Back to Journals » ImmunoTargets and Therapy » Volume 15
Carcinoembryonic Antigen Flare Under Oxaliplatin-Based Chemotherapy Predicts Benefit from Nivolumab in Metastatic Microsatellite-Stable Colorectal Cancer – A Post Hoc Analysis of METIMMOX Trial Data
Authors Meltzer S ![]() , Landmark SS, Šaltytė Benth J, Negård A, Hamre HM, Kersten C, Hofsli E
, Landmark SS, Šaltytė Benth J, Negård A, Hamre HM, Kersten C, Hofsli E ![]() , Guren MG, Sorbye H
, Guren MG, Sorbye H ![]() , Flatmark K
, Flatmark K ![]() , Ree AH
, Ree AH ![]()
Received 9 January 2026
Accepted for publication 1 May 2026
Published 14 May 2026 Volume 2026:15 594176
DOI https://doi.org/10.2147/ITT.S594176
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Michael Shurin
Sebastian Meltzer,1 Silje Sjåvik Landmark,1 Jūratė Šaltytė Benth,2,3 Anne Negård,3,4 Hanne Mari Hamre,1 Christian Kersten,1,5 Eva Hofsli,6,7 Marianne Grønlie Guren,3,8 Halfdan Sorbye,9,10 Kjersti Flatmark,3,11,12 Anne Hansen Ree1,3
1Department of Oncology, Akershus University Hospital, Lørenskog, Norway; 2Health Services Research Unit, Akershus University Hospital, Lørenskog, Norway; 3Institute of Clinical Medicine, University of Oslo, Oslo, Norway; 4Department of Radiology, Akershus University Hospital, Lørenskog, Norway; 5Department of Research, Sørlandet Hospital, Kristiansand, Norway; 6Department of Oncology, St. Olav’s Hospital, Trondheim, Norway; 7Department of Clinical and Molecular Medicine, Norwegian University of Science and Technology, Trondheim, Norway; 8Department of Oncology, Oslo University Hospital, Oslo, Norway; 9Cancer Clinic, Haukeland University Hospital, Bergen, Norway; 10Department of Clinical Science, University of Bergen, Bergen, Norway; 11Department of Surgical Oncology, Oslo University Hospital, Oslo, Norway; 12Department of Tumor Biology, Oslo University Hospital, Oslo, Norway
Correspondence: Sebastian Meltzer, Email [email protected]
Background: The randomized METIMMOX trial evaluated short-course oxaliplatin-based chemotherapy alternating with the immune checkpoint inhibitor nivolumab in patients with previously untreated, unresectable abdominal metastases from microsatellite-stable/mismatch repair-proficient colorectal cancer. A subgroup receiving this experimental treatment showed remarkably improved outcome compared to control arm patients who received chemotherapy alone and had median progression-free survival (PFS) of 9.3 months. We examined whether the kinetics of serum carcinoembryonic antigen (CEA) could provide insights into responsiveness to the METIMMOX regimen.
Methods: Patients were randomly assigned to the control arm (oxaliplatin with bolus 5-fluorouracil/folinic acid, Q2W) or the experimental arm (alternating two cycles of chemotherapy Q2W and nivolumab Q2W). In this post hoc biomarker analysis, CEA levels were measured at baseline, at each treatment administration, and every two months during prespecified treatment breaks. Patients were categorized according to CEA kinetics—Flare (transient ≥ 20% increase above baseline), Non-responding (gradual increase), and Stable/Responding (values around baseline or gradually decreasing).
Results: Flare comprised 16 out of 71 patients. According to Log rank test, experimental-arm Flare (n = 6) had significantly improved PFS (median 34.9 months) compared to Stable/Responding (n = 21; median PFS 9.9 months; p = 0.005) and Non-responding (n = 9; median PFS 2.1 months; p = 0.007). Flare was not associated with improved PFS for control-arm subjects. Adjusted Cox regression analysis indicated that experimental-arm Flare exhibited a lower progression risk than Non-responding for up to 6.2 months, creating an observation period for a potential decrease following the initial increase.
Conclusion: CEA-Flare may indicate immune checkpoint inhibitor responsiveness following short-course oxaliplatin-based chemotherapy in this patient population; however, this is an exploratory finding that requires prospective validation.
Plain Language Summary: This study examined whether changes in the blood marker CEA can help identify patients who benefit from a new treatment approach for large bowel cancer. The METIMMOX study tested alternating standard chemotherapy and immunotherapy in patients whose cancer had spread to abdominal organs and could not be surgically removed. All patients had a common type of bowel cancer that usually does not respond well to immunotherapy. Some patients who received the combined treatment performed much better than expected, with their cancer staying under control longer than those who received chemotherapy alone.
The researchers studied changes in CEA levels over time during treatment. Based on these changes, patients were grouped into the following three patterns:CEA flare: a temporary increase (at least 20%) followed by a decreaseNon-responding: a steady increase in CEAStable/responding: stable or gradually decreasing CEA levels
Among patients who received alternating chemotherapy and immunotherapy, those who showed a CEA flare had much better outcomes. Their cancer remained under control for a median time of almost 3 years, compared with approximately 10 months for patients with stable/responding CEA levels and only 2 months for those which non-responding CEA levels. This benefit was not seen in the patients who received chemotherapy alone, meaning that a CEA flare may signal a positive immune response after chemotherapy.
In summary, a short-term increase in CEA (CEA flare) may be a helpful sign that patients with large bowel cancer spread to other organs respond well to a combination of chemotherapy and immunotherapy.
Keywords: colorectal cancer, immune checkpoint inhibition, carcinoembryonic antigen, biomarker
Introduction
The introduction of immune checkpoint inhibitors (ICIs) has significantly improved survival outcomes in many solid cancers, including local, locally advanced, and metastatic disease for the subgroup of colorectal cancer (CRC) patients with microsatellite-instable/mismatch-repair (MMR)-deficient tumors.1–5 However, the large majority of CRC patients bear microsatellite-stable (MSS)/MMR-proficient disease with low tumor antigenicity and therefore low or absent ICI responsiveness. To overcome the inherent ICI resistance of MSS/MMR-proficient CRC, various approaches have been explored. These include combining ICI with radiation therapy6 or chemotherapy and an antiangiogenic agent,7–9 or dual-checkpoint ICI combinations.10 In the first-line METIMMOX trial, patients with metastatic MSS/MMR-proficient CRC were randomly assigned to oxaliplatin-based chemotherapy (the Nordic FLOX regimen11) alone or short-course FLOX alternating with the ICI nivolumab. The primary endpoint of improved progression-free survival (PFS) was not met for the intention-to-treat population of 38 subjects receiving the experimental regimen. However, we noted that 16% of experimental-arm patients achieved a radiologic complete response (CR) with eradication of all tumor manifestations, as opposed to none of control-arm patients.12
Efforts are ongoing to identify biomarkers that predict ICI responsiveness. Some are well-established for certain tumor types and used clinically, such as programmed-death ligand-1 expression and tumor mutational burden.13 However, no universal utility of these biomarkers has been proven as yet.14 Pragmatic biomarkers for response prediction are needed to select more precisely the patients who will benefit but also to avoid treating patients who are prone to ICI failure. Dynamic on-treatment biological changes could represent an alternative to the static baseline biomarkers. Changes in the circulating C-reactive protein level early during ICI treatment have been associated with response in metastatic disease from several malignancies.15–18 When administrating immunomodulating chemotherapy before ICI, as done in the METIMMOX trial, the initial adaptation reflected systemically might serve as a unique setting for dynamic biomarker discovery.
Carcinoembryonic antigen (CEA) belongs to a family of cell adhesion molecules.19 Circulating CEA is commonly elevated in advanced CRC. Although its predictive value is limited,20 serial measurements are used for surveiling recurrence risk after curative-intent treatment21 as well as in evaluation of therapy response in the metastatic setting.22 A transient increase, or flare, in CEA in patients with metastatic CRC responding to chemotherapy was first reported in two small studies in 2004 and 2006.23,24 In multivariable analysis, compared with steadily increasing CEA, flare was found to be an independent favorable predictive and prognostic factor for tumor response and survival in patients undergoing first-line chemotherapy.25 However, it remains unclear whether CEA flare also occurs when chemotherapy is combined with ICI, and whether such a flare may be predictive of ICI benefit in this experimental treatment setting.
In this post hoc analysis of METIMMOX data, we hypothesized that CEA flare may be a surrogate marker of immunogenicity incited by oxaliplatin-based chemotherapy, leading to ICI responsiveness in patients with previously untreated, unresectable metastatic MSS/MMR-proficient CRC, and that it may provide a pragmatic tool for early monitoring of treatment activity or failure.
Material and Methods
Ethics Approvals and Consent to Participate
Approvals were given by the Regional Committee for Medical and Health Research Ethics of South-East Norway (2017/1850), the Norwegian Medicines Agency (17/12,752), and the institutional review boards. The trial was conducted in accordance with the Helsinki Declaration. All patients provided written informed consent. The trial was registered with ClinicalTrials.gov, NCT03388190, by 2 January 2018.
Patients, Procedures, and Outcomes
Details have been published previously.12 To summarize for the current context, MSS/MMR-proficient CRC patients with unresectable infradiaphragmatic (liver, peritoneal, nodal) metastases were randomly assigned to first-line treatment with FLOX (oxaliplatin with bolus 5-fluorouracil/folinic acid) Q2W (control arm) or alternating two cycles of FLOX Q2W and nivolumab Q2W (experimental arm), for both trial arms with a break period after four months (eight cycles in a treatment sequence). During active treatment and breaks, radiologic response assessment was performed every eight weeks. If disease progression occurred during a break, a new treatment sequence was initiated. This go-and-stop schedule is depicted in Supplementary Figure S1. The primary endpoint PFS was defined as the time from study inclusion to the first disease progression on active therapy (progressive disease (PD)) by blinded independent central review according to Response Evaluation Criteria in Solid Tumors or iRECIST.26 For patients not experiencing PD, the time from study inclusion to an intolerable adverse event, death from causes other than cancer progression, consent withdrawal, or censoring was calculated. The best overall response (BOR) was defined as the best achieved radiologic response during study participation. A total of 80 patients were enrolled between 29 May 2018 and 22 October 2021. Data cut-off was set to 15 March 2024 when the last patient reached two years of disease-free (CR) follow-up, three years after starting METIMMOX treatment. Median follow-up time was 20.2 months (95% confidence interval (CI), 14.6–23.2).
Specimen Characteristics
The patients were monitored with standard blood tests, including CEA, by the laboratory facilities of the respective study hospitals. Serum samples were stored at 2–8 °C and analyzed within three days of venipuncture. CEA (in μg/L) was measured at baseline, with each treatment administration (every two weeks), and during the treatment breaks (every eight weeks) until censoring. All five study hospitals used the Cobas 8000 e801 analyzer (Roche Diagnostics, Mannheim, Germany) to quantify CEA using electrochemiluminescence technology. None of the patients received high doses of biotin (vitamin B7; >5 mg/day), which might have interfered with the assay.27,28
CEA Kinetics
For this post hoc analysis, patients were categorized based on the CEA kinetics during the first sequence of active therapy, requiring at least four measurements. In cases of missing values (n = 3), the categorization was based on the available measurements. Delay of treatment administration owing to an adverse event was not considered when evaluating the kinetics. The reference limit was below 5.0 μg/L for both men and women, as used by all participating hospitals. The evaluation did not account for smoking status or comorbidities, which are known to slightly elevate CEA levels.29–31 Flare was defined as at least 20% increase from baseline, consistent with previous studies.23,24,32 The three kinetics groups were 1—Flare: 20% increase above baseline followed by decrease at, at least, two subsequent measurements to 20% below baseline (for patients with baseline CEA within the reference limit, Flare was defined as 20% rise followed by decline to baseline); 2—Non-responding: Gradual increase at, at least, two subsequent measurements to 20% above baseline; 3—Stable/Responding: Levels fluctuating around baseline with occasional increases followed by normalization without clear flare (Stable) or gradual decrease below baseline (Responding). Stable and Responding were grouped together because of similar PFS to chemotherapy in the metastatic setting.25 Time until flare occurred was calculated from the start of treatment to the peak CEA value in the first treatment sequence.
Statistical Methods
Analyses were performed using STATA SE version 17 and SPSS version 29.0. Figures were generated using GraphPad Prism version 9.5.1. Continuous variables were presented as median with minimum (min)–maximum (max) values, while categorical variables were presented as frequency and percentage. Differences in PFS stratified by the kinetics groups were visualized using Kaplan-Meier curves with number-at-risk table and assessed with the Log rank test. Cox regression model was estimated to determine association between PFS and kinetics groups adjusted for age, sex, and treatment arm. An interaction between the kinetics group and treatment arm was included to assess differences between the two arms regarding association between PFS and the kinetics groups. The proportional hazards assumption was assessed by a global test and inspecting Schoenfeld residuals. It was found to be violated for the kinetics groups, which was thus entered into the model as a time-dependent variable. For variables with time-dependent effects, and for interaction terms involving such variables, a single hazard ratio (HR) is not directly interpretable; these effects were therefore presented as regression coefficients with standard errors. For covariables with proportional hazards, and for pairwise group comparisons that did not exhibit time-dependent behavior, HRs with 95% CIs were derived from the model. To aid interpretation of time-dependent associations, HRs over time within each trial arm were illustrated graphically. As a sensitivity analysis, we applied a flexible parametric survival model to assess the robustness of the Cox model results. Differences among CEA kinetics groups were assessed by Fisher’s exact test. A nominal significance level of 0.05 was used, but p-values in the Cox model should be interpreted with caution due to the limited sample size of some groups. Whenever possible, interpretation focuses on effect sizes expressed as HRs with 95% CIs, which more appropriately convey the magnitude and uncertainty of associations.
Results
CEA Features
Of the total of 80 randomized patients, 71 (n = 35, control arm; n = 36, experimental arm) had evaluable CEA kinetics in the first treatment sequence (CONSORT diagram; Supplementary Figure S2). The two arms were similar with regard to clinical characteristics (Supplementary Table S1). Of patients in the control and experimental arms, respectively, 8 (23%) and 9 (25%) were Non-responding, 17 (49%), 21 (58%) were Stable/Responding, and 10 (29%) and 6 (17%) had Flare, with no differences in distribution of baseline clinical characteristics among the three kinetics groups except slightly higher age of Flare patients (p = 0.042; Supplementary Table S2).
Among the total of 16 Flare, only one patient had baseline CEA within the reference limit (<5.0 μg/L). Baseline CEA in Flare (median, 49.1; min-max, 3.1–9173) was higher (p = 0.024) than in Non-responding (median, 41.1; min-max, 0.9–2056) and Stable/Responding (median, 8.0; min-max, 1.0–709). The peak CEA of Flare, reached at median 24 days (min-max, 11–82; Supplementary Figure S3), was higher (p = 0.008) in the control arm (median, 465; min-max, 18.0–16466) than in the experimental arm (median, 21.0; min-max, 8.8–146). However, the exact time of the treatment course coinciding with the peak CEA was delayed for some experimental-arm patients (Supplementary Figure S3).
Four control-arm subjects did not reach the first radiologic reassessment, leaving 31 patients evaluable for objective response (CONSORT diagram; Supplementary Figure S2). As shown by Figure 1, among Non-responding, all of the 9 experimental-arm patients had PD or stable disease (SD) as BOR, while 3 of the 7 (43%) evaluable control-arm patients had partial response (PR). Moreover, in the experimental arm, 3 of 6 (50%) Flare and 3 of 21 (14%) Stable/Responding had CR as BOR. By contrast, no better than PR, distributed among the three kinetics groups, was achieved as control-arm response. In summary, the CEA kinetics for experimental-arm patients, while more subdued, seemed more informative of tumor response.
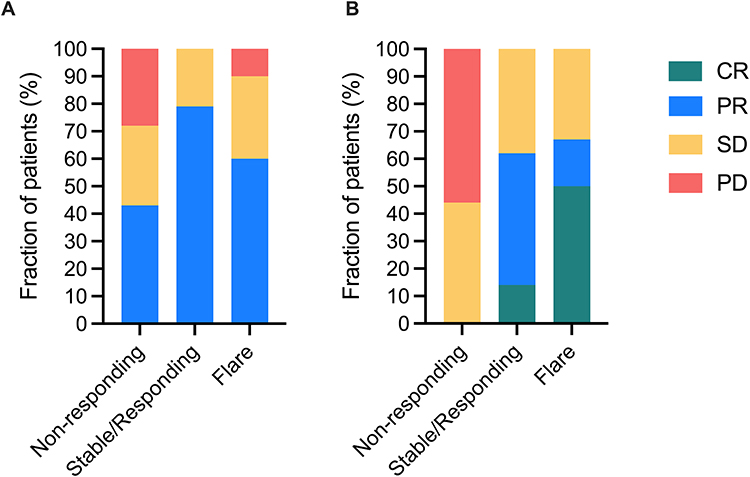 |
Figure 1 Overall response rate of the carcinoembryonic antigen (CEA) kinetics groups. Complete response (CR), partial response (PR), stable disease (SD), or progressive disease (PD) among the 67 patients who reached at least the first radiologic reassessment and thus were evaluable for objective response in the three CEA kinetics groups. (A) Control arm (n = 31). (B) Experimental arm (n = 36). |
CEA Kinetics and Patient Outcome
Following the first treatment sequence and succeeding break, only 4 of the 10 control-arm Flare but 5 of the 6 experimental-arm Flare proceeded to the second treatment sequence. Regarding the primary endpoint for the full cohort of 71 subjects (Figure 2), in the control arm, Stable/Responding showed better PFS (median, 12.2 months; 95% CI, 7.9–16.5) than Non-responding (median, 3.6 months; 95% CI, 2.2–4.9; p = 0.009) but no statistical difference with Flare (median, 7.3 months; 95% CI, 3.8–10.7; p = 0.65). In the experimental arm, by contrast, Flare showed superior PFS (median, 34.9 months; 95% CI, 5.0–64.9) compared to both Stable/Responding (median, 9.9 months; 95% CI, 6.9–12.8; p = 0.005) and Non-responding (median, 2.1 months; 95% CI, 1.7–2.6; p = 0.007).
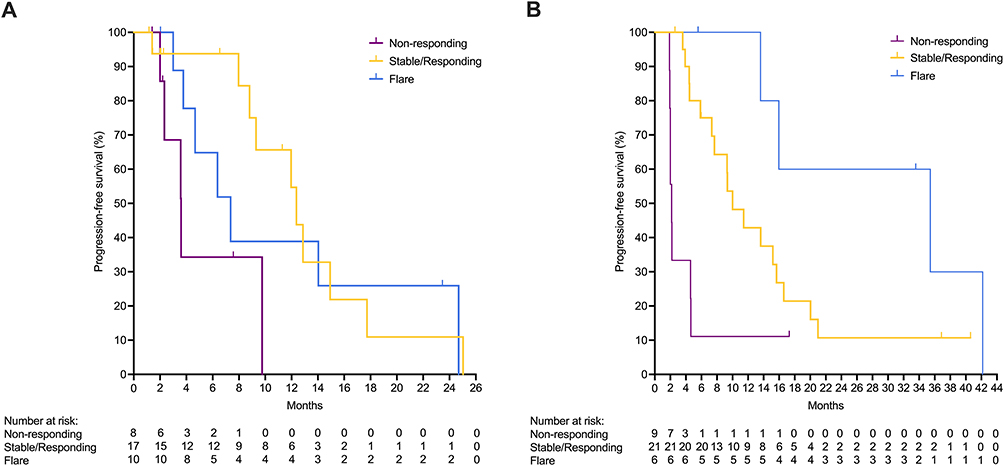 |
Figure 2 Kaplan-Meier curves of progression-free survival of the carcinoembryonic antigen (CEA) kinetics groups. Progression-free survival for the full cohort of 71 subjects in the three CEA kinetics groups. (A) Control arm (n = 35). (B) Experimental arm (n = 36). |
In the adjusted Cox regression model (Table 1), neither age nor sex was associated with PFS. To ease interpretation, the time-dependent HR for the association between the CEA kinetics groups and risk of progression in each trial arm is presented graphically (Figure 3). In the control arm, Stable/Responding and Flare had a lower hazard for progression (p < 0.05 over the time course) compared to Non-responding until 3.0 and 3.8 months had passed, respectively. A similar pattern was found in the experimental arm (p < 0.05 over the time course) but valid for 3.6 months for Stable/Responding versus Non-responding and as long as 6.2 months for Flare versus Non-responding.
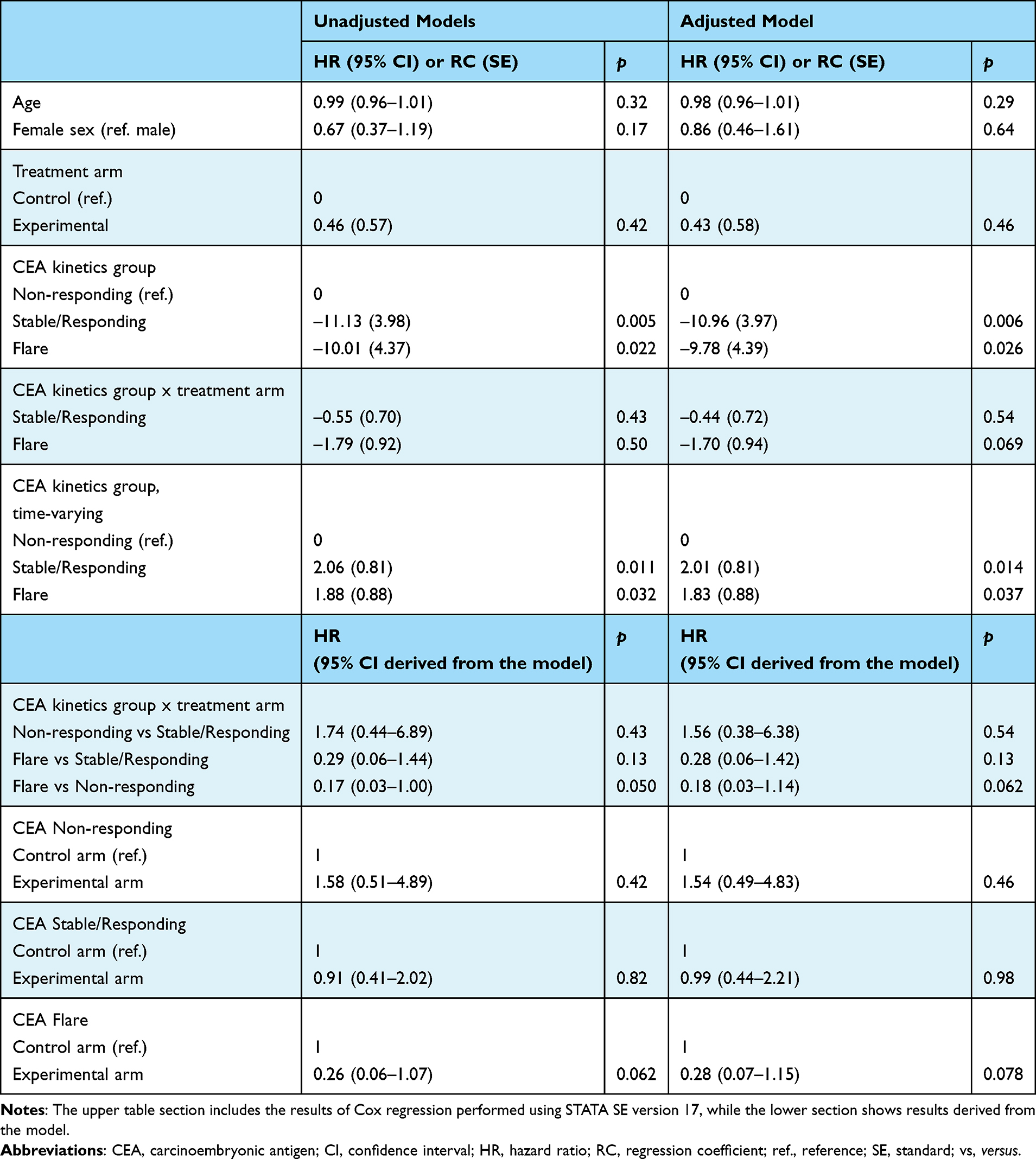 |
Table 1 Cox Regression Models for Progression-Free Survival |
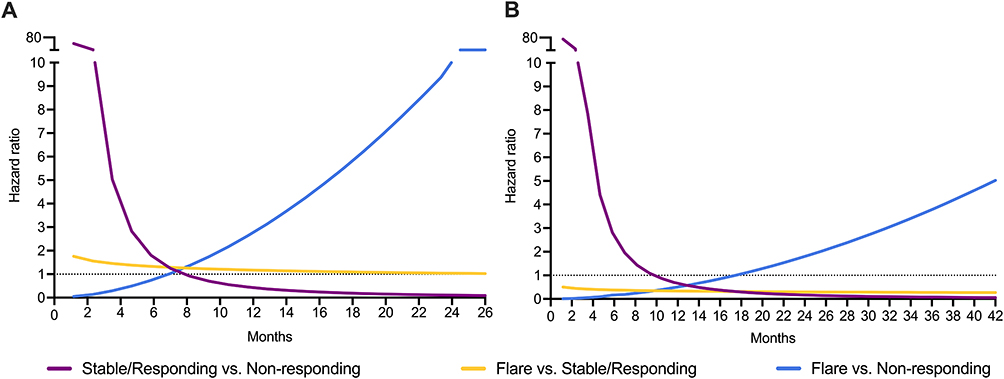 |
Figure 3 Time-varying hazard ratios (HRs) between carcinoembryonic antigen (CEA) kinetics groups; from the adjusted Cox regression model. Graphical presentation of the time-dependent HR for the association between each of the CEA kinetics groups and risk of progression. (A) Control arm (n = 35). (B) Experimental arm (n = 36). The figure illustrates numbers derived from the adjusted Cox regression model. The calculations are based on the model results (regression coefficients and standard errors) and covariances between parameter estimates (not shown), necessary for calculating uncertainties and p-values when exploring such numbers. Dashed lines: HRs of 1. |
When comparing risk of progression within the kinetics groups between the two trial arms (Table 1), the associations did not reach statistical difference. Risk of progression was lower (HR, 0.17; 95% CI, 0.03–1.00) for Flare versus Non-responding in the experimental arm compared to the control arm. This effect size was maintained in the adjusted model (HR, 0.18; 95% CI, 0.03–1.14), underlining the results of the Log rank test. The Cox regression models also allowed comparison of progression risk between the trial arms within each of the kinetics groups (Table 1). The experimental-arm Flare showed lower risk (HR, 0.26; 95% CI; 0.06–1.07) in the unadjusted model, maintained in the adjusted model (HR, 0.28; 95% CI, 0.07–1.15) and supporting the flare response as informative in patients receiving the experimental regimen.
Results from sensitivity analysis were consistent with the primary Cox model, with no changes to the overall conclusions.
Discussion
In this post hoc analysis of METIMMOX data, we found associations between CEA flare during the initial short-course oxaliplatin-based chemotherapy and the clinical response to nivolumab in patients with previously untreated, unresectable abdominal metastases from MSS/MMR-proficient CRC. To date, a small number of randomized studies on first-line use of ICI together with oxaliplatin-based chemotherapy in MSS/MMR-proficient CRC have proven the combination no better than the standard treatment without ICI.7,9,12 However, the METIMMOX trial revealed a subgroup of patients with extended response to alternating short-course FLOX and nivolumab.12 This treatment strategy may have leveraged an anti-tumor immunogenic effect invoked by oxaliplatin, as first observed in experimental CRC models33–35 and then in liver metastases of study patients.36–39 The observations also suggest that an on-treatment biomarker for potential ICI responsiveness might be more informative than a pre-treatment biomarker for capturing an evolving immunogenic process. The CEA response serves as a surrogate clinical endpoint with the advantage of being available and affordable in clinical practice.
Serum CEA levels were higher in Flare than for the two other groups already at baseline, with peak levels reached during the initial two FLOX cycles for most patients. Strikingly, the peak levels were significantly higher in the control arm, an observation which might relate to the delayed CEA response of some experimental-arm patients reaching their peak levels during the succeeding two nivolumab cycles or even later. Still, all patients regardless of trial arm had received identical treatment until the third therapy cycle from when the control-arm and experimental-arm patients proceeded with different regimens.
Regarding distribution of radiologic responses (BOR scores) among the three CEA kinetics groups, notable differences were observed between the two trial arms. In the control arm, patients with PR, SD, or PD were fairly equally distributed among the kinetics groups, suggesting that the CEA kinetics was less informative in prediction of overall chemotherapy response. Conversely, none of experimental-arm Non-responding cases demonstrated a radiologic response (significant tumor shrinkage), indicating that those with consistently rising CEA levels should not continue without chemotherapy. In contrast, most experimental-arm patients categorized as CEA-Flare and -Stable/Responding did achieve radiologic response, with some experiencing long-lasting CR. Therefore, in chemotherapy de-escalation regimens, such as that of METIMMOX, it is essential to have a safety period for monitoring CEA kinetics to distinguish between a transient flare and a continuous increase.
Regarding the trial’s primary endpoint, the similar occurrence of BOR scores in the CEA-Flare and -Stable/Responding groups of control-arm patients was mirrored by comparable PFS. By contrast, experimental-arm CEA-Flare patients experienced considerably improved PFS, but uncertain due to a small group size. It should also be noted that, in particular, the Stable/Responding category may be susceptible to some degree of subjective judgment, which could have influenced the results.
To avoid time-varying confounding, the CEA kinetics groups were analyzed as time-dependent variable in the Cox regression model. Compared to Non-responding patients, both CEA-Flare and -Stable/Responding patients in both trial arms had significantly lower risk of disease progression during the initial treatment, as long as 6 months for Flare patients in the experimental arm, in principle providing an observation period to decide if a decrease would follow an initial CEA increase. In practice, however, the treating oncologist would not wait that long without investigating a potential treatment failure. Moreover, following the initial period in this study, the statistical power was very low because of few remaining patients. The lack of statistical power, typical for post hoc analyses, also applied to the comparisons of risk of progression within and between the CEA kinetics groups of the two trial arms but favored the experimental-arm Flare in all comparisons (without reaching statistical significance).
The incidence of CEA-Flare in the METIMMOX cohort was approximately 20%, which is higher than the reported incidence of 10–15% in patients with metastatic CRC given chemotherapy.23–25,32 Previous studies have defined flare as a transient 15–20% increase above baseline. To ensure robust categorization and account for analytical and intra-individual variability, we set the cut-off value at 20% change from baseline.40 The higher proportion of CEA-Flare patients in our study might be due to the oxaliplatin-based chemotherapy. Previous chemotherapy studies also included patient receiving regimens without oxaliplatin. Notably, oxaliplatin induces immunogenic cell death41 and elevates CEA expression in CRC cells.42 This mechanism may account for the observed CEA flare, where the release of CEA into the circulation reflects the tumor cell killing effects of oxaliplatin and signifies a positive response rather than disease progression. Furthermore, the association between CEA flare and enhanced treatment efficacy aligns with the emerging therapeutic approach involving engineered chimeric antigen receptor T-cells that target CEA-expressing gastrointestinal cancers.43–45 While previous discussions of CEA flare have largely focused on response to chemotherapy in advanced CRC, the current study, to the best of our knowledge, describes this phenomenon for the first time in the context of an investigational chemotherapy-ICI schedule. We have been unable to identify studies on the role of CEA flare in treatment of MMR-deficient CRC, early-onset CRC, or in conjunction with CRC metastasis surgery.
Our study has several limitations. The association signal presented here arise from post hoc exploratory analyses that were not prespecified in the METIMMOX study protocol and are limited by the small number of patients. Althought the Cox regression model suggested that experimental-arm CEA-Flare patients had considerably lowered risk of disease progression, statistical significance was not reached. Our data must be interpreted with caution.
In conclusion, an initial and transient increase in serum CEA under oxaliplatin-based chemotherapy may suggest ICI responsiveness in a subgroup of the large majority of patients with metastatic CRC who bear MSS/MMR-proficient disease, but the results are not definitive. Because ICI responsiveness in metastatic CRC may be deep and durable, and serum CEA measurement is a cost-effective analysis in routine clinical practice, our exploratory findings warrant confirmation in larger, prospective studies.
Clinical Trial Information
The METIMMOX trial – Colorectal cancer metastasis – shaping anti-tumor immunity by oxaliplatin, is registered by clinicaltrials.gov (NCT03388190), and included patients between 29 May 2018 and 22 October 2021. Data cut-off was set to 15 March 2024.
Data Sharing Statement
Requests for data can be made to the corresponding author. The data generated in this study are subject to patient confidentiality in accordance with the General Data Protection Regulation of the European Union, and the transfer of data or materials will require approval from the Data Privacy Officer at Akershus University Hospital and on some occasions from the Regional Committee for Medical and Health Research Ethics of South-East Norway. Any shared data will be de-identified.
Ethics Approvals and Consent to Participate
Approvals were given by the Regional Committee for Medical and Health Research Ethics of South-East Norway (2017/1850), the Norwegian Medicines Agency (17/12752), and the institutional review boards. The trial was conducted in accordance with the Helsinki Declaration. All patients provided written informed consent.
Acknowledgments
We are grateful to Bristol-Myers Squibb for providing nivolumab free of charge for the trial.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Norwegian Cancer Society, including its Umbrella Foundation for Cancer Research (grants 182496, 215613, and 245151) and the South-Eastern Norway Regional Health Authority (grant 2018054).
Disclosure
SM has served on an advisory board of GSK and presented for Bristol Myers Squibb. HMH reports personal honoraria from Bristol-Myers Squibb, Bayer, and Roche and served on scientific advisory boards of Incyte, Eisai, Astellas, and AstraZeneca. EH reports personal honoraria from Bristol-Myers Squibb, AstraZeneca, Daiichi Sankyo, and Takeda. HS reports personal honoraria from Pierre Fabre and Daiichi Sankyo and has served on an advisory board of Bristol-Myers Squibb. AHR reports research support (on behalf of Akershus University Hospital) and a personal honorarium from Bristol-Myers Squibb and has served on scientific advisory boards of MSD and Takeda. The remaining authors declare no conflicts of interest in this work.
References
1. Sinicrope FA, Ou FS, Arnold D, et al. Atezolizumab plus FOLFOX for stage III mismatch repair-deficient colon cancer. N Engl J Med. 2026;394(12):1155–11. doi:10.1056/NEJMoa2507874
2. Chalabi M, Verschoor YL, Tan PB, et al. Neoadjuvant immunotherapy in locally advanced mismatch repair-deficient colon cancer. N Engl J Med. 2024;390:1949–1958. doi:10.1056/NEJMoa2400634
3. Cercek A, Foote MB, Rousseau B, et al. Nonoperative management of mismatch repair-deficient tumors. N Engl J Med. 2025;392(23):2297–2308. doi:10.1056/NEJMoa2404512
4. André T, Elez E, Lenz H-J, et al. Nivolumab plus ipilimumab versus nivolumab in microsatellite instability-high metastatic colorectal cancer (CheckMate 8HW): a randomised, open-label, Phase 3 trial. Lancet. 2025;405.
5. Andre T, Shiu KK, Kim TW, et al. Pembrolizumab in microsatellite-instability-high advanced colorectal cancer. N Engl J Med. 2020;383(23):2207–2218. doi:10.1056/NEJMoa2017699
6. Parikh AR, Szabolcs A, Allen JN, et al. Radiation therapy enhances immunotherapy response in microsatellite stable colorectal and pancreatic adenocarcinoma in a phase II trial. Nat Cancer. 2021;2(11):1124–1135. doi:10.1038/s43018-021-00269-7
7. Antoniotti C, Rossini D, Pietrantonio F, et al. Upfront FOLFOXIRI plus bevacizumab with or without atezolizumab in the treatment of patients with metastatic colorectal cancer (AtezoTRIBE): a multicentre, open-label, randomised, controlled, phase 2 trial. Lancet Oncol. 2022;23(7):876–887. doi:10.1016/S1470-2045(22)00274-1
8. Thibaudin M, Fumet JD, Chibaudel B, et al. First-line durvalumab and tremelimumab with chemotherapy in RAS-mutated metastatic colorectal cancer: a Phase 1b/2 trial. Nat Med. 2023;29:2087–2098. doi:10.1038/s41591-023-02497-z
9. Lenz HJ, Parikh A, Spigel DR, et al. Modified FOLFOX6 plus bevacizumab with and without nivolumab for first-line treatment of metastatic colorectal cancer: phase 2 results from the CheckMate 9X8 randomized clinical trial. J Immunother Cancer. 2024;12(3):e008409. doi:10.1136/jitc-2023-008409
10. Bullock AJ, Schlechter BL, Fakih MG, et al. Botensilimab plus balstilimab in relapsed/refractory microsatellite stable metastatic colorectal cancer: a phase 1 trial. Nat Med. 2024;30:2558–2567. doi:10.1038/s41591-024-03083-7
11. Sorbye H, Glimelius B, Berglund A, et al. Multicenter phase II study of Nordic fluorouracil and folinic acid bolus schedule combined with oxaliplatin as first-line treatment of metastatic colorectal cancer. J Clin Oncol. 2004;22:31–38. doi:10.1200/JCO.2004.05.188
12. Ree AH, Saltyte Benth J, Hamre HM, et al. First-line oxaliplatin-based chemotherapy and nivolumab for metastatic microsatellite-stable colorectal cancer-the randomised METIMMOX trial. Br J Cancer. 2024;130(12):1921–1928. doi:10.1038/s41416-024-02696-6
13. Yarchoan M, Albacker LA, Hopkins AC, et al. PD-L1 expression and tumor mutational burden are independent biomarkers in most cancers. JCI Insight. 2019;4. doi:10.1172/jci.insight.126908
14. Butterfield LH, Najjar YG. Immunotherapy combination approaches: mechanisms, biomarkers and clinical observations. Nat Rev Immunol. 2024;24:399–416. doi:10.1038/s41577-023-00973-8
15. Klumper N, Saal J, Berner F, et al. C reactive protein flare predicts response to checkpoint inhibitor treatment in non-small cell lung cancer. J Immunother Cancer. 2022;10:e004024. doi:10.1136/jitc-2021-004024
16. Klümper N, Schmucker P, Hahn O, et al. C-reactive protein flare-response predicts long-term efficacy to first-line anti-PD-1-based combination therapy in metastatic renal cell carcinoma. Clin Transl Immunology. 2021;10:e1358. doi:10.1002/cti2.1358
17. Klümper N, Sikic D, Saal J, et al. C-reactive protein flare predicts response to anti-PD-(L)1 immune checkpoint blockade in metastatic urothelial carcinoma. Eur J Cancer. 2022;167:13–22. doi:10.1016/j.ejca.2022.02.022
18. Saal J, Bald T, Eckstein M, et al. Early C-reactive protein kinetics predicts immunotherapy response in non-small cell lung cancer in the phase III OAK trial. JNCI Cancer Spectr. 2023;7. doi:10.1093/jncics/pkad027
19. Beauchemin N, Arabzadeh A. Carcinoembryonic antigen-related cell adhesion molecules (CEACAMs) in cancer progression and metastasis. Cancer Metastasis Rev. 2013;32:643–671.
20. Nicholson BD, Shinkins B, Pathiraja I, et al. Blood CEA levels for detecting recurrent colorectal cancer. Cochrane Database Syst Rev. 2015;10:CD011134.
21. Primrose JN, Perera R, Gray A, et al. Effect of 3 to 5 years of scheduled CEA and CT follow-up to detect recurrence of colorectal cancer: the FACS randomized clinical trial. JAMA. 2014;311:263–270. doi:10.1001/jama.2013.285718
22. Iwanicki-Caron I, Di Fiore F, Roque I, et al. Usefulness of the serum carcinoembryonic antigen kinetic for chemotherapy monitoring in patients with unresectable metastasis of colorectal cancer. J Clin Oncol. 2008;26:3681–3686. doi:10.1200/JCO.2007.15.0904
23. Sorbye H, Dahl O. Transient CEA increase at start of oxaliplatin combination therapy for metastatic colorectal cancer. Acta Oncol. 2004;43:495–498. doi:10.1080/02841860410032380
24. Ailawadhi S, Sunga A, Rajput A, Yang GY, Smith J, Fakih M. Chemotherapy-induced carcinoembryonic antigen surge in patients with metastatic colorectal cancer. Oncology. 2006;70:49–53. doi:10.1159/000091184
25. Strimpakos AS, Cunningham D, Mikropoulos C, Petkar I, Barbachano Y, Chau I. The impact of carcinoembryonic antigen flare in patients with advanced colorectal cancer receiving first-line chemotherapy. Ann Oncol. 2010;21:1013–1019. doi:10.1093/annonc/mdp449
26. Seymour L, Bogaerts J, Perrone A, et al. iRECIST: guidelines for response criteria for use in trials testing immunotherapeutics. Lancet Oncol. 2017;18:e143–e152. doi:10.1016/S1470-2045(17)30074-8
27. Avery G. Biotin interference in immunoassay: a review for the laboratory scientist. Ann Clin Biochem. 2019;56:424–430. doi:10.1177/0004563219842231
28. Wauthier L, Plebani M, Favresse J. Interferences in immunoassays: review and practical algorithm. Clin Chem Lab Med. 2022;60:808–820. doi:10.1515/cclm-2021-1288
29. Maestranzi S, Przemioslo R, Mitchell H, Sherwood RA. The effect of benign and malignant liver disease on the tumour markers CA19-9 and CEA. Ann Clin Biochem. 1998;35(Pt 1):99–103. doi:10.1177/000456329803500113
30. Fukuda I, Yamakado M, Kiyose H. Influence of smoking on serum carcinoembryonic antigen levels in subjects who underwent multiphasic health testing and services. J Med Syst. 1998;22:89–93. doi:10.1023/A:1022643102208
31. Yang Y, Xu M, Huang H, et al. Serum carcinoembryonic antigen elevation in benign lung diseases. Sci Rep. 2021;11:19044. doi:10.1038/s41598-021-98513-8
32. An X, Ding PR, Xiang XJ, et al. Carcinoembryonic antigen surge in metastatic colorectal cancer patients responding to irinotecan combination chemotherapy. Biomarkers. 2010;15:243–248. doi:10.3109/13547500903477377
33. Tesniere A, Schlemmer F, Boige V, et al. Immunogenic death of colon cancer cells treated with oxaliplatin. Oncogene. 2010;29:482–491. doi:10.1038/onc.2009.356
34. Zitvogel L, Kepp O, Senovilla L, Menger L, Chaput N, Kroemer G. Immunogenic tumor cell death for optimal anticancer therapy: the calreticulin exposure pathway. Clin Cancer Res. 2010;16:3100–3104. doi:10.1158/1078-0432.CCR-09-2891
35. Pfirschke C, Engblom C, Rickelt S, et al. Immunogenic chemotherapy sensitizes tumors to checkpoint blockade therapy. Immunity. 2016;44:343–354. doi:10.1016/j.immuni.2015.11.024
36. Ostrup O, Dagenborg VJ, Rodland EA, et al. Molecular signatures reflecting microenvironmental metabolism and chemotherapy-induced immunogenic cell death in colorectal liver metastases. Oncotarget. 2017;8:76290–76304. doi:10.18632/oncotarget.19350
37. Abrahamsson H, Jensen BV, Berven LL, et al. Antitumour immunity invoked by hepatic arterial infusion of first-line oxaliplatin predicts durable colorectal cancer control after liver metastasis ablation: 8-12 years of follow-up. Int J Cancer. 2020;146:2019–2026. doi:10.1002/ijc.32847
38. Dagenborg VJ, Marshall SE, Yaqub S, et al. Neoadjuvant chemotherapy is associated with a transient increase of intratumoral T-cell density in microsatellite stable colorectal liver metastases. Cancer Biol Ther. 2020;21:432–440. doi:10.1080/15384047.2020.1721252
39. Høye E, Dagenborg VJ, Torgunrud A, et al. T cell receptor repertoire sequencing reveals chemotherapy-driven clonal expansion in colorectal liver metastases. Gigascience. 2022;12. doi:10.1093/gigascience/giad032
40. Erden G, Barazi AO, Tezcan G, Yildirimkaya MM. Biological variation and reference change values of CA 19-9, CEA, AFP in serum of healthy individuals. Scand J Clin Lab Invest. 2008;68:212–218. doi:10.1080/00365510701601699
41. Liu P, Zhao L, Zitvogel L, Kepp O, Kroemer G. Immunogenic cell death (ICD) enhancers-Drugs that enhance the perception of ICD by dendritic cells. Immunol Rev. 2023;321(1):7–19. doi:10.1111/imr.13269
42. Prete SP, Turriziani M, Massara MC, et al. Combined effects of 5-fluorouracil, folinic acid and oxaliplatin on the expression of carcinoembryonic antigen in human colon cancer cells: pharmacological basis to develop an active antitumor immunochemotherapy. J Exp Clin Cancer Res. 2008;27(5). doi:10.1186/1756-9966-27-5
43. Feng Z, Zhang X, Peng Z, Aghamajidi A, Wu Y, Hua X. Nanobody-Directed CEA-targeting CAR T cells eliminate gastrointestinal cancer xenografts. Cancer Immunol Res. 2025;13:1160–1171. doi:10.1158/2326-6066.CIR-24-0137
44. Katz SC, Moody AE, Guha P, et al. HITM-SURE: hepatic immunotherapy for metastases phase Ib anti-CEA CAR-T study utilizing pressure enabled drug delivery. J Immunother Cancer. 2020;8:e001097. doi:10.1136/jitc-2020-001097
45. Zhang W, Zhou L, Yu G, et al. Safety and efficacy of anti-CEA CAR-T cells to prolong relapse-free survival of colorectal cancer liver metastases patients after radical resection. J Clin Oncol. 2025;43(16):3541. doi:10.1200/JCO.2025.43.16_suppl.3541
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
BICDL1 Predicts Poor Prognosis and is Correlated with Methylation and Immune Infiltration in Colorectal Cancer
Luo H, Luo J, Ding N, Zhang T, He Y
Pharmacogenomics and Personalized Medicine 2023, 16:1109-1126
Published Date: 22 December 2023
CXCL11: A Novel Biomarker in Colorectal Cancer as Metastasis Predictor
Wibowo R, Sribudiani Y, Lukman K, Rudiman R, Ruchimat T, Sulthana BAAS, Purnama A, Wijaya A, Primastari E, Nugraha P
OncoTargets and Therapy 2025, 18:657-665
Published Date: 14 May 2025
Serum tRF5-23-GlyTCC-2 Functions as a Tumor Suppressor and Novel Biomarker for Colorectal Cancer
Lv X, Dai H, Wu Y, Yang J, Wang G, Wang X
Cancer Management and Research 2025, 17:2441-2457
Published Date: 27 October 2025
Machine Learning-Integrated Analysis of SULF1, CXCL8, and PBLD Expression as Discriminative Biomarkers for Early Detection and Prognosis in Colorectal Cancer
Li Y, Shi J, Mei C, Zhou F, Zhao H, Zhang L
International Journal of General Medicine 2025, 18:7285-7308
Published Date: 4 December 2025
Linoleic Acid Reduces Paclitaxel Chemosensitivity in Colorectal Cancer
Zhou B, Pan J, Wang M, Zhou P, Li Z, Cui J, Huang C, Wang L, Fan Z
Drug Design, Development and Therapy 2026, 20:577058
Published Date: 28 April 2026