinane.2023.111234
19. Hay E, Kelly T, Wolf BJ, et al. Comparison of pericapsular nerve group and lateral quadratus lumborum blocks on cumulative opioid consumption after primary total hip arthroplasty: a randomized controlled trial. Reg Anesth Pain Med. 2024. doi:10.1136/rapm-2024-105875
20. Johnson ELH, Kelly TL, Wolf BJ, et al. Comparison of pericapsular nerve group and lateral quadratus lumborum blocks for analgesia after primary total hip arthroplasty: a randomized controlled trial. medRxiv. 2024. doi:10.1101/2024.07.18.24310628
21. Elshall A, Asaad O, Abdelhamid BM, et al. Comparison between the ultrasound guided pericapsular nerve group block and anterior quadratus lumborum block in elderly patients undergoing total hip replacement surgeries: a randomized controlled clinical trial. Minerva Anestesiol. 2025;91(11):1020–1031. doi:10.23736/s0375-9393.25.18883-4
22. Et T, Korkusuz M. Comparison of the pericapsular nerve group block with the intra-articular and quadratus lumborum blocks in primary total hip arthroplasty: a randomized controlled trial. Korean J Anesthesiol. 2023;76(6):575–585. doi:10.4097/kja.23064
23. Wang QR, Ma T, Hu J, et al. Comparison between ultrasound-guided pericapsular nerve group block and anterior quadratus lumborum block for total Hip arthroplasty: a double-blind, randomized controlled trial. Eur Rev Med Pharmacol Sci. 2023;27(16):7523–7532. doi:10.26355/eurrev_202308_33404
24. Kelly T, Wolla CD, Wolf BJ, et al. Comparison of lateral quadratus lumborum and lumbar plexus blocks for postoperative analgesia following total hip arthroplasty: a randomized clinical trial. Reg Anesth Pain Med. 2022;47(9):541–546. doi:10.1136/rapm-2022-103598
25. Nielsen TD, Moriggl B, Barckman J, et al. The lateral femoral cutaneous nerve: description of the sensory territory and a novel ultrasound-guided nerve block technique. Reg Anesth Pain Med. 2018;43(4):357–366. doi:10.1097/aap.0000000000000737
26. Wainwright TW, Gill M, McDonald DA, et al. Consensus statement for perioperative care in total hip replacement and total knee replacement surgery: Enhanced Recovery After Surgery (ERAS(®)) Society recommendations. Acta orthopaedica. 2020;91(1):3–19. doi:10.1080/17453674.2019.1683790
27. Ljungqvist O, Scott M, Fearon KC. Enhanced recovery after surgery: a review. JAMA surg. 2017;152(3):292–298. doi:10.1001/jamasurg.2016.4952
28. Stowers MD, Manuopangai L, Hill AG, et al. Enhanced recovery after surgery in elective hip and knee arthroplasty reduces length of hospital stay. ANZ J Surg. 2016;86(6):475–479. doi:10.1111/ans.13538
29. de Souza DN, Lorentz NA, Charalambous L, et al. Comprehensive pain management in total joint arthroplasty: a review of contemporary approaches. J Clin Med. 2024;13(22). doi:10.3390/jcm13226819
30. Dam M, Hansen CK, Borglum J, et al. A transverse oblique approach to the transmuscular quadratus lumborum block. Anaesthesia. 2016;71(5):603–604. doi:10.1111/anae.13453
31. Gong F, Li Y, Wen J, et al. The analgesic efficacy of ultrasound-guided quadratus lumborum block transmuscular or posterior approach after hip surgery: a systematic review and meta-analysis with trial sequential analysis. Clin J Pain. 2022;38(9):582–592. doi:10.1097/AJP.0000000000001059
32. Tulgar S, Ermis MN, Ozer Z. Combination of lumbar erector spinae plane block and transmuscular quadratus lumborum block for surgical anaesthesia in hemiarthroplasty for femoral neck fracture. Ind J Anaesthesia. 2018;62(10):802–805. doi:10.4103/ija.IJA_230_18
33. Terkawi AS, Mavridis D, Sessler DI, et al. Pain management modalities after total knee arthroplasty: a network meta-analysis of 170 randomized controlled trials. Anesthesiology. 2017;126(5):923–937. doi:10.1097/aln.0000000000001607
34. Grinman L, Elmore B, Ardon AE, et al. Use of peripheral nerve blocks for total hip arthroplasty. Current Pain Headache Rep. 2024;28(11):1113–1121. doi:10.1007/s11916-024-01287-7
35. Panzenbeck P, von Keudell A, Joshi GP, et al. Procedure-specific acute pain trajectory after elective total hip arthroplasty: systematic review and data synthesis. Br J Anaesth. 2021;127(1):110–132. doi:10.1016/j.bja.2021.02.036
36. Ye S, Wang L, Wang Q, et al. Comparison between ultrasound-guided pericapsular nerve group block and local infiltration analgesia for postoperative analgesia after total hip arthroplasty: a prospective randomized controlled trial. Orthopaed Surg. 2023;15(7):1839–1846. doi:10.1111/os.13777
37. She C, Liu H. The efficacy of pericapsular nerve group block for reducing pain and opioid consumption after total hip arthroplasty: a systematic review and meta-analysis. J Orthopaedic Surg Res. 2024;19(1):229. doi:10.1186/s13018-024-04707-x
38. Li J, Dai F, Ona Ayala KE, et al. Transmuscular quadratus lumborum and lateral femoral cutaneous nerve block in total hip arthroplasty. Clin J Pain. 2021;37(5):366–371. doi:10.1097/AJP.0000000000000923
39. Chung MMT, Ng JKF, Ng FY, et al. Effects of enhanced recovery after surgery practices on postoperative recovery and length of stay after unilateral primary total hip or knee arthroplasty in a private hospital. Hong Kong med j. 2021;27(6):437–443. doi:10.12809/hkmj208587
40. Huang Y, Lu Y, Wang J, et al. Effect of pericapsular nerve group block with different concentrations and volumes of ropivacaine on functional recovery in total hip arthroplasty: a randomized, observer-masked, controlled trial. J Pain Res. 2024;17:677–685. doi:10.2147/jpr.S445000
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Efficacy and Safety of Erector Spinae Plane Block for Perioperative Pain Management in Lumbar Spinal Surgery: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
Fu MY, Hao J, Ye LH, Jiang W, Lv YW, Shen JL, Fu T
Journal of Pain Research 2023, 16:1453-1475
Published Date: 3 May 2023
Regional Analgesia for Cesarean Delivery: A Narrative Review Toward Enhancing Outcomes in Parturients
Silverman M, Zwolinski N, Wang E, Lockwood N, Ancuta M, Jin E, Li J
Journal of Pain Research 2023, 16:3807-3835
Published Date: 10 November 2023
Erector Spinae Plane versus Pectoralis Nerve Block for Mastectomy in Cancer Patients: A Retrospective, Multicenter Cohort Study
Yap EN, Wei J, Darling C, Linehan E, Behrends M, Ng KP
Journal of Pain Research 2025, 18:4775-4785
Published Date: 16 September 2025
The Effect of Cocktail Formula Solution for Erector Spinae Plane Block on Postoperative Pain After Laparoscopic Major Upper Abdominal Surgery: A Single-Center Randomized Controlled Study
Lu D, Chen H, Hu J, He X, Bao L, Xu B, Zhang S, Fan J, Wang R
Journal of Pain Research 2026, 19:566625
Published Date: 24 January 2026
Modified Single-Side-Lying Quadratus Lumborum Block Combined with Liposomal Bupivacaine versus Transversus Abdominis Plane Block for Post-Cesarean Analgesia: A Randomized Controlled Trial
Rao J, Xiao J, Li B, Zong Y, Song J, Hu S, Luo A, Zeng L, Zhou Q
Drug Design, Development and Therapy 2026, 20:580472
Published Date: 8 June 2026