Back to Journals » Breast Cancer: Targets and Therapy » Volume 14
The Effect of Estrogen Receptor Status on Survival in Breast Cancer Patients in Ethiopia. Retrospective Cohort Study
Authors Belete AM, Aynalem YA ![]() , Gemeda BN
, Gemeda BN ![]() , Demelew TM
, Demelew TM ![]() , Shiferaw WS
, Shiferaw WS ![]()
Received 17 March 2022
Accepted for publication 10 June 2022
Published 17 June 2022 Volume 2022:14 Pages 153—161
DOI https://doi.org/10.2147/BCTT.S365295
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Pranela Rameshwar
Abebe Muche Belete,1 Yared Asmare Aynalem,2 Belete Negese Gemeda,2 Tefera Mulugeta Demelew,3 Wondimeneh Shibabaw Shiferaw2
1Department of Biomedical Science, Debre Berhan University, Debre Berhan, Ethiopia; 2Department of Nursing, Debre Berhan University, Debre Berhan, Ethiopia; 3Department of Nursing, Addis Ababa University, Addis Ababa, Ethiopia
Correspondence: Abebe Muche Belete, Department of Biomedical Science, Debre Berhan University, P.O. Box 445, Debre Berhan, Ethiopia, Tel +251 938373278, Email [email protected]
Background: There is wide global variance in survival from breast cancer, both in developed and developing country. However, the effect of estrogen receptor status has not been widely evaluated in Ethiopia where the incidence of breast cancer is rapidly increasing. Hence, the current study aimed to determine the effect of estrogen receptor status on the overall survival of breast cancer patients who were treated at Black Lion Specialized Hospital, Ethiopia.
Methods: In this institution-based retrospective cohort study a total of 368 study participants were included with a one-to-one ratio of estrogen receptor negative to estrogen receptor positive. The main outcome of interest for this study was death due to breast cancer. The authors compared the women with estrogen receptor-positive and estrogen receptor-negative breast cancer for overall survival rate using log rank test. The incidence density rate of mortality was calculated for each exposed and non-exposed variable. The effect of estrogen receptor status on breast cancer mortality was estimated using the Cox proportional hazards model.
Results: The incidence density rate of mortality among breast cancer patients for estrogen receptor positive were found to be 5.48 (95% CI=3.94– 7.64) per 1,000 person years observation; while for estrogen negative receptor status the mortality rate was found to be 10.47 (95% CI=8.19– 13.37) per 1,000 person years observation. In the Cox regression analysis after ful adjustments for confounder variables, the mortality event risk was 32% higher among estrogen receptor negative (HR=1.32; 95% CI=1.08– 2.91) as compared to estrogen receptor positive breast cancer patients.
Conclusion: We have found that the incidence density rate of mortality among breast cancer patients was significantly higher in the estrogen receptor negative groups. Therefore, clinicians should give careful attention to the impact of estrogen receptor negative status on the overall outcome of clients.
Keywords: estrogen receptor status, survival, mortality, breast cancer, Ethiopia
Background
Worldwide breast cancer is ranked as the fifth cause of death among all forms of cancers, and the second most common cancer next to lung cancer.1,2 In addition, globally more than 1.1 million women were newly diagnosed, leading to 1.6% deaths annually from it.3,4 Now it is an emerging public health danger, as the incidence of breast cancer is rapidly increasing in Africa.5 Breast cancer is responsible for one in four diagnosed and one in five cancer deaths among women in Sub-Saharan Africa (SSA).6 Similarly, in Ethiopia breast cancer is the most prevalent cancer in women, and constitutes a major public health concern.7 Moreover, a study conducted in Ethiopia showed that the incidence rate of recurrence among breast cancer was 6.5 per 100 person years follow-up.8
Across the globe, there is a huge difference in survival from breast cancer, thus the variation is due to older age, late stage at diagnosis, and missing stage at diagnosis.9 Despite the enormous evidence regarding the incidence and survival rates of breast cancer in the developed nation, data is not widely available from countries in Africa, Asia, and Central America.10,11
It is well known that the presence of hormone receptors (HR) and human epidermal growth factor receptor (HER)-2 are principal factors determining the clinical management of breast cancer. Besides, improved overall survival rates were found in several subgroups of patients with estrogen receptor (ER) positive tumors compared to ER negative.12 The status of ER expression is commonly used to direct the treatment strategies for breast cancer patients because of their predictive value in prognosis and endocrine therapy (ET) responsiveness. In ER positive early breast cancer, endocrine treatment reduces the recurrence and mortality rates.13 Similarly, studies show that ER positive breast cancer is associated with less aggressive clinical features and a better prognosis because of the benefits from endocrine therapy.14,15 However, positive ER status does not consistently correlate with a favorable prognosis. For instance, among BRCA2 mutation carriers with breast cancer, positive ER status is an adverse prognostic factor.16,17
Evidence suggests that the molecular profiles in breast tumors are generally fixed at inception;18 exposures that influence the risk of developing breast cancer might be related to the tumor molecular profiles that later affect the biology and clinical behavior of the tumors that arise. This has not been widely evaluated in an African population where the incidence of breast cancer is rapidly increasing. In addition, disparities exist in terms of survival between breast cancers among Caucasian women in industrialized and African women in developing countries.
Evidence shows that the survival advantage for women with hormone receptor-positive tumors is enhanced by treatment with adjuvant hormonal and/or chemotherapeutic regimens.19 However, few studies evaluated variations in the risks of breast cancer specific mortality across ER status by either demographic or clinical characteristics. Although the clinical significance of ER evaluation has been well established, the roles of ER on the survival outcomes of single hormone receptor status in breast cancer patients are not well unknown. Therefore, it is clinically significant to assess the ER status in overall survival rate. Nevertheless, limited information is available on the effect of ER status on long-term survival, and evidence to determine whether ER status affects clinical outcomes is lacking. Hence, this study aimed to investigate the difference between the overall survival (OS) of ER positive (ER+) and ER negative (ER-) patients who were treated at Black Lion Specialized Hospital.
Methods
Study Design, Setting, and Population
An institution-based retrospective cohort study was conducted at Black Lion Specialized Hospital, one of the largest teaching hospitals in Ethiopia, with more than 1,000 beds, from March 1 to April 28, 2018. The study populations were all patients who had newly initiated breast cancer treatment at Black Lion Specialized Hospital from January 1, 2012 to January 1, 2018. Women with a confirmed histological diagnosis of invasive breast cancer, newly-treated and enrolled in the required time (ie, January 1, 2012 to January 1, 2018) were included. But, patients with recurrent or metastatic disease at the time of their initial presentation, whose medical charts were not found, had insufficient clinical data (inconclusive histopathological reports), and incomplete documents were excluded.
Sample Size and Sampling Procedure
A total sample size of 368 was calculated using the power exponential formula for survival analysis using the 15-years breast cancer specific survival rate of 70% for those with ER-negative (exposed group) and 77% for those with ER-positive (non-exposed group) breast cancer patients.20 We assumed a 95% confidence level, 80% power, 10% of withdrawal probability, and the sample was computed using Stata version 14. The sample size allocations for exposed and non-exposed were one-to-one ratio. Then, subjects in the exposed groups were selected by consecutive sampling technique, whereas the non-exposed groups were selected using simple random sampling technique. To obtain the necessary information from both exposed and non-exposed groups, the investigator used the medical registration number of patients from the registration book.
Exposure Variable
In the case of our study, study participants were separated into two groups based on their estrogen receptor status at first treatment initiation. The exposed group was ER negative and the non-exposed group was ER positive. Estrogen receptor status was diagnosed using immunohistochemistry. Estrogen receptor expression (ER) was classified as positive/negative. The status of ER was dependent on pathology results in surgery puncture biopsy. Although there were different cut-off values for designation of tumor as ER positive or negative in several literatures; in the current paper ER status was classified as positive if at least 1% of tumor cell nuclei staining was positive (the cells tested have estrogen receptors), as recommended by the different guidelines. Otherwise the test considered the tumor as ER-negative.21
Outcome Measures
In this study the main outcome of interest was death due to breast cancer. Survival time is calculated in months by using the time from the first date of breast cancer treatment initiation to the date of death, date last known to be alive, the date of lost to follow-up (censored), or end of the study (until January 1, 2018), whichever came first. The overall survival (OS) time of patients was defined as the time from treatment initiation until the time of death. Vital status was provided by the clinician affiliated with the center for the subject after review of hospital medical records.
Confounder Variables
The histological grading using the Bloom-Richardson grading system that combined scores for nuclear grade, tubule formation, and mitotic rate,22 the tumor size, axillary nodal involvement, treatment types, menopausal status, presence of comorbidities, body mass index, and staging followed criteria of the American Joint Commission on Cancer (AJCC) Manual for Staging of Cancer23 were the confounder variables.
Data Collection Tool and Quality
The data were collected from patients medical chart with primary breast cancer diagnosis and newly-initiating treatment at the Black Lion Specialized Hospital between January 2012 and January 2018. The data collection tool was developed from previous related literature to assemble necessary information from patients’ medical files. To maintain the quality of the data, training on data abstraction was given to data collectors and supervisors for 1 day before the actual data collection. Pre-test was done on registrations that were not included in the final study for consistency of understanding the review tools and completeness of data items. The collected data were reviewed and checked for completeness every day and before data entry. All completed data collection forms were examined for completeness and consistency during data management, storage, cleaning, and analysis. Three oncology nurses, who were working on the oncology unit, collected the data. The principal investigator of the study controlled the overall activity.
Statistical Analysis
Data were coded, cleaned, entered, and edited using EPI-data Vs 4.2 and exported to STATA Vs 14 statistical software for analysis. The estrogen receptor status (ER) had a certain amount of missing information. For this reason, we used multiple imputation technique to impute ER status.24 Categorical variables were compared using the chi-square test as appropriate. Kaplan–Meier curves were plotted. The ER-positive and ER-negative breast cancer for overall survival rate was compared using log rank test. The incidence density rate of mortality was calculated for each exposed and non-exposed variables. The effect of estrogen receptor status on breast cancer mortality was estimated using the Cox proportional hazards model. Adjusted Hazard ratios (AHRs), with 95% CIs were used to determine the independent effect of ER status on time to death of breast cancer patients. Cox-proportional hazard model assumption was checked using the Schoenfeld residual test and all variables showed a P-value >0.10, which fulfilled the assumption. Lastly, a P-value of less than 0.05 was considered as significant.
Results
Sociodemographic Characteristics of Study Participants
There was no difference under age category of less than 40 years at diagnosis of breast cancer between groups (51.08% vs 48.9%, P=0.91). In the present study, we did not find a significant difference in terms of menopause status between groups (P=0.90). There was no difference in place of residence between ER positive and ER negative women; however, ER positive women were more likely to live in Addis Ababa (58.69% vs 55.97%) (Table 1).
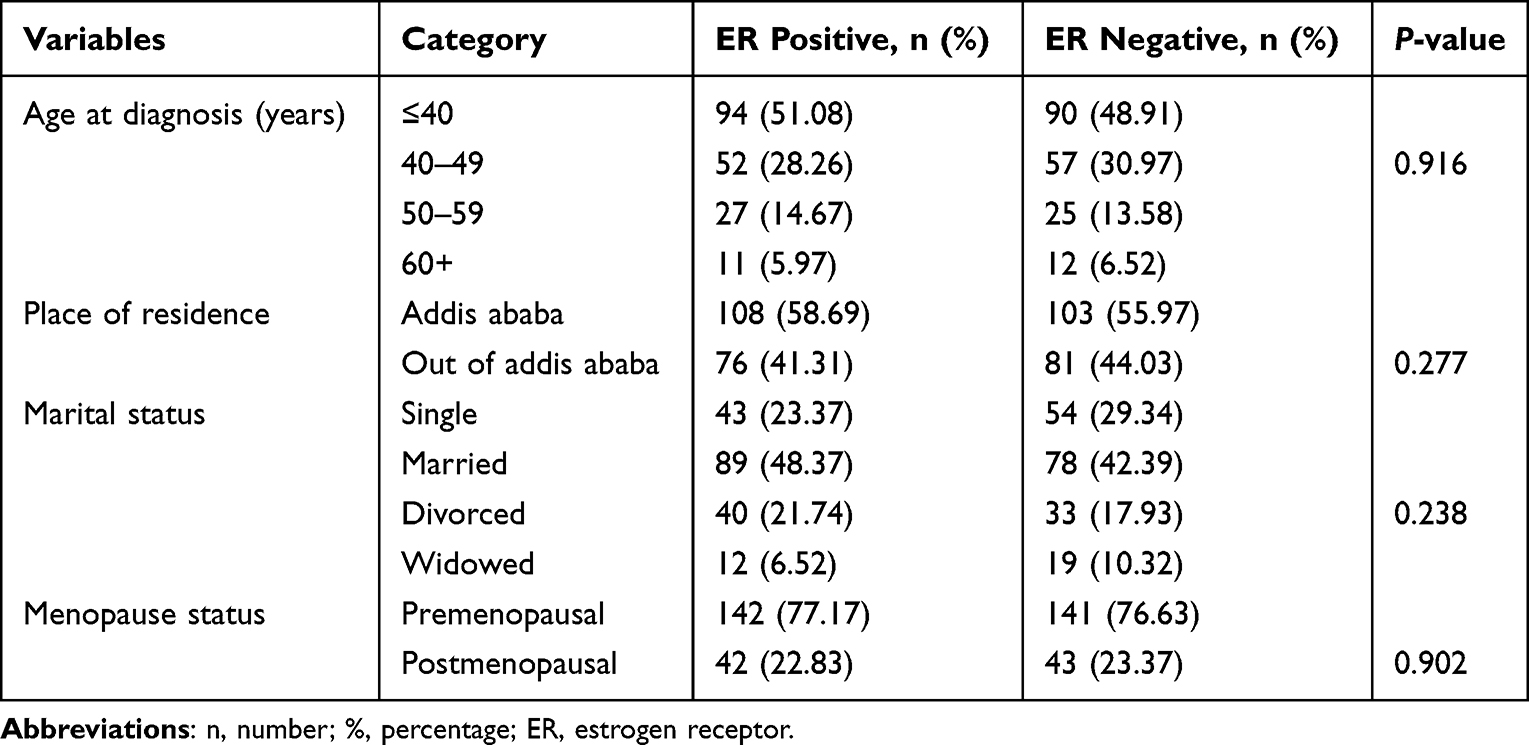 |
Table 1 Comparison of Baseline Sociodemographic Characteristics, According to ER Status |
Clinical and Treatment Related Characteristics
Estrogen receptor positive women had higher early stage tumor (39.13% vs 27.17%, P=0.015), moderate differentiation (55.43% vs 44.56%, P<0.01), negative node status (95.1% vs 29.89%, P<0.001), taken endocrine therapy (70.1% vs 57.6%, P=0.013), and free deep surgical margin (84.24% vs 63.58%, P<0.001) compared to ER negative women. There was no difference in baseline comorbidity between ER positive and ER negative women. However, ER positive women were more likely to not have baseline comorbidity (68.47% vs 63.04%) disease. Estrogen receptor positive women were found to be more likely to have a tumor size of less than or equal to 2.5 cm (63.04% vs 52.71%) compared to ER negative women. Estrogen receptor negative women were found to have more histology type of invasive ductal carcinoma (70.65% vs 66.3%) disease compared to ER positive women (Table 2).
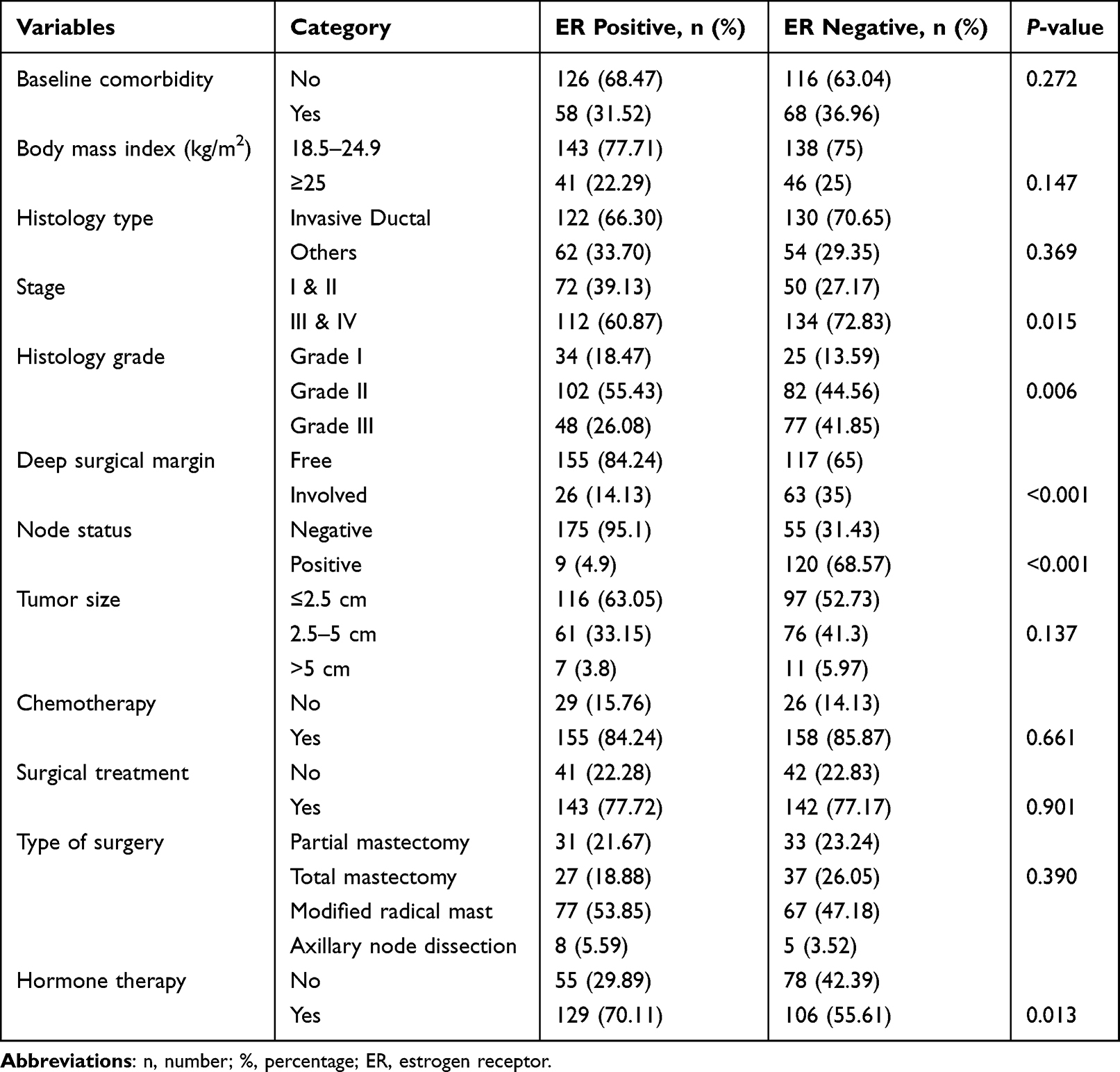 |
Table 2 Comparison of Baseline Clinical and Treatment Related Characteristics, According to ER Status |
The Effect of Estrogen Receptor Status on Breast Cancer Survival
We found that the incidence density rates of mortality among breast cancer patients were varied due to estrogen receptor status. The estrogen receptor positive with the total observation of 6,382.93 person time the mortality rate of breast cancer patients were found to be 5.48 (95% CI=3.94–7.64) per 1,000 person years observation. Whereas the mortality rate of estrogen receptor negative breast cancer patients was found to be 10.47 (95% CI=8.19–13.37) per 1,000 person years observation with the total observation of 6,113.73 person time. Besides, the overall survival rate of breast cancer patients on estrogen positive receptors was 41.51% at 6 years follow-up . However, estrogen negative receptor patients overall survival rate was found to be 21.01% at 6 years follow-up. Median follow-up time for ER negative women was 52 months and for ER positive women was 61 months. Overall median survival for the entire cohort was 58.7 months (Figure 1).
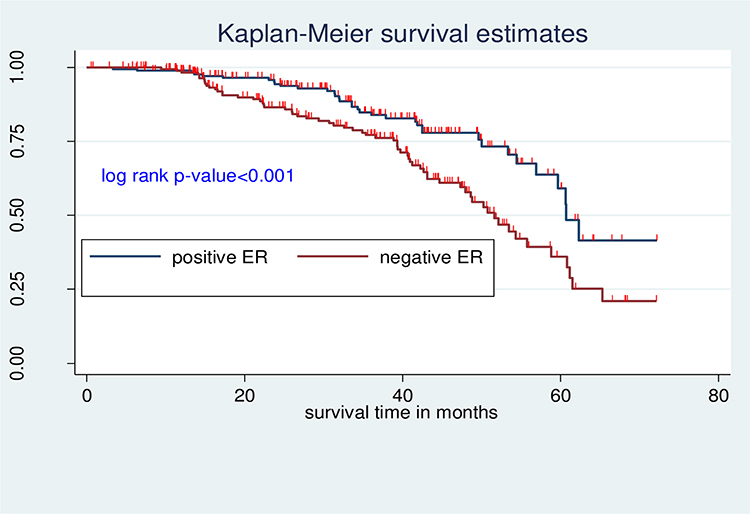 |
Figure 1 The effect of estrogen receptor status on overall survival of breast cancer in Ethiopia. |
Predictors of Breast Cancer Death by Estrogen Receptor Status
In the Cox regression analysis for the incidence of death, estrogen receptor negative women had a higher risk of mortality with an event risk of 95% (HR=1.95; 95% CI=1.29–2.94) compared with ER positive in the unadjusted model. And after full adjustments for age, clinical stage, baseline comorbidity, histological grade, surgical margin, node status, type of surgery, chemotherapy, hormone therapy, tumor size, histology type, and place of residence, the mortality event risk was 32% higher among ER negative women (HR=1.32; 95% CI=1.08–2.91) (Table 3).
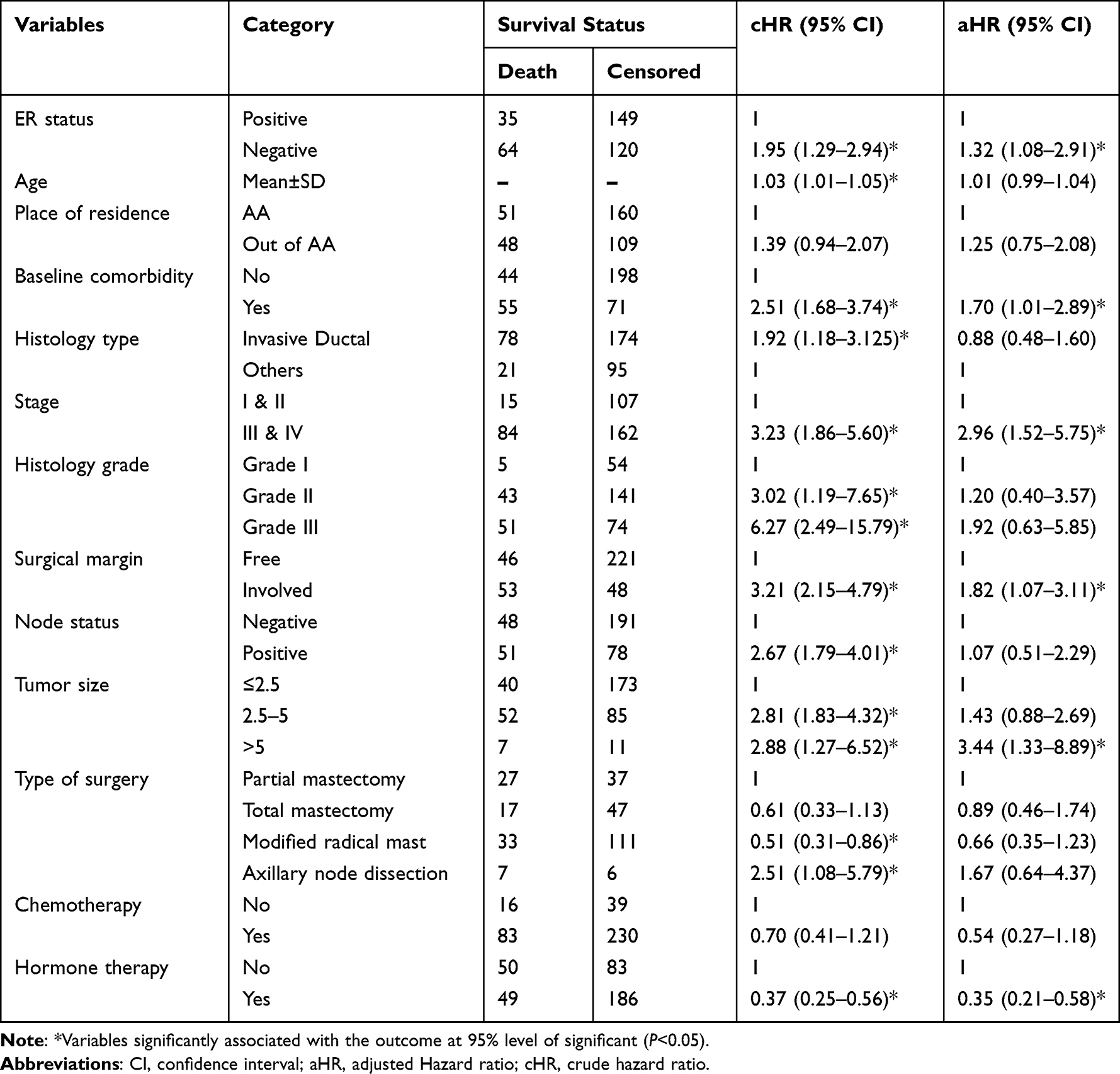 |
Table 3 Cox Regression Results for Death According to Estrogen Receptor Status |
Discussion
In this retrospective cohort study, the findings demonstrated that negative estrogen receptor is associated with an increased risk of incidence of mortality in breast cancer patients. In estrogen receptor negative patients, the 6-year cumulative survival rate was found to be 21.01%, lower compared to ER positive patients (41.51%), and the difference was also statistically significant.
The baseline clinical characteristics demonstrated ER positive women had a higher proportion of early stage tumor, moderate differentiation, negative node status, and free deep surgical margin compared to ER negative women. This finding compared with other previously published studies that reported results that were similar to ours.20,25 In our study ER negative tumors had significantly higher grade tumors compared to ER positive tumors. This is consistent with previous literature and ER negative tumors are more aggressive and carry a poorer prognosis.26 The possible justification is that the ER negative group would have higher grade tumors. This may be a factor of underlying genetic influence (somatic or germline mutations). Besides, a lack of significant differences between ER status and socio-demographic risk factors was observed.
In the Cox regression analyses, the risk of mortality was higher in ER negative compared with ER positive patients after all the adjustments. This is consistent with those of previous studies.27,28 Moreover, a study done on more than 2,450 participants in Tianjin revealed that ER negative women had an approximately 2-fold increased risk of mortality compared to ER positive women.27 In addition, a study on 482 study participants at Zhejiang showed that ER negative patients had nearly 3-fold increased risk of mortality, compared to ER positive patients.28 Furthermore, a cohort study conducted in the United States showed that ER negative patients had a 2.6-fold to 3.1-fold increased risk of mortality compared to ER positive patients.15 However, other evidence showed that positive ER-status is a strong adverse prognostic factor for women diagnosed before age 40 years and women with BRCA2 mutations.16,17,20
The reason for the discrepancy between our and other studies remains unclear. However, this may be attributed to the fact that estrogen status was probably underreported in women. It was also possible that our study had a smaller sample size. Many of the other studies included had a larger number of patients and a longer follow-up time.
It is recognized that ER-positive tumors should be treated with adjuvant tamoxifen or aromatase inhibitors, because anti-hormonal therapy is associated with an important survival benefit. Women with estrogen-positive breast cancer treated with 5 years of adjuvant tamoxifen have a 29% decreased risk of death from the disease and a 50% decreased risk for contralateral breast cancer.13
Limitations
The following limitations should be considered for further studies. First, some of the behavioral factors were not investigated due to incomplete information from the chart. Second, the data were highly liable to selection bias, hence incomplete charts had excluded. Third, some predictor variables baseline information among the exposed and non-exposed group has a significant difference and this may leadto informational bias.
Conclusion
In this study, after adjustment for other clinical factors and treatments, women with an estrogen receptor negative breast cancer had worse short-term survival compared to women with positive estrogen receptor. Therefore, future policy and clinician programmers should consider the impact of ER status more carefully. Furthermore, additional studies are required to determine to what extent chemotherapy is effective in ER negative breast cancer.
Abbreviations
AHRs, adjusted hazard ratios; AJCC, American Joint Commission on Cancer; ER+, estrogen receptor positive, ER, estrogen receptor negative; ET, endocrine therapy; SSA, Sub-Saharan Africa; HR, hormone receptors; HER2, human epidermal growth factor receptor; OS, overall survival.
Data Sharing Statement
All relevant data are within the paper. There is no separate data set to share.
Ethical Approval and Consent to Participate
The study was approved by Institutional Review Boards (IRB) at Addis Ababa University, College of Health Science (IRB protocol: aau/chs/ahnsg11/2018) and consent had been waived by ethical board. They are conducted in compliance with the Ethical Guidelines for Medical and Health Research Involving Human Subjects and the ethical principles of the Declaration of Helsinki. Then, a permission letter has been obtained from Black Lion Specialized Hospital, adult oncology unit. The study was conducted without individual informed consent as the study relied on retrospective data collected as part of routine patient care. In this retrospective study, no patient identifiers were used and data were anonymized. To keep confidentiality, names and other personal identifiers were not included in the data collection tool.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no conflicts of interest in relation to this work.
References
1. Ferlay J, Soerjomataram I, Ervik M, et al. GLOBOCAN 2012 v1. 0, Cancer Incidence and Mortality Worldwide: IARC CancerBase No. 11 [Internet]. Lyon, France: International Agency for Research on Cancer. globocan iarc fr/Default aspx 2014; 2013.
2. World Health Organization (2017). Cancer facts & figures 2016–2017. Available from: http://www.who.int/mediacentre/factsheets/fs297/en/.
3. American Cancer Society. Breast Cancer Facts & Figures 2017–2018. Atlanta: American Cancer Society I; 2018.
4. Lan N, Laohasiriwong W, Stewart J. Survival probability and prognostic factors for breast cancer patients in Vietnam. Glob Health Action. 2013;6(1):18860. doi:10.3402/gha.v6i0.18860
5. Ferlay J, Dikshit EM, Eser R, et al. Cancer incidence and mortality worldwide: IARC CancerBase; 2012:11.
6. McKenzie F, Zietsman A, Galukande M, et al. African Breast Cancer—Disparities in Outcomes (ABC-DO): protocol of a multicountry mobile health prospective study of breast cancer survival in sub-Saharan Africa. BMJ open. 2016;6(8):e011390. doi:10.1136/bmjopen-2016-011390
7. Abate S, Yilma Z, Assefa M, Tigeneh W. Trends of breast cancer in Ethiopia. Int J Cancer Res Mol Mech. 2016;2(1):1.
8. Shiferaw WS, Aynalem YA, Akalu TY, Demelew TM. Incidence and predictors of recurrence among breast cancer patients in black lion specialized hospital adult oncology unit, Addis Ababa, Ethiopia: retrospective follow-up study with survival analysis. J Cancer Prev. 2020;25(2):111. doi:10.15430/JCP.2020.25.2.111
9. Walters S, Maringe C, Butler J, et al. Breast cancer survival and stage at diagnosis in Australia, Canada, Denmark, Norway, Sweden and the UK, 2000–2007: a population-based study. Br J Cancer. 2013;108(5):1195–1208. doi:10.1038/bjc.2013.6
10. Kene TS, Odigie VI, Yusufu LM, Yusuf BO, Shehu SM, Kase JT. Pattern of presentation and survival of breast cancer in a teaching hospital in north Western Nigeria. Oman Med J. 2010;25(2):104. doi:10.5001/omj.2010.29
11. Mensah AC, Yarney J, Nokoe SK, Opoku S, Clegg-Lamptey J. Survival outcomes of breast cancer in Ghana: an analysis of clinicopathological features. Open Access Library J. 2016;3:1–11.
12. Kolarova I, Dusek L, Ryska A, et al. Impact of hormone receptor status on the behaviour of HER2+ breast cancer. In Vivo. 2020;34(6):3441–3449. doi:10.21873/invivo.12183
13. Group EBCTC. Relevance of breast cancer hormone receptors and other factors to the efficacy of adjuvant tamoxifen: patient-level meta-analysis of randomised trials. Lancet. 2011;378(9793):771–784. doi:10.1016/S0140-6736(11)60993-8
14. Colditz GA, Rosner BA, Chen WY, Holmes MD, Hankinson SE. Risk factors for breast cancer according to estrogen and progesterone receptor status. J Natl Cancer Inst. 2004;96(3):218–228. doi:10.1093/jnci/djh025
15. Dunnwald LK, Rossing MA, Li CI. Hormone receptor status, tumor characteristics, and prognosis: a prospective cohort of breast cancer patients. Breast Cancer Res. 2007;9(1):1–10. doi:10.1186/bcr1639
16. Jonasson JG, Stefansson OA, Johannsson OT, et al. Oestrogen receptor status, treatment and breast cancer prognosis in Icelandic BRCA2 mutation carriers. Br J Cancer. 2016;115(7):776–783. doi:10.1038/bjc.2016.249
17. Metcalfe K, Lynch HT, Foulkes WD, et al. Oestrogen receptor status and survival in women with BRCA2-associated breast cancer. Br J Cancer. 2019;120(4):398–403. doi:10.1038/s41416-019-0376-y
18. Sorlie T, Tibshirani R, Parker J, et al. Repeated observation of breast tumor subtypes in independent gene expression data sets. Proc Natl Acad Sci U S A. 2003;100(14):8418–8423. doi:10.1073/pnas.0932692100
19. Fisher B, Jeong J-H, Anderson S, Wolmark N. Treatment of axillary lymph node–negative, estrogen receptor–negative breast cancer: updated findings from national surgical adjuvant breast and bowel project clinical trials. J Natl Cancer Inst. 2004;96(24):1823–1831. doi:10.1093/jnci/djh338
20. Sopik V, Sun P, Narod SA. The prognostic effect of estrogen receptor status differs for younger versus older breast cancer patients. Breast Cancer Res Treat. 2017;165(2):391–402. doi:10.1007/s10549-017-4333-2
21. Glück S, Russell C, O’Shaughnessy J, et al. Relationship between survival and estrogen receptor status in patients with metastatic breast cancer treated with capecitabine and docetaxel: an exploratory data analysis.
22. Bloom H, Richardson W. Histological grading and prognosis in breast cancer: a study of 1409 cases of which 359 have been followed for 15 years. Br J Cancer. 1957;11(3):359. doi:10.1038/bjc.1957.43
23. Edge SB, Compton CC. The American Joint Committee on Cancer: the 7th edition of the AJCC cancer staging manual and the future of TNM. Ann Surg Oncol. 2010;17(6):1471–1474. doi:10.1245/s10434-010-0985-4
24. White IR, Royston P, Wood AM. Multiple imputation using chained equations: issues and guidance for practice. Stat Med. 2011;30(4):377–399. doi:10.1002/sim.4067
25. Li Y, Yang D, Yin X, et al. Clinicopathological characteristics and breast cancer–specific survival of patients with single hormone receptor–positive breast cancer. JAMA network open. 2020;3(1):e1918160–e1918160. doi:10.1001/jamanetworkopen.2019.18160
26. Galukande M, Wabinga H, Mirembe F, Karamagi C, Asea A. Difference in Risk Factors for Breast Cancer by ER Status in an Indigenous African Population. International Scholarly Research Notices 2013; 2013.
27. Zhao W, Sun L, Dong G, Wang X, Jia Y, Tong Z. Receptor conversion impacts outcomes of different molecular subtypes of primary breast cancer. Ther Adv Med Oncol. 2021;13:17588359211012982. doi:10.1177/17588359211012982
28. Ding Y, Ding K, Qian H, et al. Impact on survival of estrogen receptor, progesterone receptor and Ki-67 expression discordance pre-and post-neoadjuvant chemotherapy in breast cancer. PLoS One. 2020;15(4):e0231895. doi:10.1371/journal.pone.0231895
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Epidemiological Characteristics of Chronic Viral Hepatitis in Kazakhstan: Data from Unified Nationwide Electronic Healthcare System 2014–2019
Ashimkhanova A, Syssoyev D, Gusmanov A, Yesmembetov K, Yespotayeva A, Abbay A, Nurpeissova A, Sarria-Santamera A, Gaipov A
Infection and Drug Resistance 2022, 15:3333-3346
Published Date: 27 June 2022
COVID-19 Case Fatality Rate and Factors Contributing to Mortality in Ethiopia: A Systematic Review of Current Evidence
Girma D, Dejene H, Adugna L, Tesema M, Awol M
Infection and Drug Resistance 2022, 15:3491-3501
Published Date: 4 July 2022
Survival Status and Predictors of Mortality Among Women with Uterine Rupture at Public Hospitals of Eastern Ethiopia. Semi-Parametric Survival Analysis
Alemu A, Yadeta E, Deressa A, Debella A, Birhanu A, Heluf H, Mohammed A, Ahmed F, Beyene A, Getachew T, Eyeberu A
International Journal of Women's Health 2023, 15:443-453
Published Date: 25 March 2023
Progranulin and Breast Cancer Mortality: 13-Year Follow-Up of a Cohort Study
Koo DH, Lee KS, Sim SH, Chae H, Lee EG, Han JH, Jung SY, Lee S, Kang HS, Lee ES, Park CY, Oh SW
Breast Cancer: Targets and Therapy 2023, 15:251-261
Published Date: 14 April 2023
Risk of Subsequent Breast Cancer in Women with Early Stage HER2-Positive Breast Cancer in a Large Community Health Plan
Haque R, Chen LH, Oestreicher N, Lalla D, Chlebowski RT
Breast Cancer: Targets and Therapy 2023, 15:637-645
Published Date: 16 August 2023