Back to Journals » Journal of Pain Research » Volume 19
Baseline Inflammatory Cytokines Moderate Associations Between Intraoperative Oxidative Stress and Chronic Postsurgical Pain After Total Knee Arthroplasty: An Exploratory Study
Authors Durbhakula S, Rassu FS, Billings FT 4th, Martin JR, Polkowski GG, Milne GL, Bruehl S
Received 2 March 2026
Accepted for publication 26 May 2026
Published 6 June 2026 Volume 2026:19 602792
DOI https://doi.org/10.2147/JPR.S602792
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ryan D'Souza
Shravani Durbhakula,1 Fenan S Rassu,2 Frederic T Billings 4th,1 J Ryan Martin,3 Gregory G Polkowski,3 Ginger L Milne,4 Stephen Bruehl1
1Department of Anesthesiology, Vanderbilt University Medical Center, Nashville, TN, USA; 2Department of Physical Medicine and Rehabilitation, Johns Hopkins School of Medicine, Baltimore, MD, USA; 3Department of Orthopedics, Vanderbilt University Medical Center, Nashville, TN, USA; 4Department of Medicine, Vanderbilt University Medical Center, Nashville, TN, USA
Correspondence: Shravani Durbhakula, Vanderbilt University Medical Center, Department of Anesthesiology, 1211 21st Avenue South, Nashville, TN, 37215, USA, Email [email protected]
Purpose: A substantial proportion of patients experience chronic postsurgical pain (CPSP) following total knee arthroplasty (TKA); yet, factors contributing to CPSP remain poorly defined, limiting mechanism-based treatments. Although perioperative oxidative stress (OS) has been associated with CPSP, it is unknown whether baseline cytokine levels, which affect nociceptor sensitization, modify the impact of OS on long term post-TKA pain outcomes.
Methods: This exploratory secondary analysis included 58 adults undergoing unilateral primary total knee arthroplasty. Pre-incision, baseline plasma interleukin-6 (IL-6), tumor necrosis factor alpha (TNF-α), and interleukin-10 (IL-10) were measured. Intraoperative OS was measured by quantifying plasma concentrations of F2-isoprostanes and isofurans across three intraoperative time points. Six-month post-TKA outcomes included numeric rating scale (NRS) pain intensity, Short Form McGill Pain Questionnaire 2 (MPQ-2), PROMIS Pain Interference, and Knee Injury and Osteoarthritis Outcome Score for Joint Replacement.
Results: Baseline cytokines were positively correlated with intraoperative OS. Hierarchical regressions indicated that IL-6 positively modified the effect of OS on average 6-month NRS pain intensity, and TNF-α and IL-10 positively modified the effect of OS on the MPQ-2 Neuropathic subscale. Simple effect analyses indicated in each case that higher intraoperative OS was associated with worse pain among participants with higher baseline cytokine levels, with no association observed at lower cytokine levels.
Conclusion: Increased baseline inflammatory cytokine levels increased the association between increased intraoperative OS and six-month pain outcomes post-TKA, suggesting a biological “double-hit” in which inflammation and OS interact to increase CPSP vulnerability. Given the exploratory nature of these analyses, replication in larger cohorts is needed. These exploratory analyses were not corrected for multiple comparisons; therefore, findings should be interpreted as hypothesis-generating.
Keywords: oxidative stress, total knee arthroplasty, inflammation, cytokines
Introduction
Total knee arthroplasty (TKA) is one of the most commonly performed surgical procedures to improve mobility and quality of life in older adults, with over 1 million procedures performed annually and projected volumes exceeding 2.8 million by 2040.1 Although TKA is highly effective for most patients, at least 15% continue to experience persistent postoperative pain that impairs function long after surgical healing.2–4 Chronic postsurgical pain (CPSP) following TKA is associated with prolonged opioid use and associated risks.5 The mechanisms driving the transition from acute postoperative pain to CPSP remain incompletely understood. Identifying preoperative and intraoperative biological factors that shape long-term pain vulnerability is therefore a priority for perioperative precision medicine, with implications for patient selection, risk stratification, and targeted intervention.
Growing evidence implicates immune signaling—and specifically the cytokines interleukin-6 (IL-6), tumor necrosis factor-α (TNF-α), and interleukin-10 (IL-10)—in postoperative pain trajectories.6 Pro-inflammatory cytokines IL-6 and TNF-α contribute to leukocyte recruitment, sensitization of peripheral and central nociceptive pathways, and activation of spinal microglia7–9—mechanisms fundamental to the transition from acute to chronic pain.10 Consistent with this, elevated preoperative TNF-α predicts more severe early postoperative pain phenotypes, including heightened complex regional pain syndrome (CRPS) features at six weeks following TKA.11 In another TKA cohort, TNF-α gene expression was significantly higher preoperatively in patients who later developed CPSP,12 underscoring the role of baseline inflammatory tone in shaping pain outcomes. IL-6, while pro-inflammatory and associated with acute postoperative pain, has nonetheless been linked to reduced chronic pain risk in one musculoskeletal surgery cohort,13 highlighting its pleiotropic and context-dependent effects.
In contrast, IL-10 is generally characterized as an anti-inflammatory cytokine with important immune-regulatory effects. IL-10 suppresses pro-inflammatory cytokine production,14,15 modulates glial activation,16 and limits central sensitization.6 Clinically, reduced systemic levels of anti-inflammatory cytokines, including IL-10, have been observed in patients with widespread pain,17 and individuals who developed CPSP after TKA exhibited significantly lower preoperative synovial IL-10 concentrations than those with minimal pain.18 These findings suggest that lower IL-10 may increase vulnerability to chronic postsurgical pain. However, IL-10 can also be pleiotropic and may increase as part of a compensatory or homeostatic response to heightened inflammatory activity.19 Thus, elevated IL-10 levels may not always indicate a protected immune state, but may instead reflect an activated immune-regulatory response in the setting of greater underlying inflammatory burden. Collectively, IL-6, TNF-α, and IL-10 emerge as mechanistically and clinically relevant biomarkers that may help characterize a patient’s postsurgical pain phenotype.
Oxidative stress (OS) represents another biological pathway relevant to perioperative pain outcomes.20 Surgical ischemia—reperfusion, tissue manipulation, and metabolic demand—generate reactive oxygen species that lead to OS.21 Clinically, elevated perioperative OS has been linked to worse long-term pain and function after TKA.22,23 Human experimental work further suggests possible OS-related hyperalgesia, with associations reported between elevated OS markers and reduced pain threshold (ie., increased pain sensitivity) on evoked laboratory pain testing.24 Of note, F2-isoprostanes (IsoP; the most sensitive and specific in vivo OS marker)20,25 generated during OS have been found to sensitize and enhance firing of C-nociceptors,26 trigger release of inflammatory mediators,26 and directly activate ion channels such as TRPA1 that are implicated in chronic pain.27
Mechanistic work provides some biological support for interactions between OS and cytokine systems. Preclinical studies demonstrate that OS is linked to activation of NF-κB28 and MAPK signaling,29 and activation of MAPK in immune cells and spinal microglia stimulates production of IL-6 and TNF-α,29,30 amplifying neuroinflammatory cascades. Moreover, in vitro work indicates that pro-inflammatory cytokines can further increase OS, thus creating a positive feedback loop that may sustain inflammatory signaling.31
Despite these mechanistic insights, human investigations into whether and how OS and cytokines may interact to shape pain outcomes in the postoperative setting remain limited. One study in patients undergoing laryngeal resection reported a significant positive correlation between an OS biomarker and IL-6 in the week after surgery, however they did not report associations with postoperative pain. To our knowledge, no human study has evaluated whether preoperative cytokine levels modify the effect of intraoperative OS on long-term pain after surgery. We hypothesized that elevated pro-inflammatory cytokines would amplify the effect of intraoperative OS on chronic pain outcomes. The current exploratory study tests whether baseline (pre-incision) systemic (plasma) levels of IL-6, TNF-α, and IL-10 moderate the relationship between intraoperative OS (indexed by F2-Isoprostanes [IsoP] and isofurans [IsoF], the best available biomarkers) and six-month pain and functional outcomes following TKA.
Material and Methods
Design
This study used a mixed between/within-subjects longitudinal design. Results reported below are a secondary analysis of a dataset detailed previously.22,23
Participants
Study participants were individuals undergoing unilateral primary TKA for the treatment of degenerative knee joint changes and pain related to osteoarthritis. Participants were recruited primarily in-person from the multi-surgeon orthopedic practice at Vanderbilt University Medical Center (VUMC) by the research coordinator, in accordance with IRB requirements, and through introductory presentations during a pre-operative TKA education session. Some later enrollees were recruited by telephone in response to COVID-related modifications in clinical procedures. Individuals who expressed interest after being provided with study information were screened for eligibility. All study participants provided informed consent prior to study participation. Enrollment occurred between August 2017 and June 2021, and all study procedures were approved by the VUMC Institutional Review Board, IRB #150295. All study procedures complied with the Declaration of Helsinki.
Study participation was contingent on the following inclusion criteria: 1) intact cognitive status with ability to provide informed consent (Mini Mental State Examination score ≥24),32 2) ability to read and write in English sufficiently for understanding and completion of study questionnaires, 3) at least age 55 years, 4) scheduled unilateral TKA, and 5) a known osteoarthritis diagnosis. Exclusion criteria were: 1) scheduled TKA revision; 2) diagnosed complex regional pain syndrome, lower extremity vascular disease, inflammatory or autoimmune disorders, or malignancy; and 4) any other known medical conditions that per the orthopedic surgeons would make participation unsafe. In exchange for completing the entire study, participants were compensated $200.
Of the pool of 985 potential participants identified, 303 patients expressed their interest in the study and were screened. Of those initially screened, 120 patients provided consent but 7 subsequently failed screening for reasons such as cognitive dysfunction or medical exclusions, and the resulting sample was n = 113 with no participants lost to follow up. It was after the study started that the decision to obtain blood samples for cytokine assays was made. Thus, the number of patients available for the current study was reduced. The final analyzed sample for this study reflects all participants from the pool above with available intraoperative OS and baseline proinflammatory cytokine levels (n = 58). A comparison of the analyzed sample (n = 58) to non-analyzed participants (n = 54) on demographics, baseline pain, and 6-month outcomes revealed no significant differences (all p >0.05; Supplementary Table S2), consistent with the logistical rather than clinical nature of the missing cytokine data. For preoperative demographics of study participants and descriptive measures, see the summary presented in Table 1. The sample consisted of older adults, mostly white and non-Hispanic, with nearly 2/3 female.
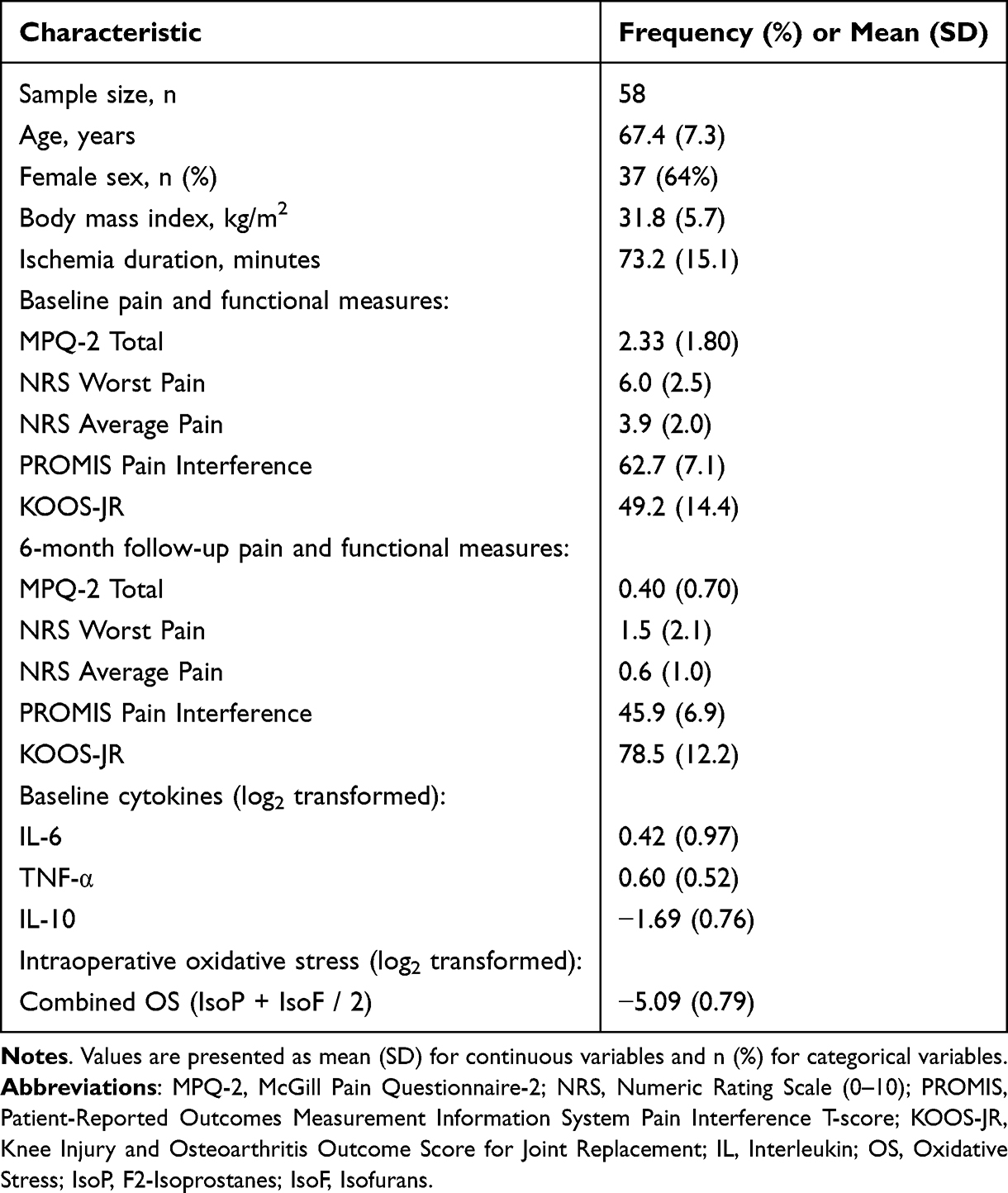 |
Table 1 Participant Demographic and Clinical Characteristics (n=58) |
Oxidative Stress Assays
We quantified systemic OS by measuring plasma concentrations of IsoP and IsoF. Both IsoP and IsoF exhibit stability in biological tissues and fluids.20,25 They are products of non-enzymatic arachidonic acid peroxidation as well as end products of a common lipid radical intermediate. Oxygen concentration determined the relative production of IsoP versus IsoF, and gas chromatography/negative ion chemical ionization mass spectrometry (GC/NICI-MS) as earlier described by our laboratory33 was used for quantification. For in depth descriptions of OS assay procedures and assay results in this sample, see our prior work.11,22,23,34 Consistent with previous work,35 to minimize the confounding effects of differing oxygen concentrations, we derived and analyzed a combined OS variable reflecting the mean concentration of IsoP and IsoF.
Inflammatory Cytokine Assays
Using a Meso Scale Diagnostics V-Plex Human Proinflammatory Panel with electrochemiluminescent detection (Meso Scale Diagnostics, Rockville, MD), circulating levels of IL-6, TNF-α, and IL-10 were measured. Assays were performed according to the manufacturer’s protocol and read using a QuickPlex SQ120 instrument (Meso Scale Diagnostics, Rockville, MD). Plasma samples were analyzed in duplicate, and assay results are reported as the mean of duplicate measurements in pg/mL. Manufacturer-reported median lower limits of detection were 0.06 pg/mL for IL-6, 0.04 pg/mL for TNF-α, and 0.04 pg/mL for IL-10. Values below the lower limit of detection were coded as 0. All samples were analyzed in a single batch, and laboratory personnel were blinded to clinical outcomes.
Pain and Functional Outcomes
Long-Term Post-TKA Pain Outcomes
Participants were asked to rate the worst and average knee pain intensity experienced in the 24 hours preceding assessment at the 6-month follow-up using a 0–10 NRS anchored with “no pain” and “worst possible pain”.36 More qualitative aspects of knee pain intensity (on a 0–10 scale) in the week prior to the 6 month follow-up visit were also rated using the Short Form-McGill Pain Questionnaire 2 (MPQ-2).37
Long-Term Post-TKA Functional Outcomes
Patients rated pain-related life interference over the past week at 6-month follow-up using the PROMIS Short Form v1.0 - Pain Interference 8a scale (PROMIS Interference).38 Scores are reported as T-scores (relative to the general population) with a mean of 50 and standard deviation of 10, with higher scores indicating greater pain-related limitations. The Knee Injury and Osteoarthritis Outcome Score for Joint Replacement (KOOS-JR)39 was used to assess movement-evoked pain and functional limitations in the week preceding the 6 month assessment. Raw scores were converted to interval scores according to standard procedures in the scoring manual, with lower scores indicating greater movement-evoked pain and worse function.
Procedure
A research coordinator performed a baseline preoperative assessment session at the participant’s home upon completion of informed consent (median = 3.0 days before surgery). During this meeting, patients completed a demographic questionnaire as well as the pain and functional measure questionnaires described above.
Intraoperative anesthesia on the day of surgery consisted of spinal anesthesia and sedation/maintenance anesthesia care for most patients (84.5%), although 15.5% of patients received general endotracheal anesthesia with a volatile anesthetic based on their preference or medical necessity. Anesthesia type did not significantly affect pain and functional outcomes at follow-up (all p’s >0.10). In the operating room following anesthesia induction, blood was drawn from an intravenous catheter for OS and inflammatory cytokine assays (8 mL). Blood was drawn three times: immediately pre-incision (for OS and cytokine assays), 45 minutes post tourniquet placement (OS only), and 15 minutes post tourniquet removal (OS only). The intraoperative tourniquet was applied for a median duration of 68.5 minutes (IQR: 18.5). Prior work in this sample indicated that tourniquet duration was independent of intraoperative OS levels.23 For all assays, blood was drawn into anticoagulant EDTA tubes with added glutathione and butylated hydroxytoluene and then immediately stored on ice. Samples were transported rapidly to the laboratory where they were centrifuged at 1000G at 4° C for 10 minutes, plasma separated and stored in a cryovial at −80°C until they were analyzed.
The research coordinator conducted follow-up assessment sessions in the participant’s home at 6 months (24–28 week window) following the surgery to again obtain the pain and functional outcomes. All participants completed follow up (none were lost).
Data Analysis
All statistical analyses were conducted using R (v4.2.3). Descriptive statistics (means, standard deviations, frequencies) were calculated for the final analytic sample (N=58). For each timepoint (pre-incision, mid-tourniquet, and post-tourniquet), IsoP and IsoF concentrations were averaged to create a Combined OS value. These three Combined OS values were then averaged across the three timepoints to create the Intraoperative Combined OS measure. This variable was then log2-transformed prior to analysis to address significant positive skewness. Cytokine variables (IL-6, TNF-α, IL-10) were similarly log2-transformed due to violations of normality assumptions.
To examine bivariate unadjusted relationships between key variables, Spearman’s rank-order correlations were computed between baseline (pre-incision) cytokine levels (IL-6, TNF-α, IL-10), the combined oxidative stress (OS) measure, and 6-month pain and functional outcomes, given the non-normal distributions of the raw biomarker variables. To test the primary hypothesis that baseline cytokines moderate the relationship between intraoperative OS and 6-month pain-related outcomes, separate hierarchical linear regression models were conducted for each combination of cytokine moderator (IL-6, TNF-α, IL-10) and pain outcome. We focused here on seven outcomes at 6-month post-TKA follow-up: MPQ-2 Total score and the MPQ-2 Continuous and Neuropathic subscales (analyses of MPQ-2 Intermittent and Affective subscales were all nonsignificant and are not detailed further); NRS Worst and Average Pain, KOOS-JR, and PROMIS Pain Interference. For each model, covariates (sex, age, BMI, and ischemia duration)23 were entered in the first step, along with the baseline value of the targeted outcome (thus, results reflected baseline-corrected change from baseline in each pain-related outcome). The main effects for intraoperative OS and the baseline cytokine moderator (both log2 transformed) were entered in the second step. A two-way multiplicative interaction term (OS × Cytokine) was entered in the final step. To address multiple testing, Benjamini-Hochberg false discovery rate (FDR) adjusted p-values were computed across all 21 interaction tests and are reported in Supplementary Table S1.
To reduce multicollinearity in interaction models and facilitate interpretation, all continuous predictors (age, BMI, ischemia duration, baseline values of the outcome measure, OS, and cytokines) were mean-centered prior to model entry. This procedure successfully reduced all variance inflation factors (VIFs) to below 2.0. Residual diagnostics were conducted for all models. Homoscedasticity assumptions were met and VIFs confirmed acceptable multicollinearity levels. As a sensitivity analysis addressing potential distributional concerns, bootstrapped 95% confidence intervals (2,000 replicates, bias-corrected and accelerated method) were computed for significant interaction terms. Bootstrapped point estimates were consistent with parametric estimates, though confidence intervals were wider, reinforcing the preliminary nature of these findings. Some departures from residual normality were observed; however, linear regression coefficient estimates are robust to moderate non-normality in samples of this size.
Given the exploratory nature of the study, for all models resulting in an OS X cytokine interaction that was significant (p < 0.05) or approaching significance (p < 0.10), formal simple effects tests were conducted to evaluate the conditional slope of OS on pain and functional outcomes at both high (+1 SD above the mean) and low (−1 SD) levels of the cytokine moderator. Standard errors and significance tests for conditional slopes were computed using the variance-covariance matrix of model coefficients. For significant interactions, Cohen’s f2 was calculated to quantify the proportion of variance explained by the interaction term beyond main effects.
Finally, in line with the exploratory nature of this study, models that did not yield an interaction that was significant or approaching significance were subsequently examined for significant main effects of either intraoperative OS or the baseline cytokine measure.
Results
Sample Characteristics and Bivariate Correlations
The final analyzed sample consisted of 58 participants (64% female, mean age 67.5 ± 7.3 years, BMI 31.8 ± 5.7 kg/m2) with complete data on baseline cytokines, intraoperative OS, and covariates (see Table 1 for full characteristics). At 6 months post-surgery, pain levels were generally low (eg., NRS Average: 0.60 ± 1.01). However, 22% (n=13) of participants continued to report worst pain in the past 24 hours of ≥3/10 at 6 month follow-up.
Bivariate correlations (Table 2) showed that pro-inflammatory cytokines were significantly intercorrelated. Baseline cytokines also demonstrated significant positive correlations with intraoperative OS. Intraoperative OS, in turn, was significantly correlated with several 6-month pain outcomes, including MPQ-2 Total and NRS Average Pain. Intraoperative OS was also significantly correlated with both functional outcomes (KOOS-JR and PROMIS Pain Interference). None of the baseline cytokines were significantly correlated with either functional measure.
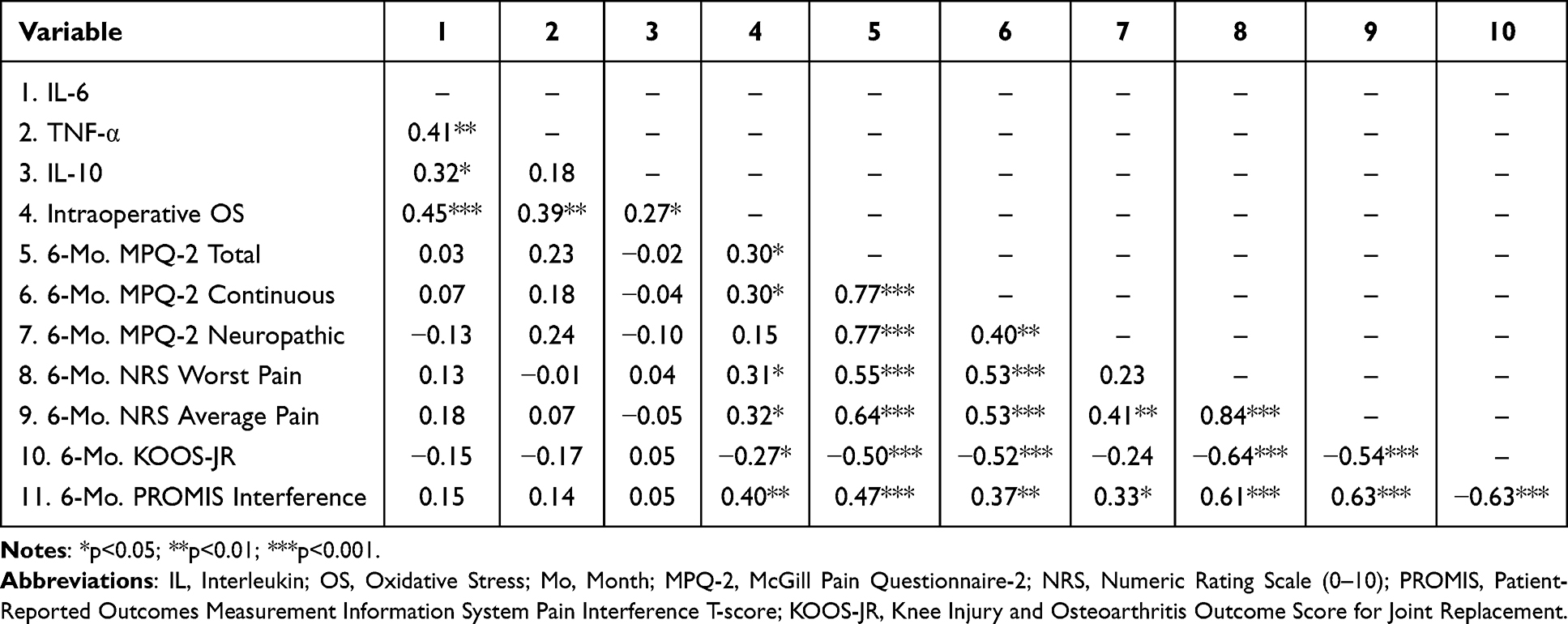 |
Table 2 Spearman Correlations Among Cytokine, OS, and 6-month Follow-up Pain Outcomes |
Primary Analysis: Cytokine Moderation of the Relationship Between OS and Pain-Related Outcomes
We identified three significant interactions between baseline cytokines and intraoperative combined OS in predicting 6-month pain outcomes. Detailed results of these significant moderation analyses are presented in Table 3. A significant interaction was found between baseline IL-6 and intraoperative OS in predicting 6-month NRS average pain intensity (β = 0.53, 95% CI [0.04, 1.02], p = 0.036, f2 = 0.095; Model R2 = 0.358), explaining an additional 6.8% of variance in the long-term pain outcome. Similarly, a significant interaction was found between baseline TNF-α and OS in predicting 6-month MPQ-2 Neuropathic pain intensity (β = 0.46, 95% CI [0.10, 0.82], p = 0.013, f2 = 0.138; Model R2 = 0.380), explaining an additional 6.7% of variance in this outcome. Finally, a significant interaction was found between baseline IL-10 and OS in predicting 6-month MPQ-2 Neuropathic pain intensity (β = 0.44, 95% CI [0.06, 0.82], p = 0.025, f2 = 0.112; Model R2 = 0.370), explaining an additional 7.1% of variance in long-term neuropathic pain features.
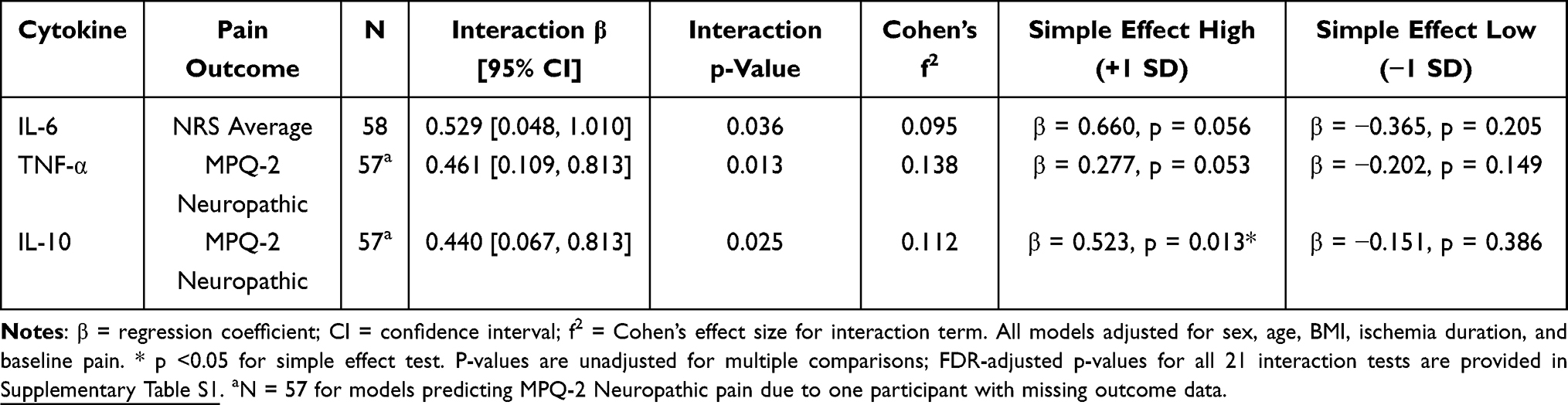 |
Table 3 Summary of Significant Moderation Analyses Testing Cytokine X Intraoperative Oxidative Stress Interactions on 6-Month Pain Outcomes |
Probing Significant Interactions: Simple Effects Tests
Simple effects tests were conducted to decompose the three significant interactions described above (see Figure 1). For IL-6 and NRS Average Pain, the analysis revealed a positive relationship approaching significance between OS and average pain intensity at high IL-6 levels (+1 SD) (β = 0.66, SE = 0.34, 95% CI [0.00, 1.32], p = 0.056). No relationship was observed at low IL-6 levels (−1 SD) (β = −0.37, SE = 0.29, 95% CI [−0.92, 0.19], p = 0.205).
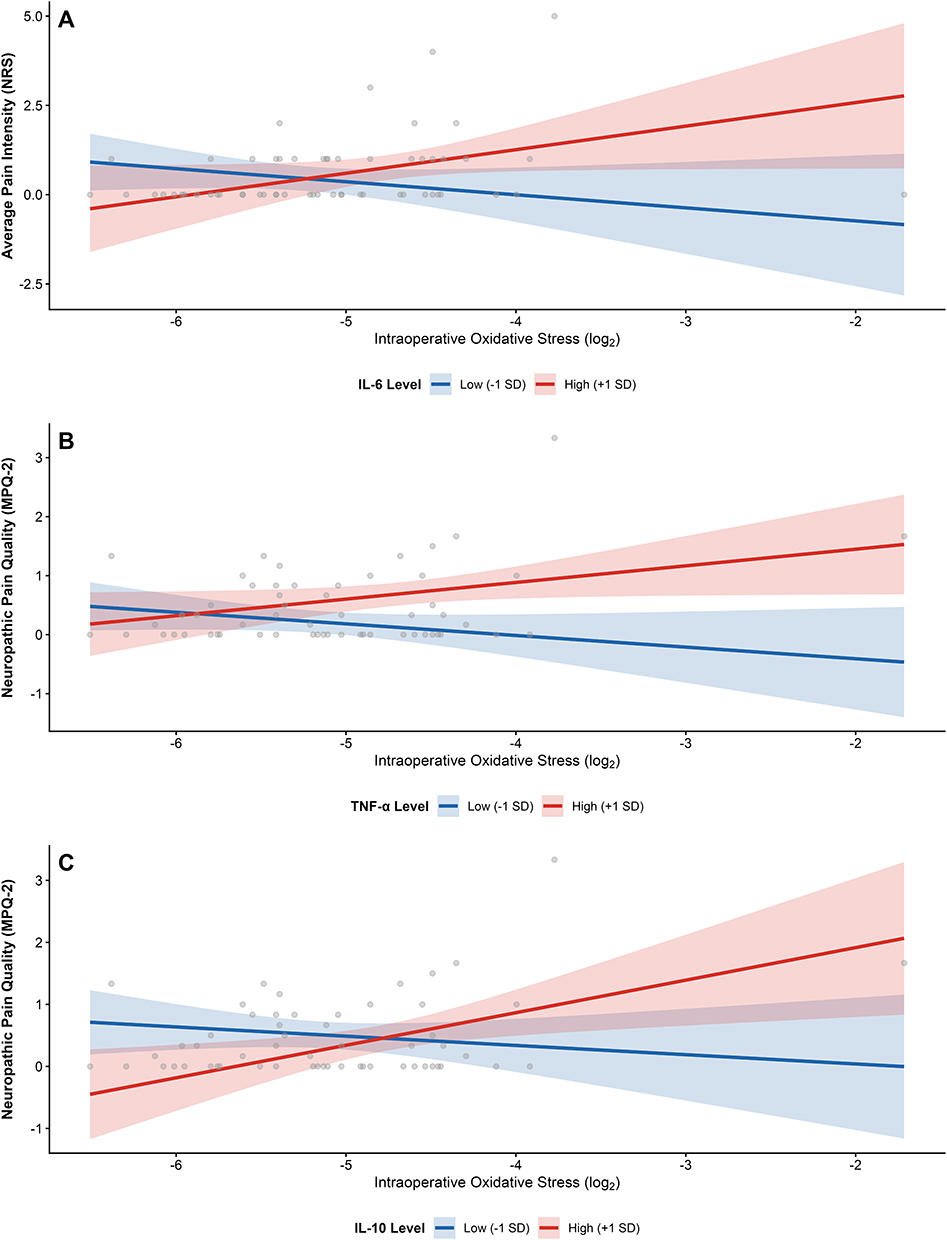 |
Figure 1 (A) Moderation by IL-6 on average pain intensity (NRS). At high IL-6 levels (+1 SD), a non-significant trend emerged for OS to predict pain (p = 0.056). N = 58. (B). Moderation by TNF-α on neuropathic pain quality (MPQ-2). At high TNF-α levels (+1 SD), a marginal trend was observed (p = 0.053). N = 57. (C). Moderation by IL-10 on neuropathic pain quality (MPQ-2). At high IL-10 levels (+1 SD), OS significantly predicted neuropathic pain (p = 0.013). N = 57. Abbreviations: OS, Oxidative Stress; NRS, Numeric Rating Scale; MPQ-2, McGill Pain Questionnaire-2. Notes: Simple slopes are estimated at ±1 SD from the mean of the pre-incision cytokine moderator, with all covariates held at their mean values. Shaded areas represent 95% confidence intervals. All models are adjusted for sex, age, BMI, ischemia duration, and baseline pain. |
For TNF-α and MPQ-2 Neuropathic Pain, a similar pattern emerged. At high TNF-α levels (+1 SD), there was a positive relationship approaching significance between OS and neuropathic pain (β = 0.28, SE = 0.14, 95% CI [0.00, 0.55], p = 0.053). No relationship was observed at low TNF-α levels (−1 SD) (β = −0.20, SE = 0.14, 95% CI [−0.47, 0.07], p = 0.149).
For IL-10 and MPQ-2 Neuropathic Pain, the simple effect at high IL-10 levels (+1 SD) revealed a statistically significant positive relationships between OS and intensity of neuropathic pain features (β = 0.52, SE = 0.20, 95% CI [0.13, 0.92], p = 0.013). In contrast, no relationship was observed at low IL-10 levels (−1 SD) (β = −0.15, SE = 0.17, 95% CI [−0.49, 0.19], p = 0.386).
In all three significant interactions, the conditional slope of OS on pain was positive (or approaching significance) at high cytokine levels, with no significant relationship observed at low cytokine levels.
Exploratory Findings: Interactions Approaching Significance and Main Effects
In exploratory analyses, three additional interactions involving baseline IL-6 and intraoperative OS approached statistical significance. These included moderation effects on MPQ-2 Total (β = 0.30, 95% CI [−0.05, 0.64], p = 0.093), MPQ-2 Continuous (β = 0.40, 95% CI [−0.05, 0.84], p = 0.083), and PROMIS Pain Interference (β = 3.13, 95% CI [−0.19, 6.44], p = 0.059). Simple effects tests for all three interactions that approached significance revealed a pattern consistent with the significant findings described above: a positive but non-significant association between OS and pain at high IL-6 levels (β range: 0.40–4.45, p-values 0.058 to 0.102), with no association at low IL-6 levels (all p > 0.35).
Finally, models with non-significant interactions were examined for independent main effects. In models where TNF-α did not significantly interact with OS, higher baseline TNF-α emerged as a significant independent predictor of more severe 6-month pain, even after controlling for OS and all covariates. Significant main effects for TNF-α were found for MPQ-2 Total (β = 0.65, 95% CI [0.32, 0.99], p < 0.001), NRS Average Pain (β = 0.89, 95% CI [0.41, 1.36], p = 0.001), and MPQ-2 Continuous (β = 0.87, 95% CI [0.44, 1.29], p < 0.001). All reflected positive associations between TNF-α and long-term post-TKA pain outcomes. No other significant main effects were observed for IL-6, IL-10, or intraoperative OS in models without significant interactions.
Discussion
We found that intraoperative OS was positively correlated with baseline inflammatory cytokines, and more importantly, that cytokines moderated the effect of OS on six-month post-TKA pain outcomes. These interaction effects were statistically significant for the NRS average pain intensity outcome (baseline IL-6) and for MPQ-2 neuropathic pain intensity (baseline TNF-α and IL-10 levels). Simple effects analyses indicated significant conditional effects consistent with a two-hit pattern, as individuals with both higher intraoperative OS and higher inflammatory cytokine levels exhibited the worst pain outcomes. This study adds a new dimension to our prior findings showing that elevated intraoperative OS is linked to risk for chronic pain following TKA.23
In addition to the observed interaction effects, baseline TNF-α demonstrated notable main effects in adjusted regression models, with higher TNF-α levels associated with greater pain intensity across several outcomes at six months following TKA. While these associations were among the stronger effects observed in adjusted models (p <0.001 across multiple outcomes), they were less apparent in unadjusted bivariate correlations (Table 2), suggesting that the relationship between TNF-α and chronic pain may be partially confounded by demographic and clinical factors controlled for in the regression models. These adjusted findings are consistent with prior mechanistic evidence that TNF-α is an upstream pro-inflammatory mediator40 with direct effects on nociceptor excitability26 and sensitization.
The observed interactions involving IL-6 and TNF-α are consistent with our hypotheses based on prior literature implicating pro-inflammatory cytokines in oxidative stress–driven neuroinflammatory cascades and risk for chronic pain. Preclinical animal and in vitro studies demonstrate that OS activates NF-κB28 and MAPK29 signaling pathways, promoting production of cytokines such as IL-6 and TNF-α.29,30 This inflammatory signaling can then further amplify OS, creating a feed-forward loop that sustains nociceptive sensitization.31 Our findings are encouraging for extending this mechanistic framework to a human surgical population, suggesting a plausible and biologically intuitive “double-hit” model in which inflammation and OS may collectively contribute to risk for chronic pain post-TKA.
The IL-10 findings are particularly interesting because the pattern of associations differed from that observed for IL-6 and TNF-α. In bivariate analyses, IL-10 was positively correlated with IL-6 and intraoperative OS, but its associations with six-month pain outcomes were weak, non-significant, and directionally mixed rather than uniformly positive. As noted above, although prior literature suggests a protective effect of IL-10 levels on pain outcomes.,6,16–18 it is also pleiotropic and may increase as part of a compensatory or homeostatic response to heightened inflammatory burden.19 In the present study, pre-incision IL-10 significantly moderated the association between intraoperative OS and MPQ-2 Neuropathic pain intensity, such that higher OS was associated with greater neuropathic pain features among participants with higher IL-10 levels. We speculate that rather than suggesting a directly pronociceptive effect of IL-10, this pattern may indicate that elevated IL-10 identifies patients with a more activated immune-regulatory state in whom intraoperative OS has greater relevance for later neuropathic pain features. We acknowledge alternative explanations, including residual confounding, correlation with unmeasured inflammatory burden, assay variability, and chance given the exploratory nature of the study. Future studies with larger samples and longitudinal cytokine assessment will be needed to clarify whether IL-10 functions primarily as a compensatory marker of inflammatory burden or has a more complex regulatory role in OS-related postoperative pain vulnerability.
A key strength of this study is the rigorous and state of the art assessment of OS. OS reflects an imbalance between the generation and elimination of reactive oxygen species (ROS), arising from excess ROS production or insufficient antioxidant defenses.41 ROS induce chemical oxidation of proteins, DNA, and lipids, leading to structural changes that alter cellular function and promote inflammation, fibrosis, and apoptosis—processes that can directly contribute to patient morbidity.42–44 The present study employed circulating F2-isoprostanes (IsoP) and isofurans (IsoF), which are widely regarded as the most sensitive and specific indices of systemic OS in vivo.20,25 IsoP and IsoF are stable end products of non-enzymatic arachidonic acid peroxidation that share a common lipid radical intermediate, with IsoF being preferentially generated under higher oxygen conditions.45 Our combined OS measure that examines the mean of IsoP and IsoF measures provides a robust index of systemic OS that is less confounded by perioperative variations in oxygen delivery.35 This combined OS measure has been associated with multiple clinically meaningful postoperative morbidities and organ injuries,35,46 strengthening confidence that the OS signal captured in this study reflects biologically-relevant processes rather than measurement artifact.
Although exploratory and requiring replication, these findings address the substantial unmet clinical need for reducing chronic pain risk following TKA. Extrapolating current incidence estimates suggests that approximately 150,000 patients undergoing TKA in the United States each year may experience chronic post-TKA pain, and in the current cohort, 22% of patients experienced clinically meaningful postoperative pain at six months.23 Post-operative pain trajectories predict risk for readmissions and emergency room visits.47 Meanwhile, patients undergoing TKAs are typically older adults, in whom pain management can be challenging, given the higher likelihood for comorbidities and polypharmacy. Despite this clinical and economic burden, there are currently no proven clinical interventions to reliably reduce CPSP risk following TKA. In this context, our results highlight preoperative OS and inflammatory burden as potential mechanistic targets for future investigation, and motivate future studies examining the potential impact of mechanism-based perioperative interventions on pain and functional outcomes. More broadly, this work highlights the future role of precision-medicine frameworks that use biomarkers to stratify risk and inform tailored, preventative perioperative strategies to reduce risk for the most vulnerable patients.
Several limitations should be considered when interpreting these findings. First, the modest sample size and exploratory nature of the analysis underscore the need for replication in larger cohorts; findings should therefore be interpreted as hypothesis-generating rather than confirmatory. Because cytokine assays were added after study initiation, only a subset of the original cohort had complete cytokine data available for the present analyses, which may have introduced selection bias. Post hoc power analyses indicated 59–74% power to detect the observed interaction effect sizes, suggesting that the study may have been underpowered for detecting small-to-moderate interaction effects, although it retained sufficient power to detect some cytokine × oxidative stress effects. Finally, given the number of interaction tests conducted across cytokine–outcome combinations, no individual interaction survived Benjamini-Hochberg FDR correction (Supplementary Table S1). Findings should therefore be interpreted cautiously as hypothesis-generating, with emphasis placed on effect sizes and the consistency of patterns across outcomes rather than on individual p-values. Covariate selection was based on the parent study to maintain consistency and avoid overfitting given the sample size; additional confounders such as preoperative opioid use, comorbidity burden, psychological factors, and anti-inflammatory medication use were not included and may have influenced the observed associations. Additionally, the ratio of predictors to observations (approximately 7:1) raises the possibility of overfitting, though the a priori selection of covariates and consistency of findings across cytokine moderators partially mitigate this concern.
Second, this study was restricted to patients undergoing TKA for osteoarthritis, which may limit generalizability to other surgical populations, procedures with different inflammatory or ischemic profiles, or patients with non-osteoarthritic pain conditions. The sample was also predominantly White and non-Hispanic and exclusively age 55 years or older, precluding evaluation of racial, ethnic and age-related differences in inflammatory or OS pathways that may influence postoperative pain vulnerability. Finally, intraoperative OS was assessed at multiple intraoperative time points and combined into a single composite measure, whereas inflammatory cytokines were analyzed only at baseline; as a result, these analyses do not provide insight into longitudinal postoperative changes in cytokine levels or their impact on chronic pain risk.
In summary, these findings suggest that interactions between intraoperative OS and baseline inflammatory biology may contribute to heterogeneity in long-term pain outcomes following TKA. By emphasizing biological context rather than uniform risk, this work is consistent with a precision-medicine approach to understanding post-TKA chronic pain risk and management. Our results motivate future studies aimed at developing and testing mechanism-based, individually tailored interventions—such as strategies targeting inflammatory and OS pathways—to possibly prevent poor postoperative pain outcomes and to prevent avoidable healthcare utilization following TKA.
Acknowledgments
An unauthorized English version of the MMSE was used by the study team without permission, however this has now been rectified with PAR. The MMSE is a copyrighted instrument and may not be used or reproduced in whole or in part, in any form or language, or by any means without written permission of PAR (https://www.parinc.com).
Funding
This work was supported in part by K23MD019351 (FR), RF1AG085287 (SB), and R01AG048915 (SB).
Disclosure
Outside of the scope of this project: Gregory G. Polkowski reports personal fees from Enovis. Stephen Bruehl reports personal fees from Akigai and Ambros Therapeutics. J Ryan Martin reports personal fees from Depuy, enovis and Restor3d. The authors report no other conflicts of interest in this work.
References
1. Jones CM, Potluri AS, Federico VP, et al. Trends in Medicare Arthroplasty Procedure Volume: projecting From 2025 to 2040. J Arthroplasty. 2025;40(11):2781–12. doi:10.1016/j.arth.2025.05.124
2. Beswick AD, Wylde V, Gooberman-Hill R, Blom A, Dieppe P. What proportion of patients report long-term pain after total Hip or knee replacement for osteoarthritis? A systematic review of prospective studies in unselected patients. BMJ open. 2012;2(1):e000435. doi:10.1136/bmjopen-2011-000435
3. Wylde V, Hewlett S, Learmonth ID, Dieppe P. Persistent pain after joint replacement: prevalence, sensory qualities, and postoperative determinants. Pain®. 2011;152(3):566–572. doi:10.1016/j.pain.2010.11.023
4. Aveline C, Le Roux A, Le Hetet H, et al. Pain and recovery after total knee arthroplasty: a 12-month follow-up after a prospective randomized study evaluating Nefopam and Ketamine for early rehabilitation. The Clinical Journal of Pain. 2014;30(9):749–754. doi:10.1097/AJP.0000000000000033
5. Larach DB, Kertai MD, Billings IVFT, et al. Preoperative Predictors of Prolonged Opioid Use in the 6 Months After Total Knee Arthroplasty. The Clinical Journal of Pain. 2023;39(10):516–523. doi:10.1097/AJP.0000000000001143
6. Vanderwall AG, Milligan ED. Cytokines in Pain: harnessing Endogenous Anti-Inflammatory Signaling for Improved Pain Management. Front Immunol. 2019;10:3009. doi:10.3389/fimmu.2019.03009
7. Ji RR, Chamessian A, Zhang YQ. Pain regulation by non-neuronal cells and inflammation. Science. 2016;354(6312):572–577. doi:10.1126/science.aaf8924
8. Clark AK, Old EA, Malcangio M. Neuropathic pain and cytokines: current perspectives. J Pain Res. 2013;6:803–814. doi:10.2147/JPR.S53660
9. Watkins LR, Milligan ED, Maier SF. Glial activation: a driving force for pathological pain. Trends Neurosci. 2001;24(8):450–455. doi:10.1016/s0166-2236(00)01854-3
10. Zhang S, Ning Y, Yang Y, et al. Decoding pain chronification: mechanisms of the acute-to-chronic transition. Front Mol Neurosci. 2025;18:1596367. doi:10.3389/fnmol.2025.1596367
11. Bruehl S, Billings FT, Anderson S, et al. Preoperative Predictors of Complex Regional Pain Syndrome Outcomes in the 6 Months Following Total Knee Arthroplasty. J Pain. 2022;23(10):1712–1723. doi:10.1016/j.jpain.2022.04.005
12. Tchetina EV, Glemba KE, Markova GA, et al. Development of Postoperative Pain in Patients with End-Stage Knee Osteoarthritis Is Associated with Upregulation of Genes Related to Extracellular Matrix Degradation, Inflammation, and Apoptosis Measured in the Peripheral Blood before Knee Surgery. Life (Basel). 2020;10(10):224. doi:10.3390/life10100224
13. Chidambaran V, Duan Q, Pilipenko V, et al. The role of cytokines in acute and chronic postsurgical pain after major musculoskeletal surgeries in a quaternary pediatric center. Brain Behav Immun. 2024;122:596–603. doi:10.1016/j.bbi.2024.08.056
14. Fiorentino DF, Zlotnik A, Mosmann TR, Howard M, O’Garra A. IL-10 inhibits cytokine production by activated macrophages. J Immunol. 1991;147(11):3815–3822. doi:10.4049/jimmunol.147.11.3815
15. Chernoff AE, Granowitz EV, Shapiro L, et al. A randomized, controlled trial of IL-10 in humans. Inhibition of inflammatory cytokine production and immune responses. J Immunol. 1995;154(10):5492–5499. doi:10.4049/jimmunol.154.10.5492
16. Porro C, Cianciulli A, Panaro MA. The Regulatory Role of IL-10 in Neurodegenerative Diseases. Biomolecules. 2020;10(7):1017. doi:10.3390/biom10071017
17. Uceyler N, Valenza R, Stock M, Schedel R, Sprotte G, Sommer C. Reduced levels of antiinflammatory cytokines in patients with chronic widespread pain. Arthritis Rheum. 2006;54(8):2656–2664. doi:10.1002/art.22026
18. Sideris A, Malahias MA, Birch G, et al. Identification of biological risk factors for persistent postoperative pain after total knee arthroplasty. Reg Anesth Pain Med. 2022;47(3):161–166. doi:10.1136/rapm-2021-102953
19. Carlini V, Noonan DM, Abdalalem E, et al. The multifaceted nature of IL-10: regulation, role in immunological homeostasis and its relevance to cancer, COVID-19 and post-COVID conditions. Front Immunol. 2023;14:1161067. doi:10.3389/fimmu.2023.1161067
20. Milne GL, Musiek ES, Morrow JD. F2-isoprostanes as markers of oxidative stress in vivo: an overview. Biomarkers. 2005;10(sup1):10–23. doi:10.1080/13547500500216546
21. Stevens JL, Feelisch M, Martin DS. Perioperative Oxidative Stress: the Unseen Enemy. Anesth Analg. 2019;129(6):1749–1760. doi:10.1213/ANE.0000000000004455
22. Bruehl S, Milne G, Polkowski G, et al. Oxidative stress mediates associations between preoperative psychosocial phenotype and pain-related outcomes at 6 months following total knee arthroplasty: a longitudinal cohort study. Pain Med. 2024;25(1):71–77. doi:10.1093/pm/pnad120
23. Bruehl S, Milne G, Schildcrout J, et al. Perioperative oxidative stress predicts subsequent pain-related outcomes in the 6 months after total knee arthroplasty. Pain. 2023;164(1):111–118. doi:10.1097/j.pain.0000000000002670
24. Vecchiet J, Cipollone F, Falasca K, et al. Relationship between musculoskeletal symptoms and blood markers of oxidative stress in patients with chronic fatigue syndrome. Neurosci Lett. 2003;335(3):151–154. doi:10.1016/s0304-3940(02)01058-3
25. Kadiiska M, Gladen B, Baird D, et al. Biomarkers of oxidative stress study II: are oxidation products of lipids, proteins, and DNA markers of CCl4 poisoning? Free Radical Biology and Medicine. 2005;38(6):698–710. doi:10.1016/j.freeradbiomed.2004.09.017
26. Evans AR, Junger H, Southall MD, et al. Isoprostanes, novel eicosanoids that produce nociception and sensitize rat sensory neurons. J Pharmacol Exp Ther. 2000;293(3):912–920. doi:10.1016/S0022-3565(24)39314-0
27. Taylor-Clark TE, Undem BJ, Macglashan Jr DW, Ghatta S, Carr MJ, McAlexander MA. Prostaglandin-induced activation of nociceptive neurons via direct interaction with transient receptor potential A1 (TRPA1). Mol Pharmacol. 2008;73(2):274–281. doi:10.1124/mol.107.040832
28. Morgan MJ, Liu ZG. Crosstalk of reactive oxygen species and NF-kappaB signaling. Cell Res. 2011;21(1):103–115. doi:10.1038/cr.2010.178
29. Liu Z, Yao X, Jiang W, et al. Advanced oxidation protein products induce microglia-mediated neuroinflammation via MAPKs-NF-kappaB signaling pathway and pyroptosis after secondary spinal cord injury. J Neuroinflammation. 2020;17(1):90. doi:10.1186/s12974-020-01751-2
30. Aoki Y, Dai H, Furuta F, et al. LOX-1 mediates inflammatory activation of microglial cells through the p38-MAPK/NF-kappaB pathways under hypoxic-ischemic conditions. Cell Commun Signal. 2023;21(1):126. doi:10.1186/s12964-023-01048-w
31. Michalak KP, Michalak AZ. Understanding chronic inflammation: couplings between cytokines, ROS, NO, Ca(i) (2+), HIF-1alpha, Nrf2 and autophagy. Front Immunol. 2025;16:1558263. doi:10.3389/fimmu.2025.1558263
32. Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189–198. doi:10.1016/0022-3956(75)90026-6
33. Milne GL, Gao B, Terry ES, Zackert WE, Sanchez SC. Measurement of F2- isoprostanes and isofurans using gas chromatography-mass spectrometry. Free Radic Biol Med. 2013;59:36–44. doi:10.1016/j.freeradbiomed.2012.09.030
34. Bruehl S, Milne G, Schildcrout J, et al. Oxidative stress is associated with characteristic features of the dysfunctional chronic pain phenotype. Pain. 2022;163(4):786–794. doi:10.1097/j.pain.0000000000002429
35. Lopez MG, Hughes CG, DeMatteo A, et al. Intraoperative Oxidative Damage and Delirium after Cardiac Surgery. Anesthesiology. 2020;132(3):551–561. doi:10.1097/ALN.0000000000003016
36. Jensen MP, Turner JA, Romano JM, Fisher LD. Comparative reliability and validity of chronic pain intensity measures. Pain. 1999;83(2):157–162. doi:10.1016/s0304-3959(99)00101-3
37. Dworkin RH, Turk DC, Revicki DA, et al. Development and initial validation of an expanded and revised version of the Short-form McGill Pain Questionnaire (SF-MPQ-2). Pain. 2009;144(1–2):35–42. doi:10.1016/j.pain.2009.02.007
38. Amtmann D, Cook KF, Jensen MP, et al. Development of a PROMIS item bank to measure pain interference. Pain. 2010;150(1):173–182. doi:10.1016/j.pain.2010.04.025
39. Lyman S, Lee YY, Franklin PD, Li W, Cross MB, Padgett DE. Validation of the KOOS, JR: a Short-form Knee Arthroplasty Outcomes Survey. Clin Orthop Relat Res. 2016;474(6):1461–1471. doi:10.1007/s11999-016-4719-1
40. Leung L, Cahill CM. TNF-alpha and neuropathic pain--a review. J Neuroinflammation. 2010;7(1):27. doi:10.1186/1742-2094-7-27
41. Jomova K, Raptova R, Alomar SY, et al. Reactive oxygen species, toxicity, oxidative stress, and antioxidants: chronic diseases and aging. Arch Toxicol. 2023;97(10):2499–2574. doi:10.1007/s00204-023-03562-9
42. Basu S. Bioactive eicosanoids: role of prostaglandin F(2alpha) and F(2)-isoprostanes in inflammation and oxidative stress related pathology. Mol Cells. 2010;30(5):383–391. doi:10.1007/s10059-010-0157-1
43. Sakamoto H, Corcoran TB, Laffey JG, Shorten GD. Isoprostanes--markers of ischaemia reperfusion injury. Eur J Anaesthesiol. 2002;19(8):550–559. doi:10.1017/s0265021502000893
44. Wang CH, Wu SB, Wu YT, Wei YH. Oxidative stress response elicited by mitochondrial dysfunction: implication in the pathophysiology of aging. Exp Biol Med (Maywood). 2013;238(5):450–460. doi:10.1177/1535370213493069
45. Fessel JP, Porter NA, Moore KP, Sheller JR, Roberts II LJ. Discovery of lipid peroxidation products formed in vivo with a substituted tetrahydrofuran ring (isofurans) that are favored by increased oxygen tension. Proc Natl Acad Sci U S A. 2002;99(26):16713–16718. doi:10.1073/pnas.252649099
46. Billings FT, Pretorius M, Schildcrout JS, et al. Obesity and oxidative stress predict AKI after cardiac surgery. J Am Soc Nephrol. 2012;23(7):1221–1228. doi:10.1681/ASN.2011090940
47. Hernandez-Boussard T, Graham LA, Desai K, et al. The Fifth Vital Sign: postoperative Pain Predicts 30-day Readmissions and Subsequent Emergency Department Visits. Ann Surg. 2017;266(3):516–524. doi:10.1097/SLA.0000000000002372
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Platelet-Activating Factor Promotes the Development of Non-Alcoholic Fatty Liver Disease
Yin H, Shi A, Wu J
Diabetes, Metabolic Syndrome and Obesity 2022, 15:2003-2030
Published Date: 8 July 2022
The Effects and Pathogenesis of PM2.5 and Its Components on Chronic Obstructive Pulmonary Disease

Wang Q, Liu S
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:493-506
Published Date: 6 April 2023
Quercetin: A Flavonoid with Potential for Treating Acute Lung Injury

Huang M, Liu X, Ren Y, Huang Q, Shi Y, Yuan P, Chen M
Drug Design, Development and Therapy 2024, 18:5709-5728
Published Date: 6 December 2024
Exercise Prescription Training in Chronic Obstructive Pulmonary Disease: Benefits and Mechanisms
Liu S, Yang A, Yu Y, Xu B, Yu G, Wang H
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:1071-1082
Published Date: 15 April 2025
Klotho Protein: A Multifaceted Guardian of Healthy Aging and Its Therapeutic Potential
Shen J, Bin W, Lin X, Lai Y, Lin X, Guan T, Liu H
International Journal of Nanomedicine 2025, 20:7251-7270
Published Date: 9 June 2025