Back to Journals » Journal of Inflammation Research » Volume 18
Combined Pan-Immune-Inflammation Value and Prognostic Nutritional Index as a Prognostic Biomarker for Colorectal Cancer Undergoing Enterectomy
Authors Chen Z, Liang L ![]() , Pan C, Ju H, Li J, Yang M, Yang J, Zhao T
, Pan C, Ju H, Li J, Yang M, Yang J, Zhao T ![]()
Received 9 October 2025
Accepted for publication 10 December 2025
Published 24 December 2025 Volume 2025:18 Pages 18039—18052
DOI https://doi.org/10.2147/JIR.S570477
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Junhao Wang
Zihao Chen,1,* Lei Liang,1,* Chenglong Pan,2,* Hongping Ju,3 Jiangyu Li,3 Man Yang,3 Jun Yang,1 Ting Zhao4
1Department of Surgical Oncology, The First Affiliated Hospital of Kunming Medical University, Kunming, Yunnan, 650032, People’s Republic of China; 2Department of Pathology, The First Affiliated Hospital of Kunming Medical University, Kunming, Yunnan, 650032, People’s Republic of China; 3School of Medicine, Kunming University, Kunming, Yunnan, 650032, People’s Republic of China; 4Department of Clinical Pharmacy, The First Affiliated Hospital of Kunming Medical University, Kunming, Yunnan, 650032, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ting Zhao, Department of Clinical Pharmacy, The First Affiliated Hospital of Kunming Medical University, Kunming, Yunnan, 650032, People’s Republic of China, Email [email protected] Jun Yang, Department of Surgical Oncology, The First Affiliated Hospital of Kunming Medical University, Kunming, Yunnan, 650032, People’s Republic of China, Email [email protected]
Background: Robust biomarkers are needed to address the prognostic heterogeneity in colorectal cancer (CRC). The pan-immune-inflammation value (PIV) and prognostic nutritional index (PNI) are biomarkers of systemic inflammation and immunonutritional status, respectively. This study aimed to develop and validate a novel combined PIV-PNI score to predict survival in CRC patients undergoing curative resection.
Methods: This study included a total of 2116 CRC patients who underwent surgical treatment. The PIV and PNI were evaluated and cut-off values were determined. The PIV-PNI value range was 0 to 2, where 2 represented high PIV (≥ 208.9) and low PNI (≤ 49.05), with high PIV or low PNI indicated by 1 and neither is represented by a 0, respectively. The Cox regression model was used to determine the independent risk factors affecting the prognosis of the patients. A nomogram based on PIV-PNI was constructed, and its performance was evaluated using the C-index, calibration curve, ROC curve, and DCA curve. Finally, the nomogram model was compared with the existing staging models.
Results: Patients with higher PIV-PNI scores had a poorer prognosis. In the multivariate analysis, it was found that the PIV-PNI score was an independent predictor for the overall survival rate and disease-free survival rate of CRC patients. The nomogram based on PIV-PNI demonstrated excellent discrimination, calibration, and clinical net benefit. The proposed nomogram performed better than other existing staging systems, as evidenced by its higher AUC value.
Conclusion: The PIV-PNI score is a potent, non-invasive prognostic biomarker. The developed nomogram facilitates accurate risk stratification, potentially guiding personalized postoperative surveillance and adjuvant therapy decisions for CRC patients.
Keywords: colorectal cancer, pan-immune inflammatory value, nutritional status indicators, intestinal resection, prognosis
Introduction
Colorectal cancer (CRC) ranks as the third most diagnosed malignancy globally and represents the second leading cause of cancer-related mortality.1 Early-stage symptoms are often nonspecific, and screening programs remain insufficiently implemented, leading to frequent diagnoses at advanced stages and a consequently unfavorable five-year survival rate among Chinese patients.2–4 Surgical resection constitutes the cornerstone of curative-intent treatment for early-stage CRC. Select patients with locally advanced disease may also achieve benefit from surgery after multidisciplinary team (MDT) assessment. Nonetheless, postoperative recurrence remains a significant concern even after radical resection. Notably, individuals with comparable clinicopathological profiles may experience divergent outcomes following uniform treatment, reflecting the profound heterogeneity of colorectal cancer.5,6 Accordingly, there is an urgent clinical need for robust biomarkers capable of precisely predicting recurrence and survival to guide personalized treatment strategies and improve prognostic management.
Accumulating evidence underscores the pivotal role of systemic inflammatory and immune status in colorectal carcinogenesis and progression.7,8 Various hematologic indices—including the neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), and systemic immune-inflammation index (SII) -have been established as prognostic biomarkers across multiple cancer types.9–11 The pan-immune inflammation value (PIV), a more recently integrated metric, has demonstrated superior discriminative capacity for outcomes in several solid malignancies.12–14 Similarly, the prognostic nutritional index (PNI), which incorporates serum albumin concentration and peripheral lymphocyte count, provides a composite measure of immunonutritional status and has been associated with survival in CRC and other cancers.15,16 Although both PIV and PNI exhibit considerable prognostic utility independently, a combined scoring system incorporating these markers has not been adequately developed or validated as a prognostic biomarker for colorectal cancer undergoing enterectomy. Therefore, this study seeks to evaluate the clinical prognostic value of a novel PIV-PNI scoring system in patients undergoing radical resection for colorectal cancer and to develop a clinically applicable risk stratification model that may inform postoperative surveillance and treatment decisions.
Materials and Methods
Patients
A total of 2116 patients who underwent radical colorectal resection for colorectal cancer at the First Affiliated Hospital of Kunming Medical University between January 2014 and June 2019 were enrolled in this study. The inclusion criteria were as follows: (1) pathologically confirmed diagnosis of colorectal cancer; (2) receipt of R0 resection, defined as complete removal of the tumor with negative microscopic margins; (3) age ≥ 18 years; and (4) availability of complete blood count testing within one week prior to surgery. Exclusion criteria included: (1) R1 or R2 resection (microscopically or macroscopically positive margins); (2) history of other malignancies; (3) concomitant acute infection, autoimmune disorder, or hematologic disease; (4) prior radiotherapy or chemotherapy; (5) Poor preoperative control of blood pressure and blood glucose levels; (6) severe postoperative complications; and (7) incomplete clinical records. This study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the Ethics Committee of the First Affiliated Hospital of Kunming Medical University (Ethics Approval No.: 124). Written informed consent was obtained from all participants prior to treatment. All patient data were handled confidentially without any intervention.
Data Collection and Definitions
Preoperative laboratory and clinical parameters were retrieved from electronic medical records, including age, sex, absolute neutrophil count, lymphocyte count, monocyte count, platelet count, and albumin level. All laboratory parameters for PIV and PNI calculation were obtained from a single routine preoperative test conducted within one week before surgery. Postoperative pathological reports were reviewed to extract data regarding tumor depth of invasion, lymph node metastasis, maximum tumor diameter, tumor differentiation, lymphovascular invasion, perineural invasion, and MMR status. The PIV was calculated as: PIV = [neutrophil count (×109/L) × platelet count (×109/L) × monocyte count (×109/L)] / lymphocyte count (×109/L). The PNI was computed as: PNI = albumin (g/L) + 5 × lymphocyte count (×109/L). A combined scoring system was constructed based on the median cut-off values for PIV and PNI. Patients were assigned 2 points for values above the PIV cut-off and below the PNI cut-off, 1 point for values above both cut-offs or between them, and 0 points for values below the PIV cut-off and above the PNI cut-off.
Follow-Up and Outcomes
Overall survival (OS) was defined as the time from surgery to death from any cancer-related cause or last follow-up. Disease-free survival (DFS) referred to the time from surgery to recurrence, progression, or death. Follow-up was conducted via telephone interviews, outpatient visits, and inpatient records.
Statistical Analysis
All statistical analyses were conducted with R software (version 4.5.1) and GraphPad Prism (version 10.10.1). Continuous variables following a normal distribution, as verified by the Shapiro–Wilk test, are presented as mean ± standard deviation; otherwise, they are reported as median with interquartile range. Categorical variables are described as frequencies and analyzed using chi-square tests. Cutoff points for the PIV and PNI were defined by their median values, while thresholds for other continuous variables, such as age and tumor size, were selected based on established clinical standards or prior studies. Prognostic factors were identified via univariate and multivariate Cox proportional hazards regression analyses. The predictive accuracy of the scoring systems was assessed using receiver operating characteristic (ROC) curves and the corresponding area under the curve (AUC). A nomogram was constructed from independent predictors in the Cox model, and its performance was evaluated through calibration plots, Harrell’s concordance index (C-index), and decision curve analysis (DCA). Patients were stratified into high-, intermediate-, and low-risk categories according to their total nomogram scores. Survival outcomes across these groups were compared with Kaplan–Meier analysis and Log rank tests. A two-sided p-value below 0.05 was deemed statistically significant.
Results
Baseline Characteristics
A total of 2,116 patients with colorectal cancer (CRC) who met the inclusion and exclusion criteria were included in this study. The patient selection process is detailed in Figure 1. As summarized in Table 1, the median age of the cohort was 62 years; 1,251 patients (59.12%) were male and 865 (40.88%) were female. Most patients were classified with TNM stage II (38.04%) or III (36.06%) disease, followed by stage I (19.61%) and stage IV (6.39%). PIV and PNI were stratified based on median values. The combined PIV-PNI score ranged from 0 to 2, with a score of 2 defined as high PIV (≥ 208.9) combined with low PNI (≤ 49.05). A score of 1 indicated either high PIV or low PNI, while a score of 0 corresponded to low PIV (< 208.9) and high PNI (> 49.05). Based on this scoring system, 682 patients (32.23%) were classified as score 0, 795 (37.57%) as score 1, and 639 (30.20%) as score 2. Higher PIV-PNI scores were associated with a significantly greater proportion of patients over 60 years of age and a higher frequency of tumors larger than 5 cm (19.06% in score 0, 29.94% in score 1, and 51.64% in score 2). The score 2 group also showed a higher prevalence of mismatch repair-deficient (dMMR) tumors (29.11% vs 24.15% in score 1 and 20.38% in score 0) and more advanced TNM stages. Conversely, lower PIV-PNI scores were associated with a lower proportion of male patients (54.69% vs 58.99% and 64.01% in scores 0, 1, and 2, respectively), better tumor differentiation (88.56% vs 87.30% and 86.23%), and lower rates of perineural invasion (37.98% vs 38.24% and 38.65%) and vascular invasion (19.59% vs 22.52% and 21.91%). Patients were randomly assigned to a training cohort (70%, n = 1,482) or a validation cohort (30%, n = 634). Chi-square tests confirmed no significant differences in baseline characteristics between the two cohorts (Supplementary Table 1).
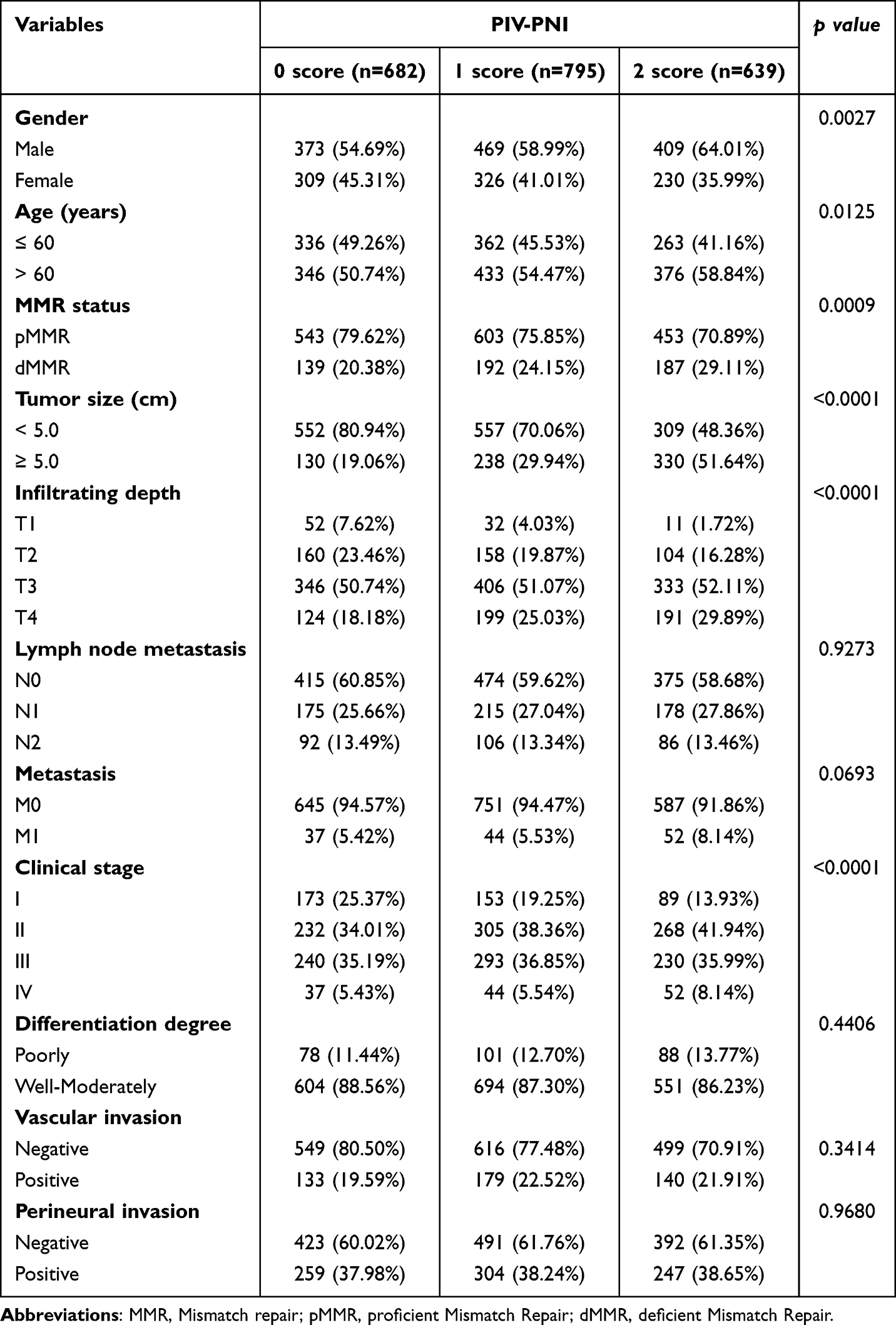 |
Table 1 The Clinical Characteristics of 2116 Patients with Colorectal Cancer |
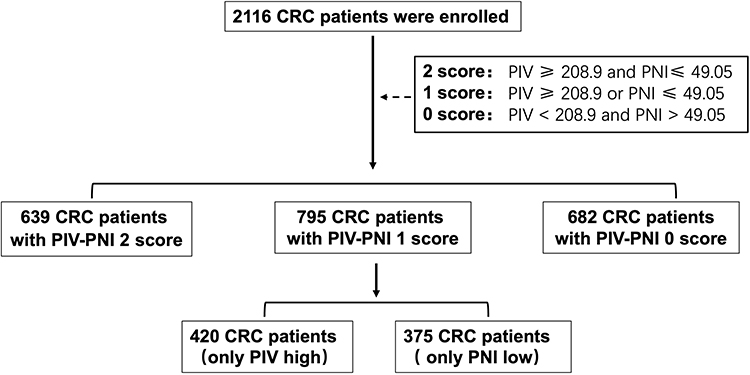 |
Figure 1 Flowchart of patient enrollment and exclusion. |
Identification of Predictive Indicators for OS and DFS
To evaluate the prognostic performance of various inflammatory and nutritional indices in predicting postoperative outcomes in colorectal cancer, receiver operating characteristic (ROC) curves were generated for overall survival (OS) and disease-free survival (DFS). The area under the curve (AUC) was calculated for the pan-immune inflammation value (PIV), prognostic nutritional index (PNI), and the combined PIV-PNI score. As illustrated in Figure 2A, the PIV-PNI score demonstrated the strongest discriminative ability for OS, achieving an AUC of 0.6451. In comparison, the AUC values for PIV and PNI alone were 0.5124 and 0.5170, respectively. Similarly, for DFS (Figure 2B), the PIV-PNI score again exhibited the highest predictive accuracy, with an AUC of 0.6059, outperforming both PIV (AUC = 0.5698) and PNI (AUC = 0.5858).
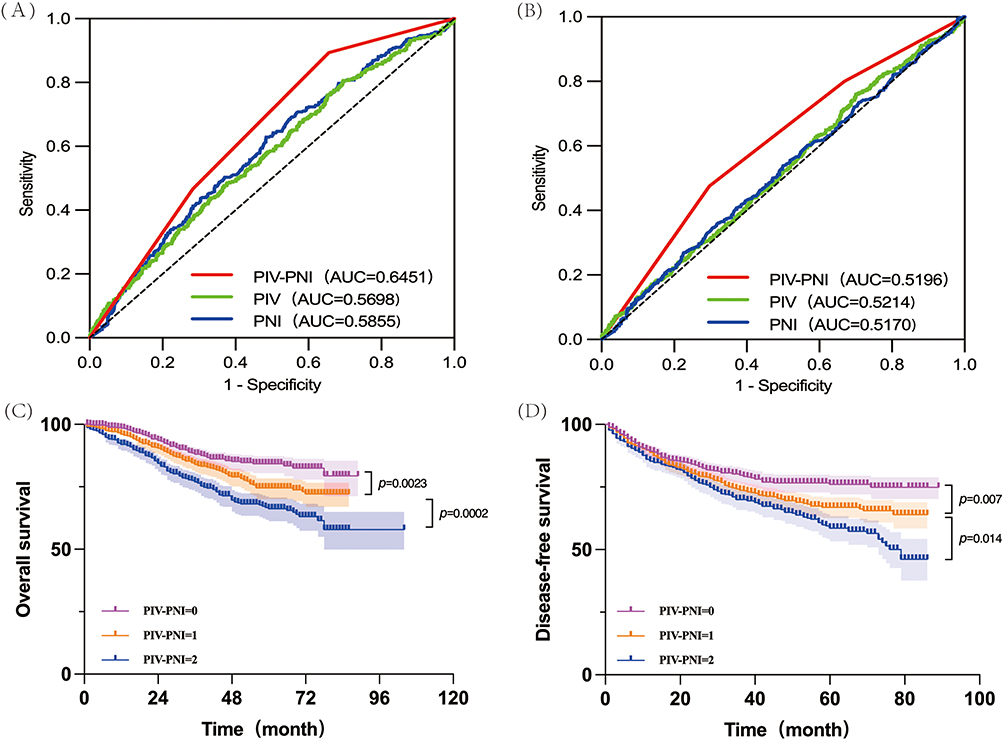 |
Figure 2 The combined PIV-PNI score serves as the optimal prognostic predictor. (A) ROC curves comparing various scoring systems for predicting overall survival. (B) ROC curves comparing various scoring systems for predicting disease-free survival. (C) Kaplan-Meier curves for overall survival stratified by the PIV-PNI score. (D) Kaplan-Meier curves for recurrence-free survival stratified by the PIV-PNI score. |
Association Between PIV-PNI Score and Prognosis
The median follow-up duration for the entire cohort was 68.7 months. The 5-year OS and DFS rates for all patients were 80.57% and 73.53%, respectively. Kaplan–Meier analysis revealed that the 5-year OS rates for patients with PIV-PNI scores of 0, 1, and 2 were 94.05%, 82.01%, and 66.27%, respectively (Figure 2C), with statistically significant differences between all groups (all p < 0.05). Similarly, the 5-year DFS rates were 84.51% for patients with a score of 0, 73.71% for those with a score of 1, and 63.05% for those with a score of 2 (Figure 2D), which also differed significantly across groups (all p < 0.05). Multivariate Cox regression analysis identified the following factors as independent predictors of OS: gender, age, depth of invasion, lymph node metastasis, distant metastasis, clinical stage, differentiation grade, type of surgical procedure, and PIV-PNI score (all p < 0.05). For DFS, independent prognostic factors included gender, tumor size, depth of invasion, distant metastasis, clinical stage, differentiation grade, type of surgical procedure, and PIV-PNI score (all p < 0.05). These results are summarized in Table 2, and the corresponding forest plots are provided in Supplementary Figures 1 and 2.
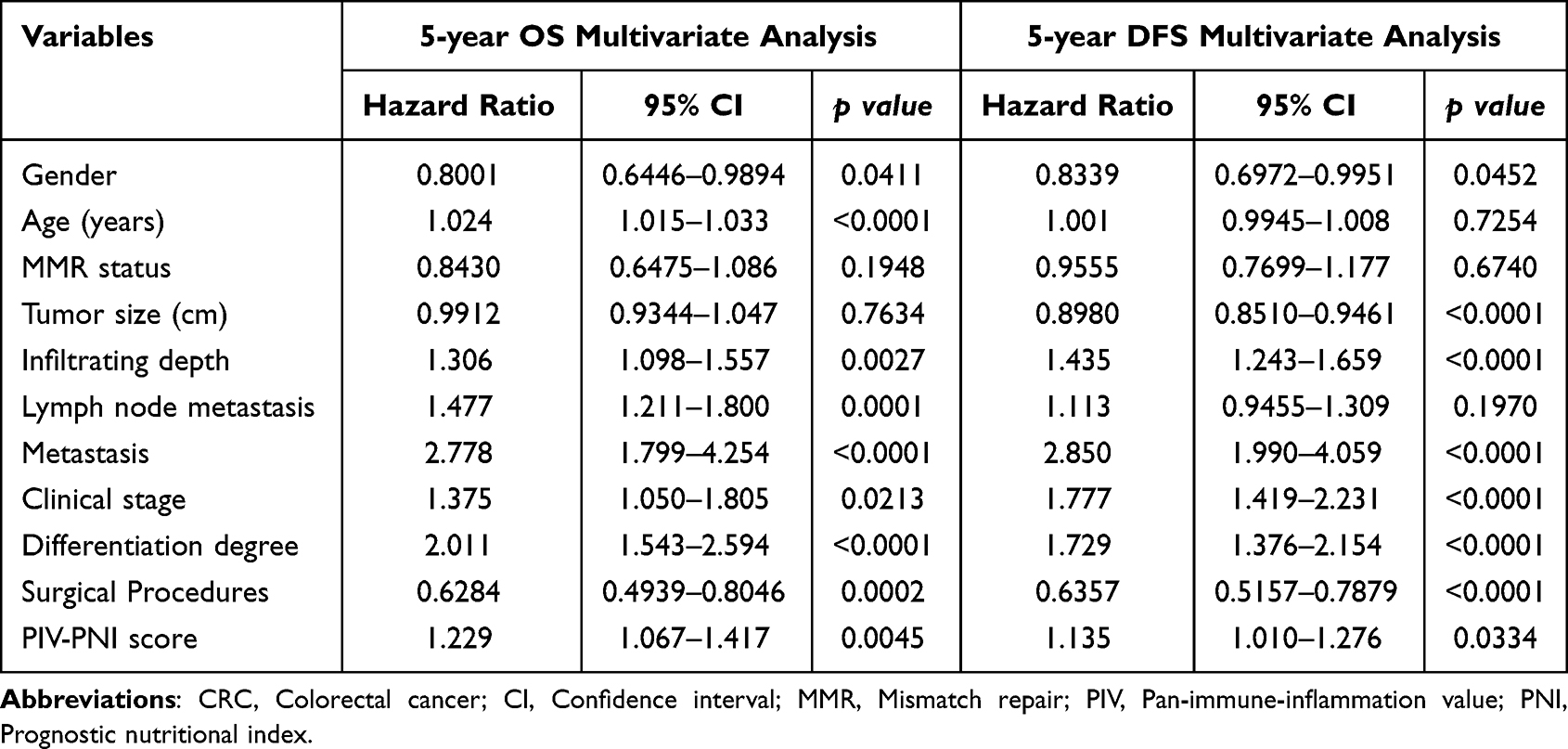 |
Table 2 Multivariate Analysis of the Clinicopathological Characteristics for the Prognosis of CRC Patients |
Model Development and Validation
Based on the independent prognostic factors identified through multivariate analysis, we constructed two comprehensive nomograms to predict 1‑, 3‑, and 5‑year OS (Figure 3A) and DFS (Figure 3B) in patients with colorectal cancer following radical resection. A key innovation of this study lies in the integration of the novel PIV-PNI score-a composite biomarker reflecting both systemic inflammatory and nutritional status-with conventional clinicopathological variables, resulting in a highly discriminative prognostic tool. The model demonstrated excellent predictive accuracy, as evidenced by bootstrap-validated C-index values. For OS, the C-index was 0.768 (95% CI: 0.739–0.797) in the training set and 0.759 (95% CI: 0.706–0.812) in the validation set. For DFS, the values were 0.755 (95% CI: 0.731–0.779) and 0.772 (95% CI: 0.729–0.814), respectively, indicating robust generalizability across cohorts. Calibration plots showed near-ideal agreement between nomogram-predicted and observed survival probabilities for both endpoints and across all timepoints (Figure 4A and B for OS; Figure 5A and B for DFS). Notably, our nomogram achieved high time-dependent AUCs for predicting survival at multiple timepoints. For OS, AUCs reached 0.818 (1-year), 0.784 (3-year), and 0.804 (5-year) in the training set, and 0.776, 0.755, and 0.781 in the validation set. Similarly, strong performance was observed for R prediction, with AUCs of 0.818, 0.766, and 0.795 (training) and 0.822, 0.774, and 0.810 (validation), underscoring the model’s consistency and reliability over time (Figure 4C and D for OS; Figure 5C and D for DFS). Decision curve analysis further confirmed the clinical utility of our model, demonstrating a significant net benefit across a wide range of threshold probabilities compared to default strategies of treating all or no patients (Figure 4E, F, 5E and F). A major innovative outcome of this study is the clinically applicable risk stratification system based on total nomogram scores, which categorized patients into three distinct risk groups with significantly differing survival outcomes (Log-rank p<0.0001; Figure 6A–D). This stratification capability enhances individualized postoperative management and supports tailored adjuvant therapy planning.
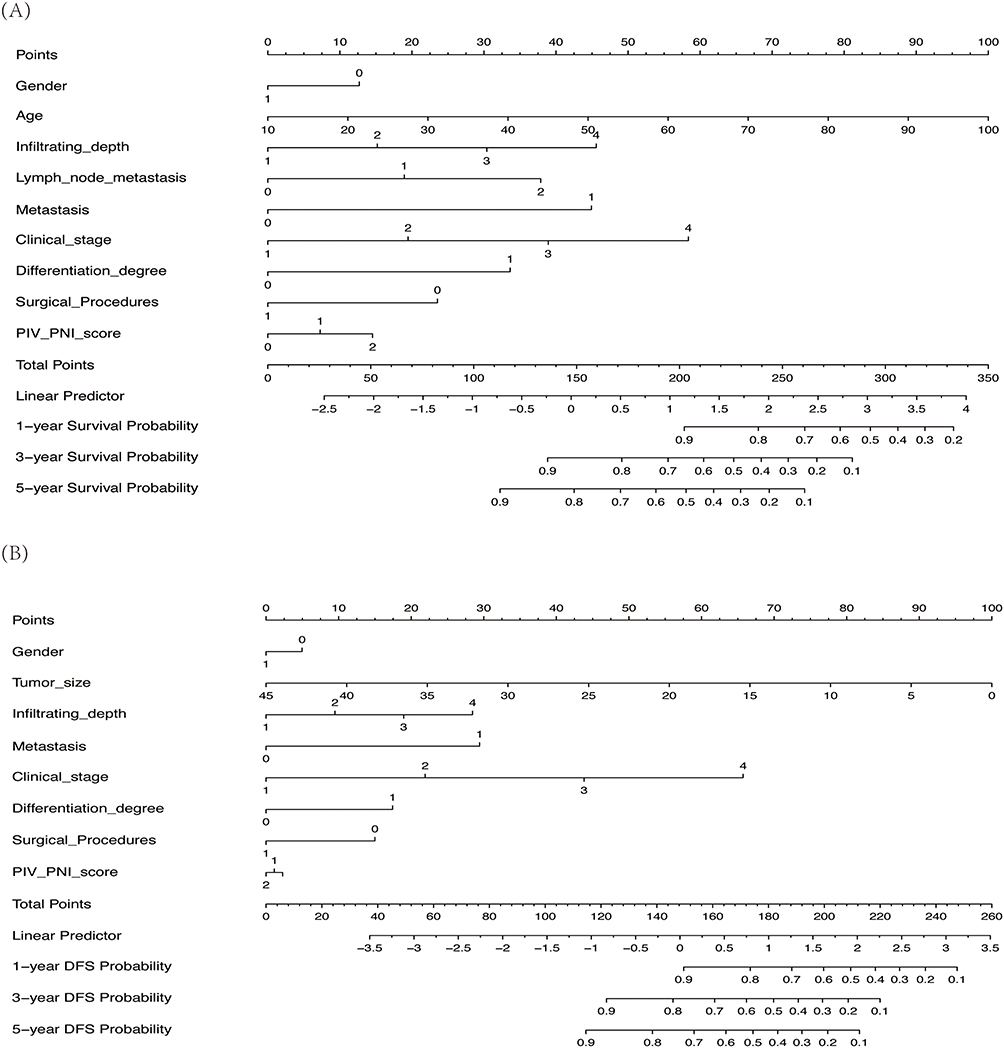 |
Figure 3 Development of prognostic nomograms. (A) Nomogram for predicting overall survival based on the PIV-PNI score. (B) Nomogram for predicting disease-free survival based on the PIV-PNI score. |
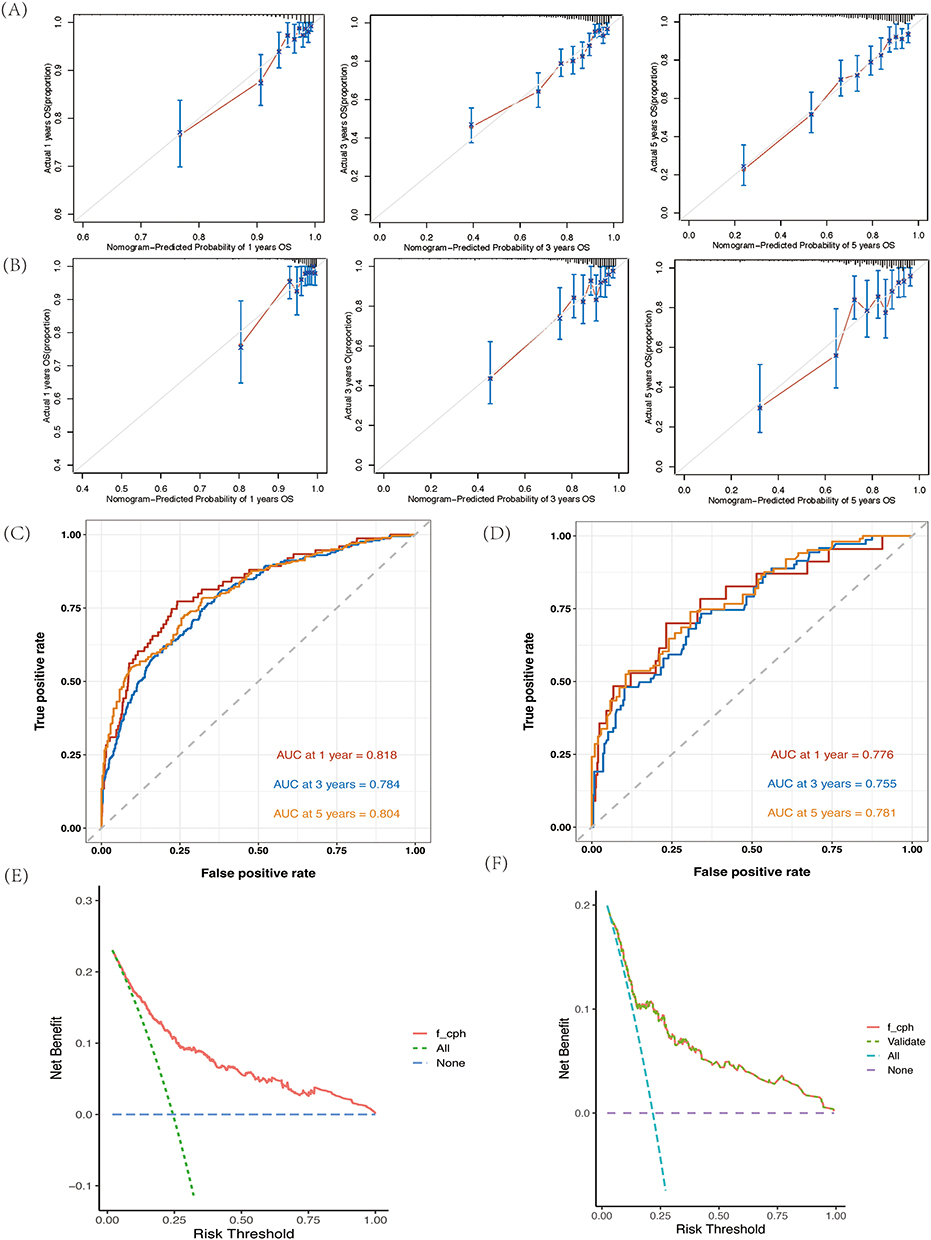 |
Figure 4 Evaluation of the nomogram for predicting overall survival. (A) Calibration curve in the training cohort. (B) Calibration curve in the validation cohort. (C) Time-dependent ROC curves in the training cohort. (D) Time-dependent ROC curves in the validation cohort. (E) Decision curve analysis (DCA) in the training cohort. (F) Decision curve analysis (DCA) in the validation cohort. |
 |
Figure 5 Evaluation of the nomogram for predicting disease-free survival. (A) Calibration curve in the training cohort. (B) Calibration curve in the validation cohort. (C) Time-dependent ROC curves in the training cohort. (D) Time-dependent ROC curves in the validation cohort. (E) Decision curve analysis (DCA) in the training cohort. (F) Decision curve analysis (DCA) in the validation cohort. |
 |
Figure 6 Risk stratification according to the nomograms. (A) Kaplan-Meier survival curves for overall survival risk groups in the training cohort. (B) Kaplan-Meier survival curves for overall survival risk groups in the validation cohort. (C) Kaplan-Meier survival curves for disease-free survival risk groups in the training cohort. (D) Kaplan-Meier survival curves for disease-free survival risk groups in the validation cohort. |
Comparison Analysis of Various Models
A comparative analysis was conducted between the proposed nomogram and established staging systems, including the American Joint Committee on Cancer (AJCC) 8th edition Tumor-Node-Metastasis (TNM) classification, Dukes staging, and MSKCC staging. The results demonstrated that the nomograms for OS and DFS exhibited superior discriminatory performance, with higher AUC values compared to all conventional staging systems (Figure 7A–D).
 |
Figure 7 Comparative assessment of predictive performance between the newly developed nomogram and conventional staging systems using ROC curves. (A) 1-year OS prediction in the training cohort. (B) 1-year OS prediction in the validation cohort. (C) 1-year DFS prediction in the training cohort. (D) 1-year DFS prediction in the validation cohort. |
Discussion
This retrospective study developed and validated a novel prognostic scoring system integrating the PIV and PNI for predicting survival outcomes in colorectal cancer (CRC) patients following intestinal resection. To our knowledge, this is the first study to establish the clinical significance of the PIV-PNI score in CRC. Our findings indicate that the PIV-PNI score serves as an independent prognostic biomarker for both OS (hazard ratio [HR]: 1.229, 95% CI: 1.067–1.417) and DFS (HR: 1.135, 95% CI: 1.010–1.276). The composite score demonstrated superior predictive performance compared to individual biomarkers, with maximum area under the curve (AUC) values of 0.6451 for OS and 0.6059 for DFS. The associated nomogram enabled effective risk stratification, categorizing patients into high-, medium-, and low-risk groups with distinct prognostic profiles. The model exhibited robust discriminative ability, with C-index values exceeding 0.66 in both training and validation cohorts. Calibration curves indicated close agreement between predicted and observed outcomes, and decision curve analysis (DCA) confirmed its clinical utility across risk strata.
CRC pathogenesis involves complex interactions between tumor cells, the host immune system and the microenvironment, where chronic inflammation plays a pivotal role.17–19 Systemic inflammatory responses are increasingly recognized as key determinants of prognosis.20,21 Although established inflammatory immune biomarkers (IIBs) such as NLR, PLR, and SII provide valuable prognostic information by reflecting immune cell balance, they remain limited in capturing the full complexity of host–tumor interactions. Recent evidence highlights the crucial role of the gut microbiota and its interplay with host immunity in shaping the systemic inflammatory landscape.22 Dysbiosis can disrupt intestinal barrier integrity, promote chronic inflammation via pathogen-associated molecular patterns, and alter local and systemic immune responses, thereby influencing cancer progression. The PIV-PNI score, by reflecting systemic inflammation and nutritional status, may indirectly capture the consequences of such microbiota-immune dysregulation. An elevated PIV and a low PNI could be the systemic manifestations of a dysregulated tumor microenvironment characterized by pro-tumorigenic microbial communities and dysfunctional immune surveillance. The tumor microenvironment in CRC is highly heterogeneous, involving pro-tumor effects mediated by neutrophils-through reactive oxygen species, cytokine release, and neutrophil extracellular traps (NETs) -and M2-type macrophages that facilitate immune suppression and angiogenesis.23–27 In contrast, lymphocytes are central to antitumor immunity, underscoring the need for composite biomarkers that reflect both inflammatory and immune status.28,29 The PIV incorporates multiple cellular components-neutrophils, platelets, monocytes, and lymphocytes-offering a more holistic representation of systemic inflammation and immune contexture.13 Elevated PIV values are associated with enhanced chronic inflammation, immunosuppression, and poorer outcomes. Recent evidence supports its prognostic value exceeding that of traditional IIBs in CRC, with potential applications in predicting neoadjuvant response, surgical complications, and nodal metastasis. Integration with PNI, which reflects nutritional and immune status, further enhances prognostic stratification. Low PNI is linked to malnutrition and impaired immune function, each independently associated with adverse outcomes. The PIV-PNI composite score thus captures complementary aspects of host response, improving risk prediction and supporting individualized treatment planning. Several mechanisms may underlie the prognostic utility of the PIV-PNI score: 1) Elevated neutrophil and/or platelet counts may promote tumor proliferation and metastasis through reactive species secretion, elastase activity, and activation of the PI3K-AKT pathway. Platelet-derived growth factors further facilitate immune evasion. 2) Lymphopenia, reflected in higher PIV-PNI scores, compromises immune surveillance and regulatory function. 3) Low serum albumin levels indicate poor nutritional status, which is correlated with diminished treatment tolerance and survival. 4) Experimental validation-such as ELISA-based assessment of PI3K-AKT pathway activation-may help confirm these hypotheses.30–34
The complexity of TME is a key determinant of treatment response. The host inflammatory-immune status, as gauged by the PIV-PNI score, is a major component of the TME. Interestingly, emerging nanomedicine strategies are designed to interact with the TME, targeting specific immune or stromal cells to reverse immunosuppression.35 Our risk stratification model could potentially identify patients who might benefit most from such innovative TME-modulating therapies. Furthermore, the PI3K/AKT/mTOR signaling pathway serves as a critical hub integrating signals from growth factors, nutrients, and inflammatory cytokines to regulate cell survival and proliferation.36,37 Chronic inflammation can constitutively activate this pathway, drive tumor progression and conferring chemotherapy resistance. Therefore, a high PIV-PNI score might not only identify high-risk patients but also imply potential susceptibility to therapies targeting the PI3K/AKT/mTOR axis, offering a rationale for future combination strategies.
The development of the PIV-PNI score aligns with the growing emphasis on integrative biomarkers in precision medicine. Current biomarker development increasingly leverages multi-omics technologies to capture disease complexity from a systemic perspective. Our score can be viewed as a readily accessible measure that reflects the systemic interplay of inflammation, immunity, and nutrition. Future studies could integrate the PIV-PNI score with molecular omics data to construct more comprehensive models. The mTOR pathway, a master regulator of cellular metabolism and growth, is a key link between the inflammatory/nutritional cues captured by our score and intracellular oncogenic signaling, further supporting its biological plausibility.38
The potential clinical utility of the PIV-PNI score extends beyond prognosis. It could inform individualized treatment decisions. For instance, high-risk patients might be candidates for more intensive postoperative surveillance to facilitate early recurrence detection. Furthermore, it raises the hypothesis of whether high-risk patients derive greater benefit from intensified or novel adjuvant therapies targeting the underlying inflammatory and nutritional vulnerabilities. While our current study cannot answer this therapeutic question, it provides a strong rationale for future prospective trials to test such intervention strategies based on PIV-PNI stratification.
Several limitations must be acknowledged. This was a single-center retrospective analysis, and despite internal validation, generalizability requires confirmation through prospective, multi-institutional studies. Although key clinical variables were adjusted for, unmeasured confounders may persist. Future research should also focus on integrating the PIV-PNI score with other promising biomarkers, such as circulating tumor DNA (ctDNA) for minimal residual disease detection, to build a more robust and multi-dimensional prognostic model that combines tumor intrinsic characteristics with host systemic factors.
Conclusions
The PIV-PNI score represents a robust and non-invasive prognostic biomarker for colorectal cancer patients after radical resection. We developed a predictive nomogram that effectively stratifies patients into distinct risk groups and demonstrates consistent performance in predicting survival outcomes. Despite the limitations of this single-center retrospective study, our findings support its potential utility in individualized prognosis evaluation and clinical decision-making. Further multi-institutional prospective studies are warranted to validate these results and explore the underlying mechanisms.
Abbreviations
CRC, Colorectal cancer; IIBs, Inflammatory immune biomarkers; PIV, Pan-immune inflammation value; PNI, Prognostic nutritional status indicators; MDT, Multidisciplinary team; NLR, Neutrophil-to-lymphocyte ratio; PLR, Platelet-to-lymphocyte ratio; SII, Systemic immune-inflammation index; OS, Overall survival; DFS, Disease-free survival; ROC, Receiver operating characteristic; AUC, Area under the curve; DCA, Decision curve analysis; AJCC, American Joint Committee on Cancer; NETs, Neutrophil extracellular traps.
Data Sharing Statement
The data of the participants on which the conclusion of this study is based (including the identification information used to support the research results) was provided by Jun Yang according to the licensing agreement and thus cannot be freely disclosed. These data are available upon request. If you wish to obtain these data, please apply to Prof Jun Yang at the Email address: [email protected].
Ethics Approval and Consent to Participate
This study was conducted with the approval of the Ethics Committee of The First Affiliated Hospital of Kunming Medical University (Approval Number: 124). All procedures were performed in accordance with the ethical standards of the responsible committee and the Declaration of Helsinki. For this research, informed consent was obtained from all participating individuals.
Author Contributions
Conceptualization: Zihao Chen, Ting Zhao; Data curation: Zihao Chen, Ting Zhao, Lei Liang; Formal analysis: Zihao Chen, Ting Zhao; Funding acquisition: Zihao Chen, Ting Zhao; Investigation: Zihao Chen, Chenglong Pan, Ting Zhao, Hongping Ju, Man Yang, Jiangyu Li, Jun Yang; Methodology: Zihao Chen, Ting Zhao, Jiangyu Li, Chenglong Pan, Jun Yang; Project administration: Zihao Chen, Ting Zhao, Hongping Ju; Resources: Zihao Chen, Ting Zhao, Hongping Ju; Software: Zihao Chen, Ting Zhao, Jiangyu Li; Supervision: Zihao Chen, Ting Zhao, Jun Yang; Validation: Zihao Chen, Ting Zhao, Chenglong Pan; Visualization: Zihao Chen, Ting Zhao; Original draft: Zihao Chen, Ting Zhao, Lei Liang, Chenglong Pan, Hongping Ju, Jiangyu Li, Man Yang; Review and editing: Ting Zhao, Zihao Chen, Jun Yang. All authors approved the final version of the paper submitted for publication, agreed to submit the paper Journal of Inflammation Research, and agreed to be accountable for the contents of the paper.
Funding
This work was supported by the Health Training Project for High-level Talents in Yunnan (Project Number: H-2024051); the Special Project for Basic Research in Yunnan (Project Numbers: 202401AU070041, 202401AU070047); the Kunming Medical University Project for Basic Research in Yunnan (Project Number: 202501AY070001-062) and Bethune Foundation (Project Number: Z04J2023E095).
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper. All authors confirm that they have no conflicts of interest to disclose regarding this study.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–263. doi:10.3322/caac.21834
2. Siegel RL, Wagle NS, Cercek A, Smith RA, Jemal A. Colorectal cancer statistics, 2023. CA Cancer J Clin. 2023;73(3):233–254. doi:10.3322/caac.21772
3. Patel SG, Karlitz JJ, Yen T, Lieu CH, Boland CR. The rising tide of early-onset colorectal cancer: a comprehensive review of epidemiology, clinical features, biology, risk factors, prevention, and early detection. Lancet Gastroenterol Hepatol. 2022;7(3):262–274. doi:10.1016/S2468-1253(21)00426-X
4. Wong CC, Yu J. Gut microbiota in colorectal cancer development and therapy. Nat Rev Clin Oncol. 2023;20(7):429–452. doi:10.1038/s41571-023-00766-x
5. Kuipers EJ, Grady WM, Lieberman D, et al. Colorectal cancer. Nat Rev Dis Primers. 2015;1:15065. doi:10.1038/nrdp.2015.65
6. Shaukat A, Levin TR. Current and future colorectal cancer screening strategies. Nat Rev Gastroenterol Hepatol. 2022;19(8):551. doi:10.1038/s41575-022-00661-3
7. Sui Q, Zhang X, Chen C, et al. Inflammation promotes resistance to immune checkpoint inhibitors in high microsatellite instability colorectal cancer. Nat Commun. 2022;13(1):7316. doi:10.1038/s41467-022-35096-6
8. Inamura K, Hamada T, Bullman S, Ugai T, Yachida S, Ogino S. Cancer as microenvironmental, systemic and environmental diseases: opportunity for transdisciplinary microbiomics science. Gut. 2022;12:gutjnl–2022–327209.
9. Nøst TH, Alcala K, Urbarova I, et al. Systemic inflammation markers and cancer incidence in the UK Biobank. Eur J Epidemiol. 2021;36(8):841–848. doi:10.1007/s10654-021-00752-6
10. Wang X, Tang X, Xu J, et al. Investigating the clinical predictive utility of inflammatory markers and nomogram development in colorectal cancer patients with malnutrition. Front Nutr. 2024;11:1442094. doi:10.3389/fnut.2024.1442094
11. Nakamoto S, Ohtani Y, Sakamoto I, Hosoda A, Ihara A, Naitoh T. Systemic immune-inflammation index predicts tumor recurrence after radical resection for colorectal cancer Tohoku. J Exp Med. 2023;261(3):229–238 doi:10.1620/tjem.2023.J074.
12. De Giorgi U, Procopio G, Giannarelli D, et al. Association of systemic inflammation index and body mass index with survival in patients with renal cell cancer treated with nivolumab. Clin Cancer Res. 2019;25(13):3839–3846. doi:10.1158/1078-0432.CCR-18-3661
13. Turan YB. The prognostic importance of the pan-immune-inflammation value in patients with septic shock. BMC Infect Dis. 2024;24(1):69. doi:10.1186/s12879-023-08963-w
14. Karacan Gölen M, Uçar Karabulut K, Kamiloğlu M, Yonar A. Pan-immune-inflammation value predicts 3-month functional outcomes in patients with acute ischemic stroke treated with mechanical thrombectomy. Brain Behav. 2025;15(3):e70397. doi:10.1002/brb3.70397
15. Raposeiras RS, Abu AE, Cespón FM, et al. Prevalence and prognostic significance of malnutrition in patients with acute coronary syndrome. J Am Coll Cardiol. 2020;76(7):828–840. doi:10.1016/j.jacc.2020.06.058
16. Jia P, Shen F, Zhao Q, et al. Association between C-reactive protein-albumin-lymphocyte (CALLY) index and overall survival in patients with colorectal cancer: from the investigation on nutrition status and clinical outcome of common cancers study. Front Immunol. 2023;14:1131496. doi:10.3389/fimmu.2023.1131496
17. Sepich-Poore GD, Zitvogel L, Straussman R, Hasty J, Wargo JA, Knight R. The microbiome and human cancer [published correction appears in Science]. Science. 2024;385(6716):eadt2260.
18. Galassi C, Chan TA, Vitale I, Galluzzi L. The hallmarks of cancer immune evasion. Cancer Cell. 2024;42(11):1825–1863. doi:10.1016/j.ccell.2024.09.010
19. de Visser KE, Joyce JA. The evolving tumor microenvironment: from cancer initiation to metastatic outgrowth. Cancer Cell. 2023;41(3):374–403. doi:10.1016/j.ccell.2023.02.016
20. Eckerling A, Ricon-Becker I, Sorski L, Sandbank E, Ben-Eliyahu S. Stress and cancer: mechanisms, significance and future directions. Nat Rev Cancer. 2021;21(12):767–785. doi:10.1038/s41568-021-00395-5
21. Jia P, Shen F, Zhao Q, et al. Association between C-reactive protein-albumin-lymphocyte index and overall survival in patients with esophageal cancer. Clin Nutr. 2025;45:212–222. doi:10.1016/j.clnu.2024.12.032
22. Lin A, Xiong M, Jiang A, et al. The microbiome in cancer. Imeta. 2025;4(5):e70070. doi:10.1002/imt2.70070
23. Li R, Liu X, Huang X, et al. Single-cell transcriptomic analysis deciphers heterogenous cancer stem-like cells in colorectal cancer and their organ-specific metastasis. Gut. 2024;73(3):470–484. doi:10.1136/gutjnl-2023-330243
24. Wu Y, Yang S, Ma J, et al. Spatiotemporal immune landscape of colorectal cancer liver metastasis at single-cell level. Cancer Discov. 2022;12(1):134–153. doi:10.1158/2159-8290
25. Qian J, Olbrecht S, Boeckx B, et al. A pan-cancer blueprint of the heterogeneous tumor microenvironment revealed by single-cell profiling. Cell Res. 2020;30(9):745–762. doi:10.1038/s41422-020-0355-0
26. Mousset A, Albrengues J. NETs unleashed: neutrophil extracellular traps boost chemotherapy against colorectal cancer. J Clin Invest. 2024;134(5):e178344. doi:10.1172/JCI178344
27. Chen J, Hou S, Liang Q, et al. Localized degradation of neutrophil extracellular traps by photoregulated enzyme delivery for cancer immunotherapy and metastasis suppression. ACS Nano. 2022;16(2):2585–2597. doi:10.1021/acsnano.1c09318
28. Pelka K, Hofree M, Chen JH, et al. Spatially organized multicellular immune hubs in human colorectal cancer. Cell. 2021;184(18):4734–4752.e20. doi:10.1016/j.cell.2021.08.003
29. Chen Y, Wang D, Li Y, et al. Spatiotemporal single-cell analysis decodes cellular dynamics underlying different responses to immunotherapy in colorectal cancer. Cancer Cell. 2024;42(7):1268–1285. doi:10.1016/j.ccell.2024.06.009
30. Antonio N, Bønnelykke-Behrndtz ML, Ward LC, et al. The wound inflammatory response exacerbates growth of pre-neoplastic cells and progression to cancer. EMBO J. 2015;34(17):2219–2236. doi:10.15252/embj.201490147
31. Tanaka Y, Ito S, Isobe K. Vancomycin-sensitive bacteria trigger development of colitis-associated colon cancer by attracting neutrophils. Sci Rep. 2016;6:23920. doi:10.1038/srep23920
32. Houghton AM, Rzymkiewicz DM, Ji H, et al. Neutrophil elastase-mediated degradation of IRS-1 accelerates lung tumor growth. Nat Med. 2010;16(2):219–223. doi:10.1038/nm.2084
33. Kitayama J, Yasuda K, Kawai K, Sunami E, Nagawa H. Circulating lymphocyte number has a positive association with tumor response in neoadjuvant chemoradiotherapy for advanced rectal cancer. Radiat Oncol. 2010;5:47. doi:10.1186/1748-717X-5-47
34. Migita K, Matsumoto S, Wakatsuki K, et al. Effect of oral nutritional supplementation on the prognostic nutritional index in gastric cancer patients. Nutr Cancer. 2021;73(11–12):2420–2427. doi:10.1080/01635581.2020.1826990
35. Chen L, Lin A, Tang B, et al. The future of cancer therapy. Nanomater Tumor Microenviron iMetaMed. 2025;e7007.
36. Li M, Fan J, Hu M, Xu J, He Z, Zeng J. Quercetin enhances 5-fluorouracil sensitivity by regulating the autophagic flux and inducing Drp-1 mediated mitochondrial fragmentation in colorectal cancer cells. Curr Mol Pharmacol. 2024;
37. Basnet R, Bahadur basnet B, Gupta R, Basnet T, Khadka S, Shan Alam M. Mammalian Target of Rapamycin (mTOR) signalling pathway–a potential target for cancer intervention: a short overview. Curr Mol Pharmacol. 2024;
38. Wu M, Wu X, Han J. KIF20A promotes CRC progression and the Warburg Effect through the C-Myc/HIF-1alpha Axis. Protein Pept Lett. 2024;31(2):107–115. doi:10.2174/0109298665256238231120093150
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
IGFBP5 is Upregulated and Associated with Poor Prognosis in Colorectal Cancer
Deng Y, Yang X, Hua H, Zhang C
International Journal of General Medicine 2022, 15:6485-6497
Published Date: 6 August 2022
Upregulation of Long Noncoding RNA MALAT1 in Colorectal Cancer Promotes Radioresistance and Aggressive Malignance
Shen W, Yu Q, Pu Y, Xing C
International Journal of General Medicine 2022, 15:8365-8380
Published Date: 28 November 2022
Fashionable, but What is Their Real Clinical Usefulness? NLR, LMR, and PLR as a Promising Indicator in Colorectal Cancer Prognosis: A Systematic Review
Misiewicz A, Dymicka-Piekarska V
Journal of Inflammation Research 2023, 16:69-81
Published Date: 7 January 2023
Screening History and 7-Year Survival in 32,099 Colorectal Cancer Patients: A Population-Based Cohort Study
Hsiao BY, Chiang CJ, Yang YW, Lin LJ, Hsu TH, Lee WC
Clinical Epidemiology 2023, 15:1009-1025
Published Date: 3 October 2023
BICDL1 Predicts Poor Prognosis and is Correlated with Methylation and Immune Infiltration in Colorectal Cancer
Luo H, Luo J, Ding N, Zhang T, He Y
Pharmacogenomics and Personalized Medicine 2023, 16:1109-1126
Published Date: 22 December 2023