Back to Journals » Neuropsychiatric Disease and Treatment » Volume 18
Associations of High-Sensitivity C-Reactive Protein and Interleukin-6 with Depression in a Sample of Italian Adolescents During COVID-19 Pandemic
Authors Serra M ![]() , Presicci A, Quaranta L
, Presicci A, Quaranta L ![]() , Achille M, Caputo E, Medicamento S, Margari F
, Achille M, Caputo E, Medicamento S, Margari F ![]() , Croce F, Margari L
, Croce F, Margari L
Received 21 February 2022
Accepted for publication 12 May 2022
Published 29 June 2022 Volume 2022:18 Pages 1287—1297
DOI https://doi.org/10.2147/NDT.S362536
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Maria Serra,1 Anna Presicci,2 Luigi Quaranta,3 Mariaclara Achille,4 Elvita Caputo,4 Silvia Medicamento,4 Francesco Margari,5 Federica Croce,5 Lucia Margari4
1Department of Pharmacy-Pharmaceutical Sciences, University of Bari “Aldo Moro”, Bari, Italy; 2Department of Neuroscience, Sense Organs and Locomotor System, University Hospital “Policlinico”, Bari, Italy; 3Department of Computer Science, University of Bari “Aldo Moro”, Bari, Italy; 4Department of Biomedical Sciences and Human Oncology, University of Bari “Aldo Moro”, Bari, Italy; 5Department of Basic Medical Science, Neuroscience and Sensory Organs, University of Bari “Aldo Moro”, Bari, Italy
Correspondence: Maria Serra, Department of Pharmacy-Pharmaceutical Sciences, University of Bari “Aldo Moro”, Via Edoardo Orabona 4, Bari, 70125, Italy, Tel +39 080 5592829, Fax +39 080 5595260, Email [email protected]
Introduction: Many studies highlighted the role of inflammation in the pathogenesis of depression, although not for every patient nor for every symptom. It is widely shared that stressors can increase inflammation and lead to depressive symptoms. Little is known about the symptom-specificity of the inflammation-depression link in adolescence, which we aimed to explore. The single symptom analysis is a core feature of the recent network approach to depression, supposing that psychiatric disorders consist of co-occurring symptoms and their tendency to cause each other.
Patients and Methods: We recruited 52 adolescents diagnosed with a Depressive Disorder during the COVID-19 stressful period. We used regression analysis to measure associations between high sensitivity C-Reactive Protein (hs-CRP) and Interleukin-6 (IL-6) and depressive symptoms assessed by the Children’s Depression Inventory 2 (CDI 2). For the study of symptom specificity, we selected 13 items from the CDI 2 Self Report corresponding with the DSM-5 diagnostic criteria for Major Depressive Disorder and we coded them as dichotomous variables to perform a regression analysis.
Results: We found that a higher CDI 2-Parent Version total score was significantly predicted by higher hs-CRP (coefficient 3.393; p 0.0128) and IL-6 (coefficient 3.128; p 0.0398). The endorsement of the symptom self-hatred, measuring the DSM-5 symptom “feelings of worthlessness”, was significantly predicted by hs-CRP (OR 10.97; 95% CI 1.29– 93.08; p 0.0282).
Conclusion: A novel symptom-specificity emerged, with hs-CRP significantly predicting the endorsement of the symptom self-hatred, recognized as a core feature of adolescent depression, following the network theory. We considered it a possible phenotypic expression of one depression endophenotype previously causally linked to inflammation. Due to the limited sample size, these preliminary findings require confirmation with future research focusing on the relationship between inflammation and self-hatred and other central nodes of the depression network, representing an opportunity for targeting interventions on crucial symptoms.
Keywords: endophenotype, inflammation, network, self-hatred, stress
Introduction
The role of inflammation in mental disorders is a topic of interest. The interaction between the immune system and neurotransmitters emerged as a mechanism underpinning mood disorders, psychosis, and anxiety disorders.1–5 Despite the scarcity of longitudinal studies investigating the role of inflammation as a precursor to mental disorders in children and adolescents, much evidence supports that inflammation is a crucial component of the pathogenesis of depression: large studies report associations between inflammatory markers such as C-Reactive Protein (CRP) and Interleukin-6 (IL-6) and depression.6–8 CRP is a non-specific acute-phase plasma protein synthesized in the liver in reaction to pro-inflammatory cytokines such as IL-6, secreted by the activated macrophages in response to infection and tissue damage.9 The high sensitivity CRP (hs-CRP) has been widely used to detect low-grade inflammation (0.2–10 mg/L).6 The literature reports evidence of a bidirectional relationship between inflammation and depression: on the one hand, inflammation predicts increases in depressive symptoms, while on the other hand, depression predicts increased inflammation in some samples.10–12
However, not all depressed patients are inflamed. Several studies suggest that inflammation would be relevant for a subset of depressed patients and not all, as well as for some but not all the affective symptoms.8,11,13
Inflammation has also been studied concerning depression endophenotypes: heritable quantitative traits, intermediate between genotype and distal phenotype.14 The endophenotype approach aims to understand psychiatric disorders by identifying some homogeneous and treatment-relevant core features.10 Not all but three of the empirically-validated depression endophenotypes have been found influenced by inflammation: (1) Exaggerated reactivity to negative information; (2) Altered reward processing; (3) Somatic syndrome.10
Increased inflammation has been demonstrated in a subset of patients with a “neurodevelopmentally-based” form of depression, originating from early exposure to stress.10,13 It is widely shared that stress can increase the risk of depression.15–19 Recent studies suggested that both loneliness and social isolation are associated with increased expression of peripheral inflammatory markers.18,20–22 The association between social isolation and CRP indicated that social isolation can act as a social stressor.18,23 Socially isolated individuals were 2–2.5 times more likely to show high levels of CRP than socially integrated people.24 Psychosocial stress has been demonstrated to activate key inflammatory pathways resulting in increased levels of peripheral pro-inflammatory cytokines such as IL-6.25
Nowadays, children and adolescents have been greatly impacted by the exposure to psychosocial stressors induced by the COVID-19 pandemic, like social isolation. Social restrictions have been psychologically distressing for anyone who experienced them, but particularly difficult for young people, who rely importantly on social connections for their emotional wellbeing, with an enhanced vulnerability to the adverse effects of social distancing and loneliness.26,27 It has been proposed that dysregulated neuroendocrine-immune interactions may underlie the psychiatric phenomena observed in quarantined people during the current pandemic.28
According to the social signal transduction theory proposed by Slavich and Irwin, the same innate immune system response, which is normally induced by tissue damage and microbial infection, can be activated in response to adverse social conditions like rejection, conflict, or isolation.15 These social stressors can activate the innate immune system response through two different pathways: the sympathetic nervous system (SNS) and the hypothalamic-pituitary-adrenal (HPA) axis.15 The SNS induces the release of norepinephrine, which upregulates transcription of the proinflammatory immune response genes IL-1, IL-6, and TNF-alfa.15 The HPA axis activation hesitates in the secretion of cortisol, which is a potent anti-inflammatory hormone, under normal conditions. But when a stressful stimulus persists, a glucocorticoid resistance occurs, empowering the inflammatory response, with peripheral cytokines reaching the central nervous system. This immunological pathway involving the brain can lead to “sickness behaviors”, very similar to depressive symptoms (anhedonia; reduced exploration, search for novelty, and social behaviors; reduced food intake; sleep disturbances), as an adaptive response to reduce the spread of infection and promote recovery.10,15 This mechanism may explain why inflammation was particularly associated with fatigue, impaired sleep, and appetite, as well as depressed mood and anhedonia.8,29 A prolonged inflammatory signal can maintain these altered behaviors by increasing the risk of depression and other psychiatric diseases.10
Despite extensive literature existing on the association between inflammation and depression, most studies concern adult populations. Moreover, only a few studies have examined the specific associations between each depressive symptom and inflammation. In this research, we recruited adolescent inpatients diagnosed with a Depressive Disorder (DD) during the COVID-19 emergency and measured their inflammatory markers hs-CRP and IL-6. The aims of this study were: (1) To disclose whether systemic inflammation predicted depressive symptoms in a stressful period like the COVID-19 pandemic when the psychosocial stressors could have altered the neuroendocrine activity with an increased inflammatory response; (2) To search for potentially specific correlations between inflammation and depression using a symptom-based approach.
Materials and Methods
Design and Participants
We consecutively recruited the adolescents from 11 to 17 years presenting with depressive symptomatology among the inpatients admitted to the Operative Units of Child Neuropsychiatry and Psychiatry of the University Hospital of Bari, Italy, who gave their consent to take part in the study. We began the recruitment at the end of the first Italian acute phase of the pandemic (June 2020), when pandemic-related mental health problems were expected to increase based on literature.30 We extended the enrolling time until October 2021 hypothesizing a period enough to capture the longstanding consequences of the first full social restrictions, given that the effects of stress exposure may need a certain degree of neurobiological development to occur.31 Neuropsychiatric diagnoses were made by child neuropsychiatrists or psychiatrists in line with DSM-5 criteria, following the semi-structured interview K-SADS-PL for DSM-5.32,33 Only patients with a diagnosis of a DD were included. Exclusion criteria were: (1) Depressive symptoms not fulfilling DSM-5 criteria for a DD but those of other disorders (eg, Bipolar and related disorders, Gender Dysphoria, Disorders related to trauma and stressor events); (2) Medical disorders likely to alter the interpretation of immunological data (ie, acute or chronic inflammatory disease, autoimmune, or endocrine disease); (3) Current use of drugs likely to compromise interpretation of inflammatory peripheral markers (ie, systemic anti-inflammatory medications, statins, corticosteroids, antibiotics, antihistamines). In total, 85 patients were considered for enrollment in the study and asked to participate. Among them, 18 people refused to participate and 15 were not recruited because of the exclusion criteria (9: diagnoses different from DD; 4: use of anti-inflammatory drugs or statins or antihistamines; 2: the presence of chronic inflammatory or autoimmune or endocrine disease). Finally, 52 individuals took part in the study.
The study protocol was approved by the Independent Ethical Committee of Azienda Ospedaliero-Universitaria Consorziale Policlinico di Bari and conducted according to the recommendations of the Helsinki Declaration. The parents of all participants provided their written informed consent.
Measurements
Depressive Symptoms
We used the Italian adaptation of the Children’s Depression Inventory 2 in its Self-Report assessment (CDI 2-SR, 28 items) and Parent Version (CDI 2-PV, 17 items).34 The whole sample completed both the SR and the PV forms. The CDI 2 provides information about the presence and severity of depressive symptoms in the past two weeks, in pediatric samples (7–17 years). Each item is rated on a Likert-type scale: from 0 to 2 for the CDI 2-SR and from 0 to 3 for the CDI 2-PV, with higher scores representing higher severity of symptoms. We used the total scores of both the scales and the four partial scores provided by the SR version (“Depressed mood/somatic symptoms”; “Negative self-esteem”; “Ineffectiveness”; “Interpersonal problems”). We used T-scores normed based on age and sex and set the clinical cut-off for depressive symptomatology at T-scores ≥ 65, as per the CDI 2 scoring guidelines.34 High internal consistency was demonstrated for the CDI 2-SR (alfa 0.87) and the CDI 2-PV (alfa 0.89).34 In this sample, alfa values were 0.91 for CDI 2-SR and 0.76 for CDI 2-PV. For the study of symptom specificity, we selected 13 items from the CDI 2-SR based on their correspondence with the DSM-5 diagnostic criterion A for Major Depressive Disorder (MDD):
(A1) Depressed mood: item 1 (depressed mood), item 10 (irritability)
(A2) Anhedonia: item 4 (anhedonia)
(A3) Appetite/weight alteration: item 17 (hypophagia), item 27 (hyperphagia)
(A4) Sleep alteration: item 15 (insomnia), item 26 (hypersomnia)
(A6) Tiredness: item 16 (tiredness)
(A7) Feelings of worthlessness and guilt: item 6 (self-hatred), item 7 (guilty)
(A8) Difficulties in concentration and taking decisions: item 14 (difficulties in concentration), item 12 (indecisiveness)
(A9) Thoughts of death/suicidal ideation: item 8 (suicidal ideation)
We excluded the symptom psychomotor alterations (A5) because it was not assessed by the CDI 2. Then we coded the selected items as dichotomous variables with responses scoring 1 or 2 indicating the presence of the symptom.
Inflammatory Markers
Blood samples were obtained from the patients with a venipuncture performed between 8 and 10 am, after an overnight fast. All the patients had not consumed caffeine on the morning of the sample and had not performed strenuous physical exercise in the previous 72 hours. Blood was collected into serum separator tubes and centrifuged within two hours from the sample collection. All laboratory analyses were performed in the first 24 hours after the blood draw. Serum hs-CRP and IL-6 levels were measured by nephelometric method and electrochemiluminescence immunoassay, respectively. The lower detection limits were 0.2 mg/L for hs-CRP and 1.5 pg/mL for IL-6.
Covariates
Based on the literature, we considered as covariates for the regression analysis several variables, because linked to both psychopathology and inflammation: age, sex, body mass index (BMI: kg/m2), markers of an unhealthy lifestyle (smoke, alcohol consumption, cannabis use), and use of Selective Serotonin Reuptake Inhibitors (SSRI) in the month preceding the blood sampling.35–38 All these variables were documented by clinical interviews. Smoke, cannabis, and alcohol consumption and SSRI use referred to the month preceding the blood sample.35,36 For smoking and cannabis use, there were three alternative answers: “often”, “occasionally”, and “never”. Alcohol consumption was defined as heavy (≥7 drinks/week), moderate (1–7 drinks/week), or absent (≤ 1 drink/week).35 The three lifestyles were recoded into dichotomous variables with “often”/“heavy” and “occasionally”/“moderate” considered as “Yes” and “never”/“absent” considered as “No”. SSRI use was coded into the dichotomous variables “Yes” (if ≥ 50% of all days in the past month) or “No”.36
Statistical Analysis
Firstly, we natural-log transformed levels of hs-CRP and IL-6 to normalize the data. Then, we used regression analysis for estimating associations between inflammatory markers as independent variables and: (1) CDI 2 scores (SR and PV total scales and SR subscales) as outcomes, with multiple linear regression; (2) Dichotomized CDI 2-SR single symptoms as outcomes, with logistic regression. After unadjusted regression analysis, we explored the impact of covariates adjusting for age and sex (except for CDI 2 total scale and subscales, because we considered normed-based T-scores), Smoking status/Alcohol consumption/Cannabis use (SAC), current SSRI medication (SSRI), BMI. We considered covariates individually and in every possible combination. In total, 608 models were analyzed. Statistical significance was set at p < 0.05.
Results
Baseline Characteristics
The total sample included 52 individuals, 38 females (73.1%) and 14 males (26.9%), from 11 to 17 years (mean age: 14.4±1.7 years). A minority of the sample declared a current smoking status (19.2%), alcohol consumption (21.2%), and cannabis use (15.4%). Five patients (9.6%) were being treated with SSRI in the last month before the hospitalization. BMI mean values were 21.6±5.5. All the recruited individuals were diagnosed with a DD, according to DSM-5 criteria: 41 (78.8%) with an MDD, 8 (15.4%) with a Persistent DD, 2 (3.8%) with an Unspecified or Other Specified DD, and 1 (1.9%) with a Disruptive Mood Dysregulation Disorder. All the patients underwent clinical and laboratory assessments. Hs-CRP data were not obtained on three patients due to technical problems and the unavailability of patients to undergo another sample. All the hs-CRP values were under 10 mg/L, remaining in the range suggestive of low-grade inflammation. The mean scores of CDI 2 total and partial scales were all above the established cut-off. The most endorsed self-reported symptoms were irritability, anhedonia, self-hatred, difficulties in concentration, indecisiveness, suicidal ideation, and depressed mood. Table 1 reports the laboratory and clinical data of the sample.
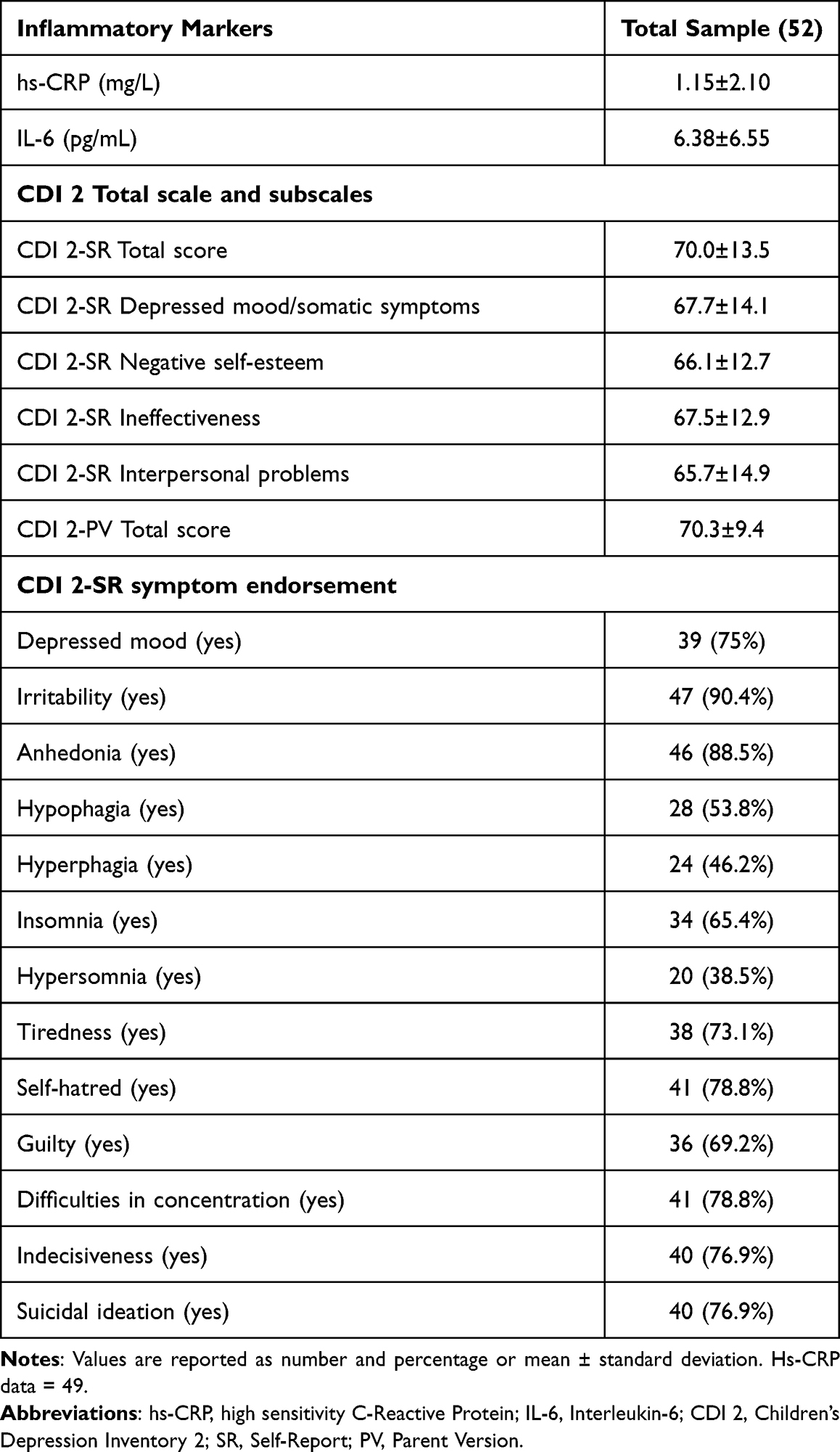 |
Table 1 Laboratory and Clinical Data of the Sample |
Associations Between Inflammation and Depression
Table 2 shows significant associations (p < 0.05) resulting from the regression analyses with inflammatory markers as independent variables and depressive symptoms as outcome measures. The complete results of the regression analyses, including all the statistically non-significant associations, are reported in Supplementary Table 1. We found significant positive associations between hs-CRP and CDI 2-PV Total score when adjusting for BMI and BMI+current SSRI medication. IL-6 was significantly associated with CDI 2-PV Total score when adjusting for BMI. The associations between inflammatory markers and the total and partial scores of CDI 2-SR were not statistically significant (Supplementary Table 1). Among the single symptom endorsement, self-hatred was the one to be significantly predicted by hs-CRP, in more than one regression model, with different combinations of covariates (Table 2).
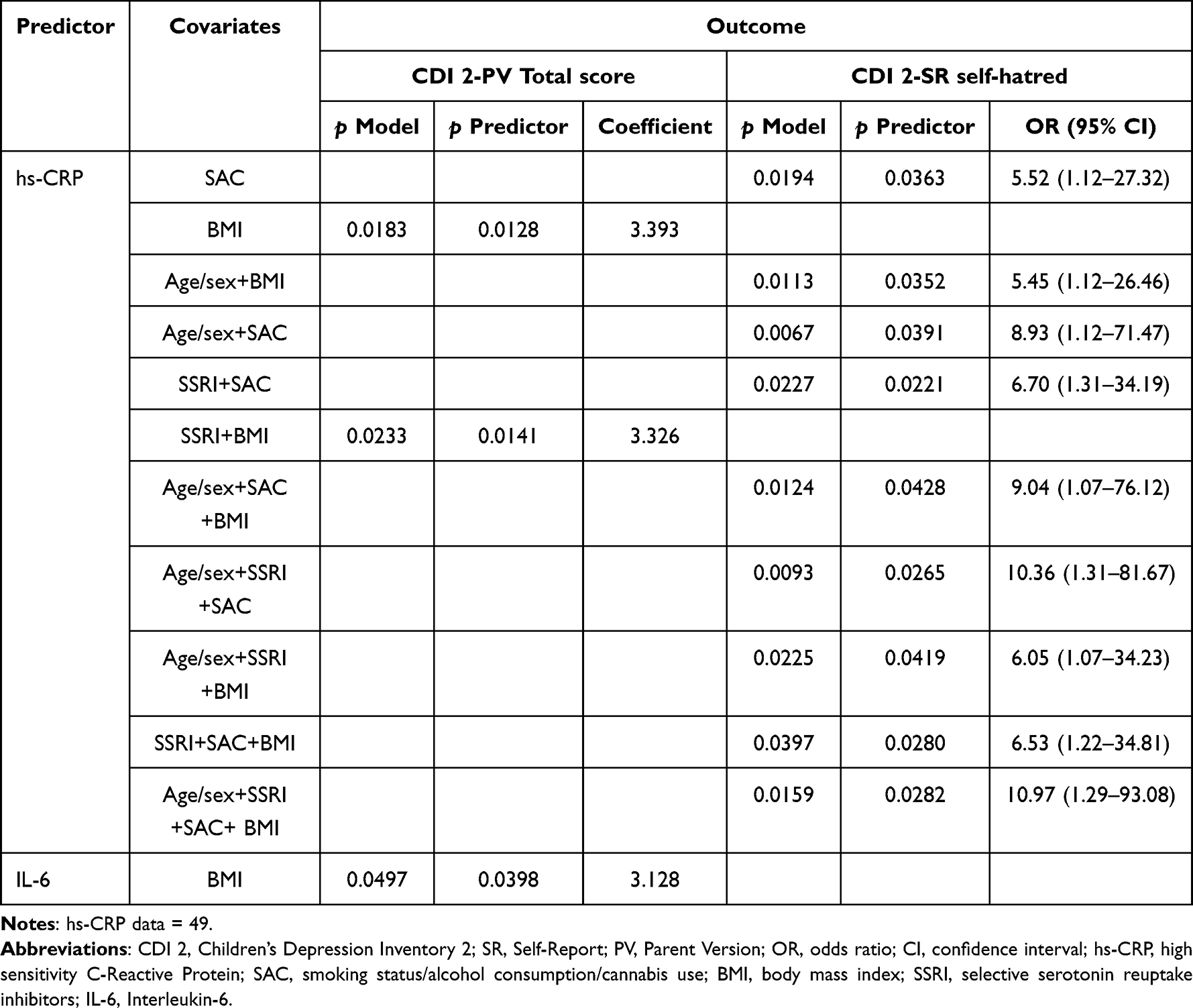 |
Table 2 Associations Between Inflammatory Markers and Depressive Symptoms |
Discussion
We studied associations between inflammatory markers and individual symptoms of depression in a sample of 52 Italian adolescents recruited during the COVID-19 pandemic. Inflammation could be particularly important during stressful periods like the current pandemic when psychosocial stressors can exert their effects by increasing inflammation with subsequent depressive modifications. We did not get measurements of self-perceived stress in daily life related to COVID-19, but the recent history tells us that the pandemic social distancing rules have enforced adolescents to a strong limitation of social relations (eg, distance learning, limitation of leisure time activities). Furthermore, we know from the literature that social isolation is considered an important psychological stressor that has been linked to increased inflammatory levels.15,18,20–22 Therefore, although we could not draw any causal inference due to the cross-sectional design of our study, we can consider as plausible that the social stress-induced inflammation could have played a role in the increased depressive rates among adolescents observed in the recent period: a recent meta-analysis estimated a global pooled prevalence of clinically elevated depression symptoms of 25.2%, during the first year of COVID-19 pandemic.39 These estimates are double the pre-pandemic ones.40
In our study, peripheral inflammatory markers were positively associated with total depressive symptoms, as reported by parents at the CDI 2-PV, and with the endorsement of the symptom self-hatred, as reported at the CDI 2-SR.
While the association between inflammation and depression has been widely studied in the adult population, limited data are available for the evolutionary age.41,42 A significant association between serum hs-CRP and depression score was detected in a sample of adolescent girls.43 In a community sample of adolescents, higher depressive symptoms were prospectively associated with elevated IL-6.44 Moreover, elevated IL-6 levels were found in a group of adolescents diagnosed with a DD compared to controls.45 Data from a recent meta-analysis of 22 studies about depression in children and adolescents confirmed a positive association between depression and current and future inflammation and their bidirectional relationship.12 On the other hand, very recent findings of children and young people showed that CRP levels were not related to depression and did not mediate the association with adverse childhood events.19 Moreover, in a recent study, proinflammatory markers were not significantly associated with psychological distress in 15–17 years old healthy adolescents.46
Our study shows that higher levels of peripheral hs-CRP were significantly associated with higher total depressive symptoms reported by parents in the CDI 2-PV when the analysis was adjusted for BMI and BMI+SSRI. We also found a significant association between IL-6 and CDI 2-PV total scores when adjusting for BMI. BMI is a known major mediator of the association between depression and inflammation. Obese people have been demonstrated to show higher levels of inflammatory markers than normal-weight people, given that the adipocytes release pro-inflammatory cytokines and promote chronic low-grade inflammation.47 Thus, it was recommended to statistically control differences in BMI when measuring the effects of inflammation in biobehavioral research, being the BMI a biological factor that can affect the circulating levels of pro-inflammatory cytokines.35 Notably, in our study, the association between inflammation and depressive symptoms was statistically significant when accounting for BMI as a confounding factor. These findings support the hypothesis that depressive symptoms are significantly predicted by peripheral inflammation. It should be taken into account the fact that the association between inflammation and depression was fully attenuated after controlling for SAC, maybe due to their potential role in explaining the association. Furthermore, maybe due to the small sample, we did not find significant correlations of inflammatory markers with total self-reported depressive levels, but only with those parent-reported, although the theoretical concurrent validity between CDI 2-SR and CDI 2-PV is good, for which high correlations between SR and PV were expectable as well as similar associations with inflammation.34
Recent studies have focused on which subgroups of depressed patients or which affective symptoms are most associated with inflammation. It has been hypothesized that IL-6 may be a “state indicator for acute exacerbation” in melancholic patients.48 Moreover, higher levels of IL-6 can predict over time the depression chronicity and higher severity.49 Other findings detected higher inflammation in association with suicidal MDD.50 Increased inflammatory markers may also characterize treatment-resistant populations of depressed patients.9,11,51
Concerning the symptom-specific link between depression and inflammation, a recent review collecting data from 21 studies reported an association between inflammation and somatic depressive symptoms but not with cognitive ones.37 Recent data from two large-scale cohorts of adults showed an association between peripheral inflammatory markers and depressed mood, anhedonia, and somatic symptoms.8 A very recent review reported a specific pattern of depressive symptoms in patients with higher blood CRP levels: fatigue, restless sleep, low energy, concentration difficulties, poor psychomotor speed, and poor executive functioning.51 Notably, most of these findings concern the adult population, while little is known about the symptom-specificity of depression-inflammation link in youngers.
We used a symptom-based approach to evaluate whether inflammation was specifically associated with certain depressive symptoms in our sample of adolescents. We selected item 6 of CDI 2-SR (self-hatred) to express the DSM-5 criteria (A7) “feelings of worthlessness”. In our study, increasing levels of hs-CRP significantly predicted the endorsement of this symptom and not others. We should consider this finding with caution, given the large width of the OR confidence intervals. This low precision of the risk estimate could be explained by the small size of the current sample, which warrants further studies. Nevertheless, the statistical significance of this association lets us consider this depressive symptom as potentially linked with inflammation.
To our knowledge, symptoms referable to worthlessness, self-deprecation, or negative self-esteem, have not yet been associated with systemic inflammation so far. On the other hand, existing data highlight the association between inflammation and somatic symptoms of depression, especially the atypical ones such as altered appetite and tiredness.52,53 However, self-hatred is one of the most important symptoms emerging from very recent studies about adolescent depression. Interestingly, in recent years, some researchers have been focusing on the network approach to psychopathology, supposing that psychiatric disorders are constituted of co-occurring symptoms and their tendency to cause each other.54 Self-hatred was the most central symptom in the adolescent depression network found by Mullarkey et al, close to sadness, loneliness, and pessimism, suggesting the high importance of these symptoms to the experience of depression in adolescence.55 Among all depressive symptoms, self-hatred had the highest strength centrality also in other two very recent studies, in clinical samples of adolescents, suggesting the idea that this symptom represents the core psychological construct in juvenile depression.56,57 Self-hatred means negatively thinking about the self. Preferential processing of negative self-referent information is a specific information processing bias that predicts an increase in depressive symptoms.58 Depression was correlated with increased negative recall bias and decreased positive recall bias.59 It is expected that more efficient processing and recall of negative descriptors about the self will lead to negative self-vision, non-acceptance, and, finally, self-hatred. Thus, self-hatred could be an extreme phenotypic expression of a “self-centered” exaggerated reactivity to negative information, which is one of the known endophenotypes of depression previously associated with inflammation.10 Inflammation was demonstrated to amplify affective and physiological responses to stressful information, contributing to reactivity to negative stimuli.10 In this way, the symptom of self-hatred could be reasonably predicted by peripheral inflammation, as resulting from the association that emerged in our study. This finding lets us consider that inflammation may activate one of the very central symptoms of the depression network, with potentially secondary activation of causally connected nodes, according to the network theory.54
A future direction of the research could be focusing on the relationship between inflammation and depression symptoms as conceptualized by the network theory. If a causal relationship between inflammation and self-hatred and other central nodes would be ascertained, it could represent a key opportunity for targeting interventions on crucial symptoms, connections between symptoms, and triggering causes of symptoms in the network.54
Another important consideration for the future direction of studies is that our findings cross data from the network theory of adolescent depression, where the symptom self-hatred is a very central node, with previous knowledge about the depression endophenotypes. Since the traits falling within the definition of an endophenotype seem to closely reflect the biological root of a specific disorder, the endophenotype approach could have a positive impact on the treatment, identifying the key biological elements underlying it. In this way, the definition of endophenotypes causally correlated with inflammation, as the “exaggerated reactivity to negative information”, could allow identifying those patient populations that could benefit from an anti-inflammatory treatment, which would instead be ineffective in unselected samples of depressed subjects.60
Strengths and limitations. This study focused on depression in adolescents, exploring the role of inflammation and its relationship with specific depressive features. This is the main strength because, to date, research examining associations between depression and inflammation has been primarily focused on the adult population. The study had important limitations needing to be highlighted. The first one was the limited size of the sample, which restricts the generalizability and reliability of findings: the large width of the OR confidence intervals is a measure of the low precision of the estimate, which is although statistically significant. Furthermore, maybe due to the small sample, we did not find significant correlations of inflammatory markers with total self-reported depressive levels, but only with those parent-reported, although the theoretical concurrent validity between CDI 2-SR and CDI 2-PV is good.29 Thus, future studies with larger samples are needed to confirm our findings; they could also assess potential sex-based differences in the depression-inflammation link which were difficult to evaluate in a sample of limited size. Second, we adopted a cross-sectional study design, which prevents causal inferences. Third, although the diagnostic assessment was carried out with a semi-structured diagnostic interview considering past and current history of depression (K-SADS PL DSM-5), we based the symptom-specific analysis on the binarization of selected items of a single psychometric instrument relative to the last two weeks (CDI 2 SR), without taking into account the previous lifetime history of depression. Fourth, the symptom “psychomotor alteration” was not included in the symptom-based analysis because it was not assessed by the CDI 2. Fifth, we used the CDI 2, a very recent psychometric instrument, but built on the DSM-IV and not DSM-5 symptomatology; this could limit the accuracy of the correspondence between the assessed symptomatology and the current diagnostic criteria of DD. Sixth, concerning the regression analysis, we did not consider other potential confounding factors of the association inflammation-depression, such as the socioeconomic level, physical inactivity, and psychiatric comorbidities, and we did not compensate for multiple comparisons. Last, we got no information about possible exposure to early negative life events, possibly linked with an enhanced inflammatory response.
Conclusion
In conclusion, in a sample of Italian adolescents affected by a DD, total depressive symptoms were positively associated with peripheral inflammatory markers, although the associations were no anymore significant in the fully-adjusted model. Furthermore, a novel symptom-specificity emerged, with hs-CRP significantly predicting the endorsement of the symptom self-hatred, recently recognized as a core feature of adolescent depression according to the network theory. From our point of view, we can consider self-hatred also as a phenotypic expression of the endophenotype “exaggerated reactivity to negative information”, previously causally linked to inflammation. Future research could focus on the relationship between inflammation and self-hatred and other central nodes of the adolescent depression network, representing a key opportunity for targeting interventions on crucial symptoms, connections between symptoms, and triggering causes of symptoms in the network.
Data Sharing Statement
The authors confirm that the data supporting the findings of this study are available within the article and its supplementary materials.
Ethics Statement
The study was approved by the Ethics Committee of the Azienda Ospedaliero Universitaria Consorziale Policlinico di Bari (Resolution n. 1858, December 2019) and conducted in accordance with the Declaration of Helsinki.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Najjar S, Pearlman DM, Alper K, Najjar A, Devinsky O. Neuroinflammation and psychiatric illness. J Neuroinflammation. 2013;10:43. doi:10.1186/1742-2094-10-43
2. Mitchell RH, Goldstein BI. Inflammation in children and adolescents with neuropsychiatric disorders: a systematic review. J Am Acad Child Adolesc Psychiatry. 2014;53(3):274–296. doi:10.1016/j.jaac.2013.11.013
3. Kiecolt-Glaser JK, Derry HM, Fagundes CP. Inflammation: depression fans the flames and feasts on the heat. Am J Psychiatry. 2015;172(11):1075–1091. doi:10.1176/appi.ajp.2015.15020152
4. Hayes JF, Khandaker GM, Anderson J, et al. Childhood interleukin-6, C-reactive protein and atopic disorders as risk factors for hypomanic symptoms in young adulthood: a longitudinal birth cohort study. Psychol Med. 2017;47(5):23–33. doi:10.1017/S0033291716003408
5. Orsolini L, Sarchione F, Vellante F, et al. Protein-C reactive as biomarker predictor of schizophrenia phases of illness? A systematic review. Curr Neuropharmacol. 2018;16(5):583–606. doi:10.2174/1570159X16666180119144538
6. Copeland WE, Shanahan L, Worthman C, Angold A, Costello EJ. Cumulative depression episodes predict later C-reactive protein levels: a prospective analysis. Biol Psychiatry. 2012;71(1):15–21. doi:10.1016/j.biopsych.2011.09.023
7. Köhler CA, Freitas TH, Maes M, et al. Peripheral cytokine and chemokine alterations in depression: a meta-analysis of 82 studies. Acta Psychiatr Scand. 2017;135(5):373–387. doi:10.1111/acps.12698
8. Milaneschi Y, Kappelmann N, Ye Z, et al. Association of inflammation with depression and anxiety: evidence for symptom-specificity and potential causality from UK Biobank and NESDA cohorts. Mol Psychiatry. 2021. 26(12):7393–7402. doi:10.1038/s41380-021-01188-w
9. Chamberlain SR, Cavanagh J, de Boer P, et al. Treatment-resistant depression and peripheral C-reactive protein. Br J Psychiatry. 2019;214(1):11–19. doi:10.1192/bjp.2018.66
10. Dooley LN, Kuhlman KR, Robles TF, Eisenberger NI, Craske MG, Bower JE. The role of inflammation in core features of depression: insights from paradigms using exogenously-induced inflammation. Neurosci Biobehav Rev. 2018;94:219–237. doi:10.1016/j.neubiorev.2018.09.006
11. Beurel E, Toups M, Nemeroff CB. The bidirectional relationship of depression and inflammation: double trouble. Neuron. 2020;107(2):234–256. doi:10.1016/j.neuron.2020.06.002
12. Colasanto M, Madigan S, Korczak DJ. Depression and inflammation among children and adolescents: a meta-analysis. J Affect Disord. 2020;277:940–948. doi:10.1016/j.jad.2020.09.025
13. Pariante CM. Why are depressed patients inflamed? A reflection on 20 years of research on depression, glucocorticoid resistance and inflammation. Eur Neuropsychopharmacol. 2017;27(6):554–559. doi:10.1016/j.euroneuro.2017.04.001
14. Gottesman II, Gould TD. The endophenotype concept in psychiatry: etymology and strategic intentions. Am J Psychiatry. 2003;160(4):636–645. doi:10.1176/appi.ajp.160.4.636
15. Slavich GM, Irwin MR. From stress to inflammation and major depressive disorder: a social signal transduction theory of depression. Psychol Bull. 2014;140(3):774–815. doi:10.1037/a0035302
16. Jonker I, Rosmalen JGM, Schoevers RA. Childhood life events, immune activation and the development of mood and anxiety disorders: the TRAILS study. Transl Psychiatry. 2017;7(5):e1112. doi:10.1038/tp.2017.62
17. Bullmore E. The art of medicine. Inflamed depression. Lancet. 2018;392(10154):1189–1190. doi:10.1016/S0140-6736(18)32356-0
18. Smith JK, Gavey S, Riddel NE, Kontari P, Victor C. The association between loneliness, social isolation and inflammation: a systematic review and meta-analysis. Neurosci Biobehav Rev. 2020;112:519–541. doi:10.1016/j.neubiorev.2020.02.002
19. Iob E, Lacey R, Giunchiglia V, Steptoe A. Adverse childhood experiences and severity levels of inflammation and depression from childhood to young adulthood: a longitudinal cohort study. Mol Psychiatry. 2022;27:2255–2263. doi:10.1038/s41380-022-01478-x
20. Lacey RE, Kumari M, Bartley M. Social isolation in childhood and adult inflammation: evidence from the National Child Development Study. Psychoneuroendocrinology. 2014;50:85–94. doi:10.1016/j.psyneuen.2014.08.007
21. Eisenberger NI, Moieni M, Inagaki TK, Muscatell KA, Irwin MR. In sickness and in health: the co-regulation of inflammation and social behavior. Neuropsychopharmacology. 2017;42(1):242–253. doi:10.1038/npp.2016.141
22. Leschak CJ, Eisenberger NI. Two distinct immune pathways linking social relationships with health: inflammatory and antiviral processes. Psychosom Med. 2019;81(8):711–719. doi:10.1097/PSY.0000000000000685
23. Hänsel A, Hong S, Cámara RJA, von Känel R. Inflammation as a psychophysiological biomarker in chronic psychosocial stress. Neurosci Biobehav Rev. 2010;35(1):115–121. doi:10.1016/j.neubiorev.2009.12.012
24. Heffner KL, Waring ME, Roberts MB, Eaton CB, Gramling R. Social isolation, C-reactive protein, and coronary heart disease mortality among community-dwelling adults. Soc Sci Med. 2011;72(9):1482–1488. doi:10.1016/j.socscimed.2011.03.016
25. Jiang NM, Cowan M, Moonah SN, Petri WA Jr. The impact of systemic inflammation on neurodevelopment. Trends Mol Med. 2018;24(9):794–804. doi:10.1016/j.molmed.2018.06.008
26. Magson NR, Freeman JYA, Rapee RM, Richardson CE, Oar EL, Fardouly J. Risk and protective factors for prospective changes in adolescent mental health during the COVID-19 pandemic. J Youth Adolesc. 2021;50(1):44–57. doi:10.1007/s10964-020-01332-9
27. Panchal U, Salazar de Pablo G, Franco M, et al. The impact of COVID-19 lockdown on child and adolescent mental health: systematic review. Eur Child Adolesc Psychiatry. 2021;18:1–27. doi:10.1007/s00787-021-01856-w
28. Raony I, Saggioro `de Figueiredo C, Pandolfo P, Giestal-de-Araujo E, Priscilla Oliveira-Silva Bomfim POS, Savino W. Psycho-neuroendocrine-immune interactions in COVID-19: potential impacts on mental health. Front Immunol. 2020;1:1170. doi:10.3389/fimmu.2020.01170
29. Jokela M, Virtanen M, Batty GD, Kivimäki M. Inflammation and specific symptoms of depression. JAMA Psychiatry. 2016;73(1):87–88. doi:10.1001/jamapsychiatry.2015.1977
30. Fegert JM, Vitiello B, Plener PL, Clemens V. Challenges and burden of the coronavirus 2019 (COVID-19) pandemic for child and adolescent mental health: a narrative review to highlight clinical and research needs in the acute phase and the long return to normality. Child Adolesc Psychiatry Ment Health. 2020;14:20. doi:10.1186/s13034-020-00329-3
31. Wade M, Prime H, Browne DT. Why we need longitudinal mental health research with children and youth during (and after) the COVID-19 pandemic. Psychiatry Res. 2020;290:113143. doi:10.1016/j.psychres.2020.113143
32. American Psychiatric Association (APA). Depressive Disorders. In: Diagnostic and Statistical Manual of Mental Disorders,
33. Kaufman J, Birmaher B, Axelson D, Perepletchova F, Brent D, Ryan N. K-SADS-PL DSM-5. Diagnostic interview for the assessment of psychopathological disorders in children and adolescents. Italian edition by Carla Sogos, Sofia Pia Di Noia, Francesca Fiorello, Giorgia Picchiotti. Trento: Erickson; 2019.
34. Kovacs M. Children’s Depression Inventory.
35. O’Connor MF, Bower JE, Cho HJ, et al. To assess, to control, to exclude: effects of biobehavioral factors on circulating inflammatory markers. Brain Behav Immun. 2009;23(7):887–897. doi:10.1016/j.bbi.2009.04.005
36. Duivis HE, Vogelzangs N, Kupper N, de Jonge P, Penninx BW. Differential association of somatic and cognitive symptoms of depression and anxiety with inflammation: findings from the Netherlands Study of Depression and Anxiety (NESDA). Psychoneuroendocrinology. 2013;38(9):1573–1585. doi:10.1016/j.psyneuen.2013.01.002
37. Majd M, Saunders EFH, Engeland CG. Inflammation and the dimensions of depression: a review. Front Neuroendocrinol. 2020;56:100800. doi:10.1016/j.yfrne.2019.100800
38. Henshaw FR, Dewsbury LS, Lim CK, Steiner GZ. The effects of cannabinoids on pro- and anti-inflammatory cytokines: a systematic review of in vivo studies. Cannabis Cannabinoid Res. 2021;6(3):177–195. doi:10.1089/can.2020.0105
39. Racine N, McArthur BA, Cooke JE, Eirich R, Zhu J, Madigan S. Global prevalence of depressive and anxiety symptoms in children and adolescents during COVID-19. JAMA Pediatr. 2021;175(11):1142–1150. doi:10.1001/jamapediatrics.2021.2482
40. Lu W. Adolescent depression: national trends, risk factors, and healthcare disparities. Am J Health Behav. 2019;43(10):181–194. doi:10.1001/jamanetworkopen.2021.30280
41. Martins LB, Delevati Colpo G, Calarge CA, Teixeira AL. Inflammatory markers profile in older adolescents during treatment with selective serotonin reuptake inhibitors. J Child Adolesc Psychopharmacol. 2021;31(6):439–444. doi:10.1089/cap.2020.0140
42. Mondelli V, Cattaneo A, Nikkheslat N, et al. Exploring the role of immune pathways in the risk and development of depression in adolescence: research protocol of the IDEA-FLAME study. Brain Behav Immun Health. 2021;18:100396. doi:10.1016/j.bbih.2021.100396
43. Tabatabaeizadeh SA, Abdizadeh MF, Meshkat Z, et al. There is an association between serum high-sensitivity C-reactive protein (hs-CRP) concentrations and depression score in adolescent girls. Psychoneuroendocrinology. 2018;88:102–104. doi:10.1016/j.psyneuen.2017.11.014
44. Mac Giollabhui N, Swistun D, Murray S, et al. Executive dysfunction in depression in adolescence: the role of inflammation and higher body mass. Psychol Med. 2020;50(4):683–691. doi:10.1017/S0033291719000564
45. Peters AT, Ren X, Bessette KL, et al. Interplay between pro-inflammatory cytokines, childhood trauma, and executive function in depressed adolescents. J Psychiatr Res. 2019;114:1–10. doi:10.1016/j.jpsychires.2019.03.030
46. Linkas J, Ahmed LA, Csifcsak G, et al. Are pro-inflammatory markers associated with psychological distress in a cross-sectional study of healthy adolescents 15–17 years of age? The fit futures study. BMC Psychol. 2022;10(1):65. doi:10.1186/s40359-022-00779-8
47. Kyrou I, Chrousos GP, Tsigos C. Stress, visceral obesity, and metabolic complications. Ann N Y Acad Sci. 2006;1083:77–110. doi:10.1196/annals.1367.008
48. Dunjic-Kostic B, Ivkovic M, Radonjic NV, et al. Melancholic and atypical major depression–connection between cytokines, psychopathology and treatment. Prog Neuropsychopharmacol Biol Psychiatry. 2013;43:1–6. doi:10.1016/j.pnpbp.2012.11.009
49. Lamers F, Milaneschi Y, Smit JH, Schoevers RA, Wittenberg G, Penninx BWJH. Longitudinal association between depression and inflammatory markers: results from the Netherlands Study of Depression and Anxiety. Biol Psychiatry. 2019;85(10):829–837. doi:10.1016/j.biopsych.2018.12.020
50. Black C, Miller BJ. Meta-Analysis of cytokines and chemokines in suicidality: distinguishing suicidal versus nonsuicidal patients. Biol Psychiatry. 2015;78(1):28–37. doi:10.1016/j.biopsych.2014.10.014
51. Orsolini L, Pompili S, Tempia Valenta S, Salvi V, Volpe U. C-reactive protein as biomarker for major depressive disorder? Int J Mol Sci. 2022;23(3):1616. doi:10.3390/ijms23031616
52. Lamers F, Milaneschi Y, de Jonge P, Giltay EJ, Penninx BWJH. Metabolic and inflammatory markers: associations with individual depressive symptoms. Psychol Med. 2018;48(7):1102–1110. doi:10.1017/S0033291717002483
53. Gialluisi A, Di Castelnuovo A, Bracone F, et al. Associations between systemic inflammation and somatic depressive symptoms: findings from the Moli-sani study. Depress Anxiety. 2020;37(9):935–943. doi:10.1002/da.23070
54. Borsboom D. A network theory of mental disorders. World Psychiatry. 2017;16(1):5–13. doi:10.1002/wps.20375
55. Mullarkey MC, Marchetti I, Beevers CG. Using network analysis to identify central symptoms of adolescent depression. J Clin Child Adolesc Psychol. 2019;48(4):656–668. doi:10.1080/15374416.2018.1437735
56. Kim KM, Kim H, Kim D, Kim JW. The analysis of network structure among the depressive symptoms in a clinical sample of children and adolescents. Asian J Psychiatr. 2021;62:102748. doi:10.1016/j.ajp.2021.102748
57. Manfro PH, Pereira RB, Rosa M, et al. Adolescent depression beyond DSM definition: a network analysis. Eur Child Adolesc Psychiatry. 2021. doi:10.1007/s00787-021-01908-1
58. Connolly SL, Abramson LY, Alloy LB. Information processing biases concurrently and prospectively predict depressive symptoms in adolescents: evidence from a self-referent encoding task. Cogn Emot. 2016;30(3):550–560. doi:10.1080/02699931.2015.1010488
59. Speed BC, Nelson BD, Auerbach RP, Klein DN, Hajcak G. Depression risk and electrocortical reactivity during self-referential emotional processing in 8 to 14 year-old girls. J Abnorm Psychol. 2016;125(5):607–619. doi:10.1037/abn0000173
60. Miller AH, Pariante CM. Trail failures of anti-inflammatory drugs in depression. Lancet Psychiatry. 2020;7(10):837. doi:10.1016/S2215-0366(20)30357-6
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Alleviating Excessive Worries Improves Co-Occurring Depression and Pain in Adolescent and Young Adult Cancer Patients: A Network Approach
Li W, Xu Y, Luo X, Wen Y, Ding K, Xu W, Garg S, Yang Y, Sun H
Neuropsychiatric Disease and Treatment 2022, 18:1843-1854
Published Date: 25 August 2022
Elevated C-Reactive Protein and Erythrocyte Sedimentation Rate Correlates with Depression in Psoriasis: A Chinese Cross-Sectional Study
Tan M, Luo Y, Hu J, Hu K, Li X, Yang J, Chen J, Zhu W, Kuang Y
Clinical, Cosmetic and Investigational Dermatology 2023, 16:397-405
Published Date: 13 February 2023
The Inhibition of Evolocumab on Non-Infarct-Related Artery Disease in Patients with ST-Elevation Myocardial Infarction
Zhao Q, Sun S, Zhou F, Yue J, Luo X, Qu X
International Journal of General Medicine 2023, 16:2771-2781
Published Date: 30 June 2023
Wenyang-Tianjing-Jieyu Decoction Improves Depression Rats of Kidney Yang Deficiency Pattern by Regulating T Cell Homeostasis and Inflammation Level
Zhang T, Wang J, Wang Y, He L, Lv S, Wang Y, Li W
Neuropsychiatric Disease and Treatment 2024, 20:631-647
Published Date: 22 March 2024
Blood Marker-Based Machine Learning Model for Survival Prediction in Patients with Pneumoconiosis: Construction and External Validation
Huang Q, Feng M, Chen Z, Zhang J, Feng Z
Journal of Inflammation Research 2026, 19:555051
Published Date: 26 February 2026