Back to Journals » Journal of Inflammation Research » Volume 19
Blood Marker-Based Machine Learning Model for Survival Prediction in Patients with Pneumoconiosis: Construction and External Validation
Authors Huang Q, Feng M, Chen Z, Zhang J, Feng Z
Received 20 July 2025
Accepted for publication 5 February 2026
Published 26 February 2026 Volume 2026:19 555051
DOI https://doi.org/10.2147/JIR.S555051
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Cynthia Koziol-White
Qiuxiang Huang,1 Mei Feng,2 Ziwei Chen,1 Jian Zhang,3 Zhencheng Feng4
1Department of Respiratory Medicine, Guangzhou Twelfth People’s Hospital, Guangzhou, 510620, People’s Republic of China; 2Department of Occupational Disease, Hengyang Traditional Chinese Medicine Hospital, Hengyang, 421009, People’s Republic of China; 3Department of Respiratory Medicine, Hengyang Traditional Chinese Medicine Hospital, Hengyang, 421009, People’s Republic of China; 4Department of Orthopedics, Guangzhou Red Cross Hospital, Jinan University, Guangzhou, 510220, People’s Republic of China
Correspondence: Zhencheng Feng, Department of Orthopedics, Guangzhou Red Cross Hospital, Jinan University, Guangzhou, People’s Republic of China, Email [email protected]
Purpose: This study aimed to investigate the association between blood inflammatory markers, including C-reactive protein (CRP) and interleukin-6 (IL-6), and the short-term prognosis of pneumoconiosis, and to develop a multifactorial prediction model.
Patients and Methods: Clinical data of 813 pneumoconiosis patients admitted to two regional tertiary hospitals from October 2016 to August 2023 were retrospectively collected and randomly divided into a training set (n=568) and an external validation set (n=245). Variables were screened by least absolute shrinkage and selection operator (LASSO) regression, a multifactorial logistic regression column-line graph model was constructed, and the relationship between risk factors and prognosis was analyzed by multifactorial Cox regression and Kaplan-Meier survival curves. The model performance was verified by consistency index (C index), receiver operating characteristic (ROC) curve, calibration curve, decision curve analysis (DCA) and clinical impact curve (CIC).
Results: The mean age was 62.1 years in the training set and 63.3 years in the validation set, with mortality rates of 11.1% and 11.9%, respectively. LASSO regression identified age, dust exposure duration, dyspnea, blood oxygen saturation (SpO2), neutrophil count, CRP, and IL-6 as predictors. CRP (OR=1.028, 95% CI: 1.016– 1.040) and IL-6 (OR=1.020, 95% CI: 1.010– 1.030) were independent risk factors for poor short-term prognosis (both P< 0.001), consistent with Cox analysis. The model demonstrated excellent discrimination with AUCs of 0.905 in the training set and 0.920 in the validation set. Calibration showed good agreement between predicted and observed risks (Hosmer–Lemeshow P> 0.05). DCA and CIC indicated high clinical value. High CRP/IL-6 levels were associated with significantly reduced survival (log-rank P< 0.001).
Conclusion: The prediction model based on CRP, IL-6, and clinical characteristics effectively identifies pneumoconiosis patients at high risk of short-term poor prognosis, providing a reliable basis for early intervention due to its high discriminatory power and clinical applicability.
Keywords: pneumoconiosis, C-reactive protein, interleukin-6, prediction model, inflammation
Introduction
Pneumoconiosis is an occupational lung disease caused by long-term inhalation of mineral dust, commonly seen in miners, construction workers, and other occupationally exposed populations. With the acceleration of industrialization, the global prevalence of pneumoconiosis continues to rise. Statistics indicate that approximately 65,000 new cases of pneumoconiosis were reported worldwide in 2020, and this number is projected to increase to 88,000 by 2030.1 Patients often experience poor prognosis due to progressive pulmonary fibrosis and respiratory failure, with a five-year mortality rate as high as 20–40%.2,3 Pneumoconiosis not only poses a severe threat to patients’ lives but also imposes a significant socioeconomic burden, making it a major global challenge in occupational health.4 Therefore, early identification of high-risk patients for poor prognosis and timely intervention are crucial for improving clinical outcomes. However, effective and practical predictive tools remain lacking.5
Prolonged dust exposure is known to activate alveolar macrophages, triggering the release of key inflammatory mediators such as interleukin-6 (IL-6) and tumor necrosis factor-α (TNF-α), which in turn promote chronic inflammation and pulmonary fibrosis. Experimental and clinical studies have demonstrated that IL-6 plays a central role in the inflammatory microenvironment of fibrotic lung diseases, including pneumoconiosis.6,7
C-reactive protein (CRP), an acute-phase protein, has been found to be significantly associated with the rate of lung function decline,8 while interleukin-6 (IL-6) exacerbates pulmonary inflammation by promoting Th17 cell differentiation.9 Additionally, clinical characteristics such as dust exposure duration, blood oxygen saturation (SpO2), and dyspnea severity have been confirmed to be closely related to prognosis.10,11 However, existing predictive models mainly rely on single biomarkers or clinical indicators, failing to integrate multidimensional data, which limits their predictive performance.12
Although inflammatory markers such as the neutrophil-to-lymphocyte ratio (NLR) and platelet count have demonstrated predictive value in other respiratory diseases,13 their application in pneumoconiosis remains controversial.14 Notably, CRP and IL-6 are easily accessible and cost-effective inflammatory markers that have shown excellent prognostic value in infectious diseases and cancer.15,16 However, their synergistic role in multifactorial models for pneumoconiosis has not been well established. Moreover, traditional models often lack external validation, limiting their clinical applicability.17
Therefore, this study aims to construct and validate a nomogram prediction model for short-term poor prognosis in pneumoconiosis patients by integrating multicenter data with inflammatory markers (CRP, IL-6) and key clinical characteristics. The findings will provide a scientific basis for early risk stratification, personalized treatment, and the optimization of medical resource allocation.
Methods
Participants and Study Design
This study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committees of the National Institute of Occupational Disease Prevention and the Guangzhou twelfth People’s Hospital. Informed consent was waived. Retrospective data from pneumoconiosis patients admitted to two regional occupational disease prevention centers from October 2016 to August 2023 were collected, with data from guangzhou twelfth People’s Hospital used as the training set (n=568) and data from Hengyang Traditional Chinese Medicine Hospital’s Occupational Disease Department as the validation set (n=245). The training set was obtained from Guangzhou Twelfth People’s Hospital between October 2016 and December 2021, while the validation set was collected from Hengyang Traditional Chinese Medicine Hospital between January 2022 and August 2023. These two centers are located in different provinces and serve distinct patient populations, ensuring both temporal and geographic independence of the validation cohort. Inclusion criteria were: (1) Clinical diagnosis according to the “Diagnostic Criteria for Pneumoconiosis” (GBZ 70); (2) Age ≥18 years; (3) Availability of complete baseline clinical data and follow-up information (including pulmonary function and imaging reports) (Figure 1).
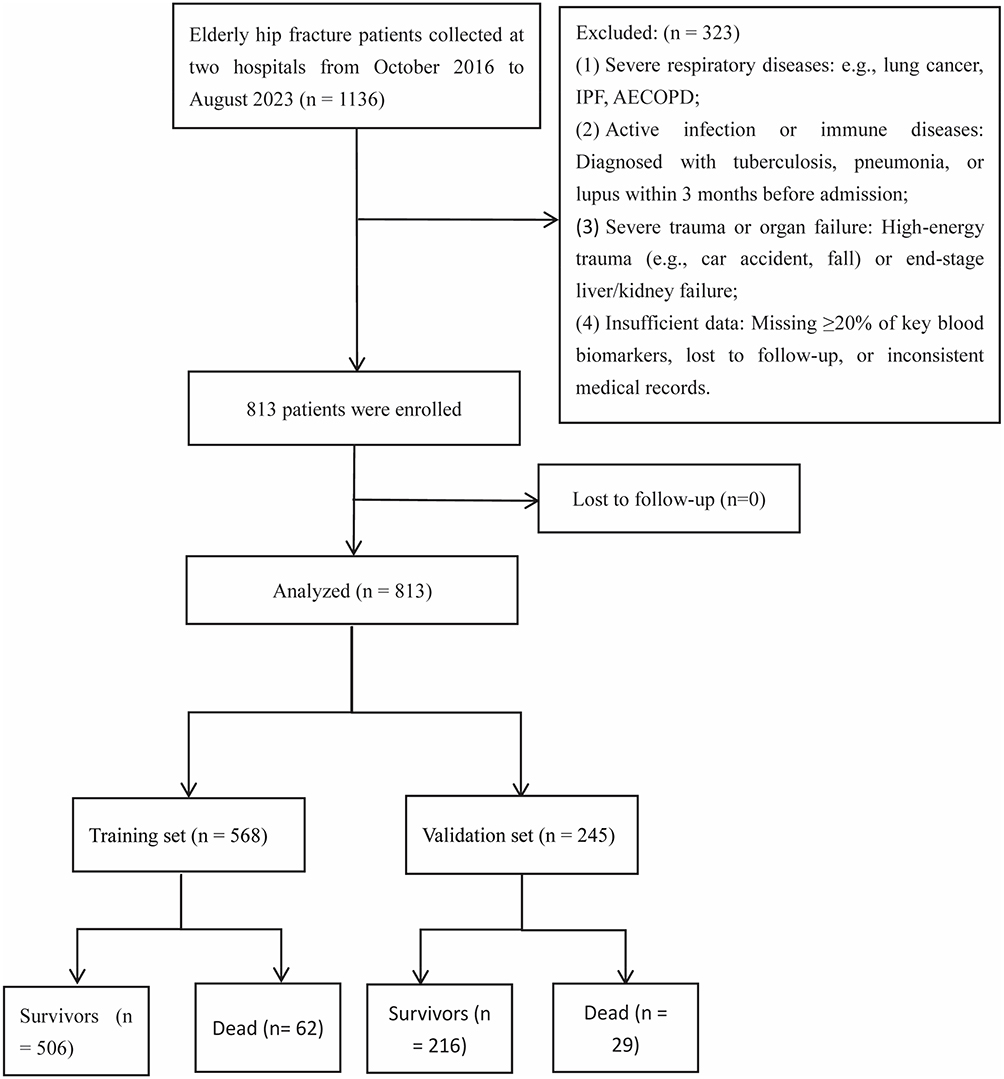 |
Figure 1 Patient enrollment flowchart. |
The primary endpoint event was all-cause mortality. During the follow-up period, patients were assessed every three months via phone and/or outpatient visits. The endpoint event was confirmed by healthcare professionals and the patient’s family members.
The outcome variable (“survived” vs “died”) was defined based on a 20-month follow-up period. Only deaths that occurred within 20 months after enrollment were considered “death” events for the short-term prediction model. Patients who were alive or lost to follow-up before 20 months were classified as “survived”. Cases with completely missing outcome information were excluded from analysis.
Data Collection
Data for all pneumoconiosis patients were independently reviewed by two researchers according to the inclusion criteria, and discrepancies were resolved through third-party expert review. The following information was extracted from electronic medical records and paper archives and entered into a standardized case report form:
- Demographic variables: age, gender, smoking, drinking, and history of influenza vaccination, etc.;
- Clinical data: dyspnea, chest pain, bronchoalveolar lavage, hemoptysis, and anti-TB treatment, etc.;
- Blood tests: serum sodium, potassium, red cell distribution width (RDW), hemoglobin, platelets, fibrinogen, white blood cells, neutrophils, erythrocyte sedimentation rate, monocytes, CRP, IL-6, etc.
The duration of dust exposure was defined as the total number of months the patient had been exposed to occupational dust. This was recorded during structured interviews with occupational physicians and verified using employment or insurance documentation when possible.
Statistical Analysis
The overall missing rate for baseline and clinical variables was < 0.5%, and all records were cross-checked with the hospital information system (HIS) to ensure data completeness. Missing values that could not be verified were excluded from the analysis.
Continuous variables were assessed for normality using the Shapiro–Wilk test. Normally distributed data were presented as mean ± standard deviation, and non-normally distributed data were presented as median (interquartile range, IQR). Categorical variables were described using frequency (percentage). The comparison of continuous variables between groups was performed using Student’s t-test (for normal distribution) or the Mann–Whitney U-test (for non-normal distribution), while categorical variables were compared using the chi-square test. Pearson correlation analysis was used to calculate the correlation between inflammatory markers.
For categorical variables (eg, dyspnea, coronary heart disease), coding was defined as 1 = presence and 0 = absence, with the “absence” group serving as the reference category in regression analyses.
To screen for independent risk factors, LASSO regression (10-fold cross-validation) was used for dimensionality reduction on the training set data. The optimal regularization parameter (λ) was selected based on partial likelihood deviance, and the λ.1se value (the largest λ within one standard error of the minimum cross-validated error) was chosen to promote model simplicity and prevent overfitting. Subsequently, multifactorial logistic regression was performed to construct a prediction model for short-term poor prognosis in pneumoconiosis patients, and a nomogram was plotted. The model’s discrimination and calibration ability were assessed using the concordance index (C-index), receiver operating characteristic curve (ROC), calibration curve, and Hosmer-Lemeshow goodness-of-fit test. The 95% confidence intervals of AUC values were estimated using 1000 bootstrap iterations with replacement sampling, where each resample was of the same size as the original dataset. Decision curve analysis (DCA) and clinical impact curve (CIC) were used to quantify the clinical net benefit and applicability of risk threshold.
In survival analysis, Kaplan-Meier survival curves were plotted, and differences between groups were compared using the Log rank test. Multifactorial Cox regression analysis was used to assess the association between independent risk factors and mortality risk.
All statistical analyses were performed using SPSS 26.0, GraphPad Prism 9.0, and R 4.3.0.
Results
Comparison of General Clinical Data of Pneumoconiosis Patients in Training and Validation Sets
A total of 813 patients were included in this study, with 568 in the training set and 245 in the validation set (Figure 1). The average age of patients in the training set was 62.1 years, with 312 males (54.9%), while the average age in the validation set was 63.3 years, with 123 males (50.2%). The mortality rates in the training set and validation set were 11.1% and 11.9%, respectively. The clinical characteristics of patients in both the training and validation sets are shown in Table 1. The distribution of features was similar between the two groups. Additionally, in both the training and validation sets, CRP and IL-6 levels were significantly higher in the deceased group compared to the survivors (Figure 2A–D). The differences were tested using the Mann–Whitney U-test, with p-values < 0.001 for all comparisons. Given the limited number of predefined comparisons, no p-value adjustments were applied. These findings suggest that high levels of CRP and IL-6 may be associated with an increased risk of death in pneumoconiosis patients, indicating that CRP and IL-6 could be important biomarkers for prognostic stratification.
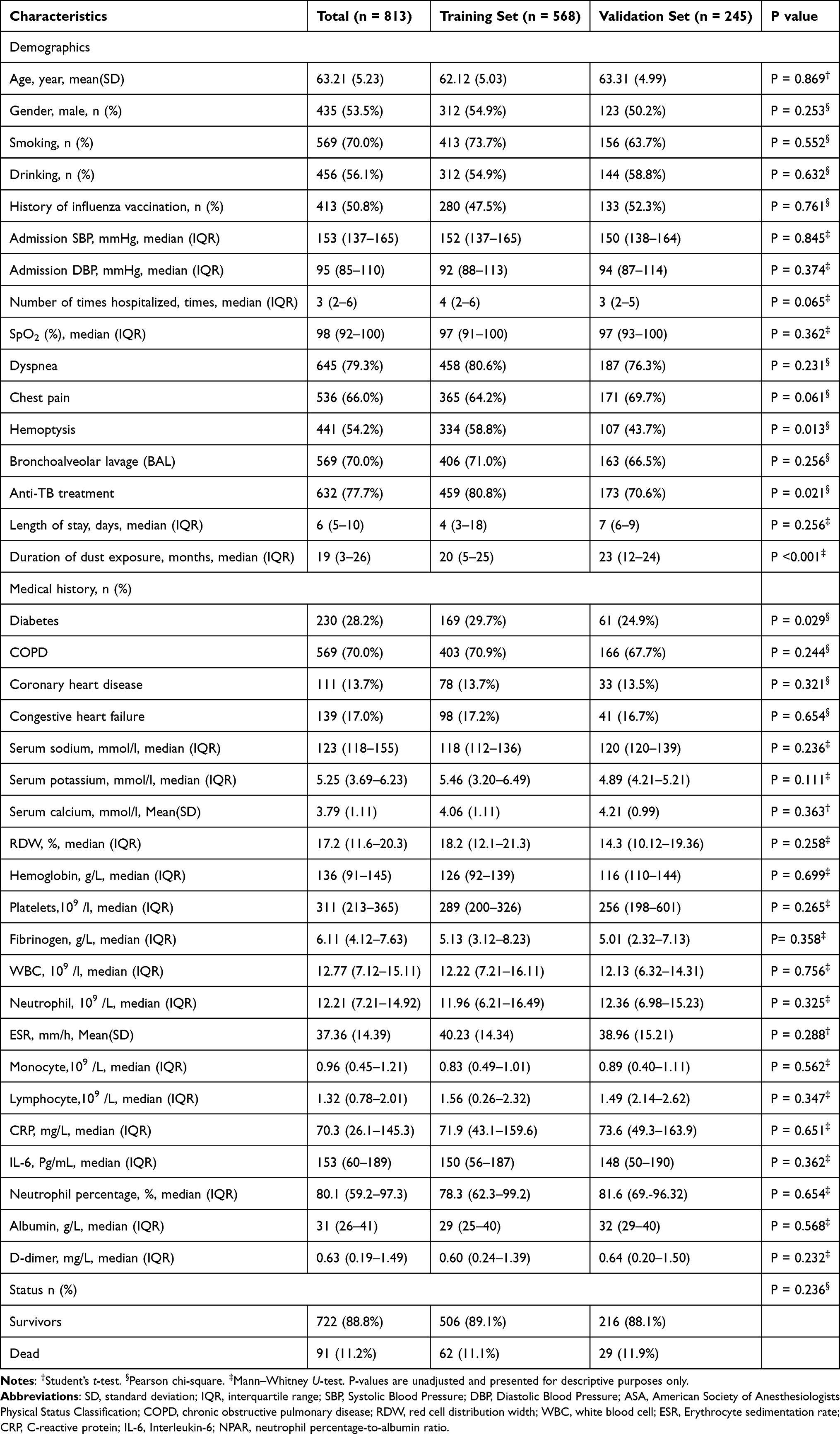 |
Table 1 Characteristics of Patients in the Training and Validation Cohorts |
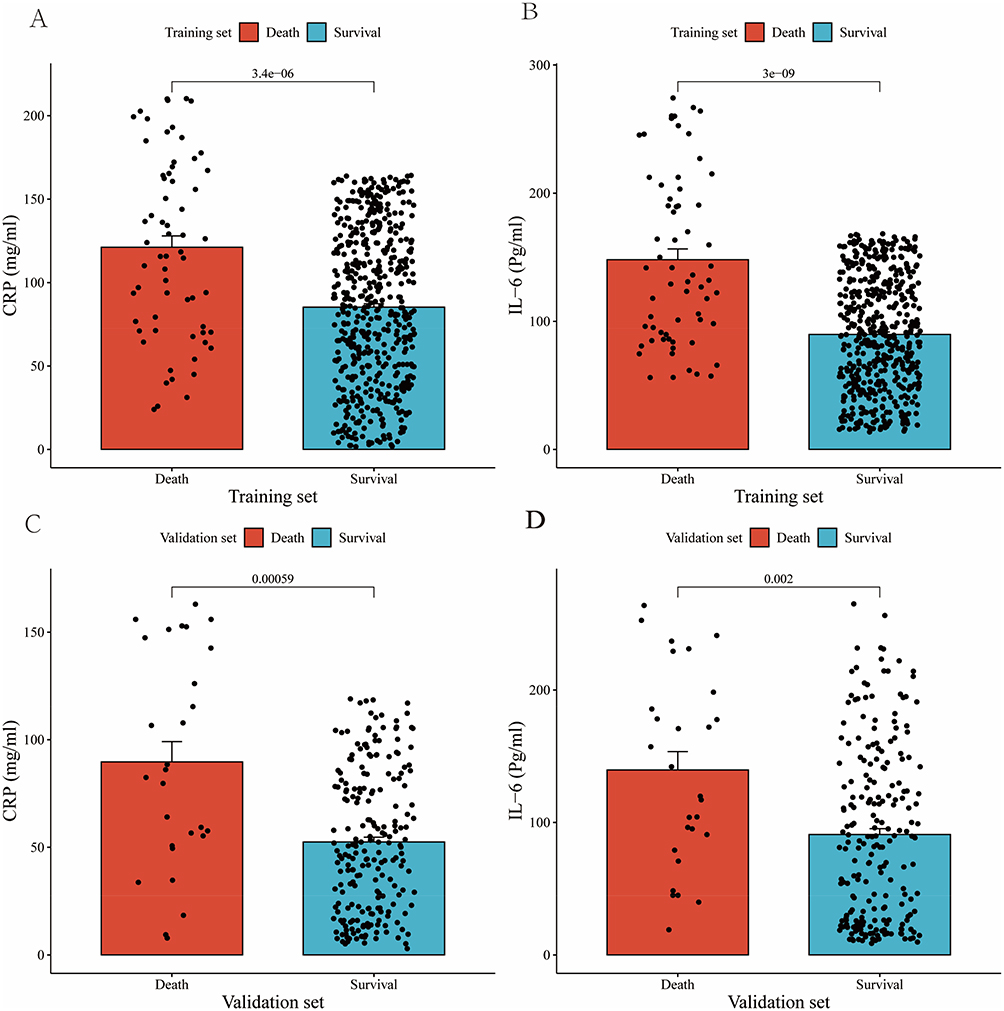 |
Figure 2 CRP and IL-6 levels at admission in the training set (A and B) and validation set (C and D). |
Lasso Regression Analysis for Risk Factor Selection
Pearson correlation analysis was used to calculate the correlation coefficients between the inflammatory markers, and the results showed a high correlation between the markers (Figure 3). Therefore, to identify independent risk factors, we performed Lasso regression analysis on all variables in the training set to identify factors associated with poor prognosis in pneumoconiosis patients. Ultimately, nine variables with the optimal lambda value were selected: age, coronary heart disease, duration of dust exposure, dyspnea, SpO2, serum potassium, neutrophil, CRP, and IL-6 (Figure 4A and B). The names and coefficients of the nine selected variables are provided in Supplementary_Material (Supplementary Tables 1 and 2).
 |
Figure 3 Pairwise Pearson correlation coefficients between inflammatory markers. Blue represents a positive correlation, while red indicates a negative correlation. Darker shades correspond to stronger correlation coefficients. Abbreviations: CRP, C-reactive protein; IL-6, interleukin-6; SpO2, peripheral capillary oxygen saturation; RDW, red cell distribution width; WBC, white blood cell count; PLT, platelet count; ESR, erythrocyte sedimentation rate. |
 |
Figure 4 LASSO regression analysis was conducted for feature selection on the candidate variables using a 10-fold cross-validation method. (A) Ten-fold cross-validation for selecting the optimal tuning parameter (lambda) in the LASSO regression model. The left vertical dashed line indicates the lambda value that yields the minimum mean cross-validated error, while the right dashed line represents the most regularized model within one standard error of the minimum. Partial likelihood deviance is used as a measure of model error, with lower values indicating better performance. Red dots denote the mean deviance, and error bars represent ±1 standard error (SE). (B) LASSO coefficient profiles of the 25 candidate variables. Each curve represents the trajectory of a variable’s coefficient as a function of the log (lambda). As the penalty parameter lambda increases, more coefficients shrink toward zero, indicating variable selection through regularization. |
Multivariable Logistic Regression for Risk Factor Selection
To identify independent risk factors for predicting short-term poor prognosis in pneumoconiosis patients, we further performed multivariable logistic regression analysis on the results of Lasso regression. Ultimately, the following variables were significantly associated with short-term poor prognosis in patients: Age (OR = 1.096, 95% CI = 0.179–1.188, P < 0.001), Coronary heart disease (OR = 0.462, 95% CI = 0.179–1.146, P = 0.109), Duration of dust exposure (OR = 1.266, 95% CI = 1.161–1.380, P < 0.001), Dyspnea (OR = 0.127, 95% CI = 0.044–0.365, P < 0.001), SpO2 (OR = 0.703, 95% CI = 0.571–0.865, P < 0.001), Serum potassium (OR = 1.612, 95% CI = 0.998–2.605, P = 0.051), Neutrophil (OR = 1.121, 95% CI = 1.070–1.373, P = 0.003), CRP (OR = 1.028, 95% CI = 1.016–1.040, P < 0.001), and IL-6 (OR = 1.020, 95% CI = 1.010–1.030, P < 0.001) (Figure 5).
 |
Figure 5 Forest plot of multivariable logistic regression analysis. Data are shown as odds ratios (ORs) with 95% confidence intervals (CIs). For categorical variables (eg, dyspnea and coronary heart disease), 1 = presence and 0 = absence, with the “absence” group as the reference. Abbreviations: CRP, C-reactive protein; IL-6, interleukin-6; SD, standard deviation. |
Multivariable Logistic Regression Model Development and Bootstrap Validation for Prognostic Prediction
In the training set, seven variables (age, duration of dust exposure, dyspnea, SpO2, neutrophil, CRP, and IL-6) were selected for multivariable logistic regression analysis to construct a nomogram for predicting short-term adverse prognosis in pneumoconiosis patients. The model demonstrated high predictive accuracy through bootstrap validation (Figure 6).
 |
Figure 6 Nomogram model for predicting the short-term prognosis of pneumoconiosis patients. |
ROC Curve Analysis of Predictive Factors
In the training set, variables with P < 0.05 from the multivariable logistic regression analysis were included in ROC curve analysis (Figure 7 and Table 2). The results indicated that the predictive performance of CRP and IL-6 was significantly superior to that of other variables, with AUC values of 0.885 (95% CI: 0.802–0.965) and 0.877 (95% CI: 0.821–0.942), respectively, both approaching 0.9, indicating strong discriminative ability. In contrast, the AUC values for other variables were all below 0.8 (eg, dust exposure duration 0.803, age 0.717), with Neutrophil (0.652) and Dyspnea (0.636) showing the lowest predictive performance. We further constructed a traditional multivariable logistic regression model without machine learning, which yielded an AUC of 0.750—substantially lower than that of the LASSO-based machine learning model (AUC = 0.885) (Supplementary_Material; Figures S1–S4).
 |
Table 2 Comparison of AUCs of CRP, IL-6, and Other Influencing Factors in the Training Set |
 |
Figure 7 ROC curves based on the results of multivariable logistic regression analysis in the training set. |
Receiver Operating Characteristic (ROC) Curves and Calibration Curves of the Multivariable Logistic Regression Models
In the training set, the ROC curve area under the curve (AUC) for the combined prediction model was 0.905 (95% CI: 0.901–0.939) (Figure 8A), indicating strong discriminative ability for predicting short-term adverse prognosis in pneumoconiosis patients. The concordance index (C-index) in the training set was 0.918 (95% CI: 0.880–0.954), calculated using 1000 bootstrap iterations, further confirming the model’s discriminative ability.In the validation set, the ROC curve AUC for the combined prediction model was 0.920 (95% CI: 0.906–0.930) (Figure 8B), indicating that the model has high discriminative ability for predicting short-term adverse prognosis in pneumoconiosis patients, with good sensitivity and specificity. In the validation set, the C-index was 0.926 (95% CI: 0.882–0.962), supporting the robustness and generalizability of the model.
 |
Figure 8 ROC curves are used to evaluate the prediction effect of (A) training set and (B) validation set. |
The calibration curve showed that the predicted probabilities from the nomogram closely matched the actual observed probabilities, suggesting excellent predictive accuracy (Figure 9A for the training set; Figure 9B for the validation set). The Hosmer–Lemeshow goodness-of-fit test results demonstrated good consistency of the model in assessing short-term adverse prognosis in pneumoconiosis patients (training set P = 0.214; validation set P = 0.168).
 |
Figure 9 Calibration curves for the logistic regression model in the training (A) and validation (B) sets. Notes: The predicted probabilities are plotted against the observed event probabilities. The calibration curves were generated using 1000 bootstrap resamples. The dashed diagonal line represents perfect calibration. The mean absolute error (MAE) between predicted and observed probabilities was calculated to assess calibration accuracy. |
Decision Curves and Clinical Impact Curves for the Multivariable Logistic Regression Models
In both the training and validation sets, predictive models were constructed based on independent risk factors such as C-reactive protein (CRP) and interleukin-6 (IL-6), and the clinical applicability of the models was evaluated through decision curve analysis (DCA) and clinical impact curve (CIC). The results showed that, compared to traditional clinical indicators, the model provided significant additional net clinical benefit in predicting short-term adverse prognosis in pneumoconiosis patients (Figure 10A and B). Further analysis of the CIC revealed that when the risk threshold reached 0.6 in both the training and validation sets, the prediction curve and the actual event curve gradually converged (Figure 11A and B).
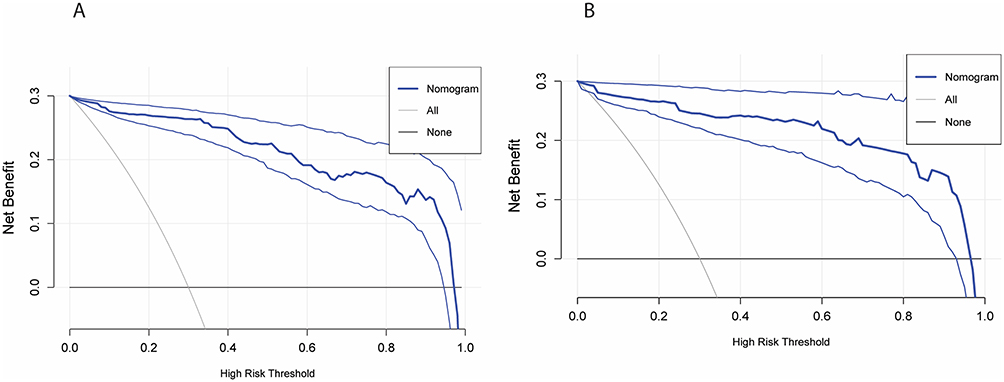 |
Figure 10 (A) Decision curve analysis for assessing prognosis in a training set; (B) Decision curve analysis for assessing prognosis in a validation set. |
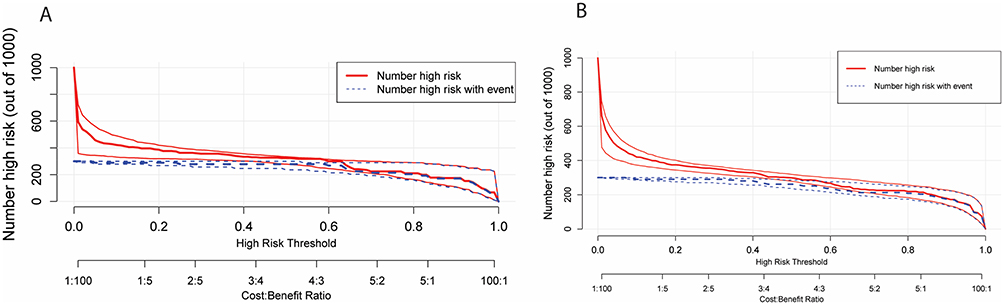 |
Figure 11 (A) Clinical impact curves for prognosis assessment in the training set; (B) Clinical impact curves for prognosis assessment in the validation set. |
Kaplan-Meier Survival Analysis and Multivariable Cox Regression Analysis
All patients were followed for up to 20 months. The median follow-up duration was 14.6 months (interquartile range [IQR]: 9.2–17.9) in the training set and 13.8 months (IQR: 8.7–17.2) in the validation set. Survival status was determined based on all-cause mortality occurring during this follow-up period. The number of patients at risk and the number censored at each time point are displayed in the Kaplan–Meier plots (Figure 12A–D).
 |
Figure 12 Kaplan–Meier survival curves of patients with high and low levels of CRP and IL-6. (A) CRP in the training set; (B) IL-6 in the training set; (C) CRP in the validation set; (D) IL-6 in the validation set. Censored cases are shown as vertical tick marks on the survival curves. The number of patients at risk and censored at each time point (0, 5, 10, 15, and 20 months) is displayed below each graph. |
In the training set, variables selected through Lasso regression were included in multivariable Cox regression analysis. The results showed that Age (HR = 1.116, 95% CI: 1.012–1.544, P < 0.001), Duration of dust exposure (HR = 1.211, 95% CI: 1.102–1.368, P < 0.001), Dyspnea (HR = 0.131, 95% CI: 0.066–0.632, P < 0.001), SpO2 (HR = 0.798, 95% CI: 0.623–0.881, P < 0.001), Neutrophil (HR = 1.229, 95% CI: 1.071–1.312, P < 0.001), CRP (HR = 1.013, 95% CI: 1.003–1.056, P < 0.001), and IL-6 (HR = 1.026, 95% CI: 1.010–1.030, P < 0.001) were all independent predictors of short-term adverse prognosis in pneumoconiosis patients (Table 3). Additionally, the Kaplan-Meier survival curves in both the training and validation sets showed that patients in the high CRP group and high IL-6 group had significantly higher risks of short-term adverse prognosis compared to those in the low CRP and low IL-6 groups (P < 0.001) (Figure 12A–D).
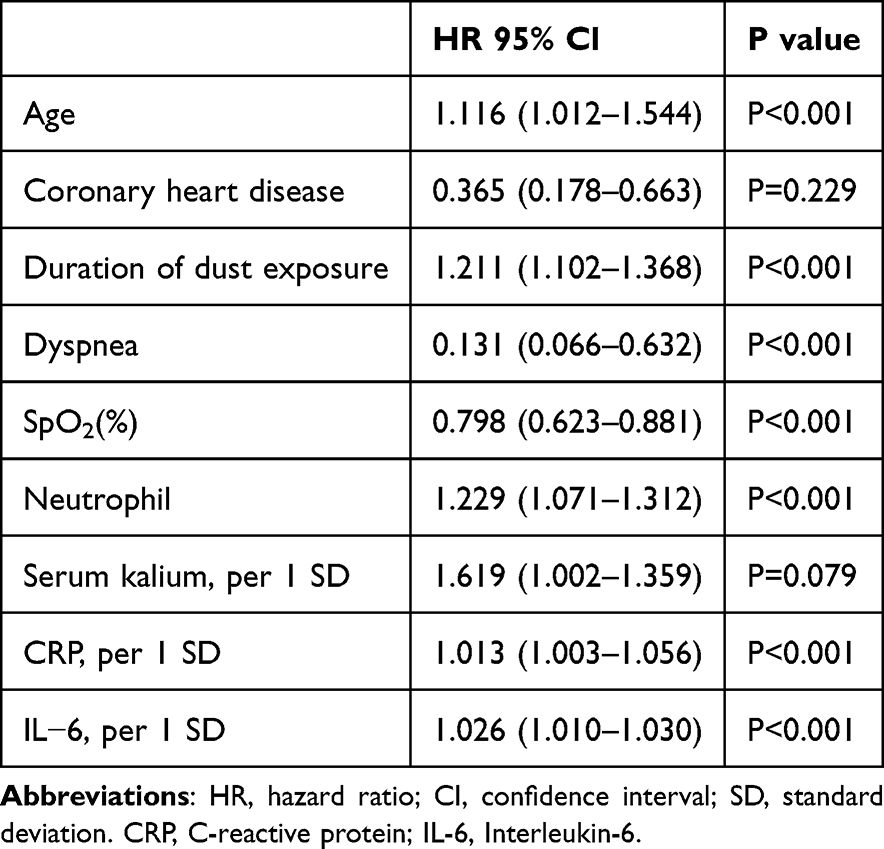 |
Table 3 Multivariable Cox Regression Analysis |
Contribution of CRP and IL-6 to Model Discrimination and Clinical Utility
To further validate the contribution of CRP and IL-6, a comparison model excluding these two predictors was constructed. The AUC values of the null model were 0.861 (95% CI 0.844–0.876) and 0.868 (95% CI 0.851–0.882) in the training and validation sets, respectively, both lower than those of the full model (0.905 and 0.920). The decision curve analysis showed that the full model achieved greater net benefit across most threshold probabilities, while the clinical impact curve demonstrated a closer match between predicted high-risk individuals and observed events, suggesting better clinical applicability (Supplementary_Material; Figures S5 and S6).
Discussion
In this study, we developed a predictive model for short-term adverse prognosis in pneumoconiosis, with a focus on analyzing the prognostic role of C-reactive protein (CRP) and interleukin-6 (IL-6) in pneumoconiosis patients. Through Lasso regression and multivariable logistic regression analysis, we found that CRP and IL-6 are significant independent risk factors, and these two biomarkers outperformed other clinical variables in predicting short-term adverse prognosis in pneumoconiosis patients. Our results not only align with some existing studies but also provide new perspectives, revealing the important role of inflammatory responses in the prognosis of pneumoconiosis.
To better understand their selection and performance, we further examined the modeling process in detail. In this study, CRP and IL-6 were selected as core biomarkers based on both statistical performance and clinical practicality. Among 12 blood variables initially included—such as fibrinogen—only neutrophils, CRP, and IL-6 were retained after LASSO regression. CRP and IL-6 showed the highest AUCs (both >0.8), indicating superior predictive power for short-term poor prognosis in pneumoconiosis. The high AUC values of CRP and IL-6 emphasize the central role of inflammatory markers in independent risk prediction and provide biological evidence supporting their combined use for diagnostic modeling and clinical risk stratification. In addition, although markers such as TNF-α are biologically relevant in pulmonary inflammation, they were not consistently available across the study cohort, with a relatively high rate of missing data and potential variability in retrospective records. As such, they were not included in the final analysis.
As an acute-phase reactant, C-reactive protein (CRP) has been widely used for prognostic evaluation in various inflammatory diseases.18–20 Long-term exposure to dust in pneumoconiosis patients activates the immune system, leading to persistent inflammation and elevated CRP levels.21,22 A previous study showed that CRP can enhance both local and systemic inflammatory responses by activating the complement system and promoting the aggregation of monocytes and neutrophils, which is closely related to pulmonary inflammation and fibrosis in pneumoconiosis patients.23 Our study found that CRP levels are significantly associated with short-term adverse prognosis in pneumoconiosis patients, with markedly higher levels observed in the mortality group compared to the survival group. This finding is consistent with the study by Cho et al, which also demonstrated a significant correlation between elevated CRP levels and increased mortality in pneumoconiosis patients.24 As a systemic inflammatory marker, CRP is elevated in pneumoconiosis and may reflect persistent systemic inflammation and unfavorable prognosis.25,26 In our study, the combination of CRP and IL-6 was identified as a highly predictive risk factor, particularly in AUC assessments, where CRP demonstrated a predictive efficacy of 0.885, significantly outperforming other variables such as dust exposure duration and age. This finding supports the central role of CRP in prognostic assessment for pneumoconiosis patients. Compared to the study by Yang et al, which developed a prediction model for pneumoconiosis risk using serum and urinary biomarkers in asbestos-exposed workers, our study differs in both objective and methodology.27 Yang’s model focused on early diagnosis in high-risk individuals, while our work aims to predict short-term prognosis among confirmed pneumoconiosis patients to support clinical decision-making. Importantly, our model was constructed using machine learning (LASSO regression) for more robust variable selection and predictive performance. In addition, we validated the model using a temporally and geographically independent external cohort, which enhances its generalizability and clinical applicability. Furthermore, unlike Yang’s model, which relied on non-routine biomarkers, we used widely available inflammatory markers (CRP and IL-6), making our approach more practical for real-world clinical settings.
However, other studies have presented different perspectives on the role of CRP. For example, Zeller et al found that elevated CRP levels in pneumoconiosis patients are not directly associated with mortality risk but are instead linked to complications such as cardiovascular diseases.28 Similarly, Koziarska-Rościszewska et al demonstrated that high-sensitivity CRP levels are closely related to metabolic disorders and cardiovascular disease risk factors.26 These findings suggest that CRP elevation may be closely related to comorbidities in pneumoconiosis patients, making it insufficient as a standalone prognostic marker. This distinction may explain the differences between our findings and those of Zeller et al. While our study demonstrates that CRP remains a strong prognostic predictor as an individual marker, we did not account for other potential factors influencing CRP levels, such as comorbid conditions. Therefore, in clinical applications, CRP should be interpreted in conjunction with the patient’s overall health status to enhance its clinical utility as a prognostic biomarker.
IL-6 is another critical inflammatory biomarker that has received widespread attention for its role in pneumoconiosis patients.29,30 Long-term exposure to dust can lead to lung cell damage and oxidative stress, which in turn induces the release of IL-6.31,32 By binding to its receptor, IL-6 activates the JAK-STAT signaling pathway, promoting the production of cytokines and exacerbating the inflammatory response.33 Our study found that IL-6 levels were significantly higher in the mortality group than in the survival group. Moreover, in multivariable logistic regression analysis, IL-6 was identified as an independent prognostic factor, significantly associated with short-term adverse outcomes in pneumoconiosis patients, similar to CRP. This finding aligns with prior work in patients with silicosis, a subtype of pneumoconiosis, showing that elevated IL-6 levels are associated with worse survival outcomes.25 As a pro-inflammatory cytokine, IL-6 reflects the body’s immune response and inflammatory state,34 making it a valuable biomarker with potential clinical utility in predicting disease progression and prognosis in pneumoconiosis patients.
However, some studies have proposed different interpretations regarding the role of IL-6. Prior evidence indicates that elevated IL-6 levels are associated with increased disease severity and fibrotic progression in pneumoconiosis,35 with mechanistic findings in silicosis supporting a role for IL-6 in chronic inflammatory and fibrotic remodeling processes.7 This finding suggests that IL-6 may be more suitable as a biomarker for assessing the long-term prognosis of pneumoconiosis patients rather than serving as an indicator of short-term prognosis. We believe that this discrepancy may be due to the fact that IL-6 levels are influenced by multiple factors, including a patient’s immune status, comorbidities, and treatment variations. Additionally, IL-6 elevation may be closely related to the chronic inflammatory process of the disease,36,37 which could limit its predictive ability in the early stages. Therefore, when using IL-6 as a short-term prognostic marker, it is essential to consider the overall clinical course of the patient.
In our study, the multifactorial prediction model incorporating CRP and IL-6 demonstrated strong predictive ability. Compared to traditional clinical indicators such as age, duration of dust exposure, and dyspnea, CRP and IL-6 exhibited significant advantages in distinguishing short-term adverse outcomes in patients with pneumoconiosis. ROC curve analysis showed that the AUC values for CRP and IL-6 were 0.885 and 0.877, respectively, both approaching 0.9, indicating strong predictive performance. These results indicate that the model can reliably identify patients with potential adverse prognosis within clinically relevant high-risk thresholds, suggesting its good clinical applicability and effectiveness. To evaluate the added value of our LASSO-based machine learning model, we also developed a traditional logistic regression model using the same dataset. This further indicates that the machine learning approach offers clear advantages in variable selection and predictive performance, providing a superior tool for clinical risk assessment. Furthermore, we assessed the clinical applicability of this model using decision curve analysis (DCA) and clinical impact curve (CIC) analysis, and the results demonstrated that the model provides significant clinical net benefit to patients. Similar studies have also supported our findings. Previous studies have shown that elevated CRP and IL-6 levels in patients with pneumoconiosis are closely associated with chronic systemic inflammation and may serve as effective prognostic indicators.25 These findings further validate the effectiveness of our multifactorial prediction model, suggesting that CRP and IL-6 are not only markers of inflammation but also powerful tools for clinical prognostic assessment.
The strengths of this study are as follows: First, our study included a relatively large sample size and integrated data from two regional medical centers, reducing selection bias and enhancing the representativeness and reliability of the findings. Second, we employed multiple statistical analysis methods, including Lasso regression, ROC curve analysis, and decision curve analysis (DCA), to comprehensively evaluate the independent role of CRP and IL-6 in predicting short-term adverse outcomes in patients with pneumoconiosis, providing more robust evidence for clinical practice. This temporal and regional separation between the training and validation sets enhances the generalizability and credibility of our model as a truly external validation. More importantly, unlike studies that focus solely on a single inflammatory biomarker or traditional clinical variables, our multifactorial prediction model not only enables a more accurate assessment of pneumoconiosis prognosis but also demonstrates good clinical feasibility and applicability. Finally, we performed internal validation of the model to ensure the robustness and reproducibility of the results.
Although this study has certain strengths, it also has some limitations. First, as a retrospective study, data collection was constrained by existing medical records. Future prospective, multicenter studies are needed to further validate our findings.
Additionally, data on lung function (eg, FVC, FEV1) and disease severity were not consistently available for all patients in this retrospective dataset. Including these variables would have substantially reduced the effective sample size and might have introduced selection bias; therefore, they were not incorporated into the final model. This limitation has been clearly acknowledged, and future studies with more comprehensive clinical datasets are warranted to further evaluate their impact on model performance.
Another limitation of our study is that we used a binary classification outcome (survived vs died) without explicitly accounting for varying follow-up times in the main predictive model. Although survival time was analyzed using Cox regression and Kaplan–Meier methods, the logistic regression model may still be influenced by censoring-related bias. Future studies may consider using fixed-time endpoints, such as 1-year survival, or conducting sensitivity analyses to assess the robustness of the model under different follow-up durations. Second, we did not include other potential prognostic factors for pneumoconiosis, such as additional inflammatory markers, genetic factors, or imaging indicators, which may limit a comprehensive understanding of the disease mechanism. Future research could integrate multi-omics data to develop a more precise predictive model. Moreover, the data in this study were primarily derived from Chinese patients, and it remains unclear whether the predictive performance of the model would be consistent across different ethnicities or regional populations. Although the training and validation cohorts were from two independent institutions, their similar clinical profiles may reflect standardized diagnostic and treatment practices in China. This could explain the model’s strong performance in external validation. Future studies should test the model in more heterogeneous populations to better evaluate its generalizability. Additionally, we did not perform multiple testing correction when comparing CRP and IL-6 levels across outcome groups, given the limited number of predefined comparisons. This decision was made to avoid overadjustment and preserve statistical power. Nevertheless, we acknowledge that this may increase the risk of false-positive results, and therefore the findings should be interpreted with caution and validated in future studies.
Conclusion
This study demonstrates that CRP and IL-6 levels play a crucial role in the short-term adverse prognosis of pneumoconiosis patients, providing strong support for the early clinical identification of high-risk patients.
Data Sharing Statement
The raw data supporting the conclusions of this article will be made available by the authors without undue reservation.
Ethics Statement
The studies involving human participants were approved by the Ethics Committee of Guangzhou Twelfth People’s Hospital and the Ethics Committee of Hengyang Traditional Chinese Medicine Hospital’s Occupational Disease Department. Written informed consent from the participants or their legal guardians was not required in accordance with national legislation and institutional requirements, as only fully anonymized retrospective data were used. No identifiable images or personal information were included in this manuscript.
Acknowledgments
We appreciate the help and support from all participants who participated in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Guangzhou Health Science and Technology General Guidance Program (Grant Number 20251A010037) to Qx H, and Guangzhou Municipal Science and Technology Bureau (Grant Number 2025A03J3379), Guangzhou Health Science and Technology General Guidance Program (Grant Number 20231A010013) to Zc.F.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Wang H, Ye Q, Zhang H, Sun X, Li T. Prevention and treatment of pneumoconiosis in the context of healthy China 2030. China CDC Weekly. 2023;5:927. doi:10.46234/ccdcw2023.162
2. Cullinan P, Reid P. Pneumoconiosis. Primary Care Respir J. 2013;22:249–18. doi:10.4104/pcrj.2013.00055
3. Jeganathan N, Smith RA, Sathananthan M. Mortality trends of idiopathic pulmonary fibrosis in the United States from 2004 through 2017. Chest. 2021;159:228–238. doi:10.1016/j.chest.2020.08.016
4. Min L, Mao Y, Lai H. Burden of silica-attributed pneumoconiosis and tracheal, bronchus & lung cancer for global and countries in the national program for the elimination of silicosis, 1990–2019: a comparative study. BMC Public Health. 2024;24:571. doi:10.1186/s12889-024-18086-9
5. Lou H-R, Wang X, Gao Y, Zeng Q. Comparison of ARIMA model, DNN model and LSTM model in predicting disease burden of occupational pneumoconiosis in Tianjin, China. BMC Public Health. 2022;22:2167. doi:10.1186/s12889-022-14642-3
6. Hamilton RF, Thakur SA, Holian A. Silica binding and toxicity in alveolar macrophages. Free Radic Biol Med. 2008;44:1246–1258. doi:10.1016/j.freeradbiomed.2007.12.027
7. Liu -T-T, Sun H-F, Han Y-X, Zhan Y, Jiang J-D. The role of inflammation in silicosis. Front Pharmacol. 2024;15:1362509. doi:10.3389/fphar.2024.1362509
8. Li F, Deng J, Song Y, et al. Pulmonary fibrosis in patients with COVID-19: a retrospective study. Front Cell Infect Microbiol. 2022;12:1013526. doi:10.3389/fcimb.2022.1013526
9. She YX, Yu QY, Tang XX. Role of interleukins in the pathogenesis of pulmonary fibrosis. Cell Death Discovery. 2021;7:52. doi:10.1038/s41420-021-00437-9
10. Park Y, Ahn C, Kim T-H. Occupational and environmental risk factors of idiopathic pulmonary fibrosis: a systematic review and meta-analyses. Sci Rep. 2021;11:4318. doi:10.1038/s41598-021-81591-z
11. Shen L, Zhang Y, Su Y, et al. New pulmonary rehabilitation exercise for pulmonary fibrosis to improve the pulmonary function and quality of life of patients with idiopathic pulmonary fibrosis: a randomized control trial. Ann Palliat Med. 2021;10:7289297. doi:10.21037/apm-21-71
12. Karthik A, Patthi S, Maheswari BU, et al. Advancing idiopathic pulmonary fibrosis prognosis through integrated CNN-LSTM predictive modeling and uncertainty quantification. Biomed Signal Process Control. 2025;100:106811. doi:10.1016/j.bspc.2024.106811
13. Buonacera A, Stancanelli B, Colaci M, Malatino L. Neutrophil to lymphocyte ratio: an emerging marker of the relationships between the immune system and diseases. Int J Mol Sci. 2022;23:3636. doi:10.3390/ijms23073636
14. Hu X, Liu SP, Zhou RS, et al. Correlation analysis between blood routine-derived inflammatory markers and respiratory function in pneumoconiosis patients. Zhonghua Lao Dong Wei Sheng Zhi ye Bing Za Zhi. 2022;40:508–514. doi:10.3760/cma.j.cn121094-20210705-00321
15. Levinson T, Wasserman A. C-reactive protein velocity (CRPv) as a new biomarker for the early detection of acute infection/inflammation. Int J Mol Sci. 2022;23:8100.
16. Kesmez Can F, Özkurt Z, Öztürk N, Sezen S. Effect of IL‐6, IL‐8/CXCL8, IP‐10/CXCL 10 levels on the severity in COVID 19 infection. Int J Clin Pract. 2021;75:e14970.
17. Rayens N, Rayens E, Tighe R. Co-occurrence of pneumoconiosis with COPD, pneumonia and lung cancer. Occup Med. 2022;72:527–533. doi:10.1093/occmed/kqac079
18. Ellulu MS, Samouda H. Clinical and biological risk factors associated with inflammation in patients with type 2 diabetes mellitus. BMC Endocr Disord. 2022;22:16. doi:10.1186/s12902-021-00925-0
19. Mumin A, Abdullah Al Amin A, Kabir S, Noor RA, Rahman U. Role of C-Reactive Protein (CRP) and Neutrophil Lymphocyte Ratio (NLR) in detecting severity & predicting outcome of acute pancreatitis patients. Dinkum J Med Innov. 2024;3:01–12. doi:10.71017/djmi.3.1.d-0236
20. Agca R, Smulders Y, Nurmohamed M. Cardiovascular disease risk in immune-mediated inflammatory diseases: recommendations for clinical practice. Heart. 2022;108:73–79. doi:10.1136/heartjnl-2019-316378
21. Katrinli S, Oliveira NC, Felger JC, Michopoulos V, Smith AK. The role of the immune system in posttraumatic stress disorder. Transl Psychiatry. 2022;12:313. doi:10.1038/s41398-022-02094-7
22. Robles TF. Annual research review: social relationships and the immune system during development. J Child Psychol Psychiatry. 2021;62:539–559. doi:10.1111/jcpp.13350
23. Noone DP, Isendoorn MME, Hamers SMWR, et al. Structural basis for surface activation of the classical complement cascade by the short pentraxin C-reactive protein. Proc Natl Acad Sci. 2024;121:e2404542121. doi:10.1073/pnas.2404542121
24. Cho S, Cho O-H. Depression and quality of life in older adults with pneumoconiosis: the mediating role of death anxiety. Geriatric Nurs. 2022;44:215–220. doi:10.1016/j.gerinurse.2022.02.018
25. Blanco-Pérez JJ, Blanco-Dorado S, Rodríguez-García J, et al. Serum levels of inflammatory mediators as prognostic biomarker in silica exposed workers. Sci Rep. 2021;11:13348. doi:10.1038/s41598-021-92587-0
26. Koziarska-Rościszewska M, Gluba-Brzózka A, Franczyk B, Rysz J. High-sensitivity C-reactive protein relationship with metabolic disorders and cardiovascular diseases risk factors. Life. 2021;11:742. doi:10.3390/life11080742
27. Yang H-Y. Prediction of pneumoconiosis by serum and urinary biomarkers in workers exposed to asbestos-contaminated minerals. PLoS One. 2019;14:e0214808. doi:10.1371/journal.pone.0214808
28. Nong Q, Zhu X, Zhong L, et al. Serum Krebs von den Lungen-6 as a potential biomarker for early diagnosis of silicosis: a case-control study. BMC Pulm Med. 2025;25:366. doi:10.1186/s12890-025-03820-9
29. Kovalchuk T, Rubtsov R. Diagnostic value of inflammatory biomarkers among mining and metallurgical workers with pneumoconiosis in combination with chronic obstructive pulmonary disease. Ukr J Occup Health. 2022;18:277–284. doi:10.33573/ujoh2022.04.277
30. Song Y, Southam K, Beamish BB, Zosky GR. Effects of chemical composition on the lung cell response to coal particles: implications for coal workers’ pneumoconiosis. Respirology. 2022;27:447–454. doi:10.1111/resp.14246
31. Oxidative Medicine and Cellular Longevity. Wiley Online Library; 2023.
32. Cui W, Li X, Xue W, et al. Exercise affects the formation and recovery of alcoholic liver disease through the il-6–p47phox oxidative–stress axis. Cells. 2022;11:1305. doi:10.3390/cells11081305
33. Yin Y, Wang Z, Hu Y, et al. Caffeic acid hinders the proliferation and migration through inhibition of IL-6 mediated JAK-STAT-3 signaling axis in human prostate cancer. Oncol Res. 2024;32:1881. doi:10.32604/or.2024.048007
34. Hirano T. IL-6 in inflammation, autoimmunity and cancer. Int Immunol. 2021;33:127–148. doi:10.1093/intimm/dxaa078
35. Zhai R, Liu G, Ge X, et al. Serum levels of tumor necrosis factor-α (TNF-α), interleukin 6 (IL-6), and their soluble receptors in coal workers’ pneumoconiosis. Respir Med. 2002;96:829–834. doi:10.1053/rmed.2002.1367
36. Nash D, Hughes MG, Butcher L, et al. IL-6 signaling in acute exercise and chronic training: potential consequences for health and athletic performance. Scand J Med Sci Sports. 2023;33:4–19. doi:10.1111/sms.14241
37. Chen J, Wei Y, Yang W, et al. IL-6: the link between inflammation, immunity and breast cancer. Front Oncol. 2022;12:903800. doi:10.3389/fonc.2022.903800
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Associations of High-Sensitivity C-Reactive Protein and Interleukin-6 with Depression in a Sample of Italian Adolescents During COVID-19 Pandemic
Serra M, Presicci A, Quaranta L, Achille M, Caputo E, Medicamento S, Margari F, Croce F, Margari L
Neuropsychiatric Disease and Treatment 2022, 18:1287-1297
Published Date: 29 June 2022
A Predictive Model Based on Inflammatory and Coagulation Indicators for Sepsis-Induced Acute Kidney Injury
Xin Q, Xie T, Chen R, Zhang X, Tong Y, Wang H, Wang S, Liu C, Zhang J
Journal of Inflammation Research 2022, 15:4561-4571
Published Date: 11 August 2022
The Inhibition of Evolocumab on Non-Infarct-Related Artery Disease in Patients with ST-Elevation Myocardial Infarction
Zhao Q, Sun S, Zhou F, Yue J, Luo X, Qu X
International Journal of General Medicine 2023, 16:2771-2781
Published Date: 30 June 2023
Platelet-to-Lymphocyte Ratio Improves the Predictive Ability of the Risk Score for Atrial Fibrillation Recurrence After Radiofrequency Ablation
Huang W, Sun H, Tang Y, Luo Y, Liu H
Journal of Inflammation Research 2023, 16:6023-6038
Published Date: 11 December 2023
The Prognostic Value of CRP/Alb Ratio in Predicting Overall Survival for Hepatocellular Carcinoma Treated with Transcatheter Intra-Arterial Therapy Combined with Molecular-Targeted Agents and PD-1/PD-L1 Inhibitors
Huang X, Peng G, Kong Y, Cao X, Zhou X
Journal of Inflammation Research 2025, 18:203-217
Published Date: 8 January 2025