Back to Journals » Psychology Research and Behavior Management » Volume 19
Association Between Sleep Quality and Cognitive Function in Patients with Hypertension in Rural Areas of Shanxi Province, China: The Chain Mediating Role of Anxiety and Depression
Authors Li S, Liang R, Liu J, Sun W, Wang J, Li S, Zhao S, Niu Q, Yu H, Zhang H, Qin X ![]() , Bai R, Li Y
, Bai R, Li Y
Received 2 January 2026
Accepted for publication 16 March 2026
Published 7 April 2026 Volume 2026:19 593258
DOI https://doi.org/10.2147/PRBM.S593258
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Gabriela Topa
Siyi Li,1 Ruifeng Liang,1– 3 Jiawei Liu,1 Wenhua Sun,1 Jue Wang,1 Simin Li,4 Shuhong Zhao,4 Qiao Niu,1,2,5 Hongmei Yu,1,2 Hongmei Zhang,1,2 Xiaojiang Qin,1,2 Runshan Bai,6 Yanjie Li7
1School of Public Health, Shanxi Medical University, Jinzhong, People’s Republic of China; 2MOE Key Laboratory of Coal Environmental Pathogenicity and Prevention, Shanxi Medical University, Taiyuan, People’s Republic of China; 3Yellow River Basin Ecological Public Health Security Center, Shanxi Medical University, Taiyuan, People’s Republic of China; 4Evaluation Center for Medical Service and Administration, Health Commission of Shanxi Province, Taiyuan, People’s Republic of China; 5Key Laboratory of Cellular Physiology (Shanxi Medical University), Ministry of Education, Taiyuan, People’s Republic of China; 6Grassroots Health Department, Health and Health Bureau of Yonghe County, Linfen, People’s Republic of China; 7Gates Project Department, Health and Health Bureau of Daning County, Linfen, People’s Republic of China
Correspondence: Ruifeng Liang, School of Public Health, Shanxi Medical University, Jinzhong, People’s Republic of China, Email [email protected]
Background: Many studies have found that sleep quality is associated with cognitive function, but how sleep quality is related to cognitive function indirectly through anxiety and depression is still unclear. This study aims to investigate the association between sleep quality and cognitive function among patients with hypertension in rural areas of Shanxi Province and to analyze the potential mediating role of anxiety and depression.
Methods: 325 patients with primary hypertension were selected as the research subjects from Daning County and Yonghe County of Shanxi Province using the multistage cluster random sampling method. The Pittsburgh Sleep Quality Index, Montreal Cognitive Assessment, Generalized Anxiety Disorder-7, and Patient Health Questionnaire-9 were used to assess their sleep quality, cognitive function, anxiety, and depression levels, respectively. Structural equation modeling was employed to analyze the mediating effects of anxiety and depression.
Results: The scores of sleep quality and cognitive function of patients with hypertension were 7.0 (4.0, 8.0) and 19.0 (15.0, 25.0), respectively. The results of the structural equation model analysis demonstrated that sleep quality was directly associated with cognitive function in patients with hypertension, with a path coefficient of − 0.544, accounting for 59.85% of the total association. Anxiety and depressive symptoms showed a mediating role in the relationship between sleep quality and cognitive function, with indirect effects of − 0.190 and − 0.069, accounting for 20.90% and 7.59% of the total association, respectively. The chain mediating role of anxiety and depressive symptoms in the relationship between sleep quality and cognitive function among patients with hypertension was − 0.105, accounting for 11.55% of the total association.
Conclusion: These findings underscore the necessity of improving sleep quality and mitigating anxiety and depression as potential strategies for addressing cognitive deterioration. It is also of great importance for screening and comprehensive management of sleep and mental health in hypertension care.
Keywords: hypertension, sleep quality, cognitive function, anxiety, depression, mediating role
Introduction
Hypertension is defined as a systolic blood pressure ≥ 140 mmHg and/or a diastolic blood pressure ≥ 90 mmHg in three measurements on different days without the use of antihypertensive drugs.1 The 2023 World Health Organization report, “Global Report on Hypertension: The Race Against a Silent Killer”, indicated that between 1990 and 2019, the number of people with hypertension worldwide doubled, increasing from 650 million in 1990 to 1.3 billion in 2019. By 2019, approximately 49% of men and 59% of women aged 30 to 79 worldwide were suffering from hypertension.2 Hypertension has become a major global public health problem. In recent years, the prevalence of hypertension among adults in China has also been on the rise, from 23.2% in 2012–20153 to 27.5% in 2018.4 The prevalence of hypertension among adults in China had reached 31.6% by 2021–2022, with a higher prevalence in rural areas (33.7%) when compared to urban areas (29.1%).5
Hypertension is a risk factor for cardiovascular disease, chronic kidney disease, stroke, and other diseases and for cognitive impairment (CogI).6,7 CogI is a syndrome characterized by acquired, persistent cognitive dysfunction that leads to diminished ability to perform daily activities and work, as well as behavioral changes. As the disease progresses, patients with CogI may gradually progress from having mild cognitive impairment (MCI) to dementia. About 10%–15% of patients with MCI develop dementia every year.8 One study found that the prevalence of CogI among patients with hypertension in China was 37.6%.9 CogI increases the economic burden of patients with hypertension and also increases the rate of rehospitalization of patients.10,11 Therefore, it is important to detect and identify the risk factors for CogI at an early stage.
The Emotion Cascade Model (ECM) was formally proposed by Selby and Joiner (2009)12 to explain the dysregulated behaviors of individuals with borderline personality disorder (BPD) and has since been widely applied in research on non-suicidal self-injury (NSSI), depression, anxiety, and other areas. Rumination is the core cognitive process of the Emotion Cascade Model (ECM), defined as the tendency of individuals to repeatedly think about the causes, situational factors, and consequences of negative emotional experiences; that is, individuals continuously think about and pay attention to emotion-related stimuli. In emotional cascading, people repeatedly and intensely think about events that trigger negative emotions, becoming increasingly uneasy in the process. The end result is a self-amplifying positive feedback loop, containing intense rumination and negative emotions. When rumination interacts with negative emotions, the cycle repeats, leading to intense and unbearable emotional experiences. The individual becomes completely focused on the emotional stimuli, making it difficult to break free. Normal distraction methods fail, creating an extremely aversive, painful, and intolerable emotional state. To “break” this cycle, individuals engage in maladaptive behaviors: disordered behaviors (such as self-harm, binge eating, and substance abuse) are used to divert attention from the emotional cascade through intense physical sensations.13
The core mechanism of ECM can be directly mapped to the sleep-emotion-cognition domain: (1) Sleep → Anxiety: Initial cascade trigger. Sleep disorders are often accompanied by pre-sleep rumination, focusing attention on the negative stimulus of “not being able to sleep”. According to ECM, this leads to an increase in the intensity and duration of anxiety. (2) Anxiety → Depression: Cascading amplification process. The positive feedback loop of ECM explains why anxiety develops into depression: anxious rumination → intensification of negative emotions → stronger rumination → further emotional deterioration. When this cycle continues, acute anxiety transforms into persistent depression.14 (3) Depression → Cognition: The ultimate cascading effect. High levels of rumination in a state of depression consume a significant amount of cognitive resources. When emotional cascading reaches its peak, normal cognitive regulation strategies fail, and cognitive functions (attention, memory, and executive functions) are impaired. Cognitive impairment becomes the “final manifestation” of emotional cascading.15 Therefore, it is crucial and valuable to study the complex relationships between sleep quality, anxiety, depression, and cognitive function in patients with hypertension.
The Relationship Between Sleep Quality and Cognitive Function
Sleep performs multiple fundamental biological functions within the human body, such as maintenance, repair, and reconstruction of the organism.16 Headaches, chest pains, and dizziness caused by hypertension often lead to a decline in patients’ sleep quality.17 In addition, some patients with hypertension have poor blood pressure control at night and may have either high or low blood pressure.18 High blood pressure can lead to excessive brain activity, making it difficult to fall asleep, whereas low blood pressure may lead to an insufficient blood supply to the brain, thereby inducing sleep disorders.19 A meta-analysis indicated that the prevalence of poor sleep quality among patients with hypertension in China was as high as 52.5%, and their risk of experiencing poor sleep quality was 2.7 times higher than that among healthy controls.20
Sleep deprivation acutely impairs fundamental cognitive functions, including concentration, alertness, and reaction speed, while also disrupting critical processes of memory consolidation and retrieval21—a phenomenon exemplified by the diminished recall often experienced by students after intensive last-minute study sessions. Beyond these immediate effects, higher-order executive functions such as planning, problem-solving, and decision-making are similarly compromised, resulting in increased error rates and reduced efficiency during complex tasks.22 In the long term, chronic poor sleep quality significantly elevates the risk of progressive cognitive decline.23 Research indicates that individuals with chronic insomnia face a 40% higher risk of developing mild cognitive impairment or dementia compared with those without insomnia (HR 1.40, 95% CI 1.07–1.85)—an increase equivalent to approximately 3.5 years of brain aging.23 Moreover, persistent sleep disturbances are associated with structural alterations in the brain, including the development of white matter hyperintensities (indicative of small vessel disease) and an increased accumulation of amyloid plaques, a key neuropathological hallmark of Alzheimer’s disease (AD).24
Studies have established a strong association between poor sleep quality and MCI, with prevalence rates of sleep disturbances estimated between 35% and 48% among MCI patients.25 This association strengthens with disease progression: sleep disorders are reported in approximately 25%26 of patients with mild-to-moderate AD, a prevalence that rises sharply to 50% among those with moderate-to-severe AD.27
The Mediating Role of Anxiety
In addition to direct effects, sleep quality may also indirectly influence cognitive function through mediating factors, with anxiety emerging as a key potential mediator.28 As a disorder of emotional regulation, anxiety may impair cognitive performance by disrupting the allocation of neurocognitive resources and interfering with emotion regulation processes.29
Existing research highlights a close interrelationship among sleep quality, anxiety, and cognitive function. Studies show that sleep quality is significantly correlated with anxiety levels. Chronically poor sleep increases an individual’s vigilance to environmental threats, thereby inducing or exacerbating anxiety.30,31 In addition, the negative impact of anxiety on cognitive function has been established across multiple domains. Research indicates that elevated anxiety is associated with deficits in executive function, working memory, and attentional control.32 For instance, anxiety may consume limited cognitive resources and reduce the efficiency of task-relevant information processing, ultimately compromising performance on cognitive tasks.33
Although existing evidence supports the two independent paths of “sleep quality-anxiety” and “anxiety-cognitive function”, few studies have systematically explored the mediating mechanism of anxiety in the relationship between sleep quality and cognitive function. It is worth noting that some studies have observed that the deterioration of sleep quality may indirectly affect cognitive performance through the emotional regulation path, suggesting that anxiety may be a psychological bridge between the two.34 An experimental study found that sleep disturbance can induce anxiety, which in turn affects the reaction speed and accuracy of subjects in attention tasks;35 another longitudinal study showed that after sleep quality improved, individuals’ anxiety levels decreased, and their performance in cognitive tests improved.36 Based on the above theoretical and empirical basis, this study proposes the hypothesis that anxiety plays a mediating role between sleep quality and cognitive function.
The Mediating Role of Depression
As a fundamental physiological process crucial for maintaining normal cognitive function, sleep quality plays a key regulatory role in attention, memory, and executive function.37 Numerous studies have shown that chronic sleep disorders, such as insomnia and poor sleep efficiency, can lead to depletion of cognitive resources and accelerate cognitive aging.38 Concurrently, depression is highly prevalent among patients with hypertension.39 Its core symptoms—including low mood, lack of motivation, and cognitive slowing—are not only strongly comorbid with sleep disturbances but may also directly impair cognitive processing efficiency, particularly in domains such as working memory, information processing speed, and decision-making ability.40
Longitudinal evidence indicates that declines in sleep quality significantly elevate the risk of depression, which in turn can further exacerbate cognitive decline, suggesting that depression may serve as a mediator between sleep and cognition.41 Specifically, poor sleep quality may trigger or worsen depressive symptoms by disrupting neuroendocrine regulation (eg, dysfunction of the HPA axis), increasing inflammatory responses, and impairing emotion regulation capacity.42 A depressive state, in turn, may contribute to reduced cognitive performance through mechanisms such as diminished cognitive engagement, heightened negative cognitive bias, and lowered psychological resilience.43 In other words, the effect of sleep on cognition is not entirely direct; part of this relationship may operate through the psychological pathway of depression.44 Based on theoretical frameworks and empirical findings, this study proposes the hypothesis that depression mediates the relationship between sleep quality and cognitive function.
The Chain Mediating Role of Anxiety and Depression
Polysomnography and actigraphy studies have demonstrated a remarkable association between poor sleep quality and impaired neuropsychological function.45 Poor sleep quality may lead to an imbalance of levels of neurotransmitters related to mood regulation in the brain, such as serotonin and dopamine, thereby increasing the risk of anxiety and depression.46 One study found that people with insomnia were nearly 40 times more likely to develop depression and more than 6 times more likely to develop anxiety than those without insomnia.47 In addition, several prospective studies have shown that anxiety symptoms can predict the onset of depressive symptoms. For example, a study by Pine et al found that anxiety and depressive symptoms in adolescence affect mental health in adolescence and remarkably increase the risk of depression in adulthood, with the risk increasing by about 2 to 3 times.48 Another study based on a New Zealand birth cohort found that in 37% of depression cases, anxiety occurred before or at the same time as depression. The relationship between sleep quality and mental health is thus well-established.49
Anxiety and depression are often associated with cognitive decline.50 People with depression are more likely to experience cognitive decline compared to healthy people, especially when depression is concurrent with anxiety.51 Neurophysiological studies have also shown that depressive symptoms may reduce the production of serum brain-derived neurotrophic factor, leading to neuronal and hippocampal atrophy, thereby affecting cognitive function.52 Based on these findings, this study proposes the hypothesis that the symptoms of anxiety affect those of depression and that anxiety and depression have a chain mediating effect between sleep quality and cognitive function.
Research Questions
The mediating effect refers to the mechanism of action in which the independent variable indirectly affects the dependent variable through the mediating variable. The chain mediating effect refers to the indirect influence mechanism in which there are multiple mediating variables in the study, and a chain of transmission is formed; that is, the process in which the independent variable is transmitted through multiple mediating variables, which ultimately affects the dependent variable. However, most of the existing studies focus on the relationship between anxiety, depression, sleep quality, and cognitive function. Whether anxiety and depression have chain mediating effects between sleep quality and cognitive function has not been fully verified.53,54 In addition, no prior study has examined sleep-cognition relationships in rural hypertensive populations in Shanxi Province, China—an underserved group with high cardiovascular risk and limited healthcare access. We employed structural equation modeling with serial mediation analysis and bootstrap inference to disentangle direct and indirect pathways, an approach rarely applied in this population. The chain mediation model advances understanding by quantifying the relative contributions of anxiety and depression as sequential mediators. Therefore, this study aims to explore the relationship between sleep quality and cognitive function and the mediating role of depression and anxiety in this relationship. We specifically put forward the following hypotheses:
Hypothesis 1: Poor sleep quality in patients with hypertension has a negative impact on cognitive function. Hypothesis 2: Anxiety has a mediating effect between sleep quality and cognitive function. Hypothesis 3: Depression has a mediating effect between sleep quality and cognitive function. Hypothesis 4: Anxiety and depression have a chain mediating effect between sleep quality and cognitive function.
Materials and Methods
Participants
In July 2024, a multistage cluster random sampling method was used to select patients with primary hypertension in Daning County and Yonghe County, Linfen City, Shanxi Province, for investigation. The inclusion criteria were as follows: (1) age ≥ 18 years; (2) patients with essential hypertension among permanent residents in Daning County or Yonghe County, in Linfen City, Shanxi Province (permanent residents refer to those who had resided in Daning County or Yonghe County, Linfen City, Shanxi Province, for 6 months or more within the past 12 months); (3) the diagnostic criteria for hypertension were based on the diagnostic criteria in the “Chinese Guidelines for the Prevention and Treatment of Hypertension (2024 Revised Edition)”.1 In patients not on antihypertensive medication, a diagnosis of hypertension can be made if three separate clinic blood pressure readings on different days exceed 140/90 mmHg, home blood pressure measurements over 5–7 consecutive days exceed 135/85 mmHg, or 24-hour ambulatory blood pressure monitoring shows an average greater than 130/80 mmHg, with daytime readings exceeding 135/85 mmHg and nighttime readings exceeding 120/70 mmHg. Patients with a history of hypertension who are currently taking antihypertensive medication should still be diagnosed with hypertension even if their blood pressure is below the above diagnostic thresholds; (4) The patient can communicate independently. Exclusion criteria: (1) age < 18 years; (2) patients with primary hypertension who are not permanent residents of Daning County or Yonghe County, Linfen City, Shanxi Province; (3) patients with secondary hypertension (such as renal hypertension and endocrine hypertension); (4) those who cannot communicate normally.
Informed consent was obtained from all the participants in the study. This study has been reviewed by the Ethics Committee of Shanxi Medical University (2020SLL201).
Sample Size Estimation
According to the sample size estimation formula of the structural equation modeling, the recommended sample size should ideally be 10 to 15 times the number of scale dimensions. In this study, the sample size was calculated by multiplying 15 by 16 dimensions, so the minimum sample size was 240. Considering a potential 15% rate of invalid questionnaires, a total sample size of 276 participants was deemed necessary. The initial study recruited 350 participants, following which 25 participants were excluded due to the obvious irregularity of their answers. Therefore, this study included a total of 325 participants.
Measures
General Information Questionnaire
The main contents included gender, age, education level, marital status, and living style.
Sleep Quality
The Pittsburgh Sleep Quality Index was compiled by Dr. Buysse and other psychiatrists at the University of Pittsburgh in the United States in 1989.55 Translated and localized by Xianchen Liu et al56 It is suitable for evaluating sleep quality in patients with sleep disorders and psychiatric conditions, as well as for assessing sleep quality in the general population. The scale comprises a total of 19 items, including 7 dimensions of sleep latency, sleep disturbance, subjective sleep quality, sleep duration, sleep efficiency, use of hypnotic drugs, and daytime dysfunction. Each dimension is scored between 0 and 3 points, and the total score is between 0 and 21 points. Among them, a total score between 0 and 5 points indicates very good sleep quality, 6 and 10 points indicate good sleep quality, 11 and 15 points indicate general sleep quality, and 16 and 21 points indicate poor sleep quality. In this study, the Cronbach’s α coefficient of the scale was 0.762.
Cognitive Function
The Montreal Cognitive Assessment (MoCA) was compiled by Nasreddine et al57 and the Beijing version was translated and localized by Wei Wang et al58 MoCA assesses the cognitive function of the subjects across seven aspects, namely, visuospatial and executive function, naming, attention, language ability, abstraction, delayed recall, and orientation. The scores of all the items were added to obtain the total score. A total score of ≥ 26 indicated normal cognitive function, and a score of < 26 indicated cognitive decline. Those with 12 years or less of education were given an additional point to correct for the influence of their education level. In this study, the Cronbach’s α coefficient of the scale was 0.789.
Depression
The Patient Health Questionnaire-9 was used to assess depressive symptoms. This scale was based on the nine-symptom criteria for depression in the Diagnostic and Statistical Manual of Mental Disorders published by the American Psychiatric Association.59 Translated and localized by Yuan Feng et al60 The scale contains nine items where each item is scored from 0 to 3; 0 means that the symptom never appears and 3 means that the symptom appears almost every day. The total score ranges from 0 to 27, with ≥ 5 indicating mild depression, ≥ 14 indicating moderate depression, and ≥ 20 indicating severe depression. In this study, the Cronbach’s α coefficient of the scale was 0.711.
Anxiety
The Generalized Anxiety Disorder-7 was compiled by Spitzer et al61 Translated and localized by Xiaoyan He et al62 The scale contains seven items to assess the anxiety status of individuals in the 2 weeks before the survey. Each item has four options (0, 1, 2, and 3), where 0 represents never and 3 represents almost every day. The total score is 0–21 points, where ≥ 5 points represents mild anxiety, ≥ 10 points represents moderate anxiety, and ≥ 15 points represents severe anxiety. In this study, the Cronbach’s α coefficient of the scale was 0.728.
Procedure
This study employed both electronic and paper-based questionnaires. The electronic questionnaire was used to investigate the general information, sleep quality, and the anxiety and depressive symptoms of patients with hypertension. The paper-based questionnaire was used to investigate the cognitive function of patients. We chose qualified designers to design the questionnaire, who fully understood the purpose and theme of the survey, and strictly implemented the correct design procedures. The questionnaires were distributed and collected by investigators who had received standardized training. The questionnaire items were explained uniformly before filling in the questionnaires to ensure consistency. The purpose of the survey was explained to make the subjects fully understand and voluntarily participate in the survey to reduce the nonresponse bias. The data collection mainly requires filling of the electronic questionnaire and is supplemented by the paper questionnaire. To ensure the integrity of the electronic questionnaire responses, it can only be submitted after all the items have been completed. The paper questionnaires were collected on the spot after completion, and the investigators checked whether there were any omissions or wrong options. If there were any, they were returned to the patients promptly for reconfirmation. The data were then entered after two people verified it.
Statistical Analysis
SPSS 27.0 software was used for the statistical analysis of the data. Harman’s single-factor test was used to analyze the common method bias of the data. Continuous variables that did not conform to the normal distribution were expressed as quartiles [M (P25, P75)], and categorical variables were expressed as n (%). Spearman correlation analysis was used to analyze the correlation between sleep quality, cognitive function, anxiety, and depression. The structural equation model was constructed by AMOS 26.0 software, and the mediating effect of the model was verified by Bootstrap. Gender, age, and education level were included as control variables. P < 0.05 was considered statistically significant. The models’ goodness of fit was evaluated using the following criteria: minimum discrepancy function based on Chi–squared divided by degrees of freedom (χ2/df) (< 3 good, < 5 acceptable), goodness of fit index (GFI) > 0.80, adjusted goodness of fit index (AGFI) > 0.80, comparative fit index (CFI) > 0.80, incremental fit index (IFI) > 0.80, Tucker–Lewis index (TLI) > 0.80, and root mean square error of approximation (RMSEA) < 0.08.63
Results
Basic Characteristics of the Study Participants
A total of 325 people were surveyed, including 133 males (40.92%) and 192 females (59.08%), 240 people (73.85%) were aged 60 years or above, 167 people (51.38%) had a primary school education or below, 290 people (89.23%) were married, and 290 people (89.23%) were living with others. The body mass index (BMI) classification showed that 112 people had a normal weight, accounting for 34.46%; 128 people were overweight, accounting for 39.38%; and 79 people were obese, accounting for 24.31%. See Table 1.
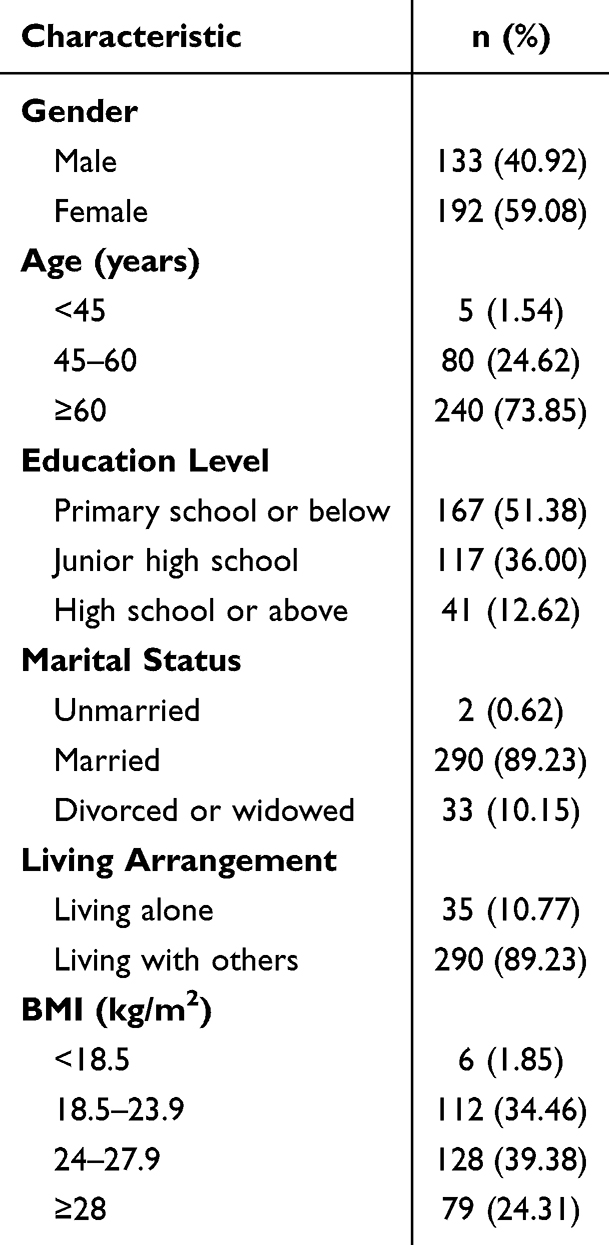 |
Table 1 Basic Characteristics of Patients with Hypertension in Daning County and Yonghe County, 2024 (N = 325) |
Scores of Sleep Quality, Cognitive Function, Anxiety, and Depression of Patients with Hypertension
The score of sleep quality of patients with hypertension was 7.0 (4.0, 8.0); the cognitive function score was 19.0 (15.0, 25.0); the anxiety score was 2.0 (0.0, 4.0); and the depression score was 3.0 (2.0, 5.0). For details on the dimensions and total scores of each scale, see Table 2.
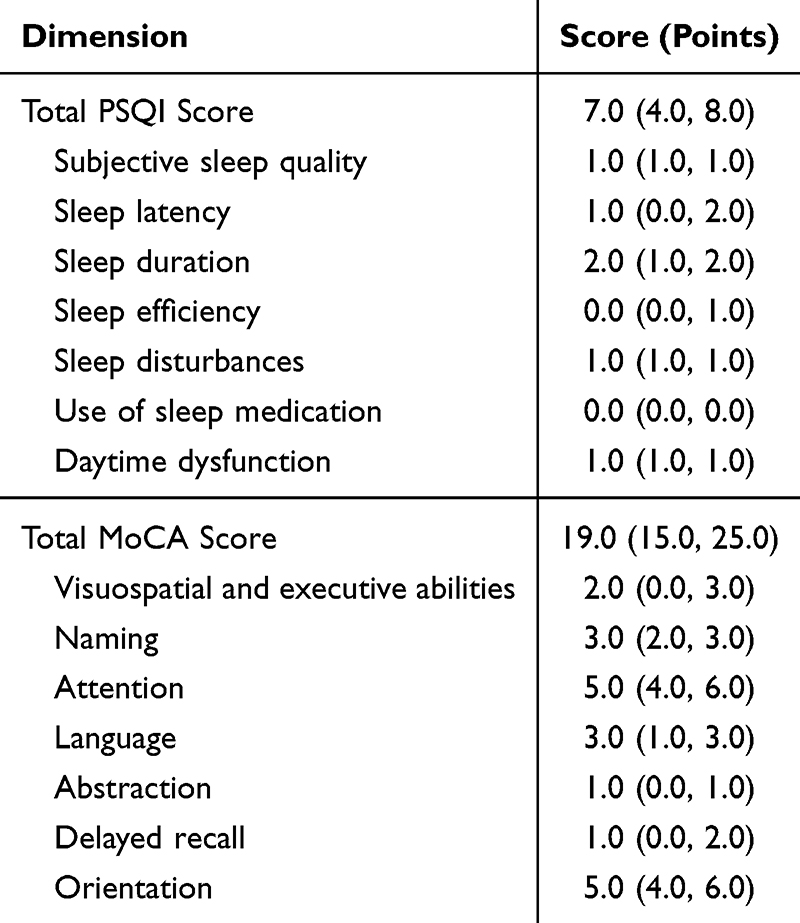 |
Table 2 PSQI and MoCA Scores in Patients with Hypertension [M (P25, P75)] |
Correlation Analysis of Sleep Quality, Cognitive Function, Anxiety, and Depression in Patients with Hypertension
Spearman correlation analysis showed that (1) the total score of sleep quality in patients with hypertension was positively correlated with the total score of anxiety (r = 0.280, P < 0.01), positively correlated with the total score of depression (r = 0.337, P < 0.01), and negatively correlated with the total score of cognitive function (r = −0.219, P < 0.01); (2) the total score of anxiety was positively correlated with the total score of depression (r = 0.711, P < 0.01) and negatively correlated with the total score of cognitive function (r = −0.303, P < 0.01); and (3) the total score of depression was negatively correlated with the total score of cognitive function (r = −0.292, P < 0.01). (Table 3).
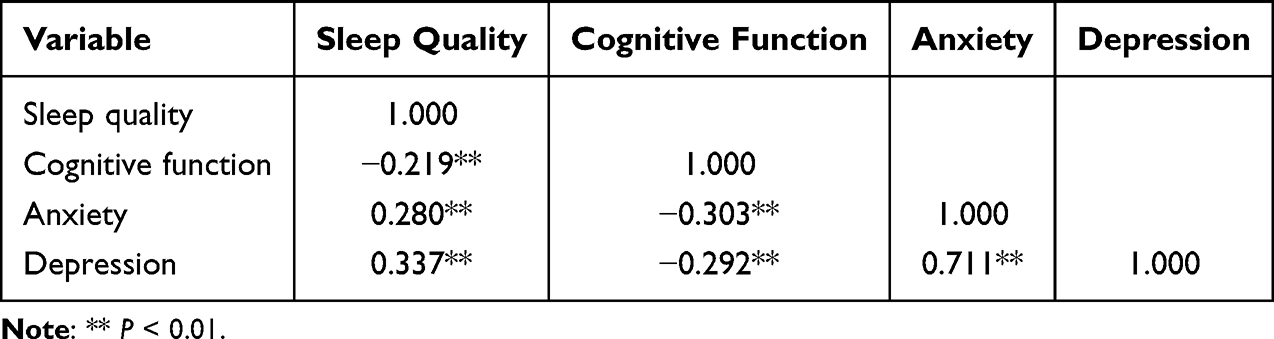 |
Table 3 Correlations Among Total Scores of Sleep Quality, Cognitive Function, Anxiety, and Depression in Patients with Hypertension (r Values) |
The Mediating Effects of Anxiety and Depression Between Sleep Quality and Cognitive Function in Patients with Hypertension
Bias Validation
Harman’s single-factor test was used to verify the common factor deviation. When the factor was not rotated, 11 characteristic root factors were > 1. The first factor could explain 17.46% of the variation. Since this was lower than the critical value standard of 40.00%, it indicates that there was no obvious common method deviation in the variables of this study.
Chain Mediating Effect of Anxiety and Depression
AMOS 26.0 was used for the analysis of mediation effects, with cognitive function as the dependent variable, sleep quality as the independent variable, and anxiety and depression as the mediating variables. The bootstrap method was used to draw samples 5000 times, and the maximum likelihood method was used to construct the structural equation model. When the 95% CI did not contain 0, the mediation effect was established. The chain mediating effect model of anxiety and depression showed that the fitting indexes met the relevant evaluation criteria: χ2/df = 2.371, GFI = 0.907, AGFI = 0.870, CFI = 0.881, IFI = 0.884, TLI = 0.850, and RMSEA = 0.065. The standardized path coefficients of the final model are shown in Figure 1.
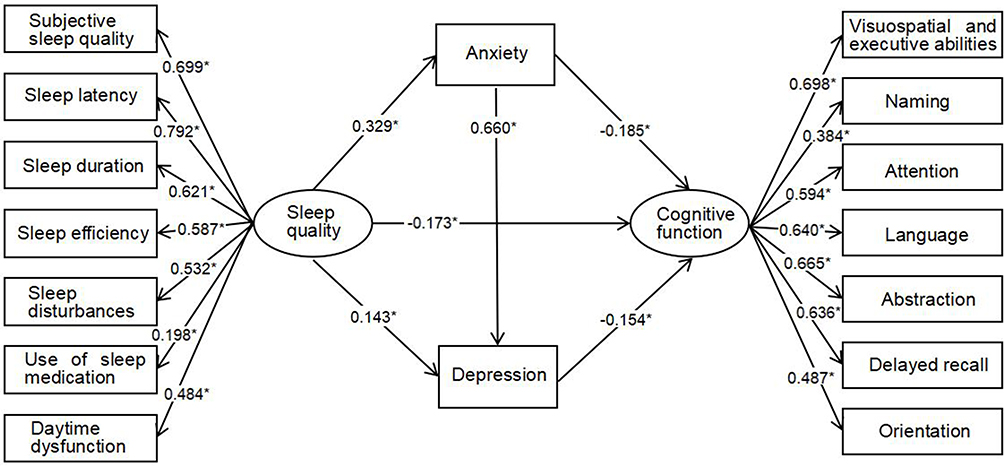 |
Figure 1 Direct and indirect relationships across sleep quality, cognitive function, anxiety and depression. The figure underscores the significant mediating effects of anxiety and depression on the relationship between sleep quality and cognitive function. Note: All the path coefficients were standardized. *P < 0.05. |
After controlling for gender, age, and education level, the chain mediation path coefficients of anxiety and depression between sleep quality and cognitive function showed (see Table 4) that all path coefficients were statistically significant (P < 0.05) and that the 95% CI did not include 0. Sleep quality in patients with hypertension was associated with cognitive function (path 1), with an association value of −0.544, accounting for 59.85% of the total association. Anxiety symptoms in patients with hypertension showed a mediating role between sleep quality and cognitive function, with an effect value of −0.190, accounting for 20.90% of the total association (path 2). Depressive symptoms in patients with hypertension showed a mediating role between sleep quality and cognitive function, with an effect value of −0.069, accounting for 7.59% of the total association (path 3). The chain mediating effect of anxiety and depression symptoms in patients with hypertension between sleep quality and cognitive function was −0.105, accounting for 11.55% of the total association (path 4). The total indirect association was −0.365, accounting for 40.15% of the total association. Total association = −0.909. The 95% CI of the above mediating effects did not include 0; hence, the mediating roles of anxiety and depression, and the chain mediating effect were all observed. (see Table 5).
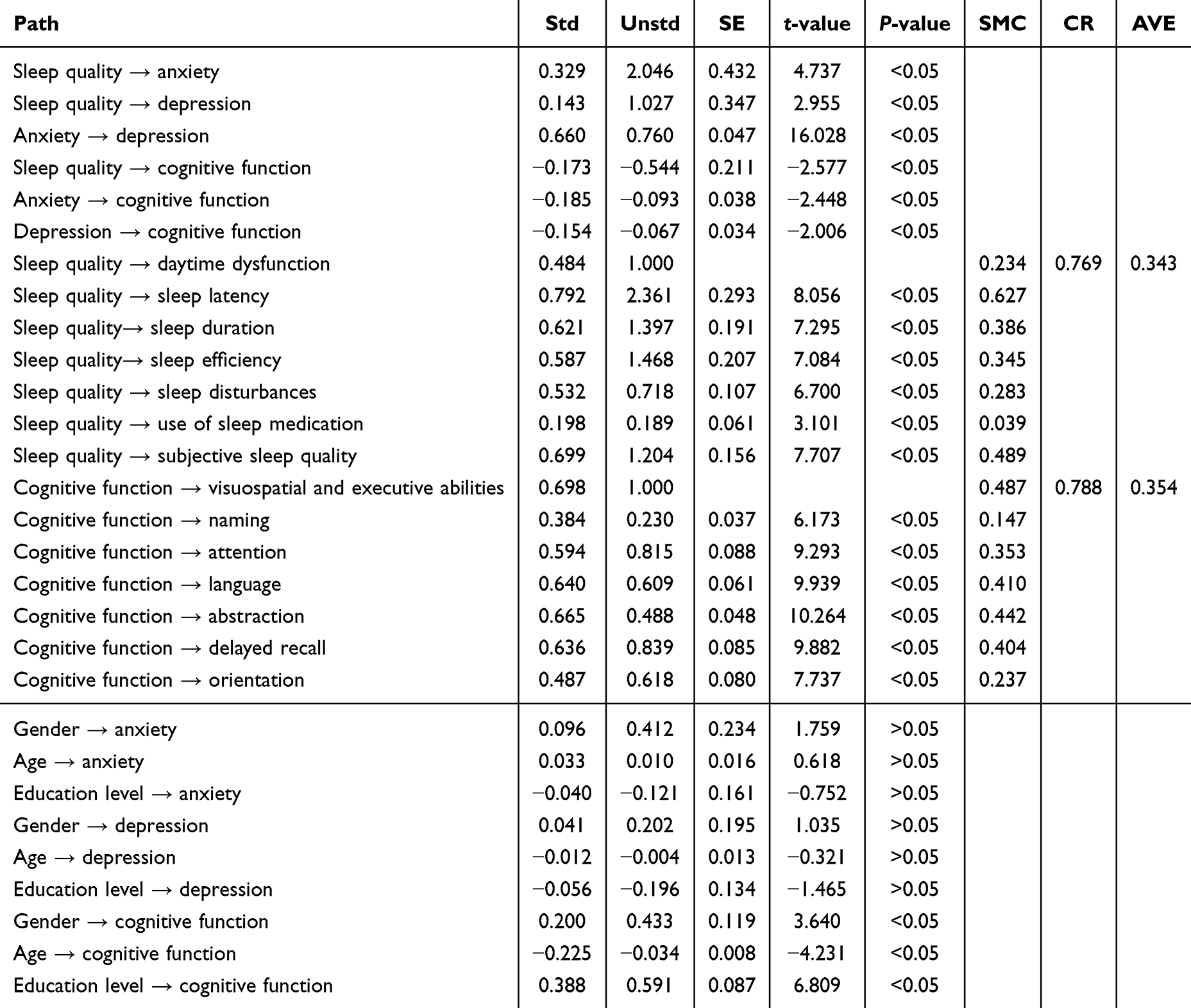 |
Table 4 Chain Mediation Path Coefficients of Anxiety and Depression in Patients with Hypertension |
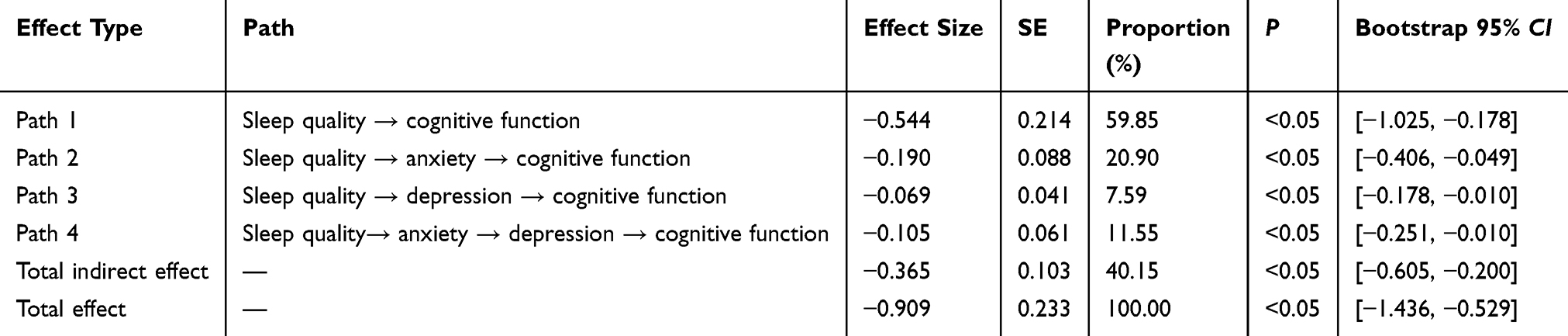 |
Table 5 Chain Mediating Effects of Anxiety and Depression in Patients with Hypertension |
Discussion
This study examined the roles of anxiety and depression in the relationship between sleep quality and cognitive function in patients with hypertension in rural areas of Shanxi Province, China. The chain mediation effect analysis showed that anxiety and depression had a mediating effect between sleep quality and cognitive function in patients with hypertension. Consequently, our findings validated the hypotheses we initially proposed.
Hypertension may contribute to cerebral small vessel disease, such as white matter lesions, microbleeds, and brain atrophy, which in turn affect cognitive function. Long-term hypertension is associated with insufficient cerebral blood perfusion, impairing normal brain metabolism and function.64 Hypertension may further trigger inflammatory responses, releasing inflammatory factors that damage neurons and affect cognitive abilities.65 A study indicates that cognitive decline following the onset of hypertension gradually accelerates over subsequent years. This suggests that the cumulative effect of hypertension on brain function is progressive, with prolonged exposure being associated with more severe CogI.66 Compared to the general population, people with hypertension are more susceptible to CogI.67,68
The chain mediation effect refers to any indirect influence mechanisms whereby independent variables affect dependent variables through multiple interrelated mediating variables. It reveals sequential transmission pathways among variables, not just the direct action of a single mediator. This study explored the mediating effect of anxiety and depression symptoms in patients with hypertension on sleep quality and cognitive function, thereby uncovering the underlying mechanisms through which sleep quality is associated with cognitive function in this population.
Our findings confirmed that poor sleep quality is associated with CogI in patients with hypertension, consistent with previous research.69,70 Sleep can replenish the body’s energy, enhance its resistance, and promote the body’s normal growth and development. It plays an extremely important role in maintaining the body’s normal psychological activities and preserving good mental health.71 Poor sleep quality, especially low sleep efficiency and short nighttime sleep duration, was associated with fatigue and excessive daytime sleepiness, which were associated with cognitive decline.72 Biomarker analysis showed that long-term sleep deprivation was associated with increased neuronal activity and excessive production and deposition of soluble β-amyloid protein that were associated with AD.73 Poor sleep quality was associated with elevated cortisol, tissue damage, and neuroinflammation in the brain,74 which in turn affects the hippocampus and impairs learning and memory,75 and was associated with cognitive decline.
This study confirmed that anxiety and depression play a mediating role between sleep quality and cognitive function in patients with hypertension. A previous study showed that the level of insomnia in patients with hypertension was higher than that in normotensives, and that the proportion of anxiety and depression in the insomnia group was much higher than that in the normal sleep group, which indicated that patients with hypertension and poor sleep quality were more likely to have anxiety and depression symptoms.76 Several studies have confirmed that there is a close relationship between sleep disorders, anxiety, and depression in patients with hypertension,77,78 which may be related to the abnormal overlap of neurotransmitters and brain structures in the sleep–wake cycle, anxiety, and depression.79 Good sleep quality can promote emotional health and prevent the development of mental disorders.80 On the contrary, sleep deprivation can have a negative impact on people’s emotions, cognition, and daily functions and increase the risk of anxiety and depression.81 Furthermore, anxiety and depression symptoms are markedly associated with CogI. Anxiety is associated with a decline in one’s working memory82 and the ability to recognize one’s emotions, and depression can damage patients’ attention, executive function, memory, and other cognitive fields.83 A study has shown that poor sleep quality may affect cognitive function, especially in people with higher levels of depression.84 A survey of rural elderly people in Guizhou Province, Xiong Yan and others found that depression may be an important mediating factor between sleep quality and cognitive function, and the mediating effect of depression (64.94%) is greater than the direct effect of sleep quality (35.06%).85 Given the mediating effect of anxiety and depression between sleep quality and cognitive function, improving sleep quality in patients with hypertension can help alleviate anxiety and depressive symptoms, thereby slowing the rate of cognitive decline.
This study confirmed the chain mediating role of anxiety and depression on sleep quality and cognitive function in patients with hypertension. A previous study has shown that poor sleep quality was associated with fatigue and excessive daytime sleepiness, which can increase anxiety levels. Slow-wave sleep and rapid eye movement sleep disturbances were associated with increased daytime fatigue and a reduced ability to relieve stress.86 In addition, when patients with hypertension are anxious, the sympathetic nervous system in the body is overexcited, leading to an increase in the secretion of catecholamines such as adrenaline and norepinephrine. These substances further increase blood pressure and affect the limbic system of the brain and the hypothalamic–pituitary–adrenal axis, which in turn affects mood regulation and increases the risk of depression.87,88 In addition, individuals with anxiety often exhibit excessive worry about the future and fear of uncertainty. This negative cognitive pattern was associated with pessimistic interpretations of life events, intensifying low mood and triggering depression.89 Depressive symptoms were associated with hippocampal atrophy, which in turn impairs memory function. Depressive symptoms were also associated with a decline in cognitive function and an accelerated rate of cognitive decline.90,91 A study found that depressive symptoms in patients with hypertension were markedly associated with cognitive decline, and the more severe the depressive symptoms, the greater the risk of cognitive decline.92 A growing body of prospective evidence suggests that depression is an important risk factor in the development of dementia in the future.93
Furthermore, the observed serial pathway from sleep quality through anxiety to depression and ultimately cognitive function may be underpinned by two interconnected biological mechanisms: circadian rhythm dysregulation and glymphatic system dysfunction. First, circadian disruption is intimately linked to both sleep disturbance and affective disorders. Dysregulated circadian rhythms alter cortisol secretion patterns and monoaminergic neurotransmission, precipitating anxiety symptoms that, when chronic, progress to depressive states—consistent with our serial mediation model.94 This circadian perspective suggests that sleep problems in hypertensive patients may indicate broader chronobiological misalignment with treatment implications (eg, timed light exposure, chronotherapeutic interventions). Second, sleep serves as the principal modulator of the glymphatic system, which clears metabolic waste and supports neuronal homeostasis. Emerging evidence indicates that glymphatic dysfunction constitutes a transdiagnostic mechanism connecting sleep disturbance, psychiatric symptoms, and cognitive impairment.95 Specifically, inadequate sleep compromises glymphatic clearance, promoting neuroinflammation and synaptic dysfunction that manifests as anxiety and depressive symptoms, with cumulative effects on cognitive performance. This framework aligns with our finding that anxiety and depression sequentially transmit sleep quality effects to cognition and underscores the need for longitudinal studies to establish causal directions.
Adequate sleep is essential for improving cognitive function and mental health. Many studies have advocated for greater cooperation between sleep specialists, neurologists, clinicians, nurses, and rehabilitation specialists to expand the understanding of this field and bring peaceful sleep to patients with hypertension. The current research results remind clinicians to pay attention to possible sleep and psychological problems when receiving patients with CogI. Researchers can consider interventions in sleep and psychology when solving for subjective cognitive problems in the future. At the same time, it is suggested that the optimization direction of the management of patients with hypertension in rural areas should shift from linear intervention to system construction, especially the need to build a mental health cultivation mechanism and strengthen the management of psychological problems.
Limitations and Future Directions
This study has several limitations that point to directions for future research. First, this study adopted a cross-sectional design, and the mediating effects observed through structural equation modeling cannot confirm the causal relationships between the variables. Future longitudinal studies can be conducted to verify the proposed causal pathways. Second, unmeasured variables (such as the duration of hypertension, medication usage, or other comorbidities) may act as confounding factors that could affect the observed associations. In the future, potential confounding factors can be comprehensively assessed to minimize their impact as much as possible. Third, the sample for this study was drawn from rural areas in two counties of Shanxi Province. Although selected from counties designated as nationally impoverished by China’s National Health Commission, it can to some extent reflect living conditions in similar regions. However, this selection may limit the applicability of our results to urban populations or other geographic regions with different socioeconomic characteristics. Rural residents in Shanxi may have distinct health behaviors, healthcare access, and lifestyle patterns compared to their urban counterparts or populations in other provinces. Future research should therefore validate these results in diverse settings, including urban areas and other provinces, to enhance the generalizability of the conclusions. Fourth, the standard MoCA education correction (one point for ≤ 12 years) may underestimate cognitive function in a rural population with predominantly low education. Caution is needed when generalizing these cognitive scores. Future research can establish cognitive test standards based on rural populations, rather than relying on standard correction methods designed for urban or higher education samples, in order to accommodate the educational level of rural populations. Finally, this study primarily relies on self-report questionnaires, lacking support from objective neuroimaging or biological indicators, which may lead to recall bias. Future studies can reduce recall bias by increasing objective measurement tools such as physiological index measurement and behavior monitoring and by connecting with the electronic medical record system of hospitals or the health record system of village health rooms.
Conclusion
These findings suggest that sleep quality in patients with hypertension is associated with cognitive function and that anxiety and depression play a chain mediating role in the relationship between sleep quality and cognitive function, thereby underscoring the necessity of improving sleep quality and mitigating anxiety and depression as potential strategies for addressing cognitive deterioration. It is also of great importance for screening and comprehensive management of sleep and mental health in hypertension care.
Ethics Approval
This study complies with the ethical principles outlined in the Declaration of Helsinki. All study procedures were approved by the Ethics Committee of Shanxi Medical University (Approval No: 2020SLL201). All study participants received informed consent.
Acknowledgments
We thank all the participants and staff at the study sites for their painstaking efforts in conducting the data collection.
Funding
This study was supported by the China-Gates Foundation Rural Basic Healthcare Project (Shanxi Sub-Project, No. PHC-I04), Open Fund from Key Laboratory of Cellular Physiology (Shanxi Medical University), Ministry of Education, China (No. CELLPHYSIOL/SXMU-2021-16), Provincial Application Basis Research Plan of Shanxi under Grant (No. 201801D121314), Shanxi Province Higher Education Billion Project Science and Technology Guidance Project and Shanxi Provincial Traditional Chinese Medicine (TCM) Research Project (No. 2024ZYY2D022).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Committee CHPaTGR, Alliance H, Care HBotCAfIEoMaH. Chinese hypertension prevention and treatment guidelines (2024 revised edition). Chin J Hypertens. 2024;32(07):603–16.
2. (NCD-RisC) NRFC. Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: a pooled analysis of 1201 population-representative studies with 104 million participants. Lancet. 2021;398(10304):957–980. doi:10.1016/S0140-6736(21)01330-1
3. Wang Z, Chen Z, Zhang L, et al. Status of hypertension in China: results from the china hypertension survey, 2012-2015. Circulation. 2018;137(22):2344–2356. doi:10.1161/CIRCULATIONAHA.117.032380
4. Zhang M, Wu J, Zhang X, et al. Prevalence and control of hypertension in adults in China, 2018. Zhonghua liu xing bing xue za zhi. 2021;42(10):1780–1789. doi:10.3760/cma.j.cn112338-20210508-00379
5. Center For Cardiovascular Diseases The Writing Committee of the Report on Cardiovascular H, Diseases In China N. Report on cardiovascular health and diseases in China 2024: an updated summary. Chin Circulation J. 2025;40(06):521–559.
6. Ou YN, Tan CC, Shen XN, et al. Blood pressure and risks of cognitive impairment and dementia: a systematic review and meta-analysis of 209 prospective studies. Hypertension. 2020;76(1):217–225. doi:10.1161/HYPERTENSIONAHA.120.14993
7. Mills KT, Stefanescu A, He J. The global epidemiology of hypertension. Nat Rev Nephrol. 2020;16(4):223–237. doi:10.1038/s41581-019-0244-2
8. Varatharajah Y, Ramanan VK, Iyer R, Vemuri P. Predicting short-term MCI-to-AD progression using imaging, CSF, genetic factors, cognitive resilience, and demographics. Sci Rep. 2019;9(1):2235. doi:10.1038/s41598-019-38793-3
9. Qin J, He Z, Wu L, et al. Prevalence of mild cognitive impairment in patients with hypertension: a systematic review and meta-analysis. Hypertension Res. 2021;44(10):1251–1260. doi:10.1038/s41440-021-00704-3
10. Guan D, Lewis MO, Li P, et al. Incremental burden on health-related quality of life, health service utilization and direct medical expenditures associated with cognitive impairment among non-institutionalized people with diabetes aged 65 years and older. Diabetes Obesity Metab. 2024;26(1):275–282. doi:10.1111/dom.15313
11. Xie C, Zhong D, Zhang Y, et al. Prevalence and risk factors of cognitive impairment in Chinese patients with hypertension: a systematic review and meta-analysis. Front Neurol. 2023;14:1271437. doi:10.3389/fneur.2023.1271437
12. Selby EA, Joiner TE. Cascades of emotion: the emergence of borderline personality disorder from emotional and behavioral dysregulation. Rev General Psychol. 2009;13(3):219. doi:10.1037/a0015687
13. Zhao J, Yang X. A review of theoretical studies on non-suicidal self-injurious behavior in adolescents and related qualitative research progresses. Adv Soc Sci. 2024;13(6):10. doi:10.12677/ass.2024.136548
14. Selby EA, Kondratyuk S, Lindqvist J, Fehling K, Kranzler A. Temporal Bayesian network modeling approach to evaluating the emotional cascade model of borderline personality disorder. Personality Disord. 2021;12(1):39–50. doi:10.1037/per0000398
15. Jungmann SM, Vollmer N, Selby EA, Witthöft M. Understanding dysregulated behaviors and compulsions: an extension of the emotional cascade model and the mediating role of intrusive thoughts. Front Psychol. 2016;7:994. doi:10.3389/fpsyg.2016.00994
16. Liu RQ, Qian Z, Trevathan E, et al. Poor sleep quality associated with high risk of hypertension and elevated blood pressure in China: results from a large population-based study. Hypertension Res. 2016;39(1):54–59. doi:10.1038/hr.2015.98
17. Fogg C, Meredith P, Culliford D, Bridges J, Spice C, Griffiths P. Cognitive impairment is independently associated with mortality, extended hospital stays and early readmission of older people with emergency hospital admissions: a retrospective cohort study. Int J Nurs Stud. 2019;96:1–8. doi:10.1016/j.ijnurstu.2019.02.005
18. Parati G, Pengo MF, Avolio A, et al. Nocturnal blood pressure: pathophysiology, measurement and clinical implications. position paper of the European society of hypertension. J Hypertension. 2025;43(8):1296–1318. doi:10.1097/HJH.0000000000004053
19. Tomitani N, Hoshide S, Kario K. Sleep and hypertension - up to date 2024. Hypertension Res. 2024;47(12):3356–3362. doi:10.1038/s41440-024-01845-x
20. Li L, Li L, Chai JX, et al. Prevalence of poor sleep quality in patients with hypertension in China: a meta-analysis of comparative studies and epidemiological surveys. Front Psychiatry. 2020;11:591. doi:10.3389/fpsyt.2020.00591
21. Punton G, Ellis JG, Jensen E, et al. The effects of acute sleep deprivation on cognitive control mechanisms associated with hallucinatory experiences. J Sleep Res. 2025:e70259. doi:10.1111/jsr.70259
22. Renn RP, Cote KA. Performance monitoring following total sleep deprivation: effects of task type and error rate. Int J Psychophysiol. 2013;88(1):64–73. doi:10.1016/j.ijpsycho.2013.01.013
23. Carvalho DZ, Kolla BP, McCarter SJ, et al. Associations of chronic insomnia, longitudinal cognitive outcomes, amyloid-PET, and white matter changes in cognitively normal older adults. Neurology. 2025;105(7):e214155. doi:10.1212/WNL.0000000000214155
24. Aktan Süzgün M, Tang Q, Stefani A. Sleep abnormalities and risk of Alzheimer’s disease. Curr Neurol Neurosci Rep. 2025;25(1):67. doi:10.1007/s11910-025-01451-5
25. Smith L, Shin JI, Jacob L, et al. Sleep problems and mild cognitive impairment among adults aged ≥50 years from low- and middle-income countries. Exp Gerontol. 2021;154:111513. doi:10.1016/j.exger.2021.111513
26. Palmer K, Mitolo M, Burgio F, Meneghello F, Venneri A. Sleep disturbance in mild cognitive impairment and association with cognitive functioning. a case-control study. Front Aging Neurosci. 2018;10:360. doi:10.3389/fnagi.2018.00360
27. Gonzales PNG, Villaraza SG, Rosa JCD. The association between sleep and Alzheimer’s disease: a systematic review. Dementia Neuropsychol. 2024;18:e20230049. doi:10.1590/1980-5764-dn-2023-0049
28. Wang P, Xie C, Qian J, et al. Dysfunctional sleep beliefs and sleep quality among Chinese university students: the mediating roles of depression, anxiety, and stress. BMC Psychol. 2025;13(1):844. doi:10.1186/s40359-025-03210-0
29. Shen Y, Zhu S, Liao S, et al. Generalized anxiety disorder patients’ cognitive control in affective contexts. Front Psychiatry. 2025;16:1506239. doi:10.3389/fpsyt.2025.1506239
30. Dressle RJ, Feige B, Spiegelhalder K, et al. HPA axis activity in patients with chronic insomnia: a systematic review and meta-analysis of case-control studies. Sleep Med Rev. 2022;62:101588. doi:10.1016/j.smrv.2022.101588
31. Tang B, Hu Y, Xu C, Wang N, Li Y, Li J. Analysis of the correlation between physical activity level, sleep quality, and anxiety levels in middle-aged and older adults: a cross-sectional study. Front Public Health. 2025;13:1629695. doi:10.3389/fpubh.2025.1629695
32. Durdurak BB, Morales-Muñoz I, de Cates AN, Wiseman C, Broome MR, Marwaha S. Underlying biological mechanisms of emotion dysregulation in bipolar disorder. Front Psychiatry. 2025;16:1552992. doi:10.3389/fpsyt.2025.1552992
33. Zhao H, Si F, Meng H, et al. Threat context impairs cognitive control of neutral words processing in social anxiety individuals: evidence from ERP and theta oscillations. BMC Neuro. 2025;26(1):54. doi:10.1186/s12868-025-00976-2
34. Ampofo J, Sun B, Bentum-Micah G, et al. Investigating the impact of sleep quality on cognitive functions among students in Tokyo, Japan, and London, UK. Front Sleep. 2025;4:1537997. doi:10.3389/frsle.2025.1537997
35. Wilson JM, Meints SM, Edwards RR, Yamin JB, Moore DJ. The role of sleep disturbance in reduced accuracy on a divided attention task among patients with fibromyalgia. Pain Reports. 2024;9(1):e1. doi:10.1097/PR9.0000000000001122
36. Yin CY, Zhang HL, Liu L, et al. Immediate improvement in anxiety and sleep quality with delayed depression response after bariatric surgery in a longitudinal cohort study. Sci Rep. 2025;15(1):32973. doi:10.1038/s41598-025-17358-7
37. Singh A, Soni R, Kaloiya GS, et al. Association of poor sleep efficiency with decreased executive function and impaired episodic memory in older adults. Cureus. 2025;17(8):e90061. doi:10.7759/cureus.90061
38. Zhang J, Ou J, Lu X, et al. Sleep disorders and the risk of cognitive decline or dementia: an updated systematic review and meta-analysis of longitudinal studies. J Neurol. 2025;272(10):689. doi:10.1007/s00415-025-13372-x
39. Tu Q, Lin S, Hafiz N, et al. Independent and joint associations of hypertension and depression with cardiovascular diseases and all-cause mortality: a population-based cohort study. J Human Hypertens. 2025;39(9):634–642. doi:10.1038/s41371-025-01045-1
40. Tamm S, Jernelöv S, Forsell E, et al. Objectively measured cognitive function in insomnia patients with and without comorbid depression treated with cognitive behavioral therapy for insomnia. BMC Psychiatry. 2025;25(1):916. doi:10.1186/s12888-025-07460-5
41. Li C, Wu X, Li Y, et al. Association between sleep duration, depression and cognitive decline trajectories: findings from a prospective cohort study in China. BMC Psychiatry. 2025;25(1):907. doi:10.1186/s12888-025-07387-x
42. Irwin MR, Boyle CC, Cho JH, et al. Inflammatory exposure and depression in older adults with insomnia: a randomized clinical trial. JAMA psychiatry. 2025;82(9):859–867. doi:10.1001/jamapsychiatry.2025.1327
43. Shimada H, Park H, Makizako H, Doi T, Lee S, Suzuki T. Depressive symptoms and cognitive performance in older adults. J Psychiatr Res. 2014;57:149–156. doi:10.1016/j.jpsychires.2014.06.004
44. Maffoni M, Magnani A, Pierobon A, et al. Executive functions and subjective cognitive decline: the moderating role of depressive symptoms. Diagnostics. 2025;15(24). doi:10.3390/diagnostics15243164
45. Naismith SL, Rogers NL, Lewis SJ, et al. Sleep disturbance relates to neuropsychological functioning in late-life depression. J Affect Disord. 2011;132(1–2):139–145. doi:10.1016/j.jad.2011.02.027
46. Minkel JD, McNealy K, Gianaros PJ, et al. Sleep quality and neural circuit function supporting emotion regulation. Biol Mood Anxiety Disord. 2012;2(1):22. doi:10.1186/2045-5380-2-22
47. Xu WQ, Lin LH, Ding KR, et al. The role of depression and anxiety in the relationship between poor sleep quality and subjective cognitive decline in Chinese elderly: exploring parallel, serial, and moderated mediation. J Affect Disord. 2021;294:464–471. doi:10.1016/j.jad.2021.07.063
48. Thapar A, Collishaw S, Pine DS, Thapar AK. Depression in adolescence. Lancet. 2012;379(9820):1056–1067. doi:10.1016/S0140-6736(11)60871-4
49. Moffitt TE, Harrington H, Caspi A, et al. Depression and generalized anxiety disorder: cumulative and sequential comorbidity in a birth cohort followed prospectively to age 32 years. Arch Gen Psychiatry. 2007;64(6):651–660. doi:10.1001/archpsyc.64.6.651
50. Suddell S, Mahedy L, Skirrow C, Penton-Voak IS, Munafo MR, Wootton RE. Cognitive functioning in anxiety and depression: results from the ALSPAC cohort. 2021.
51. Hammar Å, Ronold EH, Rekkedal G. Cognitive impairment and neurocognitive profiles in major depression-a clinical perspective. Front Psychiatry. 2022;13:764374. doi:10.3389/fpsyt.2022.764374
52. Molendijk ML, Spinhoven P, Polak M, Bus BA, Penninx BW, Elzinga BM. Serum BDNF concentrations as peripheral manifestations of depression: evidence from a systematic review and meta-analyses on 179 associations (N=9484). Mol Psychiatry. 2014;19(7):791–800. doi:10.1038/mp.2013.105
53. Pearson O, Uglik-Marucha N, Miskowiak KW, et al. The relationship between sleep disturbance and cognitive impairment in mood disorders: a systematic review. J Affect Disord. 2023;327:207–216. doi:10.1016/j.jad.2023.01.114
54. Parra-Díaz AB, Aibar-Almazán A, Martínez-Amat A, Jiménez-García JD, Álvarez-Salvago F, Hita-Contreras F. Associations of sleep quality, anxiety, and depression with cognitive and executive functions among community-dwelling women aged ≥ 65 years: a cross-sectional study. Healthcare. 2021;9(11). doi:10.3390/healthcare9111599
55. Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh sleep quality index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. doi:10.1016/0165-1781(89)90047-4
56. Liu X, Tang M, Hu L, Wang A. Study on the reliability and validity of the Pittsburgh Sleep Quality Index. Chin J Psychiatry. 1996;29(02):103–107.
57. Nasreddine ZS, Phillips NA, Bédirian V, et al. The montreal cognitive assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 2005;53(4):695–699. doi:10.1111/j.1532-5415.2005.53221.x
58. Wang W, Wang L. Application of montreal cognitive assessment scale in screening patients with mild cognitive impairment. Chin J Intern Med. 2007;46(05):414–416.
59. Lichtman JH, Bigger JT, Blumenthal JA, et al. Depression and coronary heart disease: recommendations for screening, referral, and treatment: a science advisory from the American heart association prevention committee of the council on cardiovascular nursing, council on clinical cardiology, council on epidemiology and prevention, and interdisciplinary council on quality of care and outcomes research: endorsed by the American psychiatric association. Circulation. 2008;118(17):1768–1775. doi:10.1161/CIRCULATIONAHA.108.190769
60. Feng Y, Huang W, Tian T, Geng Y. Application of the Chinese version of the patient health questionnaire depression scale (PHQ-9) and PHQ-2 in inpatients with depressive episodes. 2015.
61. Spitzer RL, Kroenke K, Williams JB, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Archiv Internal Med. 2006;166(10):1092–1097. doi:10.1001/archinte.166.10.1092
62. He X, Li C, Qian J, Cui H. Reliability and validity of a generalized anxiety disorder scale in general hospital outpatients. Shanghai Arch Psychiatry. 2010;22(4):4.
63. West SG, Taylor AB, Wu WJ. Model fit and model selection in structural equation modeling. Handb Struct Equat Model. 2012;1(1):209–231.
64. Wei W, Ma D, Li L, Zhang L. Cognitive impairment in cerebral small vessel disease induced by hypertension. Neural Regeneration Res. 2024;19(7):1454–1462. doi:10.4103/1673-5374.385841
65. Wang J, Wang H, Sun JJBS. Advances in neuroinflammation. Brain Sci. 2024;14:965.
66. Zhu S, Bo J, Xia T, Gu X. Temporal patterns of cognitive decline after hypertension onset among middle-aged and older adults in China. Sci Rep. 2025;15(1):16300. doi:10.1038/s41598-025-98267-7
67. Bao J, Liu J, Li Z, et al. Relationship between hypertension and cognitive function in an elderly population: a population-based study in Rural Northern China. Front Neurol. 2022;13:885598. doi:10.3389/fneur.2022.885598
68. Suvvari TK. Exploring the association between hypertension and cognitive impairment: evidence-based insights. Chronic Dis Transl Med. 2024;10(2):153–155. doi:10.1002/cdt3.95
69. Zhuo X, Huang M, Wu M. Analysis of cognitive dysfunction and its risk factors in patients with hypertension. Medicine. 2022;101(10):e28934. doi:10.1097/MD.0000000000028934
70. Lv S, Jiao H, Zhong X, et al. Association between sleep quality and cognitive impairment in older adults hypertensive patients in China: a case-control study. Front Public Health. 2024;12:1446781. doi:10.3389/fpubh.2024.1446781
71. Hu M, Shu X, Feng H, Xiao LD. Sleep, inflammation and cognitive function in middle-aged and older adults: a population-based study. J Affect Disord. 2021;284:120–125. doi:10.1016/j.jad.2021.02.013
72. Kong J, Zhou L, Li X, Ren Q. Sleep disorders affect cognitive function in adults: an overview of systematic reviews and meta-analyses. Sleep Biol Rhythms. 2023;21(2):133–142. doi:10.1007/s41105-022-00439-9
73. Jack CR, Bennett DA, Blennow K, et al. NIA-AA research framework: toward a biological definition of Alzheimer’s disease. Alzheimer’s Dementia. 2018;14(4):535–562. doi:10.1016/j.jalz.2018.02.018
74. Herrero Babiloni A, Baril AA, Charlebois-Plante C, et al. The putative role of neuroinflammation in the interaction between traumatic brain injuries, sleep, pain and other neuropsychiatric outcomes: a state-of-the-art review. J Clin Med. 2023;12(5):1793. doi:10.3390/jcm12051793
75. Zhu B, Dong Y, Xu Z, et al. Sleep disturbance induces neuroinflammation and impairment of learning and memory. Neurobiol Dis. 2012;48(3):348–355. doi:10.1016/j.nbd.2012.06.022
76. Kandasamy G, Subramani T, Almanasef M, et al. Mental health and hypertension: assessing the prevalence of anxiety and depression and their associated factors in a tertiary care population. Front Public Health. 2025;13:1545386. doi:10.3389/fpubh.2025.1545386
77. Birhanu TE, Getachew B, Gerbi A, Dereje D. Prevalence of poor sleep quality and its associated factors among hypertensive patients on follow up at Jimma University Medical Center. J Human Hypertens. 2021;35(1):94–100. doi:10.1038/s41371-020-0320-x
78. Liu C, Ye Z, Chen L, et al. Interaction effects between sleep-related disorders and depression on hypertension among adults: a cross-sectional study. BMC Psychiatry. 2024;24(1):482. doi:10.1186/s12888-024-05931-9
79. Peng C, Wang K, Wang J, et al. Neural correlates of insomnia with depression and anxiety from a neuroimaging perspective: a systematic review. Sleep Med Rev. 2025;81:102093. doi:10.1016/j.smrv.2025.102093
80. Baranwal N, Yu PK, Siegel NS. Sleep physiology, pathophysiology, and sleep hygiene. Prog Cardiovasc Dis. 2023;77:59–69. doi:10.1016/j.pcad.2023.02.005
81. Fang H, Tu S, Sheng J, Shao A. Depression in sleep disturbance: a review on a bidirectional relationship, mechanisms and treatment. J Cell Mol Med. 2019;23(4):2324–2332. doi:10.1111/jcmm.14170
82. Suddell S, Mahedy L, Skirrow C, Penton-Voak IS, Munafò MR, Wootton RE. Cognitive functioning in anxiety and depression: results from the ALSPAC cohort. Royal Society Open Science. 2023;10(8):221161. doi:10.1098/rsos.221161
83. Rock PL, Roiser JP, Riedel WJ, Blackwell AD. Cognitive impairment in depression: a systematic review and meta-analysis. Psychol Med. 2014;44(10):2029–2040. doi:10.1017/S0033291713002535
84. Sutter C, Zöllig J, Allemand M, Martin M. Sleep quality and cognitive function in healthy old age: the moderating role of subclinical depression. Neuropsychology. 2012;26(6):768–775. doi:10.1037/a0030033
85. Xiong Y, Yang J, Zhou Q, et al. The relationship between sleep quality and cognitive function and the mediating effect of depression in rural elderly in Guizhou Province. Chin J Dis Control Prev. 2023;27(06):
86. Descamps A, Cespuglio R. Influence of aging on the sleep rebound induced by immobilization stress in the rat. Brain Res. 2010;1335:14–23. doi:10.1016/j.brainres.2010.03.087
87. Paine NJ, Watkins LL, Blumenthal JA, Kuhn CM, Sherwood A. Association of depressive and anxiety symptoms with 24-hour urinary catecholamines in individuals with untreated high blood pressure. Psychosomatic Med. 2015;77(2):136–144. doi:10.1097/PSY.0000000000000144
88. Akangbe BO, Akinwumi FE, Adekunle DO, Tijani AA, Aneke OB, Anukam S. Comorbidity of anxiety and depression with hypertension among young adults in the United States: a systematic review of bidirectional associations and implications for blood pressure control. Cureus. 2025;17(7):e88532. doi:10.7759/cureus.88532
89. Beevers CG, Mullarkey MC, Dainer-Best J, et al. Association between negative cognitive bias and depression: a symptom-level approach. J Abnormal Psychol. 2019;128(3):212–227. doi:10.1037/abn0000405
90. Sawyer K, Corsentino E, Sachs-Ericsson N, Steffens DC. Depression, hippocampal volume changes, and cognitive decline in a clinical sample of older depressed outpatients and non-depressed controls. Aging Mental Health. 2012;16(6):753–762. doi:10.1080/13607863.2012.678478
91. Jing C, Kong M, Ng KP, Xu L, Ma G, Ba M. Hippocampal volume maximally modulates the relationship between subsyndromal symptomatic depression and cognitive impairment in non-demented older adults. J Affect Disord. 2024;367:640–646. doi:10.1016/j.jad.2024.09.018
92. Borda MG, Santacruz JM, Aarsland D, et al. Association of depressive symptoms and subjective memory complaints with the incidence of cognitive impairment in older adults with high blood pressure. Eur Geriatric Med. 2019;10(3):413–420. doi:10.1007/s41999-019-00185-1
93. Zhou Y, Xu J, Rief W. Are comparisons of mental disorders between Chinese and German students possible? An examination of measurement invariance for the PHQ-15, PHQ-9 and GAD-7. BMC Psychiatry. 2020;20(1):480. doi:10.1186/s12888-020-02859-8
94. Monteleone P, Martiadis V, Maj M. Circadian rhythms and treatment implications in depression. Prog Neuro Psychopharmacol Biol Psychiatry. 2011;35(7):1569–1574. doi:10.1016/j.pnpbp.2010.07.028
95. Barlattani T, Cavatassi A, Bologna A, et al. Glymphatic system and psychiatric disorders: need for a new paradigm? Front Psychiatry. 2025;16:1642605. doi:10.3389/fpsyt.2025.1642605
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
An Evidence-Based Nursing Intervention Decreases Anxiety, Depression, Sleep Quality and Somatic Symptoms of Patients with Acute Ischemic Stroke
Gao WJ, Bao WJ, Sun SJ
Neuropsychiatric Disease and Treatment 2022, 18:2443-2451
Published Date: 25 October 2022
Correlation Analysis Between Disease Activity and Anxiety, Depression, Sleep Disturbance, and Quality of Life in Patients with Inflammatory Bowel Disease
Yu R, Liu C, Zhang J, Li J, Tian S, Ding F, Liu Z, Wang T, Liu Z, Jiang C, Shi J, Wu K, Dong W
Nature and Science of Sleep 2023, 15:407-421
Published Date: 26 May 2023
Modulatory Effects of XIAOPI Formula on CXCL1 and Selected Outcomes in Triple-Negative Breast Cancer: A Randomized Controlled Clinical Trial
Guo L, Hong SC, Wang X, Wang SQ, Wang N, Wei XQ, Situ HL, Wang ZY
Breast Cancer: Targets and Therapy 2024, 16:289-303
Published Date: 31 May 2024
Depression and Anxiety as Mediators Between Family Functioning and Academic Burnout in First-Year Traditional Chinese Medicine Students
Zhang Y, Liu J, Wang X, Cheng J, Wang X, Zheng C, Liu Q, Li W
Psychology Research and Behavior Management 2025, 18:1717-1727
Published Date: 12 August 2025
Association Between Depression, Anxiety, and Stress and Sleep Quality Among University Students from Saudi Arabia: A Cross-Sectional Study
Gosadi IM, Shnaimer JA
Psychology Research and Behavior Management 2025, 18:2287-2298
Published Date: 14 November 2025