Back to Journals » Journal of Pain Research » Volume 19
The Effect of Cocktail Formula Solution for Erector Spinae Plane Block on Postoperative Pain After Laparoscopic Major Upper Abdominal Surgery: A Single-Center Randomized Controlled Study
Authors Lu D, Chen H, Hu J, He X, Bao L, Xu B, Zhang S, Fan J, Wang R
Received 10 September 2025
Accepted for publication 14 January 2026
Published 24 January 2026 Volume 2026:19 566625
DOI https://doi.org/10.2147/JPR.S566625
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jinlei Li
Dan Lu,1 Hongzhou Chen,1 Jian Hu,2 Xuemei He,1 Lei Bao,1 Bo Xu,1 Siyu Zhang,1 Jingsheng Fan,3,* Rurong Wang2,*
1Department of Anesthesiology, Chengdu Shangjin Nanfu Hospital/Shangjin Hospital, West China Hospital, Sichuan University, Chengdu, People’s Republic of China; 2Department of Anesthesiology, West China Hospital, Sichuan University, Chengdu, People’s Republic of China; 3Department of Anesthesiology, Dongnan Hospital, Chongqing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Rurong Wang, Department of Anesthesiology, West China Hospital, Sichuan University, No. 37 Guoxue Alley, Chengdu, 610000, People’s Republic of China, Tel +86-18980601563, Email [email protected] Jingsheng Fan, Department of Anesthesiology, Dongnan Hospital, 98 Tongjiang Avenue, Nanan District, Chongqing, 400000, People’s Republic of China, Tel +86-18523175475, Email [email protected]
Objective: This study aimed to evaluate the analgesic efficacy and duration of a single bilateral erector spinae plane block (ESPB) using a cocktail formula solution compared to plain ropivacaine in patients undergoing laparoscopic major upper abdominal surgery.
Patients and Methods: In this single-center, randomized, double-blind controlled trial, 60 patients scheduled for laparoscopic major upper abdominal surgery were randomized into two groups. The experimental group received ultrasound-guided bilateral ESPB with 40 mL of a cocktail solution (0.375% ropivacaine + 2μg/mL epinephrine + 0.1mg/mL dexamethasone + 2.5mg/mL magnesium sulfate + 15mg/mL sodium bicarbonate). The control group received bilateral ESPB with 40 mL of 0.375% ropivacaine alone. Both groups received postoperative patient-controlled intravenous analgesia (PCIA). The primary outcome was total intravenous morphine equivalent analgesic consumption (including PCIA and rescue analgesia) at 0– 48h and 24– 48h postoperatively. Secondary outcomes included modified NRS pain scores, Ramsay sedation scores, patient satisfaction scores, time to first ambulation, time to first flatus, hospital discharge time, and incidence of complications.
Results: Fifty-seven patients were included in the final analysis. The total morphine equivalent consumption at 0– 48h and 24– 48h was significantly lower in the experimental group (30.12 mg and 13.14 mg, respectively) compared to the control group (38.62 mg and 16.72 mg, respectively) (p ≤ 0.05). The experimental group also had significantly lower modified NRS pain scores at 1, 3, 6, 12, 24, 36, and 48 hours postoperatively and higher patient satisfaction scores (p ≤ 0.05). There were no significant differences in sedation scores, complication rates, or recovery indices between the groups.
Conclusion: A single ESPB with the cocktail formula solution significantly prolongs analgesia for up to 48 hours and provides superior analgesic efficacy compared to plain ropivacaine in patients undergoing laparoscopic major upper abdominal surgery, without increasing complications.
Keywords: erector spinae plane block, cocktail formula solution, major upper abdominal surgery, postoperative analgesia, randomized controlled trial
Introduction
Postoperative analgesia is a key component of perioperative management; however, the incidence of moderate-to-severe pain remains high, particularly following upper abdominal surgeries that are extensive and of long duration.1,2 Currently, a variety of analgesic modalities are available after upper abdominal surgery, including patient-controlled intravenous analgesia (PCIA),3–7 continuous epidural analgesia (PCEA),5,8–11 continuous peripheral nerve block (PCNB),3,9–12 and multimodal strategies. Although PCIA is effective, opioid-related adverse effects are significant;4,7,12,13 PCEA provides superior analgesia but is technically complex and associated with risks such as hypotension and infection.14 Single-injection nerve blocks are simple to perform but have a limited duration of action,14,15 whereas continuous nerve blocks provide sustained analgesia but may be complicated by catheter displacement and other issues.11,14
The erector spinae plane block (ESPB), a relatively new peripheral nerve block technique, involves ultrasound-guided injection of local anesthetic into the fascial plane to block the corresponding segmental nerves, thereby providing both somatic and visceral analgesia.16 ESPB is suitable for major upper abdominal surgeries, such as those involving the liver and pancreas, and is particularly safe for patients receiving anticoagulation therapy. Studies have shown that continuous ESPB provides analgesia that is superior or comparable to conventional methods and can extend up to 72 hours.17 Nevertheless, its widespread adoption remains limited by the duration of the local anesthetic and catheter management.18
To prolong the duration of single-injection nerve blocks, researchers have investigated novel drugs and combination formulations. Liposomal bupivacaine allows for the slow release of local anesthetic for up to 72 hours, but its clinical use is currently limited.19,20 Alternatively, adjuvant mixtures—such as ropivacaine in combination with epinephrine and dexamethasone—can significantly extend the duration of analgesia.21–23 Some studies have indicated that the “cocktail” formulation, which includes ropivacaine, epinephrine, dexamethasone, magnesium sulfate, and sodium bicarbonate, can effectively prolong analgesia and reduce opioid consumption in joint surgery.24 This compound solution contains magnesium sulfate and sodium bicarbonate, which further enhance ropivacaine’s nerve-blocking effect, and studies have confirmed the safety of this drug combination.24–29
Therefore, this study aims to employ this cocktail formulation as a single-injection ESPB for patients undergoing major laparoscopic upper abdominal surgery, in order to evaluate its efficacy in prolonging analgesia, reducing opioid usage, and improving the quality of postoperative recovery.
Patients and Methods
Study Design and Ethics
A single-center, randomized, double-blind, controlled trial design was employed. This study was approved by the Biomedical Ethics Committee of Chengdu Shangjin Nanfu Hospital, Approval No.: 2024 Year Review (43) No. It was registered in July 2024 at the China Clinical Trial Registration Center, Registration No. ChiCTR2400086457, and documented in the Medical Research Registration System in August 2024. Clinical research was conducted from August 2024 to March 2025. Sixty patients were randomly assigned to the control group and the experimental group in a 1:1 ratio using computer-generated random sequences, and all allocation information was concealed using sealed envelopes. The study complied with the Declaration of Helsinki throughout.
Participants
All study cases were sourced from the Anesthesiology Surgical Center of Chengdu Shangjin Nanfu Hospital.
Inclusion Criteria
- Patients undergoing elective major laparoscopic abdominal surgery (such as liver cancer, gallbladder cancer, and pancreatic cancer);
- Preoperative ASA (American Society of Anesthesiologists) classification of I–III;
- Patients aged 18–75 years;
- Patients who agreed to participate in the study and signed informed consent.
Exclusion Criteria
- History of allergy to the study drugs;
- Morphine addiction or neuromuscular disease;
- Infection at the puncture site;
- Patients unable to communicate verbally.
Withdrawal Criteria
- Patients unable to complete the trial and follow-up for various reasons;
- Patients whose surgery needs to be terminated intraoperatively due to clinical reasons, require a change in surgical method, or undergo a secondary surgery;
- The occurrence of unanticipated complications such as nerve damage or postoperative massive bleeding. Neuromuscular disease, infection at the puncture site, or inability to communicate.
Intervention
Patients were randomized to:
Control Group: 0.375% Ropivacaine, total 40mL.
Experimental Group: 0.375% Ropivacaine + adrenaline 2μg/mL + dexamethasone 0.1mg/mL + magnesium sulfate 2.5mg/mL + sodium bicarbonate 15mg/mL, total 40mL.
An independent researcher prepared the corresponding study drugs according to the enrollment number, which were provided to the block operator in a confidential manner. The researcher no longer participated in the study process prior to unblinding.
Both groups underwent bilateral erector spinae plane block (ESPB) at the T8-T9 level under ultrasound guidance after surgery completion, with 20mL of drug injected at each site.
Standardized Anesthesia Protocol
After entering the operating room, patients were subjected to the unified anesthesia and surgical protocol of our hospital. Non-invasive blood pressure, finger pulse oximetry, and ECG monitoring were conducted. Anesthesia induction was achieved with: Midazolam 0.02–0.04mg/kg or Remimazolam 0.1–0.3mg/kg, Sufentanil 0.3–0.5μg/kg, Propofol 1–2mg/kg, Cisatracurium 0.2–0.3mg/kg, or Vecuronium 0.08–0.12mg/kg. Invasive blood pressure monitoring was established after induction. Maintenance of anesthesia was performed using: Sevoflurane 1–3% and/or Propofol 4–6mg/(kg.h), Remifentanil 0.1–0.2μg/(kg.min), intermittent bolus of Cisatracurium or Vecuronium to maintain muscle relaxation. The dosage of maintenance anesthetic drugs was adjusted according to the patient’s condition during surgery.
Twenty minutes before the end of the surgery, intravenous Sufentanil 5μg was administered to control postoperative pain. At the end of the surgery, an intravenous analgesia pump was connected, with the analgesic pump formulation: Hydromorphone Hydrochloride 10mg + Granisetron 12mg + Normal Saline 155mL, analgesia pump parameters set to: background dose 1.2mL/h, bolus dose 1.5mL, lockout time 15 minutes.
Erector Spinae Plane Block Procedure
After the procedure and extubation, an experienced nerve block physician performed the erector spinae plane block under ultrasound guidance using a CCZA-type 22G x 100 mm puncture needle (Suzhou Leap Medical) and a Mindray M9 portable color Doppler ultrasound diagnostic system (UMT-500, Shenzhen Mindray Medical). The block was performed at bilateral T8–T9 levels using either an in-plane or out-of-plane approach. After the needle tip reached the designated position, the control group received an injection of 0.375% Ropivacaine 20mL on each side, totaling 40mL bilaterally. The experimental group received an injection of a cocktail consisting of 0.375% Ropivacaine + adrenaline 2μg/mL + dexamethasone 0.1mg/mL + magnesium sulfate 2.5mg/mL + sodium bicarbonate 15mg/mL, with 20mL injected on each side, totaling 40mL bilaterally. Ultrasound images were taken after drug injection for traceability and subsequent result analysis. The success criterion for the erector spinae plane block was the visualization of drug-induced expansion of the erector spinae plane space under ultrasound. The ultrasound images after drug injection into the erector spinae plane are shown in Figure 1.
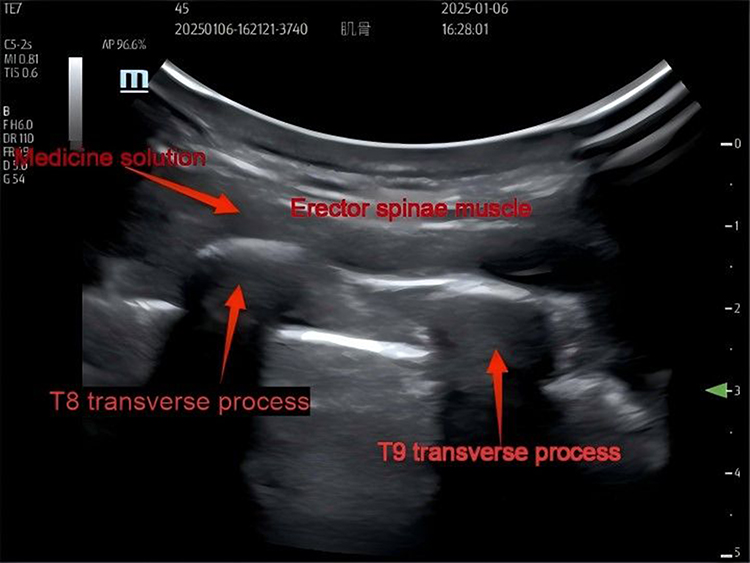 |
Figure 1 Ultrasound image of drug injection into the erector spinae plane. |
Observation Indicators
Primary Indicators
Total intravenous analgesic drug morphine equivalent dosage (including PCIA morphine equivalent dosage and supplementation analgesic morphine equivalent dosage) at postoperative intervals of 0–24h, 0–48h, 0–72h, 24–48h, and 48–72h.
Secondary Outcomes
Modified NRS pain scores, Ramsay sedation scores, patient satisfaction scores, and cumulative analgesia pump usage at 0.5 h, 1 h, 3 h, 6 h, 12 h, 24 h, 36 h, 48 h, and 72 h postoperatively; time to first request for rescue analgesia; time to first ambulation; time to first flatus; hospital discharge time; and the incidence of nausea and vomiting, hypotension, block-related complications, and surgical complications.
Efficacy Evaluation Standards
Pain assessment was conducted using the modified NRS scoring system, as shown in Table 1. The sedation score uses the Ramsay Sedation Scale. Satisfaction rating criteria, using a simple four-level subjective scoring system,6 include:1 point - Unsatisfied;2 points - Neutral;3 points - Satisfied;4 points - Very satisfied.
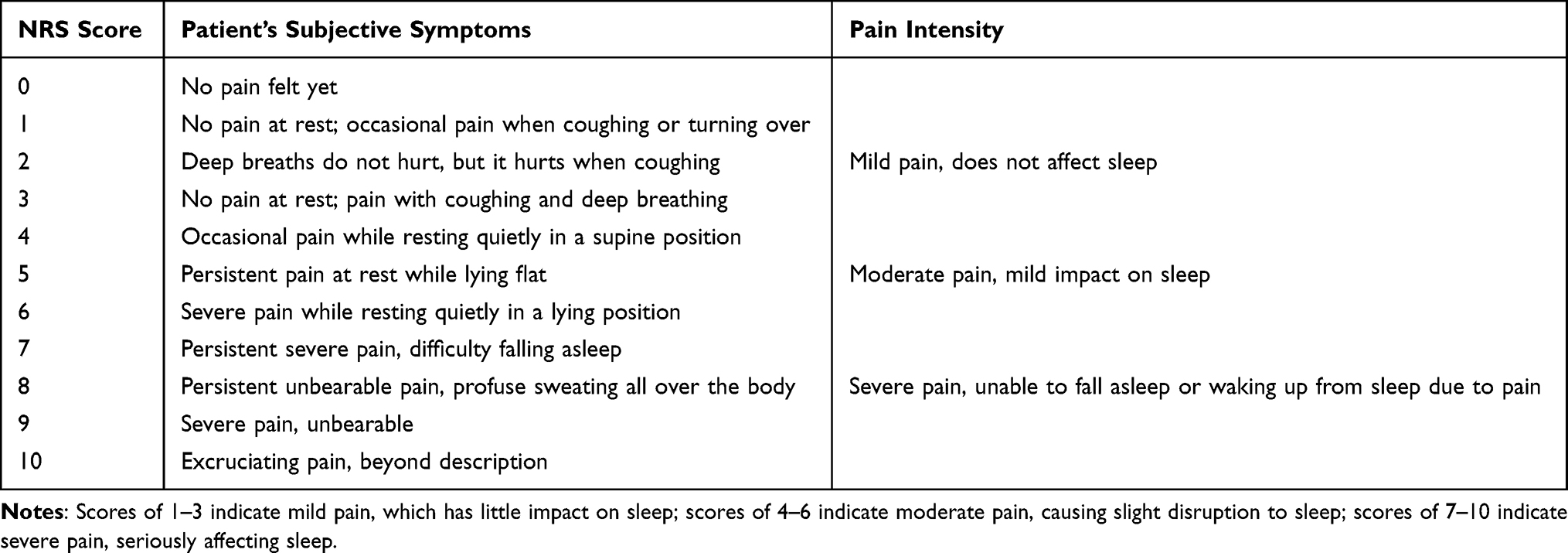 |
Table 1 Pain Modified NRS Scale |
Data Collection and Processing
Prior to the study commencement, training was provided to patients and their families on the modified NRS pain scoring, Ramsay sedation scoring, and satisfaction scoring standards, with printed copies of the scoring standards distributed. The study began at the time of erector spinae plane block, combining all observation points. The scoring registration form indicated the time points for scoring. This form was given to the patients and their families, who completed the pain scores, sedation scores, and satisfaction scores at each time point on the registration form, with bedside and telephone follow-up ensuring completion of scoring.
Research personnel recorded the amount of analgesic pump drug use and number of presses at each time point, total amount of supplemental analgesic drugs, timing of the first demand for supplemental analgesia, occurrences of nausea and vomiting, hypotension, block-related complications, and surgical complications, as well as the timing of the first out-of-bed time and time to first passage of gas, and discharge time. The amounts of analgesic pump drugs and supplemental analgesic drugs were converted into morphine equivalent dosages using the conversions below:
Intravenous Oxycodone 1mg = 1.52mg intravenous morphine, Oral Oxycodone 1mg = 0.5mg intravenous morphine.
Intravenous Dazocine 1mg = 0.6mg intravenous morphine, Oral Dazocine 1mg = 0.25mg intravenous morphine.
Intravenous Tramadol 1mg = 0.1mg intravenous morphine, Intravenous Hydromorphone 1mg = 7.5mg intravenous morphine.
Intravenous Sufentanil 1μg = 0.75mg intravenous morphine.
Statistical Analysis
Based on a pilot study results, with a 4 mg MME difference at 24–48 h, SD 5 mg, α=0.05 (two-sided), power 80%, 15% dropout; a sample size of 60 was calculated. Statistical analysis was performed using SPSS. Normally distributed measurement data were presented as mean ± standard deviation, while non-normally distributed measurement data were presented as median (interquartile range). Comparing normally distributed measurement data with equal variances was performed using independent samples t-test, while for normally distributed measurement data with unequal variances, Welch’s t-test was employed. Comparisons of other measurement data between the two groups were conducted using the Mann–Whitney U-test. Categorical variables were analyzed using chi-square tests or Fisher’s exact test. A p-value ≤ 0.05 was considered to indicate statistically significant differences.
Results
A total of 60 cases were included in the study, among which 3 patients (2 from the experimental group and 1 from the control group) exited the study due to severe surgical complications including pancreatic fistula and postoperative bleeding that required a second surgery. The remaining 57 cases, including 29 from the experimental group and 28 from the control group, were included in the statistical analysis. The study flowchart is presented in Figure 2.
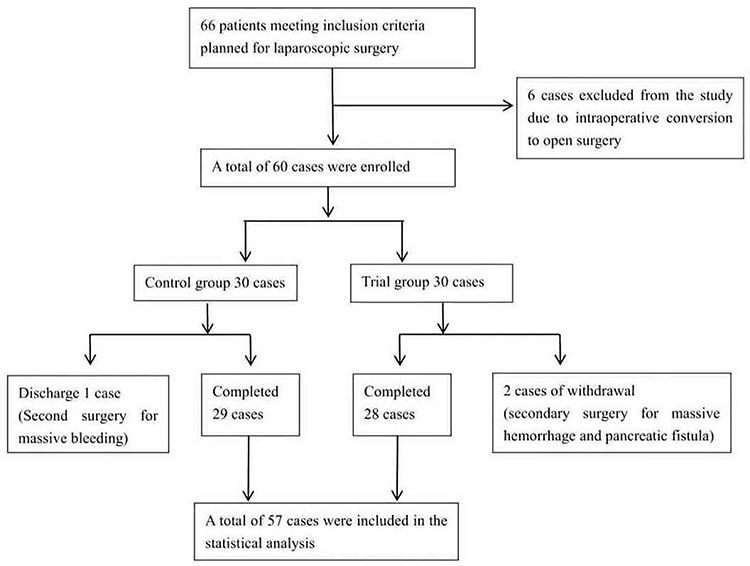 |
Figure 2 The study flowchart. |
General Information of Two Patient Groups
The general information of the two patient groups is shown in Table 2. There were no statistically significant differences in patient age, gender, height, weight, duration of surgery, anesthesia time, and intraoperative fluid volume.
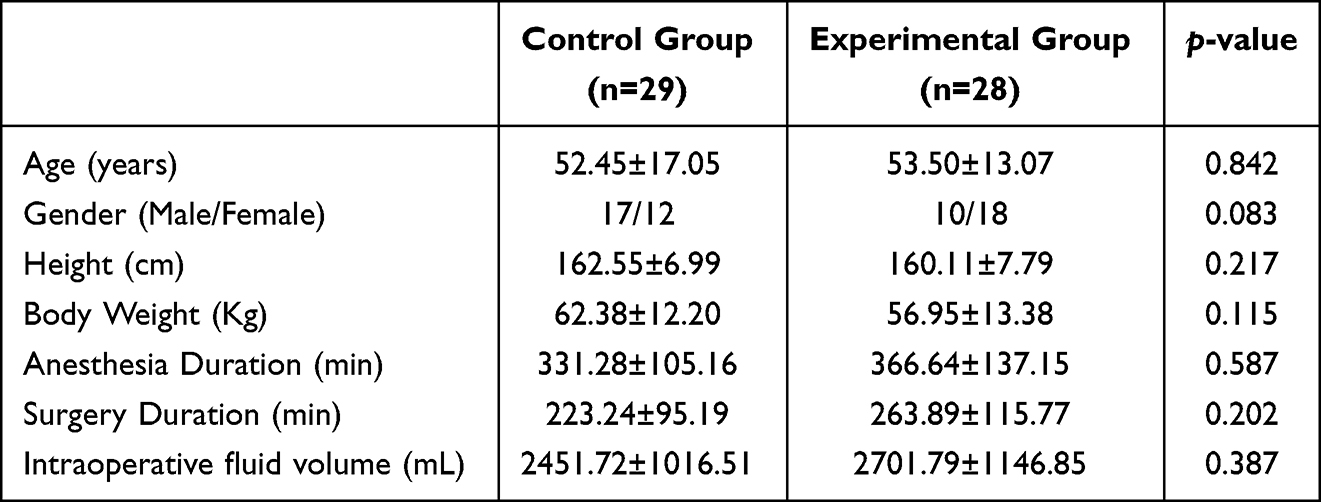 |
Table 2 General Conditions of the Two Patient Groups |
Distribution of Disease Types in Two Patient Groups
The distribution of disease types in the two patient groups is shown in Table 3. No statistically significant differences were found between the two groups (p=0.651).
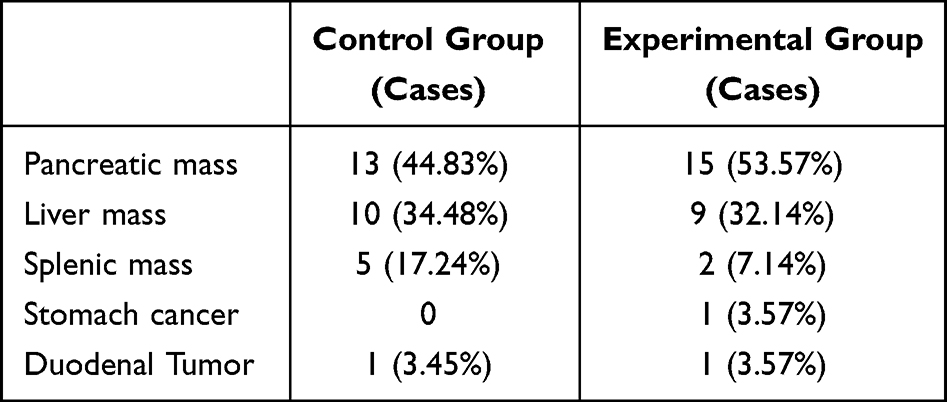 |
Table 3 Disease Distribution of Two Patient Groups (Units: Cases) |
Comparison of Total Morphine Equivalent Doses
The comparison of total analgesic morphine equivalent doses between the two groups of patients at different time points is shown in Table 4 and Figure 3. In the 0–48h and 24–48h periods, the total analgesic morphine equivalent doses in the experimental group were significantly lower than those in the control group, with statistical significance (p≤0.05). For the 0–24h, 0–72h, and 48–72h periods, the total morphine equivalent doses in the experimental group were numerically lower than those in the control group, but no statistical difference was detected.
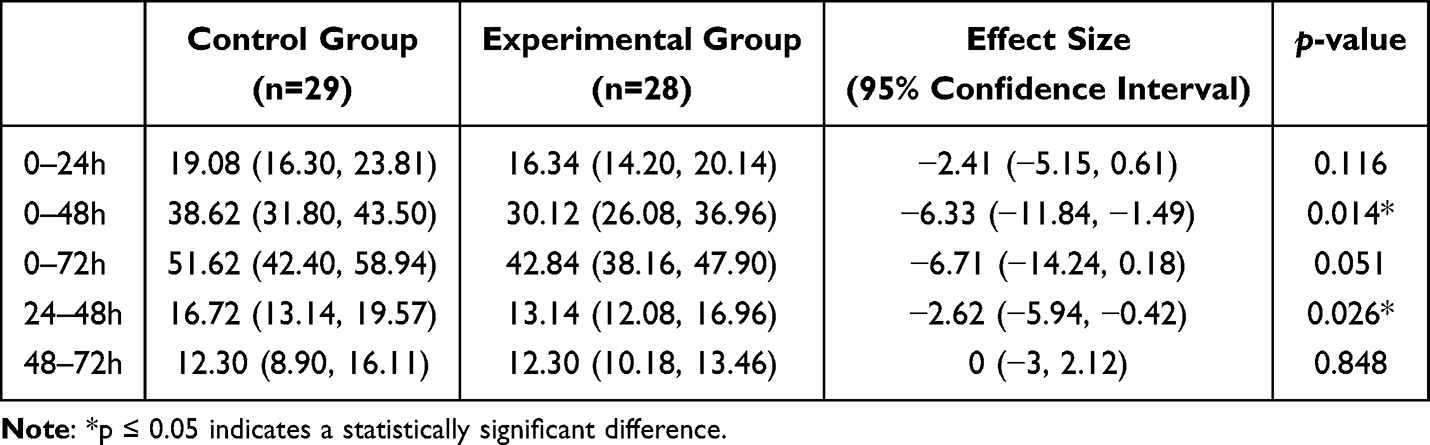 |
Table 4 Comparison of Total Analgesic Morphine Equivalent Dosage (Unit: Mg) |
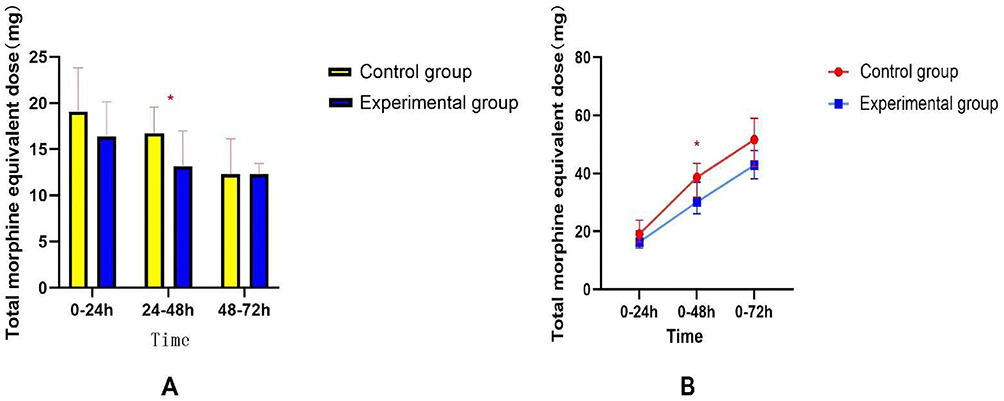 |
Figure 3 Comparison of single-day (A) and cumulative (B) total intravenous opioid morphine-equivalent doses over three days. *p ≤ 0.05, there is a statistically significant difference. |
Comparison of Equivalent Doses of Morphine in Pain Relief Pump Usage
The comparison of equivalent doses of morphine in the pain pump usage between the two groups of patients is shown in Table 5. During the time periods of 0–48 hours and 24–48 hours, the experimental group had a significantly lower equivalent dose of morphine in the pain pump compared to the control group, with statistical significance (p≤0.05). In the remaining time periods, the experimental group showed a trend of being lower than the control group, but no statistically significant differences were detected.
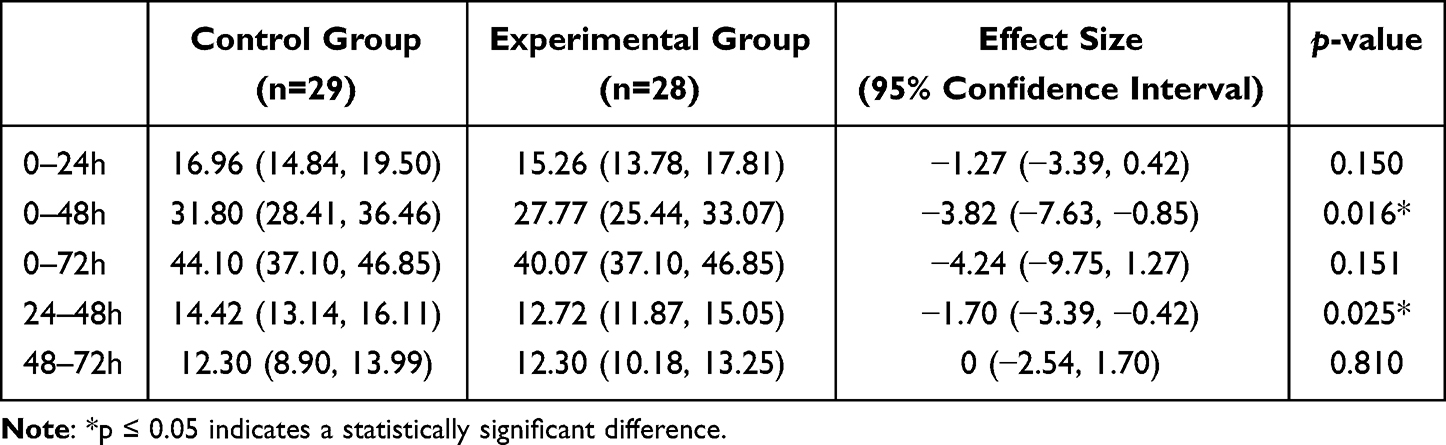 |
Table 5 Comparison of Equivalent Morphine Dosages in Analgesic Pump Use (Unit: Mg) |
Comparison of Cumulative Usage Volume of Pain Relief Pumps at Different Time Points
The cumulative usage volume of the pain relief pump at different time points for both groups of patients is shown in Figure 4. As time progressed, the difference between the two groups tended to increase, with the experimental group being significantly lower than the control group at 48 hours post-surgery, showing a statistically significant difference (p≤0.05). No statistically significant differences were found in the other time points.
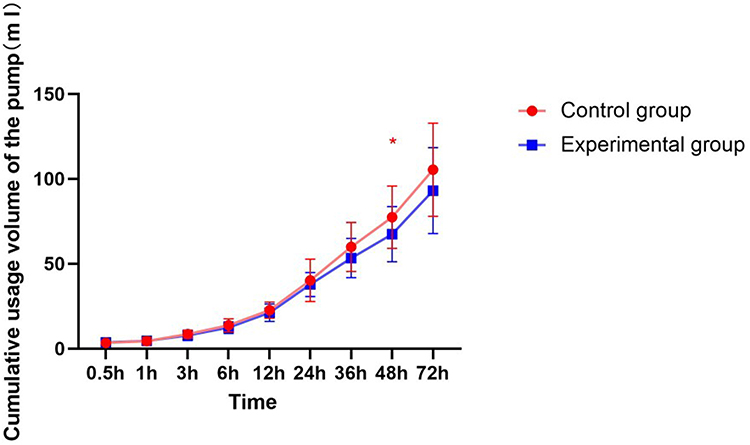 |
Figure 4 Comparison of cumulative volumes used by the analgesic pump at each time point. *p ≤ 0.05, there is a statistically significant difference. |
Usage of Rescue Analgesics
The demand for rescue analgesics in the two groups of patients is shown in Tables 6 and 7. The number of cases requiring rescue analgesia was higher in the control group, but the χ2-test did not reveal a statistically significant difference (p=0.236). There was also no statistically significant difference in the time to first rescue analgesia between the two groups (p=0.767).
 |
Table 6 Comparison of Postoperative Rescue Analgesia Requirements Between Two Patient Groups |
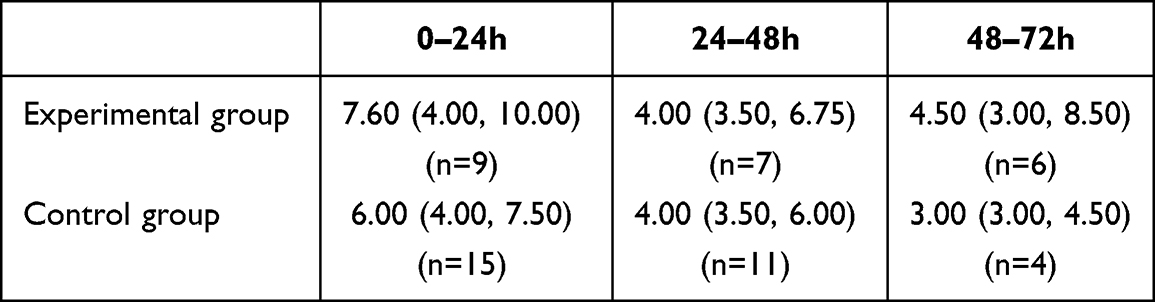 |
Table 7 Dose of Rescue Analgesic Converted to Morphine Equivalents per Day for the First Three Postoperative days in the Two Patient Groups (Unit: Mg) |
Comparison of Pain Scores
The modified NRS pain scores at each time point for the two groups of patients are shown in Table 8. The scores in the experimental group were lower than those in the control group at 1 hour, 3 hours, 6 hours, 12 hours, 24 hours, 36 hours, and 48 hours postoperatively, with a statistically significant difference (p≤0.05). No statistical difference was detected at 0.5 hours and 72 hours postoperatively.
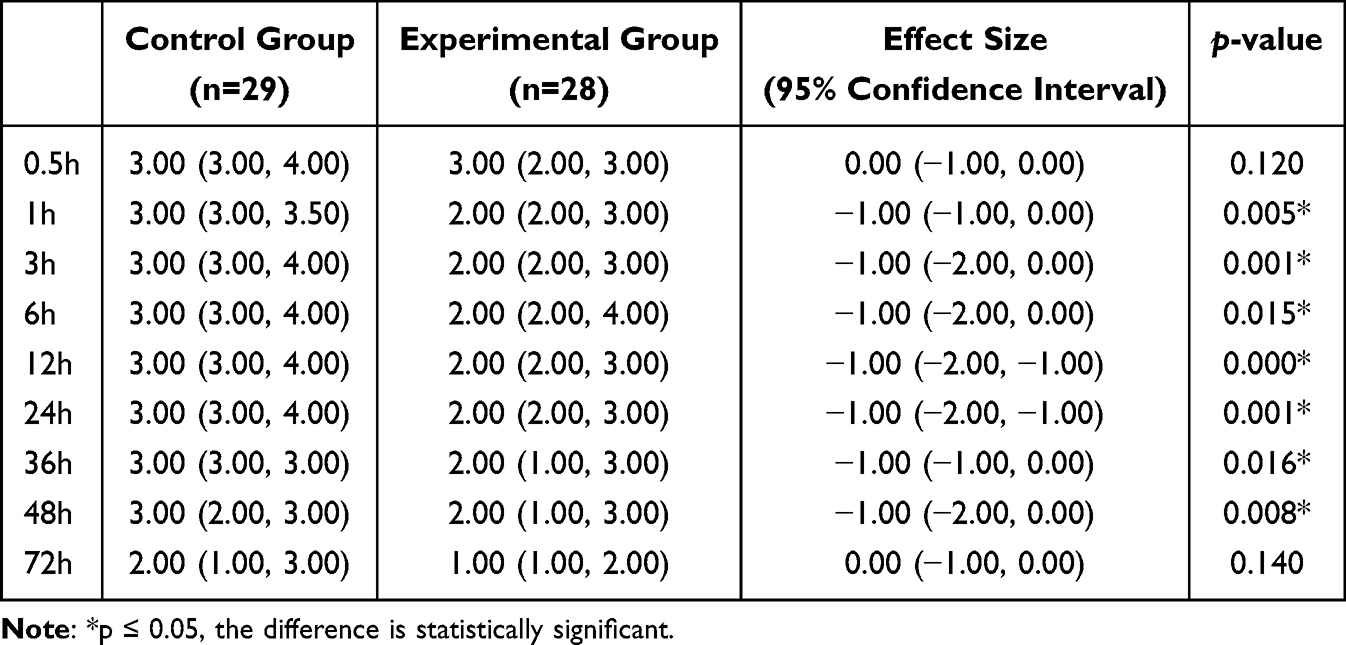 |
Table 8 Comparison of Modified NRS Pain Scores at Each Time Point Between the Two Patient Groups (Unit: Points) |
Comparison of Sedation Scores
The comparison of Ramsay sedation scores at various time points between the two groups of patients is shown in Table 9. No statistical differences were found between the experimental group and the control group.
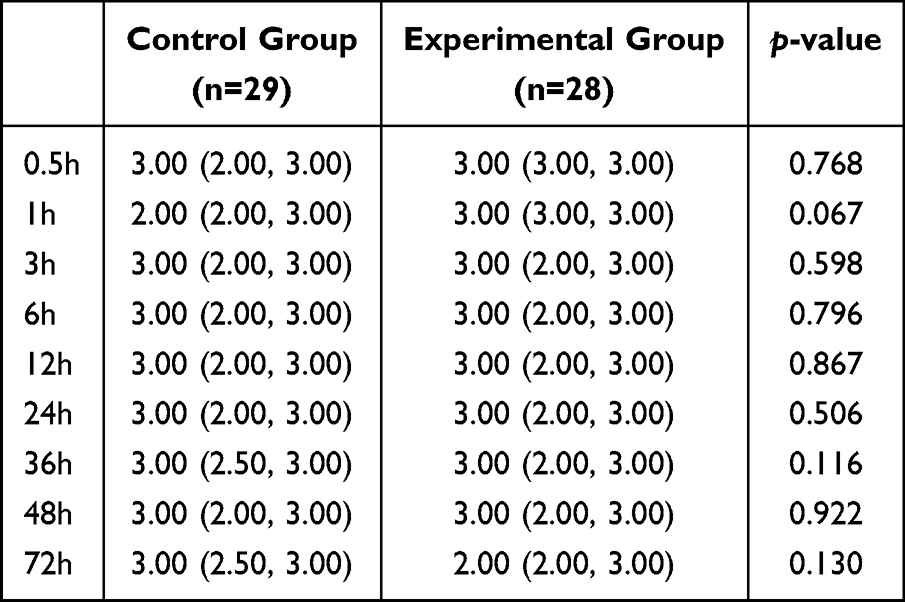 |
Table 9 Comparison of Ramsay Sedation Scores Between the Two Patient Groups at Each Time Point (Unit: Points) |
Comparison of Satisfaction Scores
The comparison of satisfaction scores using a four-point scale for the two groups of patients at different time points is shown in Table 10. The satisfaction scores for the experimental group at 1 hour, 3 hours, 6 hours, 12 hours, 24 hours, 36 hours, and 48 hours post-surgery were all higher than those of the control group, with statistically significant differences (p≤0.05). No statistical differences were observed at 0.5 hours and 72 hours post-surgery.
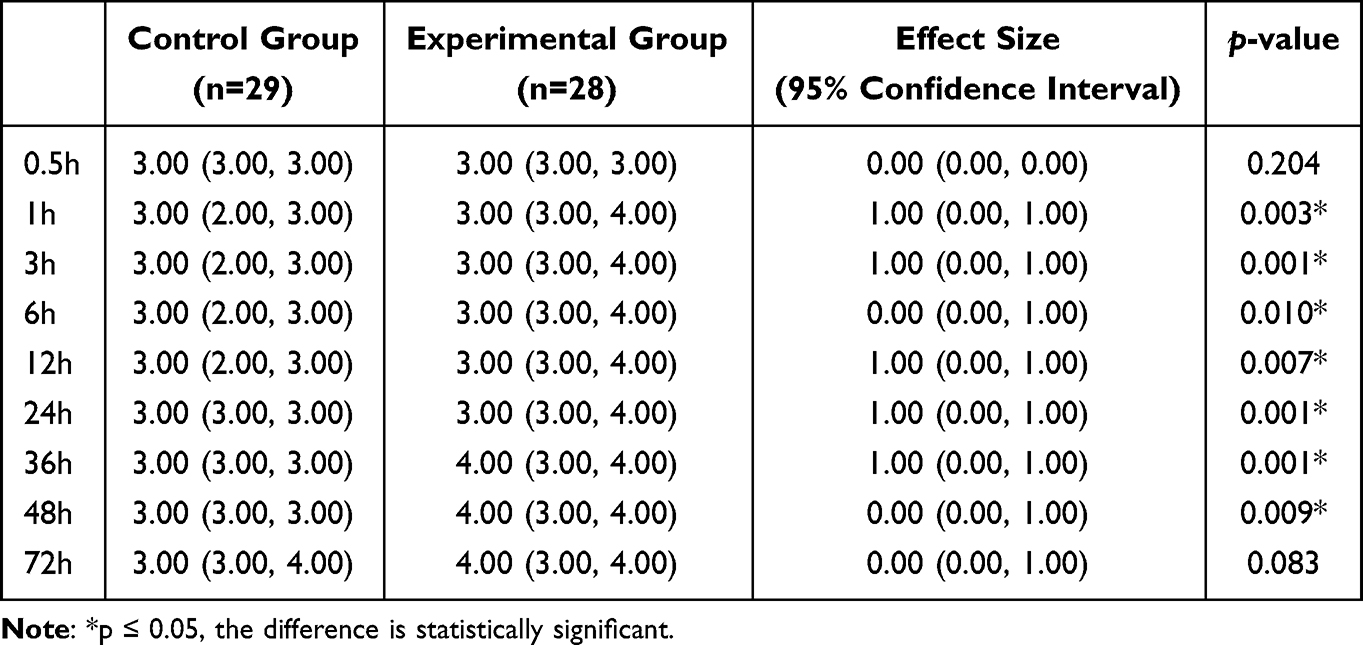 |
Table 10 Comparison of Satisfaction Scores at Each Time Point Between the Two Patient Groups (Unit: Points) |
Incidence of Complications in Two Groups
The incidence of nausea and vomiting in the two groups is shown in Table 11, with no statistically significant differences detected (p-values of 0.67 and 1.00, respectively). In the control group, 2 cases of nausea and vomiting occurred, both within 24–48 hours. In the experimental group, there were 3 cases of nausea, including 2 cases of vomiting that occurred within 0–24 hours and 1 case of nausea without vomiting that occurred within 24–48 hours. No other complications were observed in either group.
 |
Table 11 Nausea and Vomiting Occurrence (Units: Cases) |
Comparison of the First Activity Out of Bed, Time for Flatus, and Discharge Time
The details of the first activity out of bed, time for flatus, and discharge time after surgery for both groups of patients are shown in Table 12. No statistical differences were found between the groups.
 |
Table 12 Comparison of the Two Patient Groups’ Time to First Ambulation, Time to Flatus, and Length of Hospital Stay |
Discussion
The erector spinae plane block (ESPB) is an effective regional analgesic technique for postoperative abdominal surgery, confirmed by multiple clinical studies and meta-analyses,30–32 and its effects are superior to other regional analgesia techniques such as the transversus abdominis plane block.32–34 Shan et al33 performed ESPB with ropivacaine containing iodinated contrast and traced the post-block spread of the injectate. They found that the mixture of local anesthetic and contrast spread to the paravertebral space, intercostal space, and neural foramina in 96.5%, 94.2%, and 77.9% of cases, respectively. Although some studies have reported that ESPB is less effective than paravertebral block in thoracoscopic surgery,34 a prospective cohort study by Wubetu et al35 compared the efficacy of ultrasound-guided unilateral ESPB and paravertebral block in adult patients after upper abdominal surgery. The results demonstrated that VAS scores at 3, 6, 12, and 24 hours postoperatively were significantly lower in the ESPB group compared to the paravertebral block group, and opioid consumption in the first 24 hours was also significantly reduced in the ESPB group. These findings suggest that ultrasound-guided ESPB may provide superior analgesia to paravertebral block following upper abdominal surgery. Therefore, ESPB was selected as the regional nerve block technique in the present study.
The cocktail formulation group demonstrated superior analgesia compared to the ropivacaine-only group and markedly prolonged the duration of analgesic effect. At all postoperative time points assessed (1, 3, 6, 12, 24, 36, and 48 hours), modified NRS scores in the intervention group were significantly lower than those in the control group, while patient satisfaction scores were significantly higher. The total intravenous analgesic morphine equivalent dose in the experimental group was significantly lower than that in the control group for the periods of 0–48 h and 24–48 h postoperatively; this difference was also observed specifically for morphine equivalent dose administered by PCA during these periods. These results indicate that patients in the control group required more intravenous analgesics on the second postoperative day, suggesting that the cocktail formulation provided effective analgesia for at least 48 hours postoperatively. The above findings suggest that single-injection ropivacaine ESPB may only provide adequate analgesia within the first 24 hours after surgery, consistent with the known duration of ropivacaine and previous studies.14,15,18 In contrast, the cocktail group presented significantly lower modified NRS scores and significantly higher patient satisfaction scores within 24 hours postoperatively, indicating not only a stronger analgesic effect than ropivacaine alone, but also a prolonged duration of effect extending to 48 hours.
Multimodal analgesia is a fundamental strategy of perioperative pain management; thus, both groups in this study utilized PCIA. In cases where pain was not effectively relieved by PCA, with NRS scores remaining above 4, rescue analgesia was administered, which is consistent with the high intensity of postoperative pain after upper abdominal surgery. Hu et al36 reported that 0.373% ropivacaine for fascial plane block provided effective analgesia in 99% of patients undergoing hip arthroplasty, while 0.375% ropivacaine for ESPB37 yielded the best analgesic efficacy and minimal side effects in thoracoscopic surgery—hence, 0.375% ropivacaine was selected in our research. There are case reports of ESPB23 and paravertebral block38,39 being performed with 0.5–1% ropivacaine. Whether a higher concentration of ropivacaine for ESPB after major upper abdominal laparoscopic surgery can further reduce intravenous analgesic use and its associated side effects requires further investigation.
No cases of block-related bleeding, infection, or neurological complications were observed in either group. The use of ultrasound guidance enhances the precision of block placement, ensuring efficacy while minimizing complications. Kot et al,40 in a review of 125 studies on ESPB, concluded that ESPB is associated with a very low incidence of complications. Due to the significant reduction in the need for intravenous analgesics with ESPB, postoperative complications—especially nausea and vomiting—are markedly reduced.41 In our study, the incidence of postoperative nausea and vomiting was very low (two cases in the control group and three in the experimental group). Apart from ESPB, all patients received PCIA and, if necessary, additional rescue analgesia, so instances of nausea and vomiting may be attributable to intravenous opioid administration.
No statistically significant differences were detected between the two groups in terms of time to first anal exhaust, time to ambulation, or length of hospital stay. On one hand, this may be due to the use of PCIA and rescue analgesics in both groups; on the other, it may relate to our study being single-center with a potentially insufficient sample size. Whether differences between the groups exist for these indicators requires confirmation in future large-scale, multicenter studies.
The mechanism by which the cocktail formulation significantly prolongs analgesia lies in the synergistic effects of its constituent adjuvants: epinephrine slows the systemic absorption of local anesthetics, thereby extending their duration of action; dexamethasone suppresses local inflammation with anti-inflammatory and analgesic properties, enhancing and prolonging the effect of local anesthetics; magnesium sulfate, an NMDA receptor antagonist, inhibits NMDA receptor activity, blocks the influx of calcium and sodium, and suppresses neural impulse transmission; sodium bicarbonate increases the proportion of non-ionized ropivacaine, which enhances its affinity for sodium channels, more effectively blocking them and inhibiting neural transmission. Although each agent has a distinct mechanism, all contribute to enhancing and prolonging analgesic duration.24 Despite the formation of minor precipitates when mixing these adjuvants, animal studies by Yang Jing’s group confirmed no significant neurotoxicity or local tissue damage,24 and no neurological complications were observed clinically. The minor precipitate formation in the mixture is mainly due to bicarbonate alkalinizing the compound solution. The pH range of ropivacaine injection is 4.0–6.0; when the pH exceeds 6.0, ropivacaine will form a white flocculent precipitate. Laboratory animal studies have shown that precipitates are also rapidly observed after injecting ropivacaine into rats without alkalinization (no bicarbonate), and such precipitates may be difficult to avoid under physiological conditions (around pH 7.4). When the cocktail compound solution containing flocculent precipitate is injected around the sciatic nerve of experimental animals, all precipitates had been absorbed by dissection 2–3 days later, with no deposition observed around the nerve or muscle.24 In fact, it is common in clinical practice to add adjuvants to local anesthetics, which leads to varying degrees of crystallization; compared with other local anesthetics, ropivacaine has a higher tendency to precipitate.28,29 Clinically, bicarbonate-alkalinized ropivacaine is also used for lumbar epidural blocks,25 intraocular local injection in ophthalmic surgery,26 and brachial plexus blocks.27 In our study, to minimize the risk of possible adverse effects, all drugs were mixed immediately prior to administration, and no block-related complications were observed.
Limitations
This was a single-center study, and the sample size was calculated based on the morphine equivalent dose, so may have been insufficient for detecting differences in secondary outcomes. Only 0.375% ropivacaine was used; the effect of ESPB with other concentrations or formulations was not assessed, thus our results cannot provide information on the impact of various concentrations of ropivacaine for ESPB in patients undergoing major laparoscopic upper abdominal surgery. Because this was a single-center study with a small sample size, the results need to be confirmed by larger, multicenter studies.
Conclusion
The ropivacaine-based cocktail for bilateral ESPB prolongs analgesia to at least 48 h and improves postoperative pain control versus ropivacaine alone. Opioid consumption is reduced and patient satisfaction is higher without increased adverse events. The approach is a promising single-injection option for enhanced recovery after laparoscopic major upper abdominal surgery; optimal ropivacaine concentration merits further study.
Ethics Approval and Informed Consent
This study was approved by the Biomedical Ethics Committee of Chengdu Shangjin Nanfu Hospital (Approval No.: 2024 Review (43)). Written informed consent was obtained from all participants.
Acknowledgments
The authors thank the patients and nursing staff for their participation and support in this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sommer M, De Rijke JM, Van Kleef M, et al. The prevalence of postoperative pain in a sample of 1490 surgical inpatients. Eur J Anaesthesiol. 2008;25(4):267–14. doi:10.1017/S0265021507003031
2. Huang YX, Cheng Y, Wang W, et al. Intrathecal hydromorphone vs. transversus abdominis plane block for upper abdominal surgery: a propensity score-matching study. BMC Anesthesiol. 2025;25(1):231. doi:10.1186/s12871-025-03107-w
3. Wang JL, Du F, Ma YM, et al. Continuous erector spinae plane block using programmed intermittent bolus regimen versus intravenous patient-controlled opioid analgesia within an enhanced recovery program after open liver resection in patients with coagulation disorder: a randomized, controlled, non-inferiority trial. Drug Des Devel Ther. 2022;16:3401–3412. doi:10.2147/DDDT.S376632
4. Matsota PK, Koukopoulou IC, Konstantinos KA, et al. Ketamine versus tramadol as an adjunct to PCA morphine for postoperative analgesia after major upper abdominal surgery: a prospective, comparative, randomized trial. Rom J Anesth Intensive Care. 2020;27:43–51.
5. Allen S, DeRoche A, Adams L, et al. Effect of epidural compared to patient-controlled intravenous analgesia on outcomes for patients undergoing liver resection for neoplastic disease. J Surg Oncol. 2017;115:402–406. doi:10.1002/jso.24534
6. Gao YT, Deng XM, Yuan HB, et al. Patient-controlled intravenous analgesia with combination of dexmedetomidine and sufentanil on patients after abdominal operation a prospective, randomized, controlled, blinded, multicenter clinical study. Clin J Pain. 2018;34:155–161. doi:10.1097/AJP.0000000000000527
7. Sethi M, Sethi N, Jain P, et al. Role of epidural ketamine for postoperative analgesia after upper abdominal surgery. Indian J Anaes. 2011;55(2):141–145. doi:10.4103/0019-5049.79894
8. Kim YJ, Lee DK, Kwon HJ, et al. Programmed intermittent epidural bolus versus continuous epidural infusion in major upper abdominal surgery: a retrospective comparative study. J Clin Med. 2021;10:5382. doi:10.3390/jcm10225382
9. Niraj G, Kelkar A, Jeyapalan I, et al. Comparison of analgesic efficacy of subcostal transversus abdominis plane blocks with epidural analgesia following upper abdominal surgery. Anaesthesia. 2011;66:465–471. doi:10.1111/j.1365-2044.2011.06700.x
10. Subramaniam K, Subramaniam B, Pawar DK, et al. Evaluation of the safety and efficacy of epidural ketamine combined with morphine for postoperative analgesia after major upper abdominal surgery. J Clin Anesth. 2001;13:339–344. doi:10.1016/S0952-8180(01)00278-1
11. Nour HM, Abdalla HEE, Abogabal S, et al. Comparing thoracic epidural anaesthesia to rectus sheath catheter analgesia for postoperative pain after major abdominal surgeries: a systematic review. Cureus. 2023;15:e48842. doi:10.7759/cureus.48842
12. Niraj G, Kelkar A, Fox AJ. Oblique sub-costal transversus abdominis plane (TAP) catheters: an alternative to epidural analgesia after upper abdominal surgery. Anaesthesia. 2009;64:1137–1140. doi:10.1111/j.1365-2044.2009.06006.x
13. Boyev A, Prakash LR, Chiang YJ, et al. Postoperative opioid use is associated with increased rates of Grade B/C pancreatic fistula after distal pancreatectomy. J Gastrointest Surg. 2023;27:2135–2144. doi:10.1007/s11605-023-05751-4
14. Chelly JE, Ghisi D, Fanelli A. Continuous peripheral nerve blocks in acute pain management. British J Anaesth. 2010;105:i86–96. doi:10.1093/bja/aeq322
15. Dost B, De Cassai A, Balzani E, et al. Analgesic benefits of pre - operative versus postoperative transversus abdominis plane block for laparoscopic cholecystectomy: a frequentist network meta - analysis of randomized controlled trials. BMC Anesthesiol. 2023;23:408. doi:10.1186/s12871-023-02369-6
16. Coppens S, Ni Eochagain A, Hoogma DF, et al. Stranger things: the erector spinae block, extra sensory perception, or paranormal block by proxy?. Anesthesiol Perioper Sci. 2023;1:12. doi:10.1007/s44254-023-00007-5
17. Kang RA, Chin KJ, Kim GS, et al. Bilateral continuous erector spinae plane block using a programmed intermittent bolus regimen versus intrathecal morphine for postoperative analgesia in living donor laparoscopic hepatectomy: a randomized controlled trial. J Clin Anesth. 2021;75:110479. doi:10.1016/j.jclinane.2021.110479
18. Kang RA, Chin KJ, Gwak MS, et al. Bilateral single-injection erector spinae plane block versus intrathecal morphine for postoperative analgesia in living donor laparoscopic hepatectomy: a randomized non-inferiority trial. Reg Anesth Pain Med. 2019;23:100902. doi:10.1136/rapm-2019-100902
19. Malik O, Kaye AD, Kaye A, et al. Emerging roles of liposomal bupivacaine in anesthesia practice. J Anaesthesiol Clin Pharmacol. 2017;33:151–156. doi:10.4103/joacp.JOACP_375_15
20. Rodney AG, Ilfeld BM. An updated review on liposome bupivacaine. Curr Anesthesiol Rep. 2019;9:321–325. doi:10.1007/s40140-019-00327-y
21. Rasmussen SB, Saied NN, Bowens CJ, et al. Duration of upper and lower extremity peripheral nerve blockade is prolonged with dexamethasone when added to ropivacaine: a retrospective database analysis. Pain Med. 2013;14:1239–1247. doi:10.1111/pme.12150
22. Kimachi PP, Martins EG, Peng P, et al. The erector spinae plane block provides complete surgical anesthesia in breast surgery: a case report. A A Pract. 2018;11:186–188. doi:10.1213/XAA.0000000000000777
23. Lee JK, Lee GS, Kim SB, et al. A comparative analysis of pain control methods after ankle fracture surgery with a peripheral nerve block: a single-center randomized controlled prospective study. Medicina. 2023;59:1302. doi:10.3390/medicina59071302
24. Wang QR, Zhao CC, Hu J, et al. Efficacy of a modified cocktail for periarticular local infiltration analgesia in total knee arthroplasty a prospective, double-blinded, randomized controlled trial. J Bone Joint Surg Am. 2023;105:354–362. doi:10.2106/JBJS.22.00614
25. Ramos G, Pereira E, Simonetti MPB. Does alkalinization of 0.75% ropivacaine promote a lumbar peridural block of higher quality? Reg Anesth Pain Med. 2001;26(4):357–362. doi:10.1053/rapm.2001.24257
26. Guerrier G, Boutboul D, Chanat C, Samama CM, Baillard C. Bicarbonate-buffered ropivacaine-mepivacaine solution for medial caruncle anaesthesia. Anaesth Crit Care Pain Med. 2017; 36(4): 219–221. doi:10.1016/j.accpm.2016.09.007
27. Kour L, Sharma G, Tantray SH. Evaluation of addition of sodium bicarbonate to dexamethasone and ropivacaine in supraclavicular brachial plexus block for upper limb orthopedic procedures. Anesthesia. 2021;15(1):26–31. doi:10.4103/aer.aer_45_21
28. Fulling PD, Peterfreund RA. Alkalinization and precipitation characteristics of 0.2% ropivacaine. Reg Anesth Pain Med. 2000;25(5):518–521. doi:10.1053/rapm.2000.8931
29. Hoerner E, Stundner O, Putz G, Steinfeldt T, Mathis S, Gasteiger L. Crystallization of ropivacaine and bupivacaine when mixed with different adjuvants: a semiquantitative light microscopy analysis. Reg Anesth Pain Med. 2022;47(10):625–629. doi:10.1136/rapm-2022-103610
30. Viderman D, Aubakirova M, Abdildin YG. Erector spinae plane block in abdominal surgery: a meta-analysis. Front Med. 2022;9:812531. doi:10.3389/fmed.2022.812531
31. Sia CJY, Wee S, Au-Yong APS, et al. Analgesia efficacy of erector spinae plane block in laparoscopic abdominal surgeries: a systemic review and meta-analysis. Int J Surg. 2024;110:4393–4401. doi:10.1097/JS9.0000000000001421
32. Cai Q, Liu GQ, Huang LS, et al. Effects of erector spinae plane block on postoperative pain and side-effects in adult patients underwent surgery: a systematic review and meta-analysis of randomized controlled trials. Int J Surg. 2020;80:107–116. doi:10.1016/j.ijsu.2020.05.038
33. Shan T, Zhang XD, Zhao ZY, et al. Spread of local anaesthetic after erector spinae plane block: a randomised, three-dimensional reconstruction, imaging study. Br J Anaesth. 2025;134:830–838. doi:10.1016/j.bja.2024.10.046
34. Sandeep B, Huang X, Li Y, et al. A comparison of regional anesthesia techniques in patients undergoing video-assisted thoracic surgery: a network meta-analysis. Int J Surg. 2022;105:106840. doi:10.1016/j.ijsu.2022.106840
35. Wubetu P, Kasahun B, Bati T, et al. Analgesic effectiveness of ultrasound-guided unilateral erector spine block versus paravertebral block for postoperative management among adult patients undergoing upper abdominal surgery: a prospective cohort study. Ann Med Surg. 2025;87:2568–2575. doi:10.1097/MS9.0000000000003192
36. Hu J, Li XC, Wang QR, et al. Minimum effective concentration of ropivacaine for ultrasound-guided transmuscular quadratus lumborum block in total Hip arthroplasty: a randomized clinical trial. Braz J Anesthesiol. 2024;74:744461. doi:10.1016/j.bjane.2023.08.005
37. Chung HW, Chang H, Hong D, et al. Optimal ropivacaine concentration for ultrasound-guided erector spinae plane block in patients who underwent video-assisted thoracoscopic lobectomy surgery. Niger J Clin Pract. 2023;26:1139–1146. doi:10.4103/njcp.njcp_63_23
38. Goravanchi F, Kee SS, Kowalski AM, et al. A case series of thoracic paravertebral blocks using a combination of ropivacaine, clonidine, epinephrine, and dexamethasone. J Clin Anesth. 2012;24:664–667. doi:10.1016/j.jclinane.2012.05.005
39. Kalava A, Clendenen S, McKinney JM, et al. Bilateral thoracic paravertebral nerve blocks for placement of percutaneous radiologic gastrostomy in patients with amyotrophic lateral sclerosis: a case series. Rom J Anaesth Intensive Care. 2016;23:149–153.
40. Kot P, Rodriguez P, Granell M, et al. The erector spinae plane block: a narrative review. Korean J Anesthesiol. 2019;72:209–220. doi:10.4097/kja.d.19.00012
41. Sachdev D, Mamikunian G, Kia C, et al. Narrative review: erector spinae block in spine surgery. J Spine Surg. 2023;9:454–462. doi:10.21037/jss-23-14
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Efficacy and Safety of Erector Spinae Plane Block for Perioperative Pain Management in Lumbar Spinal Surgery: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
Fu MY, Hao J, Ye LH, Jiang W, Lv YW, Shen JL, Fu T
Journal of Pain Research 2023, 16:1453-1475
Published Date: 3 May 2023
Erector Spinae Plane versus Pectoralis Nerve Block for Mastectomy in Cancer Patients: A Retrospective, Multicenter Cohort Study
Yap EN, Wei J, Darling C, Linehan E, Behrends M, Ng KP
Journal of Pain Research 2025, 18:4775-4785
Published Date: 16 September 2025
Comparison of Quadratus Lumborum Plus Modified Erector Spinae Plane Block versus Pericapsular Nerve Group Block Plus Lateral Femoral Cutaneous Block on Postoperative Analgesia and Functional Recovery in Total Hip Arthroplasty: A Retrospective Propensity Score-Matched Study
Wu X, Wang M, Du M, Wang Y, Chen X, Zhang D, Xu Y
Journal of Pain Research 2026, 19:567827
Published Date: 13 January 2026
Effect of Intrathecal Hydromorphone on the Duration and Efficacy of Postoperative Analgesia in Patients Undergoing Benign Anorectal Surgery: Protocol for a Randomized, Double-Blind, Controlled Trial
Cao Y, Zhou Y, Zhou D, Xiong C, Fu L, Chen X, Zhang X
Journal of Pain Research 2026, 19:569284
Published Date: 26 February 2026
Efficacy and Safety of Ultrasound-Guided Erector Spinae Plane Block at Different Injection Depths for Percutaneous Kyphoplasty: A Randomized Controlled Trial
Liu Y, Yu Y, Gao X, Wang Q, Wang Y, Xia X
Drug Design, Development and Therapy 2026, 20:601168
Published Date: 16 June 2026