Back to Journals » Cancer Management and Research » Volume 17

Artificial Intelligence in Breast Cancer Diagnosis and Surgical Decision-Making: An Updated and Comprehensive Overview of Precision and Personalization in Current Evidence
Authors Alenezi AM
Received 31 January 2025
Accepted for publication 22 September 2025
Published 30 September 2025 Volume 2025:17 Pages 2261—2275
DOI https://doi.org/10.2147/CMAR.S520224
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Lu-Zhe Sun
Anfal Mohammed Alenezi
Department of Surgery, College of Medicine, Jouf University, Sakaka, Aljouf, Saudi Arabia
Correspondence: Anfal Mohammed Alenezi, Department of Surgery, College of Medicine, Jouf University, Sakaka, Aljouf, 72388, Saudi Arabia, Tel +966 50 849 6882, Email [email protected]
Abstract: Breast cancer (BC) surgery has been advanced through artificial intelligence (AI), which helps surgeons to gain more accurate results and apply surgical procedures. Despite the increasing focus on AI in BC management, there are knowledge gaps in the current understanding that can be readily identified from the existing works of literature. This narrative review aims to provide an update on the influencing role of AI technologies in precise and personalized clinical decision-making in BC surgery. We included articles published in English during the past 5 years from the major databases. Furthermore, this review used appropriate keywords with and without Boolean operators like “AND”, “OR” and “NOT”. We considered three major aspects for surgical practice: preoperative planning, intraoperative decision-making, and postoperative outcomes, while interpreting the studies. We found that AI-assisted BC surgery has advanced through the development of a new real-time, accurate tumor identifier, margin assessment, and robotic-assisted surgeries. Moreover, AI-based algorithms are gradually incorporated into the evaluation of the postoperative probability of reoccurrence, complications, and patient satisfaction. It is documented that integrating AI technologies into BC care is inevitable and set to expand further in all aspects. Furthermore, this review identified some major challenges in the algorithm and ethical aspects. The limitations, such as lack of external validation, integration barriers, and the “black box” nature of some AI models, remain unresolved. To fully utilize AI’s capabilities, it is recommended that surgeons, AI developers, and policymakers collaborate on more advanced AI that is enhanced for personalized care by including patients’ genetics, medical history, and lifestyle factors. Additionally, future prospective and exploratory cost-effective analysis studies are to be done.
Keywords: breast cancer, personalized care, intraoperative, machine learning, deep learning
Introduction
Globally, breast cancer (BC) remains one of the important health challenges, as reported by the World Health Organization and the global cancer statistics. BC accounts for almost 2.3 million cases annually, rendering it the most prevalent cancer among adults.1,2 In 95% of nations, BC ranks as the primary or secondary cause of mortality among female cancer patients.2,3
The management flow of BC includes risk reduction, screening, imaging, biopsy, treatment, and follow-up. There are various treatment modalities for BC, including surgical, radiotherapy, chemotherapy, and immunotherapy.4,5 Despite the fact that new approaches for early diagnosis and management of BC have evolved over the past decade, the global BC statistics indicate the reality of persistent global obstacles in reducing the incidence and improving the survival of BC patients.3,6,7 In recent years, artificial intelligence (AI) has emerged as a promising adjunct to conventional treatment approaches, particularly in enhancing the precision and personalization of surgical decision-making, for instance, in BC treatment.8,9
Among the available treatment approaches, surgical modalities (except in metastatic cancer) remain the first approach, followed by other therapies. The surgical options are lumpectomy (partial mastectomy) and mastectomy. Traditional methods often face limitations in terms of human variability, time constraints, and difficulty in interpreting complex, high-dimensional data. The surgeons may decide on further supplementary procedures, including sentinel lymph node biopsy, axillary lymph node dissection, and breast reconstructive surgery, according to the existing guidelines, the patient’s condition and preference, and numerous other potential factors that can influence surgical decisions.5,10 Nonetheless, it is stated that BC’s surgical decision is moving away from “one size fits for all” to personalized and precision care.11–13
AI makes use of the most recent machine learning (ML) and deep learning (DL) algorithms and methods, including computer vision, among others (such as neural networks: convolutional, recurrent, and artificial and generative adversarial networks), to interpret sophisticated data. Large language models represent a category of AI that employs natural language processing techniques to analyze user prompts and provide human-like responses. DL involves multilayered neural networks for analyzing imaging data. Convolutional neural networks are a subset of DL specialized in medical image recognition. Reinforcement learning enables systems to improve decisions based on trial-and-error feedback. Natural language processing helps extract insights from clinical notes and medical literature.14–16 The role of AI in BC care ranges from screening to predicting prognostic values.9 For example, in BC screening, AI algorithms have the potential to significantly improve radiologists’ workflow by offering quantitative assessments that are free from human bias, which might lead to data-driven recommendations for doubtful mammograms that could be interpreted in numerous ways. To provide patients with answers more quickly, AI-powered software can automate the interpretation of MRI, ultrasound, and breast mammography data.17,18 Additionally, the role of AI in preoperative (surgical decision-making and patients’ health education), intraoperative (margin evaluation and accurate tumor removal), and postoperative prediction (prognosis, complications, and survival rate) has been documented in recent studies. Kothari et al formed an integrated model (ML and Laser Raman spectroscopy) to accurately identify the cancer tissue margins, a crucial step in breast conservative techniques.19 Similarly, Xu et al assessed the surgical decision-making model and found that about 5% of treating surgeons reworked their decisions after using this model.20
More recent work has focused on the application of AI in reconstructive surgical treatment decision-making in the context of BC.21,22 For instance, assessing ML methods for the prediction of donor-related complications in microsurgical breast reconstruction by Myung et al stated that using ML, the doctor can make a personalized surgical choice for better postoperative outcomes.21 Despite the increasing focus on AI in BC management, there are knowledge gaps in the current understanding that can be readily identified from the existing works of literature. Several studies have been conducted with a small sample size and a retrospective nature. Although some reviews have been conducted on how artificial intelligence can be used in BC care, most of them have been restricted to either diagnostic imaging or early detection, with fewer reviews done on its overall contribution to the decision-making process of the surgery. Some recent reviews have targeted certain AI applications in the field of surgery, yet these did not encompass a wide range of technologies nor the implications for patients. Apart from that, there are other disadvantages to using AI in BC, including data protection, privacy, and ethical issues, which is less explored in previous reviews.23,24 Finally, because of such dynamics and progressive changes in the application of AI in BC management in recent years, it is vital to obtain up-to-date information. Thus, the current narrative review seeks to provide a more holistic, up-to-date map of all applicable AI use cases in BC surgery decision-making and follow-up processes. Furthermore, the present review provides recommendations for future research directions to overcome the limitations and make use of AI efficiently in BC management.
Search Strategies
The present study included relevant literature published in the past five years (from January 2019 to September 2024). We used a diverse range of databases, namely, PubMed/Medline, Embase, Cochrane Library, Web of Science, Saudi Digital Library, IEEE Xplore, and Scopus, to find the latest published studies. This review used appropriate keywords with and without Boolean operators like “AND”, “OR”, and “NOT”. The following keywords were used in the study: “Artificial Intelligence”, “Breast Cancer”, “Surgical Decision-Making”, “Machine Learning”, “Deep Learning”, “Decision Support Techniques”, “Treatment Outcome”, “Patient Satisfaction”, “Survival Rate”, “Precision Medicine”, “Surgical Outcomes”. Moreover, the articles included were peer-reviewed with a digital object identifier (DOI) to ensure reliability and accessibility, even if the web address changed. This review excluded expert opinions, non-published articles, case series, case reports, editorial comments, studies not focused on AI in BC management, and non-English articles. After applying all these inclusion and exclusion criteria, the final number of included articles in the present review’s main text was 116. The search strategies are summarized in Table 1, and the study selection process in each stage is shown in a flow chart in Figure 1. Furthermore, the full database-specific search histories are presented as a supplementary file (Please find Appendix A – full search strategies by database for more information).
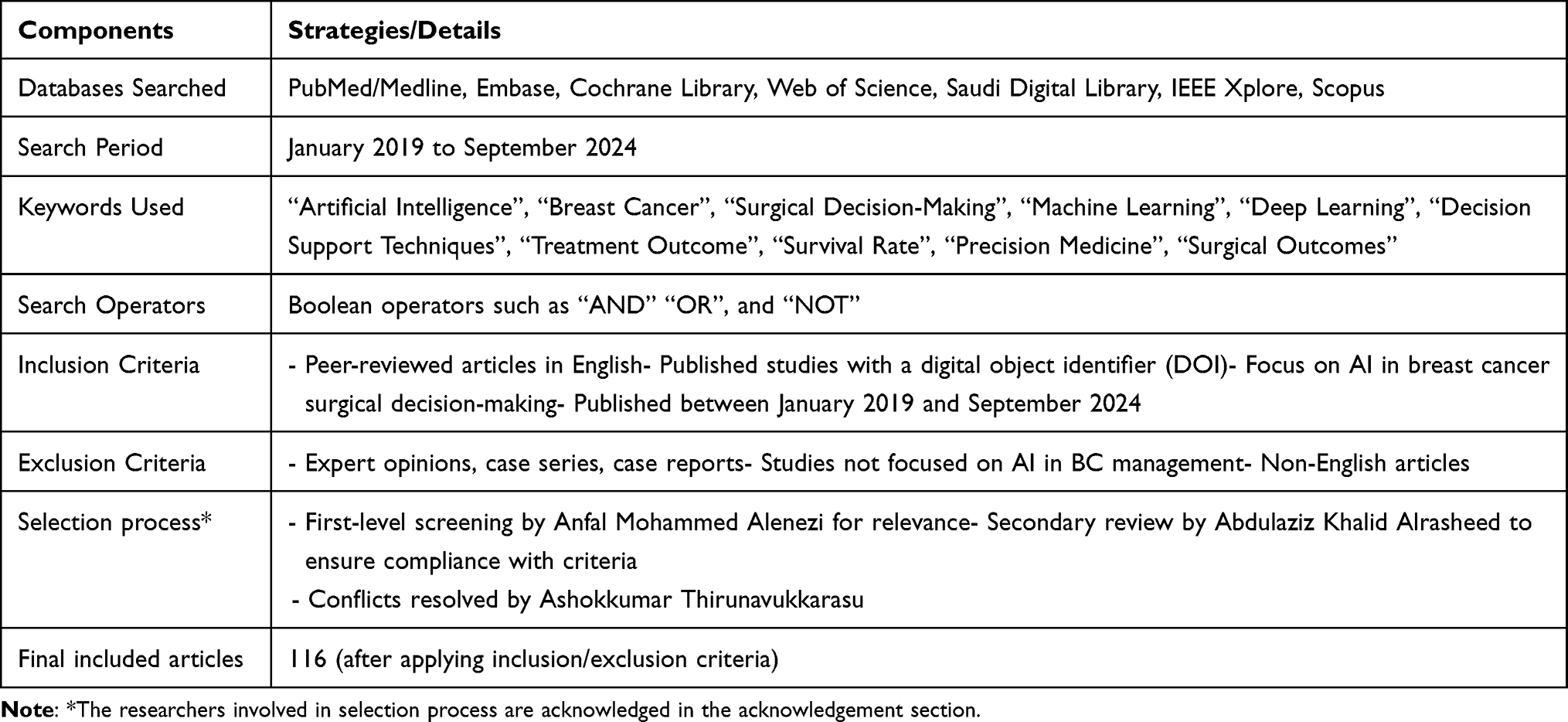 |
Table 1 Search Strategy for the Review |
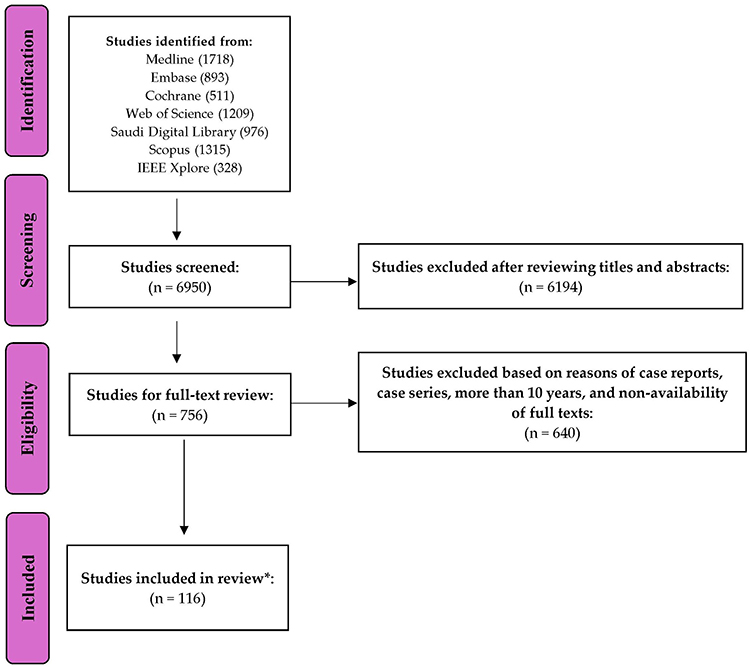 |
Figure 1 Diagram depicting the Flow of Study Screening and Selection Process. Note: *Number of articles included in the main text. |
Main Text
This review’s main text constitutes the discussion of AI applications in surgical decision-making (preoperative/intraoperative/postoperative), challenges and barriers to AI integration in clinical practice, and future directions and recommendations. The common AI models and their roles in BC surgical care are depicted in Figure 2.
 |
Figure 2 AI models and their roles in BC surgical care. |
AI Applications in Surgical Decision-Making
Role of AI in Preoperative BC Care
Some authors recently explored the significance of AI in preoperative BC care, and it was observed that AI could potentially transform and help in improving diagnostic precision, refining risk classification, and personalized care.25,26 AI is now utilized in medical imaging and histopathology for breast diseases due to the latest developments in computer vision algorithms and expanding training datasets.27,28 A prospective study by Dembrower et al 2023 reported that when AI replaced one radiologist to read screening mammograms independently, the non-inferior cancer detection rate was 4% higher than when two radiologists’ reading was used. According to their research, AI has the potential to be used under controlled conditions in the study environment and performance monitoring in real-world scenarios. However, they also stated that the significant limitations were AI availability during consensus discussions, lack of real-time adjustment due to retrospective data, and generalizability of the findings due to specific workflow, equipment, and population studied.17
Imaging modalities play a critical role in the preoperative assessment of BC patients. The imaging studies include mammograms, ultrasound imaging, magnetic resonance imaging, and contrast-enhanced mammograms.29,30 In 2023, on the evaluation of enhanced AI models, Zhu et al stated the significance of dataset-specific preprocessing methods and the capability of advanced AI models such as ViT and U-KAN to improve the precision of early BC diagnosis markedly.31 MRI is especially important as it appears to be very sensitive to the detection of invasive neoplasms, making it a crucial technique for preoperative evaluation. There have been reports that MRI can be used to detect additional cancer foci that would have been overlooked either by clinical evaluation or other imaging modalities.25 Being able to accurately depict the disease is a prerequisite for determining the surgical approach to be taken, particularly for patients who qualify for breast-conserving surgery. Such models help provide crucial information concerning tumor biology and help the surgeon decide whether surgery is warranted and to what degree. Nonetheless, Park et al stated that there is a lack of clarity on integrating the model into real-world screening programs.32
Additionally, using AI applications has been proven to reduce unnecessary biopsies, according to various studies. However, they are presented with some limitations, including the need for large datasets, lack of reproducibility, validation issues, integration into workflows, and resource constraints for smaller institutions.30 For an enhanced computer vision, Kaffashbashi et al, in 2024, published an article that evaluated the ensemble learning (voting) model and found that the model (convolutional neural network) showed a 98% accuracy in BC images with varying magnification factors.33 Considering the limitations of some of the AI models, such as convolutional neural network, recurrent neural network, and decision tree, Irshad Khan et al proposed a model (BC-AI) for the prompt and accurate diagnosis of BC, and their study reported more than 99% accuracy and sensitivity.28 A study done by Ahmed et al evaluated BC risk prediction using six ML algorithms. They stated that Support Vector Machine had the highest prediction rate of about 97% with the lowest error rate.34 Cè et al concluded that using AI algorithms, more complicated tasks in breast imaging, such as risk classifications and molecular characteristics of the tumor. However, these AI algorithms are limited by the need for large quantities of high-quality data.30
Recent advancements in predictive modeling (as documented by studies) using ML have emerged as significant developments in preoperative surgical decision-making. These models integrate clinical, pathological, and imaging data to determine the estimated course of the patient’s condition, including the chance of lymph nodes being involved and the rate of the patient’s overall survival.35–37 A recent study (2024) by Liu et al explored that a radiomics-based model helped determine sentinel lymph node biopsy, which affects the decision-making for the need for axillary dissection.38 The preoperative evaluation of axillary lymph nodes is crucial in managing BC as it helps tailor the treatment and the subsequent expected patient outcome. In 2024, Qian et al stated that DL -and radionics-based ultrasound nomograms could precisely predict axillary lymph node status in metastatic BC patients, and which can support personalized patient care and improvement in quality of life among patients.39
Biopsy is the gold standard for pathological assessment of several malignancies, including BC, and pathologists are dedicated to helping surgeons manage BC precisely. Hence, for personalized treatment, an accurate diagnosis is very important.40–42 Some recent studies described in their paper that AI algorithms can allocate patients for cancer assessment in BC clinics based on various clinical findings.43
As AI becomes more widely used in breast pathology, it helps with pathology diagnosis to increase accuracy and lessen pathologists’ burden, and offers fresh insights into prognosis and treatment response prediction. Recent studies, including a study by Shen et al in 2021, stated that the use of AI models reduces the false positives of breast imaging studies and the need for biopsies. The AI system achieved a sensitivity of 94.5% at the average radiologist’s specificity, representing a 4.4% absolute increase over human readers, who averaged 90.1% sensitivity.44 Aljondi et al explored an instance where AI was able to assist in breast cancer diagnosis. In their study, the AI detection agreed with the histopathological result was 91.3%, while the radiologist’s interpretation agreed with the pathology report was 73.8%.45 Using an ML model, Rao et al found that AI with neural network algorithms is efficient enough to identify patients who require biopsy. Their retrospective study was conducted among 794 cases who were assessed for their breast symptoms.46 This is important considering the global scenario of BC is changing, and incidence in women with fewer risk factors and in young women is expected to increase further. Hence, it is important to refine referral guidelines as AI can help identify patients needing biopsies promptly, potentially leading to earlier diagnosis and treatment. That is to say, AI has the potential to decrease the false negative rate in BC diagnosis, which improves the reliability of biopsy results. Furthermore, AI models can process imaging data to help identify critical areas that may need several interventions, such as a biopsy.47,48 This is a logical conclusion as combining AIs and human experts will enable better judgment on whether the lesion should be biopsied or not, increasing the diagnostic capability as well as the outcome of the patients.48,49 However, some authors are concerned about the black-box limitations associated with the AI models, especially in DL.50,51
The concern over the workload and efficiency of pathologists has been heightened in recent times due to the increased number of BC biopsies carried out. AI could be useful to pathologists by reducing the time needed to diagnose and automating the analysis of the biopsy samples, thus improving the consistency of interpretation.52–54 Sandbank et al undertook a study in which they validated a computer-assisted algorithm for the detection of breast cancer in the biopsy specimen, and the authors proved its usefulness in clinical practice. The AI algorithm differentiates the different types of carcinoma with high sensitivity and specificity (more than 90%).48 As noted in the studies, the AI was able to make quality and timely diagnoses with high accuracy and the identification of cancers initially missed by the reviewing pathologist. Thus, it can address the concerns of the pathologists’ workload. However, being a single-center study and lacking external validations were significant limitations in implementing the proposed AI models from previous studies.17,54
As discussed earlier, AI models can help with surgical decision-making in numerous ways. By offering the possibility of more accurate evaluations of the problems related to the tumor, its characteristics, and its nature of metastases, AI is able to suggest the most appropriate surgical strategies to the surgeon.8,51,55 For example, AI-imaging techniques that enable the detection of other noticeable cancers may, in some instances, result in the move from breast conservative surgeries to mastectomy to improve patient care. Also, AI tools that are able to estimate postoperative complications and survival rates are useful in preoperative counseling and shared management and decision-making by the patients and their doctors as they play a role in predicting outcomes.56,57
The applicability of such models in routine practice has been endorsed by several studies, which have recommended their incorporation together with biomarkers into clinical guidelines for managing BC patients. These areas are still developing, and one can anticipate an even more active integration of these technologies into treatment protocols and the improvement of standard care for BC patients.22,32,58,59
The AI helps the patients to make the right choice when it comes to treatment options. One example is AI-powered 3D imaging and augmented reality, which lets patients glimpse what may happen during breast augmentation or reconstruction. The personalized approach sets up patient engagement and satisfaction while setting realistic expectations of the surgical process and fostering trust in the process. In addition, natural language processing tools woven into patient education platforms use pre-existing text repositories to deliver custom information to address an individual’s concerns and clarify the complexities of medical procedures.60–63
Role of AI in Intraoperative BC Care
AI has made important advances in the area of surgical oncology, including decision support for BC surgery.35,64 Many of the aforementioned approaches, such as ML techniques, including DL, convolutional neural network, artificial neural network, and reinforcement learning, are useful in resolving intraoperative issues from different perspectives and creating opportunities to better the outcomes of BC surgery.14
ML, as a subset of multiple other AI domains, assists in predicting patient outcomes and increasing tumor localization efficiency during procedures such as BC surgery. Intraoperative complications can be predicted by ML models, which analyze patients, tumor characteristics, and historical data.59,65 Furthermore, ML can adjust the analyses based on age, genetics, and size of the tumor and predict complications like bleeding, infection, and extended recovery. With integration into real-time imaging analysis, for example, ultrasound or MRI, ML makes it easier for surgeons to differentiate between normal tissues and malignant ones, which largely decreases the chances of missing tumor tissues or the need to perform surgeries on the same site (reoperation).
DL is the latest branch of ML where multiple neural networks are cascaded to work over large amounts of data to provide efficiency with image work tasks in BC surgery. DL models provide detailed information on imaging data that can improve the evaluation of tumor margins and help with surgical navigation hand in hand.54,66–68 This is, in particular, significant in breast conservative surgeries. For example, a study published by Veluponnar et al in 2023 evaluated an AI model based on pre-trained neural networks. Comparing the segmentation results to the histology data, the authors able to predict a close margin with a sensitivity of 96% and a specificity of 76%. The authors described that the developed model could be further enhanced by algorithm changes, identifying the artifacts (such as hematomas), and further validation of real-time margin assessment is required. Sub-analyses on tumor characteristics and clinical workflow integration are needed for broader application.67 Pradipta augmented reality et al also proposed the necessity of more advanced AI models that help in real‐time intraoperative management of breast margins in live tissues.69 Convolutional neural networks are composed of several layers of neuron cells where each layer focuses on image pixels, and through pattern recognition, they identify features sometimes impossible for the human eye to detect. Research shows that samples taken from breast tissue put through a convolutional neural network, which was trained on histopathologic data, are able to detect cancerous cells; this, in return, aids the surgeon in getting a clear margin, hence reducing the chances of reoperation. Such a level of automation is helpful during BC surgery, where severe attention is required for the amount of tumor tissues being scraped off and healthy ones being spared.70–72 In addition, DL models with augmented reality functionality can help guide the surgeon to enhance his visibility and aid in the performance of the surgery by anchoring the data on the particular areas in the surgical field that are to be operated on. For example, a 3D model of a breast cancerous tumor may be created from preoperative MRI scans and displayed on the surgical field during the surgery. For instance, a randomized controlled trial conducted by Lee et al in 2024 reported better safety, outcome, and reliability in the augmented reality localization group. Hence, they concluded that augmented reality localization can be another option for tumor localization.73 However, the lack of detailed demographic characteristics limits their study findings. This model, complemented with DL, makes it easy for surgeons to dissect difficult regions of the body precisely, thus shortening surgical time and improving patients’ outcomes.27,73,74 However, cost, accessibility, and adequate training were the major challenges encountered in implementing real-world scenarios.
The practicality of reinforcement learning in fine-tuning and optimizing surgical skills in the context of BC surgery seems reasonable, considering that reinforcement learning is a subfield of ML where algorithms learn maximum reward through different experimentations. RL algorithms solve several possible situations that might occur during the tumor removal process to develop the best strategy for removing the tumor. Such algorithms are quite flexible since they rely on current data; therefore, they enhance intra-operative accuracy while avoiding undue risks and play a significant role in precision oncology.75–77 A deep reinforcement model was developed by Almutairi et al using two big data sets, stating that their proposed model achieved high accuracy in comparison to the traditional techniques. This can help the surgeons to identify precise margins, which, in turn, can help in decision-making during surgical procedures.78 The application of Generative Adversarial Networks in the field of DL can assist in generating models where synthetic data is sparse and thereby assist models in BC surgery. AI models created using Generative Adversarial Networks can create and supplement existing datasets with synthetic images to increase the accuracy and performance of convolutional neural networks in identifying BC tissue images. This is especially significant in BC surgery, where large amounts of data with corresponding labels are hard to come across, and the data created using Generative Adversarial Networks aids in improving the generalizability of the AI models.79–82 Apart from data generation, GANs can also be used to build 3-dimensional (3D) models of tumors and other relevant tissues, which can be used for surgical simulation, where complex surgical resections can be practiced in virtual reality.83–85
Role of AI in Postoperative BC Care
In the context of BC surgery, AI improves the management of care after discharge from the hospital by monitoring recovery processes, preventing or predicting complications, and adjusting the follow-up depending on the patient’s needs.86–89 Patients’ imaging studies, wearable devices, electronic health records, and work as AI models that assist in patient data analysis. This part of the review focuses on the importance of several AI models, including but not limited to ML, DL, convolutional neural networks, reinforcement learning, and natural language processing, in improving overall postoperative BC care.86,90–92 ML models are used to correlate potential postoperative complications with intraoperative factors like length of surgery, blood loss, weight, and additional illnesses such as obesity.
In 2023, Zuo et al, developed a prediction model using eleven different ML-based models that evaluated the possibility of BC recurrence among the patients. Their retrospective study generated a model (AdaBoost) that was based on the patients’ clinical and laboratory parameters using ML algorithms.93 They reported that the AdaBoost algorithm model consistently forecasts the likelihood of BC recurrence. The authors cautioned about the limitations, including sample size, lack of external validation, and the necessity of further clinical details for making valuable personalized care. A retrospective cohort study by Mansour et al in 2024 reported that using AI models in analyzing helped in postoperative imaging accuracy and ruled out the recurrence of BC.94 These AI models not only improve clinical outcomes by out, enabling postoperative monitoring, but also assist with patient satisfaction. Because potential complications may be predicted with the aid of intelligent models, patients become less anxious, having been made aware of this feature.86,89,95 DL models, especially those focused on the analysis of postoperative histopathological tissues and imaging data, are also important in determining cancer recurrence cases. DL in oncological follow-up aids tumor recurrence risk assessment by reviewing previous expectative data and postoperative tumor samples. This also allows for the planning of care time in future follow-ups by oncologists.96–98 This helps patients’ contentment as it provides them with tailored plans, ensuring that the plans for recovery and monitoring are within their specific risks.
Another recently concluded cross-sectional study that was conducted among 66 female patients who had undergone breast conservative surgeries by Eissa et al 2024 stated that AI-augmented mammograms enhanced the ability to rule out postoperative malignancy with 100% sensitivity.99 Nonetheless, the smaller sample size, lack of accountability of the AI algorithm with clinical characteristics, and lack of long-term follow-up data were the limitations of their study findings. Both imaging analysis in the search for recurrence and monitoring of the wound during the postoperative phase of BC patients utilize convolutional neural networks. Such models are very effective in the region of postoperative mammography, MRI, and ultrasound images, as well as those looking for chances of recurrence through abnormal body tissues.100,101 Regarding wound monitoring, convolutional neural networks help analyze clear pictures of surgical wounds and can determine postoperative infection, necrosis, or dehiscence.102,103 Remote monitoring via AI platforms is useful in BC postoperative care as it reduces physical visits to the hospital. Wound images can also be taken at home by the patients, and patients can receive expert feedback when the images do not require immediate attention; this eases the worry created by the procedure and promotes effective injury healing, better care, and improved quality of life.104,105 Besides, AI wearable devices and mobile health applications also achieve remote, uninterrupted monitoring of patient vital signs and activity levels, thereby interpreting recovery trends. The patients can wear sensors capable of measuring heart rate, temperature, and movement, and ML models process these parameters to detect outliers in expected recovery stage characteristics. This increases patient satisfaction since it provides safety without requiring numerous clinical appointments.106–108 A recent study by Cloß et al stated that the available evidence of the use of wearable devices is higher in BC care than in other types of cancers, indicating the growing importance of these devices in BC management.109
Natural language processing facilitates the analysis of unstructured data embedded in electronic health records regarding the measures of a patient’s recovery. It can analyze determinants from reports and documents that have been associated with specific events or negative outcomes through patterns established within the interference of physicians’ notes and patient reports. As the networks generate more synthetic data, they, in turn, help the AI models make better postoperative prediction models. This serves as a complication in training datasets, which give the network information on rare complications.110,111 With the increased data, trained models will be better equipped for AI tools to predict patient complications accurately across diverse populations. In the realm of BC postoperative assistance, the particularity of an AI in formulating algorithm-driven individual follow-up schedules, as well as monitoring in distant locations, is indispensable. The follow-up schedule is determined by analyzing the patient-outlined data with a view of the postoperative complications. Hence, personalized follow-up plan strategies can be formulated by the treating surgeons.107,109,112
In summary, postoperative BC care AI enhances the outcome by providing more personalized, faster, and easier service. With predictive modeling, recurrence monitoring, wound assessment, and management, wound healing supportive attention, and remote monitoring, AI paves the way for a more patient-centered postoperative process that meets the medical and psychological aspects of the patients. As AI technology advances, the effectiveness of patient’ satisfaction and the quality of postoperative care are likely to improve, which gives a bright hope for more individualized BC care in the future.113,114 For example, in a Korean hospital study where breast cancer patients’ cases were discussed by a multidisciplinary team using Watson for Oncology, 86.8% of patients in the AI-assisted group reported a positive change in their perception of the hospital’s care, compared to 71.2% in the non-AI group.113
The outline of some important research related to AI and its applications and limitations in all stages (preoperative, postoperative, and intraoperative) in BC surgical decision-making is depicted in Appendix B–Supplementary Table Also, a comparative summary of most common AI Models in BC surgery is depicted in Table 2.
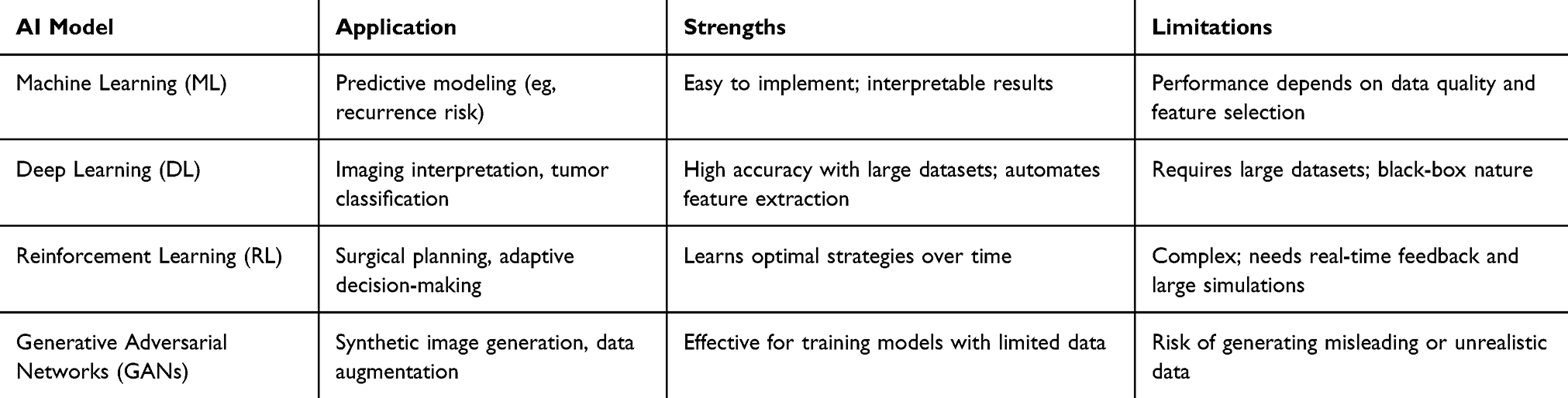 |
Table 2 Comparative Summary of AI Models in Breast Cancer Surgery |
Challenges and Barriers to AI Integration in Surgical Practice Related to BC
The present review noted that AI plays a crucial role in the personalized and precision care of BC. Nonetheless, implementing these innovations is not easy without limitations. The most prominent example of this scenario revolves around the ML and DL architectural models that largely depend on adequate and robust datasets to operate.25,115,116 For example, missing data can significantly decrease the full potential of the use of AI models. Some of those elements are histopathological slides, imaging, and the patient’s ends, which are often stored in separate institutions with different standards.30,117 In addition, several countries, such as the USA, restrict data sharing due to patients’ safety and confidentiality.118,119
Another clear barrier is the “black-box” character of many AI models, particularly those based on configurations like DL, as they often find it difficult to account for how their decisions evolve throughout the use of the system.50,120 In high-stakes situations like BC surgery, clinicians need AI systems that provide clear and interpretable outputs to ensure trust and reliability. The issue of AI models and lack of transparency in such elaborate algorithms are further aggravated in situations of trust once the nature of AI and AI recommendations for surgery are taken into account, as data scarcity limits the use of AI.103,121,122 Also, ethical issues stem from the data used to create and train AI systems. In instances where the training data consists of the same age group or race, then the resulting model or AI system is going to be less effective on patients of older age or other different races than those of the mixed-race sample population used to create that AI model.123,124 Such issues are very pertinent in BC treatment as in BC, the disease and treatment response vary for genetic and heterogeneous reasons, and BC treatment’s biased AI systems provide unequal treatment recommendations.125–127
AI integration often faces dramatic obstacles, as it requires altering the existing surgical systems, such as accepting and enhancing the knowledge of the practitioners.128 Some AI algorithms, such as convolutional neural networks, lack transparency (as some models use secondary data).72 Therefore, some surgeons may hesitate to use AI. The use of AI in BC surgeries requires standardized training. Therefore, the utilization varies between those with adequate training and those without.129,130 Similar to other technologies, there is a possibility of commercialization in the healthcare industry of AI marketing. However, structural factors, such as regulatory and legal requirements, still play a huge role in constraining the operational potential of AI.131,132 In this landscape, the role of an AI developer, a hospital, or a surgeon becomes unclear, which further complicates the adoption of AI tools in surgical units. Financial constraints could be another challenge in implementing AI in surgical practice. AI also uses and requires a steady supply of hardware, software, and maintenance, which often does not make financial sense. Hence, the country’s healthcare policy and economic situation also play a role in implementing AI in BC surgical care.133
A few studies have found an improved return on investment in AI systems in BC surgery, but few have also found the investment to be too high without sufficient long-term funding support.132,134 Finally, continuously updated data is critical, and the AI models based on older databases will be out of date and will no longer be accurately predictive of future events.135,136 Any of these problems will make it impossible to solve these issues without a broad and unified strategy throughout the fundamental research, as well as the law and practice. If there are no targeted measures to boost the quality of data, raise openness, create ethical and legal structures, and prove profitability, the dream of artificial intelligence cutting-edge solutions in transforming BC surgical practice will remain just that a dream.
The availability of AI systems in healthcare and the growing use of practical implementations beyond theoretical models invite us to expect their use in real-time clinical decision-making. The AI tool could provide precise localization of tumors, predict complications, and propose tailored surgical strategies to individual patients, thereby increasing accuracy and efficiency in delivering care by surgeons. In addition, AI can dramatically enhance healthcare disparities by closing resource-poor distances where no specialists may be present. Besides practical medical use, AI can also serve as an educational aid and let surgeons cultivate their skills using AR-based training modules and simulations. Together, these will collectively lead to AI’s transition from a promising innovation to a pillar of modern care for BC patients.
Unique Contributions and Strengths of This Review
This review article presents a comprehensive overview of the clinical use of AI in BC surgical decision-making in all stages, offering several distinct contributions to what is currently available in the literature. The key strengths and unique aspects of this work are summarized as follows:
- Inclusion of the Latest Advancements: This review incorporated studies published up to that date (past 5 years) in order to include the most recent updates on AI applications for BC surgery. Reading materials include exploring emerging technologies like DL models (eg, convolutional neural networks and generative adversarial networks) and augmented reality integration for intraoperative tumor localization. Hence, surgeons and other readers can interpret the state of the art in AI driving innovation. Also, clinicians can be aware of the limitations of the latest AI models before they use them in their clinical practice.
- Identification of Knowledge Gaps: While previous studies have covered AI applications broadly, this work identifies and addresses specific gaps in the literature. Furthermore, the review included some of the underexplored/unexplored AI technologies to keep readers informed.
- Practical Recommendations: The manuscript provides practical recommendations to all stakeholders (clinicians, policymakers, and developers). These recommendations are derived from recent evidence. So that clinicians can apply AI effectively to surgical decision-making workflows in all stages, make recommendations for developing AI guidelines, and train healthcare professionals to use AI appropriately and intelligently for policymakers. This review also explored issues like cost, accessibility, and interoperability in clinical environments.
- Real-World Case Studies: Real-world examples with more detailed explanations of included studies (like country, funding sources, external validation, etc)., including their limitations in practical use, are included to enhance the practical relevance of this review. Therefore, the lessons derived from other settings can guide the future use of AI in various clinical settings.
- The review discussed ethical aspects in detail to provide a holistic view of AI applications. Furthermore, the discussion of black-box concepts, which are discussed in very few manuscripts, added more novelty to the present review.
- Future Research Directions: The present review recommends forward-looking ideas, proposing a roadmap for advancing AI in breast cancer surgery. This includes developing AI models to overcome the “black box” issue and encouraging large multicenter studies for external validation so that this futuristic technology can be used effectively on a wider basis.
Limitations
This review was made with the standard method. However, some limitations that should be acknowledged. Firstly, this review’s findings were synthesized based only on English-language articles, which may introduce language bias and exclude valuable evidence from non-English-speaking countries. Similarly, we did not include grey literature and unpublished studies. Secondly, we relied on studies with varying designs and sample sizes, which may affect the generalizability and strength of the evidence synthesized from the present review. Next, there was also variability in the AI methodologies used across studies, including differences in model training, validation techniques, and outcome measures. Thus, making direct comparison challenging. Finally, the heterogeneity in clinical settings, patient populations, and institutional resources may limit the applicability of some AI tools across diverse healthcare systems.
Conclusion
The present review observed that AI has a significant scope in the surgical decision-making process in all stages. However, numerous challenges are present in implementing AI on a broader and more regular basis. First, using AI systems as black boxes, as in many systems (such as DL and convolutional neural networks), increases concerns regarding privacy, accountability, and clinical relevance. There are still no uniform and clear laws around liability, and the lack of a transparent accountability model does not encourage wider adoption. Hence, making reliable and secure data-sharing policies for the concerned authorities is critical. The high costs involved in use and maintenance further constrain small organizations, especially in resource-limited settings. While advanced AI tools may enhance decision-making and surgical precision, there is a risk of widening disparities across countries. Therefore, ensuring equitable access requires investments in infrastructure, clinician training, and the development of inclusive, multiethnic datasets. Additionally, future prospective and exploratory cost-effective analysis studies are to be done. Furthermore, economic viability and the ability to devise efficient AI systems for the variable dynamics involved in BC surgery are also important. Only in that way can the complete potential of AI be harnessed so that the clinical results of BC surgery and the quality of care of patients with BC can be improved.
Acknowledgments
The author would like to thank Dr. Abdulaziz Khalid Alrasheed from King Saud Medical City for his immense contribution to the present article. The author extends sincere thanks to Dr. Ashokkumar Thirunavukkarasu for his support in the study selection process.
Funding
This work was funded by the Deanship of Graduate Studies and Scientific Research at Jouf University under grant No. (DGSSR-2023-01-02470).
Disclosure
The author reports no conflicts of interest in this work.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–263. doi:10.3322/caac.21834
2. World Health Organization. Breast cancer. World Health Organization. 2024. Available from: https://www.who.int/news-room/fact-sheets/detail/breast-cancer.
3. Arnold M, Morgan E, Rumgay H, et al. Current and future burden of breast cancer: global statistics for 2020 and 2040. Breast. 2022;66:15–23. doi:10.1016/j.breast.2022.08.010
4. Bhushan A, Gonsalves A, Menon JU. Current state of breast cancer diagnosis, treatment, and theranostics. Pharmaceutics. 2021;13(5):723. doi:10.3390/pharmaceutics13050723
5. Wang J, Wu SG. Breast cancer: an overview of current therapeutic strategies, challenge, and perspectives. Breast Cancer. 2023;15:721–730. doi:10.2147/bctt.S432526
6. Loibl S, André F, Bachelot T, et al. Early breast cancer: ESMO clinical practice guideline for diagnosis, treatment and follow-up☆. Ann Oncol. 2024;35(2):159–182. doi:10.1016/j.annonc.2023.11.016
7. Ginsburg O, Yip C-H, Brooks A, et al. Breast cancer early detection: a phased approach to implementation. Cancer. 2020;126(S10):2379–2393. doi:10.1002/cncr.32887
8. Liao J, Li X, Gan Y, et al. Artificial intelligence assists precision medicine in cancer treatment. Front Oncol. 2022;12:998222. doi:10.3389/fonc.2022.998222
9. Seth I, Lim B, Joseph K, et al. Use of artificial intelligence in breast surgery: a narrative review. Gland Surg. 2024;13(3):395–411. doi:10.21037/gs-23-414
10. Belkacemi Y. Advances and challenges in breast cancer management: a history made of evolutions and revolutions. Cancers. 2023;15(6):1713. doi:10.3390/cancers15061713
11. Sulaiman A, McGarry S, Han X, Liu S, Wang L. CSCs in breast cancer-one size does not fit all: therapeutic advances in targeting heterogeneous epithelial and mesenchymal CSCs. Cancers. 2019;11(8):1128. doi:10.3390/cancers11081128
12. Lancet Oncology T. The Lancet O. Breast cancer screening: one size does not fit all. Lancet Oncol. 2023;24(12):1287. doi:10.1016/S1470-2045(23)00590-9
13. Tufail M, Hu -J-J, Liang J, et al. Predictive, preventive, and personalized medicine in breast cancer: targeting the PI3K pathway. J Transl Med. 2024;22(1):15. doi:10.1186/s12967-023-04841-w
14. Jiang B, Bao L, He S, Chen X, Jin Z, Ye Y. Deep learning applications in breast cancer histopathological imaging: diagnosis, treatment, and prognosis. Breast Cancer Res. 2024;26(1):137. doi:10.1186/s13058-024-01895-6
15. Yamashita R, Nishio M, Do RKG, Togashi K. Convolutional neural networks: an overview and application in radiology. Insights Into Imaging. 2018;9(4):611–629. doi:10.1007/s13244-018-0639-9
16. Jayaraman P, Desman J, Sabounchi M, Nadkarni GN, Sakhuja A. A primer on reinforcement learning in medicine for clinicians. NPJ Digit Med. 2024;7(1):337. doi:10.1038/s41746-024-01316-0
17. Dembrower K, Crippa A, Colón E, Eklund M, Strand F. Artificial intelligence for breast cancer detection in screening mammography in Sweden: a prospective, population-based, paired-reader, non-inferiority study. Lancet Digit health. 2023;5(10):e703–e711. doi:10.1016/S2589-7500(23)00153-X
18. Díaz O, Rodríguez-Ruíz A, Sechopoulos I. Artificial intelligence for breast cancer detection: technology, challenges, and prospects. Eur J Radiol. 2024;175:111457. doi:10.1016/j.ejrad.2024.111457
19. Kothari R, Jones V, Mena D, et al. Raman spectroscopy and artificial intelligence to predict the Bayesian probability of breast cancer. Sci Rep. 2021;11(1):6482. doi:10.1038/s41598-021-85758-6
20. Xu F, Sepúlveda MJ, Jiang Z, et al. Artificial intelligence treatment decision support for complex breast cancer among oncologists with varying expertise. JCO Clin Cancer Inform. 2019;3:1–15. doi:10.1200/cci.18.00159
21. Myung Y, Jeon S, Heo C, et al. Validating machine learning approaches for prediction of donor related complication in microsurgical breast reconstruction: a retrospective cohort study. Sci Rep. 2021;11(1):5615. doi:10.1038/s41598-021-85155-z
22. Seth I, Bulloch G, Joseph K, Hunter-Smith DJ, Rozen WM. Use of artificial intelligence in the advancement of breast surgery and implications for breast reconstruction: a narrative review. J Clin Med. 2023;12(15):5143. doi:10.3390/jcm12155143
23. Carter SM, Rogers W, Win KT, Frazer H, Richards B, Houssami N. The ethical, legal and social implications of using artificial intelligence systems in breast cancer care. Breast. 2020;49:25–32. doi:10.1016/j.breast.2019.10.001
24. AlSamhori JF, AlSamhori ARF, Duncan LA, et al. Artificial intelligence for breast cancer: implications for diagnosis and management. J Med Surg Public Health. 2024;3:100120. doi:10.1016/j.glmedi.2024.100120
25. Bahl M. Artificial intelligence: a primer for breast imaging radiologists. J Breast Imag. 2020;2(4):304–314. doi:10.1093/jbi/wbaa033
26. Taleghamar H, Jalalifar SA, Czarnota GJ, Sadeghi-Naini A. Deep learning of quantitative ultrasound multi-parametric images at pre-treatment to predict breast cancer response to chemotherapy. Sci Rep. 2022;12(1):2244. doi:10.1038/s41598-022-06100-2
27. Żydowicz WM, Skokowski J, Marano L, Polom K. Navigating the metaverse: a new virtual tool with promising real benefits for breast cancer patients. J Clin Med. 2024;13(15):4337. doi:10.3390/jcm13154337
28. Irshad Khan A, Abushark YB, Alsolami F, et al. Prediction of breast cancer based on computer vision and artificial intelligence techniques. Measurement. 2023;218:113230. doi:10.1016/j.measurement.2023.113230
29. Zheng D, He X, Jing J. Overview of artificial intelligence in breast cancer medical imaging. J Clin Med. 2023;12(2):419. doi:10.3390/jcm12020419
30. Cè M, Caloro E, Pellegrino ME, et al. Artificial intelligence in breast cancer imaging: risk stratification, lesion detection and classification, treatment planning and prognosis-a narrative review. Explor Target Antitumor Ther. 2022;3(6):795–816. doi:10.37349/etat.2022.00113
31. Zhu Z, Sun Y, Honarvar Shakibaei Asli B. Early breast cancer detection using artificial intelligence techniques based on advanced image processing tools. Electronics. 2024;13(17):3575. doi:10.3390/electronics13173575
32. Park EK, Lee H, Kim M, et al. Artificial intelligence-powered imaging biomarker based on mammography for breast cancer risk prediction. Diagnostics. 2024;14(12):1212. doi:10.3390/diagnostics14121212
33. Kaffashbashi A, Sobhani V, Goodarzian F, Jolai F, Aghsami A. Augmented data strategies for enhanced computer vision performance in breast cancer diagnosis. J Ambient Intell Humaniz Comput. 2024;15(7):3093–3106. doi:10.1007/s12652-024-04803-0
34. Ahmed MR, Ali MA, Roy J, Ahmed S, Ahmed N. Breast cancer risk prediction based on six machine learning algorithms.
35. Qiu Y, Zhang X, Wu Z, et al. MRI-based radiomics nomogram: prediction of axillary non-sentinel lymph node metastasis in patients with sentinel lymph node-positive breast cancer. Front Oncol. 2022;12:811347. doi:10.3389/fonc.2022.811347
36. Liu Z, Hong M, Li X, Lin L, Tan X, Liu Y. Predicting axillary lymph node metastasis in breast cancer patients: a radiomics-based multicenter approach with interpretability analysis. Eur J Radiol. 2024;176:111522. doi:10.1016/j.ejrad.2024.111522
37. Lin G, Chen W, Fan Y, et al. Machine learning radiomics-based prediction of non-sentinel lymph node metastasis in chinese breast cancer patients with 1-2 positive sentinel lymph nodes: a multicenter study. Acad Radiol. 2024;31(8):3081–3095. doi:10.1016/j.acra.2024.02.010
38. Liu H, Zou L, Xu N, et al. Deep learning radiomics based prediction of axillary lymph node metastasis in breast cancer. Npj Breast Cancer. 2024;10(1):22. doi:10.1038/s41523-024-00628-4
39. Qian L, Liu X, Zhou S, et al. A cutting-edge deep learning-and-radiomics-based ultrasound nomogram for precise prediction of axillary lymph node metastasis in breast cancer patients ≥ 75 years. Front Endocrinol. 2024;15:1323452. doi:10.3389/fendo.2024.1323452
40. Caswell-Jin JL, Sun LP, Munoz D, et al. Analysis of breast cancer mortality in the US-1975 to 2019. JAMA. 2024;331(3):233–241. doi:10.1001/jama.2023.25881
41. Saednia K, Tran WT, Sadeghi-Naini A. A hierarchical self-attention-guided deep learning framework to predict breast cancer response to chemotherapy using pre-treatment tumor biopsies. Med Phys. 2023;50(12):7852–7864. doi:10.1002/mp.16574
42. Aswolinskiy W, Munari E, Horlings HM, et al. PROACTING: predicting pathological complete response to neoadjuvant chemotherapy in breast cancer from routine diagnostic histopathology biopsies with deep learning. Breast Cancer Res. 2023;25(1):142. doi:10.1186/s13058-023-01726-0
43. Kumar Singh L, Khanna M, singh R. A novel enhanced hybrid clinical decision support system for accurate breast cancer prediction. Measurement. 2023;221:113525. doi:10.1016/j.measurement.2023.113525
44. Shen Y, Shamout FE, Oliver JR, et al. Artificial intelligence system reduces false-positive findings in the interpretation of breast ultrasound exams. Nat Commun. 2021;12(1):5645. doi:10.1038/s41467-021-26023-2
45. Aljondi R, Alghamdi SS, Tajaldeen A, Alassiri S, Alkinani MH, Bertinotti T. Application of artificial intelligence in the mammographic detection of breast cancer in Saudi Arabian women. Appl Sci. 2023;13(21):12087. doi:10.3390/app132112087
46. Rao A, Manley L, Smith S. Use of artificial intelligence to identify patients to be assessed in a breast clinic on 2-week wait: a retrospective cohort study. Ann Med Surg. 2023;85(11):5459–5463. doi:10.1097/ms9.0000000000001293
47. Gjesvik J, Moshina N, Lee CI, Miglioretti DL, Hofvind S. Artificial intelligence algorithm for subclinical breast cancer detection. JAMA Network Open. 2024;7(10):e2437402–e2437402. doi:10.1001/jamanetworkopen.2024.37402
48. Sandbank J, Bataillon G, Nudelman A, et al. Validation and real-world clinical application of an artificial intelligence algorithm for breast cancer detection in biopsies. Npj Breast Cancer. 2022;8(1):129. doi:10.1038/s41523-022-00496-w
49. Soliman A, Li Z, Parwani AV. Artificial intelligence’s impact on breast cancer pathology: a literature review. Diagn Pathol. 2024;19(1):38. doi:10.1186/s13000-024-01453-w
50. Gastounioti A, Kontos D. Is It Time to Get Rid of Black Boxes and Cultivate Trust in AI? Radiol Artif Intell. 2020;2(3):e200088. doi:10.1148/ryai.2020200088
51. Ahn JS, Shin S, Yang SA, et al. Artificial intelligence in breast cancer diagnosis and personalized medicine. J Breast Cancer. 2023;26(5):405–435. doi:10.4048/jbc.2023.26.e45
52. Pfob A, Heil J. Artificial intelligence to de-escalate loco-regional breast cancer treatment. Breast. 2023;68:201–204. doi:10.1016/j.breast.2023.02.009
53. George K, Faziludeen S, Sankaran P, Joseph KP. Breast cancer detection from biopsy images using nucleus guided transfer learning and belief based fusion. Comput Biol Med. 2020;124:103954. doi:10.1016/j.compbiomed.2020.103954
54. Boissin C, Wang Y, Sharma A, et al. Deep learning-based risk stratification of preoperative breast biopsies using digital whole slide images. Breast Cancer Res. 2024;26(1):90. doi:10.1186/s13058-024-01840-7
55. Koh D-M, Papanikolaou N, Bick U, et al. Artificial intelligence and machine learning in cancer imaging. Communicat Med. 2022;2(1):133. doi:10.1038/s43856-022-00199-0
56. Corti C, Cobanaj M, Marian F, et al. Artificial intelligence for prediction of treatment outcomes in breast cancer: systematic review of design, reporting standards, and bias. Cancer Treat Rev. 2022;108:102410. doi:10.1016/j.ctrv.2022.102410
57. Jones MA, Islam W, Faiz R, Chen X, Zheng B. Applying artificial intelligence technology to assist with breast cancer diagnosis and prognosis prediction. Front Oncol. 2022;12:980793. doi:10.3389/fonc.2022.980793
58. Nardone V, Marmorino F, Germani MM, et al. The role of artificial intelligence on tumor boards: perspectives from surgeons, medical oncologists and radiation oncologists. Current Oncol. 2024;31(9):4984–5007. doi:10.3390/curroncol31090369
59. Soh CL, Shah V, Arjomandi Rad A, et al. Present and future of machine learning in breast surgery: systematic review. Br J Surg. 2022;109(11):1053–1062. doi:10.1093/bjs/znac224
60. Gouveia PF, Luna R, Fontes F, et al. Augmented reality in breast surgery education. Breast Care. 2023;18(3):182–186. doi:10.1159/000529587
61. Abi-Rafeh J, Bassiri-Tehrani B, Kazan R, et al. Preoperative patient guidance and education in aesthetic breast plastic surgery: a novel proposed application of artificial intelligence large language models. Aesthetic Surg J Open Forum. 2024;6:ojae062. doi:10.1093/asjof/ojae062
62. Chartier C, watt A, Lin O, Chandawarkar A, Lee J, Hall-Findlay E. BreastGAN: artificial intelligence-enabled breast augmentation simulation. Aesthetic Surg J Open Forum. 2022;4:ojab052. doi:10.1093/asjof/ojab052
63. Didier AJ, Moss G, Sutton JM. Applications of artificial intelligence for cancer patient education. J Cancer Educ. 2024;40(3):313–314. doi:10.1007/s13187-024-02471-4
64. Cahill RA, O’Shea DF, Khan MF, et al. Artificial intelligence indocyanine green (ICG) perfusion for colorectal cancer intra-operative tissue classification. Br J Surg. 2021;108(1):5–9. doi:10.1093/bjs/znaa004
65. Sugimoto M, Hikichi S, Takada M, Toi M. Machine learning techniques for breast cancer diagnosis and treatment: a narrative review. Ann Breast Surg. 2021;7.
66. Zhang S, Yang B, Yang H, et al. Potential rapid intraoperative cancer diagnosis using dynamic full-field optical coherence tomography and deep learning: a prospective cohort study in breast cancer patients. Sci Bull. 2024;69(11):1748–1756. doi:10.1016/j.scib.2024.03.061
67. Veluponnar D, de Boer LL, Geldof F, et al. Toward intraoperative margin assessment using a deep learning-based approach for automatic tumor segmentation in breast lumpectomy ultrasound images. Cancers. 2023;15(6):1652. doi:10.3390/cancers15061652
68. Choi MS, Chang JS, Kim K, et al. Assessment of deep learning-based auto-contouring on interobserver consistency in target volume and organs-at-risk delineation for breast cancer: implications for RTQA program in a multi-institutional study. Breast. 2024;73:103599. doi:10.1016/j.breast.2023.103599
69. Pradipta AR, Tanei T, Morimoto K, Shimazu K, Noguchi S, Tanaka K. Emerging technologies for real-time intraoperative margin assessment in future breast-conserving surgery. Adv Sci. 2020;7(9):1901519. doi:10.1002/advs.201901519
70. Gonçalves CB, Souza JR, Fernandes H. CNN architecture optimization using bio-inspired algorithms for breast cancer detection in infrared images. Comput Biol Med. 2022;142:105205. doi:10.1016/j.compbiomed.2021.105205
71. Huang J, Mei L, Long M, et al. BM-Net: CNN-Based MobileNet-V3 and Bilinear Structure for Breast Cancer Detection in Whole Slide Images. Bioengineering. 2022;9(6):261. doi:10.3390/bioengineering9060261
72. Alanazi SA, Kamruzzaman MM, Islam Sarker MN, et al. Boosting Breast Cancer Detection Using Convolutional Neural Network. J Healthc Eng. 2021;2021:5528622. doi:10.1155/2021/5528622
73. Lee M, Woo J, Peak SH, et al. An exploratory clinical trial of preoperative non-invasive localization before breast-conserving surgery using augmented reality technology. Breast Cancer Res Treat. 2024;206(1):31–44. doi:10.1007/s10549-024-07272-3
74. Gouveia PF, Costa J, Morgado P, et al. Breast cancer surgery with augmented reality. Breast. 2021;56:14–17. doi:10.1016/j.breast.2021.01.004
75. Eckardt JN, Wendt K, Bornhäuser M, Middeke JM. Reinforcement Learning for Precision Oncology. Cancers. 2021;13(18):4624. doi:10.3390/cancers13184624
76. van Egdom LSE, Pusic A, Verhoef C, Hazelzet JA, Koppert LB. Machine learning with PROs in breast cancer surgery; caution: collecting PROs at baseline is crucial. Breast J. 2020;26(6):1213–1215. doi:10.1111/tbj.13804
77. Khajuria R, Sarwar A. Review of reinforcement learning applications in segmentation, chemotherapy, and radiotherapy of cancer. Micron. 2024;178:103583. doi:10.1016/j.micron.2023.103583
78. Almutairi S, M S, Kim B-G, Aborokbah MM, N C. Breast cancer classification using Deep Q Learning (DQL) and gorilla troops optimization (GTO). Appl Soft Comput. 2023;142:110292. doi:10.1016/j.asoc.2023.110292
79. Liu L, Liu Z, Chang J, Qiao H, Sun T, Shang J. MGGAN: a multi-generator generative adversarial network for breast cancer immunohistochemical image generation. Heliyon. 2023;9(10):e20614. doi:10.1016/j.heliyon.2023.e20614
80. Huang ZH, Chen L, Sun Y, Liu Q, Hu P. Conditional generative adversarial network driven radiomic prediction of mutation status based on magnetic resonance imaging of breast cancer. J Transl Med. 2024;22(1):226. doi:10.1186/s12967-024-05018
81. Wang D, Chen Z, Zhao H. Prototype transfer generative adversarial network for unsupervised breast cancer histology image classification. Biomed Signal Process Control. 2021;68:102713. doi:10.1016/j.bspc.2021.102713
82. Haq IU, Ali H, Wang HY, Cui L, Feng J. BTS-GAN: computer-aided segmentation system for breast tumor using MRI and conditional adversarial networks. Eng Sci Technol Int J. 2022;36:101154. doi:10.1016/j.jestch.2022.101154
83. Yao Z, Luo T, Dong Y, et al. Virtual elastography ultrasound via generative adversarial network for breast cancer diagnosis. Nat Commun. 2023;14(1):788. doi:10.1038/s41467-023-36102-1
84. Zama S, Fujioka T, Yamaga E, et al. Clinical utility of breast ultrasound images synthesized by a generative adversarial network. Medicina. 2024;60(1). doi:10.3390/medicina60010014
85. Zhang H, Xu H, Zhang Z-X, Zhang Q. Efficacy of virtual reality-based interventions for patients with breast cancer symptom and rehabilitation management: a systematic review and meta-analysis. BMJ Open. 2022;12(3):e051808. doi:10.1136/bmjopen-2021-051808
86. Zeng L, Liu L, Chen D, et al. The innovative model based on artificial intelligence algorithms to predict recurrence risk of patients with postoperative breast cancer. Front Oncol. 2023;13:1117420. doi:10.3389/fonc.2023.1117420
87. Gomez-Cabello CA, Borna S, Pressman SM, et al. Artificial intelligence in postoperative care: assessing large language models for patient recommendations in plastic surgery. Healthcare. 2024;12(11):1083. doi:10.3390/healthcare12111083
88. Vehviläinen-Julkunen K, Turpeinen S, Kvist T, et al. Experience of ambulatory cancer care: understanding patients’ perspectives of quality using sentiment analysis. Cancer Nurs. 2021;44(6):E331–e338. doi:10.1097/ncc.0000000000000845
89. Wei X, Lu Q, Jin S, et al. Developing and validating a prediction model for lymphedema detection in breast cancer survivors. Eur J Oncol Nurs. 2021;54:102023. doi:10.1016/j.ejon.2021.102023
90. Atkinson CJ, Seth I, Xie Y, et al. Artificial intelligence language model performance for rapid intraoperative queries in plastic surgery: chatGPT and the deep inferior epigastric perforator flap. J Clin Med. 2024;13(3):900. doi:10.3390/jcm13030900
91. Nassar A, Lymona AM, Lotfy MM, et al. Tumor mutation burden prediction model in egyptian breast cancer patients based on next generation sequencing. Asian Pac J Cancer Prev. 2021;22(7):2053–2059. doi:10.31557/APJCP.2021.22.7.2053
92. M-Y Duan, Y-q YE, Zhang L. A preliminary study of the significance of artificial intelligence in the clinical practice of breast cancer postoperation. Chinese J Pract Sur. 2019:964–967.
93. Zuo D, Yang L, Jin Y, Qi H, Liu Y, Ren L. Machine learning-based models for the prediction of breast cancer recurrence risk. BMC Med Inf Decis Making. 2023;23(1):276. doi:10.1186/s12911-023-02377-z
94. Mansour S, Azzam H, El-Assaly H. Artificial intelligence as a negative predictive tool for breast cancer postoperative recurrence. Egypt J Radiol Nucl Med. 2024;55(1):102. doi:10.1186/s43055-024-01272-5
95. Wu X, Guan Q, Cheng AS, et al. Comparison of machine learning models for predicting the risk of breast cancer-related lymphedema in Chinese women. Asia PacJ Oncol Nurs. 2022;9(12):100101. doi:10.1016/j.apjon.2022.100101
96. Guo J, Chen B, Cao H, et al. Cross-modal deep learning model for predicting pathologic complete response to neoadjuvant chemotherapy in breast cancer. Npj Precision Oncol. 2024;8(1):189. doi:10.1038/s41698-024-00678-8
97. Carriero A, Groenhoff L, Vologina E, Basile P, Albera M. Deep Learning in Breast Cancer Imaging: state of the Art and Recent Advancements in Early 2024. Diagnostics. 2024;14(8):848. doi:10.3390/diagnostics14080848
98. Cardoso MJ, Houssami N, Pozzi G, Séroussi B. Artificial intelligence (AI) in breast cancer care - Leveraging multidisciplinary skills to improve care. Breast. 2021;56:110–113. doi:10.1016/j.breast.2020.11.012
99. Eissa MAG, Al-Tohamy SF, Omar OS, Salaheldin LA. Post-operative breast imaging: a management dilemma. Can mammographic artificial intelligence help? Egypt J Radiol Nucl Med. 2024;55(1):197. doi:10.1186/s43055-024-01363-3
100. Kirelli Y, Arslankaya S, Koçer HB, Harmantepe T. CNN-based deep learning method for predicting the disease response to the Neoadjuvant Chemotherapy (NAC) treatment in breast cancer. Heliyon. 2023;9(6):e16812. doi:10.1016/j.heliyon.2023.e16812
101. Schnitzler T, Ruppert C, Hejduk P, et al. Automatic Detection of Post-Operative Clips in Mammography Using a U-Net Convolutional Neural Network. J Imaging. 2024;10(6):147. doi:10.3390/jimaging10060147
102. Garcia-Moreno FM, Ruiz-Espigares J, Gutiérrez-Naranjo MA, Marchal JA. Using deep learning for predicting the dynamic evolution of breast cancer migration. Comput Biol Med. 2024;180:108890. doi:10.1016/j.compbiomed.2024.108890
103. Anisuzzaman D, Patel Y, Rostami B, Niezgoda J, Gopalakrishnan S, Yu Z. Multi-modal wound classification using wound image and location by deep neural network. Sci Rep. 2022;12(1):20057. doi:10.1038/s41598-022-21813-0
104. Temple-Oberle C, Yakaback S, Webb C, Assadzadeh GE, Nelson G. Effect of smartphone app postoperative home monitoring after oncologic surgery on quality of recovery: a randomized clinical trial. JAMA Surgery. 2023;158(7):693–699. doi:10.1001/jamasurg.2023.0616
105. Spaulding A, Loomis E, Brennan E, et al. Postsurgical remote patient monitoring outcomes and perceptions: a mixed-methods assessment. Mayo Clin Proc Innov Qual Outcomes. 2022;6(6):574–583. doi:10.1016/j.mayocpiqo.2022.09.005
106. McCready TM, Stabile C, Vickers A, et al. A remote symptom monitoring tool as part of ambulatory cancer surgery recovery: a qualitative analysis of patient experience. JCO Oncol Pract. 2023;19(8):595–601. doi:10.1200/OP.23.00017
107. Hwang H. Electronic wound monitoring after ambulatory breast cancer surgery: improving patient care and satisfaction using a smart phone app. Br Colombia Med J. 2021;58(8):448–453.
108. Anik AR, Hasan K, Islam MM, Hasan MM, Ali MF, Das SK. Non-invasive portable technologies for monitoring breast cancer related lymphedema to facilitate telehealth: a scoping review. IEEE J Biomed Health Inform. 2023;27(9):4524–4535. doi:10.1109/JBHI.2023.3280196
109. Cloß K, Verket M, Müller-Wieland D, et al. Application of wearables for remote monitoring of oncology patients: a scoping review. Digital Health. 2024;10:20552076241233998. doi:10.1177/20552076241233998
110. Park JI, Park JW, Zhang K, Kim D. Advancing equity in breast cancer care: natural language processing for analysing treatment outcomes in under-represented populations. BMJ Health Care Inform. 2024;31(1):e100966. doi:10.1136/bmjhci-2023-100966
111. KDR L, Tay SBP, Choy KT, Verjans J, Sasanelli N, Kong JCH. Applications of natural language processing tools in the surgical journey. Front Surg. 2024;11:1403540. doi:10.3389/fsurg.2024.1403540
112. Stearns SA, Lee D, Bustos VP, et al. Enhancing post-mastectomy care: telehealth’s impact on breast reconstruction accessibility for breast cancer patients. Cancers. 2024;16(14):2555. doi:10.3390/cancers16142555
113. Lee K, Lee SH. Artificial intelligence-driven oncology clinical decision support system for multidisciplinary teams. Sensors. 2020;20(17). doi:10.3390/s20174693
114. Pesapane F, Giambersio E, Capetti B, et al. Patients’ perceptions and attitudes to the use of artificial intelligence in breast cancer diagnosis: a narrative review. Life. 2024;14(4):454. doi:10.3390/life14040454
115. Wichmann JL, Willemink MJ, De Cecco CN. Artificial intelligence and machine learning in radiology: current state and considerations for routine clinical implementation. Invest Radiol. 2020;55(9):619–627. doi:10.1097/rli.0000000000000673
116. Prior F, Almeida J, Kathiravelu P, et al. Open access image repositories: high-quality data to enable machine learning research. Clin Radiol. 2020;75(1):7–12. doi:10.1016/j.crad.2019.04.002
117. DeCamp M, Lindvall C. Latent bias and the implementation of artificial intelligence in medicine. J Am Med Inform Assoc. 2020;27(12):2020–2023. doi:10.1093/jamia/ocaa094
118. Edemekong PF, Annamaraju P, Haydel MJ. Health insurance portability and accountability act. In: StatPearls. StatPearls Publishing; 2024.
119. Walimohamed F, Keshavjee K. Lack of data access, but not availability, hinders ai training for high-risk conditions in Ontario. Stud Health Technol Inform. 2024;312:69–74. doi:10.3233/shti231314
120. Savage N. Breaking into the black box of artificial intelligence. Nature. 2022. doi:10.1038/d41586-022-00858-1
121. Al-Bazzaz H, Janicijevic M, Strand F. Reader bias in breast cancer screening related to cancer prevalence and artificial intelligence decision support-a reader study. Eur Radiol. 2024;34(8):5415–5424. doi:10.1007/s00330-023-10514-5
122. Fehr J, Citro B, Malpani R, Lippert C, Madai VI. A trustworthy AI reality-check: the lack of transparency of artificial intelligence products in healthcare. Front Digit Health. 2024;6:1267290. doi:10.3389/fdgth.2024.1267290
123. Marinovich ML, Wylie E, Lotter W, et al. Artificial intelligence (AI) for breast cancer screening: breastScreen population-based cohort study of cancer detection. eBioMedicine. 2023;90:104498. doi:10.1016/j.ebiom.2023.104498
124. Hantel A, Clancy DD, Kehl KL, Marron JM, Van Allen EM, Abel GA. A process framework for ethically deploying artificial intelligence in oncology. J Clin Oncol. 2022;40(34):3907–3911. doi:10.1200/jco.22.01113
125. Jaremko JL, Azar M, Bromwich R, et al. Canadian association of radiologists white paper on ethical and legal issues related to artificial intelligence in radiology. Canad Associat Radiolog Jl. 2019;70(2):107–118. doi:10.1016/j.carj.2019.03.001
126. Parikh RB, Teeple S, Navathe AS. Addressing bias in artificial intelligence in health care. JAMA. 2019;322(24):2377–2378. doi:10.1001/jama.2019.18058
127. Akingbola A, Adegbesan A, Ojo O, Otumara JU, Alao UH. Artificial intelligence and cancer care in Africa. J Med Surg Public Health. 2024;3:100132. doi:10.1016/j.glmedi.2024.100132
128. Oh S, Kim JH, Choi SW, Lee HJ, Hong J, Kwon SH. Physician confidence in artificial intelligence: an online mobile survey. J Med Internet Res. 2019;21(3):e12422. doi:10.2196/12422
129. Fazlollahi AM, Yilmaz R, Winkler-Schwartz A, et al. AI in surgical curriculum design and unintended outcomes for technical competencies in simulation training. JAMA Network Open. 2023;6(9):e2334658. doi:10.1001/jamanetworkopen.2023.34658
130. Riddle EW, Kewalramani D, Narayan M, Jones DB. Surgical simulation: virtual reality to artificial intelligence. Curr Prob Surg. 2024;61(11):101625. doi:10.1016/j.cpsurg.2024.101625
131. Mucha T, Halminen O, Tenhunen H, Seppälä T. Commercial adoption of ai in the healthcare sector: an exploratory analysis of S&P500 companies. Stud Health Technol Inform. 2020;270:113–117. doi:10.3233/shti200133
132. Upadhyay U, Gradisek A, Iqbal U, Dhar E, Li YC, Syed-Abdul S. Call for the responsible artificial intelligence in the healthcare. BMJ Health Care Inform. 2023;30(1):e100920. doi:10.1136/bmjhci-2023-100920
133. Ramezani M, Takian A, Bakhtiari A, Rabiee HR, Fazaeli AA, Sazgarnejad S. The application of artificial intelligence in health financing: a scoping review. Cost Eff Resour Alloc. 2023;21(1):83. doi:10.1186/s12962-023-00492-2
134. Khanna NN, Maindarkar MA, Viswanathan V, et al. Economics of artificial intelligence in healthcare: diagnosis vs. treatment. Healthcare. 2022;10(12):2493. doi:10.3390/healthcare10122493
135. Jiang M, Rocktäschel T, Grefenstette E. General intelligence requires rethinking exploration. R Soc Open Sci. 2023;10(6):230539. doi:10.1098/rsos.230539
136. Acosta JN, Falcone GJ, Rajpurkar P. The need for medical artificial intelligence that incorporates prior images. Radiology. 2022;304(2):283–288. doi:10.1148/radiol.212830
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Machine Learning Algorithm to Estimate Distant Breast Cancer Recurrence at the Population Level with Administrative Data
Izci H, Macq G, Tambuyzer T, De Schutter H, Wildiers H, Duhoux FP, de Azambuja E, Taylor D, Staelens G, Orye G, Hlavata Z, Hellemans H, De Rop C, Neven P, Verdoodt F
Clinical Epidemiology 2023, 15:559-568
Published Date: 5 May 2023
Nomogram Based on Super-Resolution Ultrasound Images Outperforms in Predicting Benign and Malignant Breast Lesions
Yang L, Ma Z
Breast Cancer: Targets and Therapy 2023, 15:867-878
Published Date: 2 December 2023
A Systematic Review of Real-Time Deep Learning Methods for Image-Based Cancer Diagnostics
Sriraman H, Badarudeen S, Vats S, Balasubramanian P
Journal of Multidisciplinary Healthcare 2024, 17:4411-4425
Published Date: 9 September 2024
Integrated Network Pharmacology, Machine Learning and Experimental Validation to Identify the Key Targets and Compounds of TiaoShenGongJian for the Treatment of Breast Cancer

Ying H, Kong W, Xu X
OncoTargets and Therapy 2025, 18:49-71
Published Date: 16 January 2025
An Artificial Intelligence Pipeline for Hepatocellular Carcinoma: From Data to Treatment Recommendations
Zhang X, Yang L, Liu C, Yuan X, Zhang Y
International Journal of General Medicine 2025, 18:3581-3595
Published Date: 2 July 2025