")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Anxiety and Depression in Family Members of Critically Ill Covid-19 Inpatients: Brief Psychological Interventions via Telephone, an Exploratory Study
Authors Caballero-Suárez NP, Barrientos-Casarrubias V, Gutiérrez-Velilla E, González Avilés LM, Pérez-López LD, Alvarado-De la Barrera C, Ávila-Ríos S, Mora-Gallegos J
Received 9 August 2023
Accepted for publication 18 October 2023
Published 7 November 2023 Volume 2023:16 Pages 3319—3331
DOI https://doi.org/10.2147/JMDH.S434448
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Nancy Patricia Caballero-Suárez,1 Vania Barrientos-Casarrubias,1 Ester Gutiérrez-Velilla,1 Lilian Margarita González Avilés,2 Luis Daniel Pérez-López,1,2 Claudia Alvarado-De la Barrera,1 Santiago Ávila-Ríos,1 Janella Mora-Gallegos3
1Centro de Investigación en Enfermedades Infecciosas (CIENI), Instituto Nacional de Enfermedades Respiratorias “Ismael Cosío Villegas” (INER), Mexico City, Mexico; 2Programa de Maestría en Psicología, Universidad Nacional Autónoma de México (UNAM), Mexico City, Mexico; 3Programa de Atención a Pacientes y Familiares (PAPyF), Instituto Nacional de Enfermedades Respiratorias “Ismael Cosío Villegas” (INER), Mexico City, Mexico
Correspondence: Nancy Patricia Caballero-Suárez, Departamento de Investigación en Enfermedades Infecciosas (CIENI), Instituto Nacional de Enfermedades Respiratorias (INER), Calzada de Tlalpan 4502, Sección XVI, Tlalpan, Mexico City, 14080, Mexico, Tel +52 155 56667985 ext. 169, Email [email protected]
Purpose: This study aimed to assess the level of anxiety and depression in relatives of critically ill COVID-19 patients admitted to the intensive care unit (ICU), and to perform an exploratory pilot study on the implementation of telephone psychological interventions to reduce the initial levels of anxiety and depression in this population.
Patients and Methods: Family members of COVID-19 inpatients at ICU answered GAD-7, PHQ-9 and questions on socio-demographic data. A brief psychological intervention was applied via telephone based on the needs of the participants (with adequate adaptation, with symptoms of anxiety, depression, or both). After intervention, participants completed the Patient Global Impression of Change Scale.
Results: A total of 1307 relatives were included (66.5% female), 34% and 29% had anxiety and depressive symptoms, respectively. These symptoms were associated with female gender, unemployment, and being the parent or partner of the patient. After intervention, 57.9% reported felt better, 31.3% a little better and 6.6% much better; and with emotional regulation techniques and psychoeducation, higher percentages of feeling better or much better were reported.
Conclusion: Brief interventions to reduce the psychological impact of inpatient family members could be effective but will need to be explored further in future studies.
Keywords: pandemic, relatives, mental health, brief psychotherapy
A Letter to the Editor has been published for this article.
A Response to Letter by Dr Syaekhu has been published for this article.
Introduction
Family members of patients hospitalized in intensive care units (ICU) are prone to develop adverse psychological outcomes such as anxiety, acute stress disorder, post-traumatic stress, depression, reduced quality of life, and complicated grief.1–3 During the first and second waves of the coronavirus disease pandemic (COVID-19) in the United States, respectively, 18% and 10% of patients required invasive mechanical ventilation, and in the case of Mexico, this occurred in up to one-third of the patients,4 a condition that has been associated with more than 82% mortality.5,6 There was also an important role for the media in the generation of fear and the experience of community fear.7,8 For these reasons, mental health manifestations could have been even more severe in family member of COVID-19 patients, also due to the highly invasive procedures applied, the visiting restrictions, and the high mortality that occurred at the beginning of the pandemic, which involved a profound impact on the quality of life of patients’ families.9,10
Evidence from studies with general patients hospitalized in ICU from different countries suggest that possible determinants of mental health impairment in family members include fear of losing their loved ones, deterioration of the family structure, concerns about the future, coping with the hospital environment,11 and uncertainty about their patient’s acute condition and prognosis.12 In this regard, it has been found percentages of 40%–70% of anxiety symptoms, 22% of depression symptoms, and over 60% of post-traumatic stress symptoms in family members of critically ill patients. Factors associated with increased anxiety symptoms in this population included being female, being the spouse of the patient, the unpredictability of admission to ICU, a lower education status, poor sleep pattern, and fatigue. In addition, the patient’s death has been associated with higher levels of depression and post-traumatic stress.13,14
Specifically, caregivers of critically ill COVID-19 patients have not been as extensively studied, but it has been reported that between 40% and 60% of the caregivers of COVID-19 patients present depressive symptoms, with a four-times higher risk in females,15 and these were accompanied by problems at the workplace.16 These percentages were higher than those found in the general population during the pandemic, where 20.8% had anxiety and 27.5% had depression symptoms.17 In addition, greater post-traumatic stress, depression, and anxiety symptoms have been reported in family members of COVID-19 patients than in relatives of other respiratory diseases.18 If these mentioned difficulties are not adequately addressed in patient’s caregivers, it could lead to the development of the so-called Post-Intensive Care Syndrome-Family,19 which includes the presence of post-traumatic stress, anxiety, depression, and non-specific emotional discomfort. This may be present even 4 years after ICU discharge, and its psychological repercussions can affect the family member’s ability to engage in necessary care-giving functions after hospitalization.1,20
Therefore, it is key to provide adequate follow-up and mental health interventions in hospitalized patients to prevent the development of psychological complications in them and their relatives.1 Even so, there have been a limited number of studies on psychological interventions to family members of patients currently hospitalized in ICU, and results have been inconclusive.21–26 Some findings indicate that providing timely information about health status and prognosis of patients to family members helps to reduce their anxiety,13,27 as well as providing brief and effective psychological interventions.23 For example, cognitive-behavioral therapy has been shown to be effective as first-line nonpharmacologic treatment for many psychological symptoms and psychiatric disorders.28,29 This is a brief therapy that has been successfully delivered even by mobile technology, including to individuals with critical illness and their family members,29–31 so these interventions have been proposed as an option to address the psychological needs of relatives of patients in the ICU.23
However, to our knowledge, the efficacy of this psychological interventions has not been evaluated in relatives of critically ill COVID-19 patients, who can suffer very stressful effects.18 In this sense, it can be very useful to evaluate and address family members of patients, especially in emergency contexts such as the COVID-19 pandemic, as this can have implications for their physical and mental health, and for the health and progression of the hospitalized family member. Interventions that can be used in this context should be brief and adaptable to the conditions of intensive care units in low-resource settings. Therefore, the objective of this study was to identify the levels of anxiety and depression in relatives receiving the daily medical report of critically ill COVID-19 inpatients admitted to ICU, to evaluate its association with sociodemographic variables, and to perform an exploratory pilot study on the implementation of psychological interventions provided via telephone to reduce the initial levels of anxiety and depression in this population.
Materials and Methods
Participants
This cross-sectional exploratory study was performed at a National Institute in Mexico City, the largest third-level national referral center for COVID-19. From early March 2020, the institution was gradually repurposed for the treatment of patients with COVID-19 exclusively. The study participants were family members of critically ill COVID-19 patients admitted to critical care areas. Since we were interested in having as heterogeneous and representative a sample as possible, we considered all individuals aged 16 years or older, who were family members of a critically ill COVID-19 patient and who were responsible for receiving the daily medical report. Relatives who did not give their informed consent for the evaluation and/or psychological intervention, or those who did not complete the evaluation were excluded from this study. All eligible family members were invited to participate. Given the restrictions imposed by the SARS-COV-2 pandemic, participants were contacted by telephone. On the phone call, verbal informed consent for answering the psychological assessment was obtained, and psychological intervention was provided. The data collection was carried out from June 2020 to March 2021, during the first and second COVID-19 waves in Mexico.
Measurements
We obtained information about sex and age from the clinical records of the patients. We also obtained sociodemographic data of family members on the psychological assessment phone call. This information included gender, age, occupation, place of residence, and relationship with the patients.
Anxiety symptoms of relatives were assessed with the culturally adapted Spanish version of the GAD-7.32 This instrument was selected as it is a widely used tool, self-applicable and brief, which contains 7 items based on the diagnostic criteria of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) for detection of generalized anxiety and other anxiety disorders.33 This tool provides information about the level of anxiety and recommended interventions. Answers ranged from “0” (not at all) to “3” (nearly every day). Scale scores ranged from 0 to 21 and cut-off scores were defined as 0–4 (no anxiety symptoms); 5–9 (mild anxiety symptoms); 10–14 (moderate anxiety symptoms); and 15–21 (severe anxiety symptoms). The internal consistency of this instrument in Mexican population has been reported to be adequate (Cronbach’s alpha =0.82).
Depression symptoms of relatives were assessed by using the culturally adapted Spanish version of the PHQ-9.34,35 As GAD-7, this is a self-applicable scale including 9 items based on the diagnostic criteria of the DSM-IV of the depressive disorder.36 Answers ranged from “0” (not at all) to “3” (nearly every day). Scale scores ranged from 0 to 27. Cut-off scores were defined as 0–4 (no depression symptoms); 5–9 (mild depression symptoms); 10–14 (moderate depression symptoms); 15–19 (moderately severe depression symptoms); and 20–27 (severe depression symptoms). The internal consistency of the PHQ-9 in Mexican population was good (Cronbach’s alpha >0.80).
To measure the intervention in a simple and timely manner, it was considered to assess the perception of change/improvement at the end of the phone call through a single-item self-report that has shown adequate reliability indices, the Global Improvement rating of the Patient Global Impression of Change Scale.37 This single-item measure was first developed for use in psychopharmacology trials as part of the National Institute of Mental Health (NIMH) collaborative study of schizophrenia.37 Since then, it has been used as a standard primary outcome measure in studies investigating the efficacy of treatments for psychiatric conditions such as depression,38 social anxiety disorder,39 panic disorder,40 post-traumatic stress disorder,41 and binge-eating disorder.42 It is a 7-point verbal scale, with the options “very much improved”, “much improved”, “minimally improved”, “no change”, “minimally worsened”, “much worsened”, and “very much worsened”.
Intervention
To provide educational and psychological support to the families of hospitalized patients, as this has been shown to be effective in reducing distress and promoting coping,43 thirteen clinical psychologists with training in cognitive behavioral therapy provided brief psychology intervention by telephone after carrying out the evaluation through PHQ-9 and GAD-7 (see Figure 1). The interventions contained one or more of the strategies described below.
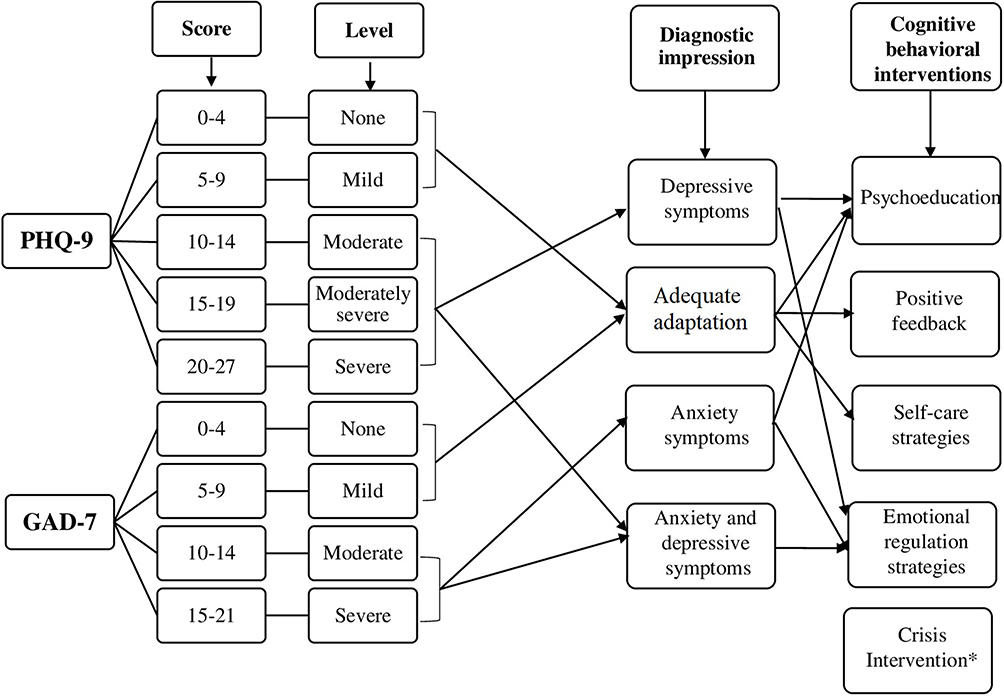 |
Figure 1 Impression Diagnostic Established According to Score and Level of Phq-9 and Gad-7, And Psychological Intervention Delivered According to diagnostic impression. *This intervention was implemented in critical situations related to the severity of the family member’s illness as well as the death of the patient with severe illness due to covid-19. |
1) Psychoeducation,44 in addition to providing the necessary information related to hospitalization process and the medical care, and additional information requested by relatives (clarified doubts), psychologists explained how the situation could cause psychological stress to family members of inpatients. Psychologists explained the conceptualization of the symptoms of anxiety and/or depression and confirmed that the information was understood. They also explained that misinformation is associated with increased emotional distress. Information was delivered to relatives who identified lack of knowledge about the hospital process or uncertainty and were detected to present or to be at risk of developing emotional symptoms.
2) Self-care strategies,45 aimed at reducing distress by promoting improved sleep patterns and health habits, training problem solving and fostering support networks. These strategies were given in cases in which the role of caregiver was identified as a burden, and individuals required self-care improvement habits (eg, eating, sleeping, and being supported by others when possible).
3) Positive feedback,46 aimed at reinforcement of adaptive coping strategies. Psychologists provided positive feedback when relatives made decisions that promoted physical and psychological self-care and when they had an active and functional coping style as a caregiver.
4) Emotional regulation strategies47 aimed at promoting emotional self-control through cognitive-behavioral exercises that promote calm states and attenuate dysfunctional emotional states. When psychologists identified dysfunctional thoughts of catastrophic and overgeneralization type, emotional regulation strategies were implemented. The exercises consisted of relaxation techniques (deep breathing or progressive muscle relaxation), cognitive restructuring (thought-stopping, gathering evidence, performing a cost–benefit analysis, and generating alternatives) or both.
5) Crisis intervention,48 aimed at containing intense emotional reactions to critical situations related to the severity of the health status as well as the death of the patient with severe illness due to COVID-19. Crisis intervention was the urgent and temporary care provided to individuals in order to interrupt their maladaptive behavior and return them to their usual level of pre-crisis functioning.
Procedure
Relatives were contacted via telephone by a clinical psychologist between 24h and 48h after they were transferred from the emergency room to ICU. Identification and contact data of relatives were retrieved from clinical records. The phone call lasted between 30 and 45 minutes and was structured in four segments: First, the psychologist explained that the objective of the call was to identify psychological needs of the relative and obtain the verbal consent to answer the assessment and psychometric tests. In the second segment, we applied the assessment on sociodemographic data, the General Anxiety Disorder Scale-7 (GAD-7),32 and the Patient Health Questionnaire-9 (PHQ-9).34,35 Psychologists gave feedback to the participants about their anxiety and depression scores. Based on participants answers and GAD-7/PHQ-9 scores, psychologists established a diagnostic impression with the following categories: adequate adaptation (absence of anxiety and depression symptoms or mild symptoms in GAD-7 and/or PHQ-9), anxiety symptoms (moderate or severe anxiety in GAD-7), depressive symptoms (moderate, moderately severe, or severe depression in PHQ-9), anxiety and depressive symptoms (moderate or severe anxiety and depression in GAD-7 and PHQ-9), see Figure 1. In the third segment of the phone call, relatives without clinical symptoms of anxiety and depression (adequate adaptation) mostly received psychoeducation, self-care strategies and/or positive feedback, aimed at validating the emotional reaction of adaptation and reinforcing self-care behaviors and active and functional coping styles. Participants with moderate or severe levels of anxiety or depression mostly received psychoeducation and emotional regulation techniques, aimed at promoting decrease of anxiety and depressive symptoms (see Figure 1). Participants in which there was a need for psychiatric assessment were referred to a specialist. In the fourth segment of the phone call, the relative’s perception of improvement after the intervention received was evaluated through the Patient Global Impression of Change Scale. The subjective perception of improvement after the brief-telephonic psychological intervention was assessed through Global Improvement rating of the Patient Global Impression of Change Scale.37
Data Analyses
Sociodemographic variables of patients and their relatives, as well as severity of depression and anxiety symptoms, were described using frequencies, percentages, means, and standard deviations (SD). With the information from the quartiles, age groups were established. We used chi-square test to explore possible associations of anxiety and depression levels with gender (male/female), age, occupation of relatives (unemployed, informal employed, formal employed, homemaker, student, or pensioner/retired) and kinship (mother/father; wife/husband; domestic partner; daughter/son; sister/brother; other). Values were considered significant if p<0.05. We also performed multiple logistic regression analysis with sociodemographic variables as predictors of absence/presence of anxiety and depression symptoms (absence = none or mild symptoms and presence = moderate or severe symptoms according to GAD-7 y PHQ-9). The type of psychological intervention received (psychoeducation, self-care strategies, positive feedback, emotional regulation strategies, or crisis intervention) and the perception of improvement (without changes, little better, better, or much better) were described with frequencies and percentages. The association between the different psychological interventions received and perception of improvement was done through the chi-square test.
Ethics Statement
Verbal informed consent was obtained from all participants included in the study. All procedures in studies involving human participants were performed in accordance with the ethical standards of the Research Ethics Committee of the Ismael Cosío Villegas National Institute of Respiratory Diseases, and the protocol research was approved with the number C34-21. The study was conducted in accordance with the guidelines of the Declaration of Helsinki.49
Results
Sociodemographic Characteristics
During the period between June 2020 and March 2021, 1929 patients were admitted at the INER, and we were able to contact 1371 relatives of critically ill COVID-19 patients. Of those, 1307 (95.3%) relatives accepted and completed data from the psychological evaluation and were included in this study. Most participants were female (66.5%, n=869) and the mean age was 42.3 years (SD=12.2). Most participants lived in Mexico City (61.1%, n=799) and were employed (54.0%, n=706). The most reported kinships were sons/daughters (48.3%, n=631), and partners of the patients (39.7%, n=519). Sociodemographic characteristics of the family members are shown in Table 1. Regarding sociodemographic characteristics of the patients, most of them were male (65.1%, n=851) with a mean age of 57.5 years (SD=13.6).
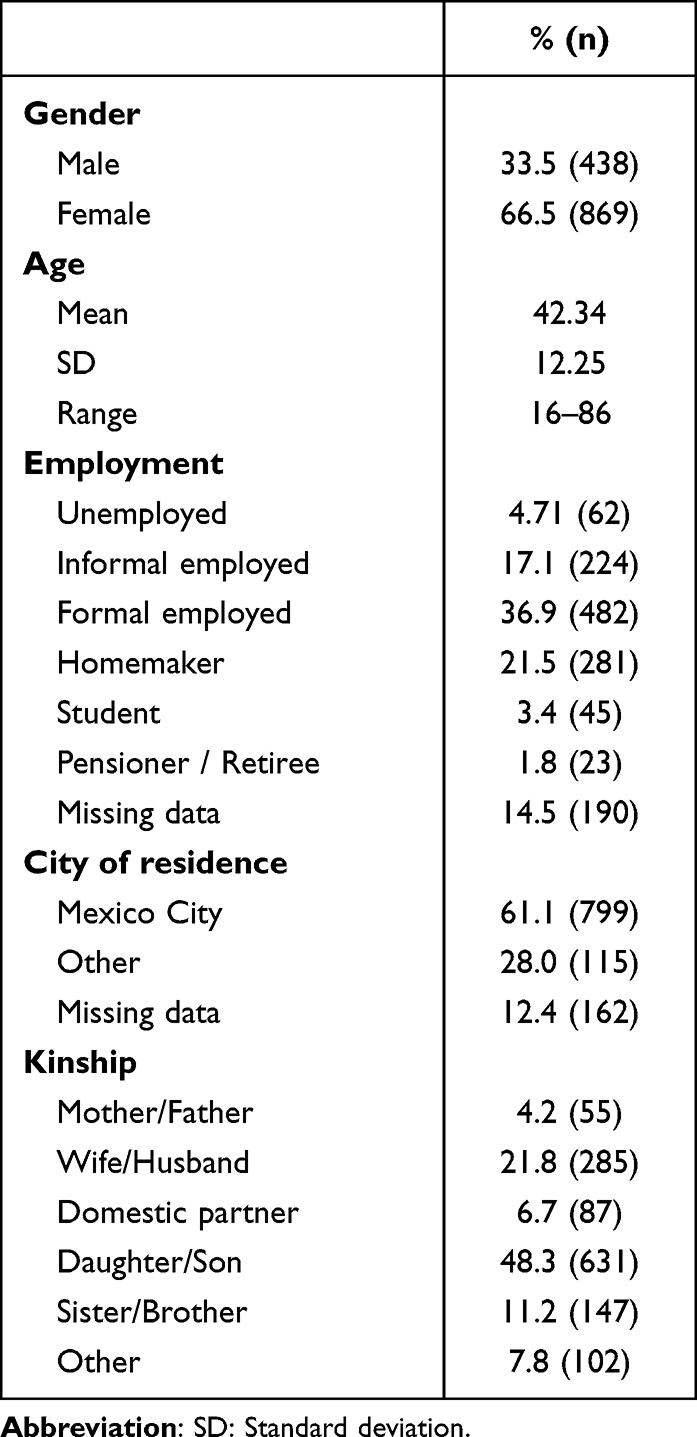 |
Table 1 Sociodemographic Characteristics of Relatives of Covid-19 Patients |
Anxiety and Depression Symptoms in Relatives of Critically Ill COVID-19 Patients
The sample of relatives (n=1307) had a mean GAD-7 score of 7.5 (SD=4.9) and a mean PHQ-9 score of 6.7 (SD=5.4). One hundred twenty-three relatives (9.4%) had severe anxiety symptoms and 325 (24.9%) moderate anxiety symptoms. Regarding depressive symptoms, 33 relatives (2.5%) had severe symptoms; 84 (6.4%) moderately severe symptoms and 267 (20.4%) moderate symptoms. The percentages of relatives in each level of anxiety and depression are shown in Figure 2. The psychologists established a diagnostic impression of both anxiety and depression symptoms in 321 relatives (24.6%); exclusively anxiety symptoms in 128 (9.8%); exclusively depression symptoms in 63 (4.8%); and adequate adaptation in 795 relatives (60.8%).
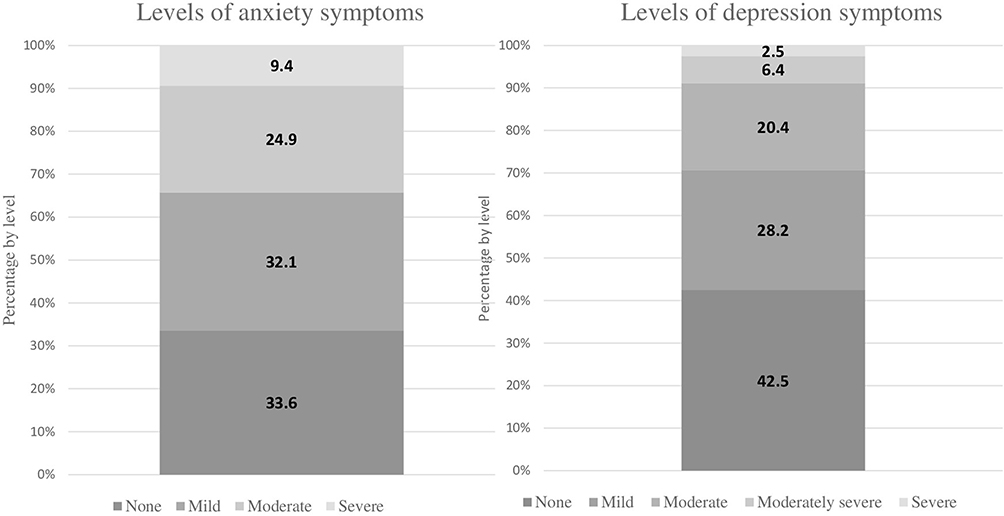 |
Figure 2 Percentages of Relatives in Each Level of Anxiety and Depression. |
Association of Anxiety and Depression Levels with Sociodemographic Characteristics in Relatives
Severe and moderate anxiety symptoms were significantly more common in women than in men (11.6% vs 5.0%, p<0.001 and 27.0% vs 20.5% p<0.001). Similarly, moderate, moderately severe and severe depression symptoms were significantly more common in women than in men (22.8% vs 15.8%, p<0.001; 7.4% vs 4.6% p<0.001; and 3.1% vs 1.4% p<0.001, respectively). Severe depression symptoms were significantly more common in unemployed relatives than in the employed ones (4.6% vs 1.6%, p=0.021). Parents and partners had higher proportions of severe anxiety symptoms (p=0.012) and severe depression symptoms (p<0.001) compared to individuals with another type of kinship. No significant differences were found in anxiety and depression levels by age groups. The complete data about association between anxiety and depression levels with sociodemographic characteristics of relatives are shown in Table 2 and Table 3.
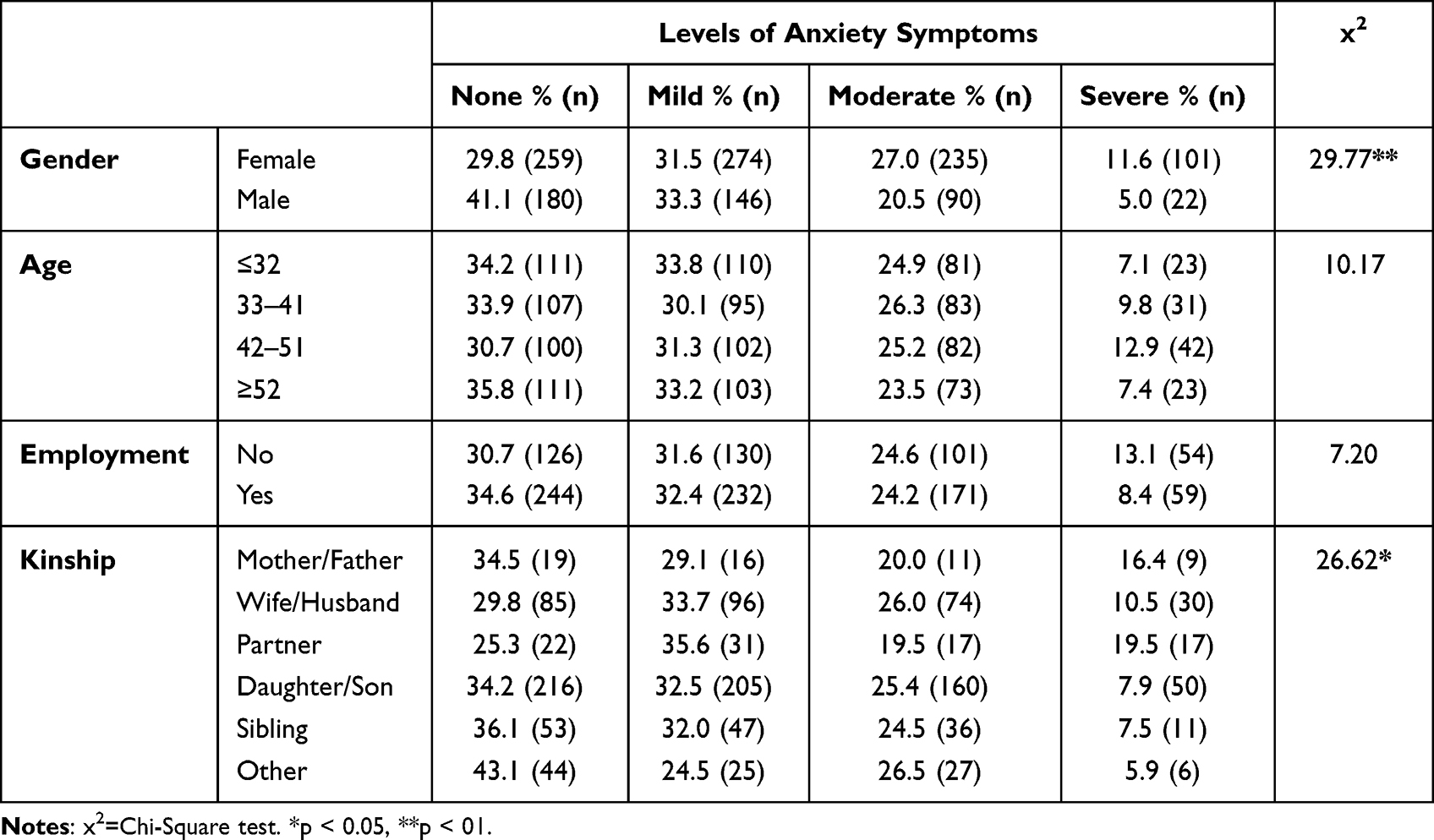 |
Table 2 Association Between Anxiety Levels and Sociodemographic Characteristics of Relatives of Critically Ill Covid-19 Patients |
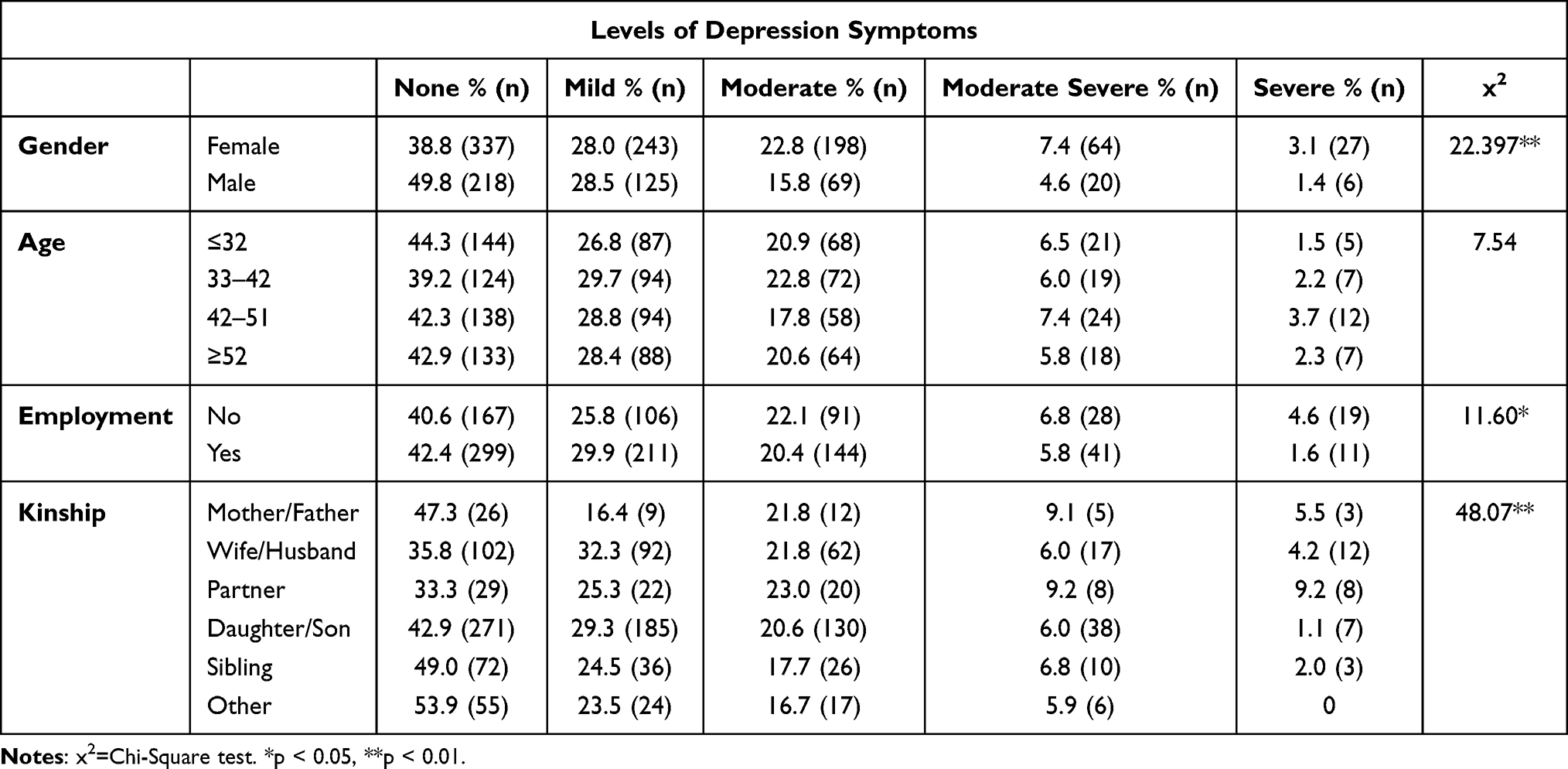 |
Table 3 Association Between Depression Levels and Sociodemographic Characteristics of Relatives of Critically Ill Covid-19 Patients |
The logistic regression models about the absence and presence of depressive and anxious symptoms were not significant (x2= 8.367, p=0.212 and x2= 2.441, p=0.931). In both models, sex was the only significant predictor of anxiety (OR=2.199, 95% CI 1.606–3.011, p<0.001) and depressive symptoms (OR=1.780, 95% CI 1.310–2.420, p<0.001).
Psychological Interventions and Improvement Perception
The most used interventions were emotional regulation techniques (42.2%, n=551) and psychoeducation (40.5%, n=529), while the others were used to a lesser extent, self-care strategies (6.7%, n=88), crisis intervention (6.4%, n=83) and positive feedback (4.3%, n=56). More than half of the relatives with adequate adaptation received psychoeducation (52.1%, n=414). About three quarters of the relatives with both anxiety and depression symptoms received regulation techniques (66.0%, n=212). The proportion of family members who received each psychological intervention, according to their diagnostic impression, is shown in Table 4.
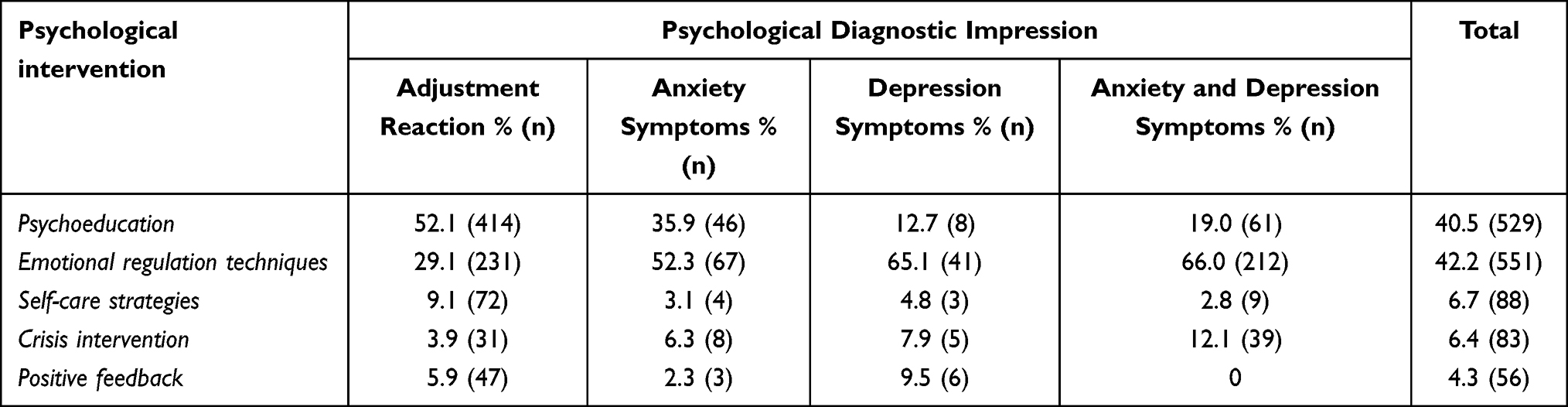 |
Table 4 Psychological Interventions Given According to the Diagnostic Impression |
A total of 1071 (82.0%) relatives completed the assessment of improvement, 620 felt better after the psychological intervention provided (57.9%); 335 felt a little better (31.3%); 72 felt much better (6.6%); 38 did not perceive any change (3.5%); and 6 felt worse (0.6%). The individuals who reported feeling better were more likely to have received psychoeducation (98.7%, n=464) and emotional regulation techniques (97.8%, n=405) (Table 5). Family members who received positive feedback were those who reported no improvement with higher frequency (36.8%). Some participants (n=236, 18%) were unable to complete the evaluation of the Patient Global Impression of Change due to lack of time. We did not find differences in sociodemographic data between relatives who completed the assessment and those who did not. However, those who did not complete the assessment were more likely to have had an adequate adaptation (p=0.026) or to be received emotional regulation techniques (p<0.001), which were somewhat longer interventions.
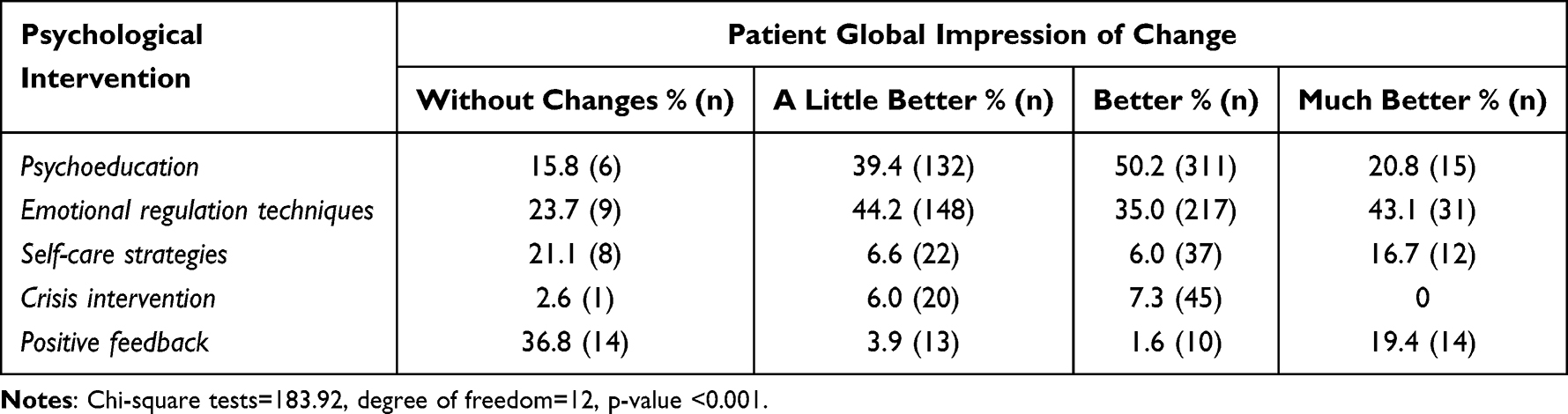 |
Table 5 Association Between Type of Psychological Interventions and Patient Global Impression of Change |
Discussion
One of the main objectives of this study was to identify the levels of anxiety and depression symptoms in relatives receiving the daily medical report of critically ill COVID-19 patients admitted to critical care areas. At the study site, due to pandemic restrictions, visitors were not allowed, but family members received a daily report on the status of their relative by phone call. We found that 34% and 29% of the relatives of critically ill COVID-19 patients had moderate to severe symptoms of anxiety and depression, respectively, according to scores of the GAD-7 and PHQ-9 tests. When the diagnostic impression was established by the psychologists, 25% of relatives had both anxiety and depression symptoms, 10% had exclusively anxiety symptoms and 5% had exclusively depression symptoms, indicating a high comorbidity of these psychological conditions. It is relevant to remind that the assessment was performed in the first 24h-48h from the time the patient was transferred from the emergency area (where they entered the hospital) to the ICU area. This is important for understanding the results of the study, since stress and anxiety levels can change throughout the hospital stay.
In our study, slightly more symptoms of anxiety and depression (34% and 29%) were found in relatives of ICU patients at the time of hospitalization than in other studies conducted during the pandemic (22%).16 Also, our results are consistent with the existing literature regarding the levels of anxiety and depression in relatives of patients admitted to the ICU (not for COVID-19) and those about the family members of COVID-19 patients.14–16 Our findings are also in line with those reported by Czeisler and cols,50 using the PHQ-4 in caregivers of older adults with chronic conditions during the COVID-19 pandemic. On the other hand, the percentage of family members with symptoms of anxiety in this study was higher than that reported by Gao et al51 for the general population during the COVID-19 pandemic. However, they reported lower symptoms of depression in relatives of the patients than those reported here. It is relevant to mention that depression and anxiety in the general population are associated with quarantine duration, infection fears, frustration, boredom, inadequate supplies and information, financial loss and stigma.52 Family members of COVID-19 patients of this study reported that depression and anxiety were to a large extent directly related to the hospitalization and the clinical condition of their patients.
We found that 65% of the patients were male and 66% of the relatives were females, these results support previous findings indicating that a greater number of men were affected by COVID-19 and had more complications.53 On the other hand, our findings corroborate the notion that women more often play the role of caregivers.54,55 In addition, the elevated proportion of women with moderate and severe symptoms of anxiety and depression found in our study, was similar to that reported in the general population,51 and informal primary caregivers.13,15 As reported by Scott and cols,13 the kinship is an important variable to consider, since a greater proportion of family members who were partners or parents, had severe and moderate symptoms of anxiety and depression compared with those having another type of relationship. It has been reported that mainly the partners in charge of caregiving activities may be those who present the greatest stress due to the high emotional involvement with the suffering family member.54
Regarding the objective of the performance, an exploratory pilot study on the implementation of psychological interventions to reduce the initial levels of anxiety and depression in this population, it was identified that the intervention most used by specialists was psychoeducation, preferred for family members receiving the diagnostic impression of “adequate adaptation”. Emotional regulation techniques were also implemented for relatives with symptoms of anxiety, depression, or both. Family members reported higher percentages of feeling better or much better with these techniques, and particularly with psychoeducation, supporting the notion that relatives have a great need of information about the health status and prognosis of their patient,13,27,56 although it is important to keep in mind that the techniques used were chosen depending on the needs and level of symptomatology of participants, which could affect these results.
Cognitive-behavioral therapy is an evidence-based intervention designed to change dysfunctional thoughts and behavior in several psychological disorders.28 This intervention is effective when delivered face to face and also when it is technology-based.29,57 However, some studies suggest that implementation via technology improves adherence as much as face-to-face but with a high risk of poorer maintenance in follow-up measures.58 Our results about perception of improvement with the use of emotional regulation techniques and psychoeducation via telephone could indicate that these kinds of interventions are suitable to improve emotional regulation in relatives of critically ill COVID‑19 patients. Regarding the participants who did not complete the assessment and ended the call earlier, they were probably people who spent more time on the phone, for example, with emotional regulation techniques, and were more likely to end the call abruptly. On the other hand, it could have been that people who did not find this intervention useful cut it off earlier, such as those with an adaptive reaction. This could have biased these results and should be taken into account when adapting the intervention to other populations. To our knowledge, this is the first study using emotional regulation techniques in relatives of critically ill COVID-19 patients. This is relevant for future studies on this topic, given the aforementioned importance for improved adaptation to hospitalization, better functioning in patient care after discharge and the increased likelihood of better grief in a given case. Nevertheless, we observed that these techniques can be difficult to apply via telephone (without the possibility of using visual aids, etc.), and psychologists should receive specific training to properly implement these cognitive-behavioral interventions in this way.
Implications for Practice
For those who are in charge of providing care to family members of patients who have to be hospitalized in intensive care units due to the severity of their health condition, it will be very important to specifically address informational needs, as well as to provide emotional regulation strategies that can mitigate the stressful effects of this situation. It is also important to identify those who have more symptoms of anxiety and/or depression, and in this regard, special attention should be paid to female caregivers and the patients’ partners and parents, as they may develop a worse reaction to the potentially disturbing situation. The interventions to be implemented can be from the first hours of hospitalization, to reduce the negative impact of the situation and can be brief and remote, which can favor adherence to the intervention and reach more people. For people with more marked needs, longer interventions, or even face-to-face interventions, should be explored to reduce the risk of them cutting off the call and not being able to receive the interventions they need.
Limitations
Our study has a large sample size as a strength, although it was limited by the cross-sectional nature of the study, which prevents us from understanding the long-term repercussions of these interventions. On the other hand, the sample belonged to a single center, with specific characteristics, so caution should be exercised before concluding that these results apply to other types of populations. Furthermore, in this study, we can only count on the information of those who voluntarily agreed to participate, which could imply a selection bias, since they may have been the people least affected or most motivated to face the situation. Also, 18% of the data about perception of improvement with psychological intervention was missing, and this may represent an additional bias in the analysis performed with this variable, despite we found no difference in sociodemographic variables between the family members who completed the evaluation and those who did not. Another study limitation was that we assessed the perception of improvement after psychological interventions in one phone call, with a one-item self-reporting measure, which may not represent the real effectiveness of the interventions, but only the perception of those who received them. In this sense, a longitudinal evaluation of the intervention would be very useful. Also, we recommend for future studies to consider other variables such educational level of participants, prior ICU experience, prior psychiatric diagnosis or the outcome of the hospitalized family member (clinical improvement, clinical deterioration, or death), or the fact that medical treatments for COVID-19 improved over the course of the study, which could affect caregivers’ anxiety and depression. For future studies, it could be useful to also include objective measures of the clinical condition of the patient to improve the external validity of the findings. It is also important to systematize the care provided by the different psychologists and use experimental designs (RCT) to explore the true effectiveness of these interventions.
Conclusions
Family members of critically ill patients who must be hospitalized in the intensive care unit are a population at risk of presenting moderate to severe symptoms of anxiety and depression, so it is important to address them as early as possible to reduce the impact of hospitalization. This will be especially important if the family member is female and/or the patient’s partner, as they are the most likely to develop these symptoms. In this sense, it will be important to carry out brief interventions that include elements of psychoeducation and emotional regulation strategies, since the participants reported greater changes with these techniques. In addition, in contexts where it is necessary, it is possible to provide these interventions remotely, by telephone, as they allow greater coverage and are well received. However, for longer interventions, in people who present high symptomatology and/or comorbidity of anxiety and depression, it is important to explore the possibility of doing it in person, since longer interventions are more difficult to complete over the phone.
Abbreviations
ICU, Intensive care unit; COVID-19, Coronavirus disease pandemic; GAD-7, General Anxiety Disorder Scale-7; PHQ-9, Patient Health Questionnaire-9; NIMH, National Institute of Mental Health.
Data Sharing Statement
The current article includes the complete raw data set collected in the study including the participants’ data set. The data file was uploaded to the Figshare repository, https://doi.org/10.6084/m9.figshare.20473821.v1.
Acknowledgments
The authors are gratefully indebted to the study participants. We thank social workers Graciela Guzman Valdes and Uriel Contreras Osorio, as well as the Coordination of Epidemiology and Statistics at the INER for the support provided during data collection. We also acknowledge the work of psychologists who collected the data: Rosa Cruz-Maycott, Lydia E. Perrusquia Ortiz, Gabriela Obregón Godinez, Gabriela Lara Rivas, Guadalupe Aguilar Estrada, Víctor Hugo Maldonado Troncoso, Nancy Castillo Linares, Eryka Urdapilleta Herrera, and to the psychology students Roberto Adrian Barriguete Rodriguez, Lizbeth Luna and Casandra Pineda.
Ethics Approval
Verbal informed consent was obtained from all participants included in the study. All procedures in studies involving human participants were performed in accordance with the ethical standards of the Research Ethics Committee of the Ismael Cosío Villegas National Institute of Respiratory Diseases, and the protocol research was approved with the number C34-21.
Patient Consent to Participate
Given restrictions imposed by the Severe Acute Respiratory Syndrome Coronavirus 2 pandemic, participants were invited by telephone and asked to give their verbal informed consent to participate in this study.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no potential conflicts of interest in this work.
References
1. Davidson JE, Jones C, Bienvenu OJ. Family response to critical illness: postintensive care syndrome-family. Crit Care Med. 2012;40(2):618–624. doi:10.1097/CCM.0b013e318236ebf9
2. Lee RY, Engelberg RA, Curtis JR, et al. Novel risk factors for PTSD symptoms in family members of ARDS survivors. Crit Care Med. 2019;47(7):934–941. doi:10.1097/CCM.0000000000003774
3. Onrust M, Lansink-Hartgring AO, van der Meulen I, et al. Coping strategies, anxiety and depressive symptoms in family members of patients treated with extracorporeal membrane oxygenation: a prospective cohort study. Heart Lung. 2022;52:146–151. doi:10.1016/j.hrtlng.2022.01.002
4. Garcia-Gordillo JA, Camiro-Zúñiga A, Aguilar-Soto M, et al. COVID-IRS: a novel predictive score for risk of invasive mechanical ventilation in patients with COVID-19. PLoS One. 2021;16(4):e0248357. doi:10.1371/journal.pone.0248357
5. García LF. immune response, inflammation, and the clinical spectrum of COVID-19. Front Immunol. 2020;11. doi:10.3389/fimmu.2020.01441
6. Ñamendys-Silva SA. Patients with coronavirus disease 2019 requiring invasive mechanical ventilation in Mexico in the first, second, and exponential growth phase of the third wave of the coronavirus disease 2019 pandemic. Crit Care Explor. 2021;3(10):e556. doi:10.1097/CCE.0000000000000556
7. Anwar A, Malik M, Raees V, et al. Role of mass media and public health communications in the COVID-19 pandemic. Cureus. 2020;12(9):e10453. doi:10.7759/cureus.10453
8. Melki J, Tamim H, Hadid D, et al. Mitigating infodemics: the relationship between news exposure and trust and belief in COVID-19 fake news and social media spreading. PLoS One. 2021;16(6):e0252830. doi:10.1371/journal.pone.0252830
9. Honarmand K, Mehta S. Consequences of visitor restriction policies in the intensive care unit during the COVID-19 pandemic. Can J Anaesth. 2021;68(10):1465–1470. doi:10.1007/s12630-021-02048-5
10. Nakanishi N, Liu K, Kawakami D, et al. Post-intensive care syndrome and its new challenges in coronavirus disease 2019 (COVID-19) pandemic: a review of recent advances and perspectives. J Clin Med. 2021;10(17):3870. doi:10.3390/jcm10173870
11. Imanipour M, Kiwanuka F, Akhavan Rad S, et al. Family members’ experiences in adult intensive care units: a systematic review. Scand J Caring Sci. 2019;33(3):569–581. doi:10.1111/scs.12675
12. Cypress BS. Understanding uncertainty among critically ill patients in the intensive care unit using mishel’s theory of uncertainty of illness. Dimens Crit Care Nurs. 2016;35(1):42–49. doi:10.1097/DCC.0000000000000152
13. Scott P, Thomson P, Shepherd A. Families of patients in ICU: a Scoping review of their needs and satisfaction with care. Nurs Open. 2019;6(3):698–712. doi:10.1002/nop2.287
14. Naef R, von Felten S, Ernst J. Factors influencing post-ICU psychological distress in family members of critically ill patients: a linear mixed-effects model. Biopsychosoc Med. 2021;15(1):4. doi:10.1186/s13030-021-00206-1
15. Sharma A, Singh T, Bharti A, et al. mental health status among the family members of COVID‑19 patients in Jabalpur district madhya pradesh: a cross‑sectional study. J Prim Care Special. 2020;1(1):8–12. doi:10.4103/jopcs.jopcs_7_20
16. Heesakkers H, van der Hoeven JG, Corsten S, et al. Mental health symptoms in family members of COVID-19 ICU survivors 3 and 12 months after ICU admission: a multicentre prospective cohort study. Intensive Care Med. 2022;48(3):322–331. doi:10.1007/s00134-021-06615-8
17. Galindo-Vázquez O, Ramírez-Orozco M, Costas-Muñiz R, et al. Symptoms of anxiety, depression and self-care behaviors during the COVID-19 pandemic in the general population. Gac Med Mex. 2020;156(4):298–305. doi:10.24875/GMM.20000266
18. Azoulay E, Resche-Rigon M, Megarbane B, et al. Association of covid-19 acute respiratory distress syndrome with symptoms of posttraumatic stress disorder in family members after ICU discharge. JAMA. 2022;327(11):1042–1050. doi:10.1001/jama.2022.2017
19. Needham DM, Davidson J, Cohen H, et al. Improving long-term outcomes after discharge from intensive care unit: report from a stakeholders’ conference*. Crit Care Med. 2012;40(2):502. doi:10.1097/CCM.0b013e318232da75
20. Zante B, Camenisch SA, Schefold JC. Interventions in post-intensive care syndrome-family: a systematic literature review. Crit Care Med. 2020;48(9):e835–e840. doi:10.1097/CCM.0000000000004450
21. Applebaum AJ, Breitbart W. Care for the cancer caregiver: a systematic review. Palliat Support Care. 2013;11(3):231–252. doi:10.1017/S1478951512000594
22. Cherak SJ, Rosgen BK, Amarbayan M, et al. Mental health interventions to improve psychological outcomes in informal caregivers of critically ill patients: a systematic review and meta-analysis*. Crit Care Med. 2021;49(9):1414–1426. doi:10.1097/CCM.0000000000005011
23. Chiang VCL, Chien WT, Wong HT, et al. A brief cognitive-behavioral psycho-education (B-CBE) program for managing stress and anxiety of main family caregivers of patients in the intensive care unit. Int J Environ Res Public Health. 2016;13(10):962. doi:10.3390/ijerph13100962
24. Lally RM, Brooks C. Psychoeducational interventions for supporters of women with breast cancer: an integrative review. J Cancer Educ. 2016;31(4):626–632. doi:10.1007/s13187-015-0883-3
25. Malouff JM, Thorsteinsson EB, Schutte NS. The efficacy of problem solving therapy in reducing mental and physical health problems: a meta-analysis. Clin Psychol Rev. 2007;27(1):46–57. doi:10.1016/j.cpr.2005.12.005
26. Northouse LL, Katapodi MC, Song L, et al. Interventions with family caregivers of cancer patients: meta-analysis of randomized trials. CA Cancer J Clin. 2010;60(5):317–339. doi:10.3322/caac.20081
27. Chien W-T, Chiu YL, Lam L-W, et al. Effects of a needs-based education programme for family carers with a relative in an intensive care unit: a quasi-experimental study. Int J Nurs Stud. 2006;43(1):39–50. doi:10.1016/j.ijnurstu.2005.01.006
28. Hofmann SG, Asnaani A, Vonk IJJ, et al. The efficacy of cognitive behavioral therapy: a review of meta-analyses. Cogn Ther Res. 2012;36(5):427–440. doi:10.1007/s10608-012-9476-1
29. Petrinec A, Wilk C, Hughes JW, et al. Delivering cognitive behavioral therapy for post–intensive care syndrome–family via a mobile health app. Am J Crit Care. 2021;30(6):451–458. doi:10.4037/ajcc2021962
30. Alqahtani MMJ, Alkhamees HA, Alkhalaf AM, et al. Toward establishing telepsychology guideline. Turning the challenges of COVID-19 into opportunity. Ethics Med Public Health. 2021;16:100612. doi:10.1016/j.jemep.2020.100612
31. Cox CE, Hough CL, Carson SS, et al. Effects of a telephone- and web-based coping skills training program compared with an education program for survivors of critical illness and their family members. A randomized clinical trial. Am J Respir Crit Care Med. 2018;197(1):66–78. doi:10.1164/rccm.201704-0720OC
32. Gutiérrez-Velilla E, Barrientos-Casarrubias V, Cruz-Maycott R, et al. Assessment of anxiety in Mexican persons living with HIV using a culturally-adapted version of the GAD-7 test. J Health Psychol. 2022;2022:13591053211072688.
33. Spitzer RL, Kroenke K, Williams JBW, et al. A Brief Measure for Assessing Generalized Anxiety Disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092–1097. doi:10.1001/archinte.166.10.1092
34. Arrieta J, Aguerrebere M, Raviola G, et al. Validity and Utility of the Patient Health Questionnaire (PHQ)-2 and PHQ-9 for screening and diagnosis of depression in rural chiapas, Mexico: a cross-sectional study. J Clin Psychol. 2017;73(9):1076–1090. doi:10.1002/jclp.22390
35. Familiar I, Ortiz-Panozo E, Hall B, et al. Factor structure of the Spanish version of the patient health questionnaire-9 in Mexican women. Int J Methods Psychiatr Res. 2015;24(1):74–82. doi:10.1002/mpr.1461
36. Spitzer RL, Kroenke K, Williams JBW, et al. Validation and Utility of a Self-report Version of PRIME-MDThe PHQ Primary Care Study. JAMA. 1999;282(18):1737–1744. doi:10.1001/jama.282.18.1737
37. Guy W. ECDEU Assessment Manual for Psychopharmacology. Washington, D. C: Department of Health Education and Welfare; 1976.
38. Hellerstein DJ, Yanowitch P, Rosenthal J, et al. A randomized double-blind study of fluoxetine versus placebo in the treatment of dysthymia. Am J Psychiatry. 1993;150:1169–1175.
39. Stein MB, Liebowitz MR, Lydiard RB, et al. Paroxetine treatment of generalized social phobia (social anxiety disorder)a randomized controlled trial. JAMA. 1998;280(8):708–713. doi:10.1001/jama.280.8.708
40. Barlow DH, Gorman JM, Shear MK, et al. Cognitive-behavioral therapy, imipramine, or their combination for panic disorder: a randomized controlled trial. JAMA. 2000;283(19):2529–2536. doi:10.1001/jama.283.19.2529
41. Brady K, Pearlstein T, Asnis GM, et al. Efficacy and safety of sertraline treatment of posttraumatic stress disorder: a randomized controlled trial. JAMA. 2000;283(14):1837–1844. doi:10.1001/jama.283.14.1837
42. Hudson JI, McElroy SL, Raymond NC, et al. Fluvoxamine in the treatment of binge-eating disorder: a multicenter placebo-controlled, double-blind trial. Am J Psychiatry. 1998;155(12):1756–1762. doi:10.1176/ajp.155.12.1756
43. Navidian A, Rezaei J, Payan H. Efficacy of supportive - educational intervention on psychological reactions of family members of intensive care unit patients. J Nurs Educ. 2016;5(4):51–58. doi:10.21859/jne-05047
44. Dolan N, Simmonds-Buckley M, Kellett S, et al. Effectiveness of stress control large group psychoeducation for anxiety and depression: systematic review and meta-analysis. Br J Clin Psychol. 2021;60(3):375–399. doi:10.1111/bjc.12288
45. Bermejo-Martins E, Luis EO, Fernández-Berrocal P, et al. The role of emotional intelligence and self-care in the stress perception during COVID-19 outbreak: an intercultural moderated mediation analysis. Personal Individ Differ. 2021;177:110679. doi:10.1016/j.paid.2021.110679
46. Caballo V. Manual de Técnicas de Terapia y Modificación de Conducta. México: Siglo XXI; 2009.
47. Aldao A, Nolen-Hoeksema S, Schweizer S. Emotion-regulation strategies across psychopathology: a meta-analytic review. Clin Psychol Rev. 2010;30(2):217–237. doi:10.1016/j.cpr.2009.11.004
48. Zhang J, Wu W, Zhao X, et al. Recommended psychological crisis intervention response to the 2019 novel coronavirus pneumonia outbreak in China: a model of West China Hospital. Precis Clin Med. 2020;3(1):3–8. doi:10.1093/pcmedi/pbaa006
49. Editorial E. Declaración de Helsinki de la Asociación Médica Mundial. Arbor. 2008;184:349–352.
50. Czeisler MÉ, Lane RI, Petrosky E, et al. Mental health, substance use, and suicidal ideation during the COVID-19 Pandemic — United States, June 24–30, 2020. Morb Mortal Wkly Rep. 2020;69(32):1049–1057. doi:10.15585/mmwr.mm6932a1
51. Gao J, Zheng P, Jia Y, et al. Mental health problems and social media exposure during COVID-19 outbreak. PLoS One. 2020;15(4):e0231924. doi:10.1371/journal.pone.0231924
52. Brooks SK, Webster RK, Smith LE, et al. The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet Lond Engl. 2020;395(10227):912–920. doi:10.1016/S0140-6736(20)30460-8
53. Hu J, Wang Y. The clinical characteristics and risk factors of severe COVID-19. Gerontology. 2021;67(3):255–266. doi:10.1159/000513400
54. Vázquez ÓG, García AM, Gómez ÁH, et al. Escala Hospitalaria de Ansiedad y Depresión (HADS) en cuidadores primarios informales de pacientes con cáncer: propiedades psicométricas. Psicooncología. 2015;12:383–392.
55. Torres-Avendaño B, Agudelo-Cifuentes MC, Pulgarin-Torres ÁM, et al. Factores asociados a la sobrecarga en el cuidador primario Medellín, 2017. Univ Salud. 2018;20(3):261–269. doi:10.22267/rus.182003.130
56. Kynoch K, Chang A, Coyer F, et al. The effectiveness of interventions to meet family needs of critically ill patients in an adult intensive care unit: a systematic review update. JBI Evid Synth. 2016;14:181–234.
57. Stiles-Shields C, Kwasny MJ, Cai X, et al. Therapeutic alliance in face-to-face and telephone-administered cognitive behavioral therapy. J Consult Clin Psychol. 2014;82(2):349–354. doi:10.1037/a0035554
58. Mohr DC, Ho J, Duffecy J, et al. Effect of telephone-administered vs face-to-face cognitive behavioral therapy on adherence to therapy and depression outcomes among primary care patients: a randomized trial. JAMA. 2012;307(21):2278–2285. doi:10.1001/jama.2012.5588
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.