")
Back to Journals » Journal of Inflammation Research » Volume 17
Assessment of Immune Status in Patients with Mismatch Repair Deficiency Endometrial Cancer
Authors Ma J , Lin J, Lin X , Ren Y, Liu D, Tang S, Huang L, Xu S, Mao X , Sun P
Received 6 December 2023
Accepted for publication 20 March 2024
Published 2 April 2024 Volume 2024:17 Pages 2039—2050
DOI https://doi.org/10.2147/JIR.S453337
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ning Quan
Jincheng Ma,1– 3,* Jiansong Lin,4,* Xite Lin,1– 3 Yuan Ren,1– 3 Dabin Liu,5 Shuting Tang,1– 3 Leyi Huang,1– 3 Shuxia Xu,4 Xiaodan Mao,1– 3 Pengming Sun1– 3,5
1Laboratory of Gynecologic Oncology, Fujian Maternity and Child Health Hospital College of Clinical Medicine for Obstetrics & Gynecology and Pediatrics, Fujian Medical University, Fuzhou, Fujian Province, People’s Republic of China; 2Key Laboratory of Women and Children’s Critical Diseases Research, Fujian Maternity and Child Health Hospital College of Clinical Medicine for Obstetrics & Gynecology and Pediatrics, Fujian Medical University, Fuzhou, Fujian Province, People’s Republic of China; 3Fujian Clinical Research Center for Gynecological Oncology, Fujian Maternity and Child Health Hospital (Fujian Obstetrics and Gynecology Hospital), Fuzhou, Fujian Province, People’s Republic of China; 4Department of Pathology, Fujian Maternity and Child Health Hospital College of Clinical Medicine for Obstetrics & Gynecology and Pediatrics, Fujian Medical University, Fuzhou, Fujian Province, People’s Republic of China; 5Department of Gynecology, Fujian Maternity and Child Health Hospital College of Clinical Medicine for Obstetrics & Gynecology and Pediatrics, Fujian Medical University, Fuzhou, Fujian Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaodan Mao; PengMing Sun, Email [email protected]; [email protected]
Objective: This study introduced a novel subtype classification method for endometrial cancer (EC) with mismatch repair deficiency (MMRd) by employing immune status and prognosis as the foundational criteria. The goal was to enhance treatment guidance through precise subtype delineation.
Methods: Study Cohort: This study encompassed a cohort of 119 patients diagnosed with MMRd-EC between 2015 and 2022. Analyses using t-tests and Mann–Whitney U-tests were performed to assess prognostic markers and peripheral blood immune cell profiles in patients with MutS deficiency (MutS-d) versus those with MutL deficiency (MutL-d). Logistic regression analysis was used to identify independent risk factors. Bioinformatics Analysis: An online database was used to assess the prognostic implications, immune cell infiltration, and immune checkpoint involvement associated with the deficiency of MutS versus MutL in EC.
Results: Patients with MutL-d exhibited heightened risk factors, including elevated cancer grade and increased myometrial invasion, leading to poorer prognosis and shorter overall survival and progression-free survival. Regarding systemic immune status, patients with MutL-d demonstrated decreased peripheral blood lymphocyte percentage, lymphocyte count, and CD8+ T cell percentage. For local immunity, the infiltration of natural killer cells, CD8+ T cells, and cytotoxic T lymphocytes in the tumor tissue was reduced in patients with MutL-d. Additionally, patients with MutL-d exhibited lower expression of immune checkpoint markers. The composition of immune subtypes and survival outcomes also indicate that patients with MutL-d have a poorer immune status and prognosis than the patients with MutS-d.
Conclusion: Patients with MMRd-EC can be subclassified according to MutS or MutL deficiency. Patients with MutS-d exhibited better immune status, prognosis, and immunotherapy benefits than those with MutL-d. These results can help guide patients to a more precise treatment.
Keywords: endometrial cancer, mismatch repair-deficiency, immune, molecular classification, MutL, MutS
Introduction
Endometrial cancer (EC) is a prevalent malignant epithelial tumor, and its incidence is increasing every year.1 The heterogeneity of EC is evident from the diverse genetic and molecular profiles of cancer cells. Traditional classification methods often lack the ability to adequately address tumor heterogeneity, thereby, limiting their clinical applicability. Molecular typing of EC via classifications, such as ProMisE and TCGA, plays a vital role in prognosis prediction and facilitation of precision treatments.2,3
Mismatch repair deficiency (MMRd)-EC account for 29% of all EC cases. Therefore, patients with MMRd-EC may benefit from immunotherapy.4,5 However, real-world data suggest that the response to immune checkpoint blockade is inconsistent.6 The heterogeneity observed in MMRd-EC necessitates the creation of more refined subgroups to effectively guide clinical treatment.
Mismatch repair genes comprise two distinct families: MutS family members, MSH2 and MSH6 that recognize and pinpoint mismatched bases, whereas MutL family members, MLH1 and PMS2, facilitate the hydrolysis of mismatched regions.7 Deletions in different mismatch repair families may result in different clinical outcomes.8 However, the relationship between specific deficiencies in various mismatch repair family members and their association with EC remains unclear.
Our study aimed to elucidate the prognosis and immunological characteristics inherent to MutS-d and MutL-d with the ultimate goal of establishing an innovative method for subgrouping MMRd-EC. By delineating these subgroups, we can refine the precise treatment strategies to tailor them according to the needs of the patients diagnosed with MMRd-EC.
Methods
Patient Selection
Cohort data: This retrospective study comprised 1240 patients who underwent initial hysterectomy for EC with immunohistochemical pathology at Fujian Provincial Maternity and Children’s Hospital between January 2015 and January 2022. Exclusion criteria were as follows: (1) incomplete clinical and pathological data (n = 122); (2) absence of molecular typing marker tests (n = 558); (3) absence of MMRd diagnosis (n = 397); and (4) the presence of other types of tumors or pre-carcinomas (n = 10), hematological and immune system disorders (n = 4), acute inflammation (n = 3), or non-endometrioid adenocarcinomas (n = 6) within the subset of patients diagnosed with MMRd (n = 163). After applying these criteria, a final sample of 119 patients was included. This retrospective study was approved by the Ethics Committee of Fujian Maternal and Child Health Hospital. Bioinformatics analysis: MMRd-EC patient data were obtained from TCGA database and various online sources (http://bioinfo.life.hust.edu.cn/GSCA, http://cis.hku.hk/TISIDB/index.php).
Data Collection
Demographic and clinical indicators were retrieved from the healthcare information system of the Fujian Maternal and Child Health Hospital. Pathological information included the International Federation of Gynecology and Obstetrics stage, histologic type, tumor grade, deep myometrial invasion (DMI), lymphovascular space invasion (LVSI), lymph node metastasis (LNM), and expression levels of estrogen receptor (ER), progesterone receptor (PR), Ki67, Vimentin, P16, MLH1, PMS2, MSH2, and MSH6. Peripheral hematology parameters including white blood cell count, percentage of neutrophils (Neu%), percentage of lymphocytes (Lym%), percentage of monocytes (Mon%), neutrophil count (Neu), lymphocyte count (Lym), percentage of monocyte (Mon%), percentage of B cells (B cell %), percentage of T cells (T cell %), percentage of NK cells (NK cell %), percentage of helper T cells (CD4+ T cell %), percentage of suppressor T cells (CD8+ T cell %), T-helper/T-suppressor ratio (TH/TS, CD4/CD8), and cancer antigen 125 (CA125). Blood tests were performed one week before surgery. Bioinformatics data including survival curves, immune cell infiltration, immune checkpoints, and immune subtypes were analyzed using TCGA, TISIDB, and GSCA online databases.
MMRd and Subgroup Diagnosis
The ProMisE classification was performed as described in the original article.2 Immunohistochemistry was conducted to identify MMR proteins (MLH1, MLH2, MSH6, and PMS2) in the EC tissues. Samples were classified into MutS (MSH2/MSH6) deficiency and MutL (MLH1/PMS2) deficiency groups according to protein expression status.7 Patients with protein deficiencies in both the MutS and MutL families were excluded.
Statistical Analysis
Statistical analyses were conducted using SPSS (version 22.0; IBM Corp., Armonk, NY, USA) and R version 4.0.2. The data were visualized using the R package ggplot2. Continuous variables were analyzed using the Student’s t-test or Mann–Whitney U-test. Categorical variables are presented as frequencies and percentages. Receiver operating characteristic (ROC) curves were generated to determine the optimal cutoff values for the continuous variables. Categorical variables were analyzed using the chi-squared test or Fisher’s exact test. Multiple logistic regression analysis was conducted to explore the binary associations. p<0.05 was considered to be statistically significant.
Results
Patients with MutL-d-EC Have More Risk Factors for Poor Prognosis and a Worse Survival Prognosis Than Those with MutS-d-EC
This retrospective study included 1240 patients with EC. After screening, 119 patients with MMRd-EC were included (Figure 1). We classified them into MutL-d (n=83) and MutS-d (n=36) groups based on their deficiencies in mismatch repair. The patients with MutL-d had higher cancer grade (p=0.006) and more DMI (p=0.010), indicating a higher prevalence of poor prognostic risk factors (Table 1). As no instances of death or disease progression were reported during the follow-up period for the included patients, we used the TCGA database to analyze the impact of deficiency on survival. In patients with EC, those carrying MutL-d were significantly associated with shorter overall survival (OS) (p=0.041) and progression-free survival (PFS) (p=0.01) compared with those carrying MutS-d (Figure 2).
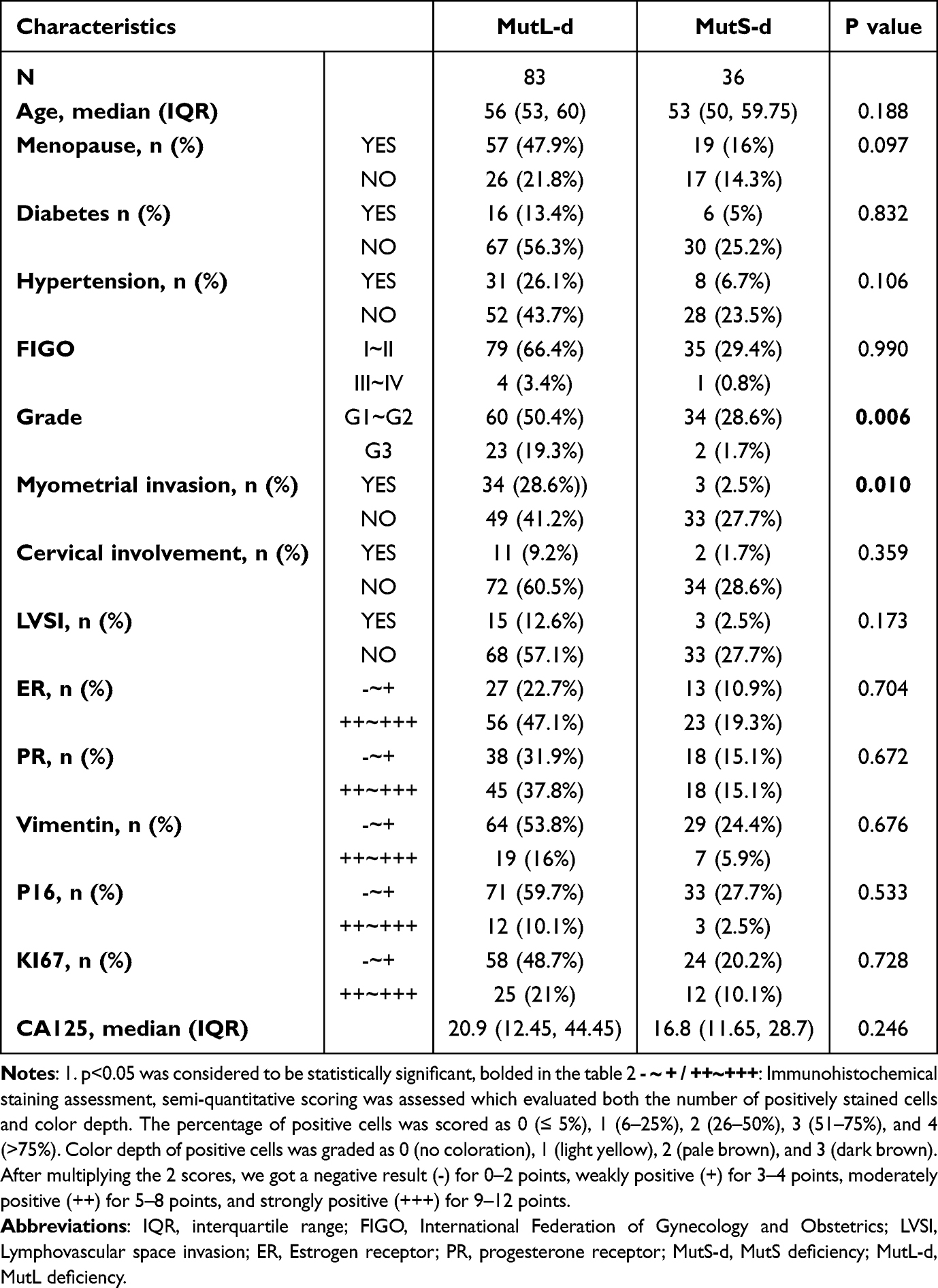 |
Table 1 Baseline Characteristics of Patients with MutL-d and MutS-d EC |
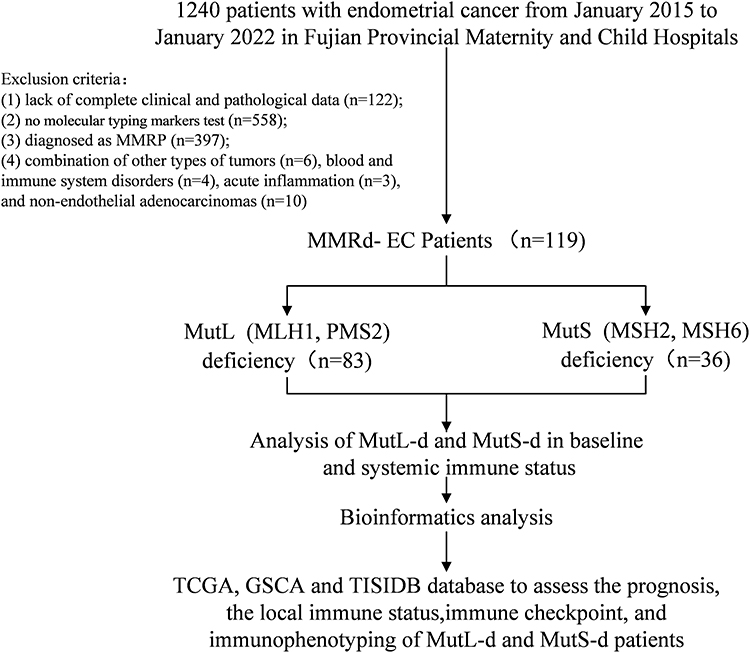 |
Figure 1 Study cohort flowchart. Abbreviations: EC, Endometrial cancer; MMRd, Mismatch repair deficiency; MutS-d, MutS deficiency; MutL-d, MutL deficiency; TCGA, The Cancer Genome Atlas; GSCA, Gene Set Cancer Analysis. |
 |
Figure 2 Prognosis of MutS-d and MutL-d. (A) OS was shorter in the MutL-d group, (B) DFI in the MutL-d and MutS-d groups, (C) DSS in the MutL-d and MutS-d groups, (D) PFS was shorter in the MutL-d group. Abbreviations: MutS-d, MutS deficiency; MutL-d, MutL deficiency; OS, overall survival; DSS, disease-specific survival; DFI, disease free interval; PFS, progression-free survival. Note: p<0.05 indicates significant differences. |
Characteristics of Systemic Immune Status of MutL-d and MutS-d Subgroups
The status of peripheral blood immune cells represents the systemic immune status. Analysis of the selected patients’ peripheral blood immune cells showed a significantly lower lymphocyte percentage (p=0.041), lymphocyte count (p=0.005), and monocyte count (p=0.039) in the MutL-d group (Figure 3A and B). Subsequently, differential indicators of the selected patients were included in a multifactorial analysis. ROC curves were generated to determine the optimal cutoff values for continuous variables (Figure 3C–E). Logistic regression analysis confirmed that low lymphocyte count and lymphocyte percentage, and increased myometrial infiltration were independent risk factors for MutL-d (all p<0.05) (Figure 3F). Considering the lymphocyte differences between the two groups, we analyzed the peripheral blood lymphocyte subtypes of the patients in detail. Patients with MutL-d had lower levels of CD8+ T cells (%) (p=0.022), whereas the CD4+ T cells (%) (p=0.005) and TH/TS (p=0.005) were higher than those in patients with MutS-d (Figure 4A). ROC curve analysis and logistic regression confirmed that a low percentage of CD8+ T cells (%) was an independent risk factor for MutL-d (Figure 4B–E).
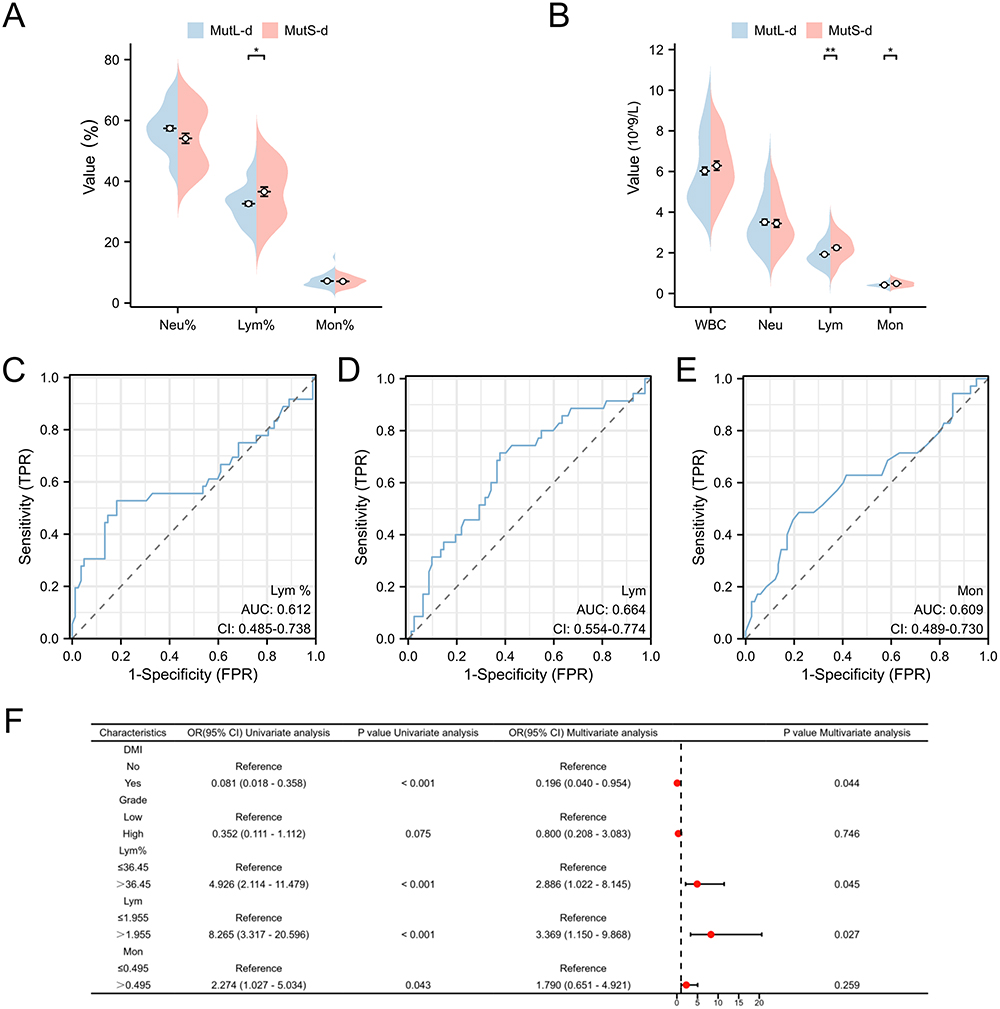 |
Figure 3 Low Lym%, Low Lym, and further DMI are independent risk factor for MutL-d group. (A and B) Peripheral blood immune cells in the MutL-d and MutS-d groups; (C–E) ROC curves were implemented to obtain the cutoff value of Lym%, Lym and Mon between MutL-d and MutS-d (The solid blue line is the ROC curve and the dashed black line is the reference line). The cutoff values for these indicators were identified as cut off (Lym%) =36.45, cut off (Lym)=1.955, and cut off (Mon) =0.495; (F) Logistic regression analyses for the MutL-d group, Low Lym%, Low Lym and further DMI were independent risk factors. Abbreviations: WBC, white blood cell count; Neu%, percentage of neutrophils; Lym%, percentage of lymphocytes; Mon%, percentage of monocytes; Neu, neutrophil count; Lym, lymphocyte count; Mon%, monocyte count; CI, Confidence intervals; AUC, Areas under the curve; DMI, Deep myometrial invasion; ROC, Receiver operating characteristic. Notes: *p < 0.05; **p < 0.01; p<0.05 indicates significant differences. |
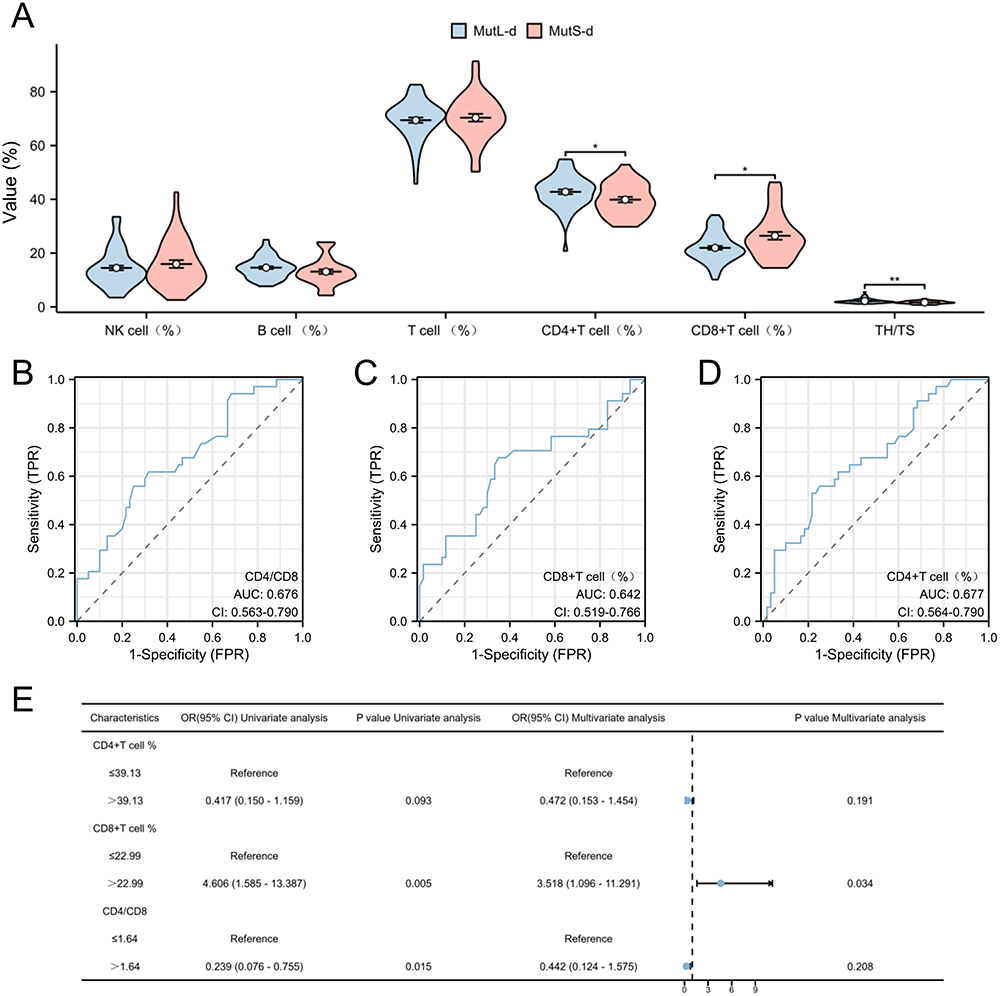 |
Figure 4 Low CD8+ T cell (%) is an independent risk factor for MutL-d group. (A) Lymphocyte status in the MutL-d and MutS-d groups; (B–D) ROC curves were implemented to obtain the cutoff value of CD4/CD8, CD8+ T cell % and CD4+ T cell % between MutL-d and MutS-d (The solid blue line is the ROC curve and the dashed black line is the reference line). The cutoff values for these indicators were identified: cutoff (CD4/CD8) =1.64, cutoff (CD8+ T cell %) =22.99, cutoff (CD4+ T cell %) =39.13; (E) Logistic regression analyses for MutL-d group, Low CD8+ T cell (%) is an independent risk factor. Abbreviations: B cell %, percentage of B cells; T cell %, percentage of T cells; NK cell %, percentage of NK cells; CD4+ T cell %, percentage of helper T cells, CD8+ T cell %, percentage of suppressor T cells, TH/TS, T-helper/T-suppressor ratio; CI, Confidence intervals; AUC, Areas under the curve. Notes: *p < 0.05; **p < 0.01; p<0.05 indicates significant differences. |
Features of Local Immune Infiltration of MutL-d and MutS-d Subgroups
Immune cell infiltration was assessed using the TCGA database. The numbers of NK cells (p<0.05) and CD8+ T cells (p<0.05) were lower in patients with MutL-d-EC than in those with MutS-d (Figure 5A). Subsequently, we analyzed the CD4+ and CD8+ T cell subtypes. Patients with MutL-d-EC had lower levels of CTLs and higher levels of naïve-like CD8+ T cells (Figure 5B). To investigate the factors contributing to these differences in immune infiltration, we analyzed the impact of single-gene deletions on immune infiltration. Correlation analysis conducted using the TISIDB database revealed a stronger negative correlation between MSH2 and MSH6 and chemokines and chemokine receptors, including CCL14, CCL17, CCL22, CCL24, CXCL2, CXCL14, CXCL17, XCL2, CCR7, CXCR1, CXCR2, CXCR3, and CXCR5. Therefore, when MSH2 and MSH6 (MutS) are deleted, the expression levels of chemokines and their receptors increase. This recruits more immune cells. (Figure 5C and D)
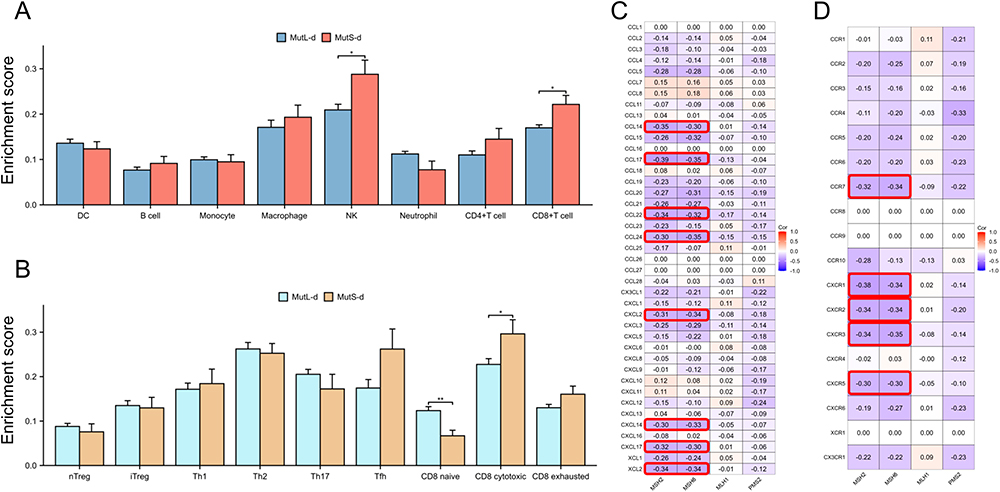 |
Figure 5 Local immune infiltration of MutS-d and MutL-d. (A and B) Infiltration of DC, B cells, monocytes, macrophages, NK cells, neutrophils, CD4+T cells, CD8+T cells, nTregs, iTregs, Th1, Th2, Th17, Tfh, CD8 naïve, CD8 cytotoxic, and CD8 exhausted cells between MutS-d and MutL-d; (C and D) Association of MSH2, MSH6, MLH1, and PMS2 with chemokines and chemokine receptors. Red outline boxes represent chemokines and chemokine receptors with high relevance to MSH2/MSH6. The absolute value of the correlation is greater than or equal to 0.3. Abbreviations: MutS-d, MutS deficiency; MutL-d, MutL deficiency; DC, Dendritic cell; NK, natural killer cell; Treg, regulatory T cells; Th, Helper T cells; Tfh, Follicular helper T cell. Notes: *p < 0.05; **p < 0.01; p<0.05 indicates significant differences. |
Profiles of Immune Checkpoint of MutL-d and MutS-d Subgroups
We assessed immune checkpoint expression between the MutS-d and MutL-d using the TCGA database, which revealed significantly lower expression levels of several immune checkpoints in the MutL-d group compared to that in the MutS-d group. Statistically significant differences were observed in the expression levels of PD-1, TIM-3, CTLA-4, LAG-3, TIGIT, ICOS, BTLA, and VISTA (Figure 6A). Higher expression levels of immune checkpoints correlate with more favorable treatment outcomes within a certain range.
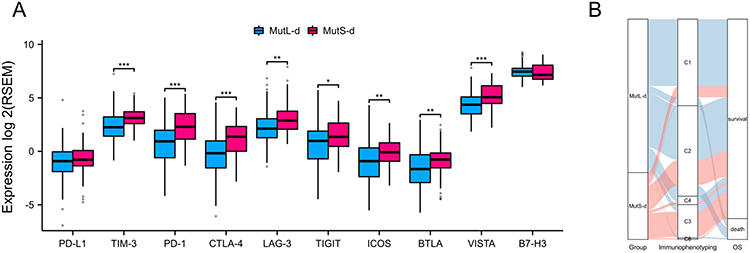 |
Figure 6 Profiles of immune checkpoint and immunophenotyping composition of MutS-d and MutL-d. (A) Expression of the MutS-d and MutL-d immune checkpoints. (B) Immunophenotyping and prognosis of MutS-d and MutL-d. Abbreviations: MutS-d, MutS deficiency; MutL-d, MutL deficiency; OS, overall survival; C1, wound-healing type; C2, IFN-γ dominant type; C3, inflammatory type; C4, lymphocyte depleted type, C5, immunologically quiet type; C6, TGF-β dominant type. Notes: *p < 0.05; **p < 0.01; ***p < 0.001; p<0.05 indicates significant differences. |
Profiles of Immunophenotyping Composition of MutL-d and MutS-d Subgroups
Thorsson et al delineated six discrete immune subtypes of tumors: C1 (wound-healing), C2 (IFN-γ dominant), C3 (inflammatory), C4 (lymphocyte depleted), C5 (immunologically quiet), and C6 (TGF-β dominant).9 We employed data from TCGA and TISIDB databases to analyze the patients’ immune subtypes. Among the patients with MutS-d, 18.75% had subtype C1, 37.5% had subtype C2, 37.5% had subtype C3, 4.17% had subtype C4, and 2.08% had subtype C6. In contrast, for patients with MutL-d, the distribution was 48.18% for C1, 42.73% for C2, 5.45% for C3, and 3.64% for C4 (Figure 6B). C3 exhibited exceptional OS, whereas C2 and C1 showed inferior prognoses. Conversely, C4 and C6 are associated with the most unfavorable prognosis.9 This also indicates that the immune status and prognosis of MutS-d are better than those of MutL-d.
Discussion
EC exhibits the highest MMRd occurrence ratio among gynecological tumors.10 Previous studies have classified MMRd-EC/MSI-H into subtypes including MLH1-hypermethylated EC (EC-met), Lynch syndrome-associated EC (EC-ls), and mismatch repair gene double somatic pathogenic variants (EC-dspv). Patients with EC-met were the oldest, had the highest incidence, and a poorer prognosis than the other two subtypes.11,12 Pasanen et al divided MMRd-EC into two subgroups: EC with highly methylated MLH1 (EC-met), and EC without highly methylated MLH1 (EC-non-met). Patients with EC-met exhibited an older age of onset along with higher rates of LVSI and LNM than EC-nonmet cases.13 These classification methods involving methylation detection pose economic and technical challenges that hinder their widespread application. Our analysis proposes a subgrouping of MMRd-ECs based on MutS (MSH2, MSH6) and MutL (MLH1, PMS2) deletions. This classification method relies exclusively on the immunohistochemical staining of relevant proteins, eliminating additional economical and technical complexities and making it more feasible for widespread adoption and utilization. From the above groupings, it was found that patients with MutL-d exhibit heightened risk factors, including elevated cancer grading and increased DMI, leading to a poorer prognosis with shorter OS and PFS. In all patients with colorectal cancer (CRC), the median OS was longer in MutS co-loss (N=153) than in MutL co-loss (N=986) (54.6 months (m) vs 36 months; hazard ratio (HR) = 0.766; p=0.025). In all patients with EC, the median OS was longer in MutS co-loss (N=104) compared to MutL co-loss (N=1870) (81.5 m vs 48.2 m; HR= 0.535, p<0.001).14 When subdividing the MMR-d group into MLH1/PMS2 loss and other MMR-d subgroup (including MSH2/MSH6 loss, MSH6 only and PMS2 only loss), MLH1/PMS2 loss was significantly associated with inferior PFS (p=0.008).15 Doulgeraki et al revealed a correlation between MLH1/PMS2 deletion and the depth of myometrial infiltration, whereas MSH6 protein deletion was notably correlated with lymph node metastasis.16 These findings are consistent with our observations, suggesting that distinct mismatch repair protein types can serve as prognostic indicators of different tumor subtypes.
Elevated levels of tumor-infiltrating lymphocytes (TILs) are recognized as reliable prognostic markers.17 Bohaumilizky et al revealed that Lynch syndrome-associated endometrial cancer (EC-ls) showed notably higher counts of CD8+ T cells, increased PD-L1 expression, and a higher incidence of beta-2-microglobulin mutations compared to sporadic MMRd-EC.18 Similarly, research conducted by Ramchander et al highlighted significantly higher counts of CD3+, CD8+, CD45RO+, and PD-1+ T lymphocytes in EC-ls tumor tissues than in EC-met.19 Our findings suggest that MutL-d is associated with reduced infiltration of immune cells, including NK cells, CD8+ T cells, and CTLs, in contrast to MutS-d. This indicated that the local immune status of MutL-d was impaired.
Peripheral blood immune cell subpopulations, particularly lymphocyte subsets, play a pivotal role in tumor development and serve as crucial indicators for the assessment of the systemic immune status. An increase in CD8+ T cells is observed in the peripheral blood of patients with early-stage colon cancer and a decrease in advanced disease stages.20 Remarkably, individuals with MutL-d demonstrated lower peripheral blood lymphocyte counts, lymphocyte percentages, and CD8+ T cell percentages, which is indicative of a compromised immune status. Hence, MutL-d and MutS-d can potentially serve as indicators of systemic and local immune status in tumor subtypes.
MMRd tumors exhibit increased accumulation of somatic mutations, leading to increased expression of antigenic materials. Consequently, MMRd tumors become more susceptible to immune recognition and subsequent immune-mediated responses, which contributes to the observed clinical benefits of immunotherapy in patients with MMRd.10,21 The mean tumor mutational burden (TMB) in MutS co-loss was 44 mut/Mb versus 40.5 mut/Mb (q<0.059) in CRC and 30 mut/Mb versus 22 mut/Mb (q<0.0001) in EC.14 Previous studies proposed that among all tumors, loss of co-expression of MSH2/MSH6 was associated with a higher mean TMB (46.83 mut/Mb) than loss of MLH1/PMS2 (25.03 mut/Mb; p<0.0001). This indicates a potentially greater significance of the MutSα protein complex (MSH2/MSH6) in ensuring intact MMR compared to the MutLα complex (MLH1/PMS2).22 TMB is a predictive biomarker for ICIs. A comprehensive study involving 1662 patients across 10 cancer types treated with ICIs (anti-CTLA-4 or anti-PD-1/PD-L1 drugs) demonstrated a distinct dose-response relationship between TMB and OS after ICI initiation. Patients whose tumors ranked within the top 10% of TMB within their respective histology experienced prolonged OS compared to those in the 10–20% range, who, in turn, exhibited longer survival than the remaining 80%.23 In ICI-treated patients with CRC, the median OS was longer for MutS co-loss (N=32) than for MutL co-loss (N=184) (not reached (NR) vs 36 months; HR= 0.378, p=0.011). In ICI-treated patients with EC, the median OS in patients with MutS co-loss (N=16) compared to those with MutL co-loss (N=324) was NR vs 42.2 m (HR= 0.845, p=0.711).14
Based on the heterogeneity of MMRd-EC, our proposed classification approach offers a streamlined and economically viable alternative technique that effectively stratifies patients with MMRd and informs them of treatment choices. Patients with MutS-d EC have a favorable prognosis and immune phenotype. Hence, immunotherapy is recommended for these patients. However, patients with MutL-d EC have worse prognosis and immune phenotype. Therefore, it is essential to consider implementing more proactive and comprehensive treatment methods for patients with MutL-d EC. This allows for better precision in the treatment of patients with MMRDs. Furthermore, assessment of peripheral blood immune cell status can be used as an indicator for evaluating tumor progression and treatment efficacy in patients with MMRd EC.
Relative to previous studies,14,15 the strength of this study lies in its ability to harness proprietary and publicly accessible datasets to cross-validate the drawn results. Differences between the patients with MutS-d and MutL-d were clarified by comparing the risk factors for poor prognosis and survival analysis. Differences in the immune statuses of MutS-d and MutL-d were described by comparing peripheral blood immune cells, local immune cell infiltration in tumor tissues, cytokine secretion, expression of immune checkpoints, and immunophenotyping in a comprehensive and multilevel manner. This study had several limitations. This study, conducted at a single center, featured a homogeneous population, which may have introduced potential epidemiological biases. Therefore, it is necessary to validate these findings in larger multicenter trials. Notably, the diagnosis and management of Lynch syndrome were not addressed in this study. Finally, this study did not include in vivo studies. Next, we validated the differences in survival and immune status between patients with MutS-d and MutL-d by constructing a mouse model of patient-derived tumor xenografts. Further cohort studies on patients with MutS-d and MutL-d are needed to obtain more data on prognosis, immune status assessment, and clinical immunotherapy.
Conclusion
MMRd-EC patients can be subclassified according to their MutS or MutL deficiency. Patients with MutS-d exhibit a better immune status, better prognosis and better immunotherapy benefits compared to MutL-d. From there, this can guide MMRd patients to more precise treatment.
Abbreviations
EC, Endometrial cancer; FIGO, International Federation of Gynecology and Obstetrics; LVSI, Lymphovascular space invasion; LNM, lymph node metastasis; DMI, Deep myometrial invasion; BMI, Body mass index; ORs, Odds ratios; CIs, Confidence intervals; ROC, Receiver operating characteristic; AUC, Areas under the curve; TCGA, The Cancer Genome Atlas; MMRd, Mismatch repair deficiency; MutS-d, MutS deficiency; MutL-d, MutL deficiency; ER, Estrogen receptor; PR, progesterone receptor; CD4/CD8 or TH/TS, T-helper/T-suppressor ratio; OS, overall survival; PFS, progression-free survival; DSS, disease-specific survival; DC, Dendritic cell; NK, natural killer cell; cytotoxic T lymphocytes, CTLs; tumor mutational burden, TMB; immune-checkpoint inhibitors, ICIs; colorectal cancers; WBC, white blood cell count; Neu%, percentage of neutrophils; Lym%, percentage of lymphocytes; Mon%, percentage of monocytes; Neu, neutrophil count; Lym, lymphocyte count; Mon%, monocyte count; B cell %, percentage of B cells; T cell %, percentage of T cells; NK cell %, percentage of NK cells; CD4+ T cell %, percentage of helper T cells, CD8+ T cell %, percentage of suppressor T cells, CA125, cancer antigen 125.
Data Sharing Statement
The datasets analyzed in the current study are available from the corresponding author upon request.
Ethics Approval and Consent to Participate
This study conformed to the Declaration of Helsinki on Human Research Ethics standards and was approved by the Ethics Committee of Fujian Maternal and Child Health Hospital (Approval No. 2022KYLLRO3028). The need for written informed consent was waived by the Ethics Committee of Fujian Maternal and Child Health Hospital because of its retrospective design (Approval No. 2023KYLLRK01088). This study strictly protected the privacy of the patients and maintained the confidentiality of their personal information. Patient-identifiable information is hidden when data are analyzed for reporting purposes.
Acknowledgments
We express our gratitude to Tianai Chen, Zhenjie Chen, and Lirui Yu for their assistance in collecting clinical samples and conducting clinical examinations. We also acknowledge the contributions of Xiantaoxueshu (www.xiantao.love) for their support in data visualization and statistical analyses. We would like to thank Editage (www.editage.cn) for English language editing.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Support from National Key Technology Research and Developmental Program of China (No. 2022YFC2704303); Startup Fund for scientific research, Fujian Medical University (No. 2022QH2045); the National Natural Science Foundation of China (No. 82203739); Joint Funds for the innovation of science and Technology, Fujian province (No.2021Y9157; No. 2020Y9160); Fujian Province Central Government-Guided Local Science and Technology Development Project (2023L3019).
Disclosure
The authors have no conflicts of interest to declare.
References
1. Lortet-Tieulent J, Ferlay J, Bray F, Jemal A. International patterns and trends in endometrial cancer incidence, 1978–2013. J Natl Cancer Inst. 2018;110(4):354–361. doi:10.1093/jnci/djx214
2. T A, Mk M, L S, et al. A clinically applicable molecular-based classification for endometrial cancers. Br J Cancer. 2015;113(2). doi:10.1038/bjc.2015.190
3. Kandoth C, Schultz N, Cherniack AD, et al.; Cancer Genome Atlas Research Network. Integrated genomic characterization of endometrial carcinoma. Nature. 2013;497(7447):67–73. doi:10.1038/nature12113
4. Eskander RN, Sill MW, Beffa L, et al. Pembrolizumab plus chemotherapy in advanced endometrial cancer. N Engl J Med. 2023;388(23):2159–2170. doi:10.1056/NEJMoa2302312
5. Mirza MR, Chase DM, Slomovitz BM, et al. Dostarlimab for primary advanced or recurrent endometrial cancer. N Engl J Med. 2023;388(23):2145–2158. doi:10.1056/NEJMoa2216334
6. Willvonseder B, Stögbauer F, Steiger K, et al. The immunologic tumor microenvironment in endometrioid endometrial cancer in the morphomolecular context: mutual correlations and prognostic impact depending on molecular alterations. Cancer Immunol Immunother. 2021;70(6):1679–1689. doi:10.1007/s00262-020-02813-3
7. Gupta D, Heinen CD. The mismatch repair-dependent DNA damage response: mechanisms and implications. DNA Repair. 2019;78:60–69. doi:10.1016/j.dnarep.2019.03.009
8. He Y, Zhang L, Zhou R, Wang Y, Chen H. The role of DNA mismatch repair in immunotherapy of human cancer. Int J Biol Sci. 2022;18(7):2821–2832. doi:10.7150/ijbs.71714
9. Thorsson V, Gibbs DL, Brown SD, et al. The Immune Landscape of Cancer. Immunity. 2018;48(4):812–830.e14. doi:10.1016/j.immuni.2018.03.023
10. Le DT, Durham JN, Smith KN, et al. Mismatch-repair deficiency predicts response of solid tumors to PD-1 blockade. Science. 2017;357(6349):409–413. doi:10.1126/science.aan6733
11. Chika N, Eguchi H, Kumamoto K, et al. Prevalence of Lynch syndrome and Lynch-like syndrome among patients with colorectal cancer in a Japanese hospital-based population. Jpn J Clin Oncol. 2017;47(2):191. doi:10.1093/jjco/hyw200
12. Hampel H, Pearlman R, de la Chapelle A, et al. Double somatic mismatch repair gene pathogenic variants as common as Lynch syndrome among endometrial cancer patients. Gynecol Oncol. 2021;160(1):161–168. doi:10.1016/j.ygyno.2020.10.012
13. Xia Y, Li W, Li Y, et al. The clinical value of the changes of peripheral lymphocyte subsets absolute counts in patients with non-small cell lung cancer. Transl Oncol. 2020;13(12):100849. doi:10.1016/j.tranon.2020.100849
14. Khushman MM, Toboni MD, Xiu J, et al. Differential responses to immune checkpoint inhibitors are governed by diverse mismatch repair gene alterations. Clin Cancer Res off J Am Assoc Cancer Res. 2024. doi:10.1158/1078-0432.CCR-23-3004
15. Kim MK, So KA, Chun YK, et al. Clinicopathologic significance of mismatch repair protein expression in endometrioid endometrial cancer. Taiwan J Obstet Gynecol. 2023;62(5):724–728. doi:10.1016/j.tjog.2023.07.015
16. Doulgeraki T, Vagios S, Kavoura E, et al. Mismatch repair status in high-grade endometrial carcinomas of endometrioid and non-endometrioid type. J BUON off J Balk Union Oncol. 2019;24(5):2020–2027.
17. Denkert C, von Minckwitz G, Darb-Esfahani S, et al. Tumour-infiltrating lymphocytes and prognosis in different subtypes of breast cancer: a pooled analysis of 3771 patients treated with neoadjuvant therapy. Lancet Oncol. 2018;19(1):40–50. doi:10.1016/S1470-2045(17)30904-X
18. Bohaumilitzky L, von Knebel Doeberitz M, Kloor M, Ahadova A. Implications of hereditary origin on the immune phenotype of mismatch repair-deficient cancers: systematic literature review. J Clin Med. 2020;9(6):1741. doi:10.3390/jcm9061741
19. Ramchander NC, Ryan NAJ, Walker TDJ, et al. Distinct immunological landscapes characterize inherited and sporadic mismatch repair deficient endometrial cancer. Front Immunol. 2020;10:3023. doi:10.3389/fimmu.2019.03023
20. Evans CFM, Galustian C, Bodman-Smith M, Dalgleish AG, Kumar D. The effect of colorectal cancer upon host peripheral immune cell function. Colorectal Dis. 2010;12(6):561–569. doi:10.1111/j.1463-1318.2009.01819.x
21. Maby P, Tougeron D, Hamieh M, et al. Correlation between Density of CD8+ T-cell infiltrate in microsatellite unstable colorectal cancers and frameshift mutations: a rationale for personalized immunotherapy. Cancer Res. 2015;75(17):3446–3455. doi:10.1158/0008-5472.CAN-14-3051
22. Salem ME, Bodor JN, Puccini A, et al. Relationship between MLH1, PMS2, MSH2 and MSH6 gene-specific alterations and tumor mutational burden in 1057 microsatellite instability-high solid tumors. Int, J, Cancer. 2020;147(10):2948–2956. doi:10.1002/ijc.33115
23. Lee M, Samstein RM, Valero C, Chan TA, Morris LGT. Tumor mutational burden as a predictive biomarker for checkpoint inhibitor immunotherapy. Hum Vaccines Immunother. 2019;16(1):112–115. doi:10.1080/21645515.2019.1631136
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Novel lncRNA Panel for Risk Stratification and Immune Landscape in Breast Cancer Patients
Li C, Wang X, Chen T, Li W, Yang Q
International Journal of General Medicine 2022, 15:5253-5272
Published Date: 27 May 2022
Construction and Identification of an NLR-Associated Prognostic Signature Revealing the Heterogeneous Immune Response in Skin Cutaneous Melanoma
Geng Y, Sun YJ, Song H, Miao QJ, Wang YF, Qi JL, Xu XL, Sun JF
Clinical, Cosmetic and Investigational Dermatology 2023, 16:1623-1639
Published Date: 26 June 2023
Significance of Pyroptosis in Immunoregulation and Prognosis of Patients with Acute Respiratory Distress Syndrome: Evidence from RNA-Seq of Alveolar Macrophages
Liu B, Li Y, Xiang J, Li Y, Zhou M, Ren Y, Fu Z, Ding F
Journal of Inflammation Research 2023, 16:3547-3562
Published Date: 21 August 2023
A Risk Score Based on Immune- and Oxidative Stress-Related LncRNAs Predicts Prognosis in Lung Adenocarcinoma: Insights from in vitro Experiments and Large-Scale Transcriptome Analysis
Liu X, Zhao F, Wang X, Ma Z, Yan H, Lu X, Li S, Zhu H, Gao S
Journal of Inflammation Research 2024, 17:1453-1465
Published Date: 5 March 2024