Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Association Between Chronic Obstructive Pulmonary Disease and Survival in Patients with Lung Cancer: A Nationwide Cohort Study
Authors Chan KH, Liu WC, Chang YC, Konara Mudiyanselage SP, Chuang TJ, Tsai YT
Received 27 April 2026
Accepted for publication 9 June 2026
Published 23 June 2026 Volume 2026:21 617198
DOI https://doi.org/10.2147/COPD.S617198
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jill Ohar
Kai-Hsiang Chan,1 Wen-Chun Liu,2 Yu-Chia Chang,3 Sriyani Padmalatha Konara Mudiyanselage,4,5 Tzu-Jung Chuang,6 Yi-Tseng Tsai3
1Department of Radiation Oncology, An Nan Hospital, China Medical University, Tainan, Taiwan; 2College of Nursing, National Tainan Junior College of Nursing, Tainan, Taiwan; 3School of Nursing, China Medical University, Taichung, Taiwan; 4Institute of Behavioral Medicine, The National Cheng Kung University, Tainan, Taiwan; 5School of Nursing & Midwifery, International Institutes of Health Sciences (IIHS), Welisara, Sri Lanka; 6Department of Public Health, College of Medicine, National Cheng Kung University, Tainan, Taiwan
Correspondence: Yi-Tseng Tsai, School of Nursing, China Medical University, Taichung, Taiwan, Email [email protected]
Purpose: Chronic obstructive pulmonary disease (COPD) frequently co-occurs with lung cancer and may adversely influence survival through reduced respiratory reserve, systemic inflammation, immune dysregulation, and impaired treatment tolerance. However, its independent prognostic impact in large real-world lung cancer populations remains uncertain. This nationwide cohort study examined the association between pre-existing COPD and four-year all-cause mortality among patients with newly diagnosed lung cancer.
Methods: We conducted a nationwide retrospective cohort study using linked data from Taiwan’s National Health Insurance Research Database, Cancer Registry, and Death Registry. Adults newly diagnosed with lung cancer between 2011 and 2019 were included and followed until death or the end of 2023. COPD was defined using diagnostic codes recorded before or at cancer diagnosis. Propensity score matching at a 1:3 ratio was used to balance baseline characteristics. Survival was assessed using Kaplan–Meier methods and Cox proportional hazards models.
Results: The matched cohort included 34,832 patients, including 8,708 with COPD and 26,124 without COPD. Four-year survival was lower among patients with COPD than among those without COPD, 31.6% versus 36.8%, respectively; log-rank P < 0.001. Mortality rates were 29.91 and 25.44 per 100 person-years in the COPD and non-COPD groups, respectively. After multivariable adjustment, COPD was independently associated with higher mortality, hazard ratio 1.13; 95% confidence interval 1.09– 1.16. This association was consistent across subgroups and was particularly evident among men, older adults, patients with advanced-stage disease, and those receiving immunotherapy.
Conclusion: Using nationwide linked claims, cancer registry, and mortality data, this study provides population-level evidence that pre-existing COPD is an independent host-related prognostic factor for poorer four-year survival among patients with newly diagnosed lung cancer. Integrating COPD identification, pulmonary optimization, and multidisciplinary pulmonary–oncology care into routine lung cancer management may support risk stratification and improve long-term outcomes.
Keywords: chronic obstructive pulmonary disease, COPD, lung cancer, mortality, survival, comorbidity, cohort study, prognosis
Introduction
Lung cancer remains the leading cause of cancer-related mortality worldwide, accounting for nearly one in five cancer deaths annually.1,2 Although advances in screening, surgical techniques and systemic therapies have improved outcomes for selected patients, overall long-term survival remains poor, particularly among those diagnosed at advanced stages.3 Increasingly, attention has shifted beyond tumor-specific characteristics toward host-related factors that influence respiratory reserve, immune competence and treatment tolerance, all of which may critically shape survival trajectories.4–6 Among these factors, chronic obstructive pulmonary disease (COPD), a progressive inflammatory condition characterized by persistent airflow limitation has emerged as a potentially important modifier of lung cancer outcomes.7
COPD and lung cancer share overlapping pathogenic mechanisms, including chronic airway inflammation, oxidative stress, protease–antiprotease imbalance, and cumulative DNA damage associated with tobacco exposure and ageing. Recurrent epithelial injury and aberrant tissue remodeling may contribute to a carcinogenic microenvironment that promotes tumor initiation and progression. Beyond local airway effects, COPD is increasingly recognized as a systemic disorder.8 Chronic hypoxemia and sustained inflammatory activation may impair pulmonary mechanics, alter immune surveillance, and disrupt metabolic homeostasis, thereby reducing treatment tolerance and potentially compromising the effectiveness of chemotherapy, targeted therapy, and immunotherapy.
COPD and lung cancer share overlapping pathogenic mechanisms, including chronic airway inflammation, oxidative stress, protease–antiprotease imbalance and cumulative DNA damage associated with tobacco exposure and ageing.9,10 Recurrent epithelial injury and aberrant tissue remodeling contribute to a carcinogenic microenvironment that promotes tumor initiation and progression.8,11 Beyond local airway effects, COPD is increasingly recognized as a systemic disorder. Chronic hypoxemia and sustained inflammatory activation may impair pulmonary mechanics, alter immune surveillance and disrupt metabolic homeostasis, thereby reducing treatment tolerance and compromising the effectiveness of chemotherapy, targeted therapy and immunotherapy.12,13 Collectively, these processes suggest that COPD could adversely influence both cancer-specific and overall survival in patients with lung cancer.
Despite strong biological plausibility, the prognostic impact of COPD in lung cancer remains incompletely defined. Prior studies have reported inconsistent findings. Some have demonstrated higher postoperative morbidity and worse long-term survival among patients with COPD,14,15 whereas others observed attenuation of risk after adjustment for smoking and comorbidities.15,16 Interpretation has been limited by small sample sizes, heterogeneous definitions of COPD, inadequate characterization of cancer stage and treatment, and insufficient follow-up. Moreover, few investigations have examined whether the prognostic relevance of COPD varies across contemporary treatment contexts, including immunotherapy and molecularly targeted therapies.
To address these gaps, we conducted a nationwide, population-based cohort study using linked data from Taiwan’s National Health Insurance Research Database (NHIRD), Taiwan Cancer Registry (TCR), and Taiwan Death Registry (TDR).17–20 These comprehensive databases provide near-complete population coverage and validated longitudinal information on diagnoses, treatments and mortality. Our primary objective was to examine the association between pre-existing COPD and four-year all-cause mortality among patients with newly diagnosed lung cancer. We further aimed to determine whether this association differed across demographic, clinical and treatment subgroups. We hypothesized that COPD independently predicts poorer long-term survival and that its adverse prognostic impact persists across diverse patient populations. By leveraging large-scale real-world data with extended follow-up, this study seeks to clarify the prognostic significance of COPD in lung cancer and to inform integrated risk stratification and multidisciplinary care strategies.
Study Design and Methods
Study Design, Population and Data Sources
We conducted a nationwide, retrospective, population-based cohort study to examine the association between COPD and long-term mortality among patients with newly diagnosed lung cancer. Patients were classified according to the presence or absence of COPD at or before the time of lung cancer diagnosis and were followed longitudinally to compare survival outcomes.
Data was obtained through individual-level linkage of three nationwide administrative databases in Taiwan: NHIRD, TCR, and the TDR. Together, these databases provide near-complete population coverage (>99%) and comprehensive information on diagnoses, comorbidities, cancer characteristics, treatments, healthcare utilisation and validated mortality outcomes, enabling robust longitudinal survival analyses.21,22
The NHIRD contains longitudinal claims data for more than 23 million residents, representing approximately 99.9% of the Taiwanese population.23,24 It includes detailed records of outpatient and inpatient encounters, diagnostic and procedural codes, prescription claims, and enrolment information. Data quality is ensured through routine audits conducted by the National Health Insurance Administration, which randomly reviews claims to verify diagnostic accuracy and internal consistency.22
The TCR, established in 1979, is a mandatory reporting system for all hospitals with ≥50 beds and achieves case completeness exceeding 98%.19 The registry includes validated information on cancer sites, histology, stage and treatment, and was used to confirm lung cancer diagnoses and characterize tumor profiles. The TDR, maintained by the Ministry of Health and Welfare, provides official mortality data, including date and cause of death, coded according to the International Classification of Diseases and subject to standardized verification procedures to minimize misclassification.20 Integration of these databases enabled construction of a nationwide cohort with longitudinal tracking of exposures, comorbidities, treatments and mortality outcomes.
Databased Access Procedure
This study utilized data obtained from the Data Science Center of the Ministry of Health and Welfare (MOHW), Taiwan, which maintains integrated nationwide healthcare databases, including the Taiwan Cancer Registry, the National Death Registry, and National Health Insurance claims data. Access to these datasets requires a formal application, independent scientific and ethical review by external experts, and approval from Institutional Review Boards (IRBs) (IRB No. CMUH115-REC3-118 and TMANH114-REC024).
All analyses were performed on-site within the secure data environment of the MOHW Data Science Center, in compliance with stringent data protection and governance regulations. Applicants are required to clearly define the research objectives and anticipated outcomes and to adhere to mandatory reporting requirements, including submission of final research outputs for audit and disclosure purposes. Each approved project is granted access to the data for a period of one year.
To safeguard data security and participant confidentiality, all procedures related to data access, import, and export are strictly controlled and subject to official review and authorization. All data were irreversibly de-identified prior to release, and all study procedures complied with applicable laws and regulations governing the use of secondary health data in Taiwan.
Study Population
The source population comprised adults aged ≥20 years with newly diagnosed lung cancer between 1 January 2011 and 31 December 2019. Lung cancer cases were identified using ICD-9-CM codes B101, 162, 162.0, 162.2–162.5, 162.8 and 162.9, and ICD-10-CM codes C33–C34, D02.1–D02.2, D38.1, 231.1–231.2, 231.8 and 235.7.25,26 To enhance diagnostic validity, patients were required to have at least three outpatient visits or one inpatient admission with a primary diagnosis of lung cancer. All eligible cases were cross validated with the TCR to confirm diagnosis and staging.
Patients were excluded if they had incomplete demographic information, missing cancer stage, unavailable smoking or alcohol use data, age <20 years at diagnosis, or follow-up <6 months. These criteria ensured data completeness, reduced misclassification and established a clear temporal relationship between exposure and outcome. Participants were followed from the date of lung cancer diagnosis until death or 31 December 2023, whichever occurred first.
COPD Definition and Exposure Assessment
COPD was identified using ICD-9-CM codes 490, 491.x, 492.x, 493.2 and 496, and ICD-10-CM codes J41.x, J42, J43.x, J44.0, J44.1 and J44.9.27,28 To increase diagnostic specificity and minimize misclassification inherent in claims-based data, patients were classified as having COPD only if they had at least three outpatient visits or at least one hospital admission with a COPD diagnosis before or at the time of lung cancer diagnosis. This approach captured clinically recognized and actively managed COPD and reduced the likelihood of incidental or rule-out diagnoses. Any under-ascertainment of mild COPD would be expected to bias results toward the null.
The index date was defined as the date of lung cancer diagnosis. Patients were categorized into COPD and non-COPD groups based on diagnoses recorded before or at the index date. This ensured appropriate temporal ordering between exposure and outcome and reduced the risk of immortal time and reverse causation bias. The comparison cohort comprised patients with lung cancer without any recorded diagnosis of COPD throughout the observation period.
Outcome Measures
The primary outcome was four-year all-cause mortality. Mortality data were obtained from the TDR, which provides validated information on death date and cause. Survival time was calculated from the date of lung cancer diagnosis to death or end of follow-up. Patients who remained alive were censored on 31 December 2023. Secondary outcomes included subgroup-specific survival analyses stratified by age, sex, cancer stage and treatment modality.
Covariates
A comprehensive set of demographics, socioeconomic, lifestyle and clinical variables was included to control for potential confounding. Demographic variables included age at diagnosis, sex and marital status. Socioeconomic status was assessed using monthly insurance premium-based income categories (≤NT$29,000; NT$30,000–49,999; NT$50,000–69,999; ≥NT$70,000). Lifestyle factors included smoking status and alcohol consumption, identified from claims and medical records. Contextual factors included level of urbanisation (high, moderate, low) based on established indices of healthcare accessibility. Clinical covariates included comorbidity burden measured by the Charlson Comorbidity Index (CCI), and specific conditions including anxiety, depression, other psychiatric disorders, substance use disorders and sleep disturbances. Cancer-related variables included stage at diagnosis and treatment modalities, including surgery, chemotherapy, radiotherapy, targeted therapy and immunotherapy. All covariates were selected as a priori to account for clinical vulnerability, healthcare utilization patterns and sociodemographic disparities that could influence both COPD ascertainment and survival outcomes.
Propensity Score Matching
To reduce baseline imbalances between patients with and without COPD, propensity score matching (PSM) was performed at a 1:3 ratio. Propensity scores were estimated using multivariable logistic regression models incorporating age, sex, marital status, income, comorbidities, cancer stage and treatment modalities. Marital status and income were included as proxies of social support and socioeconomic status, which may influence healthcare utilization and diagnostic intensity.
Smoking was not included in the propensity score model because it represents a shared etiologic factor for both COPD and lung cancer rather than a determinant of COPD exposure conditional on lung cancer diagnosis. To avoid over-adjustment and potential collider bias, smoking was adjusted for in outcome models rather than in matching. Eligible controls were required to be alive on the index date of their matched case and to have no diagnosis of COPD during follow-up. Balance between groups was assessed using absolute standardized mean differences, with values <0.1 indicating acceptable balance.
Statistical Analysis
Person-years at risk were calculated from lung cancer diagnosis to death or censoring. Survival probabilities were estimated using the Kaplan–Meier method and compared using the Log rank test. Cox proportional hazards regression was used to estimate hazard ratios (HRs) and 95% confidence intervals (CIs) for four-year all-cause mortality. Multivariable models were adjusted for age, sex, marital status, income, smoking, alcohol use, urbanization, comorbidities, cancer stage and treatment modalities. The proportional hazards assumption was assessed using log-minus-log survival plots and tests of time-dependent covariates.29,30 Prespecified subgroup analyses were conducted by age, sex, comorbidity burden, cancer stage and treatment type. Sensitivity analyses were performed using alternative matching ratios and restricting follow-up to four years to assess robustness.
All analyses were two-sided, with P<0.05 considered statistically significant. Data management and analyses were conducted using SAS version 9.4 (SAS Institute, Cary, NC).31
Results
Baseline Characteristics
From an initial cohort of 118,804 adults newly diagnosed with lung cancer between 1 January 2011 and 31 December 2019, 43,340 were excluded because of missing demographic data (n=481), missing cancer stage (n=8,425), incomplete smoking or alcohol records (n=11,720), age <20 years (n=30), or follow-up <6 months (n=22,684) (Figure 1). The remaining 75,464 patients formed the eligible cohort. Of these, 8,890 had a diagnosis of COPD recorded after lung cancer diagnosis and 66,574 did not. After excluding individuals whose COPD developed after the cancer diagnosis, the final analytic sample comprised 34,832 patients, including 8,708 (25.0%) with pre-existing COPD and 26,124 (75.0%) without COPD.
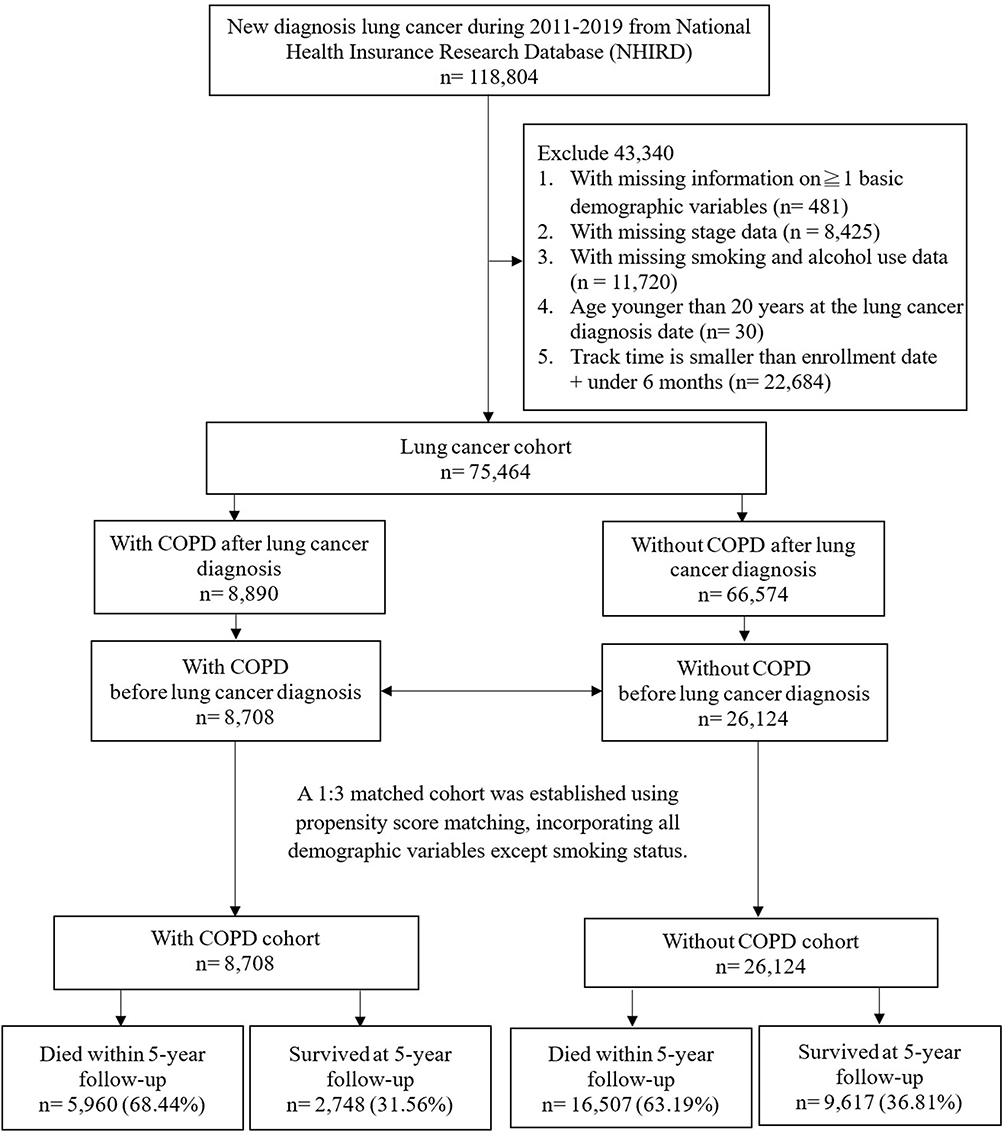 |
Figure 1 Flowchart of study population selection from the NHIRD, TCR, and TDR databases. The index date was defined as the date of lung cancer diagnosis. Patients were classified according to whether they had COPD before or at lung cancer diagnosis. Survival outcomes were assessed over a four-year follow-up period after the index date. |
Before matching, patients with COPD were older (mean age 71.2±11.0 vs 64.7±12.0 years), more frequently male (73.9% vs 48.4%), and had greater comorbidity burden (CCI ≥4: 26.6% vs 20.1%) than those without COPD (Table 1). They were also more likely to be smokers, have lower income, reside in less urbanised areas, and present with advanced-stage disease. Psychiatric disorders, substance use, and sleep disturbances were more prevalent among patients with COPD. They were less likely to undergo surgery (32.5% vs 38.8%) and more likely to receive targeted therapy.
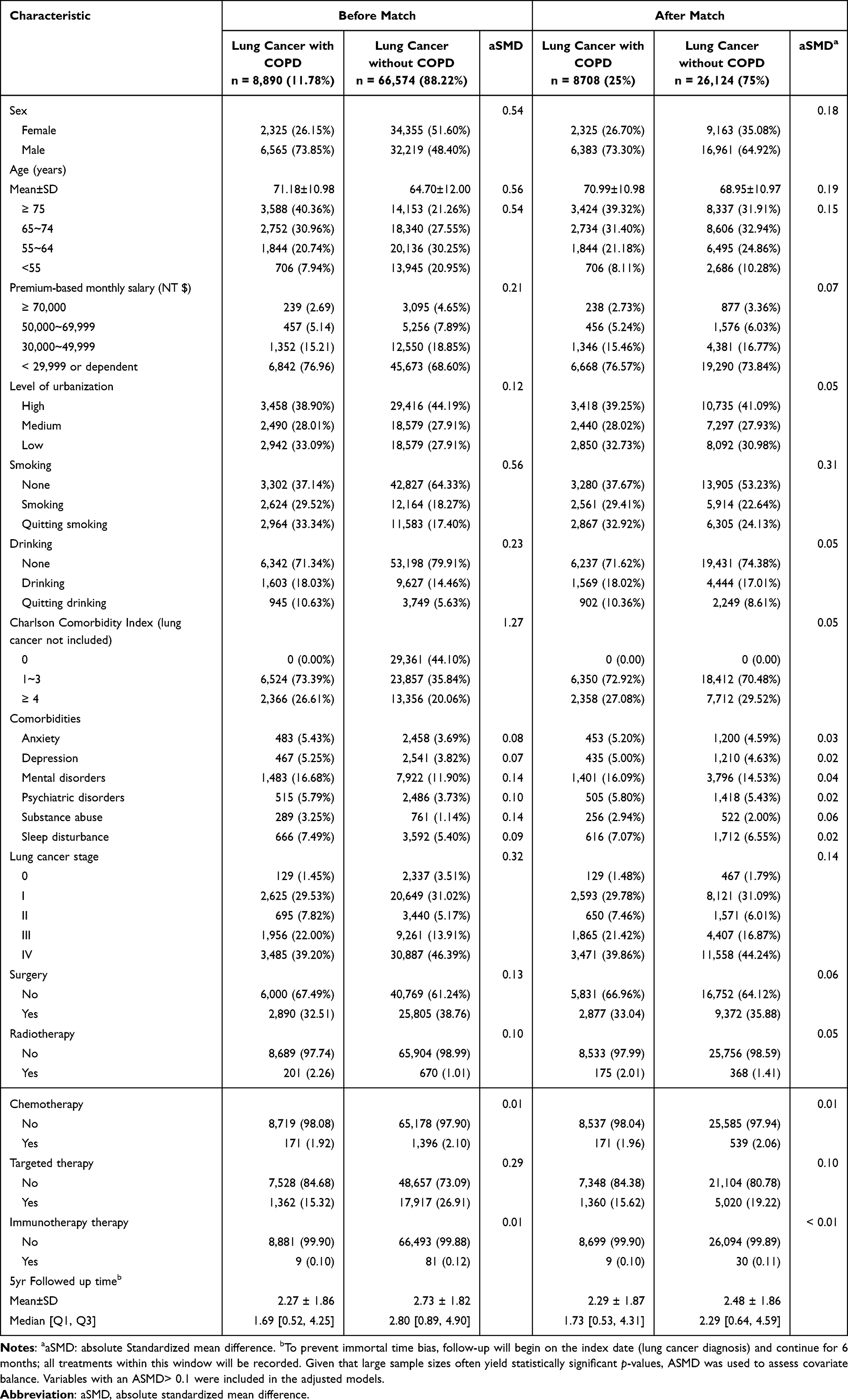 |
Table 1 Characteristics of Lung Cancer with/without COPD |
Propensity score matching at a 1:3 ratio achieved satisfactory covariate balance, with all absolute standardised mean differences <0.1. After matching, patients with COPD remained slightly older (71.0±11.0 vs 69.0±11.0 years) and predominantly male (73.3% vs 64.9%). Mean follow-up time was shorter in the COPD group (2.29±1.87 years; median 1.73, IQR 0.53–4.31) than in the non-COPD group (2.48±1.86 years; median 2.29, IQR 0.64–4.59).
Survival and Mortality Rates
During four years of follow-up, mortality was consistently higher among patients with COPD. A total of 5,960 deaths (68.4%) occurred in the COPD cohort and 16,507 deaths (63.2%) in the non-COPD cohort (Table 2). Corresponding four-year survival rates were 31.6% and 36.8%, respectively. Kaplan–Meier curves demonstrated early and sustained separation between groups, with significantly poorer survival among patients with COPD (log-rank P<0.001). Survival divergence emerged within the first two years after diagnosis and persisted throughout follow-up.
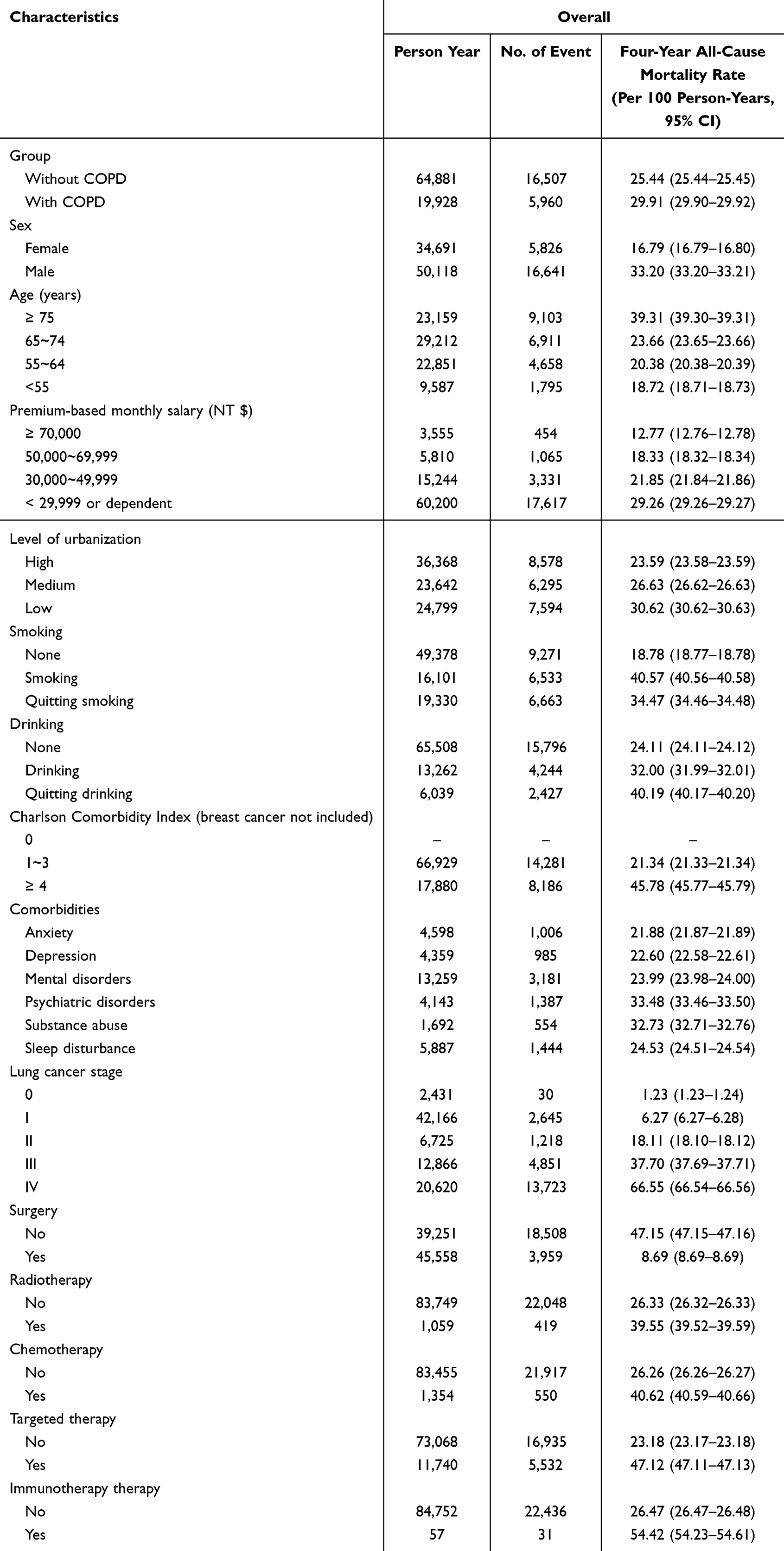 |
Table 2 Overall and Subgroup-Specific All-Cause Mortality Rates Among Patients with Lung Cancer |
Overall mortality incidence was 29.91 per 100 person-years (95% CI 29.90–29.92) in patients with COPD compared with 25.44 per 100 person-years (95% CI 25.44–25.45) in those without COPD. Mortality increased markedly with age, reaching 39.31 per 100 person-years among patients aged ≥75 years and was lowest among those aged <55 years (18.72 per 100 person-years). Men experienced substantially higher mortality than women (33.20 vs 16.79 per 100 person-years).
Socioeconomic disadvantage was associated with poorer outcomes. Patients with monthly income ≤NT$29,999 had mortality of 29.26 per 100 person-years, compared with 12.77 per 100 person-years among those earning ≥NT$70,000. Mortality was higher in low-urbanisation areas than in highly urbanised regions (30.62 vs 23.59 per 100 person-years). Lifestyle factors were also influential: smokers had a mortality rate of 40.57 per 100 person-years, and alcohol users 32.00 per 100 person-years, with the highest mortality observed among former drinkers (40.19 per 100 person-years).
Comorbidity burden strongly influenced survival. Patients with CCI ≥4 had a mortality rate of 45.78 per 100 person-years, more than double that observed in patients with lower comorbidity burden (21.34 per 100 person-years). Psychiatric disorders and substance use were also associated with elevated mortality. Cancer stage demonstrated a steep gradient, increasing from 6.27 per 100 person-years in stage I disease to 66.55 per 100 person-years in stage IV disease. Regarding treatment, patients undergoing surgery had the lowest mortality (8.69 per 100 person-years), whereas those receiving targeted therapy and immunotherapy—reflecting more advanced disease—had the highest mortality (47.12 and 54.42 per 100 person-years, respectively).
Multivariable Analyses
After adjustment for demographic, socioeconomic, clinical and treatment-related variables, COPD remained independently associated with increased four-year all-cause mortality (adjusted HR 1.13, 95% CI 1.09–1.16; P<0.001) (Table 3). Male sex was associated with higher mortality risk (HR 1.61, 95% CI 1.56–1.66). Compared with patients aged ≥75 years, progressively lower risks were observed in younger age groups (HR 0.71 for 65–74 years; HR 0.60 for 55–64 years; HR 0.56 for <55 years; all P<0.0001).
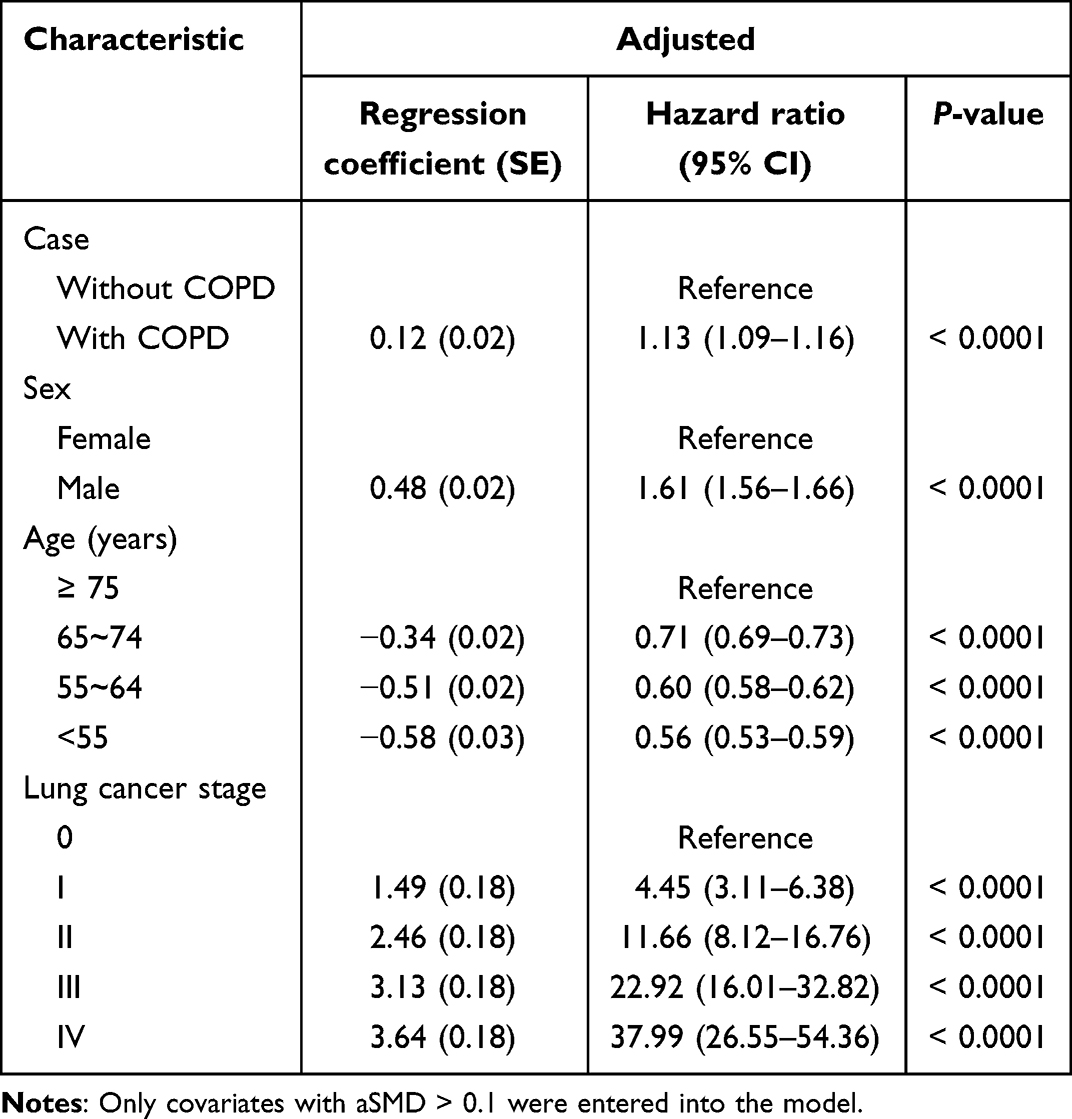 |
Table 3 Hazard Ratios of Suicide in Lung Cancer with COPD Compared with Control Participants |
Mortality risk increased substantially with advancing cancer stage. Relative to stage 0, hazard ratios rose stepwise from 4.45 for stage I to 37.99 for stage IV disease (all P<0.0001), highlighting the dominant influence of tumour burden alongside host factors.
Subgroup and Sensitivity Analyses
The adverse prognostic impact of COPD was broadly consistent across predefined subgroups (Figure 2). Elevated risks were observed in men (HR 1.17, 95% CI 1.13–1.21) and were more pronounced in older patients. COPD remained associated with increased mortality across comorbidity strata, among those with psychiatric disorders, and among patients without depression. When stratified by cancer stage, the relative effect of COPD was greatest in early-stage disease and attenuated with advancing stage, though remaining statistically significant.
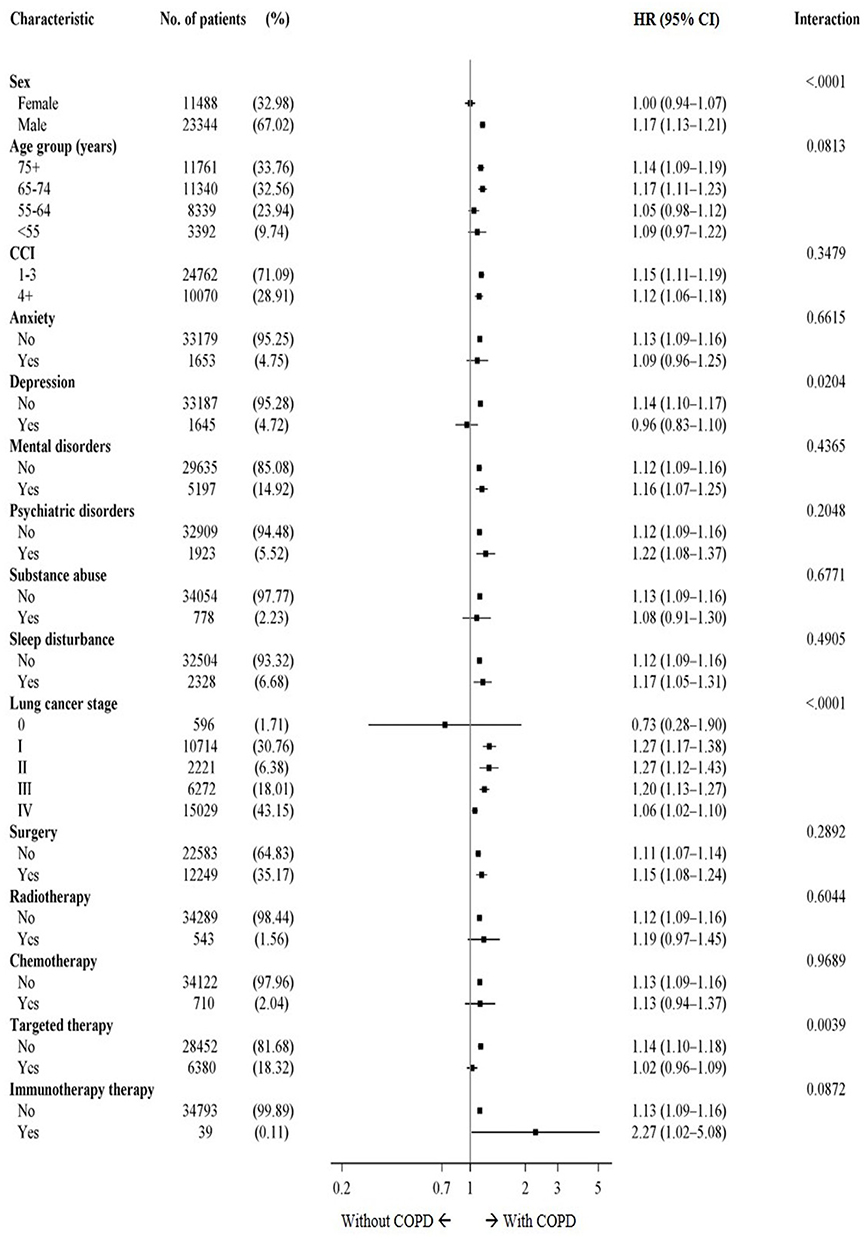 |
Figure 2 Subgroup-specific hazard ratios for four-year mortality associated with COPD among patients with lung cancer. Hazard ratios and 95% confidence intervals are shown for predefined demographic, clinical, comorbidity, cancer-stage, and treatment subgroups. |
By treatment modality, COPD was associated with increased mortality among patients undergoing surgery and radiotherapy, with the strongest association observed among those receiving immunotherapy (HR 2.27, 95% CI 1.02–5.08). Sensitivity analyses using alternative matching ratios, extended follow-up and exclusion of short-term survivors yielded comparable results, confirming the robustness of the findings.
Discussion
Principal Findings and Clinical Relevance
In this nationwide, population-based cohort study, pre-existing COPD was independently associated with significantly higher four-year all-cause mortality among patients with lung cancer in Taiwan. After comprehensive adjustment for demographic characteristics, comorbidities, cancer stage, and treatment modalities, COPD conferred an approximately 13% excess risk of death compared with no COPD. Although the adjusted hazard ratio for COPD was modest, this effect is clinically meaningful at the population level because COPD is common among patients with lung cancer, potentially identifiable, and partly modifiable. Even a modest independent increase in mortality risk may have important implications for risk stratification, treatment planning, and supportive care decisions. These findings support the integration of COPD assessment and management into lung cancer care, including pulmonary function evaluation, smoking cessation support, optimization of inhaled therapies, pulmonary rehabilitation, and multidisciplinary pulmonary–oncology collaboration. Importantly, this association was consistent across major clinical subgroups and robust in multiple sensitivity analyses, demonstrating that COPD is not merely a coincidental comorbidity but a clinically meaningful host-related prognostic factor in lung cancer.
By integrating three national datasets, the NHIRD, TCR and TDR, covering more than 99% of Taiwanese residents, this study provides one of the most comprehensive population-level assessments of the prognostic impact of COPD in lung cancer. This design enabled precise adjustment for cancer characteristics and treatment exposure, overcoming key limitations of earlier single-centre or surgically restricted cohorts that were vulnerable to selection bias and incomplete follow-up. Our findings therefore extend existing evidence by confirming the independent prognostic role of COPD across the entire lung cancer continuum, from early-stage disease to patients receiving contemporary systemic therapies.
Notably, the adverse survival impact of COPD was most pronounced among older adults, men, and patients treated with immunotherapy. These subgroup patterns suggest a multifactorial interaction between age-related vulnerability, cumulative pulmonary injury, systemic inflammation, and immune dysregulation. However, the subgroup analysis among patients receiving immunotherapy should be interpreted with caution because this subgroup included a relatively small number of patients. The wide confidence interval indicates limited statistical precision, and this finding should be considered exploratory rather than confirmatory. Further studies with larger immunotherapy-treated cohorts are needed to clarify whether COPD modifies survival or treatment response in this population. Collectively, these data support a reconceptualization of COPD not simply as a coexisting respiratory disease, but as a systemic inflammatory disorder capable of shaping tumor biology, treatment tolerance, and long-term survival.
Biological Mechanisms and Relationship to Prior Evidence
The biological plausibility of COPD as a determinant of lung cancer prognosis is supported by substantial mechanistic and translational evidence. COPD and lung cancer share overlapping pathogenic pathways centred on chronic inflammation, oxidative stress and dysregulated immunity. Persistent airway inflammation in COPD promotes sustained release of pro-inflammatory mediators, including IL-6, IL-8 and TNF-α, with downstream activation of nuclear factor-κB and STAT3 signaling pathways.32–36 These cascades facilitate tumour proliferation, angiogenesis, epithelial mesenchymal transition and resistance to apoptosis, thereby contributing not only to carcinogenesis but also to tumour progression and metastatic potential.
Beyond local airway pathology, COPD exerts important systemic effects. Chronic hypoxemia and oxidative stress promote mitochondrial dysfunction, DNA damage and genomic instability, processes that are closely linked to aggressive tumor phenotypes and therapeutic resistance.37,38 Activation of hypoxia-inducible factor-1α may further drive angiogenesis and metabolic reprogramming, enhancing tumor survival in hostile microenvironments.39,40
Equally important are COPD-associated immune alterations. Impaired cytotoxic T-cell activity, expansion of exhausted T-cell populations and altered macrophage polarisation can collectively blunt antitumour immune surveillance.41,42 These immune disturbances628081provide a compelling biological explanation for our observation that the relative mortality risk associated with COPD was highest among patients receiving immunotherapy, suggesting that pre-existing immune dysfunction may attenuate treatment efficacy.
Our findings are concordant with prior clinical studies demonstrating poorer oncologic outcomes among patients with COPD. Roy et al showed that COPD increased postoperative complications43 and reduced long-term survival following lung cancer resection,14 while Sato et al reported that CT-defined emphysema independently predicted recurrence and mortality in early-stage disease.44 A recent meta-analysis further confirmed that COPD is associated with worse overall survival in lung cancer.45–47 However, earlier investigations were often constrained by heterogeneous COPD definitions, limited adjustment for cancer characteristics or restricted populations, contributing to inconsistent conclusions.48–50
By leveraging standardized national data with long-term follow-up and comprehensive covariate control, our study provides stronger population-level evidence that COPD independently influences survival. Importantly, we extend prior literature by demonstrating that the prognostic relevance of COPD persists across treatment contexts, including immunotherapy and targeted therapy, highlighting the importance of host inflammatory and immune status in the modern therapeutic era.
Clinical Implications and Future Directions
These findings support an integrated pulmonary–oncology care pathway for patients with lung cancer and coexisting COPD. At or near the time of lung cancer diagnosis, patients should undergo structured respiratory assessment, including smoking history, symptom burden, exacerbation history, oxygenation status, and spirometry where feasible. Optimization of inhaled bronchodilator and anti-inflammatory therapy, smoking cessation support, vaccination, nutritional assessment, and pulmonary rehabilitation should be considered before and during cancer treatment. For patients undergoing surgery, radiotherapy, chemotherapy, targeted therapy, or immunotherapy, multidisciplinary collaboration between oncologists, pulmonologists, rehabilitation specialists, nurses, and supportive care teams may help reduce pulmonary complications, improve treatment tolerance, and support individualized risk stratification. COPD should be recognized as a critical host-related determinant of long-term outcomes and incorporated into prognostic stratification and treatment planning. Early identification and optimization of COPD at the time of cancer diagnosis may offer opportunities to improve treatment tolerance, reduce complications and potentially enhance survival. Routine respiratory assessment, including spirometry, symptom burden evaluation and optimization of inhaled therapies, should be integrated into oncologic pathways,51,52 particularly for older patients and those receiving curative-intent or systemic treatments.
The results also underscore the need for structured multidisciplinary care models. Close collaboration between oncologists, pulmonologists and rehabilitation specialists is essential. For patients undergoing surgery or radiotherapy, perioperative pulmonary optimization and tailored rehabilitation programs may mitigate postoperative morbidity and accelerate recovery.44,53 Among those receiving chemotherapy, targeted therapy or immunotherapy, regular monitoring of lung function and inflammatory biomarkers may allow early identification of pulmonary toxicity and facilitate timely treatment modification.54 COPD may also increase vulnerability to treatment-related pulmonary toxicity, including radiation pneumonitis, immune-related pneumonitis, COPD exacerbations, respiratory infections, and treatment interruptions. This may be particularly relevant among patients receiving immunotherapy or thoracic radiotherapy. Although treatment-related pulmonary toxicity was not systematically available in the current dataset, these findings support the need for closer pulmonary monitoring and individualized treatment planning in patients with coexisting COPD and lung cancer. Establishing integrated co-management pathways could improve treatment continuity, symptom control and quality of life, while potentially translating into survival benefits.55,56
Beyond supportive care, our findings point toward important translational opportunities. The apparent interaction between COPD-related inflammation and cancer immunobiology raises the possibility that adjunctive anti-inflammatory or immune-modulatory strategies could improve therapeutic responsiveness.57,58 Future studies should explore whether inhaled corticosteroids, phosphodiesterase-4 inhibitors59 or biologics targeting IL-660 or TNF-α61 pathways can favorably modulate systemic inflammation and immune competence. Incorporating molecular and immunologic biomarkers into future clinical trials will be essential to clarify tumor–host interactions and to identify phenotypes most likely to benefit from targeted supportive interventions.62,63
Strengths and Limitations
Several limitations should be considered. The retrospective design precludes causal inference; therefore, the findings should be interpreted as associations rather than evidence of a causal relationship between COPD and mortality. Although propensity score matching, multivariable adjustment, and sensitivity analyses improved comparability between groups, residual confounding and selection bias cannot be fully eliminated. COPD was identified using administrative claims data rather than spirometry-confirmed diagnoses. Therefore, misclassification is possible, and information on COPD severity, including GOLD stage, FEV1 values, symptom burden, exacerbation history, and treatment intensity, was unavailable. Residual confounding may also remain. Although the models adjusted for available demographic, socioeconomic, clinical, smoking, alcohol, cancer-stage, and treatment-related variables, the databases did not provide detailed information on smoking intensity or duration, pack-years, second-hand smoke exposure, physical activity, nutritional status, body mass index, pulmonary performance, or functional status. These unmeasured factors may have influenced both COPD status and survival outcomes. Information on molecular tumour profiles, treatment dosing, treatment-related pulmonary toxicity, and cause-specific mortality was also limited, preventing more granular analyses. Finally, as this study was conducted within Taiwan’s single-payer health system, caution is warranted when extrapolating to other healthcare contexts.
Nevertheless, the nationwide scope, large sample size, long follow-up, and comprehensive data linkage represent major strengths. The ability to examine real-world outcomes across the entire lung cancer population provides strong external validity and reinforces the clinical relevance of COPD as a prognostic determinant.
Conclusion
In this nationwide linked cohort study, pre-existing COPD independently predicted poorer four-year survival among patients with newly diagnosed lung cancer. By integrating national claims, cancer registry, and mortality data, this study provides population-level evidence that COPD is a clinically relevant host-related prognostic factor across the lung cancer care continuum. These findings highlight the need to integrate COPD identification, pulmonary optimization, and multidisciplinary pulmonary–oncology care into routine lung cancer management.
Data Sharing Statement
The data that support the findings of this study were obtained from the Taiwan National Health Insurance Research Database (NHIRD) maintained by the Health and Welfare Data Science Center, Ministry of Health and Welfare, Taiwan. Restrictions apply to the availability of these data, which were used under license for the current study, and are not publicly available. Data may be available from the corresponding author upon reasonable request and with permission from the NHIRD and approval from an Institutional Review Board.
Acknowledgments
We thank the volunteers for their support and contributions to this research.
Disclosure
Dr Yi-Tseng Tsai reports support from An Nan Hospital, China Medical University, Tainan, Taiwan (Grant No. ANHRF114-12), during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Bray F, Laversanne M, Sung H. et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–16. doi:10.3322/caac.21834
2. Li C, Lei S, Ding L, et al. Global burden and trends of lung cancer incidence and mortality. Chin Med J. 2023;136(13):1583–1590. doi:10.1097/CM9.0000000000002529
3. Jeon DS, Kim HC, Kim SH, et al. Five-year overall survival and prognostic factors in patients with lung cancer: results from the Korean Association of Lung Cancer Registry (KALC-R) 2015. Cancer Res Treat. 2023;55(1):103–111. doi:10.4143/crt.2022.264
4. Huang Y, Ma W, Wu D, et al. Prognostic relevance of immune-related adverse events in lung cancer patients undergoing immune checkpoint inhibitor therapy: a systematic review and meta-analysis. Transl Lung Cancer Res. 2024;13(7):1559–1584. doi:10.21037/tlcr-24-299
5. Lee S, Eo W, Jeon H, Park S, Chae J. Prognostic significance of host-related biomarkers for survival in patients with advanced non-small cell lung cancer. J Cancer. 2017;8(15):2974–2983. doi:10.7150/jca.20866
6. Wang P, Wang S, Sun Z, et al. Systemic inflammation influences the prognosis of patients with radically resected non-small cell lung cancer and correlates with the immunosuppressive microenvironment. Int J Cancer. 2023;153(4):826–842. doi:10.1002/ijc.34547
7. Qi C, Sun SW, Xiong XZ. From COPD to lung cancer: mechanisms linking, diagnosis, treatment, and prognosis. Int J Chron Obstruct Pulmon Dis. 2022;17:2603–2621. doi:10.2147/COPD.S380732
8. Heinrich EL, Walser TC, Krysan K, et al. The inflammatory tumor microenvironment, epithelial mesenchymal transition and lung carcinogenesis. Cancer Microenviron. 2012;5(1):5–18. doi:10.1007/s12307-011-0089-0
9. Ding T, Lin Q, Qu X. From chronic obstructive pulmonary disease (COPD) to lung cancer: a Mendelian randomization study revealing mediation pathways through plasma metabolomics, proteomics, and immunophenotyping. Discov Oncol. 2025;16(1):629. doi:10.1007/s12672-025-02434-1
10. Durham AL, Adcock IM. The relationship between COPD and lung cancer. Lung Cancer. 2015;90(2):121–127. doi:10.1016/j.lungcan.2015.08.017
11. Arandhara A, Bhuyan P, Das BK. Exploring lung cancer microenvironment: pathways and nanoparticle-based therapies. Discov Oncol. 2025;16(1):159. doi:10.1007/s12672-025-01902-y
12. Boudoussier A, Larrouture I, Henrot P, et al. COPD patients with non-small cell lung cancer respond better to anti-PD-(L)1 immune checkpoint inhibitors. Sci Rep. 2025;15(1):17145. doi:10.1038/s41598-025-02251-0
13. Ju S, Lee HR, Kim JY, et al. Impact of coexistent chronic obstructive pulmonary disease on the survival of patients with small cell lung cancer receiving chemotherapy. Thorac Cancer. 2018;9(10):1271–1278. doi:10.1111/1759-7714.12832
14. Roy E, Rheault J, Pigeon MA, et al. Lung cancer resection and postoperative outcomes in COPD: a single-center experience. Chron Respir Dis. 2020;17:1479973120925430. doi:10.1177/1479973120925430
15. Zimmermann J, Schon J, Pfeiffer V, et al. COPD severity as an independent predictor of long-term survival in operable lung cancer: a retrospective analysis from a high-volume thoracic surgery center. Int J Chron Obstruct Pulmon Dis. 2025;20:3073–3091. doi:10.2147/COPD.S518084
16. Chen H, Hu XB, Zhou J, He CY, Wang K, Yi Q. Association of chronic obstructive pulmonary disease with risk of lung cancer in individuals aged 40 years and older: a cross-sectional study based on NHANES. PLoS One. 2024;19(10):e0311537. doi:10.1371/journal.pone.0311537
17. Chiang JK, Lin CW, Wang CL, Koo M, Kao YH. Cancer studies based on secondary data analysis of the Taiwan’s National Health Insurance Research Database: a computational text analysis and visualization study. Medicine. 2017;96(17):e6704. doi:10.1097/MD.0000000000006704
18. Siu WHS, Lim AY, Liu JR, et al. Cancer publications using real-world data from the Taiwan National Health Insurance Research Database: conceptual framework and bibliometric analysis. J Chin Med Assoc. 2025;88(5):398–409. doi:10.1097/JCMA.0000000000001227
19. Yang ZY, Chen WL, Wu WT, Lai CH, Ho CL, Wang CC. Return to work and mortality in breast cancer survivors: a 11-year longitudinal study. Int J Environ Res Public Health. 2022;19(21). doi:10.3390/ijerph192114418
20. Welfare NHIAMoHa. Database user manual; 2019. Available from: https://dep.mohw.gov.tw/dos/lp-3147-113-2-20.html.
21. Chen YC,;, Lee WC. Examples of data analysis and application using Taiwan’s National Health Insurance Database in Healthcare. Formosan J Med. 2016;20(6):602–608. doi:10.6320/fjm.2016.20(6).6
22. Hsieh CY, Su CC, Shao SC, et al. Taiwan’s National Health Insurance Research Database: past and future. Clin Epidemiol. 2019;11:349–358. doi:10.2147/clep.S196293
23. Lin L-Y, Warren-Gash C, Smeeth L, Chen PC. Data resource profile: the National Health Insurance Research Database (NHIRD). Epidemiol Health. 2018;40:e2018062. doi:10.4178/epih.e2018062
24. Lin CL, Chung CH, Tsai YH, Chien WC. Association between sleep disorders and injury: a nationwide population-based retrospective cohort study. Inj Prev. 2016;22(5):342–346. doi:10.1136/injuryprev-2015-041844
25. Jani CT, Kareff SA, Morgenstern-Kaplan D, et al. Evolving trends in lung cancer risk factors in the ten most populous countries: an analysis of data from the 2019 Global Burden of Disease Study. EClinicalMedicine. 2025;79:103033. doi:10.1016/j.eclinm.2024.103033
26. Balzi W, Roncadori A, Danesi V, et al. How to discriminate non-small cell lung cancer (NSCLC) cases from an Italian administrative database? A retrospective, secondary data use study for evaluating a novel algorithm performance. BMJ Open. 2021;11(9):e048188. doi:10.1136/bmjopen-2020-048188
27. Cooke CR, Joo MJ, Anderson SM, et al. The validity of using ICD-9 codes and pharmacy records to identify patients with chronic obstructive pulmonary disease. BMC Health Serv Res. 2011;11:37. doi:10.1186/1472-6963-11-37
28. Fernández-García A, Pérez-Ríos M, Candal-Pedreira C, et al. Where do chronic obstructive pulmonary disease patients die? 8-year trend, with special focus on sex-related differences. Int J Chron Obstruct Pulmon Dis. 2022;17:1081–1087. doi:10.2147/copd.S351259
29. Tan HF, Tseng HF, Chang CK, Lin W, Hsiao SH. Accessibility assessment of the health care improvement program in rural Taiwan. J Rural Health. 2005;21(4):372–377. doi:10.1111/j.1748-0361.2005.tb00110.x
30. Tsai YT, Chuang TJ, Mudiyanselage SPK, et al. The impact of sleep disturbances on suicide risk among people living HIV: an eleven-year national cohort. J Affect Disord. 2024;346:122–132. doi:10.1016/j.jad.2023.10.045
31. VanderWeele TJ. Causal mediation analysis with survival data. Epidemiology. 2011;22(4):582–585. doi:10.1097/EDE.0b013e31821db37e
32. Czarnecka-Chrebelska KH, Mukherjee D, Maryanchik SV, Rudzinska-Radecka M. Biological and genetic mechanisms of COPD, its diagnosis, treatment, and relationship with lung cancer. Biomedicines. 2023;11(2). doi:10.3390/biomedicines11020448
33. Parris BA, O’Farrell HE, Fong KM, Yang IA. Chronic obstructive pulmonary disease (COPD) and lung cancer: common pathways for pathogenesis. J Thorac Dis. 2019;11(Suppl 17):S2155–S72. doi:10.21037/jtd.2019.10.54
34. Khusnurrokhman G, Wati FF. Tumor-promoting inflammation in lung cancer: a literature review. Ann Med Surg. 2022;79:104022. doi:10.1016/j.amsu.2022.104022
35. King PT. Inflammation in chronic obstructive pulmonary disease and its role in cardiovascular disease and lung cancer. Clin Transl Med. 2015;4(1):68. doi:10.1186/s40169-015-0068-z
36. Mao H, Zhao X, Sun SC. NF-kappaB in inflammation and cancer. Cell Mol Immunol. 2025;22(8):811–839. doi:10.1038/s41423-025-01310-w
37. Zong Y, Li H, Liao P, et al. Mitochondrial dysfunction: mechanisms and advances in therapy. Signal Transduct Target Ther. 2024;9(1):124. doi:10.1038/s41392-024-01839-8
38. Bae T, Hallis SP, Kwak MK. Hypoxia, oxidative stress, and the interplay of HIFs and NRF2 signaling in cancer. Exp Mol Med. 2024;56(3):501–514. doi:10.1038/s12276-024-01180-8
39. Infantino V, Santarsiero A, Convertini P, Todisco S, Iacobazzi V. Cancer cell metabolism in hypoxia: role of HIF-1 as key regulator and therapeutic target. Int J Mol Sci. 2021;22(11). doi:10.3390/ijms22115703
40. Keith B, Johnson RS, Simon MC. HIF1alpha and HIF2alpha: sibling rivalry in hypoxic tumour growth and progression. Nat Rev Cancer. 2011;12(1):9–22. doi:10.1038/nrc3183
41. Brusselle GG, Joos GF, Bracke KR. New insights into the immunology of chronic obstructive pulmonary disease. Lancet. 2011;378(9795):1015–1026. doi:10.1016/S0140-6736(11)60988-4
42. Wang J, Niu H, Kang J, Liu H, Dong X. Macrophage polarization in lung diseases: from mechanisms to therapeutic strategies. Immunol Invest. 2025;54(6):743–769. doi:10.1080/08820139.2025.2490898
43. Sato S, Nakamura M, Shimizu Y, et al. The impact of emphysema on surgical outcomes of early-stage lung cancer: a retrospective study. BMC Pulm Med. 2019;19(1):73. doi:10.1186/s12890-019-0839-1
44. Gao YH, Guan WJ, Liu Q, et al. Impact of COPD and emphysema on survival of patients with lung cancer: a meta-analysis of observational studies. Respirology. 2016;21(2):269–279. doi:10.1111/resp.12661
45. Lin M, Huang Z, Chen Y, Xiao H, Wang T. Lung cancer patients with chronic obstructive pulmonary disease benefit from anti-PD-1/PD-L1 therapy. Front Immunol. 2022;13:1038715. doi:10.3389/fimmu.2022.1038715
46. Qi Y, Yan Y, Tang D, et al. Inflammatory and immune mechanisms in COPD: current status and therapeutic prospects. J Inflamm Res. 2024;17:6603–6618. doi:10.2147/JIR.S478568
47. Zhao T, Zhang C, Dai H, Li J, Hao L, Liu Y. A comparative study of CT-guided radiofrequency ablation and targeted therapy: intervention efficacy and survival rates in lung cancer patients. Curr Med Imaging. 2025. doi:10.2174/0115734056311827241211092432
48. Ajimizu H, Ozasa H, Sato S, et al. Survival impact of treatment for chronic obstructive pulmonary disease in patients with advanced non-small-cell lung cancer. Sci Rep. 2021;11(1):23677. doi:10.1038/s41598-021-03139-5
49. Lee SJ, Lee J, Park YS, et al. Impact of chronic obstructive pulmonary disease on the mortality of patients with non-small-cell lung cancer. J Thorac Oncol. 2014;9(6):812–817. doi:10.1097/JTO.0000000000000158
50. Tan LE, Razak AM, Lim CS. Association of chronic obstructive pulmonary disease and postresection lung cancer survival: a systematic review and meta-analysis. J Investig Med. 2017;65(2):342–352. doi:10.1136/jim-2016-000059
51. Chen B, Yan X, Wang X, Mao Y. Effectiveness of precise and quantitative rapid pulmonary rehabilitation nursing program for elderly patients with lung cancer during the perioperative period: a randomized controlled trial. Pak J Med Sci. 2023;39(572):–.
52. Fuzhi Y, Dongfang T, Wentao F, et al. Rapid recovery of postoperative pulmonary function in patients with lung cancer and influencing factors. Front Oncol. 2022;12.
53. Yoneyama R, Saji H, Takeuchi S, Ikeda N. Lung cancer and obstructive lung disease in never smokers. J Thorac Dis. 2020;12(8):3934–3939. doi:10.21037/jtd.2020.04.29
54. Semenza GL. HIF-1 mediates metabolic responses to intratumoral hypoxia and oncogenic mutations. J Clin Invest. 2013;123(9):3664–3671. doi:10.1172/JCI67230
55. Cheng FK. The comprehensive cancer centre: development, integration, and implementation. Ann Innov Med. 2024.
56. Whooley PD, Doolin J, Avigan D, et al. Informing the future of multidisciplinary oncology clinics: system-wide insights from an academic-community health system. JCO Oncol Practice. 2025.
57. Di YP, Liu C-H, Chen Z, et al. Inflammation synergistically promotes cigarette smoke carcinogen-induced lung tumorigenesis and determines immunotherapy efficacy. J Immunol. 2020.
58. Riondino S, Rosenfeld R, Formica V, et al. Effectiveness of immunotherapy in non-small cell lung cancer patients with a diagnosis of COPD: is this a hidden prognosticator for survival and a risk factor for immune-related adverse events? Cancers. 2024;16.
59. Yuan J, Li X, Fang N, et al. Perilla Leaf Extract (PLE) attenuates COPD airway inflammation via the TLR4/Syk/PKC/NF-κB pathway in vivo and in vitro. Front Pharmacol. 2022;12.
60. S R, N M, D L, K N, S G, Kk B. Could disease severity and inflammatory markers (IL-6, Hs-CRP, TNF-α) be related to frailty in COPD? A prospective study. J Assoc Physicians India. 2022;70(4):11–12.
61. Yoshizaki K. Pathogenic role of IL-6 combined with TNF-α or IL-1 in the induction of acute phase proteins SAA and CRP in chronic inflammatory diseases. Adv Experiment Med Biol. 2011;691:141–150.
62. Lycan TW, Norton DL, Ohar JA. COPD and immune checkpoint inhibitors for cancer: a literature review. Int J Chronic Obstruct Pulmon Dis. 2024;19:2689–2703.
63. Alkhotani NM, Saud Khoj M, Almahfoudh NE, et al. The role of immunotherapy in managing chronic respiratory conditions with infectious etiologies. J Healthcare Sci. 2024.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Effect of Estrogen Receptor Status on Survival in Breast Cancer Patients in Ethiopia. Retrospective Cohort Study
Belete AM, Aynalem YA, Gemeda BN, Demelew TM, Shiferaw WS
Breast Cancer: Targets and Therapy 2022, 14:153-161
Published Date: 17 June 2022
Cancer Diagnosis and Prognosis After Guillain–Barré Syndrome: A Population-Based Cohort Study
Girma B, Farkas DK, Laugesen K, Skajaa N, Henderson VW, Boffetta P, Sørensen HT
Clinical Epidemiology 2022, 14:871-878
Published Date: 19 July 2022
Normal Gastrointestinal Mucosa at Biopsy and Overall Mortality: Nationwide Population-Based Cohort Study
Ludvigsson JF, Sun J, Olén O, Song M, Halfvarson J, Roelstraete B, Khalili H, Fang F
Clinical Epidemiology 2022, 14:889-900
Published Date: 21 July 2022
Prognostic Properties of the GOLD 2023 Classification System
Brat K, Svoboda M, Zatloukal J, Plutinsky M, Volakova E, Popelkova P, Novotna B, Dvorak T, Koblizek V
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:661-667
Published Date: 20 April 2023
Risk Factors of Gastrointestinal Perforation with a Poor Prognosis
Yuan W, Zhou X, Cai Z, Qiu J, Li X, Tong G
International Journal of General Medicine 2023, 16:4637-4647
Published Date: 16 October 2023