Back to Journals » Journal of Pain Research » Volume 16
Regional Analgesia for Cesarean Delivery: A Narrative Review Toward Enhancing Outcomes in Parturients
Authors Silverman M, Zwolinski N, Wang E, Lockwood N, Ancuta M, Jin E, Li J ![]()
Received 3 August 2023
Accepted for publication 28 October 2023
Published 10 November 2023 Volume 2023:16 Pages 3807—3835
DOI https://doi.org/10.2147/JPR.S428332
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Rushna Ali
Matthew Silverman,1 Nicholas Zwolinski,1 Ethan Wang,2 Nishita Lockwood,1 Michael Ancuta,1 Evan Jin,1 Jinlei Li1
1Department of Anesthesiology, Yale University School of Medicine, New Haven, CT, USA; 2Yale University School of Medicine, New Haven, CT, USA
Correspondence: Jinlei Li, Yale University School of Medicine, Department of Anesthesiology, 333 Cedar Street, P.O. Box 208051, New Haven, CT, 06520-8051, USA, Email [email protected]
Introduction: With the current surge on peripheral nerve blocks in post-cesarean pain management and the historical lack of unequivocal evidence supporting its universal use, this review intended to re-examine the extended scope of literature on regional anesthesia and postoperative analgesia in low-transverse cesarean section.
Methods: A literature search was conducted up to April 2023 using PubMed to identify articles relevant to our search words “cesarean section”, “neuraxial morphine”, “post-cesarean analgesia”, as well as the name of each individual nerve block. The literature search was ultimately narrowed to systematic reviews and randomized controlled trials published between 2012 and 2023. We define, describe, and discuss the evidence surrounding each individual regional anesthetic technique in the presence and absence of intrathecal morphine, which is used as the gold standard when appropriate.
Results: In the absence of neuraxial morphine, all regional anesthetic techniques have some level of analgesic benefit in the post-cesarean analgesia. Transversus Abdominis Plane blocks continue to have the most studies in their use. Newer fascia plane blocks including the anterior Quadratus Lumborum, and Erector Spinae Plane blocks provide significant analgesia. In addition, direct comparison among peripheral nerve blocks consistently favors the more proximal, centralized techniques. Conversely, in the presence of neuraxial morphine, no peripheral anesthetic technique has reliably and reproducibly demonstrated an added analgesic benefit regardless of the peripheral nerve block technique or location of local anesthetic injection in the post-cesarean population.
Conclusion: Neuraxial morphine continues to be the gold standard for post-cesarean section analgesia, the benefit of additional single injection regional anesthetic is currently not evidence supported. In cases where neuraxial opioids have not or cannot be given, there is overwhelming evidence that regional anesthetic techniques improve post-cesarean section analgesia and decrease post-operative opioid consumption. Even though there is no consensus on the optimal peripheral nerve block, emerging evidence suggests more centralized abdominal fascia plane block trends towards better analgesia.
Keywords: cesarean section, peripheral nerve block, neuraxial morphine, erector spinae plane block, quadratus lumborum block, transversus abdominis plane block
Introduction
In 2020, greater than 1.1 million cesarean sections were performed in the United States.1 Neuraxial anesthesia as the gold standard2 is associated with well-documented risk reduction associated with cesarean delivery including difficult or failed intubation, aspiration, surgical site infections, and venous thromboembolic events,3,4 as well as additional benefits such as postoperative analgesia, reduced blood loss, greater maternal bonding, and decreased maternal morbidity and mortality.5
With the increasing emphasis on early recovery after surgery, neuraxial anesthesia in conjunction with ultrasound-guided peripheral regional anesthetic techniques has recently become a growing field within obstetric anesthesiology. However, there is a lack of evidence supporting its universal use for cesarean section. Further information is needed on the type and efficacy of common nerve blocks and comparison to intrathecal or epidural morphine. Our review begins with an examination of the current scope of literature involving neuraxial anesthesia in cesarean section, with particular emphasis on neuraxial opiate modality. We then cross-examine current literature for various regional techniques in cesarean patients by peripheral nerve block type. We aim to organize the data for the purpose of providing a comprehensive summary of the current literature on central neuraxial and peripheral regional anesthesia techniques offered to parturients.
Cesarean Delivery: Surgical Techniques and Anatomic Information
There are multiple surgical approaches to cesarean delivery. For simplicity, most techniques vary by location and direction of both the incision through the skin and the uterus. Either may be incised vertically or horizontally and at varying locations. Our review is limited to discussion of the lower-segment transverse hysterotomy with a transverse skin incision, otherwise known as the Pfannenstiel-Kerr approach. Alternative techniques to cesarean section exist but are less common. Therefore, they are not the focus of our literature review.
The most common skin incision for cesarean section is the low transverse incision, which has been shown to decrease postoperative pain, incur a lower risk of complications including wound dehiscence/infection/hernia development, and attain better cosmetic results than a midline vertical incision.6 The location and curvature of this incision may vary by technique but the most common worldwide is the Pfannenstiel, a curved incision a few centimeters above the level of the pubic symphysis, and the Joel-Cohen, a straight incision roughly 3cm caudal to an imagined horizontal line connecting the anterior superior iliac spines. After skin incision, the subcutaneous tissue and the fascial layers are commonly dissected bluntly. The rectus muscle may be dissected bluntly or divided vertically with scissors. The approach to the uterine incision depends on many factors, including gestational age, fetal and placental location, and acuity of operation. The most common hysterotomy is the Kerr incision, a transverse incision of the lower uterine segment. It has been shown to decrease blood loss, lower the risk of bladder injury, and lower the risk of future gestation uterine rupture when compared to vertical incision.7 The uterine incision is then expanded, after which the newborn and placenta are removed. Closure of the above layers then follows.
While intra-operative cesarean section via neuraxial anesthesia typically requires a dense sensory block extending from sacral dermatomes to the level of T4, post-cesarean analgesia does not require such extensive coverage.8 Post-cesarean pain can be narrowed to the dermatomal distribution of skin incision, myotome innervation to abdominal wall layers, and visceral innervation to the uterus.9 In Pfannenstiel incisions, the somatic innervation of the skin is often composed of the ilioinguinal and iliohypogastric nerves derived from the T11-L1 spinal nerve roots. The entire anterior abdominal wall and fascial layers are innervated by a multitude of nerves including the thoracoabdominal (T7-T11), subcostal (T12), iliohypogastric (L1), and ilioinguinal nerves (L1), the majority of which run through the fascial plane between the internal oblique and transversus abdominis muscles.10 The uterus receives its sympathetic innervation from the low thoracic T11-12/high lumbar L1-3 nerve roots via the hypogastric plexus and its parasympathetic supply from the pelvic splanchnic nerve derived from the S2 to S4 nerve roots.11 Thus, the goal of regional anesthesia is to infiltrate local anesthetic along the components of this innervation if possible.
Methods
A comprehensive literature review was performed via PubMed up to April 2023 to identify all articles relating to interventional post-cesarean analgesia. Articles were identified using the search keywords “cesarean section”, “neuraxial morphine”, “post-cesarean analgesia”, “epidural analgesia”, “peripheral nerve block”, “nerve block”, “paravertebral block”, “erector spinae plane block”, “Quadratus Lumborum block”, “Transversus abdominis block”, “Ilioinguinal/Iliohypogastric block”, “rectus sheath block”, local infiltration. The literature search was narrowed to randomized controlled trials and systematic reviews/meta-analyses for the past decade between 2012 and 2023. Articles meeting inclusion criteria had the studied population as parturients undergoing cesarean section with a Pfannenstiel-Kerr incision. Articles were excluded if they were case reports, if they did not provide a description of block technique to ensure that the named block was consistent with its label, and if the peripheral nerve blockade was performed without ultrasound guidance/assistance (excluding those describing neuraxial anesthesia, and wound infiltration of local anesthetic by the surgeon). Special attention was paid to whether the article mentioned the inclusion or exclusion of long-acting neuraxial opioid.
Review of Regional Anesthesia Techniques
Neuraxial Anesthesia
Anatomical Definition
Neuraxial anesthesia refers to injecting medication such as local anesthetic with or without adjuvants such as opioids or epinephrine into the epidural space (epidural anesthesia) or into the subarachnoid/intrathecal space (spinal anesthesia) (Figure 1). It is commonly used in chest, abdominal and lower extremity anesthesia and analgesia, including cesarean delivery and post-cesarean pain control.12
 |
Figure 1 Animation of Transverse Section of Anatomical Targets of Regional Anesthesia Techniques for Cesarean Delivery. 1 –- Transverse process. 2 – Quadratus lumborum muscle. 3 – Abdominal wall muscles from deep to superficial: transversus abdominis, internal oblique, external oblique. |
Technique
The patient is commonly placed in a sitting or lateral decubitus position. After sterile skin preparation and draping, the spinous processes are palpated or identified via ultrasound. Local infiltration is placed at an interspace between spinous processes in midline approach or between lamina in paramedian approach. A needle is advanced to the epidural or intrathecal space stepwise based on loss of resistance technique, with or without ultrasound assistance. Spinal anesthesia (SA) is typically a single injection while epidural anesthesia (EA) is administered through a catheter for continuous infusion. There is also the option of combined spinal-epidural analgesia (CSE).12
Ultrasound guidance can assist in the process. A transverse scan of the lumbar spine can visualize the posterior and anterior complexes of the dura, allowing for an estimate of the loss-of-resistance depth (Figure 2Ai). A sagittal scan of the lumbar spine at the lamina can also visualize the interlaminar space and allow for possible real-time placement of the neuraxial block under ultrasound guidance (Figure 2Aii).13
 |
Figure 2 Sonographic approach for common regional anesthesia approaches for caesarean delivery. (A) Epidural Anesthesia. (Ai) Ultrasound of lumbar back for epidural or spinal anesthesia placement, transverse orientation. Yellow line – midline. Red line – posterior complex. Green line – anterior complex. (Aii) Ultrasound of lumbar spine for epidural or spinal anesthesia placement, sagittal orientation. Black lines – lamina. Red asterisk – approximate location of epidural space. Red line – posterior complex. Green line – anterior complex. (B) Paravertebral Block Green lines – Transverse processes. Red line – pleura. (C) Erector Spinae Plane Block Green lines – transverse processes. (D) Quadratus Lumborum Blocks. (E) Transversus Abdominis Plane Block. (F) Rectus Sheath Block. *Quadratus lumborum muscle. Yellow line – plane for lateral QL block. Red line – plane for posterior QL block. Green line – plane for anterior QL block. *Target plane for TAP block. *Target plane for rectus block superficial to the posterior rectus sheath superficially and the peritoneum deep. Abbreviations: PM, psoas major; TP, transverse process; ESP, erector spinae plane; EO, external oblique; IO, internal oblique; TA, transversus abdominis; RA, rectus abdominis. |
Efficacy in Cesarean Anesthesia and Analgesia
Neuraxial anesthesia is commonly used in lower abdominal and lower extremity surgeries, including cesarean delivery, for a dense surgical block.12 In addition, medications are routinely administered neuraxially for post-operative analgesia, either through a single injection or continuous fashion. Post-operative analgesia does not require near the level of density of a block that neuraxial anesthesia requires.
While there is more than one way of providing neuraxial analgesia for pain management, neuraxial opioid administration, and more specifically epidural or intrathecal morphine administration, is the “gold standard” of post-cesarean pain control. It is also a crucial aspect of multimodal analgesia, supported by guidelines provided by the American Society of Anesthesiologists (ASA).14 The more recent sources cited in the ASA guidelines demonstrate improved patient outcomes with neuraxial opioids compared to parentally or intramuscularly administered opioids.15,16 This is true in terms of both pain control as well as side effects associated with opioid use in post-cesarean analgesia, such as pruritus, nausea, vomiting, and added surveillance for risk of respiratory depression.17 However, in recent years the development and refinement of newer methods of peripheral analgesia, discussed later, has challenged the conclusions drawn by these guidelines. When compared to these alternative methods, early data has shown neuraxial morphine to consistently provide superior analgesia than peripheral nerve blockade alone,18–23 and combining various regional anesthetic techniques including quadratus lumborum and transversus abdominis plane block with neuraxial morphine does not appear to provide significant additional analgesic benefit.24,25 With regional anesthetic techniques and the medications injected constantly advancing, the increasing awareness of physical and psychological adverse impacts of poorly controlled postpartum pain on parturients, emphasis on early recovery after surgery and minimization of persistent postsurgical pain, further research is needed to continually evaluate each individual peripheral nerve block’s efficacy in the absence of and in conjunction with neuraxial morphine.
Paravertebral Block (PVB)
Anatomical Definition
The thoracic paravertebral block (PVB) is widely used for analgesia for chest and upper abdominal surgeries. It is performed by entering a space bound by the vertebral body medially, the pleura anteriorly, and the superior costotransverse ligament posteriorly. Within this location lies the spinal nerve root after it exits the epidural space, with the sympathetic trunk close by.
The thoracic paravertebral space ends at L1 with the superior attachment of the psoas muscle.26 The L1 nerve root enters a different compartment within the psoas muscle to form the lumbar plexus and thus is not thought to be blocked reliably with the thoracic paravertebral block.27 While a thoracic paravertebral nerve block at T12-L1 may not reliably cover the Pfannenstiel incision at L1, it has the advantage of possibly spreading medially to the epidural space and blocking visceral pain at the surrounding epidural levels.28
Technique
The patient can be placed in sitting, lateral decubitus or prone positioning and the block performed via landmark or ultrasound-guidance. The ultrasound technique with a paramedian sagittal in-plane approach is most common, although transverse in-plane approach has been described. For the paramedian sagittal in-plane approach, the patient’s T11 and T12 vertebral levels are identified using the inferior border of the rib cage as a landmark. A low-frequency, curvilinear ultrasound probe is placed in the sagittal plane in the midline and slowly translated laterally until the transverse processes appear. A slight lateral tilt will usually then expose the pleura in the spaces between the transverse processes (Figure 2B). In some cases, the costotransverse ligament can be visualized in the interspace above the pleura. After local infiltration, a needle is inserted in plane with the ultrasound beam (Table 1). The goal is to place the needle between the transverse processes and through the costotransverse ligament if visible. Block success is determined by a downward depression of the pleura on injection of the local anesthetic26 and ideally lack of superficial spread toward the erector spinae muscle (Figure 2B).
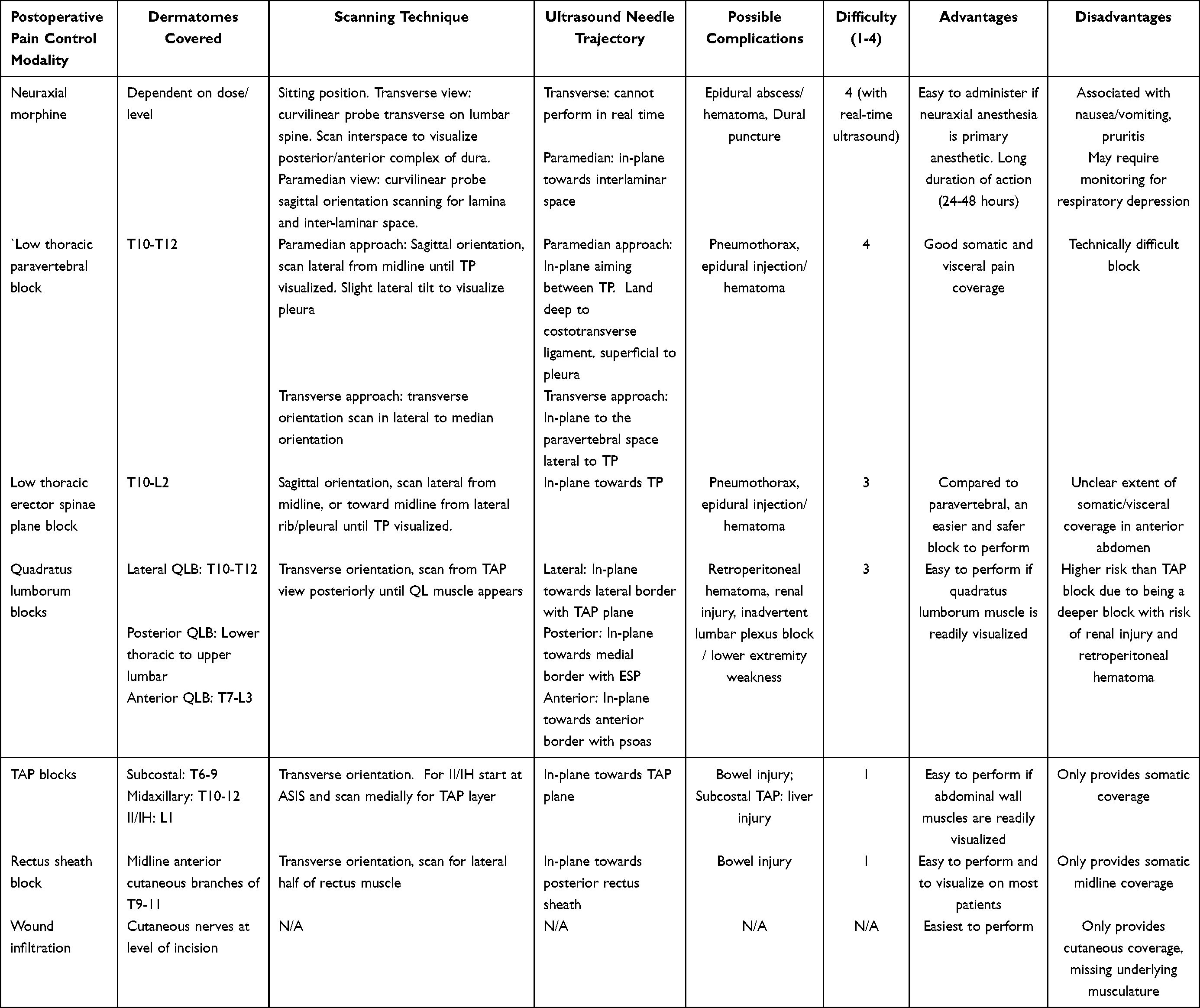 |
Table 1 Comparative Summary of Common Regional Anesthesia Techniques in Caesarean Delivery |
Efficacy in Cesarean Analgesia
The wide adoption of ultrasound makes it possible to precisely assess the efficacy and location of injection of paravertebral blocks as compared to landmark technique, and clearly distinguish between paravertebral versus erector spinae plane blocks. While direct comparison between ultrasound-guided and landmark PVB are sparse, ultrasound-guided PVB has been demonstrated to increase the likelihood of block success and post-operative analgesia.29,30 Nonetheless, evidence regarding the utility of paravertebral block for post-cesarean pain control is scarce. Randomized controlled trials and evidence beyond case reports are lacking.
Erector Spinae Plane Block (ESP)
Anatomical Definition
The ESP block refers to longitudinal local anesthetic spread in the fascial plane anterior to the erector spinae muscle but posterior to the transverse process.31 While only the dorsal rami are contained in this plane, the block’s efficacy in anterior chest wall surgeries suggests that the ventral rami are sometimes, though not reliably, blocked as well. One theory is that the local anesthetic spreads anteriorly through ligamentous structures into the paravertebral space.32 Without an articulating rib, it is hypothesized that the ventral rami would have better extension at and below the level of the L1 nerve root compared to thoracic injections. The erector spinae plane is posterior to the psoas muscle and local anesthetic can spread freely in the cranio-caudal direction. Small cadaver and live-subject studies have suggested anterior spread of local anesthetic into the lumbar plexus plausible.32 There is also the possibility of epidural spread, as local anesthetic that tracks into the paravertebral or lumbar plexus region can also spread into the epidural space.33
Technique
The patient can be placed in sitting, lateral decubitus or prone position. The patient’s T11 and T12 vertebrae are identified using the inferior border of the rib cage as a landmark. ESP is almost always performed under ultrasound guidance. Depending on patient body habitus, a high-frequency linear or low-frequency curvilinear ultrasound probe is placed in the sagittal plane in the midline and scans laterally until the transverse processes appear. A slight lateral tilt can help expose the pleura but is not necessary in all cases. After local infiltration, a needle is inserted in plane with the ultrasound beam and advanced to just posterior to the transverse process through the erector spinae muscle (Figure 2C). Block success is determined by cranial and caudal spread of local anesthetic in the plane between the transverse process and erector spinae muscle.31
Efficacy in Cesarean Analgesia
Erector spinae plane blocks have emerged as a theoretically safer and easier-to-perform alternative to thoracic paravertebral nerve blocks for chest wall, abdominal and spine surgeries. A relatively new technique, the ESP and its efficacy in cesarean section has only been studied in the past few years. Multiple separate RCTs have been able to demonstrate that in the absence of intrathecal morphine, the addition of ESP block compared to control of non-peripheral nerve block multimodal analgesia provided significantly decreased 24-hour opioid consumption,34 prolonged time to first rescue analgesic, and lowered post-operative pain scores.35
One systematic review and meta-analysis consisting of three RCTs from 2020 focused on comparing ESP block to other post-operative analgesic interventions including other abdominal wall blocks and intrathecal morphine.36 Two of the RCTs included in this meta-analysis produced consistent results when comparing ESP block to TAPs block post-cesarean section; ESP block provided significantly superior analgesia for significantly longer duration, and the patients in the TAPs block cohort consumed more supplemental opioid and requested rescue analgesia sooner than those who received ESP.37,38 When included with a third study in a systematic review, ESP block no longer showed a significant improvement in resting pain scores over the alternatives, although the other conclusions above including length of analgesia and reduction in supplemental opioid requirement persisted.36 A separate RCT of 52 patients comparing low thoracic ESP block to the posterior QL block found no significant differences in pain scores or block efficacy.39 A similar result of equal analgesic effect was found in an RCT comparing low thoracic ESP block to the anterior QL block.40 Further comparison between ESP and alternative peripheral nerve blocks in this patient population has yet to be studied.
Stratify with Intrathecal Morphine
The majority of RCTs evaluating ESP block after cesarean section do not involve neuraxial opioid. However, one RCT compared 140 patients, half of whom received an ESP block with bupivacaine without neuraxial opioid and half received intrathecal morphine and an ESP block with saline. This study revealed a significantly lower oral opioid requirement, lower pain scores in the first 24 hours, and longer time to first supplemental analgesic in the patients who received the ESP block with bupivacaine.41 These results suggest that ESP may have a superior analgesic effect to intrathecal morphine, although these results have yet to be reproduced nor studied on a larger population scale. It would also be worthwhile to assess the efficacy of ESP in the presence of intrathecal morphine, and whether there would be added benefit.
Lateral, Posterior and Anterior Quadratus Lumborum Blocks (QLBs)
Anatomical Definition
The quadratus lumborum blocks (QLBs) target the fascial planes surrounding the quadratus lumborum (QL) muscle, a posterior abdominal wall muscle that originates inferiorly on the posterior iliac crest and iliolumbar ligament and inserts superiorly on the twelfth rib as well as the L1-L5 transverse processes (Figure 1). Posterior to the QL is the erector spinae muscle, and the fascia between them is the middle thoracolumbar fascia. Anterior to the QL is the psoas muscle, and the fascia between them is the anterior thoracolumbar fascia. The fascial plane lateral to the quadratus lumborum is contiguous with the transversus abdominis plane. The lateral QLB targets this lateral border and gives a spread of local anesthetic similar to a TAP block as described below and was the first of the QLBs to be described (previously referred to as QL-1). The posterior QLB (previously referred to as QL-2) targets the middle thoracolumbar fascia posterior to the QL muscle and may possibly spread to the thoracic paravertebral spaces through this fascial plane. The anterior or trans-muscular QLB, the most recent QLB described (previously referred to as QL-3), targets the anterior thoracolumbar fascia and may possibly spread to the thoracic paravertebral spaces. Some studies report medication spread as high as the T7 paravertebral space with the posterior QLB, while others only to T9-10.1,2 As for lumbar spread, there is the possibility of spreading to the upper lumbar nerve roots (as far as L3) but this was largely observed in cadaver studies (Table 2). Of note, the ilioinguinal and iliohypogastric nerves, branches of L1, do course over the anterior surface of the quadratus lumborum on their way to the upper pelvic region.42
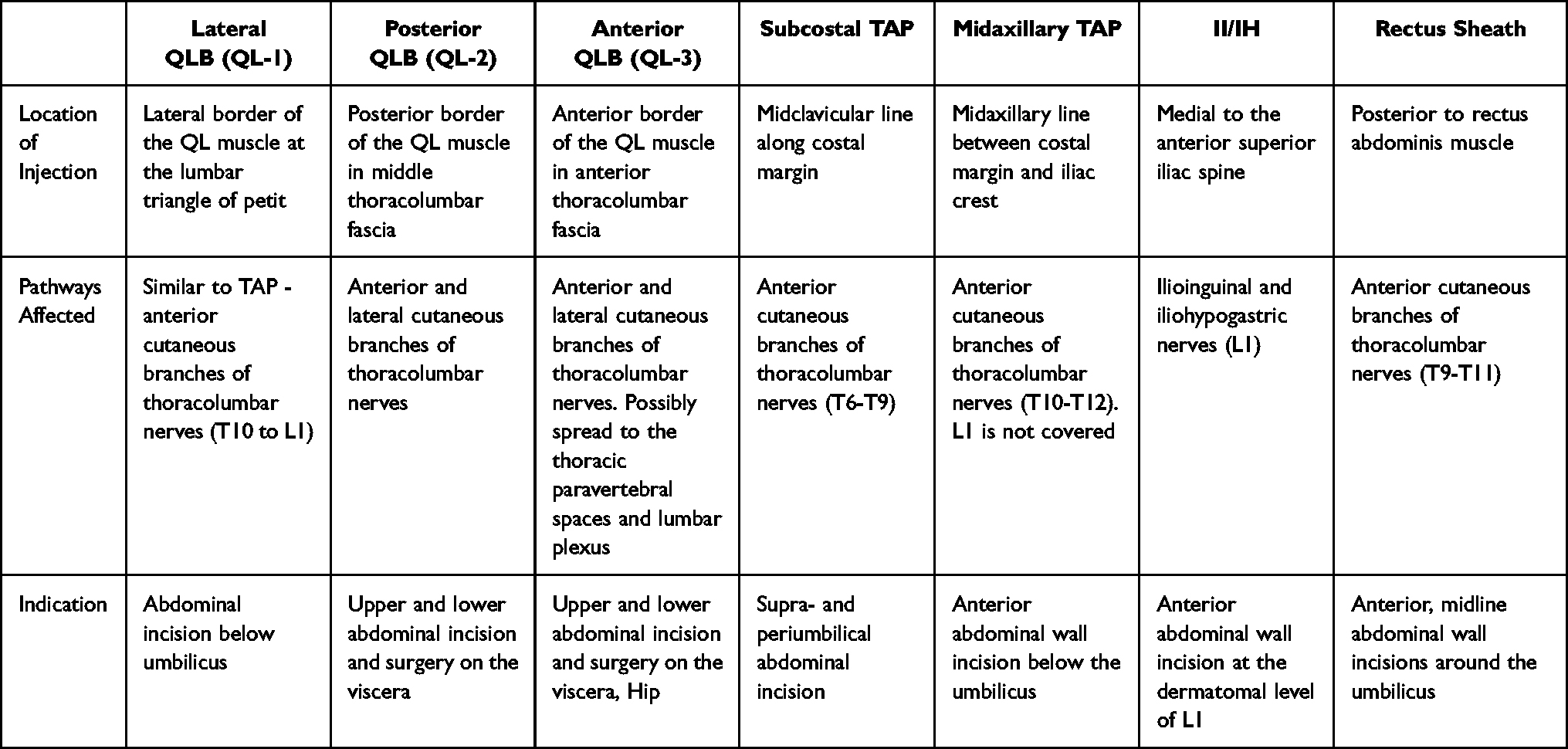 |
Table 2 Comparison of Quadratus Lumborum, Transverse Abdominis Plane, Ilioinguinal/Iliohypogastric and Rectus Sheath Blocks |
Technique
Bilateral QLBs can be achieved with the patient supine for lateral QLB or in lateral decubitus or prone position for posterior and anterior QLB. Depending on patient body habitus and the type of QLB chosen, a high-frequency linear or low-frequency curvilinear ultrasound probe can be used to scan in a transverse plane. The probe starts anterior to the midaxillary line to identify the external oblique, internal oblique, and transversus abdominis muscles. The practitioner then focuses on the plane between the internal oblique and transversus abdominis muscles (the transversus abdominis plane or TAP plane) and follows that plane posteriorly. The internal oblique muscle will eventually taper off and the TAP plane superficial to the transversus abdominis muscle will join with the fascia deep to the transversus abdominis muscle. Both these fasciae together will abut the superficial posterior border of the QL muscle. To confirm the identity of the QL muscle, one can seek out the “shamrock sign” with the transverse process forming a “stem” and the psoas, quadratus lumborum, and erector spinae muscles forming the clovers43 (Figure 2D).
Once the quadratus lumborum muscle is identified, one can perform a lateral QLB superficial to the QL and look for spread of local anesthetic into the TAP plane. To perform a posterior QLB, one can place the needle on the posterior border of the QL where the QL meets the erector spinae muscle and inject within the middle thoracolumbar fascia. To perform an anterior QLB, one can place the needle deep to the QL muscle where it borders the psoas and inject local anesthetic in the anterior thoracolumbar fascia. A successful trans-muscular anterior QL block will show downward depression of the psoas muscle via ultrasound.43 In difficulty anatomy, it can be helpful to know that the QL muscle tends to be less echogenic than the psoas muscle.
Efficacy in Cesarean Analgesia
Randomized controlled trials have demonstrated that in the absence of neuraxial morphine, the lateral QLB,44,45 posterior QLB46 and anterior QLB47 are effective in reducing post-operative pain scores and opioid consumption in parturients after cesarean section as compared to controls. In addition, one RCT in 2021 comparing the anterior QLB to posterior QLB in patients under neuraxial anesthesia in the absence of neuraxial morphine found that anterior QLB led to a significantly greater reduction in pain scores, 24-hour opioid consumption, and time to first analgesic.48 These results were redemonstrated in 2022, an RCT of 104 patients who had a cesarean under general anesthesia, further supporting anterior QLB as a superior analgesic in the absence of neuraxial morphine.49
Many RCTs have focused on comparing different QLB techniques to TAP blocks to determine whether one provides superior analgesia or reduction in opioid consumption. A 2020 meta-analysis of 31 RCTs compared all 3 types of QLBs against midaxillary and subcostal TAP blocks in patients who had not received neuraxial morphine, and found that these blocks were equivalent in their analgesic effect.24 However, many individual RCTs have found evidence suggesting that QLBs do provide greater reduction in pain scores and opioid consumption when compared to TAP blocks, with one study additionally suggesting a prolonged effect of QL when compared to TAP.50–53
Whereas most research focuses on the acute analgesic effects of these blocks and is limited to block duration, Borys et al used the Neuropathic Pain Symptom Inventory (NPSI) scale to evaluate post-operative pain months after patients were randomly assigned to receive either a posterior QL block, TAP block, or nothing in the absence of neuraxial opioid. They found a significant reduction in pain scores at 1 month and 6 months in the QL and TAP groups compared to control, but were unable to demonstrate a significant difference in chronic pain score between the QL and TAP group.54 This unique study demonstrates that regional analgesic benefits exceed the duration of the block itself, and future studies could expand and quantify this effect further.
Stratify with Intrathecal Morphine
Multiple meta-analyses have been able to demonstrate a significant analgesic effect of QL block when compared to control in patients who did not receive neuraxial opioids.20,25 However, in a meta-analysis of 10 RCTs, Tan et al found no significant improvement in analgesia in patients that received both QLB and neuraxial opioids when compared to those who received neuraxial opioids alone.25 This finding was redemonstrated in an additional meta-analysis of 31 studies that admittedly shared some but not all the sources utilized by Tan et al. El-Boghdadly et al’s meta-analysis of anterior, lateral, and posterior QLB found that in the presence of neuraxial opioid there was no significant difference in analgesia in the patients who received QL blocks vs control.24 While these analyses suggest that QL blocks of all types have limited efficacy in patients already receiving neuraxial opioids, one author directly compared posterior QL block to patients who received intrathecal morphine and found surprising results. Salama was able to demonstrate that patients who received single shot posterior QL block with 0.375% ropivacaine had significantly reduced resting and moving pain scores, decreased supplemental opioid consumption at 48 hours, and significantly fewer adverse events than those who received 100mcg intrathecal morphine and no peripheral nerve block. Salama also demonstrated a 70% supplemental opioid reduction in the QL group compared to control whereas the intrathecal morphine group had a 30% total opioid reduction over controls.55 These results have not been redemonstrated.
Transversus Abdominis Plane Block (TAP): Subcostal, Midaxillary and Ilioinguinal/Iliohypogastric (II/IH) Nerve Blocks
Anatomic Definition
The transversus abdominis plane block is a commonly used fascial plane block for abdominal surgeries. There are multiple approaches to the TAP block to target different dermatome levels but they all aim to inject medication at the fascial layer between two abdominal wall muscles. The subcostal TAP block, which targets the fascial plane at the midclavicular line directly inferior to the rib cage between the posterior rectus sheath and the transversus abdominis muscle, is believed to cover dermatomes T6-T9. The midaxillary TAP block, previously referred to as the lateral TAP block, targets the fascial plane between the internal oblique and transversus abdominis on the midaxillary line halfway between the ribs and the pelvis. The midaxillary TAP is believed to cover dermatomes T10-T12 from midline to midclavicular line. Previously known as the anterior TAP block, the combined ilioinguinal/iliohypogastric (II/IH) nerve block targets the same fascial plane as the midaxillary TAP but is performed medial to the anterior superior iliac spine (ASIS) to cover the ilioinguinal and iliohypogastric nerves which address the L1 contribution.56,57 Of note, these blocks are not thought to reach the neuraxial space nor spread to the sympathetic trunk and thus do not cover visceral pain.
Technique
For cesarean section with Pfannenstiel incision, the II/IH and/or midaxillary TAP are preferred given their distribution as above. With a patient in a supine position, a high-frequency linear transducer is placed in a transverse orientation on the patient’s abdomen just superior to the iliac crest at the midaxillary line for the midaxillary TAP block, or just medial to the ASIS for the II/IH. The two oblique muscles and the transversus abdominis are identified, and a needle is inserted in the fascial plane between the internal oblique muscle and transversus abdominis (Figure 2E). The ilioinguinal and iliohypogastric nerves lie next to each other within this fascial plane and may be recognized by their hyperechoic oval shape. Block success is determined by downward depression of the transversus abdominis muscle and underlying peritoneum.56
Efficacy in Cesarean Analgesia
It is well established that both the midaxillary TAP and II/IH blocks do provide some post-operative analgesia to patients undergoing cesarean section.58–61 The subcostal TAP block is not frequently studied in this population, likely due to its low likelihood of incisional coverage. A meta-analysis of 17 studies comprised of 11,000 patients demonstrated the analgesic efficacy of TAP block when compared to controls in the absence of neuraxial morphine; patients who received a TAP block needed fewer oral opioid equivalents and a longer time before they required their first breakthrough opioid.58
TAP blocks have been compared to each other as well as many other peripheral nerve blocks to evaluate their efficacy for post-cesarean pain control. As mentioned above, RCTs comparing TAPs to ESP blocks have demonstrated the superiority of ESP block for decreasing total opioid consumption as well as increasing the time to first rescue analgesic.37,38 Further, while a meta-analysis has found no significant difference in analgesic effect of TAP compared to various types of QL blocks,24 multiple RCTs have individually produced results demonstrating TAPs inferiority to QL.50–53 A systematic review of 5 RCTs found similar efficacy for post-cesarean analgesia when comparing midaxillary TAP blocks to II/IH blocks.62 Two meta-analyses of post-cesarean patients in the absence of neuraxial morphine were unable to find significant analgesic advantage to an ultrasound guided TAP block versus direct wound infiltration of local anesthetic in the subcutaneous tissue by the surgeon.63,64
Stratify with Intrathecal Morphine
Multiple meta-analyses, which admittedly do have some overlap in the RCTs they contain, have reviewed post-cesarean patients who have received neuraxial morphine as well as an ultrasound guided TAP block. Analysis of 524 patients in 2012 and later 1100 patients in 2020 have been unable to conclude that the addition to TAP block to neuraxial morphine has any analgesic benefit.58,59 A meta-analysis of midaxillary TAP blocks and lateral QL-blocks found that in the presence of neuraxial opioid there was no significant difference in analgesia in the patients who received regional anesthesia vs control.24 An RCT looking specifically at a population meeting the criteria for severe pre-eclampsia was able to redemonstrate that in the presence of neuraxial opioid, TAP block does not appear to significantly reduce opioid requirement or dynamic pain scores.65 However, in 2022 Ryu et al performed the largest meta-analysis to date on the topic including 76 studies consisting of 6278 post-cesarean section patients comparing various regional techniques including neuraxial, ESP, transverse fascia plane, QL, ilioinguinal-iliohypogastric, TAP, rectus sheath, and surgeon wound infiltration. In patients receiving interventional analgesia, Ryu et al suggest that only one peripheral nerve block in conjunction with neuraxial morphine provides additional analgesic effect than neuraxial morphine alone: a combination of ilioinguinal and anterior TAP blocks.60
With the efficacy of TAP blocks in question in patients who have also received neuraxial morphine, authors have studied the addition of liposomal bupivacaine, trade name “Exparel”, to evaluate for added analgesic benefit or duration, if any exists. Two RCTs have demonstrated the addition of liposomal bupivacaine to a TAP block to provide non-inferior analgesia than standard TAP block with plain bupivacaine in both patients who have and have not received neuraxial morphine,23 one of which was able to demonstrate reduced opioid consumption over a longer period in those who received liposomal bupivacaine in their TAP block.66 More data is needed to further expand on these findings.
Rectus Sheath Block (RSB)
Anatomic Definition
The rectus sheath encloses the rectus abdominis muscles. It is a fibrous compartment formed by the aponeuroses of the transversus abdominis, internal oblique, and external oblique muscles. It contains the thoracoabdominal nerves after they course through the transversus abdominis plane. After entering the posterior rectus sheath, they then give off perforating anterior cutaneous branches to the midline abdominal wall. Of note, this arrangement is only present above the arcuate line which is located just caudal to the umbilicus. Below the arcuate line there is no posterior rectus sheath and as such the thoracoabdominal nerves perhaps course anterior to the rectus muscle. The classic technique of injecting into the layer posterior to the rectus abdominis muscle will likely not anesthetize the nerves below the arcuate line and thus does not provide a reliable block.67
Technique
A linear transducer scans above the umbilicus to visualize the oval-shaped rectus abdominis muscles. Below the rectus abdominis are two hyperechoic lines, the upper line being the posterior rectus sheath and the lower being the peritoneum (Figure 2F). A needle is inserted in-plane towards the space between the two, ideally at the lateral third of the rectus muscle to anesthetize the thoracoabdominal nerve before it perforates the rectus muscle. Local anesthetic is injected into the space with downward depression of the peritoneum.67
Efficacy in Cesarean Analgesia
Few studies have assessed the efficacy of analgesia of the rectus sheath block in cesarean section with a low Pfannenstiel incision. Efficacy in vertical incision is outside of the scope of this manuscript. An RCT comparing rectus sheath block to controls in the absence of neuraxial morphine did not reveal a significant difference in pain scores nor a reduction in 24-hour opioid consumption, raising concern that rectus sheath block may be ineffective at providing analgesia for this procedure. This same RCT compared rectus sheath block to TAP block and demonstrated a significant reduction in total opioid consumption as well as post-operative pain scores in the TAP block group.68
Stratify with Intrathecal Morphine
A 2020 trial randomized 131 women undergoing neuraxial anesthesia for cesarean section to one of three groups, either receiving both neuraxial morphine and a rectus sheath block with bupivacaine (M+RS+), neuraxial morphine and a rectus sheath block with saline (M+RS-), or a rectus sheath block with bupivacaine without neuraxial morphine (M-RS+). Notably, the rectus sheath blocks were performed under direct visualization by the surgeon. Intrathecal morphine appeared to have improved both resting and dynamic post-operative pain scores regardless of whether the patient received a rectus sheath block with bupivacaine or saline. No analgesic benefit was demonstrated comparing the rectus sheath bupivacaine to rectus sheath saline in the presence of neuraxial morphine.69
Local Wound Infiltration Analgesia
Technique
The surgeon at the close the procedure can inject local anesthetic directly into the surgical field in a location at his or her discretion, there is no one standard location for this technique. The surgeon can decide to place the local anesthetic deep to the rectus fascia, within the plane between the subcutaneous tissue and the rectus fascia, or solely infiltrate the subcutaneous tissue. Additionally, the surgeon can decide to do a single injection or place an indwelling catheter in the plane they choose to continually infuse local anesthetic.28
Efficacy in Cesarean Analgesia
Both TAP blocks and local wound infiltration, whether by single shot or continuous catheter technique, have been shown to decrease 24-hour opioid consumption and provide significant analgesia when compared to control in the absence of neuraxial opioid.58,59,70 However, a meta-analysis of 42 RCTs comparing TAP to wound infiltration and wound catheter found no statistically significant difference in 24-hr opioid consumption, 24-hour pain scores, or time to first supplementary analgesic between the two techniques.63 A second meta-analysis reproduced the same results; TAP blocks may have small to no significant advantage in post-operative pain reduction when compared to wound infiltration of local anesthetic by a surgeon.64 Separately, one RCT found that continuous wound catheter infiltration with ropivacaine did not provide any reduction in pain scores or post-operative opioid consumption when compared to a control who had continuous wound catheter infiltration with saline.71
Stratify with Intrathecal Morphine
An RCT comparing 24-hour opioid requirements and pain scores between patients who received intrathecal morphine compared to those receiving continuous wound infiltration with ropivacaine found a significant reduction in post-operative opioid use in the first 24 hours in the intrathecal morphine group.71 More data is needed to expand on their conclusion which suggests intrathecal morphine is superior to continuous wound infiltration of local anesthetic for post-cesarean analgesia.
Discussion
The goal of this review is to exam the current state of the literature on peripheral nerve block techniques on post-operative analgesia in patients who underwent low-transverse cesarean section, with the understanding that meta-analysis is nearly impossible due to the high data heterogenicity in emerging nerve blocks. Specifically, we aim to compare the gold standard, neuraxial morphine, to the various available regional blocks and assess the efficacy and safety of each block in the presence and absence of neuraxial morphine (Table 3).
 |
Table 3 Overview of Regional Anesthesia in Cesarean Delivery: RCT, Systemic Review and Meta-Analysis |
Nearly all the literature currently available directly comparing neuraxial morphine and individual regional anesthetics favors neuraxial morphine for post-operative analgesia, regardless of the peripheral nerve technique used. In fact, much of the literature demonstrates no significant analgesic benefit to peripheral blocks when placed in conjunction with neuraxial morphine. The largest meta-analysis to date on the subject suggests that only one peripheral nerve block in conjunction with neuraxial morphine provides additional analgesic effect than neuraxial morphine alone: a combination of ilioinguinal and anterior TAP blocks. Newer data from individual RCTs that have yet to be reproduced suggest other blocks may provide some analgesic benefit, one supporting low thoracic ESPB and one supporting posterior QLB. All of these findings are in support of the 2021 PROSPECT guidelines for analgesia for elective cesarean section,74 namely the use neuraxial morphine when able or, if unable, appropriate regional nerve block would be indicated.
Most of the regional anesthetic techniques have been reliably shown to provide some amount of analgesic benefit to the patient compared to placebo in the absence of neuraxial morphine, with TAP being the most used regional anesthesia technique. Comparing the emerging QLB with TAP blocks, while many individual RCTs have demonstrated analgesic benefit to all three QL block techniques over the TAPs block, the largest meta-analysis available comparing the two refutes this finding. When comparing the QL techniques against each other, the newest technique, the anterior QL block, appears superior in its ability to decrease post-cesarean pain and opioid consumption. Though ESPB is much less studied, preliminary data suggests it may have an analgesic benefit over TAPs block. It appears, perhaps unsurprisingly, the closer to the spinal nerve root and/or sympathetic trunk that the block occurs, the better the analgesic benefit (Figure 1). Additionally, the stepwise difference in analgesic benefit is more noticeable the further apart the blocks are from each other. These new trends from our literature review calls for confirmational studies.
Despite the possible benefits of the regional techniques closer to the spinal nerve root such as the anterior QLB and ESPB, their associated technical difficulty along with the challenge of turning a patient lateral or prone immediately following open abdominal surgery under either neuraxial or general anesthesia presents numerous risks and logistic challenges that need to be carefully assessed. It is possible that even if strong evidence were to emerge favoring these blocks, TAP blocks may continue to be routinely performed for post-cesarean analgesia in part due to the lower complexity in placing them – the anatomy is less nuanced, and they are readily performed in the supine position.
There are limitations in this review. First, existing study protocol heterogenicity (block techniques, local anesthetics and their dosing and concentration, adjuvants, multimodal analgesia components, etc.) made it impossible to draw reliable conclusions regarding the effectiveness of individual nerve block techniques, particularly the emerging peripheral nerve blocks, both in the presence and absence of neuraxial morphine. The purpose of this literature review is therefore to guide clinical decision making in evidence-based practice based on a review of available data, which is limited in quantity and heterogenous in study design. Continuous data accumulation would make a systemic review and/or meta-analysis meaningful in the near future. Additionally, there is sparse data on continuous regional catheters in this population; investigation of continuous peripheral nerve catheter infusions may prolong the benefit of regional anesthetics beyond that provided by neuraxial morphine and reveal an analgesic benefit to the blocks that does not exist with single shot regional anesthetics. Furthermore, few studies explored the clinical relevance of the statistical significance observed. Does a statistically significant reduction in pain scores or opioid requirement equate to a clinically significant finding that justifies the risks of performing regional anesthesia? Future studies on the short- and long-term effects of single injection or continuous peripheral nerve block with or without adjuvants in cesarean delivery could offer some directions.
Regardless of the anesthetic or the components of the multimodal analgesic chosen to perform a cesarean delivery, there remains a high incidence of postoperative pain and persistent post surgical pain after cesarean section. In fact, inadequate postoperative pain control is a leading cause of poor patient satisfaction after cesarean delivery.75 Sufficient pain control in this population is critical as it facilitates maternal–fetal bonding and leads to lower incidence of postpartum depression and maternal mortality.5,6 While ERAS protocols aim to address this outcome, more data is required to draw a definitive conclusion on the utility of and preferred technique for regional anesthesia in this patient population.
Conclusion
Neuraxial morphine continues to be the gold standard for post-cesarean section analgesia. The short-term benefits of performing a single injection regional anesthetic in patients who have already received neuraxial morphine may not be substantial regardless of the technique or location of the peripheral nerve block. In cases where neuraxial opioids have not or cannot be given, there is overwhelming evidence to support that regional anesthetic techniques can improve post-cesarean section analgesia and decrease opioid consumption immediately post-operative. TAP blocks currently have the largest amount of evidence to support their use, while evidence for better analgesic efficacy from emerging more central fascia plane blocks such as anterior QL and ESP blocks continues to accumulate.
Disclosure
The authors report no conflicts of interest in this work.
References
1. CDC. FastStats - Births - Method of Delivery. US Dept of Health and Human Services; 2022. Available from: https://www.cdc.gov/nchs/fastats/delivery.htm.
2. Mhyre JM, Sultan P. General anesthesia for cesarean delivery occasionally essential but best avoided. Anesthesiology. 2019;130(6):864–866. doi:10.1097/ALN.0000000000002708
3. Ring L, Landau R, Delgado C. The current role of general anesthesia for cesarean delivery. Curr Anesthesiol Rep. 2021;11(18):18–27. doi:10.1007/S40140-021-00437-6
4. Guglielminotti J, Landau R, Li G. Adverse events and factors associated with potentially avoidable use of general anesthesia in cesarean deliveries. Anesthesiology. 2019;130(6):912–922. doi:10.1097/ALN.0000000000002629
5. Riley ET. Regional anesthesia for cesarean section. Tech Reg Anesth Pain Manag. 2003;7:204–12. doi:10.1053/S1084-208X(03)00038-7
6. Bolla D, Schöning A, Drack G, Hornung R. Technical aspects of the cesarean section. Gynecol Surg. 2010;7(2):127–132. doi:10.1007/S10397-010-0560-9/METRICS
7. Caughey AB, Shipp TD, Repke JT, Zelop CM, Cohen A, Lieberman E. Rate of uterine rupture during a trial of labor in women with one or two prior cesarean deliveries. Am J Obstet Gynecol. 1999;181:872–876. doi:10.1016/S0002-9378(99)70317-0
8. Oliver J, Zeballos JL. Essential clinical anesthesia review: keywords, questions and answers for the boards. Spinal Anesthesia. 2022:187–189. doi:10.1017/CBO9781139584005.058
9. McDonnell NJ, Keating ML, Muchatuta NA, Pavy TJG, Paech MJ. Analgesia after caesarean delivery. Anaesth Intensive Care. 2009;37(4):539–551. doi:10.1177/0310057X0903700418
10. Jelinek LA, Scharbach S, Kashyap S, Ferguson T. Anatomy, Abdomen and Pelvis: Anterolateral Abdominal Wall Fascia. StatPearls; 2022.
11. Ameer MA, Fagan SE, Sosa-Stanley JN, Peterson DC. Anatomy, Abdomen and Pelvis: Uterus. StatPearls; 2022.
12. Tsen LC. Anesthesia for obstetric care and gynecologic surgery. In: Longnecker DE, Mackey SC, Newman MF, Sandberg WS, Zapol WM, editors. Anesthesiology, 3e. New York, NY: McGraw-Hill Education; 2017.
13. Ultrasound Imaging of the Lumbar Spine for Central Neuraxial Blocks | Atlas of Sonoanatomy for Regional Anesthesia and Pain Medicine | AccessAnesthesiology | McGraw Hill Medical. Available from: https://accessanesthesiology.mhmedical.com/content.aspx?bookid=2220§ionid=171517099.
14. Chou R, Gordon DB, De Leon-Casasola OA, et al. Management of postoperative pain: a clinical practice guideline from the American Pain Society, the American Society of Regional Anesthesia and Pain Medicine, and the American Society of Anesthesiologists’ Committee on Regional Anesthesia, Executive Committee, and Administrative Council. J Pain. 2016;17(2):131–157. doi:10.1016/J.JPAIN.2015.12.008
15. Bonnet M-P, Mignon A, Mazoit J-X, Ozier Y, Marret E. Analgesic efficacy and adverse effects of epidural morphine compared to parenteral opioids after elective caesarean section: a systematic review. Eur J Pain. 2010;14(9):e1–894. doi:10.1016/J.EJPAIN.2010.03.003
16. Lim Y, Lim Y, Jha S, Sia AT, Rawal N. Morphine for post-caesarean section analgesia: intrathecal, epidural or intravenous? Singapore Med J. 2005;46:392.
17. Carvalho B, Butwick AJ. Postcesarean delivery analgesia. Best Pract Res Clin Anaesthesiol. 2017;31:69–79. doi:10.1016/J.BPA.2017.01.003
18. Tamura T, Yokota S, Ando M, Kubo Y, Nishiwaki K. A triple-blinded randomized trial comparing spinal morphine with posterior quadratus lumborum block after cesarean section. Int J Obstet Anesth. 2019;40:32–38. doi:10.1016/J.IJOA.2019.06.008
19. Pangthipampai P, Dejarkom S, Poolsuppasit S, Luansritisakul C, Tangchittam S. Bilateral posterior quadratus lumborum block for pain relief after cesarean delivery: a randomized controlled trial. BMC Anesthesiol. 2021;21(1). doi:10.1186/S12871-021-01309-6
20. Hussain N, Brull R, Weaver T, Zhou M, Essandoh M, Abdallah FW. Postoperative analgesic effectiveness of quadratus lumborum block for cesarean delivery under spinal anesthesia. Anesthesiology. 2021;134(1):72–87. doi:10.1097/ALN.0000000000003611
21. Huang JY, Wang LZ, Chang XY, Xia F. Impact of transversus abdominis plane block with bupivacaine or ropivacaine versus intrathecal morphine on opioid-related side effects after cesarean delivery: a meta-analysis of randomized controlled trials. Clin J Pain. 2021;38(3):231–239. doi:10.1097/AJP.0000000000001014
22. Dereu D, Savoldelli GL, Mercier Y, Combescure C, Mathivon S, Rehberg B. The impact of a transversus abdominis plane block including clonidine vs. intrathecal morphine on nausea and vomiting after caesarean section: a randomised controlled trial. Eur J Anaesthesiol. 2019;36(8):575–582. doi:10.1097/EJA.0000000000001013
23. Habib AS, Nedeljkovic SS, Horn JL, et al. Randomized trial of transversus abdominis plane block with liposomal bupivacaine after cesarean delivery with or without intrathecal morphine. J Clin Anesth. 2021:75. doi:10.1016/J.JCLINANE.2021.110527.
24. El-Boghdadly K, Desai N, Halpern S, et al. Quadratus lumborum block vs. transversus abdominis plane block for caesarean delivery: a systematic review and network meta-analysis. Anaesthesia. 2021;76(3):393–403. doi:10.1111/ANAE.15160
25. Tan H, Sen Taylor C, Weikel D, Barton K, Habib AS. Quadratus lumborum block for postoperative analgesia after cesarean delivery: a systematic review with meta-analysis and trial-sequential analysis. J Clin Anesth. 2020;67. doi:10.1016/J.JCLINANE.2020.110003
26. Hadzic A. Chapter 36: Paravertebral Block. In: Hadzic’s Peripheral Nerve Blocks and Anatomy for Ultrasound-Guided Regional Anesthesia, 3e. New York, NY: McGraw-Hill; 2021.
27. Hadzic A. Chapter 21: Lumbar Plexus Block. In: Hadzic’s Peripheral Nerve Blocks and Anatomy for Ultrasound-Guided Regional Anesthesia, 3e. New York, NY: McGraw-Hill; 2021.
28. Mitchell KD, Smith CT, Mechling C, Wessel CB, Orebaugh S, Lim G. A review of peripheral nerve blocks for cesarean delivery analgesia. Reg Anesth Pain Med. 2019;45(1):52–62. doi:10.1136/RAPM-2019-100752
29. Patnaik R, Chhabra A, Subramaniam R, et al. Comparison of paravertebral block by anatomic landmark technique to ultrasound-guided paravertebral block for breast surgery anesthesia: a randomized controlled trial. Reg Anesth Pain Med. 2018;43(4):385–390. doi:10.1097/AAP.0000000000000746
30. Seidel R, Wree A, Schulze M. Thoracic-paravertebral blocks: comparative anatomical study with different injection techniques and volumes. Reg Anesth Pain Med. 2020;45(2):102–106. doi:10.1136/RAPM-2019-100896
31. Hadzic A. Chapter 37: Erector Spinae Plane Block. In: Hadzic’s Peripheral Nerve Blocks and Anatomy for Ultrasound-Guided Regional Anesthesia, 3e. New York, NY: McGraw-Hill; 2021.
32. Chin KJ, El-Boghdadly K. Mechanisms of action of the erector spinae plane (ESP) block: a narrative review. Can J Anaesth. 2021;68(3):387–408. doi:10.1007/S12630-020-01875-2
33. Elkoundi A, Zemmouri A, Najout H, Bensghir M. Erector spinae plane block for rescue analgesia following caesarean delivery. Anaesthesiol Intensive Ther. 2021;53(3):277–278. doi:10.5114/AIT.2021.103514
34. Aygun H, Ozturk NK, Ugur M, et al. Evaluation of ultrasound-guided bilateral low thoracic erector spinae plane block for postoperative analgesia in cesarean delivery patients: a prospective, randomized, controlled clinical trial. Braz J Anesthesiol. 2022;72(4):444–449. doi:10.1016/J.BJANE.2021.07.032
35. Dostbil A, Ince I, Altinpulluk EY, et al. Analgesic effect of erector spinae plane block after cesarean section: a randomized controlled trial. Niger J Clin Pract. 2023;26(2):153–161. doi:10.4103/NJCP.NJCP_1636_21
36. Ribeiro Junior IDV, Carvalho VH, Brito LGO. Erector spinae plane block for analgesia after cesarean delivery: a systematic review with meta-analysis. Braz J Anesthesiol. 2022;72(4):506–515. doi:10.1016/J.BJANE.2021.09.015
37. Malawat A, Verma K, Jethava D, Jethava D. Erector spinae plane block and transversus abdominis plane block for postoperative analgesia in cesarean section: a prospective randomized comparative study. J Anaesthesiol Clin Pharmacol. 2020;36(2):201–206. doi:10.4103/JOACP.JOACP_116_19
38. Boules ML, Goda AS, Abdelhady MA, Abu El SA, El-Azeem NA, Hamed MA. Comparison of analgesic effect between erector spinae plane block and transversus abdominis plane block after elective cesarean section: a prospective randomized single-blind controlled study. J Pain Res. 2020;13:1073–1080. doi:10.2147/JPR.S253343
39. Priya TK, Singla D, Talawar P, Sharma RS, Goyal S, Purohit G. Comparative efficacy of quadratus lumborum type-II and erector spinae plane block in patients undergoing caesarean section under spinal anaesthesia: a randomised controlled trial. Int J Obstet Anesth. 2023;53. doi:10.1016/J.IJOA.2022.103614
40. Bakshi A, Srivastawa S, Jadon A, Mohsin K, Sinha N, Chakraborty S. Comparison of the analgesic efficacy of ultrasound-guided transmuscular quadratus lumborum block versus thoracic erector spinae block for postoperative analgesia in caesarean section parturients under spinal anaesthesia-A randomised study. Indian J Anaesth. 2022;
41. Hamed MA, Yassin HM, Botros JM, Abdelhady MA. Analgesic efficacy of Erector spinae plane block compared with intrathecal morphine after elective cesarean section: a prospective randomized controlled study. J Pain Res. 2020;13:597–604. doi:10.2147/JPR.S242568
42. Elsharkawy H, El-Boghdadly K, Barrington M. Quadratus Lumborum Block: anatomical Concepts, Mechanisms, and Techniques. Anesthesiology. 2019;130(2):322–335. doi:10.1097/ALN.0000000000002524
43. Hadzic A. Chapter 40: Quadratus Lumborum Blocks. In: Hadzic’s Peripheral Nerve Blocks and Anatomy for Ultrasound-Guided Regional Anesthesia, 3e. New York, NY: McGraw-Hill; 2021.
44. Krohg A, Ullensvang K, Rosseland LA, Langesæter E, Sauter AR. The analgesic effect of ultrasound-guided quadratus lumborum block after cesarean delivery: a randomized clinical trial. Anesth Analg. 2018;126(2):559–565. doi:10.1213/ANE.0000000000002648
45. Mieszkowski MM, Mayzner-Zawadzka E, Tuyakov B, et al. Evaluation of the effectiveness of the Quadratus Lumborum Block type I using ropivacaine in postoperative analgesia after a cesarean section - a controlled clinical study. Ginekol Pol. 2018;89(2):89–96. doi:10.5603/GP.A2018.0015
46. Blanco R, Ansari T, Girgis E. Quadratus lumborum block for postoperative pain after caesarean section: a randomised controlled trial. Eur J Anaesthesiol. 2015;32(11):812–818. doi:10.1097/EJA.0000000000000299
47. Hansen CK, Dam M, Steingrimsdottir GE, et al. Ultrasound-guided transmuscular quadratus lumborum block for elective cesarean section significantly reduces postoperative opioid consumption and prolongs time to first opioid request: a double-blind randomized trial. Reg Anesth Pain Med. 2019;44(9):896–900. doi:10.1136/RAPM-2019-100540
48. Koksal E, Aygun H, Genç C, Kaya C, Dost B. Comparison of the analgesic effects of two quadratus lumborum blocks (QLBs), QLB type II vs QLB type III, in caesarean delivery: a randomised study. Int J Clin Pract. 2021;75(10). doi:10.1111/IJCP.14513
49. Yetik F, Yilmaz C, Karasu D, Haliloǧlu Dastan N, Dayioǧlu M, Ç B. Comparison of ultrasound-guided quadratus lumborum block-2 and quadratus lumborum block-3 for postoperative pain in cesarean section: a randomized clinical trial. Medicine. 2022;
50. Blanco R, Ansari T, Riad W, Shetty N. Quadratus lumborum block versus transversus abdominis plane block for postoperative pain after cesarean delivery: a randomized controlled trial. Reg Anesth Pain Med. 2016;41(6):757–762. doi:10.1097/AAP.0000000000000495
51. Benedicta R, Jain M, Dixit N, Shivappagoudar V. The efficacy of ultrasound-guided transversus abdominis plane block versus quadratus lumborum block for postoperative analgesia in lower-segment cesarean section with low-dose bupivacaine: a randomized controlled trial. Anesth Essays Res. 2022;16(203). doi:10.4103/AER.AER_84_22
52. Khanna S, Krishna Prasad GV, Sharma VJ, Biradar M, Bhasin D. Quadratus lumborum block versus transversus abdominis plane block for post Caesarean analgesia: a randomized prospective controlled study. Med J Armed Forces India. 2022;
53. Faiz SHR, Alebouyeh MR, Derakhshan P, Imani F, Rahimzadeh P, Ghaderi Ashtiani M. Comparison of ultrasound-guided posterior transversus abdominis plane block and lateral transversus abdominis plane block for postoperative pain management in patients undergoing cesarean section: a randomized double-blind clinical trial study. J Pain Res. 2018;11:5–9. doi:10.2147/JPR.S146970
54. Borys M, Zamaro A, Horeczy B, et al. Quadratus Lumborum and Transversus Abdominis Plane Blocks and Their Impact on Acute and Chronic Pain in Patients after Cesarean Section: a Randomized Controlled Study. Int J Environ Res Public Health. 2021. doi:10.3390/IJERPH18073500
55. Salama ER. Ultrasound-guided bilateral quadratus lumborum block vs. intrathecal morphine for postoperative analgesia after cesarean section: a randomized controlled trial. Korean J Anesthesiol. 2020;73(2):121–128. doi:10.4097/KJA.D.18.00269
56. Hadzic A. Chapter 38: Transversus abdominis plane blocks. In: Hadzic’s Peripheral Nerve Blocks and Anatomy for Ultrasound-Guided Regional Anesthesia, 3e. New York, NY: McGraw-Hill; 2021.
57. Tsai HC, Yoshida T, Chuang TY, et al. Transversus abdominis plane block: an updated review of anatomy and techniques. Biomed Res Int. 2017;2017:1–12. doi:10.1155/2017/8284363
58. Wang P, Chen X, Chang Y, Wang Y, Cui H. Analgesic efficacy of ultrasound-guided transversus abdominis plane block after cesarean delivery: a systematic review and meta-analysis. J Obstet Gynaecol Res. 2021;47(9):2954–68. doi:10.1111/JOG.14881
59. Mishriky BM, George RB, Habib AS. Transversus abdominis plane block for analgesia after Cesarean delivery: a systematic review and meta-analysis. Can J Anaesth. 2012;59(8):766–778. doi:10.1007/S12630-012-9729-1
60. Ryu C, Choi GJ, Jung YH, Baek CW, Cho CK, Kang H. Postoperative analgesic effectiveness of peripheral nerve blocks in cesarean delivery: a systematic review and network meta-analysis. J Pers Med. 2022;12(4):634. doi:10.3390/JPM12040634
61. Kupiec A, Zwierzchowski J, Kowal-Janicka J, et al. The analgesic efficiency of transversus abdominis plane (TAP) block after caesarean delivery. Ginekol Pol. 2018;89(8):421–424. doi:10.5603/GP.a2018.0072
62. Yetneberk T, Chekol B, Teshome D. The efficacy of TAP block versus ilioinguinal block for post-cesarean section pain management: a systematic review and meta-analysis. Heliyon. 2021;7(8):e07774. doi:10.1016/J.HELIYON.2021.E07774
63. Sultan P, Patel SD, Jadin S, Carvalho B, Halpern SH. Transversus abdominis plane block compared with wound infiltration for postoperative analgesia following Cesarean delivery: a systematic review and network meta-analysis. Can J Anaesth. 2020;67:1710–27. doi:10.1007/S12630-020-01818-X
64. Riemma G, Schiattarella A, Cianci S, et al. Transversus abdominis plane block versus wound infiltration for post-cesarean section analgesia: a systematic review and meta-analysis of randomized controlled trials. Int J Gynaecol Obstet. 2021;153(3):383–392. doi:10.1002/IJGO.13563
65. Yan Z-R, Chen L-J, Zhang S-J, et al. The transversus abdominis plane block in conjunction with intrathecal morphine use after cesarean section in women with severe pre-eclampsia: a randomized controlled trial. BMC Anesthesiol. 2023;23(1):100. doi:10.1186/s12871-023-02061-9
66. Nedeljkovic SS, Kett A, Vallejo MC, et al. Transversus abdominis plane block with liposomal bupivacaine for pain after cesarean delivery in a multicenter, randomized, double-blind, controlled trial. Anesth Analg. 2020;131(6):1830–1839. doi:10.1213/ANE.0000000000005075
67. Hadzic A. Chapter 39: Rectus sheath block. In: Hadzic’s Peripheral Nerve Blocks and Anatomy for Ultrasound-Guided Regional Anesthesia, 3e. New York, NY: McGraw-Hill; 2021.
68. Yörükoğlu HU, Şahin T, Kula AÖ. Transversus abdominis plane block versus rectus sheath block for postoperative pain after caesarean delivery: a randomised controlled trial. Turk J Anaesthesiol Reanim. 2023;51(1):43–48. doi:10.5152/TJAR.2023.22724
69. Lui MW, Li TKT, Lui F, Ong CYT. A randomised, controlled trial of rectus sheath bupivacaine and intrathecal bupivacaine, without or with intrathecal morphine, vs. intrathecal bupivacaine and morphine after caesarean section. Anaesthesia. 2017;72(10):1225–1229. doi:10.1111/ANAE.13998
70. Garmi G, Parasol M, Zafran N, Rudin M, Romano S, Salim R. Efficacy of single wound infiltration with bupivacaine and adrenaline during cesarean delivery for reduction of postoperative pain: a randomized clinical trial. JAMA Netw Open. 2022;5(11):e2242203. doi:10.1001/jamanetworkopen.2022.42203
71. Kainu JP, Sarvela J, Halonen P, et al. Continuous wound infusion with ropivacaine fails to provide adequate analgesia after caesarean section. Int J Obstet Anesth. 2012;21(2):119–124. doi:10.1016/J.IJOA.2011.12.009
72. Telnes A, Skogvoll E, Lonnee H. Transversus abdominis plane block vs wound infiltration in Caesarean section: a randomised controlled trial. Acta Anaesthesiol Scand. 2015;59(4):496–504. doi:10.1111/aas.12498
73. Cole J, Hughey S, Longwell J. Transversus abdominis plane block and intrathecal morphine use in cesarean section: a retrospective review. Reg Anesth Pain Med. 2019;44(11):1035–1037. doi:10.1136/rapm-2019-100483
74. Roofthooft E, Joshi GP, Rawal N, Van de Velde M; PROSPECT Working Group* of the European Society of Regional Anaesthesia and Pain Therapy and supported by the Obstetric Anaesthetists’ Association. PROSPECT guideline for elective caesarean section: updated systematic review and procedure-specific postoperative pain management recommendations. Anaesthesia 2021. 76: 5 665–680. doi:10.1111/anae.15339
75. Champaneria R, Shah L, Wilson MJ, Daniels JP. Clinical effectiveness of transversus abdominis plane (TAP) blocks for pain relief after caesarean section: a meta-analysis. Int J Obstet Anesth. 2016;28:45–60. doi:10.1016/J.IJOA.2016.07.009
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Ultrasound-Guided Quadratus Lumborum Block at the Lateral Supra-Arcuate Ligament versus Subcostal Transversus Abdominis Plane Block for Postoperative Analgesia Following Open Hepatectomy: A Randomized Controlled Trial
Mao Y, Zhao W, Hao M, Xing R, Yan M
Journal of Pain Research 2023, 16:1429-1440
Published Date: 27 April 2023
Comparison of Quadratus Lumborum Plus Modified Erector Spinae Plane Block versus Pericapsular Nerve Group Block Plus Lateral Femoral Cutaneous Block on Postoperative Analgesia and Functional Recovery in Total Hip Arthroplasty: A Retrospective Propensity Score-Matched Study
Wu X, Wang M, Du M, Wang Y, Chen X, Zhang D, Xu Y
Journal of Pain Research 2026, 19:567827
Published Date: 13 January 2026