")
Back to Journals » International Journal of General Medicine » Volume 16
The Inhibition of Evolocumab on Non-Infarct-Related Artery Disease in Patients with ST-Elevation Myocardial Infarction
Authors Zhao Q, Sun S, Zhou F, Yue J, Luo X , Qu X
Received 3 May 2023
Accepted for publication 26 June 2023
Published 30 June 2023 Volume 2023:16 Pages 2771—2781
DOI https://doi.org/10.2147/IJGM.S417481
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Yuriy Sirenko
Qi Zhao,1,* Siyuan Sun,2,* Fanghui Zhou,3,* Jingkun Yue,2 Xing Luo,4 Xiufen Qu1
1Department of Cardiology, 1st Affiliated Hospital of Harbin Medical University, Harbin, 150086, People’s Republic of China; 2Department of Cardiology, People’s Hospital of Taihe County, Taihe, Anhui, 236600, People’s Republic of China; 3Department of Hematology, 2nd Affiliated Hospital of Harbin Medical University, Harbin, 150001, People’s Republic of China; 4Department of Cardiology, 2nd Affiliated Hospital of Harbin Medical University, Harbin, 150001, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xing Luo; Xiufen Qu, Email [email protected]; [email protected]
Purpose: The effects of combing evolocumab and statin on the clinical outcome and physiological function of coronary arteries in STEMI patients with non-infarct-related artery (NIRA) disease are still unclear.
Methods: A total of 355 STEMI patients with NIRA were enrolled in this study, who underwent combined quantitative flow ratio (QFR) at baseline and after 12 months of treatment with statin monotherapy or statin plus evolocumab.
Results: Diameter stenosis and lesion length were significantly lower in the group undergoing statin plus evolocumab. While the group exhibited significantly higher minimum lumen diameter (MLD), and QFR values. Statin plus evolocumab (OR = 0.350; 95% CI: 0.149– 0.824; P = 0.016) and plaque lesion length (OR = 1.223; 95% CI: 1.102– 1.457; P = 0.033) were independently associated with rehospitalization for unstable angina (UA) within 12 months.
Conclusion: Evolocumab combined with statin therapy can significantly improve the anatomical and physiological function of the coronary arteries and downregulate the re-hospitalization rate due to UA in STEMI patients with NIRA.
Keywords: PCSK9 inhibition, C-reactive protein, inflammation, physiological assessment, quantitative flow ratio, non-infarct-related artery
Introduction
Although there are currently a variety of therapeutic measures existing for patients with atherosclerotic cardiovascular disease (ASCVD), including lipid-lowering therapy, anti-inflammatory therapy, antiplatelet therapy and revascularization, recurrent cardiovascular events are still common and lead to substantial morbidity.1,2 Substantial evidence has suggested that low density lipoprotein (LDL-C) lowering treatment is effective in reducing mortality in patients with ASCVD.3,4 As we know, for patients with acute coronary syndrome, the earliest possible use of statins could significantly improve long-term outcomes.5,6 However, several studies have shown that the Chinese have a low tolerance to high-intensity statin therapy, and the probability of adverse reactions in the digestive, motor and nervous systems is significantly increased. Therefore, there is an urgent need for other lipid-lowering drugs combined with statins to improve lipid levels.7,8 As an effective new LDL-C lowering agent, protein-converting enzyme prosubtilisin (PCSK9) inhibitor has been clinically implicated to reduce LDL-C levels and improve cardiovascular adverse events, but its underlying mechanism remains unclear.9
It is common in patients with ST-segment elevation myocardial infarction (STEMI) to develop non-infarct-related arteries (NIRAs). Nevertheless, NIRA disease has not been well understood in terms of its clinical effects. Meanwhile, there is no conclusive evidence that NIRA disease has potential to affect clinical outcomes. Based on existing studies data, Kim et al have found that recurrent percutaneous coronary intervention (PCI) increased while no difference was illustrated in aspect of mortality at 1 year.10 Recently, with the wide application of fractional flow reserve (FFR), Physiological evaluation of coronary arteries for patients could be carried out to optimize the procedure of interventional surgery.11,12 And increased evidence has suggested that inflammation contributed significantly to the progression of atherosclerosis, which increases the risk of acute coronary syndrome incidence.13 Furthermore, adverse cardiovascular outcomes are independently predicted by CRP levels.13,14 However, evidence on the effects of PCSK9 on inflammation levels and plaque physiological function in patients with NIRA disease is still lacking.15–17
This study was conducted with the aim of evaluating the effects of operating evolocumab (an inhibitor of PCSK9 which is widely used) on statin therapy in aspects of clinical outcome, coronary plaque composition, and physiological function, which would facilitate us to further understand the effects and underlying mechanisms of PCSK9 inhibitors in improving clinical outcomes of patients with NIRA disease.
Materials and Methods
Study Design and Population
The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki.
The study was approved by the Harbin Medical University ethics committee, all the patients provided written informed consent. We identified 355 STEMI patients with NIRA disease who underwent evaluation of quantitative coronary angiography (QCA), quantitative flow ratio (QFR) and lipid-lowering therapy in the 1st Affiliated Hospital of Harbin Medical University from January 2018 to December 2020. Patients were divided into two groups according to statin monotherapy (20 mg rosuvastatin once a day) who refused evolocumab treatment or statin (20 mg rosuvastatin once a day) plus evolocumab (140 mg every 2 weeks). Follow-up was performed 1 year later (telephone or outpatient follow-up should be conducted once a month). Clinical data, QCA and QFR were analyzed.
The following criteria were used to determine inclusion: (1) Patients displaying a typical pain of chest lasting longer than 30 minutes within 12 hours of symptoms onset; (2) A ST-segment elevation of at least 1 mm in two continuously recorded electrocardiographic leads, or the onset of a complete left bundle branch block for the first time; and (3) PCI including aspiration of thrombus, balloon angioplasty and/or implantation of stent; (4) NIRA disease (coronary stenosis ≥50% stenosis in at least one NIRA), and (5) LDL-C level ≥1.4 mmol/L.18 The following criteria were used to exclude candidates: (1) any of chronic diseases, including cancerous disease, cirrhosis of the liver, heart failure, or kidney failure in an end stage (2) a life expectancy of less than one year.
Clinical Data Collection
We analyzed clinical data, New York Heart Association functional class, laboratory data, and echocardiographic data. Laboratory data included white blood cell count, serum creatinine, C-reactive protein (CRP), total cholesterol (TC), LDL-C, high-density lipoprotein cholesterol, triglycerides, and levels of troponin I during admission and follow-up.
Computation of QFR
The QFR was operated to evaluate the anatomic and physiological functions of coronary lesions in hospitals. The evaluations of three-dimensional QCA and QFR were carried out by a core laboratory with an independent organization via operating software with dedicated features (AngioPlus 2.0, Pulse Medical Imaging Technology (Shanghai) Co., Ltd) (Figure 1). Software calculated QFR value automatically by applying adjustment of TIMI frame-count to the calculation method.18 QFR was performed via using a pre-trained offline deep learning algorithm arranged in two phases.19 The first phase involved interpreting the features from the input via using a multilevel neural network with three fully connected layers.20 Images from the arterial tree reconstruction were used to extract input, as described previously,21 characteristics of lesion and proximal/distal markers of each lesion were all included. The second phase comprised a bidirectional recursive neural network that received the feature sequence to the next layer and returned the QFR value corresponding to each input neuron.
 |
Figure 1 Typical picture of QFR. A representative case with RCA for QFR =0.87. Abbreviations: RCA, right coronary artery; QFR, quantitative flow ratio. |
Definition
NIRA disease is defined as ≥50% stenosis in at least one NIRA.22 Serious adverse events (SAEs) were defined as all-cause mortality, cardiovascular death, acute myocardial infarction, stroke, or rehospitalization for unstable angina (UA). QFR value ≤0.80 referred to lesion-specific ischemia, and QFR value >0.80 referred to non-ischemia-specific lesions.23,24
Statistical Analyses
The Kolmogorov–Smirnov test was used as a distribution normality test. Quantitative variables were reported as mean ± standard deviation for normally distributed data or as median (25th–75th percentiles) for non-normally distributed data. Levene’s test was performed before Student’s t test. Independent sample t-test or Mann–Whitney U-test was performed for comparison of quantitative variables between groups.
Percentage and total number were used to express qualitative variables. Comparison of categorical variables was conducted via using the Chi-square and Fisher’s exact tests.
Multivariate analysis of logistic regression was used to identify independent predictors of UA rehospitalization 12 months after discharge. Two-sided p-values of 0.05 were considered statistically significant. Analyses of all statistical data were conducted via operating SPSS version 23.0 (SPSS Inc., Chicago, IL, USA).25
Results
Baseline Characteristics
A total of 355 STEMI patients with NIRA disease were enrolled in this retrospective study. The demographic and clinical data of the two groups are shown in Table 1. The baseline characteristics did not differ significantly. Table 2 exhibits the primary characteristics of the two groups on angiography and interventional therapy. Based on the results, we could find that in comparison with statin plus evolocumab group, the rate of IRA for right coronary artery (RCA) was higher in statin monotherapy group.
 |
Table 1 Patient Demographics and Clinical Data |
 |
Table 2 Primary Angiographic and Interventional Therapy Characteristics |
Blood Lipid and Inflammatory Characteristics
Variations in blood lipid levels and inflammatory characteristics are shown in Figure 2. The mean levels of TC, LDL-C, and CRP on admission decreased during the follow-up in both groups (Figure 2A and B). Although TC, LDL-C, and CRP levels at admission were not significantly different, statin plus evolocumab reduced TC and LDL-C levels significantly compared to statin monotherapy (Figure 2C).
 |
Figure 2 Blood lipid and inflammatory characteristics. (A) Blood lipid and inflammatory changing trends in statin monotherapy group. *P<0.05 vs baseline (B) Blood lipid and inflammatory changing trends in statin plus evolocumab group. *P<0.05 vs baseline (C) Blood lipid and inflammatory measurements between two groups. *P<0.05 vs statin plus evolocumab. |
Characteristics of the QFR
QFR was also utilized to evaluate the physiological effects of PCSK9 on plaque. The results indicated that the diameter stenosis and plaque lesion length were significantly lower in the group of statins plus evolocumab in comparison with the group of statin monotherapy (Table 3). The group of the statin plus evolocumab exhibited significantly higher MLD and QFR values than those in the group of statin monotherapy (Table 3).
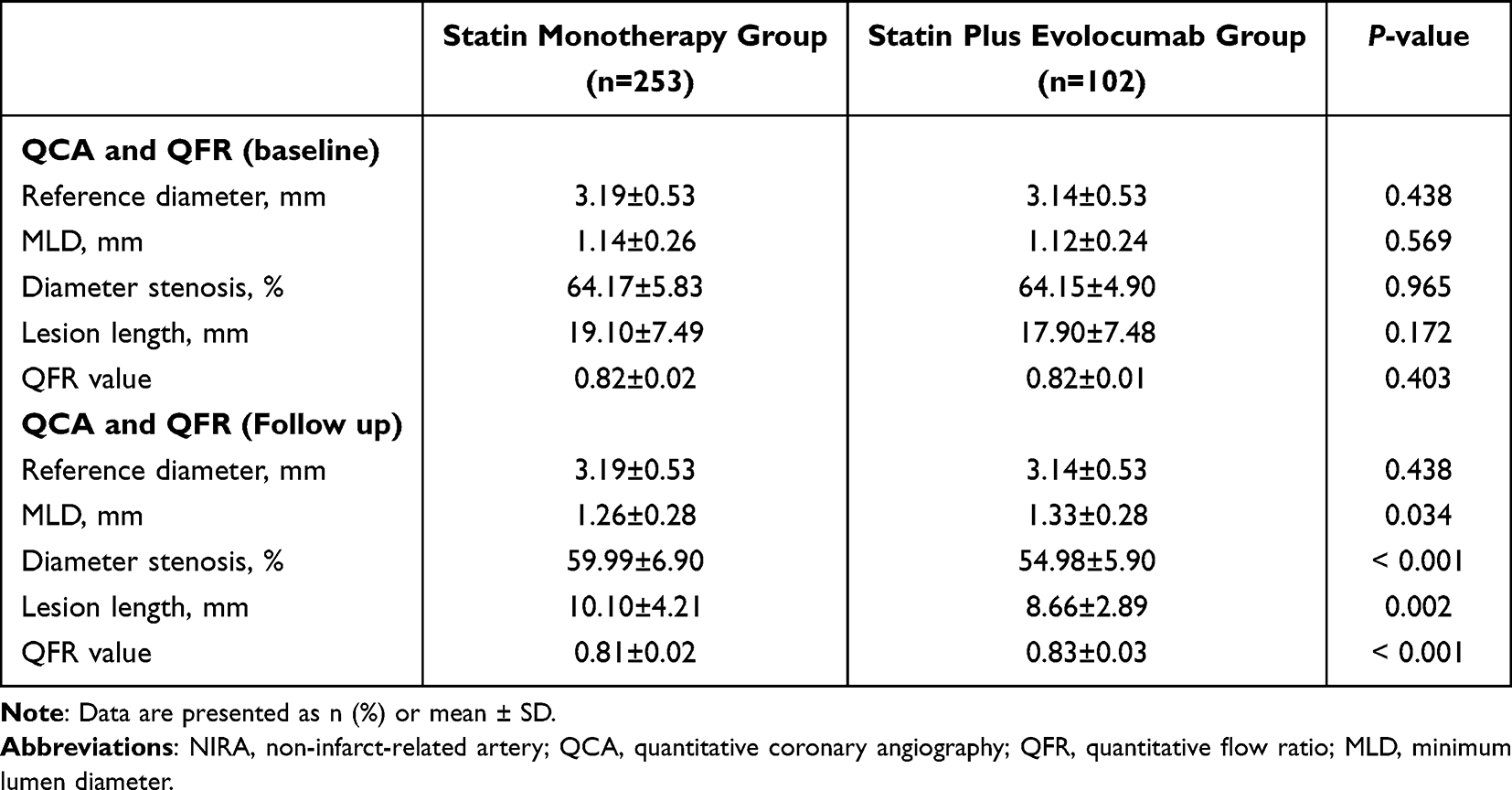 |
Table 3 Non-Infarct-Related Artery Characteristics |
One Year Follow-Up
The safety of statins plus evolocumab was recorded, there is no statistical difference in statin monotherapy and statin plus evolocumab groups (Table 4). Blood pressure and HbA1c between two groups were shown in Figure 3. The results in Figure 4 reveal that a higher rate of SAEs at follow-up was observed in the group of statin monotherapy in comparison with that in the group of statins plus evolocumab. Furthermore, we found that the proportion of patients who were re-hospitalized and implanted coronary stents for UA reduced significantly in the statin plus evolocumab group, whereas all-cause death, cardiovascular death, nonfatal AMI, or stroke did not differ significantly between the two groups (Table 4). To further investigate the risk factors for rehospitalization with UA, we compared the clinical baseline coronary anatomical and physiological features of the two groups (Supplemental Tables 1 and 2). The results demonstrated that the patients who re-hospitalized for UA were older than those in the non-rehospitalization group, and higher CRP and total cholesterol levels and a longer plaque length were observed in the re-hospitalized for UA group.
 |
Table 4 Adverse Events in Follow Up |
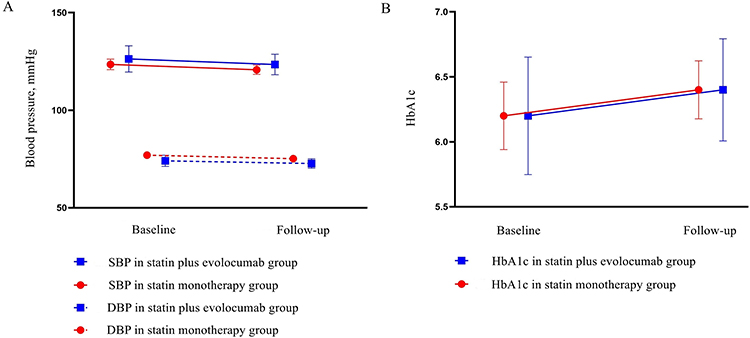 |
Figure 3 Blood pressure and HbA1c in statin monotherapy and statin plus evolocumab groups. (A) Blood pressure; (B) HbA1c. Error bars are 95% CIs. Abbreviations: SBP, systolic pressure; DBP, diastolic pressure; HbA1c, glycosylated hemoglobin. |
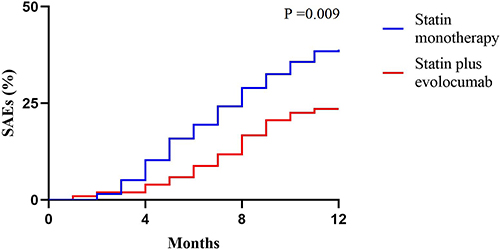 |
Figure 4 Serious adverse events between two groups in follow-up. |
In addition, the proportion of patients receiving statins combined with PCSK9 was significantly lower compared with that in the group of non-rehospitalization. Multivariate analysis was used to investigate whether the above variables were independently associated with rehospitalization for UA. Statin plus evolocumab, age, total cholesterol, CRP and Lesion length were included into the multivariable model. The results showed that statin plus evolocumab (OR = 0.350; 95% CI 0.149–0.824; P = 0.016) and plaque length (OR = 1.223; 95% CI 1.102–1.457; P = 0.033) were independently associated with rehospitalization for UA at 12 months (Table 5).
 |
Table 5 Univariate and Multivariate Regression Analysis for Rehospitalization for UA |
Discussion
Based on the findings of this study, the following conclusions could be listed as follows: 1). In view of coronary physiological function, diameter stenosis and plaque lesion length in QFR were significantly lower in the group of statins plus evolocumab. MLD and QFR values were also higher in the group of statins plus evolocumab; 2). Statin plus evolocumab and plaque length were independently associated with rehospitalization for UA at 12 months. All of which mentioned above suggest that compared with stain application alone, the use of statin plus evolocumab could effectively improve vascular physiological function and reduce readmission risk of STEMI patients with NIRA diseases.
The reduction of ASCVD events via statin therapy was observed in corresponding with the reducing magnitude of LDL-C.26 According to current guidelines and evidence-based medical evidence, statins are considered as the first-line therapy for acute coronary syndrome.27 However, certain patients with moderate or high-intensity statin therapy still do not achieve the desired clinical results, who need to be treated with non-statin lipid-lowering agents.28 The lipid-lowering mechanism of PCSK9 inhibitors is to reduce circulating LDL-C levels by binding PCSK9 and preventing LDL-C receptor degradation.29 Futhermore, therapeutic monoclonal antibodies directed against PCSK9 have proven to be highly effective for treating ASCVD patients with disorder of lipid.29,30 Studies on PCSK9 inhibition have shown that PCSK9 inhibitors can effectively reduce LDL-C levels in patients regardless of sex and race differences.31,32 In our study, we enrolled patients in the Asian population, and we also found that the adding (140 mg every two weeks) to high-intensity statins therapy could contribute to significantly lower levels of LDL-C than high-intensity statins alone, which is consistent with previous studies.33 In the meantime, the data are concordant with prior clinical observations in which patients with a clinical burden of atherosclerosis experienced a larger benefit with PCSK9 inhibition.2,34 Our study also indicated a significant relationship between decreased LDL-C and reduction of SAEs while additional decreased LDL-C occurred in STEMI patients with NIRA disease. Multivariate analysis also suggested that statin plus evolocumab (OR = 0.350, P = 0.016) was independently associated with UA readmission.
Recently, FFR calculations based on angiography (QFR) have been successfully implicated to evaluate patients’ coronary physiological functions. It has been confirmed that coronary physiological function parameters obtained by QFR is highly consistent with FFR. It has been demonstrated that vascular physiological function acts as a direct reflection of vascular ischemia. In our study, QFR test was performed on the patients at baseline and follow-up. No significant difference in QFR values were obtained of two groups at baseline. However, QFR values were significantly higher after one year in the group of statin plus evolocumab in comparison with the group of statin alone, indicating that combining statin and evolocumab can improve the physiological function of diseased blood vessels in NIRA disease to some extent. Meanwhile, several studies have examined the effects of evolocumab on vascular plaque characteristics using endovascular imaging, but have not drawn a consistent conclusion. It was reported that evolocumab, a PCSK9 inhibitor, might increase fibrous-cap thickness and decrease lipid-rich plaque thickness when added to statin therapy.35 A study following for 76 weeks found that in comparison with statin monotherapy, evolocumab addition did not alter plaque composition.36 Even so, no studies have reported the effects of PCSK9 inhibitors combined with statins on vascular physiological function. Our results suggest that the combination of evolocumab and statin may improve the physiological function of diseased vessels more than statin therapy alone.
The effects of PCSK9 inhibitors on the inflammatory response have also attracted much attention in recent years. We observed a significant decrease in CRP levels in both the statin treatment alone group and the statin combined with evolocumab group at the one-year follow-up. However, there are other studies demonstrating that evolocumab had no effect on the inflammatory response in patients. Stiekema et al have reported that evolocumab significantly improved lipid levels, while a slight decrease in CRP was observed by the late phase of dosing.37,38 Another study has found that significant improvements in lipids and inflammation were observed in patients receiving intensive lipid-lowering therapy (140 mg evolocumab on top of 20 mg/day rosuvastatin).39 Furthermore, as for our population, the subjects of this study were Han Chinese. These results suggest that the anti-inflammatory effects of PSCK9 inhibitors may be related to the patient population, requiring more evidence to be confirmed in future studies.
The current clinical use of PCSK9 inhibitors mainly include alirocumab and evolocumab. However, the clinical benefits of alirocumab and evolocumab are different. A meta-analysis was performed to compare the effects of alirocumab and evolocumab on all-cause mortality. It was reported that the use of alirocumab was associated with reductions in all-cause mortality compared with control, while evolocumab was associated with increased all-cause mortality compared with alirocumab. These results suggest that alirocumab might provide the optimal benefits regarding all-cause mortality with relatively lower SAE risks, and evolocumab might provide the optimal benefits regarding myocardial infarction for secondary prevention in patients with high-risk of cardiovascular events.40 Further research confirmed that inclisiran also has a potent lipid-lowering effect.41 However, further data are needed to confirm whether alirocumab and inclisiran can improve the physiological function of non-criminal lesions in addition to statins.
In our study, patients were treated with 20 mg rosuvastatin once a day or statin (20 mg rosuvastatin once a day) plus evolocumab (140 mg every 2 weeks). Compared with Caucasians, statin doses are lower.42 It was reported that adverse effects of statin are more common in the Chinese population, including rhabdomyolysis, liver damage, and neurological symptoms.7 Therefore, compared with Caucasians, Chinese patients with coronary heart disease receive a lower dose of statins. In addition, the Chinese guidelines for dyslipidemia also recommend the use of rosuvastatin 20mg.43,44
As a powerful lipid-lowering drug, it is well known that combining evolocumab with statins has the potential to downregulate the levels of LDL-C and cardiovascular events risks.9,45,46 However, the evidence of PCSK9 combined with statin therapy for the clinical outcome of patients with NIRA disease is lacking. Some patients are prone to develop vulnerable plaques or even ACS events. Therefore, it is of great clinical significance to study lipid-lowering strategies in STEMI patients with NIRA disease. Our results suggest that non-use of PCK9 serves as a risk factor independently for UA hospitalization of patients with NIRA disease. Although no significant differences were observed in other cardiovascular adverse events, the combination of PCSK9 may improve quality of life in patients with NIRA disease.
Conclusion
Evolocumab combined with statin therapy could significantly improve the physiological function of the coronary arteries and downregulate the re-hospitalization rate of STEMI patients with NIRA disease.
Study Limitations
Several potential limitations could be identified in our study. Firstly, from a single center, a non-random and retrospective selection of patients was conducted. For example, our patients are all from the northern part of China. Cold climate and dietary habits may lead to our conclusion not applicable to all patients. Therefore, multicenter studies are needed to further confirm our results; Meanwhile, our results might be influenced by selection bias. Secondly, as well as in Europe and the USA, atorvastatin 20 mg/day is regarded as a mild-intensity treatment. However, for Chinese patients whose body weights are lighter than Caucasians, 10 mg/day of rosuvastatin is the most appropriate dose for the first time in aspect of aggressive lipid-lowering treatment.44 Therefore, further research is needed to confirm whether evolocumab could improve the rate of hospitalization and the physiological function of non-criminal function beyond moderate and above statin therapy. Thirdly, an invasive measurement of microvascular dysfunction was not performed, meaning that we cannot understand the differences in QFR values between the two groups. Fourthly, in the current study, we only followed patients for 12 months, and the study endpoint was only readmission for unstable angina. Follow-up time was short and hard clinical endpoints were absent. Follow-up studies need to extend follow-up time and increase clinical endpoints such as cardiovascular adverse events.
Data Sharing Statement
Upon reasonable request, the original data can be obtained from the corresponding authors.
Approval of Ethics and Consent to Participate
The ethics committee of 1st Affiliated Hospital of Harbin Medical University has approved the study, which was conducted in view of the principles of the Declaration of Helsinki. Patient consents were obtained in writing by each of participants before participating in the study.
Acknowledgments
Thank you for funding our research. Qi Zhao, Siyuan Sun, and Fanghui Zhou are co-first authors for this study.
Funding
Support for this research comes from the National Natural Science Foundation of China (No. 81970297 and 82270319), and Fund of Key Laboratory of Myocardial Ischemia, Ministry of Education (KF202020/LX).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Mozaffarian D, Benjamin EJ, Go AS, et al. Heart disease and stroke statistics--2015 update: a report from the American Heart Association. Circulation. 2015;131(4):e29–322.
2. Marston NA, Kamanu FK, Nordio F, et al. Predicting benefit from evolocumab therapy in patients with atherosclerotic disease using a genetic risk score: results from the Fourier trial. Circulation. 2020;141(8):616–623.
3. Baigent C, Blackwell L, Emberson J, et al. Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170,000 participants in 26 randomised trials. Lancet. 2010;376(9753):1670–1681.
4. Koskinas KC, Siontis GCM, Piccolo R, et al. Effect of statins and non-statin LDL-lowering medications on cardiovascular outcomes in secondary prevention: a meta-analysis of randomized trials. Eur Heart J. 2018;39(14):1172–1180.
5. Cecha P, Chromik A, Piotrowska I, Zabojszcz M, Dolecka-ślusarczyk M, Siudak Z. Assessment of application of the new 2019 European Society of Cardiology/ European Atherosclerosis Society Guidelines for the Management of Dyslipidaemias in daily clinical practice - one center study. Folia Med Cracov. 2021;61(3):43–54.
6. Grundy SM, Stone NJ, Bailey AL, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: a Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2019;73(24):e285–e350.
7. Tsui L, Ye P, Xu S, et al. Adverse drug reactions of statin therapy in China from 1989 to 2019: a national database analysis. Eur j Hospital Pharm. 2022;1:56.
8. Lin JL, Chen PS, Lin HW, Tsai LM, Lin SH, Li YH. Real-World Analyses of the Safety Outcome among a General Population Treated with Statins: an Asian Population-Based Study. J Atheroscler Thromb. 2022;29(8):1213–1225.
9. Sabatine MS, Giugliano RP, Keech AC, et al. Evolocumab and clinical outcomes in patients with cardiovascular disease. N Engl J Med. 2017;376(18):1713–1722.
10. Kim DH, Burton JR, Fu Y, Lindholm L, Van de Werf F, Armstrong PW. What is the frequency and functional and clinical significance of complex lesions in non-infarct-related arteries after fibrinolysis for acute ST-elevation myocardial infarction? Am Heart J. 2006;151(3):668–673.
11. Shiono Y, Kuramitsu S, Matsuo H, et al. Thrombotic risk and cardiovascular events in patients with revascularization deferral after fractional flow reserve assessment. JACC Cardiovasc Interv. 2022;15(4):427–439.
12. Griffin WF, Choi AD, Riess JS, et al. AI Evaluation of Stenosis on Coronary CT Angiography, Comparison With Quantitative Coronary Angiography and Fractional Flow Reserve: a CREDENCE Trial Substudy. JACC Cardiovasc Imaging. 2022:64.
13. Li L, Liu QW, Li Z, et al. The utility of high-sensitivity C-reactive protein levels in patients with moderate coronary lesions and gray-zone fractional flow reserve. Anatolian j Cardiol. 2018;20(3):143–151.
14. Soysal D, Karakuş V, Yavaş HH, Biçeroğlu S, Köseoğlu M, Yeşil M. C-reactive protein in unstable angina pectoris and its relation to coronary angiographic severity and diffusion scores of coronary lesions. Anatolian j Cardiol. 2010;10(5):421–428.
15. Tu S, Westra J, Yang J, et al. Diagnostic Accuracy of Fast Computational Approaches to Derive Fractional Flow Reserve From Diagnostic Coronary Angiography: the International Multicenter FAVOR Pilot Study. JACC Cardiovasc Interv. 2016;9(19):2024–2035.
16. Tesche C, De Cecco CN, Baumann S, et al. Coronary CT Angiography-derived Fractional Flow Reserve: machine Learning Algorithm versus Computational Fluid Dynamics Modeling. Radiology. 2018;288(1):64–72.
17. Coenen A, Kim YH, Kruk M, et al. Diagnostic Accuracy of a Machine-Learning Approach to Coronary Computed Tomographic Angiography-Based Fractional Flow Reserve: result From the MACHINE Consortium. Circ Cardiovasc Imaging. 2018;11(6):e007217.
18. Hwang D, Choi KH, Lee JM, et al. Diagnostic agreement of quantitative flow ratio with fractional flow reserve and instantaneous wave-free ratio. J Am Heart Assoc. 2019;8(8):e011605.
19. Wang ZQ, Zhou YJ, Zhao YX, et al. Diagnostic accuracy of a deep learning approach to calculate FFR from coronary CT angiography. J Geriatr Cardiol. 2019;16(1):42–48.
20. Brandt V, Bekeredjian R, Schoepf UJ, et al. Prognostic value of epicardial adipose tissue volume in combination with coronary plaque and flow assessment for the prediction of major adverse cardiac events. Eur J Radiol. 2022;148:110157.
21. Chen K, Zhang Y, Pohl K, Syeda-Mahmood T, Song Z, Wong ST. Coronary artery segmentation using geometric moments based tracking and snake-driven refinement. Ann International Conf IEEE Eng Med Biol IEEE Eng Med Biol Society Ann Int Conf. 2010;2010:3133–3137.
22. Shah R, Clare RM, Chiswell K, et al. Impact of Non-Infarct-Related Artery Disease on Infarct Size and Outcomes (from the CRISP-AMI Trial). Am J Med. 2016;129(12):1307–1315.
23. Danad I, Szymonifka J, Twisk JWR, et al. Diagnostic performance of cardiac imaging methods to diagnose ischaemia-causing coronary artery disease when directly compared with fractional flow reserve as a reference standard: a meta-analysis. Eur Heart J. 2017;38(13):991–998.
24. Piątek Ł, Janion-Sadowska A, Piątek K, et al. Long-term clinical outcomes in patients with unstable angina undergoing percutaneous coronary interventions in a contemporary registry data from Poland. Coron Artery Dis. 2020;31(3):215–221.
25. Strähl M, Schindler M, Keller LS, et al. Diagnostic performance of angiography-based quantitative flow ratio for the identification of myocardial ischemia as assessed by (13) N-ammoniamyocardial perfusion imaging positron emission tomography. Int J Cardiol. 2020;314:13–19.
26. Ray KK, Del Prato S, Müller-Wieland D, et al. Alirocumab therapy in individuals with type 2 diabetes mellitus and atherosclerotic cardiovascular disease: analysis of the ODYSSEY DM-DYSLIPIDEMIA and DM-INSULIN studies. Cardiovasc Diabetol. 2019;18(1):149.
27. Hussain A, Ballantyne CM, Saeed A, Virani SS. Triglycerides and ASCVD Risk Reduction: recent Insights and Future Directions. Curr Atheroscler Rep. 2020;22(7):25.
28. Perk J, De Backer G, Gohlke H, et al. European Guidelines on cardiovascular disease prevention in clinical practice (version 2012). The Fifth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of nine societies and by invited experts). Eur Heart J. 2012;33(13):1635–1701.
29. Sabatine MS. PCSK9 inhibitors: clinical evidence and implementation. Nat Rev Cardiol. 2019;16(3):155–165.
30. Ruscica M, Tokgözoğlu L, Corsini A, Sirtori CR. PCSK9 inhibition and inflammation: a narrative review. Atherosclerosis. 2019;288:146–155.
31. Rosenson RS, Hegele RA, Fazio S, Cannon CP. The Evolving Future of PCSK9 Inhibitors. J Am Coll Cardiol. 2018;72(3):314–329.
32. Tombling BJ, Zhang Y, Huang YH, Craik DJ, Wang CK. The emerging landscape of peptide-based inhibitors of PCSK9. Atherosclerosis. 2021;330:52–60.
33. Stroes E, Colquhoun D, Sullivan D, et al. Anti-PCSK9 antibody effectively lowers cholesterol in patients with statin intolerance: the GAUSS-2 randomized, placebo-controlled Phase 3 clinical trial of evolocumab. J Am Coll Cardiol. 2014;63(23):2541–2548.
34. Sabatine MS, De Ferrari GM, Giugliano RP, et al. Clinical Benefit of Evolocumab by Severity and Extent of Coronary Artery Disease: analysis From Fourier. Circulation. 2018;138(8):756–766.
35. Yano H, Horinaka S, Ishimitsu T. Effect of evolocumab therapy on coronary fibrous cap thickness assessed by optical coherence tomography in patients with acute coronary syndrome. J Cardiol. 2020;75(3):289–295.
36. Nicholls SJ, Puri R, Anderson T, et al. Effect of Evolocumab on Coronary Plaque Composition. J Am Coll Cardiol. 2018;72(17):2012–2021.
37. Choi SW, Kim J, Jang GW, et al. Acute Effect of Evolocumab on Lipoprotein(a) Level and Inflammation in Patients with Coronary Artery Disease. J Cardiovascular Dev Dis. 2022;9:4.
38. Stiekema LCA, Stroes ESG, Verweij SL, et al. Persistent arterial wall inflammation in patients with elevated lipoprotein(a) despite strong low-density lipoprotein cholesterol reduction by proprotein convertase subtilisin/kexin type 9 antibody treatment. Eur Heart J. 2019;40(33):2775–2781.
39. Ou Z, Yu Z, Liang B, et al. Evolocumab enables rapid LDL-C reduction and inflammatory modulation during in-hospital stage of acute coronary syndrome: a pilot study on Chinese patients. Front Cardiovascular Med. 2022;9:939791.
40. Wang X, Wen D, Chen Y, Ma L, You C. PCSK9 inhibitors for secondary prevention in patients with cardiovascular diseases: a Bayesian network meta-analysis. Cardiovasc Diabetol. 2022;21(1):107.
41. Strilchuk L, Fogacci F, Cicero AF. Safety and tolerability of injectable lipid-lowering drugs: an update of clinical data. Expert Opin Drug Saf. 2019;18(7):611–621.
42. Nanna MG, Navar AM, Zakroysky P, et al. Association of Patient Perceptions of Cardiovascular Risk and Beliefs on Statin Drugs With Racial Differences in Statin Use: insights From the Patient and Provider Assessment of Lipid Management Registry. JAMA cardiol. 2018;3(8):739–748.
43. Joint committee issued Chinese guideline for the management of dyslipidemia in adults. 中国成人血脂异常防治指南修订联合委员会. 中国成人血脂异常防治指南 (2016年修订版) [2016 Chinese guideline for the management of dyslipidemia in adults]. Zhonghua Xin Xue Guan Bing Za Zhi. 2016;44(10):833–853. Chinese.
44. Wei Y, Guo H, The E, et al. Persistent lipid abnormalities in statin-treated coronary artery disease patients with and without diabetes in China. Int J Cardiol. 2015;182:469–475.
45. Giugliano RP, Pedersen TR, Park JG, et al. Clinical efficacy and safety of achieving very low LDL-cholesterol concentrations with the PCSK9 inhibitor evolocumab: a prespecified secondary analysis of the Fourier trial. Lancet. 2017;390(10106):1962–1971.
46. Bonaca MP, Nault P, Giugliano RP, et al. Low-Density Lipoprotein Cholesterol Lowering With Evolocumab and Outcomes in Patients With Peripheral Artery Disease: insights From the Fourier Trial (Further Cardiovascular Outcomes Research With PCSK9 Inhibition in Subjects With Elevated Risk). Circulation. 2018;137(4):338–350.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.