Back to Journals » Drug Design, Development and Therapy » Volume 20
Modified Single-Side-Lying Quadratus Lumborum Block Combined with Liposomal Bupivacaine versus Transversus Abdominis Plane Block for Post-Cesarean Analgesia: A Randomized Controlled Trial
Authors Rao J, Xiao J, Li B, Zong Y, Song J, Hu S, Luo A, Zeng L ![]() , Zhou Q
, Zhou Q
Received 10 November 2025
Accepted for publication 30 May 2026
Published 8 June 2026 Volume 2026:20 580472
DOI https://doi.org/10.2147/DDDT.S580472
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Muzammal Hussain
Jingzi Rao,1,* Jingyuan Xiao,1,* Bing Li,2,* Yuan Zong,1 Jie Song,1 Songquan Hu,1 Ailin Luo,3 Lian Zeng,1 Qun Zhou1
1Department of Anesthesiology, Jiangxi Maternal and Child Health Hospital, Nanchang Medical College, Nanchang, 330000, People’s Republic of China; 2Department of Anesthesiology, Longyan First Affiliated Hospital of Fujian Medical University, Longyan, 364000, People’s Republic of China; 3Department of Anesthesiology and Pain Medicine, Hubei Key Laboratory of Geriatric Anesthesia and Perioperative Brain Health, and Wuhan Clinical Research Center for Geriatric Anesthesia, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430022, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Lian Zeng, Department of Anesthesiology, Jiangxi Maternal and Child Health Hospital, Nanchang Medical College, Nanchang, 330000, People’s Republic of China, Email [email protected] Qun Zhou, Department of Anesthesiology, Jiangxi Maternal and Child Health Hospital, Nanchang Medical College, Nanchang, 330000, People’s Republic of China, Email [email protected]
Background: Inadequate post-cesarean analgesia remains a common clinical issue, associated with increased opioid use and risks of chronic pain and postpartum depression. Although the anterior quadratus lumborum block (QLB III) is more effective than transversus abdominis plane (TAP) block, it requires repeated positioning and may cause quadriceps numbness. To address these limitations, we designed a modified QLB to overcome these drawbacks. This study evaluated its analgesic efficacy and safety when combined with liposomal bupivacaine in cesarean delivery.
Methods: This single-center, randomized, single-blind trial enrolled 70 patients undergoing elective cesarean delivery. Patients were randomized to modified QLB (Group Q) or TAP block (Group T). The primary outcome was postoperative Day 1 VAS pain score. Secondary outcomes included VAS scores on Days 2, 3, during uterine compression and oxytocin infusion, opioid consumption, recovery metrics, and adverse events.
Results: Baseline characteristics were well balanced between the two groups (all p> 0.05). The modified QLB group achieved significantly lower VAS pain scores at rest, during uterine palpation and oxytocin infusion throughout the first three postoperative days (all p< 0.001), alongside fewer PCIA demands and reduced morphine-equivalent consumption. Recovery indicators and overall adverse event rates were comparable between groups, with no severe neurological or local complications observed in either cohort.
Conclusion: Modified single lateral decubitus QLB combined with liposomal bupivacaine yields superior analgesia and reduces opioid consumption compared with the TAP block, demonstrating favorable safety and clinical value for enhancing postoperative recovery following cesarean delivery. Nevertheless, these findings are limited by the single-center design and relatively small sample size, and long-term follow-up of chronic pain and postpartum mental outcomes was not performed.
Trial Registration Number: ChiCTR2400094584. The trial is publicly available and is registered at https://www.chictr.org.cn on December 25, 2024.
Keywords: cesarean delivery, quadratus lumborum block, liposomal bupivacaine, postoperative analgesia, opioid-sparing
Introduction
Cesarean delivery is among the most performed surgical procedures globally.1 Following the administration of single-shot spinal anesthesia, patients often experience severe postoperative pain, attributable to both the relatively large surgical incision and subsequent uterine contractions. Epidemiological data indicate that 68% of women undergoing cesarean delivery have insufficient postoperative pain relief, and 98% require additional opioids to control residual pain.2 This type of pain triggers extensive neuroendocrine stress responses; inadequate analgesia further increases the risk of breastfeeding failure, impaired maternal-infant interaction, chronic pain, postpartum depression, and postoperative morbidities, while compromising quality of life.3 Opioids remains the cornerstone of pain management following cesarean section.4 However, opioids are associated with a range of adverse effects, including pruritus, nausea, vomiting, and constipation.5 Moreover, their excretion in breast milk raises concerns about potential neonatal exposure, creating a clinical dilemma for breastfeeding mothers.6 With the global adoption of ERAS principles, regional anesthesia techniques have gained increasing attention for postoperative analgesia due to their targeted pain relief and favorable safety profile—characterized by fewer systemic side effects compared to opioids.7,8
Regional blocks are preferred for reduction in opioid use, but current options have limitations. TAP is widely used for its simplicity and applicability, yet it only relieves incision pain and fails to address visceral pain during oxytocin infusion or uterine massage. The conventional QLB III achieves comprehensive analgesia by facilitating local anesthetic spread toward the paravertebral space to block both somatic and visceral pain pathways.9,10 However, the standard procedure requires repeated patient repositioning; furthermore, inadvertent diffusion of the injectate to the lumbar plexus may lead to quadriceps weakness or numbness.11,12 Studies have shown that the subcostal QLB can also allow the spread of local anesthetics to the paravertebral space, and the high-level anterior QLB has not been shown to cause the side effect of quadriceps muscle numbness.13 Additionally, the most commonly used local anesthetic for nerve blocks in clinical practice is ropivacaine. However, conventional ropivacaine’s short duration limits its efficacy. Liposomal bupivacaine, a macromolecular sustained-release local anesthetic, has been validated for prolonged postoperative analgesia in various regional blocks, with demonstrated advantages of extended duration of action compared to conventional local anesthetics.14–16 Nevertheless, its diffusion capacity in the context of QLB III remains uncertain. There are concerns that the large molecular structure of the liposomal formulation may impede adequate penetration through the fascial planes of the quadratus lumborum muscle to reach the paravertebral space, potentially compromising analgesic outcomes. To date, no studies have directly addressed this pertinent anatomical and clinical question.
In this study, we developed a modified QLB technique that enables both an upper L2-level anterior QLB and a lower subcostal anterior QLB to be performed in a single lateral position. This dual-site approach is hypothesized to provide superior analgesia for post-cesarean patients with the dual burden of incisional and uterine contraction-related pain. No studies to date have validated this efficacy, so that the present randomized controlled trial was designed to evaluate the analgesic efficacy of a modified single-side-lying QLB combined with liposomal bupivacaine for post-cesarean delivery pain management. The findings aim to provide evidence-based guidance for optimizing analgesic protocols in clinical practice.
Materials and Methods
Study Design and Population
This study was prospectively registered at the Chinese Clinical Trial Registry (ChiCTR2400094584) and approved by the Ethics Committee of Jiangxi Provincial Maternity and Child Health Hospital (Approval No. EC-KY-2024118). The trial was conducted in strict compliance with the principles of the Declaration of Helsinki, and written informed consent was obtained from all patients or their legally authorized representatives before enrollment.
A single-center, randomized, single-blind, active-controlled Phase IV clinical trial was conducted at Jiangxi Provincial Maternity and Child Health Hospital between January 5, 2025, and July 29, 2025. A total of 70 patients scheduled for elective cesarean delivery were enrolled. And eligible participants were limited to primiparous or once-cesarean-delivered women aged 18–35 years, with ASA II status and normal BMI (18.5–24.9 kg/m2), who voluntarily requested nerve block for elective cesarean delivery, excluding those with placental abnormalities, pre-existing neurological/cardiovascular comorbidities, inability to provide informed consent, history of failed neuraxial block, or other contraindications such as local anesthetic allergy or anticipated emergency conditions (Figure 1).
 |
Figure 1 The flow diagram of patient enrollment, inclusion and exclusion. |
Randomization and Blinding
Patients were randomized to either the TAP block group (TAP group) or the modified QLB group (QLB group). The randomization sequence was generated by an independent researcher not involved in patient recruitment, data collection, or clinical procedures, using a computerized random number generator. To ensure allocation concealment, the sequence was sealed in sequentially numbered, opaque, tamper-evident envelopes.
Prior to the nerve block procedure, the operator responsible for performing the block opened the sequentially designated envelope to confirm the patient’s group assignment, after which the nerve block was administered. All other clinical staff involved in patient care and personnel responsible for data collection and analysis remained blinded to the group allocation throughout the study period.
Anesthetic and Analgesic Protocols
All patients received single-shot spinal anesthesia at the T6 to S sensory level with 0.5% hyperbaric bupivacaine (dose adjusted by height: 1.8 mL for height≤150 cm, titrated linearly from 1.8 mL to 2.6 mL for height 150–180 cm, 2.6 mL for height≥180 cm) via a 25-gauge (25G) Quincke spinal needle (90 mm in length) without adjuvant opioids. Immediately after surgery, both groups received PCIA to manage breakthrough pain. The PCIA pump contained nalbuphine 60 mg, trometamol injection 120 mg (1 mL: 30 mg specification; Chengdu BETTER Pharmaceutical Co., Ltd., China),17 ondansetron 12 mg, and dexamethasone 5 mg18 in a total volume of 60 mL, programmed with a background infusion rate of 0 mL/h, a bolus dose of 2 mL, and a lockout time of 10 minutes. Liposomal bupivacaine (1.33%, 13.3 mg/mL; Bupivacaine Liposome Injectable Suspension, Ahipin®, Jiangsu Hengrui Medicine, Lianyungang, China) and 20-gauge, 1.88-inch intravenous catheters (BD Angiocath™, Becton Dickinson, USA) were uniformly used for nerve block administration in both groups, with the liposomal bupivacaine diluted to 0.665% (20 mL, 133 mg) for clinical injection.
In the TAP group, With the patients in the supine position, a high-frequency linear ultrasound transducer (6–13 MHz; SonoSite Ultrasound System) was placed 10 cm lateral to the umbilicus. Under real-time ultrasound guidance, the transversus abdominis muscle was identified, and a 22G needle was advanced in-plane to the fascial plane between the internal oblique and transversus abdominis muscles. A total of 133 mg liposomal bupivacaine (0.665%, 6.65 mg/mL, 20 mL) was injected, with ultrasound confirmation of fusiform spread of the injectate between the two fascial layers. The procedure was repeated on the contralateral side to ensure bilateral analgesic coverage.
As show in Figure 2, in the modified QLB Group, patients were positioned in the lateral decubitus position to facilitate the administration of two distinct blocks. First, the upper L2-level anterior QLB was performed using a low-frequency curvilinear ultrasound transducer (2–5 MHz; SonoSite Ultrasound System) placed perpendicular to the lumbar spine to identify the “shamrock sign,” a sonographic landmark comprising the psoas major, quadratus lumborum, and erector spinae muscles. A 22-gauge (22G) needle was advanced in-plane to the space between the psoas major and quadratus lumborum muscles, and 133 mg liposomal bupivacaine (0.665%, 6.65 mg/mL, 20 mL) was injected. The success of the injection was verified through ultrasound visualization of separation between the two muscles. Subsequently, the lower subcostal anterior QLB was conducted by repositioning the transducer 6–8 cm lateral to the midline at the subcostal level, parallel to the lumbar spine, to identify the 12th rib, kidney, and quadratus lumborum muscle. A 22G needle was advanced out-of-plane to the fascial space between the quadratus lumborum muscle and anterior thoracolumbar fascia (ATLF). An additional 133 mg of liposomal bupivacaine (0.665%, 6.65 mg/mL, 20 mL) was administered, with ultrasound confirmation of separation between the quadratus lumborum muscle and ATLF. Upon the completion of both block procedures, patients were immediately repositioned to the supine position.
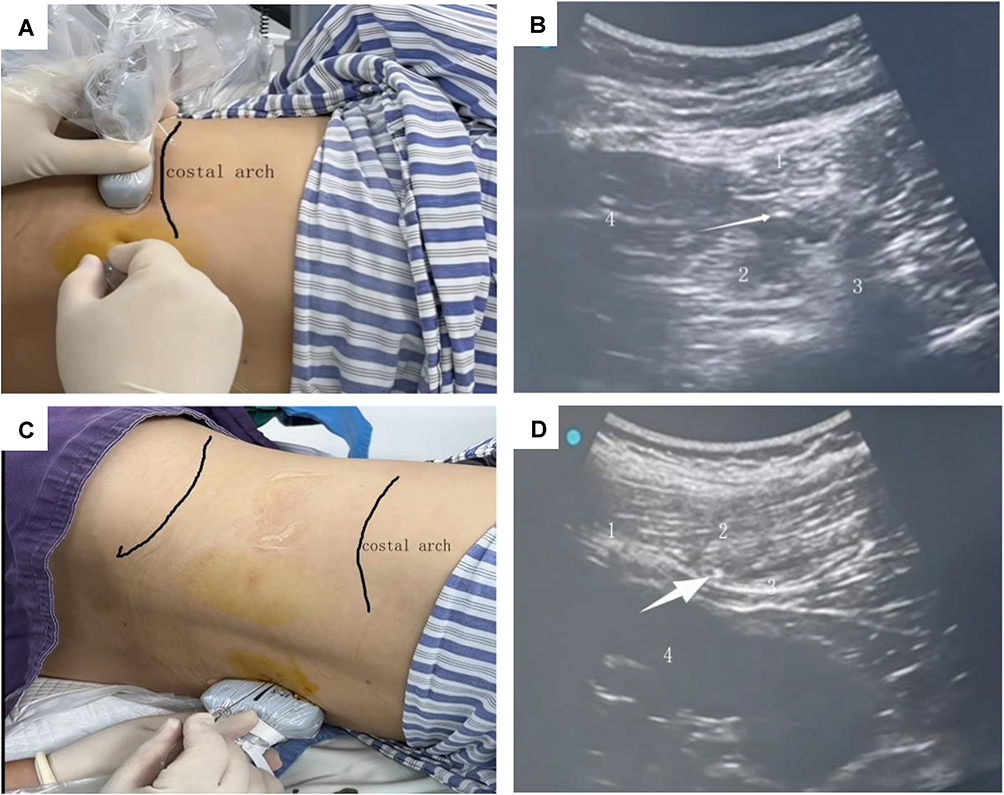 |
Figure 2 The illustration of ultrasound-guided modified quadratus lumborum block: step-by-step procedure with corresponding ultrasound imaging. (A and B) Schematic diagram and ultrasound image of anterior lumbar block operation at L2 vertebral body level (1: quadratus lumborum; 2: psoas major; 3: transverse process; 4: kidney; white arrow: needle tip; blue point: ultrasound indicator point). (C and D) Schematic diagram and ultrasound image of out-of-plane Subcostal Quadratus Lumborum Block (1: 12th rib; 2: quadratus lumborum; 3: Thoracolumbar Fascia; 4; kidney; white arrow: needle tip; blue point: ultrasound indicator point). |
Outcomes
The primary endpoint was the intensity of pain on postoperative Day 1, assessed using the VAS. Secondary outcomes were categorized into three mechanistic domains, as outlined below: 1. Postoperative Analgesia Profile: Pain intensity, assessed via VAS, was recorded on postoperative Days 2 and 3, with additional evaluations conducted during uterine palpation and oxytocin administration. 2. Postoperative Recovery Metrics: These included measurements of patient-controlled analgesia (PCA) consumption, time to first defecation, time to first ambulation, duration of urinary catheterization, and total hospital length of stay (LOS). 3. Safety Evaluation: Monitored adverse events (AEs) included nausea, vomiting, pruritus, constipation, urinary retention, allergic reactions, local infection at the nerve block site, bleeding/hematoma formation, hypoesthesia, and hypotension. This structured classification of outcomes ensures that all reported results are directly aligned with the dual research objectives of evaluating the efficacy and safety of the modified intervention.
Sample Size Calculation
Based on a preliminary study (n=20) showing a mean VAS score of 2.20 ± 1.19 in the TAP group and assuming a clinically meaningful difference of 1 point, a sample size of 30 per group was calculated using PASS 15 with α=0.05 and 90% power; ultimately, 35 participants were enrolled per group to accommodate a potential 15% attrition rate.
Statistical Analysis
All statistical evaluations were conducted utilizing SPSS software (Version 24.0; IBM Corp., Armonk, NY, USA). The assessment of data distribution normality was executed via the Shapiro–Wilk test. Continuous variables that exhibited a normal distribution were conveyed as mean ± standard deviation, and these variables were compared employing independent samples t-tests. Conversely, non-normally distributed data, such as total fluid infusion, were represented as median (interquartile range [IQR]) and subjected to analysis through Mann–Whitney U-tests. Ordinal categorical variables, including VSA scores, were also expressed as median (IQR) and evaluated using the Wilcoxon rank-sum test, in alignment with their hierarchical distribution characteristics. Categorical data were summarized as counts (percentage) [n (%)]. For comparative analysis of categorical variables between groups, the Chi-square (χ2) test was applied. In instances where the expected frequency in any cell was less than 1 or when the total sample size was below 40, Fisher’s exact test was employed to mitigate potential bias in results. A two-tailed p-value of less than 0.05 was deemed statistically significant for all conducted analyses.
Results
Demographic Data
Following an exhaustive evaluation of 70 prospective candidates, 2 individuals were excluded, 5 did not satisfy the established selection criteria, and 1 opted out of participation. Consequently, this randomized controlled trial successfully enrolled 64 qualified participants utilizing computerized block randomization, as illustrated in the CONSORT-compliant flowchart (Figure 1). The study cohort exhibited rigorous adherence to the protocol, achieving complete retention (100% compliance) and reporting no serious adverse events across both interventional arms. A thorough examination of baseline characteristics indicated no statistically significant differences between the groups (p>0.05) (Table 1). Furthermore, a comparative evaluation of intraoperative parameters confirmed parity between the groups.
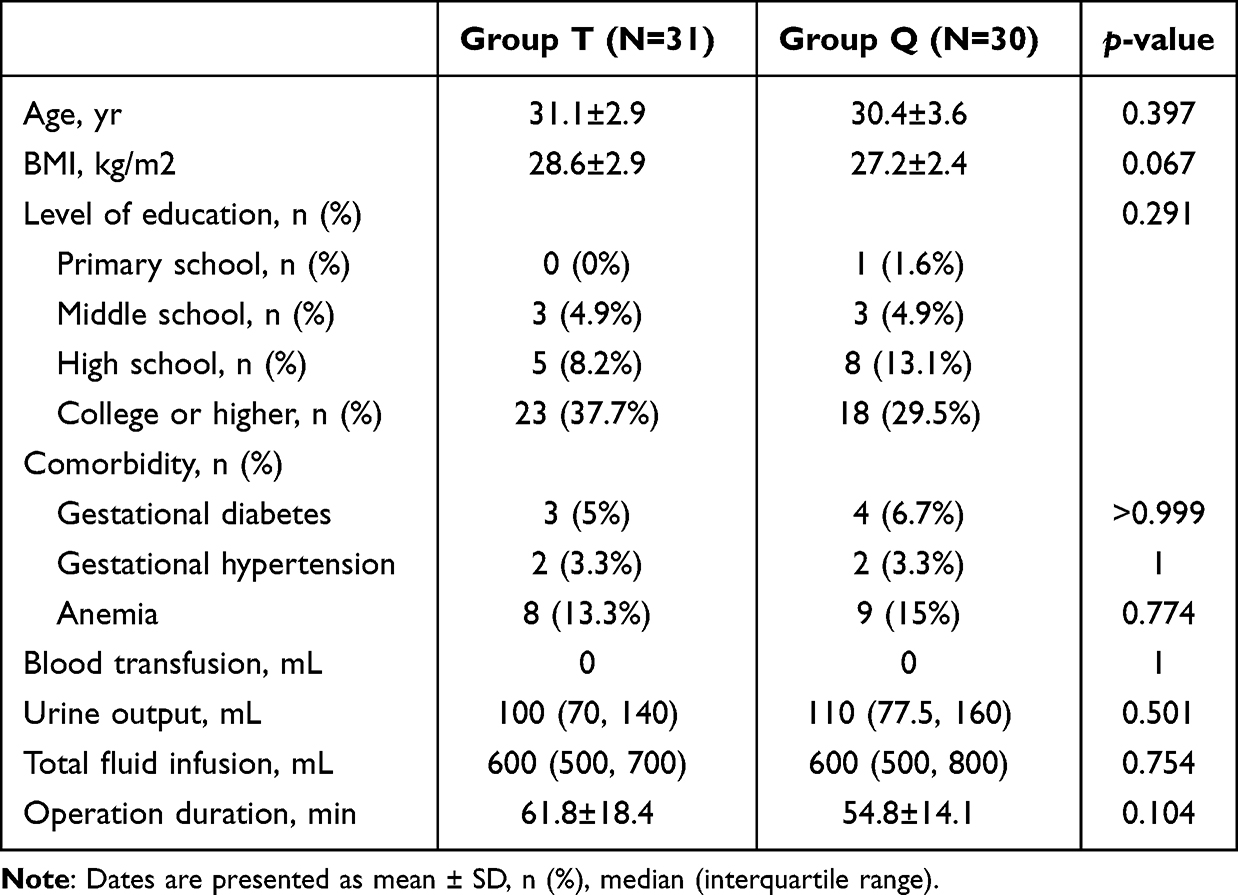 |
Table 1 Patient Characteristics and Procedural Data |
Efficacy Outcomes
Comparative analysis of postoperative pain revealed that the QLB group (N = 30) demonstrated significantly lower VAS scores than the TAP group (N = 31) across all postoperative 6 h, 24 h (day 1), 48 h (day 2) and 72 h (day 3) time points and provocative scenarios. Specifically, at rest at 24 h (postoperative day 1) (1.0 [0.0–1.3] vs 2.0 [2.0–3.0]), at 48 h (postoperative day 2) (1.0 [0.0–1.0] vs 2.0 [1.0–2.0]), at 72 h (postoperative day 3) (0.0 [0.0–0.0] vs 1.0 [0.0–1.0]), the median differences were 1 point (all p<0.001). Pain scores during uterine compression and oxytocin administration were recorded at 6 hours postoperatively. During uterine compression (2.0 [1.0–3.0] vs 4.0 [3.0–5.0]) and oxytocin injection (3.0 [1.8–3.0] vs 5.0 [4.0–5.0]), the median differences reached 2 points (both p<0.001), indicating consistently superior analgesia with the QLB approach under both static and dynamic conditions (all p<0.001; Table 2).
 |
Table 2 Postoperative Visual Analogue Scale (VAS) |
Regarding postoperative recovery, the QLB group required significantly fewer patient-controlled analgesia activations (3 [2.8–3.0] vs 7 [7–8] times; p<0.001) and lower morphine consumption (6 [3.5–13.6] vs 16 [10–24] mg; p<0.001). However, no significant differences were observed between groups in time to first defecation (49.1 ± 17.8 vs 43.3 ± 16.6 h; p=0.196), duration of catheter indwelling (22.2 ± 4.6 vs 19.8 ± 4.7 h; p=0.051), time to first ambulation (23.7 ± 3.7 vs 22.0 ± 4.4 h; p=0.106), or length of hospital stay (3 [2–3] vs 3 [2–3] days; p > 0.05) (Table 3). The observed delays in indwelling urinary catheter removal and first ambulation were attributed to institutional standardized clinical protocols for cesarean section patients, rather than opioid-related adverse effects (opioid consumption was effectively reduced by regional blocks in both groups). All patients received 24-hour postoperative bed rest for maternal hemodynamic stability and uterine involution monitoring, with indwelling urinary catheters routinely removed after bed rest and confirmation of spontaneous urination ability. This protocol was uniformly applied to both groups, eliminating intergroup bias and ensuring outcome comparability.
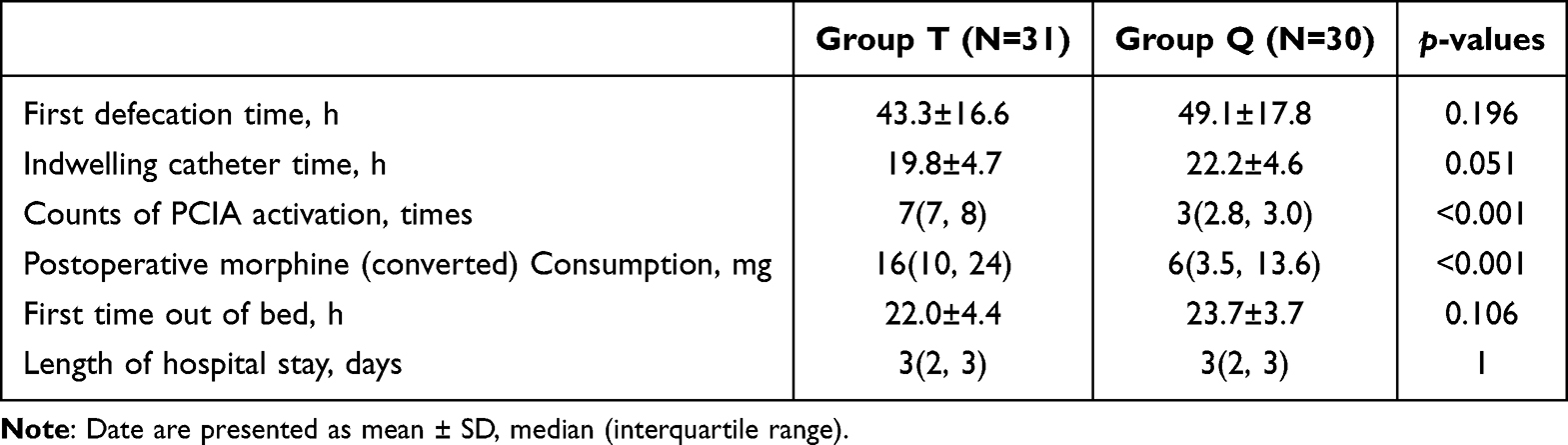 |
Table 3 Postoperative Outcomes |
Safety Outcomes
The two groups exhibited comparable safety profiles, with no statistically significant differences in overall adverse events (15.0% vs 13.3%; p=0.774) or specific incidents, including nausea/vomiting (1.6% vs 4.9%; p=0.629), constipation (8.2% vs 4.9%; p=0.668), urinary retention (4.9% vs 1.6%; p=0.581), or hypoesthesia (0% vs 1.6%; p>0.05). No cases of pruritus, allergic reactions, local infection, or hypotension were reported in either group. These results indicate that the QLB technique offers significantly improved analgesic efficacy without compromising safety compared to TAP block (Table 4).
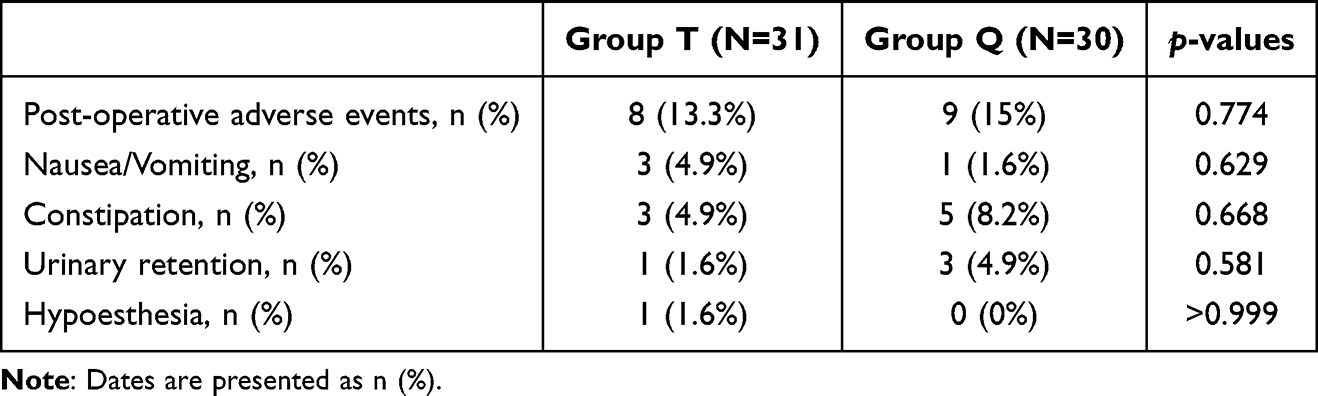 |
Table 4 Safety Outcomes |
Discussion
This randomized controlled trial evaluated the analgesic efficacy of a modified single-side-lying quadratus lumborum block in comparison to the transversus abdominis plane block, both supplemented with liposomal bupivacaine, for managing post-cesarean delivery pain management and the results demonstrate the clinical superiority of the modified QLB approach. We have demonstrated that this combination of single lateral decubitus position L2-3 anterior QLB and subcostal QLB is a new clinical application. The traditional anterior QLB requires two lateral positions,19 which is very inconvenient for the clinical operation of passive body position for patients after cesarean section. Some researchers have proposed a technique of performing the anterior QLB in the supine position.20,21 However, these supine positions present a notable disadvantage postoperatively, particularly following a cesarean section, as they necessitate the introduction of gas into the abdominal cavity. This can adversely affect ultrasound imaging, rendering it unsuitable for such patients. A comparable approach to ours is that of Ashok Jadon et al,22 who also performed bilateral QLB in a single lateral position. The primary distinction lies in their application of the traditional anterior QLB at the L3-4 level, whereas our technique was performed at the L2-3 level, with the injection administered between the quadratus lumborum and the anterior thoracolumbar fascia on the lower side. We opted for a higher position and employed the subcostal QLB for the lower side. The conventional L3-4 anterior QLB carries the risk of inducing numbness in the quadriceps muscles.23 Such numbness post-procedure may lead patients to fear potential nerve damage, thereby heightening their anxiety. Furthermore, LU et al did not reported this complication during L2-3 anterior QLB,13 nor did our study. This absence of complications may be attributed to the limited sample size. However, the higher anatomical position is likely distant from the lumbar plexus, which theoretically reduces the likelihood of this complication. Additionally, the anterior QLB predominantly diffuses into the paravertebral region. The subcostal QLB also demonstrates effective analgesic outcomes through paravertebral diffusion,24,25 aligning with findings from autopsy studies.26 Our findings indicate that this analgesic approach is relatively effective. Compared to the TAP block, it exerts a more pronounced effect on visceral pain, particularly during uterine compression and oxytocin administration for uterine contractions. This observation is consistent with previous research on the analgesic efficacy of the anterior QLB technique following cesarean sections.27
Furthermore, our research findings indicate that bupivacaine liposomes are both feasible and effective for lumbar paraspinal block. However, there is ongoing debate regarding the analgesic efficacy of bupivacaine liposomes in clinical settings. Previous research on the use of bupivacaine liposomes for local infiltration has demonstrated no significant difference compared to the clinical effects of bupivacaine hydrochloride.28–30 Some randomized controlled trials have also reported negative outcomes for bupivacaine liposomes. Specifically, studies on bupivacaine liposomes for local infiltration have consistently shown no difference in clinical efficacy compared to bupivacaine hydrochloride. Additionally, bupivacaine liposomes have been used for supraclavicular brachial plexus block.15 However, it is important to note that many studies have focused on local infiltration and low-dose nerve blocks. Recently, larger-dose liposomal bupivacaine blocks at the fascial plane have demonstrated relatively significant effects. Notably, a study utilizing bupivacaine liposomes for internal rectal block reported excellent clinical outcomes.31 The investigations into the use of bupivacaine liposomes for transversus abdominis plane (TAP) block have consistently demonstrated prolonged analgesic effects post-surgery.32,33 Additionally, bupivacaine liposomes have exhibited significant efficacy when employed for the serratus anterior plane (SAP) block.34 It is noteworthy that a different formulation of bupivacaine liposome was utilized for the SAP block, which did not yield any positive clinical outcomes.35 Upon comparison, it was observed that the study by Zhang et al involved diluting bupivacaine liposomes with saline, whereas Donn’s research incorporated bupivacaine liposomes with hydrochloric bupivacaine. In our study, we diluted bupivacaine with hydrochloric acid to achieve a total volume of 40 mL, reaching a concentration of 266 mg. The potential impact of combining bupivacaine liposomes on the duration of action remains unexplored. Overall, our research has established that 0.664% bupivacaine liposomes, as a large molecule, can permeate the fascial plane of the quadratus lumborum muscle to the paravertebral area, producing a sustained blocking effect with clinical significance.
In addition, the utilization of opioid medications remains a significant concern. Our research indicates that by implementing an enhanced approach incorporating bupivacaine liposomes, we can substantially decrease the required dosage of opioids. Our findings align with those of Ferit et al, demonstrating a notable reduction in opioid consumption following anterior QLB.36 The median postoperative morphine dosage (after conversion) was reduced to merely 6 mg, with the median number of PCIA use limited to three. These results suggest the potential for employing oral opioids as an adjunct in pain management.
This study presents several limitations that require careful consideration. As a single-center trial with a relatively small sample size (n = 70), the generalizability of the findings may be limited. Additionally, the single-blind design—where only outcome assessors were blinded—could have introduced performance bias in subjective measures, such as VAS. Another limitation is the inability to objectively assess the extent of the nerve block due to the concurrent use of intraspinal anesthesia, which may result in deviations arising from incomplete sensory blockade. To minimize this potential variability, all nerve blocks were administered by the same experienced operator. For future research, we recommend conducting larger, multicenter, randomized controlled trials to validate these findings. Furthermore, prospective cohort studies are necessary to evaluate the incidence of chronic post-surgical pain and to investigate the impact of postoperative pain management on patients with preexisting depressive symptoms, employing validated pain and psychological assessment tools.
Conclusions
This randomized controlled trial demonstrated that the modified unilateral lateral decubitus position quadratus lumborum block (QLB), in conjunction with liposomal bupivacaine, provided superior analgesic effects following cesarean section. Specifically, it significantly reduced pain scores within the first three days postoperatively, with a notable reduction in visceral pain, decreased opioid consumption, and exhibited favorable safety and operational convenience. The “L2-3 + subcostal” design, coupled with the sustained-release properties of liposomal bupivacaine, effectively addressed the limitations associated with traditional regional blocks, such as the requirement for multiple positional adjustments and inadequate coverage of internal organs.
Data Sharing Statement
Data are available from Lian Zeng on reasonable request.
Ethics Approval and Informed Consent
This study was prospectively registered at the Chinese Clinical Trial Registry (ChiCTR2400094584) and approved by the Ethics Committee of Jiangxi Provincial Maternity and Child Health Hospital (Approval No. EC-KY-2024118).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Project of Jiangxi Provincial Administration of Traditional Chinese Medicine (2025022601), Project of Jiangxi Provincial Health Commission (202610085), Key Scientific Research Project of Jiangxi Provincial Department of Education (GJJ2503424); National Natural Science Foundation of China (82371208, 81974160).
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Einum A, Harmon QE, Sørbye LM, et al. Associations between term cesarean delivery in the first pregnancy and second-pregnancy preterm delivery. Acta Obstet Gynecol Scand. 2025;104(1):68–10. doi:10.1111/aogs.14996
2. Bjørnstad J, Ræder J. Post-operative pain after caesarean section. Tidsskr nor Laegeforen. 2020;140(7). doi:10.4045/tidsskr.19.0506
3. Mo X, Zhao T, Chen J, et al. Programmed intermittent epidural bolus in comparison with continuous epidural infusion for uterine contraction pain relief after cesarean section: a randomized, double-blind clinical trial. Drug Des Devel Ther. 2022;16:999–1009. doi:10.2147/DDDT.S350418
4. Prabhu M, Dubois H, James K, et al. Implementation of a quality improvement initiative to decrease opioid prescribing after cesarean delivery. Obstet Gynecol. 2018;132(3):631–636. doi:10.1097/AOG.0000000000002789
5. Zimmerman A, Laitman A. Safe management of adverse effects associated with prescription opioids in the palliative care population: a narrative review. J Clin Med. 2024;13(10):2746. doi:10.3390/jcm13102746
6. Heerfordt IM, Gotfredsen DR, Horwitz H, et al. EudraVigilance insights: suspected adverse drug reactions in infants through breastfeeding. Br J Clin Pharmacol. 2025;91(8):2431–2436. doi:10.1002/bcp.70063
7. Gupta R, Van De Ven T, Pyati S. Post-thoracotomy pain: current strategies for prevention and treatment. Drugs. 2020;80(16):1677–1684. doi:10.1007/s40265-020-01390-0
8. Zhou LZ, Li X, Zhou LM. Global trends in research of perioperative analgesia over past 10 years: a bibliometric analysis. J Pain Res. 2023;16:3491–3502. doi:10.2147/JPR.S429719
9. Qin Y, Yang Y, Qin S, et al. Regional nerve block in postoperative analgesia after cesarean section: a narrative review. Medicine. 2024;103(52):e41159. doi:10.1097/MD.0000000000041159
10. Jing Y, Zhao S, Guo W, et al. Comparison of analgesic modalities after cesarean section: a network meta-analysis and systematic review. Int J Surg. 2025;111(5):3599–3612. doi:10.1097/JS9.0000000000002352
11. Kim DH, Liu J, Beathe JC, et al. Interscalene brachial plexus block with liposomal bupivacaine versus standard bupivacaine with perineural dexamethasone: a noninferiority trial. Anesthesiology. 2022;136(3):434–447. doi:10.1097/ALN.0000000000004111
12. Kadoya Y, Tanaka N, Suzuka T, et al. Anterior quadratus lumborum block and quadriceps strength: a prospective cohort study. J Clin Med. 2023;12(11):3837. doi:10.3390/jcm12113837
13. Lu Y, Zhang J, Xu X, et al. Sensory assessment and block duration of transmuscular quadratus lumborum block at L2 versus L4 in volunteers: a randomized controlled trial. Minerva Anestesiol. 2019;85(12). doi:10.23736/S0375-9393.19.13656-5
14. Zhao H, Dou W, Meng X, et al. Liposomal bupivacaine vs. Ropivacaine for wound infiltration on chronic postsurgical pain after video-assisted thoracoscopic lung surgery: protocol for a randomized, double-blind, controlled trial. Ann Med. 2025;57(1):2543522. doi:10.1080/07853890.2025.2543522
15. Chan TCW, Wong JSH, Wang F, et al. Addition of liposomal bupivacaine to standard bupivacaine versus standard bupivacaine alone in the supraclavicular brachial plexus block: a randomized controlled trial. Anesthesiology. 2024;141(4):732–744. doi:10.1097/ALN.0000000000005035
16. Nedeljkovic SS, Kett A, Vallejo MC, et al. Transversus abdominis plane block with liposomal bupivacaine for pain after cesarean delivery in a multicenter, randomized, double-blind, controlled trial. Anesthesia Analg. 2020;131(6):1830–1839. doi:10.1213/ANE.0000000000005075
17. Nitschke LF, Schlösser CT, Berg RL, et al. Does patient-controlled analgesia achieve better control of pain and fewer adverse effects than intramuscular analgesia? A prospective randomized trial. Arch Surg. 1996;131:417–423.
18. Ryoo S-H, Yoo JH, Kim MG, et al. The effect of combination treatment using palonosetron and dexamethasone for the prevention of postoperative nausea and vomiting versus dexamethasone alone in women receiving intravenous patient-controlled analgesia. Korean J Anesthesiol. 2015;68:267–273.
19. Abd Elmaksoud OSM, Elansary SEM, Fahmy NG, et al. A comparative study between postoperative analgesia of fascia iliaca compartment block and anterior quadratus lumborum block in proximal femur fracture. Anesthesiol Res Pract. 2022;2022:1–7. doi:10.1155/2022/3465537
20. Diwan S, Blanco R, Kulkarni M, et al. Abordagem supina axilar média coronal para realização de bloqueio do quadrado lombar anterior: relato de casos. Braz J Anesthesiol. 2020;70(4):443–447. doi:10.1016/j.bjan.2020.04.007
21. Dai J, Li S, Weng Q, et al. Opioid-free anesthesia with ultrasound-guided quadratus lumborum block in the supine position for lower abdominal or pelvic surgery: a randomized controlled trial. Sci Rep. 2024;14(1):4652. doi:10.1038/s41598-024-55370-5
22. Jadon A, Jain P, Dhanwani L. Bilateral transmuscular quadratus lumborum block performed in single lateral decubitus position without changing position to the contralateral side. Indian J Anaesth. 2018;62(4):314. doi:10.4103/ija.IJA_750_17
23. Tanggaard K, Nielsen MV, Holm UHU, et al. No quadriceps muscle weakness following anterior quadratus lumborum block compared with placebo: a randomized, non-inferiority, blinded, volunteer trial. Reg Anesth Pain Med. 2025;50(7):568–574. doi:10.1136/rapm-2024-105313
24. Balocco AL, López AM, Kesteloot C, et al. Quadratus lumborum block: an imaging study of three approaches. Reg Anesth Pain Med. 2021;46(1):35–40. doi:10.1136/rapm-2020-101554
25. Elsharkawy H, Ahuja S, Degrande S, et al. Subcostal approach to anterior quadratus lumborum block for pain control following open urological procedures. J Anesth. 2019;33(1):148–154. doi:10.1007/s00540-018-02605-1
26. Elsharkawy H, El-Boghdadly K, Kolli S, et al. Injectate spread following anterior sub-costal and posterior approaches to the quadratus lumborum block: a comparative cadaveric study. Eur J Anaesthesiol. 2017;34(9):587–595. doi:10.1097/EJA.0000000000000680
27. Hansen CK, Dam M, Steingrimsdottir GE, et al. Ultrasound-guided transmuscular quadratus lumborum block for elective cesarean section significantly reduces postoperative opioid consumption and prolongs time to first opioid request: a double-blind randomized trial. Reg Anesth Pain Med. 2019;44(9):896–900. doi:10.1136/rapm-2019-100540
28. Ilfeld BM, Eisenach JC, Gabriel RA. Clinical effectiveness of liposomal bupivacaine administered by infiltration or peripheral nerve block to treat postoperative pain. Anesthesiology. 2021;134(2):283–344. doi:10.1097/ALN.0000000000003630
29. Hussain N, Brull R, Sheehy B, et al. Perineural Liposomal Bupivacaine Is Not Superior to Nonliposomal Bupivacaine for Peripheral Nerve Block Analgesia. Anesthesiology. 2021;134(2):147–164. doi:10.1097/ALN.0000000000003651
30. Vandepitte CF, Van Boxstael S, Duerinckx JF, et al. Effect of bupivacaine liposome injectable suspension on sensory blockade and analgesia for dupuytren contracture release. J Hand Surg Glob Online. 2019;1(4):191–197. doi:10.1016/j.jhsg.2019.09.008
31. Xu M, Wang S, Meng Y, et al. The analgesic efficacy of liposomal bupivacaine in adductor canal block following knee arthroplasty: a single-center, prospective, randomized and controlled clinical trial. Drug Des Devel Ther. 2025;19:7591–7601. doi:10.2147/DDDT.S535901
32. Liu HH, Qiu D, Xu DR, et al. Recovery quality of transversus abdominis plane block with liposomal bupivacaine after cesarean delivery: a randomized trial. J Clin Anesth. 2024;99:111608. doi:10.1016/j.jclinane.2024.111608
33. Park RH, Chou J, Devito RG, et al. Effectiveness of liposomal bupivacaine transversus abdominis plane block in DIEP flap breast reconstruction: a randomized controlled trial. Plast Reconstr Surg. 2024;154(4S):52S–59S. doi:10.1097/PRS.0000000000011326
34. Zhang Y, Li W, Wei A, et al. Comparing liposomal bupivacaine and ropivacaine in serratus anterior plane block for thoracoscopic lobectomy: a randomized controlled trial. Drug Des Devel Ther. 2025;19:4717–4726. doi:10.2147/DDDT.S513287
35. Marciniak D, Raymond D, Alfirevic A, et al. Combined pectoralis and serratus anterior plane blocks with or without liposomal bupivacaine for minimally invasive thoracic surgery: a randomized clinical trial. J Clin Anesth. 2024;97:111550. doi:10.1016/j.jclinane.2024.111550
36. Yetik F, Yilmaz C, Karasu D, et al. Comparison of ultrasound-guided quadratus lumborum block-2 and quadratus lumborum block-3 for postoperative pain in cesarean section: a randomized clinical trial. Medicine. 2022;101(49):e31844. doi:10.1097/MD.0000000000031844
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comparison of Quadratus Lumborum Plus Modified Erector Spinae Plane Block versus Pericapsular Nerve Group Block Plus Lateral Femoral Cutaneous Block on Postoperative Analgesia and Functional Recovery in Total Hip Arthroplasty: A Retrospective Propensity Score-Matched Study
Wu X, Wang M, Du M, Wang Y, Chen X, Zhang D, Xu Y
Journal of Pain Research 2026, 19:567827
Published Date: 13 January 2026
ED95 of Liposomal Bupivacaine for Postoperative Local Infiltration Analgesia in Women Undergoing Cesarean Section: A Randomized Controlled Trial
Liu J, Zhang Y, Liu L, Zhang W
Drug Design, Development and Therapy 2026, 20:571871
Published Date: 6 February 2026
Anterior Quadratus Lumborum Block with Liposomal Bupivacaine versus Ropivacaine for Postoperative Recovery in Laparoscopic Colorectal Surgery: A Randomized Controlled Trial
Liu D, Luo C, Zhang Y, Huang H, Yang Y
Drug Design, Development and Therapy 2026, 20:611347
Published Date: 12 May 2026
Single-Injection Liposomal Bupivacaine Adductor Canal Block for Pain Control and Recovery After Total Knee Arthroplasty: A Randomized Controlled Double‑Blinded Study
Wen J, Peng H, Jiang Y, Chen M, Ou J, Huang W, Li P, Zhou J, Wu X
Drug Design, Development and Therapy 2026, 20:587861
Published Date: 20 May 2026
Effects of Liposomal Bupivacaine for Superficial Parasternial Intercostal Plane Block on Postoperative Stress and Analgesia in Patients Undergoing Median Sternotomy: A Prospective, Randomized, Double-Blind Trial
Yu W, Li Y, Wei A, Chen S, Zhang Y
Drug Design, Development and Therapy 2026, 20:597889
Published Date: 22 June 2026