Back to Journals » Neuropsychiatric Disease and Treatment » Volume 22
Changes in Anxiety Severity and Acceptability of Venlafaxine in Generalized Anxiety Disorder in the United States: Results From a Real-World Study
Authors Correll CU ![]() , Subramaniam K
, Subramaniam K ![]() , Purushottamahanti P
, Purushottamahanti P ![]() , Bayan B, Bryden LA, Palmer EOC
, Bayan B, Bryden LA, Palmer EOC ![]() , Lipunova N
, Lipunova N
Received 21 March 2026
Accepted for publication 10 June 2026
Published 9 July 2026 Volume 2026:22 608897
DOI https://doi.org/10.2147/NDT.S608897
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Roger Pinder
Christoph U Correll,1– 5 Kannan Subramaniam,6 Pradeep Purushottamahanti,7 Bituparna Bayan,8 Luke A Bryden,9 Emily OC Palmer,9 Nadia Lipunova9
1Department of Psychiatry, Zucker Hillside Hospital, Northwell Health, Glen Oaks, NY, USA; 2Department of Psychiatry and Molecular Medicine, Zucker School of Medicine at Hofstra/Northwell, Hempstead, NY, USA; 3Center for Psychiatric Neuroscience, Feinstein Institute for Medical Research, Manhasset, NY, USA; 4Department of Child and Adolescent Psychiatry, Charité Universitätsmedizin, Berlin, Germany; 5German Center for Mental Health (DZPG), Partner Site Berlin, Berlin, Germany; 6Global Medical Affairs, Viatris Inc, Auckland, New Zealand; 7Global Medical Affairs, Viatris Inc, Bangalore, Karnataka, India; 8Real-World Evidence and Outcomes Research, Viatris Inc, Bangalore, Karnataka, India; 9Real-World Evidence, Holmusk Technologies Inc, London, UK
Correspondence: Christoph U Correll, Department of Child and Adolescent Psychiatry Charité Universitätsmedizin Campus Virchow, Augustenburger Platz, Berlin, 113353, Germany, Tel +0049/30-450-566202, Fax +0049/30-450-566921, Email [email protected]
Background: Anxiety disorders, including the common generalized anxiety disorder (GAD), are among the leading causes of disability globally. Clinical practice guidelines recommend venlafaxine, a serotonin and norepinephrine reuptake inhibitor, as a first-line pharmacological treatment option for GAD.
Methods: This retrospective cohort study utilized longitudinal real-world data from the US-based database, Holmusk NeuroBlu Data, to explore anxiety severity changes following 30– 90 days of venlafaxine prescription in adults with GAD. The main outcome was change from baseline (mean and median) in the 7-item Generalized Anxiety Disorder Questionnaire (GAD-7) score, as well as clinically meaningful change (a difference of ≥ 4 points).
Results: Of 756 patients with GAD (78.6% female, 78.4% White, mean [standard deviation] age 38.5 [14.4 years]), 71.8% had a diagnosis of comorbid major depressive disorder (MDD) at baseline and 23.0% had another anxiety/phobic disorder. Median (interquartile range [IQR]) GAD-7 scores decreased significantly (P< 0.001) from 14.0 (10.0– 18.0) at baseline (− 30 to +7 days from first venlafaxine prescription) to 9.0 (5.0– 14.0) points at follow-up (30– 90 days after first venlafaxine prescription), a median (IQR) change of − 3.0 (− 8.0– 0.0), corresponding to a shift from moderate to mild anxiety severity. Stratified by baseline anxiety severity, symptom improvement was more pronounced among patients with greater baseline severity. Overall, 48.1% of patients had a clinically meaningful decrease of ≥ 4 points in GAD-7 score, while only 7.5% significantly worsened. Altogether, 63.6% of patients continued venlafaxine for ≥ 90 days after first venlafaxine prescription.
Conclusion: In this real-world cohort, improved GAD-7 scores were observed to be associated with venlafaxine prescription.
Keywords: all-cause discontinuation, anxiety disorders, effectiveness, real-world evidence, serotonin and noradrenaline reuptake inhibitor
Introduction
Anxiety disorders are one of the greatest causes of disability globally,1,2 with data from the Global Burden of Disease study (2023 update) providing an estimated global prevalence of anxiety disorders of approximately 6%.3
Generalized anxiety disorder (GAD) is one of the most common types of anxiety disorder, characterized by excessive anxiety and worry that are difficult to control, along with other symptoms, such as restlessness, feeling on edge, sleep disturbance, being easily fatigued, difficulty concentrating and irritability, not attributable to another mental, substance use or medical disorder.4 Importantly, GAD is associated with substantial impact on quality of life and frequently co-occurs with depression, insomnia, and substance use disorders.5
The two main treatment options for GAD are cognitive behavioral therapy and pharmacotherapy,6 with the selective serotonin reuptake inhibitors (SSRIs) and serotonin and norepinephrine reuptake inhibitors (SNRIs) recommended as first-line pharmacological treatment options for GAD. The SNRI venlafaxine is a guideline-recommended first-line pharmacological option,6,7 with randomized controlled trials (RCTs) demonstrating response rates of 66–69% for venlafaxine, compared with 39–46% for placebo.8–10
In patients receiving pharmacological treatment for GAD, ongoing monitoring is essential to evaluate treatment effectiveness and guide therapeutic adjustments.5,11 In RCTs, the Hamilton Anxiety Rating Scale (HAM-A) is one of the most widely used measurements for assessing GAD treatment efficacy.12,13 However, this 14-item clinician-administered format requires extended time, limiting its utility in routine practice, where brief self-report measures are preferred and more practical to use.14 One such measure is the 7-item Generalized Anxiety Disorder Questionnaire (GAD-7), which is a validated, brief, self-administered scale for measuring the frequency of and changes in anxiety symptoms.5,14,15 While the GAD-7 is a measurement tool that can be used in everyday clinical practice, use remains inconsistent across care providers.16,17
Although most real-world studies do not establish causal treatment effects, these studies are playing an increasingly important role in improving our understanding of treatment effectiveness outside clinical trial settings.18 While real-world evidence (RWE) studies using European electronic health record (EHR) datasets19 and United States (US) claims databases20,21 have described prescription patterns and healthcare costs associated with GAD, evidence gaps remain for effectiveness and patient outcomes in routine practice, where conditions differ substantially from RCT settings, including patients with comorbidities, comedications, and more severe illness burden.18 The aim of this study was to explore the changes in the severity of anxiety following venlafaxine prescription, and to explore clinical and demographic factors associated with such changes, in patients diagnosed with GAD in routine clinical practice, thereby bridging the gap between RCT efficacy data and real-world effectiveness.
Methods
Study Design and Data Source
This retrospective cohort study utilized Holmusk NeuroBlu Data (V24R5), a longitudinal behavioral health real-world database comprising structured and unstructured patient-level records from US healthcare providers (predominantly specialist care) spanning 1999 to 2024. NeuroBlu Data are deidentified at source, thus institutional review board approval was not deemed necessary for this study. NeuroBlu Data has received a waiver of authorization for analysis of de-identified healthcare data from the Western-Copernicus Group (WCG) Institutional Review Board (Ref: WCG-IRB 1–1,470,336-1).
Time-Related Variables
The overall study period was 1999–2024, with patients meeting eligibility criteria at any point within this calendar period included in the analysis. The index date was defined as the first recorded venlafaxine prescription. The baseline period was defined as a 5-week window (−30/+7days) around the index date to assess demographic and clinical characteristics of the population at the point of venlafaxine treatment initiation. A pre-index date lookback period of 90 days was used to ensure the presence of clinical activity prior to the first recorded venlafaxine prescription, increasing confidence that the index prescription reflected treatment initiation. The post-index period extended up to 150 days following venlafaxine initiation. Within this post-index period, the outcome assessment window was between 30 and 90 days (Supplementary Figure 1), a timeframe consistent with the onset of anxiolytic response to venlafaxine observed in clinical trials.8,22 The requirement for a longer post-index period than outcome assessment window was to account for gaps in prescriptions (see exposure section).
Patient Population
The population of interest was adult patients with generalized anxiety disorder and a prescription of venlafaxine. Inclusion criteria were: (1) patients aged ≥18 years at the time of first venlafaxine prescription; (2) a diagnosis record of GAD (ICD-10: F41.1 or ICD-9: 300.02) within the baseline period; (3) at least one GAD-7 assessment at baseline (−30/+7days around the index date) and one GAD assessment during the outcome assessment window (+30-90 days after the index date). In addition, all patients were required to have observable clinical data across the 150-day post-index period. Only patients where the index dose of venlafaxine was ≤75 mg were included, as doses exceeding 75mg are unlikely to represent patients with GAD newly initiating venlafaxine, given the FDA approved starting dose of 75 mg/day (with the option to start at 37.5mg for some patients for the first 4–7 days).23 Patients with psychiatric, neurodegenerative, or neurodevelopmental comorbidities, listed in Supplementary Table 1, were excluded. Individual EHR records, where data was available, were searched for exclusion diagnostic codes up to 6-months before and 6-months after the index date. It is important to note that this 12-month window represents a screening range for exclusion diagnoses rather than a mandatory data-availability requirement. Further, patients were excluded if venlafaxine was discontinued before the follow-up GAD-7 outcome assessment.
Exposure
Patients with at least one venlafaxine prescription were eligible for study inclusion. Prescriptions separated by ≤60 days were merged and considered a continuous treatment period. Treatment discontinuation was defined as a gap of >60 days between prescriptions. This approach was taken to account for the paucity of prescription end dates in EHR data; however, it should be acknowledged that this may introduce misclassification bias in exposure duration. To ensure complete capture of the treatment period and discontinuation events, patients were required to have ≥60 days of observable data following the outcome assessment window.
Outcomes
The main outcome was change in anxiety severity using GAD-7.14 Change was assessed by: a) mean and median change in total GAD-7 score, calculated as the difference between follow-up and baseline scores; and b) clinically meaningful change, defined as a difference of ≥4 points (categorized as clinically meaningful improvement [decrease of ≥4 points] and clinically meaningful worsening [increase of ≥4 points]).15 Analyses were stratified by sex and by category of baseline anxiety severity. Baseline GAD-7 severity was classified using established thresholds:14 minimal (0–4), mild (5–9), moderate (10–14), and severe (15–21).
Exploratory Analysis
To gain insight into real-world treatment acceptability, an exploratory analysis was conducted following initial data analysis to assess venlafaxine treatment discontinuation during the 30–90-day period following the index venlafaxine prescription. Discontinuation was defined as a gap of >60 days without a recorded prescription. The proportions of patients discontinuing treatment was calculated for intervals of 30 to 60 days and 61 and 90 days after the index prescription, as well as cumulatively over the full 30–90-day period. Discontinuation rates were also stratified by sex and by category of baseline anxiety severity.
Data Analysis
Continuous variables were summarized using mean and standard deviation (SD) or median and interquartile range (IQR), as appropriate. Categorical and ordinal variables were summarized using frequencies and percentages. Change in GAD-7 score from baseline to follow-up was assessed using the Wilcoxon signed-rank test, with effect size estimated using a matched-pairs rank-biserial correlation analysis, using R (version 4.3.1), effectsize package (version 1.0.1).
Multivariable logistic regression analysis was conducted to identify clinical features associated with a clinically meaningful improvement in the GAD-7 total score. Patients with a GAD-7 score of ≤3 at baseline were excluded from this responder analysis as it was not possible for them to experience the outcome of improvement of 4 points. The covariates included age (at index date), sex, index year, race, geographical region, baseline psychiatric comorbidities, baseline GAD-7 score, baseline psychiatric medication prescriptions (antidepressants, anxiolytics, antipsychotics, mood stabilizers, anticonvulsants, hypnotics or sedatives – see Supplementary Table 2 for a list of included medications), and index venlafaxine dose. Post-hoc subgroup analyses were conducted to further explore the findings of the multivariable analysis, and a sensitivity analysis was also conducted in which the baseline period was limited to −30 days to 0 day to avoid early post-treatment changes that could theoretically affect baseline GAD-7 scores. All statistical analyses were two-sided with an alpha of 0.05 and without correction for multiple comparisons.
Results
Baseline Demographics and Clinical Characteristics
Altogether, 756 patients met the eligibility criteria and were included in the study (Figure 1). The included population was predominantly female (78.6%) and white (78.4%), with a mean age at the time of the first recorded venlafaxine prescription of 38.5±14.4 years (Table 1). Most patients had moderate (32.3%) or severe (46.8%) anxiety at baseline. There were no statistically significant differences in baseline demographics between males and females (Table 1). In unadjusted between-group comparisons stratified by baseline anxiety severity, a statistically significant association was observed between baseline anxiety severity and race (P=0.023; Table 1), with higher proportions of Black or African American patients having greater anxiety severity, although sample sizes were small. Most patients in this study received their first recorded venlafaxine prescription in an outpatient (93%) or other (7%) setting (telehealth/case management), with no index prescriptions recorded in an inpatient or emergency department setting.
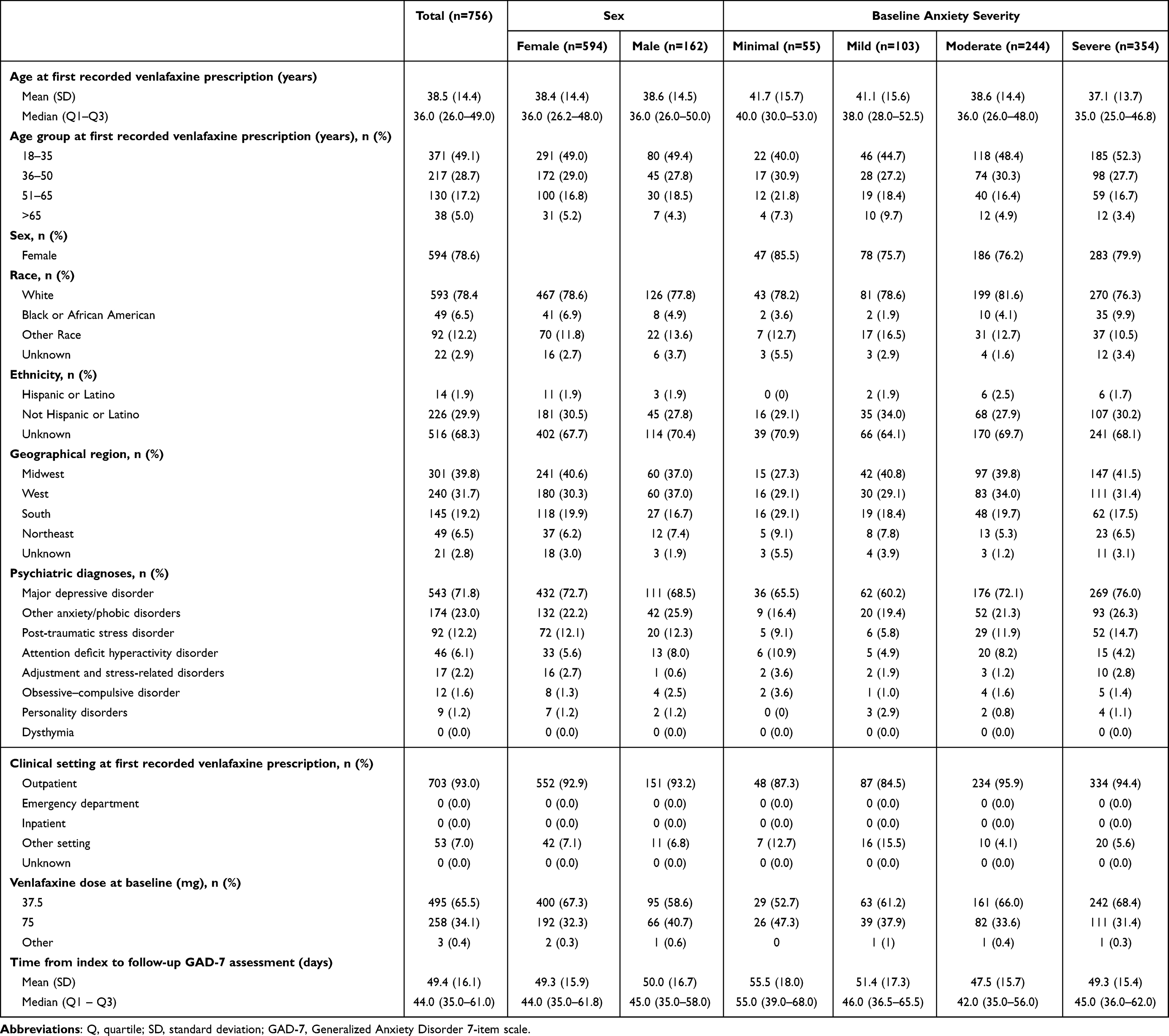 |
Table 1 Demographic and Clinical Characteristics. All Characteristics Were Recorded at Baseline Unless Stated Otherwise |
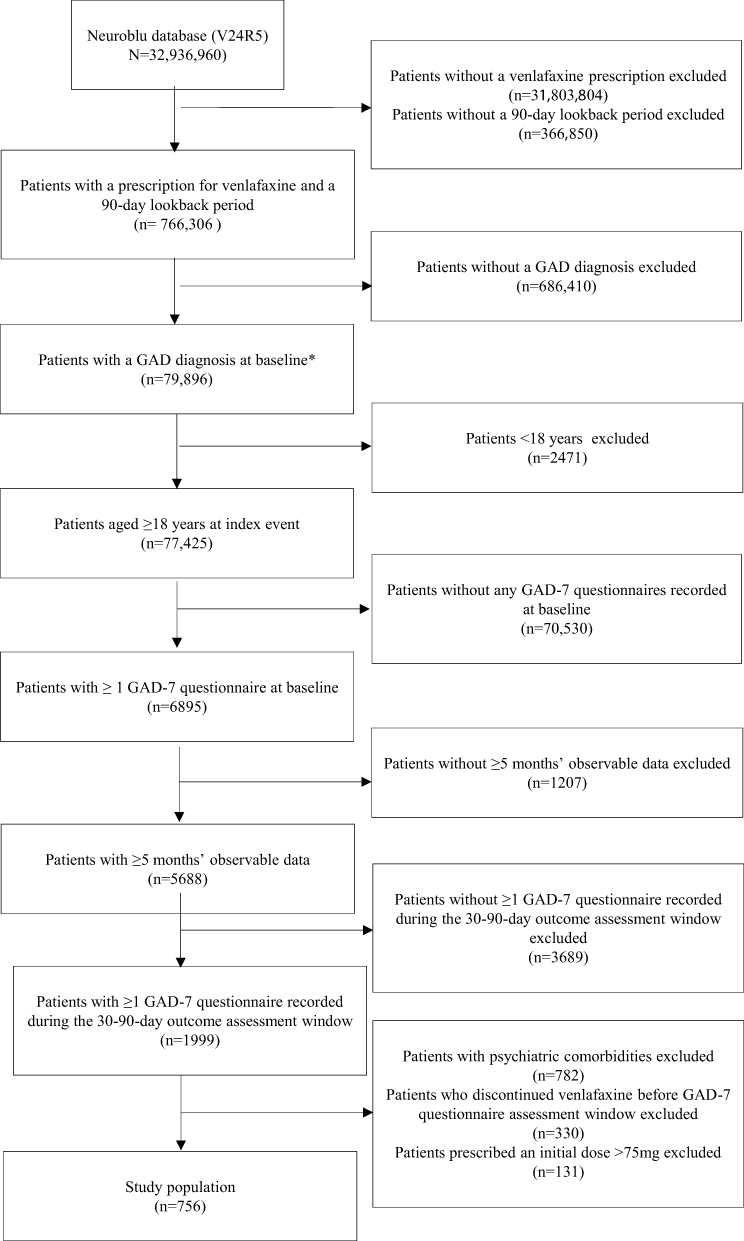 |
Figure 1 Patient population flowchart. *Baseline defined as from 30 days before to 7 days after the index event. Abbreviation: GAD-7, Generalized Anxiety Disorder 7-item scale. |
Altogether, 71.8% of patients had a diagnosis of comorbid MDD recorded at baseline and 23.0% also had another anxiety/phobic disorder (Table 1). Comorbid MDD was more prevalent among patients with moderate or severe anxiety (72.1% and 76.0% respectively), compared with patients with minimal or mild anxiety (65.5% and 60.2% respectively).
Venlafaxine Treatment Characteristics
The initial venlafaxine prescription dose was 37.5mg in 65.5% of patients, with the remaining patients receiving 75mg (Table 1). Females were more likely to receive an initial dose of 37.5mg than males (67.3% vs 58.6%; P=0.049). At the time of the follow-up GAD-7 assessment, the most prescribed dose of venlafaxine was 75mg (46.2%), followed by 37.5mg (33.3%), and 150mg (17.6%). There was no statistically significant association between baseline anxiety severity and venlafaxine dose, at either the first or last recorded prescription before follow-up GAD-7 assessment.
Concomitant psychotropic medication prescription decreased from baseline to follow-up. At baseline, patients were receiving a mean of 1.7±1.4) psychiatric medications (excluding venlafaxine), decreasing to 0.8±1.0 during follow-up (Table 2). The most frequently recorded medication classes were antidepressants and anxiolytics, and the use of these also decreased from baseline (65.2% and 39.7%) to follow-up (31.5% and 21.3%).
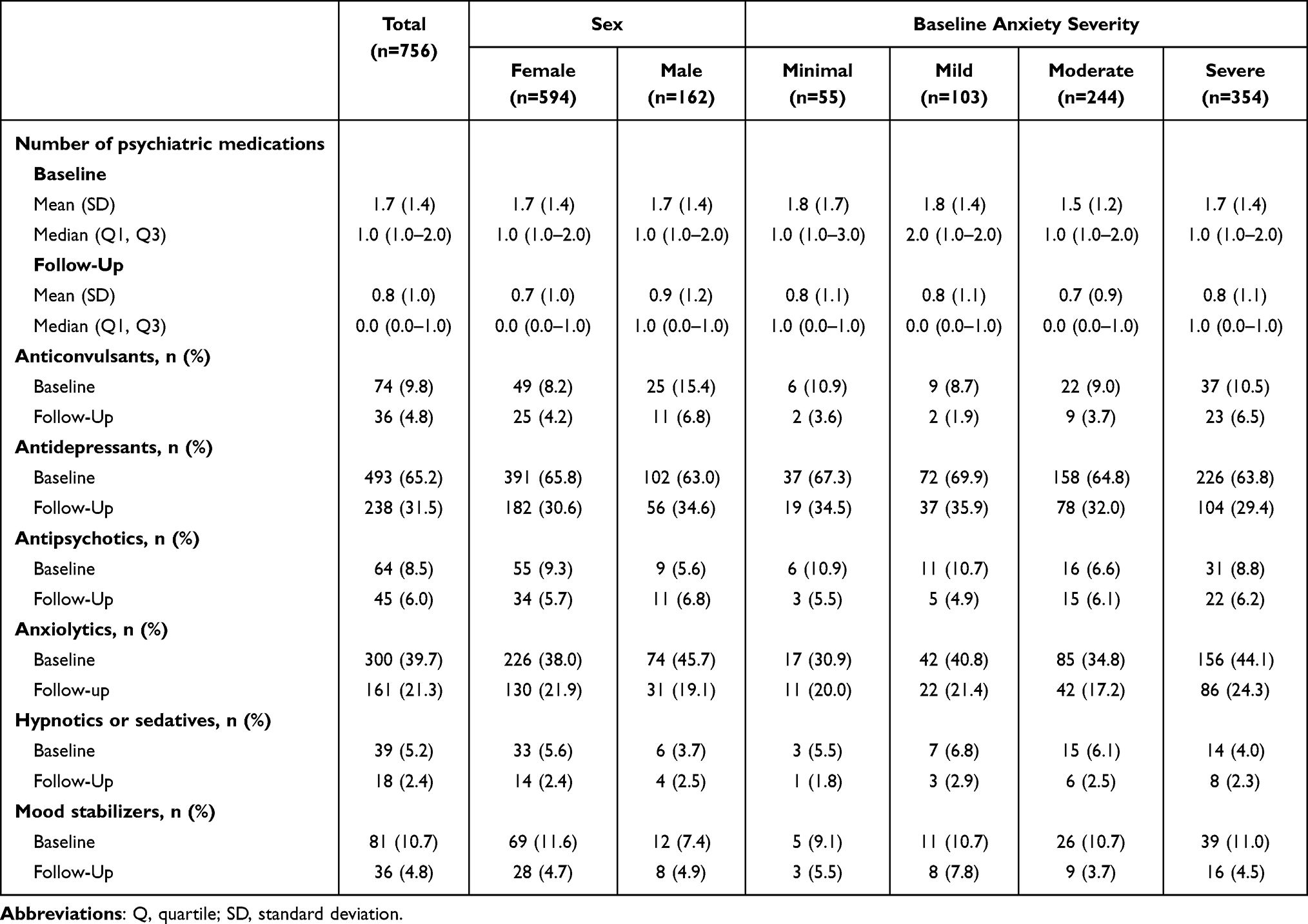 |
Table 2 Psychiatric Medications Prescriptions at Baseline and Follow-Up |
GAD-7
Between baseline and follow-up (the 30–90 days after the index event), median (IQR) GAD-7 score decreased significantly (P<0.001) from 14.0 (10.0–18.0) to 9.0 (5.0–14.0) points, a median change of −3.0 (−8.0–0.0), corresponding to a shift from moderate to mild anxiety severity, with similar decreases seen for male and female patients (Figures 2a and b). When stratified by baseline anxiety severity, symptom improvement was more pronounced among patients with greater baseline severity (Figure 2c). In contrast, patients with mild severity showed the smallest changes. The timing of the follow-up GAD-7 assessment was ~50 days after index for the study population and was similar for male and female patients and across baseline anxiety severity groups (Table 1). Results of a sensitivity analysis in which the baseline period was defined as −30 days to 0 day relative to the first recorded venlafaxine prescription were consistent with those of the main analysis in terms of baseline and follow-up GAD-7 scores and time to follow-up GAD-7 assessment (Supplementary Table 3). These consistent findings indicate that the incorporation of 7 post-index days into the baseline period had no material influence on the observed GAD-7 score values or timing.
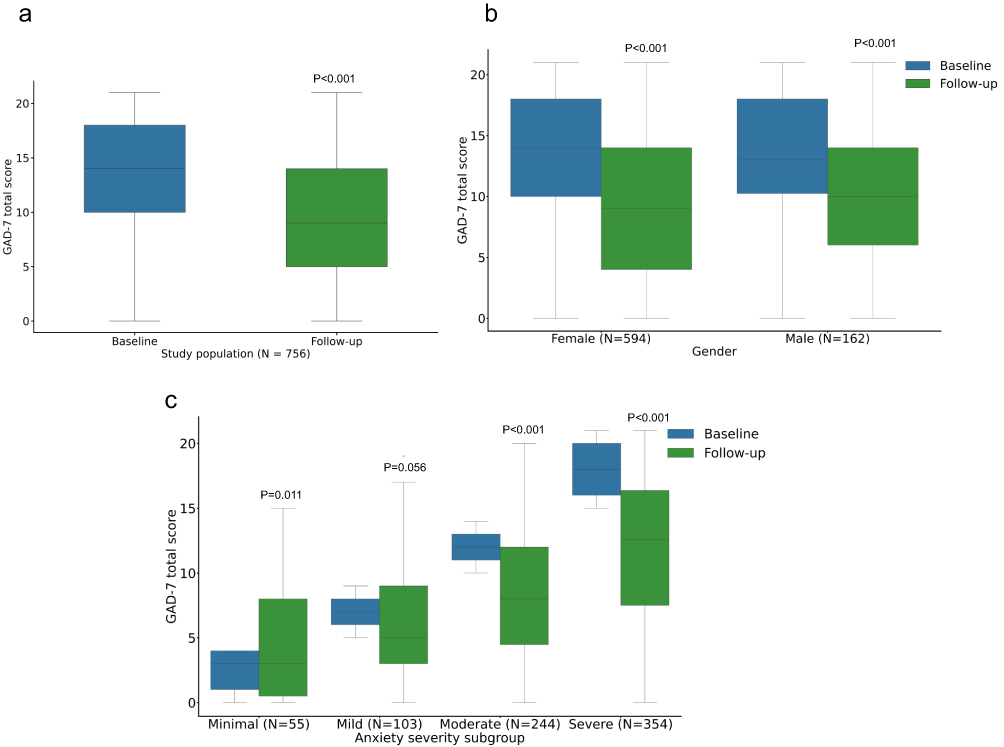 |
Figure 2 Median GAD-7 score at baseline and follow-up for (a) the total population, (b) for males and females and (c) by baseline anxiety severity. In the boxplots, the center line denotes the median value (50th percentile) and the box contains the 25th to 75th percentiles of data. The black whiskers mark the 5th and 95th percentiles. All reported P values are for change in GAD-7 score from baseline to follow-up (Wilcoxon Signed Rank test). Abbreviations: GAD-7, Generalized Anxiety Disorder 7-item scale; SD, standard deviation. |
Clinically Meaningful Change in GAD-7
Altogether, 48.1% of patients experienced a clinically meaningful improvement in GAD-7 score (a decrease of ≥4 points) (Figure 3a). A further 24.3% experienced improvement that was not considered clinically meaningful (a decrease of <4 points). Clinically meaningful worsening (increase of ≥4) was experienced by 7.5% of patients, with a further 12.2% experiencing a numerical, but not clinically meaningful worsening; 7.8% of patients experienced no change in GAD-7 score.
 |
Figure 3 Clinically meaningful change in GAD-7 score for (a) the total population and for males and females and (b) stratified by baseline anxiety severity. Abbreviation: GAD-7, Generalized Anxiety Disorder 7-item scale. |
There was no statistically significant association between sex and any of the clinically meaningful change categories on unadjusted between-group comparisons (Figure 3a). When stratified by baseline anxiety severity, the proportion of patients achieving clinically meaningful improvement was greater among patients with greater initial severity. (Figure 3b).
Altogether, 719 patients with a baseline GAD-7 score of ≥4 were included in the logistic regression analysis conducted to examine the association between clinically meaningful improvement in GAD-7 and baseline patient characteristics (Table 3). In unadjusted univariate analysis, baseline factors associated with significantly reduced odds of reaching a clinically meaningful improvement were a concomitant anticonvulsant prescription (odds ratio [OR] 0.55, 95% CI 0.34–0.88; P=0.014), antidepressant prescription (OR 0.52, 0.37–0.73; P<0.001), antipsychotic prescription (OR 0.60, 0.37–0.96; P=0.033), anxiolytic prescription (OR 0.66, 0.49–0.88; P=0.005) and venlafaxine dose at baseline (OR 0.99, 0.98–1.00; P=0.010). The only factor associated with a significantly increased odds of reaching a clinically meaningful improvement in GAD-7 was baseline GAD-7 score (OR 5.84, 3.77–9.05; P<0.001).
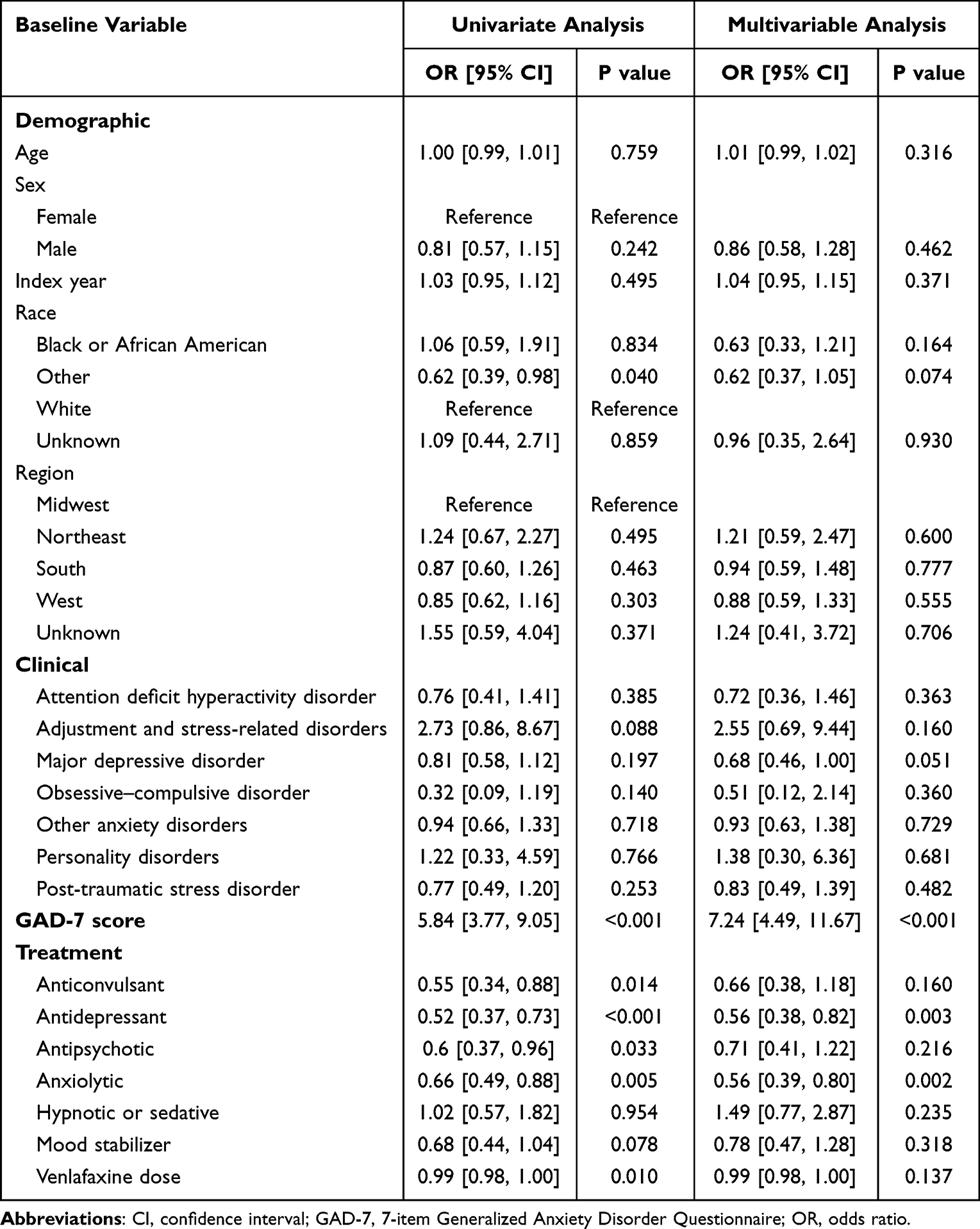 |
Table 3 Logistic Regression Analysis of the Association Between Clinically Meaningful Improvement in GAD-7 and Baseline Demographic, Clinical and Treatment Characteristics |
In multivariable analysis, the only significant associations with reduced odds of reaching a clinically meaningful improvement in GAD-7 were antidepressant prescription (OR 0.56, 0.38–0.82; P=0.003) and anxiolytic prescription (OR 0.56, 0.39–0.80; P=0.002). As in the univariate analysis, baseline GAD-7 score was associated with a significantly increased odds of reaching a clinically meaningful improvement in GAD-7 score (OR 7.24, 4.49–11.67; P<0.001). Results of a sensitivity analysis in which the baseline period was defined as −30 days to 0 day relative to the first recorded venlafaxine prescription were consistent with those of the main univariate and multivariable analysis (Supplementary Table 4). These consistent findings indicate that the incorporation of 7 post-index days into the baseline period had no material influence on the observed associations between baseline characteristics and clinically meaningful improvement in GAD-7 score.
Subsequent subgroup analyses indicated that during follow-up after first venlafaxine prescription, patients who also did vs did not have an antidepressant prescription at baseline had a smaller median change from baseline in GAD-7 score (−3.0 vs −5.0; P<0.001) and a smaller proportion of patients achieving a clinically meaningful improvement in GAD-7 score (44.0% vs 55.9%; P=0.002). Notably, both patients with and those without antidepressant prescription at baseline had similar baseline GAD-7 scores and experienced a significant decrease in GAD-7 scores from baseline. Baseline, follow-up and median change in GAD-7 scores for subgroups of patients with or without antidepressant or anxiolytic prescriptions, at baseline or at follow-up, are shown in Table 4, along with the proportion of patients in each subgroup achieving a clinically meaningful improvement in GAD-7.
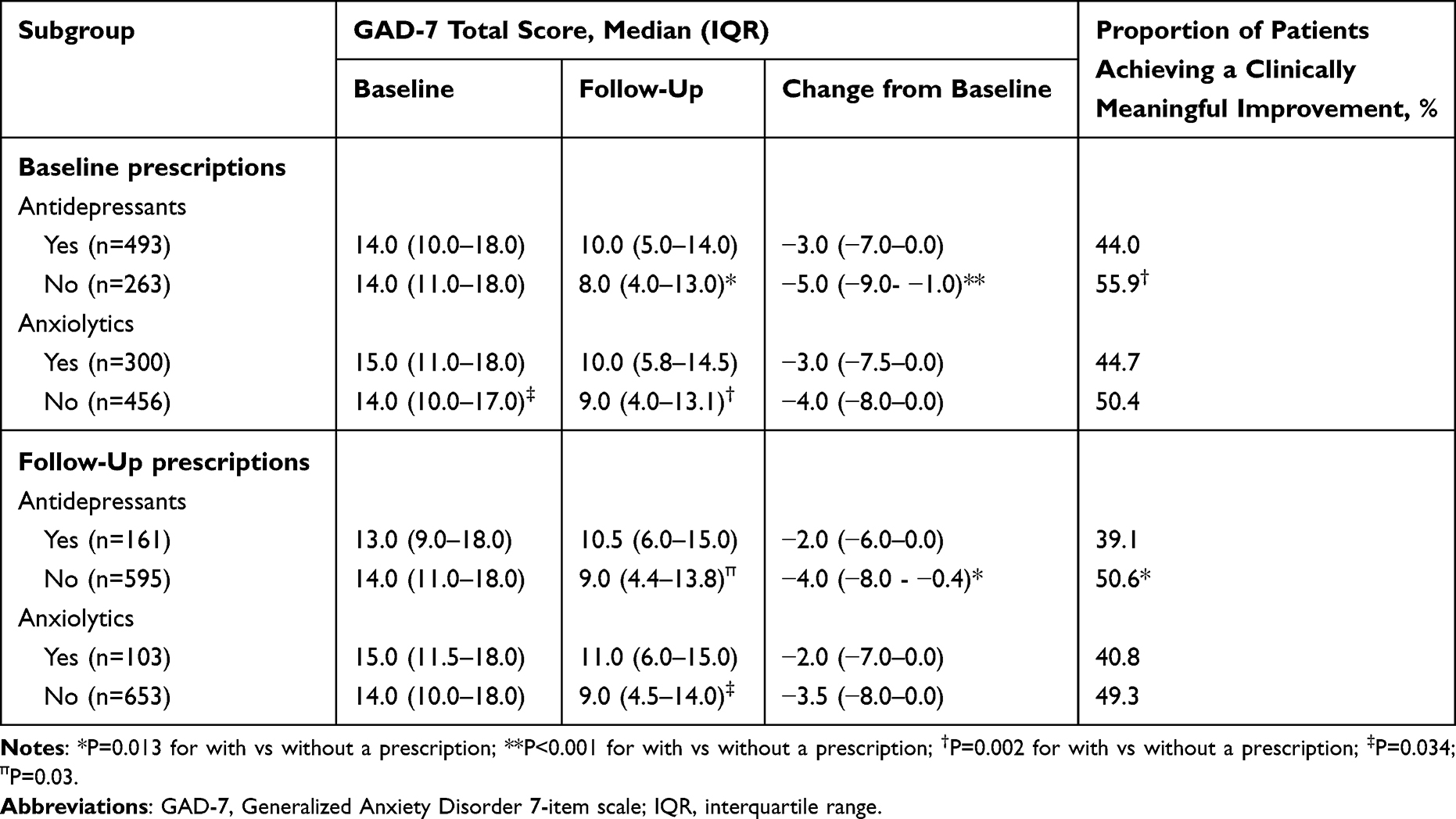 |
Table 4 Subgroup Analysis in Patients with or Without Antidepressant (in Addition to Venlafaxine) or Anxiolytic Presentation at Baseline or at the Time of Follow-Up GAD-7 Assessment |
As noted, baseline GAD-7 score was significantly associated with achieving a clinically meaningful improvement, on both univariate and multivariable analysis, and subgroup analyses revealed that increasing baseline GAD-7 score was associated with increasing odds of achieving a clinically meaningful improvement in GAD-7 following venlafaxine treatment, with each 1-point increase in baseline GAD-7 score associated with higher odds of achieving clinically meaningful improvement although this was a non-linear relationship (Supplementary Figure 2).
Exploratory Treatment Discontinuation Analysis
Overall, 63.6% of patients had no recorded discontinuation during the 30–90-day follow-up period. There were 23.5% of patients who met the discontinuation definition (no recorded prescription of venlafaxine for more than 60 days) between 30 and 60 days after the index venlafaxine prescription, and a further 12.8% met the definition between 61 and 90 days. In the 30–60-day interval, discontinuation proportions differed across baseline anxiety severity categories (minimal 9.1%, mild 21.4%, moderate 26.2%, severe 24.6%, respectively; P=0.049). No statistically significant differences by anxiety severity were observed for discontinuation occurring between 61 and 90 days or for discontinuation assessed over the entire 30–90-day period. Discontinuation during the 61–90-day interval was more frequent among males than females (17.9% vs 11.4%; P=0.041).
Discussion
In the current study, most patients were female, and a concomitant MDD diagnosis was frequently recorded, both of which are consistent with the clinical presentation of GAD in usual practice.24 Overall, this real-world study shows reduction in GAD-7 scores in patients treated with venlafaxine, with almost half of them achieving clinically meaningful improvement in 30–90 days after a first recorded prescription. While the observed improvement cannot be conclusively attributed to the prescription of venlafaxine alone due to the design of the study, the lack of a comparator and potential confounders, the result is congruent to randomised-controlled clinical trials which establish the efficacy of venlafaxine in GAD. Notably, the median GAD-7 score at baseline (14.0) indicates that at least half of all included patients who were prescribed venlafaxine around the time of a recorded GAD diagnosis had moderate or severe anxiety, which is comparable to previous observational studies using the GAD-7 in primary care settings.14,25 Moreover, the median GAD-7 score of 9.0 during follow-up indicates that after treatment with venlafaxine there was a shift from moderate anxiety at baseline to mild anxiety during follow-up. However, it should be noted that the exclusion of patients who discontinued venlafaxine before their follow-up GAD-7 assessment in the present study may have biased the change in GAD-7 score, leading to changes of larger magnitude.
The magnitude of improvement in GAD-7 score was largest in those with moderate or severe anxiety at baseline, without significant change in GAD-7 score in patients with mild baseline anxiety. This result is consistent with previous clinical trial results showing reductions in anxiety following treatment with venlafaxine in patients with moderate to severe anxiety,10 while patients with mild anxiety maintained their stability. Achieving a 4-point decrease in GAD-7 in this population is particularly challenging due to measurement floor effects. Notably, one third of patients remained below the recommended target dose of 75 mg,23 which may have further contributed to attenuated response rates. Notably, in our study males were prescribed higher doses of venlafaxine at baseline than females, which may reflect differential prescribing practices, despite a lack of any evidence from prior research that would suggest a need to dose venlafaxine differentially based on sex, with similar pharmacokinetics in females and males.26
In the current study, the proportion of patients with GAD who were already prescribed antidepressants (65%) or anxiolytics (40%) at baseline were consistent with those of previous studies in GAD using data from routine care.19,21 The decrease in these proportions during the follow-up period suggests that patients may have been switched from these medications to venlafaxine. Patients included in the study may have been prescribed venlafaxine for the treatment of GAD or for both GAD and MDD in patients with both diagnoses, because venlafaxine is also a first-line treatment option for MDD. The 90-day lookback window was utilized to increase the likelihood of only including patients initiated on venlafaxine for the proximal GAD diagnosis. Moreover, patients initiated on a dose of venlafaxine higher than 75mg were excluded from the study to reduce the likelihood of including patients who were already receiving venlafaxine, as it was unlikely that patients would be started on such a high dose without previous venlafaxine exposure. The finding of higher doses during the follow-up period may point towards dose optimization and further supports this point.
The inclusion of patients with MDD and patients receiving concomitant antidepressants is an important feature of our study population as it reflects real-world characteristics. This contrasts with clinical trials in patients with anxiety, which often exclude those with comorbid MDD.8,10,22,27,28 The results of the regression analyses demonstrated that patients included in the current study who were receiving an antidepressant or anxiolytic in addition to venlafaxine had significantly lower odds of achieving a clinically meaningful improvement in GAD-7. Moreover, subgroup analyses of change from baseline in GAD-7 score demonstrated that a baseline prescription of an antidepressant in addition to a venlafaxine prescription was associated with a significantly smaller decrease in GAD-7 score than in those without an antidepressant prescription at baseline. These findings of the regression and subgroup analyses are consistent with the results of a pooled analysis of placebo-controlled studies of venlafaxine in GAD, which found that a history of antidepressant or anxiolytic treatment for anxiety reduced the odds of achieving a response to venlafaxine,29 either due to prior treatment effects reducing room for improvement or these patients may represent patients with more complex presentation or a treatment-resistant subgroup. However, the design of the present study does not account for confounding by indication or the time-varying nature of antidepressant or anxiolytic treatments and therefore interpretation of these results is subject to important caveats. Specifically, the observed reduction in concomitant antidepressant and anxiolytic prescribing during follow-up suggests that treatment regimens were actively modified over the study period. Long-term studies evaluating treatment response patterns in these patients may provide better clinical insights.
The discontinuation rates reported in this study, which can be considered as a proxy for acceptability,30 are broadly consistent with RCTs, which have generally reported overall discontinuation rates of approximately 20% to 30% at 8 weeks.9,10,31
An important strength of the current study is the use of the GAD-7, which is not typically available in real-world datasets. However, there are also some important limitations to be considered. Previous research on changes in anxiety severity in patients with GAD receiving treatment with venlafaxine have primarily been conducted in clinical trial settings utilizing measures such as the HAM-A,8,10,22,27 limiting direct comparisons with the results of the current analysis. However, these studies that utilized HAM-A have also demonstrated significant reductions in anxiety severity with venlafaxine and there is evidence from a GAD-7 validity study demonstrating a high level or correlation between GAD-7 and HAM-A.25 Other limitations include the possibility that patients may have received prior venlafaxine treatment at centers not captured in NeuroBlu Data, and previous patient clinical history may be incomplete for some patients. Additionally, the impact of side effects and tolerability on anxiety severity changes were not assessed in the present study, which could be addressed in future studies. Furthermore, NeuroBlu Data only includes prescription data and is not linked to pharmacy claims and predominantly captures specialized healthcare centers and may not accurately represent patients with GAD who are managed in primary care.
As with all studies utilizing EHR data, our data (while novel in its measurement of anxiety symptoms), has not been collected for the purpose of this study and therefore data may be missing, and/or collected at inconsistent time points. There are several other important methodological limitations that should be considered. The study does not utilize a comparator group and therefore improvement cannot solely be attributed to venlafaxine treatment, as there are other factors such as the natural course of anxiety symptoms, concomitant medications and changes in concomitant medications. Inclusion of baseline GAD-7 score as a covariate in the multivariable model accounts for differences in initial severity and the associated ceiling/floor effects on change. However, in the absence of a control group, regression to the mean cannot be fully excluded as a contributor to the observed improvement; this is an inherent limitation of single-arm pre-post observational studies.
Conclusions
In this selected real-world US-based cohort of patients with GAD, improvement in GAD-7 scores was observed to be associated with venlafaxine prescription. However, this result should be interpreted with caution, due to the retrospective design of the study and absence of controls.
Acknowledgments
We thank Marie Cheeseman who provided medical writing support on behalf of Research Review, funded by Viatris.
Funding
This study was funded by Viatris. The funder contributed to the study design and interpretation of results. Data analysis was conducted by Holmusk Technologies Inc., UK.
Disclosure
CU Correll has been a consultant and/or advisor to or has received honoraria from: AbbVie, Alkermes, Allergan, Angelini, Aristo, Autobahn, Axsome, Boehringer-Ingelheim, Bristol-Meyers Squibb, Cardio Diagnostics, Cerevel, CNX Therapeutics, Compass Pathways, Darnitsa, Delpor, Denovo, Draig, Eli Lilly, Eumentis Therapeutics, Gedeon Richter, GH Research, Hetero, Hikma, Holmusk, IntraCellular Therapies, Jamjoom Pharma, Janssen/J&J, Karuna, LB Pharma, Lundbeck, MedInCell, MedLink Global, Merck, Mindpax, Mitsubishi Tanabe Pharmaceuticals, Maplight, Mylan, Neumora Therapeutics, Neuraxpharm, Neurocrine, Neurelis, Neurosterix, NeuShen, Neusignal Therapeutics, Newron, Noven, Novo Nordisk, Orion Pharma, Otsuka, PPD Biotech, Recognify Life Science, Recordati, Relmada, Response Pharmaeutical, Reviva, Rovi, Saladax, Sanofi, Seqirus, Servier, Sumitomo Pharma America, Sunovion, Sun Pharma, Supernus, Tabuk, Takeda, Teva, Terran, Tolmar, Vertex, Viatris and Xenon Pharmaceuticals. He provided expert testimony for Janssen, Lundbeck, Neurocrine, and Otsuka. He served on a Data Safety Monitoring Board for Compass Pathways, IntraCellular Therapies, Relmada, Reviva, Rovi. He has received grant support from Boehringer-Ingelheim, Janssen and Takeda. He received royalties from UpToDate and is also a stock option or stock holder of Cardio Diagnostics, Kuleon Biosciences, LB Pharmaceuticals, MedLink Global, Mindpax, Quantic, Terran. Kannan Subramaniam and Pradeep Purushottamahanti report employment with Viatris and hold stock in the company. Bituparna Bayan reports employment with Viatris. Luke A Bryden, Emily OC Palmer and Nadia Lipunova report employment with and equity ownership in KKT Technologies Pte. Ltd. The authors report no other conflicts of interest in this work.
References
1. Bie F, Yan X, Xing J, et al. Rising global burden of anxiety disorders among adolescents and young adults: trends, risk factors, and the impact of socioeconomic disparities and COVID-19 from 1990 to 2021. Front Psychiatry. 2024;15:1489427. doi:10.3389/fpsyt.2024.1489427
2. Lancet Psychiatry T. The Lancet Psychiatry. Global Burden of Disease 2021: mental health messages. Lancet Psychiatry. 2024;11(8):573. doi:10.1016/S2215-0366(24)00222-0
3. Institute for Health Metrics and Evaluation (IHME). GBD Compare. Seattle, WA: IHME, University of Washington; 2023.
4. American Psychiatric Association. Diagnostic and statistical manual of mental disorders, text revision (DSM-5-TR).2022.10.1176/appi.books.9780890425787.
5. DeMartini J, Patel G, Fancher TL. Generalized Anxiety Disorder. Ann Intern Med. 2019;170(7):Itc49–15. doi:10.7326/aitc201904020
6. DeGeorge KC, Grover M, Streeter GS. Generalized anxiety disorder and panic disorder in adults. Am Fam Physician. 2022;106(2):157–164.
7. Bandelow B, Allgulander C, Baldwin DS, et al. World Federation of Societies of Biological Psychiatry (WFSBP) guidelines for treatment of anxiety, obsessive-compulsive and posttraumatic stress disorders – version 3. Part I: anxiety disorders. World J Biol Psychiatry. 2023;24(2):79–117. doi:10.1080/15622975.2022.2086295
8. Gelenberg AJ, Lydiard RB, Rudolph RL, Aguiar L, Haskins JT, Salinas E. Efficacy of venlafaxine extended-release capsules in nondepressed outpatients with generalized anxiety disorder: a 6-month randomized controlled trial. JAMA. 2000;283(23):3082–3088. doi:10.1001/jama.283.23.3082
9. Katz IR, Reynolds CF 3rd, Alexopoulos GS, Hackett D. Venlafaxine ER as a treatment for generalized anxiety disorder in older adults: pooled analysis of five randomized placebo-controlled clinical trials. J Am Geriatr Soc. 2002;50(1):18–25. doi:10.1046/j.1532-5415.2002.50003.x
10. Montgomery SA, Sheehan DV, Meoni P, Haudiquet V, Hackett D. Characterization of the longitudinal course of improvement in generalized anxiety disorder during long-term treatment with venlafaxine XR. J Psychiatr Res. 2002;36(4):209–217. doi:10.1016/s0022-3956(02)00005-5
11. Schawo SJ, Carlier IVE, van Hemert AM, de Beurs E. Measuring treatment outcome in patients with anxiety disorders: a comparison of the responsiveness of generic and disorder-specific instruments. J. Anxiety Disord. 2019;64:55–63. doi:10.1016/j.janxdis.2019.04.001
12. Thompson E. Hamilton Rating Scale for Anxiety (HAM-A). Occup Med. 2015;65(7):601. doi:10.1093/occmed/kqv054
13. Hamilton M. The assessment of anxiety states by rating. Br J Med Psychol. 1959;32(1):50–55. doi:10.1111/j.2044-8341.1959.tb00467.x
14. Spitzer RL, Kroenke K, Williams JBW, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch. Intern. Med. 2006;166(10):1092–1097. doi:10.1001/archinte.166.10.1092
15. Toussaint A, Hüsing P, Gumz A, et al. Sensitivity to change and minimal clinically important difference of the 7-item Generalized Anxiety Disorder Questionnaire (GAD-7). J Affect Disord. 2020;265:395–401. doi:10.1016/j.jad.2020.01.032
16. Waheed A, Afridi AK, Rana M, et al. Knowledge and behavior of primary care physicians regarding utilization of standardized tools in screening and assessment of anxiety, depression, and mood disorders at a large integrated health system. J Prim Care Community Health. 2024;15:21501319231224711. doi:10.1177/21501319231224711
17. Force UPST, Nicholson WK, Silverstein M. Screening for anxiety disorders in adults: us preventive services task force recommendation statement. JAMA. 2023;329(24):2163–2170. doi:10.1001/jama.2023.9301
18. Sherman RE, Anderson SA, Pan GJD, et al. Real-World Evidence — what Is It and What Can It Tell Us? N Engl J Med. 2016;375(23):2293–2297. doi:10.1056/NEJMsb1609216
19. Chollet J, Saragoussi D, Clay E, François C. A clinical research practice datalink analysis of antidepressant treatment patterns and health care costs in generalized anxiety disorder. Value Health. 2013;16(8):1133–1139. doi:10.1016/j.jval.2013.09.001
20. François C, Despiégel N, Maman K, Saragoussi D, Auquier P. Anxiety disorders, major depressive disorder and the dynamic relationship between these conditions: treatment patterns and cost analysis. J Med Econ. 2010;13(1):99–109. doi:10.3111/13696991003591321
21. Berger A, Edelsberg J, Bollu V, et al. Healthcare utilization and costs in patients beginning pharmacotherapy for generalized anxiety disorder: a retrospective cohort study. BMC Psychiatry. 2011;11(1):193. doi:10.1186/1471-244X-11-193
22. Rickels K, Pollack MH, Sheehan DV, Haskins JT. Efficacy of extended-release venlafaxine in nondepressed outpatients with generalized anxiety disorder. Am J Psychiatry. 2000;157(6):968–974. doi:10.1176/appi.ajp.157.6.968
23. Viatris Inc. Effexor XR (Venlafaxine Extended-Release) Capsules: Prescribing Information; September 4, 2023.
24. Ferries E, Suponcic S, Louie D, et al. The prevalence and burden of generalized anxiety disorder in the United States healthcare system: real-world prevalence and incidence from 2020 to 2023. J Mood Anxiety Disord. 2026;13:100172. doi:10.1016/j.xjmad.2026.100172
25. Ruiz MA, Zamorano E, García-Campayo J, Pardo A, Freire O, Rejas J. Validity of the GAD-7 scale as an outcome measure of disability in patients with generalized anxiety disorders in primary care. J Affect Disord. 2011;128(3):277–286. doi:10.1016/j.jad.2010.07.010
26. Klamerus KJ, Parker VD, Rudolph RL, Derivan AT, Chiang ST. Effects of age and gender on venlafaxine and O-desmethylvenlafaxine pharmacokinetics. Pharmacotherapy. 1996;16(5):915–923. doi:10.1002/j.1875-9114.1996.tb03009.x
27. Davidson JR, DuPont RL, Hedges D, Haskins JT. Efficacy, safety, and tolerability of venlafaxine extended release and buspirone in outpatients with generalized anxiety disorder. J Clin Psychiatry. 1999;60(8):528–535. doi:10.4088/jcp.v60n0805
28. Zhou Y, Cao Z, Yang M, et al. Comorbid generalized anxiety disorder and its association with quality of life in patients with major depressive disorder. Sci Rep. 2017;7:40511. doi:10.1038/srep40511
29. Pollack MH, Meoni P, Otto MW, Simon N, Hackett D. Predictors of outcome following venlafaxine extended-release treatment of DSM-IV generalized anxiety disorder: a pooled analysis of short- and long-term studies. J Clin Psychopharmacol. 2003;23(3):250–259. doi:10.1097/01.jcp.0000084025.22282.84
30. Müller TJ, Künzi A, Heitlinger E, et al. Comparative efficacy and acceptability of anxiolytic drugs for the treatment of anxiety disorders: a systematic review and network meta-analysis. Eur Arch Psychiatry Clin Neurosci. 2025. doi:10.1007/s00406-025-02082-0
31. Silverstone PH, Salinas E. Efficacy of venlafaxine extended release in patients with major depressive disorder and comorbid generalized anxiety disorder. J Clin Psychiatry. 2001;62(7):523–529. doi:10.4088/jcp.v62n07a04
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effectiveness of Vortioxetine in Patients with Major Depressive Disorder in Real-World Clinical Practice in Italy: Results from the RELIEVE Study
De Filippis S, Pugliese A, Christensen MC, Rosso G, Di Nicola M, Simonsen K, Ren H
Neuropsychiatric Disease and Treatment 2022, 18:1665-1677
Published Date: 9 August 2022
Effectiveness of Vortioxetine in Patients with Major Depressive Disorder in Real-World Clinical Practice: French Cohort Results from the Global RELIEVE Study
Polosan M, Rabbani M, Christensen MC, Simonsen K, Ren H
Neuropsychiatric Disease and Treatment 2022, 18:1963-1974
Published Date: 31 August 2022
Long-Term Treatment with Trazodone Once-A-Day (TzOAD) in Patients with MDD: An Observational, Prospective Study
Shrashimirova M, Tyanev I, Cubała WJ, Wichniak A, Vodickova-Borzova C, Ruggieri A, Bonelli A, Lipone P, Comandini A, Cattaneo A
Neuropsychiatric Disease and Treatment 2023, 19:1181-1193
Published Date: 12 May 2023
Tactical Considerations for Designing Real-World Studies: Fit-for-Purpose Designs That Bridge Research and Practice
Dreyer NA, Mack CD
Pragmatic and Observational Research 2023, 14:101-110
Published Date: 25 September 2023
Patient-Reported Well-Being in Value-Based Routine Care in Psoriatic Disease Using Tildrakizumab: 2-Year Data of the Phase IV POSITIVE Study
Mrowietz U, Sommer R, Reguiai Z, Gerdes S, Daudén E, Weger W, Maul JT, Naldi L, Ghislain PD, Laws PM, De Jong EMGJ, Mburu S, Koscielny V, Massana E, Sapena V, Domenech A, Kasujee I, Augustin M
Psoriasis: Targets and Therapy 2026, 16:590189
Published Date: 12 May 2026