Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Socioeconomic Status Related to Prescription of Triple Therapy and Anticholinergic Monotherapy in Patients with Chronic Obstructive Pulmonary Disease (COPD) in Sweden - A Retrospective National Registry Study
Authors Larsson K ![]() , Betnér S, Fuchs B, Vanfleteren LEGW
, Betnér S, Fuchs B, Vanfleteren LEGW ![]() , Stridsman C
, Stridsman C ![]()
Received 13 May 2025
Accepted for publication 28 October 2025
Published 7 November 2025 Volume 2025:20 Pages 3597—3606
DOI https://doi.org/10.2147/COPD.S539470
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jill Ohar
Kjell Larsson,1 Staffan Betnér,2 Barbara Fuchs,3 Lowie EGW Vanfleteren,4,5 Caroline Stridsman6
1National Institute of Environmental Medicine, Integrative Toxicology, Karolinska Institutet, Stockholm, Sweden; 2Department of Public Health and Clinical Medicine, Northern Registry Centre, Umeå University, Umeå, Sweden; 3Chiesi Pharma AB, Medical Affairs, Stockholm, Sweden; 4Department of Respiratory Medicine and Allergology, COPD Center, Sahlgrenska University Hospital, Gothenburg, Sweden; 5Department of Internal Medicine and Clinical Nutrition, Institute of Medicine, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden; 6Department of Public Health and Clinical Medicine, Division of Medicine/The OLIN-Unit/Sunderby hospital, Umeå University, Umeå, Sweden
Correspondence: Caroline Stridsman, Department of Public Health and Clinical Medicine, Division of Medicine/The OLIN-unit/Sunderby Sjukhus, Sjukhusvägen 10, S-971 88, Luleå, Sweden, Tel +46-920 28 44 82, Email [email protected]
Purpose: There is an association between low socioeconomic status and chronic obstructive pulmonary disease (COPD), but it is not known whether this impacts on drug prescription for COPD treatment. The aim of the study was to explore whether drug prescription differs between COPD patients with low and high socioeconomic status.
Patients and methods: Data from patients with incident and prevalent COPD (age> 40 years), without an asthma diagnosis, visiting primary care in 2021– 2022 were extracted from The Swedish National Airway Register (SNAR) and linked to Swedish National Health registries. Socioeconomic status was assessed by educational level and annual income. Statistical analyses were conducted by means of chi square tests, together with post-hoc test.
Results: In total, 38692 patients (mean age 73.6 years, 55.5% women, FEV1 59.5% of predicted value) were included. Subdivision into GOLD group A, B and E was possible in 29128 patients. Triple therapy (long-acting antimuscarinic antagonists, LAMA + long-acting beta-2-agonist, LABA + inhaled steroids, ICS), was more often prescribed in the low education group (observed/expected ratio 1.09; p< 0.0001) and low income group (ratio 1.05; p< 0.05) and less often in the high education group (ratio 0.87; p< 0.0001) and high income group (ratio 0.88; p< 0.0001). Monotherapy (LAMA) was more often prescribed in patients with high income (ratio 1.09; p< 0.0001) and less often in patients with low income (ratio 0.93; p=0.0004). Differences between high and low education and income were driven by differences in group B.
Conclusion: Prescription patterns were associated with small, statistically significant differences, between COPD patients with low and high socioeconomic status. Triple therapy was more often prescribed to patients with low socioeconomic status, and monotherapy with LAMA more often to patients with high. The reason for this is not clear but may be caused by differences in exacerbation rate between the socioeconomic groups.
Keywords: prescription, education, income, socioeconomic status, COPD
Introduction
From a global perspective morbidity and mortality associated with chronic obstructive pulmonary disease (COPD) is increasing. The most important cause of the disease is exposure to airway irritants, mainly from tobacco smoke, but also other risk factors such as exposure to biomass fuels increase the risk of developing COPD.1 There are data suggesting that low socioeconomic status, defined as lower education and income, is itself associated with increased risk of respiratory symptoms and development of COPD independent of the effect of smoking.2,3 When assessing socioeconomic status by occupation, COPD is associated with manual occupations. This may be due to a higher prevalence of smoking in the group, as well as increased exposure to vapors, gases, dust or fumes in the industrial setting compared to non-industrial workplaces.4 Moreover, patients with COPD who are disabled have lower health-related quality of life compared with employed individuals with the same severity of COPD.5 In persons suffering from COPD, it seems clear that higher socioeconomic status is associated with better health outcomes and lower mortality.6 The specific reasons for these differences are not understood. However, one possible explanation could be different prescription patterns between low and high socioeconomic status groups.
Like other healthcare systems, the Swedish system aims for equal access to care and treatment for all patients, regardless of socioeconomic status. Recent Swedish reports indicates that differences may exist and individuals with higher socioeconomic status tend to seek healthcare more often than those with lower socioeconomic status.7 In this regard, the differences in seeking care in groups stratified by their level of education have been of the most concern.8,9 As the risk of developing COPD is increasing in individuals with low socioeconomic status,10,11 it is of great importance to assure that the structure of public healthcare is adjusted accordingly and that this patient group is receiving the same quality of care as patients with a more favorable socioeconomic situation. It is unclear if access to prescription medication or choice of medication by the healthcare provider varies between socioeconomic groups. This could be a contributing factor to the difference in outcome. We hypothesized that dispensation of triple therapy, ie a combination of long-acting muscarinic antagonists (LAMA), long-acting beta2-agonists (LABA) and inhaled corticosteroids (ICS), is more frequently prescribed than monotherapy with LAMA in patients with high socioeconomic status.
Methods
Patient data were extracted from national registries: The Swedish National Airway Register (SNAR),12 The longitudinal integrated database for health insurance and labour market (LISA), Statistic Sweden (SCB),13 The National Prescribed Drug Register and the National Patient Register (The National Board of Health and Welfare).14 The current study was approved by the Swedish Ethics Review Authority (2019–04915; 2020–00508). Informed consent is not required in Sweden when anonymized public register data is used for research.
Study Population and Design
A retrospective observational study using Swedish national registries was undertaken. The COPD cohort was defined by data obtained from SNAR and consisted of incident and prevalent patients with COPD (J44, ICD-10) aged 40 years or older. The patients had visited primary care and registered at least once in the SNAR from January 2021 to December 2022. If multiple registrations, the last registration was used as index-date. Patients with concomitant asthma (J45, ICD-10) were excluded from the study population, Figure 1.
 |
Figure 1 Flow-chart of the study population. Abbreviations: SNAR, Swedish National Airway Register, GOLD, Global Initiative for Chronic Obstructive Lung Disease. Notes: *Others=Patients with missing data on CAT and/or information on prescribed OCS or no hospitalization 12 months pre-index. |
Extracted data from SNAR included sex, age, Body Mass Index (BMI), smoking habits (non-smoker, ex-smoker since more than 6 months, current smoker), the COPD Assessment Test (CAT), and lung function values. Swedish reference values for lung function were used.15,16
Linkages of SNAR to other Swedish registers were conducted. Level of education and annual household income were extracted from The Longitudinal Integrated Database for Health Insurance and Labor Market (LISA). The level of education was divided into low (elementary school), medium (high school) and high (university education). Data on annual household annual income was divided into tertiles: low: ≤181 000 SEK (16,250 €) per year, medium:181000- ≤253 000 SEK per year, and high: >253 000 SEK (22,715 €) per year.
Dispensation of pharmacological maintenance treatments were collected from The National Prescribed Drug Register in 2022; inhaler treatment both as monotherapy and separate combination of drugs (R03), cardiovascular and hypertension medication (C01, C02, C07, C08, C09), antidepressive medication (N06), and diabetes medication (A10). To define moderate and severe exacerbations, the use of oral corticosteroids (OCS; H02AB) was extracted from the National Prescribed Drug Register and respiratory hospitalization (J41-J44, J96, J12-J18 or J20-J22) was extracted from the National Patient Register 12-months pre-index date. Based on CAT and exacerbation history patients were categorized into group A (CAT <10, ≤1 non-hospitalized exacerbation last year), B (CAT ≥10, ≤1 non-hospitalized exacerbation last year) and E (≥2 exacerbation or one hospitalization due to an exacerbation last year) according to GOLD criteria.1 Patients with missing data on CAT and/or information on prescribed OCS or no hospitalization 12 months pre-index, were labeled as “others”.
Statistical Methods
The association between categorical variables was assessed using Pearson’s Chi-square test. In cases where any cell in the contingency table had an expected count of less than five, p-values were calculated using Monte Carlo simulations (with 10,000 replications), ensuring robustness despite sparse data. If an overall Chi-square test yielded a statistically significant result, a post-hoc analysis was conducted to identify which specific cells contributed to the association. The statistical significance for each cell was determined using the exact approach detailed by Shan and Gerstenberger.17 Specifically, the contingency table was collapsed into a 2×2 table for each cell of interest (comparing the observed cell count against the counts of all other cells in its row and column). Fisher’s exact test was then applied to each of these 2×2 tables to generate a cell-wise p-value. The resulting set of p-values was subsequently adjusted for multiple comparisons using Hommel’s method18 to control the family-wise error rate. This adjustment procedure was chosen as it is valid for the positively associated test that arise from this type of cell-wise analysis, while being more powerful than traditional corrections like Bonferroni.19 To quantify the direction and magnitude of each contribution, the ratio of observed to expected counts was calculated for each cell.
To confirm the robustness of the primary findings, a sensitivity analysis using log-linear (Poisson) regression was conducted. A series of models were fitted to test for potential three-way interaction between type of COPD medication, socioeconomic factors, and other variables (smoking habits and exacerbations). No three-way interactions were found to be statistically significant. The overall lack of significant higher-order interactions supported the reporting of the simpler two-way Chi-square analyses. A p-value <0.05 was considered statistically significant. All statistical analyses were conducted using R version 4.4.2.20
Results
Study Population
In total 38,692 patients with COPD (55.5% women) were included in the study. Mean age was 73.6 (SD 9.09) years and mean FEV1 was 59.5% (SD 18.9) of predicted value. Full information on CAT score and exacerbation history enabled classification into GOLD groups A, B and E in 29,128 patients. For the remaining 9564 patients no group was assigned, and they were analyzed as “others”. Patient data are given in Table 1.
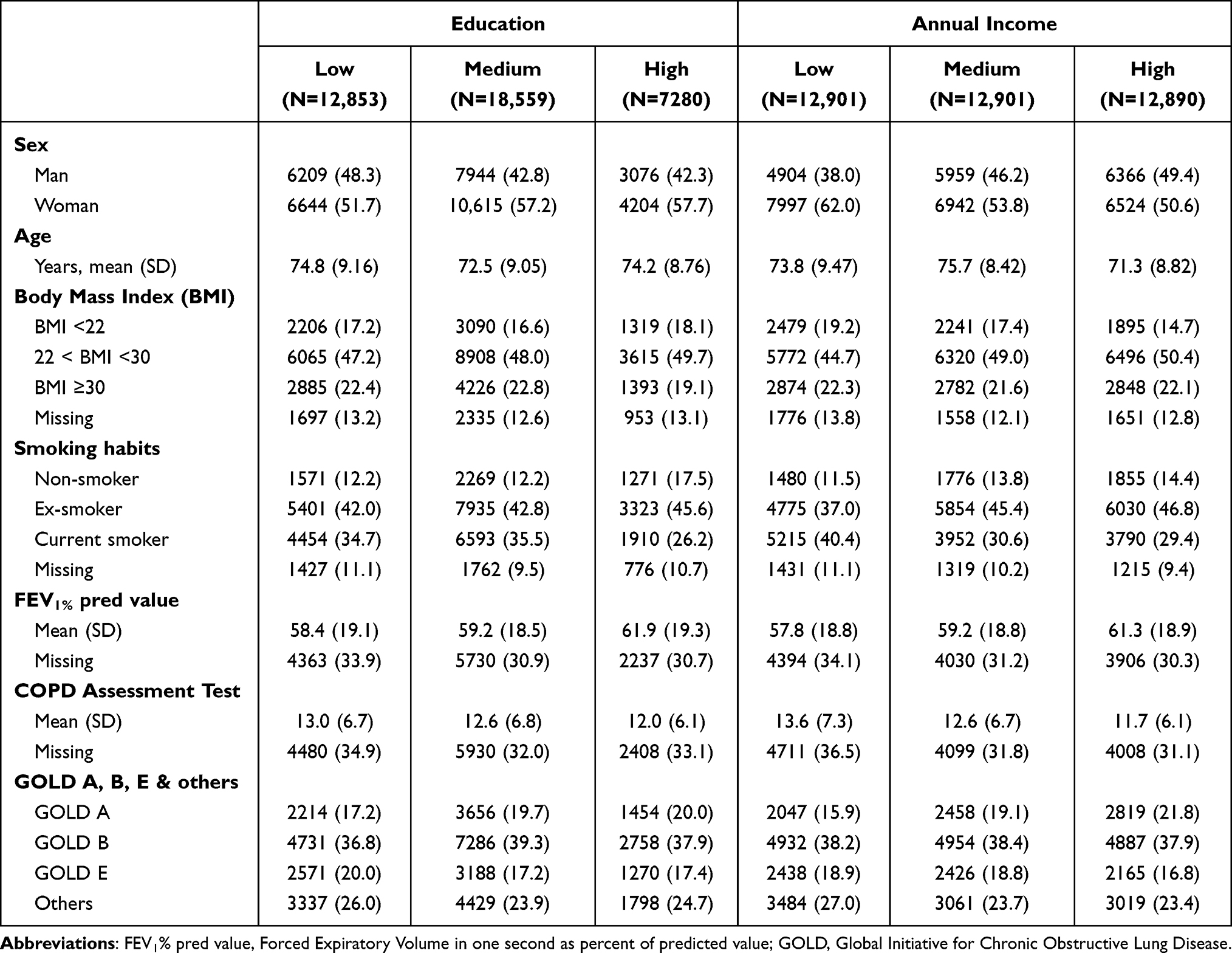 |
Table 1 Patient Characteristics. Number of Patients with Percent Within Brackets Are Given if Not Otherwise Indicated |
No COPD medication was prescribed for 17.5% of the patients in GOLD A, 6.6% in group B and 5.0% in group E. Among group A and B patients who had experienced one exacerbation during the last year no medication was prescribed to 9.0% and 2.6% of the patients, respectively. Dual bronchodilatation (long-acting antimuscarinic agents, LAMA + long-acting beta-2 agonists, LABA), fixed or open combination, as the only treatment was prescribed to 19.1% in group A, to 25.7% in group B, and to 15.5% in group E. A fixed or open combination of inhaled steroids (ICS) and LABA as the only treatment was prescribed to 8.4% of the patients in group A, 7.0% of the patients in group B and 14.4% in group E. Triple therapy (LAMA + LABA + ICS) was prescribed to 17.1% of the patients in group A, 33.9% in group B and to 51.5% of the patients in group E. Among patients in group A who had not experienced an exacerbation last year 15.7% had been prescribed triple therapy and in group B, triple therapy had been prescribed to 31.5% of the patients without a history of exacerbation last year. Cardiovascular drugs were prescribed to 30,026 patients (77.6%), antidepressive medication to 11530 patients (29.8%) and diabetes medication to 8311 patients (21.5%). Pharmacological treatment for COPD (divided by GOLD group A, B and E) and treatment for other conditions stratified by level of education and income are shown in Table 2.
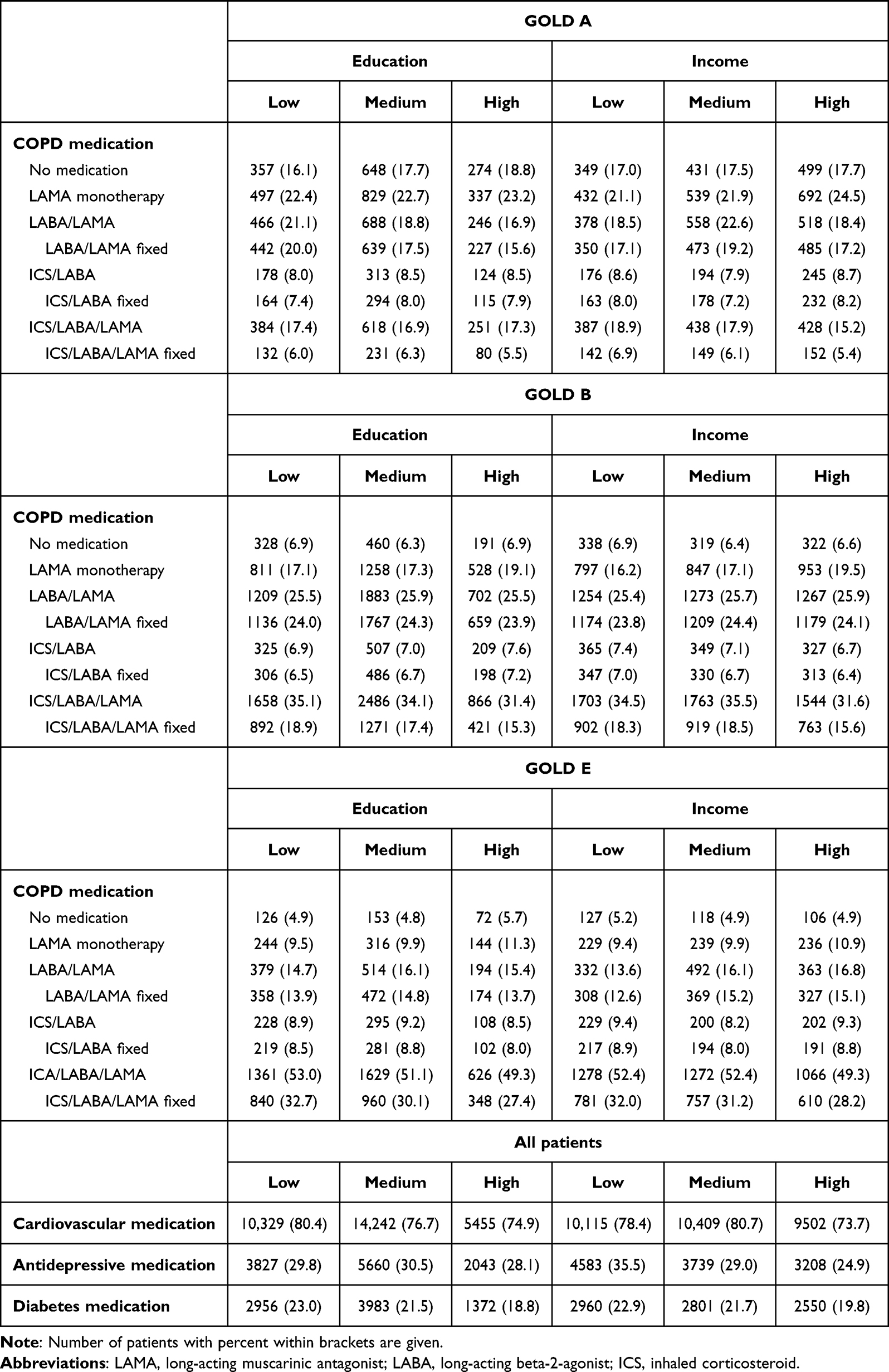 |
Table 2 The Most Frequently Used Pharmacological Treatment for COPD (Divided by GOLD Group A, B and E) and Treatment for Other Conditions in Patients with Low, Medium and High Education and with Low, Medium and High Income. Drug Combinations Are Presented as Total Use (Drugs Given in Separate Inhalers or as Fixed Combination in One Inhaler) and Use of Fixed Combination in One Inhaler |
Gender Distribution
Based on the expected distribution of patients within the different GOLD groups there was a significant over-representation of women (ratio 1.04) and under-representation of men (ratio 0.95) in group E (p=0.001) whereas no such differences were found in group A and B. More men (ratio 1.14) and less women (ratio 0.89) than expected had no pharmacological treatment (p<0.0001). Fixed combinations of bronchodilators (LAMA + LABA) were more often prescribed than expected among men (ratio 1.05) and more seldom among women (ratio 0.96; p=0.002) and there was an over-representation of treatment with open triple therapy in women (ratio 1.06) and the opposite in men (ratio 0.92; p<0.0001, Table 3).
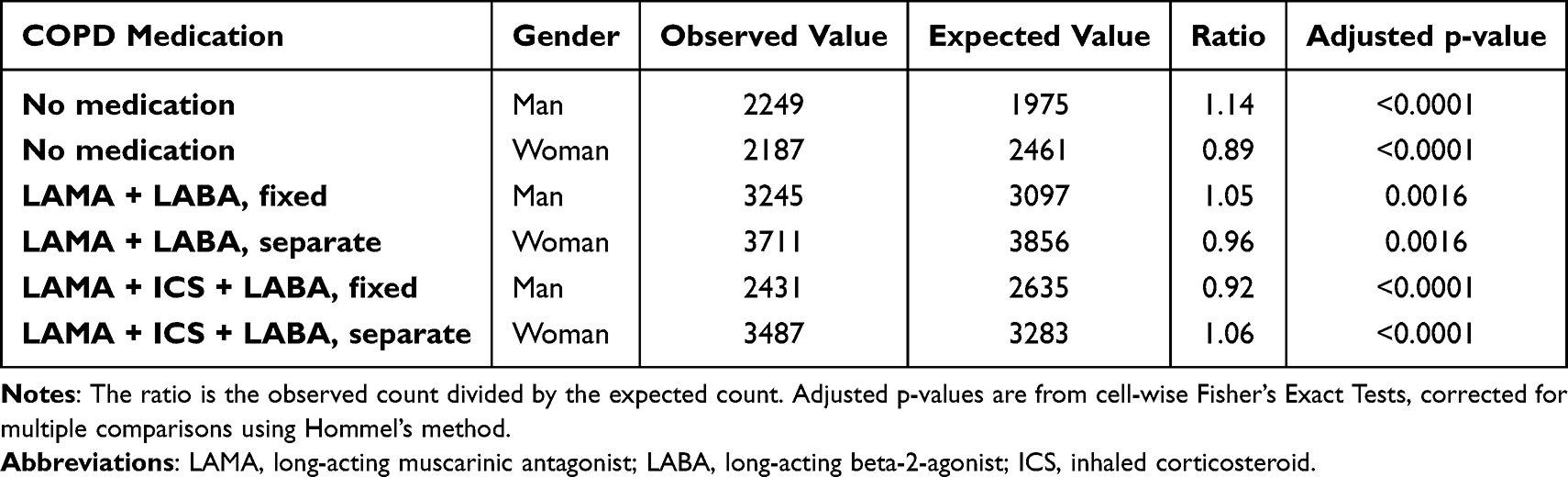 |
Table 3 Observed and Expected Proportion of Female and Male Patients with COPD Who Did Not Receive Any Pharmacological Treatment and Who Received Dual Bronchodilatation (LAMA + LABA) and Triple Therapy (LAMA + LABA + ICS). For All Other Drug or Drug Combination Treatment No Statistically Significant Differences Were Found |
Education
The proportion of patients in group E was slightly higher in patients with low education (20.0%) than in patients with medium (17.2%) and high education (17.4%, Table 1). Fixed triple combination (LAMA/LABA/ICS) was more frequently prescribed than expected for patients with low education (ratio 1.09) and the opposite for patients with high education (ratio 0.87; p<0.0001 for both, Table 4). In group A and group E and in “Others” prescription of drugs and combination of drugs did not differ from what was expected, neither in patients with low, medium nor high education. In group B triple therapy was less often than expected prescribed in patients with high education (ratio 0.87; p=0.0250, Table 4).
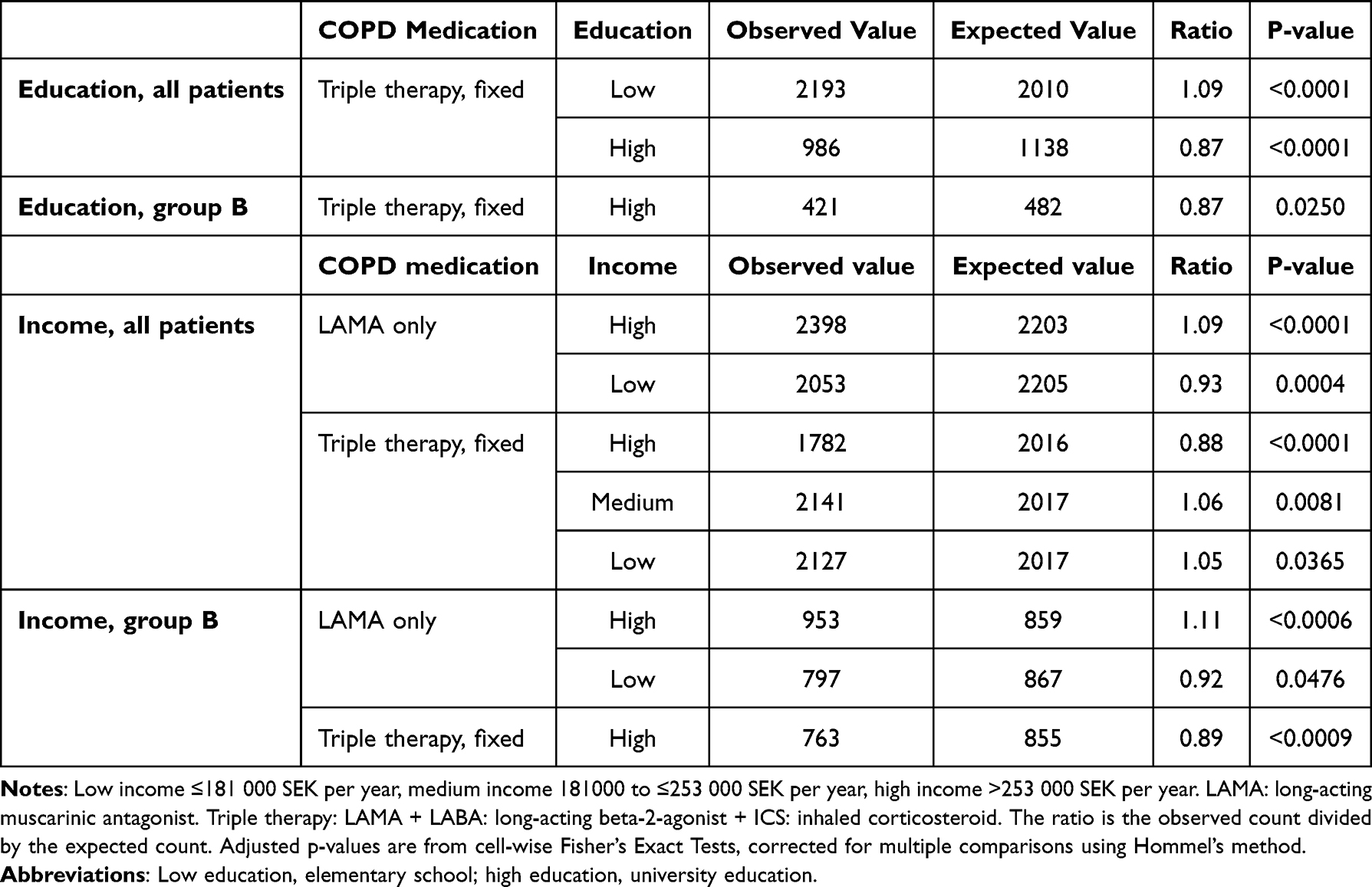 |
Table 4 In the Table Prescription of COPD Medication Related to Educational Level and Income Is Presented Among All Patients and in GOLD Group B Patients Where Statistically Significant Differences Were Found. Among Patients in Group A and E Prescription Did Not Differ Statistically Significant Between Different Education or Income Levels (Data Not Presented) |
Income
The proportion of patients in group E was slightly lower in patients with high income (16.8%) than in patients with medium (18.8%) and low (18.9%) income (Table 1). LAMA as monotherapy was more frequently prescribed among patients with high income (ratio 1.09; p<0.0001) and less frequently prescribed among patients with low income (ratio 0.93; p=0.0004, Table 4). Triple therapy was less often prescribed than expected in patients with high income (ratio 0.88; p<0.0001) and more often in patients with medium (ratio 1.06; p=0.0081) and low (ratio 1.05; p=0.0365) income (Table 4). In group A and group E and in “Others” prescription of drugs and combination of drugs did not differ from what was expected in patients with low, medium and high income. In group B monotherapy with LAMA was more often prescribed than expected among high income (ratio 1.11, p<0.0006) and less often than expected among patients with low income (ratio 0.92, p=0.0476, Table 4). In group B fixed combinations of triple therapy were less frequently prescribed than expected in patients with high income (ratio 0.89, p=0.0009, Table 4).
Discussion
In the present study small, but statistically significant, differences in prescription pattern related to socioeconomic factors were demonstrated. Thus, fixed triple therapy was more often prescribed than expected to patients with low socioeconomic status whereas monotherapy with LAMA was more often prescribed to patients with high socioeconomic status as reflected by education and income. Due to the reimbursement system in Sweden, there is a ceiling for the patients costs of drugs which imply that most patients can afford to collect prescribed drugs from the pharmacy. In addition, the cost does not differ much between different drugs and drug combinations used for treatment of COPD. In conclusion, this implies that economic and other socioeconomic factors such as education and annual income do not seem to influence much on how prescribed inhaled therapy in COPD is chosen in Sweden. Interestingly, it was found that prescription of fixed triple therapy was more often observed than expected in patients with low education and medium and low income whereas the opposite was found in patients with high education and high income. In addition, monotherapy with LAMA was more often prescribed than expected in patients with high income and less often in patients with low income. The reason for this is not clear but severity of the disease may have been of importance. It could not be excluded that a higher exacerbation rate in patients with low socioeconomic status may contribute to the higher prescription of triple therapy in that group. A slightly lower prevalence of exacerbations in patients with a higher socioeconomic status implies treatment with bronchodilators, e g monotherapy with LAMA, rather than inhaled steroids. The slightly higher prevalence of exacerbations in patients with low income and low education may be a contributing factor to these differences in prescription pattern.
Our results did not confirm the findings of Töttenborg et al21 who showed that COPD outpatients with high educational level were more likely to receive high standard care. In another Danish study it was demonstrated that low income and low education, among other factors, were associated with poor or non- adherence to prescribed pharmacologic treatment and to increased exacerbation rate and mortality in patients with COPD.22 This may indicate a difference from the results of the present study in which triple therapy was more often observed in patients with low socioeconomic status and that monotherapy with LAMA more often is observed in patients with high socioeconomic status. However, in the present observational study clinical outcomes and adherence to treatment were not assessed, indicating that firm clinical conclusions could not be drawn from the differences in prescription pattern.
An intriguing observation was that prescription of pharmacological treatment, both monotherapy and drug combinations, at the different educational levels and annual income did not differ from the expected prescription in group A and E whereas there were prescription differences in group B in that regard. In patients with minor symptoms and few exacerbations (group A) and in patients with frequent exacerbations (group E) the choice for drug treatment is often more obvious. In patients with a more complex clinical picture with frequent symptoms which are not always easy to classify as exacerbations, ie patients in group B, the choice of prescription may not be as clear as it is in group A and E.
In Sweden the mortality due to COPD has steadily decreased among men during the last 25 years while, during that time, an increased mortality has been observed in women. The mortality due to COPD is thus higher among women than among men in Sweden since the last 15 years.23 It has been shown that the mortality and readmission to hospital after a severe exacerbation is higher in patients with low socioeconomic status24 and that mortality decreases slower over time in patients with low socioeconomic status.6 Recent data support that not only individual but also neighborhood socioeconomic status is of importance for the mortality in COPD.25,26 A close relationship between exacerbations and mortality in COPD is well established. In the present study 11.6% of patients in group A and 16.3% of patients in group B experienced one exacerbation throughout the last year while the remaining patients in group A and B were free from exacerbations. We found a clear over-representation of women in group E indicating that frequent exacerbations are more common in women than in men in Sweden. The findings may indicate that COPD would more severely affect women than men. These findings are in accordance with the finding that women were more often than expected treated with triple therapy which includes inhaled steroids and that men more often than expected did not receive any pharmacological treatment for their disease. Also, the over-representation of men being prescribed dual bronchodilation indicates that treatment of COPD in men may be more guided by symptoms, mainly dyspnea, while treatment in women is more focused on preventing exacerbations.
Prescription of COPD medication was twice as common in group A patients who had experienced an exacerbation last year compared with those who were free from exacerbations, and prescription of bronchodilators was similar in group A and B patients with and without a history of exacerbations. Furthermore, triple therapy was more often prescribed to group B patients with a history of exacerbation than group B patients without exacerbations. These results indicate that symptoms seem important for prescription of bronchodilators and that exacerbations are important for the decision to add ICS to the treatment.
More than one patient out of four were treated with drugs for cardiovascular diseases and/or hypertension. The prescription of cardiovascular drugs was similar in group A and B and slightly higher in group E. Lung function was similar in group A, B, E and “Others” (FEV1 55.6–62.7% of predicted value) implicating that most patients were in stage 2 according to GOLD. This confirms earlier findings that cardiovascular comorbidities and events are common in mild and moderate COPD.27–30
The strength of the study is the large national sample based on extensive registry data including all patients visiting the included primary healthcare centers during the years 2021 and 2022. The data does not allow conclusions about clinical implications or adherence to prescribed treatment which are limitations of the study. Thus, future research on adherence to COPD medication in relation to socioeconomic status is needed. Although not crucial for the interpretation of the results, other limitations are missing data on FEV1% of predicted value (32%) and CAT-scores (35%).
In conclusion, from previous Swedish studies it is known that patients with COPD have a lower socioeconomic status than matched patients with other diagnoses.31 In the present study we found small, but statistically significant, differences in prescription pattern associated with socioeconomic status. There was a difference in prescription pattern with fixed triple treatment, which was more often prescribed to patients with low socioeconomic status and monotherapy with LAMA more often prescribed to patients with high socioeconomic status. To reach maximal health equity it is of importance that current guidelines for treatment of COPD are followed and that treatment is prescribed irrespective of socioeconomic status.
Abbreviations
COPD, chronic obstructive pulmonary disease; CAT, COPD assessment test; BMI, body mass index; FEV1, forced expiratory volume in one second; LAMA, long-acting antimuscarinic agents; LABA, long-acting beta-2 agonists; ICS, inhaled steroids; SNAR, the Swedish national airway register; LISA, the longitudinal integrated database for health insurance and labour market.
Acknowledgments
This study was funded by Chiesi Pharma AB, Sweden. Acknowledgements are given to all the patients and healthcare professionals who contribute with registrations in SNAR, and to the SNAR steering committee and register coordinators.
Disclosure
KL has, during the last five years, on one or more occasion served in an advisory board and/or served as speaker and/or participated in education arranged by AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Novartis and Sanofi. BF is current employee at Chiesi Pharma AB. LEGWV reports grants from AstraZeneca and personal fees for lectures and/or advisory board work from AstraZeneca, GSK, Novartis, Boehringer, Pulmonx, Grifols, Sanofi, and Chiesi. CS reports personal fees from AstraZeneca and GSK, and institutional fees from Chiesi and TEVA, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Global initiative for chronic obstructive pulmonary disease (GOLD). Global strategy for the diagnosis, management and prevention of COPD 2024 report. Available from: https://goldcopd.org/.
2. Eagan TM, Gulsvik A, Geir E, et al. The effect of educational level on the incidence of asthma and respiratory symptoms. Respir Med. 2004;98(8):730–736. doi:10.1016/j.rmed.2004.02.008
3. Kunutsor SK, Young JS, Mäkikallio TH, et al. High fitness levels offset the increased risk of chronic obstructive pulmonary disease due to low socioeconomic status: a cohort study. Respir Med. 2021;189:106647. doi:10.1016/j.rmed.2021.106647
4. Jalasto J, Lassmann-Klee P, Schyllert C, et al. Occupation, socioeconomic status and chronic obstructive respiratory diseases - the EpiLung study in Finland, Estonia and Sweden. Respir Med. 2022;191:106403. doi:10.1016/j.rmed.2021.106403
5. Orbon KH, Schermer TR, van der Gulden JW, et al. Employment status and quality of life in patients with chronic obstructive pulmonary disease. Int Arch Occup Environ Health. 2005;78(6):467–474. doi:10.1007/s00420-005-0617-7
6. Gershon AS, Hwee J, Victor JC, et al. Trends in socioeconomic status-related differences in mortality among people with chronic obstructive pulmonary disease. Ann Am Thorac Soc. 2014;11(8):1195–1202. doi:10.1513/AnnalsATS.201403-094OC
7. Vård och omsorgsanalys. Vården ur befolkningens perspektiv. International health policy survey (IHP) 2023. 2024. Article number 2024:3. Available from: www.vardanalys.se.
8. The Public Health Agency of Sweden. The development of public health. Annual report. 2022. Article number 22026. Available from: www.folkhalsomyndigheten.se.
9. The National Board of Health and Welfare. Arbetssätt för Jämlik vård. Redovisning av metodutvecklingsprojekt på Socialstyrelsen 2019. Article number 2020-2-6636. Available from: www.socialstyrelsen.se.
10. Gershon AS, Warner L, Cascagnette P, et al. Lifetime risk of developing chronic obstructive pulmonary disease: a longitudinal population study. Lancet. 2011;378(9795):991–996. doi:10.1016/S0140-6736(11)60990-2
11. Beran D, Heather JZ, Perrin C, et al. Burden of asthma and chronic obstructive pulmonary disease and access to essential medicines in low-income and middle-income countries. Lancet Respir Med. 2015;3(2):159–170. doi:10.1016/S2213-2600(15)00004-1
12. Stridsman C, Konradsen JR, Vanfleteren L, et al. The Swedish national airway register (SNAR): development, design and utility to date. Eur Clin Respir J. 2020;7(1):1833412. doi:10.1080/20018525.2020.1833412
13. Statistics Sweden (SCB). About statistics sweden. 2024. Available from: www.scb.se/en.
14. The Swedish National Board of Health and Welfare. Statistical databases. 2024. Available from: www.socialstyrelsen.se/en/statistics-and-data/registers.
15. Hedenström H, Malmberg P, Agarwal K. Reference values for lung function tests in females. Regression equations with smoking variables. Bull Eur Physiopathol Respir. 1985;21(6):551–557.
16. Hedenstrom H, Malmberg P, Fridrikson H. Reference values for lung function tests in men: regression equations with smoking variables. Ups J Med Sci. 1986;91(3):299–310. doi:10.3109/03009738609178670
17. Shan G, Gerstenberger S. Fisher’s exact approach for post hoc analysis of a chi-squared test. PLoS One. 2017;12(12):e0188709. doi:10.1371/journal.pone.0188709
18. Hommel G. A stagewise rejective multiple test procedure based on a modified bonferroni test. Biometrika. 1988;75(2):383–386. doi:10.1093/biomet/75.2.383
19. Sarkar SK, Chang CK. The simes method for multiple hypothesis testing with positively dependent test statistics. J Am Stat Assoc. 1997;92(440):1601–1608. doi:10.1080/01621459.1997.10473682
20. R Core Team. R: a language and environment for statistical computing. R foundation for statistical computing. 2024. Available from: https://www.R-project.org/.
21. Tottenborg SS, Lange P, Thomsen RW, et al. Reducing socioeconomic inequalities in COPD care in the hospital outpatient setting - A nationwide initiative. Respir Med. 2017;125:19–23. doi:10.1016/j.rmed.2017.02.016
22. Tottenborg SS, Lange P, Paaske Johnsen S, et al. Socioeconomic inequalities in adherence to inhaled maintenance medications and clinical prognosis of COPD. Respir Med. 2016;119:160–167. doi:10.1016/j.rmed.2016.09.007
23. The national board of health and welfare cause of death register. 2021. Available from: www.socialstyrelsen.se.
24. Gershon AS, Thirucheivam D, Aaron S, et al. Socioeconomic status (SES) and 30-day hospital readmissions for chronic obstructive pulmonary (COPD) disease: a population-based cohort study. PLoS One. 2019;14(5):e0216741. doi:10.1371/journal.pone.0216741
25. Cho KH, Nam CM, Lee EJ, et al. Effects of individual and neighborhood socioeconomic status on the risk of all-cause mortality in chronic obstructive pulmonary disease: a nationwide population-based cohort study, 2002-2013. Respir Med. 2016;114:9–17. doi:10.1016/j.rmed.2016.03.003
26. Galiatsatos P, Paulin LM, Kind A, et al. The association between neighborhood socioeconomic disadvantage and chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2020;15:981–993. doi:10.2147/COPD.S238933
27. Berry CE, Wise RA. Mortality in COPD: causes, risk factors, and prevention. COPD. 2010;7(5):375–382. doi:10.3109/15412555.2010.510160
28. Kunisaki KM, Dransfield MT, Anderson JA, et al. Exacerbations of chronic obstructive pulmonary disease and cardiac events. A Post Hoc cohort analysis from the SUMMIT randomized clinical trial. Am J Respir Crit Care Med. 2018;198(1):51–57. doi:10.1164/rccm.201711-2239OC
29. Vogelmeier CF, Rhodes K, Garbe E, et al. Elucidating the risk of cardiopulmonary consequences of an exacerbation of COPD: results of the EXACOS-CV study in Germany. BMJ Open Respir Res. 2024;11(1):e002153. doi:10.1136/bmjresp-2023-002153
30. Graul EL, Nordon C, Rhodes K, et al. Temporal risk of nonfatal cardiovascular events after chronic obstructive pulmonary disease exacerbation: a population-based study. Am J Respir Crit Care Med. 2024;209(8):960–972. doi:10.1164/rccm.202307-1122OC
31. Larsson K, Lisspers K, Ställberg B, et al. Treatment patterns, socioeconomic status and clinical burden in mild COPD: a Swedish real-world, retrospective cohort study, the arctic study. Int J Chron Obstruct Pulmon Dis. 2022;17:1409–1421. doi:10.2147/COPD.S364932
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Interaction Between Venous Thromboembolism and Socioeconomic Status on the Risk of Disability Pension
Jørgensen H, Horváth-Puhó E, Laugesen K, Braekkan SK, Hansen JB, Sørensen HT
Clinical Epidemiology 2022, 14:489-500
Published Date: 14 April 2022
Basic Determinants of Disease Knowledge in COPD Patients: Results from COSYCONET
Fischer C, Jörres RA, Alter P, Trudzinski FC, Yildirim, Bals R, Vogelmeier CF, Kauffmann-Guerrero D, Behr J, Watz H, Holle R, Kahnert K
Patient Preference and Adherence 2022, 16:1759-1770
Published Date: 26 July 2022
Associations Between Adult Attention-Deficit/Hyperactivity Disorder (ADHD) Traits and Sociodemographic Characteristics in Japanese Workers
Suzuki T, Wada K, Nakazato M, Ohtani T, Yamazaki M, Ikeda S
Neuropsychiatric Disease and Treatment 2023, 19:759-773
Published Date: 5 April 2023
Cardiovascular Disease in China: Socioeconomic Status Variation in Prevalence
Zhang C, Shen Y, Wang A, Wang D, Cao L, Yue W
Risk Management and Healthcare Policy 2023, 16:2077-2084
Published Date: 9 October 2023
Intersectional Stigma Among Older People with HIV and COPD in Alabama: A Qualitative Study of Three Cases
Byun JY, Chapman Lambert C, Fazeli PL, Iyer AS, Batey DS, Vance DE
Nursing: Research and Reviews 2023, 13:77-85
Published Date: 20 December 2023