Back to Journals » Clinical Epidemiology » Volume 14
The Interaction Between Venous Thromboembolism and Socioeconomic Status on the Risk of Disability Pension
Authors Jørgensen H ![]() , Horváth-Puhó E
, Horváth-Puhó E ![]() , Laugesen K
, Laugesen K ![]() , Braekkan SK, Hansen JB, Sørensen HT
, Braekkan SK, Hansen JB, Sørensen HT ![]()
Received 14 February 2022
Accepted for publication 5 April 2022
Published 14 April 2022 Volume 2022:14 Pages 489—500
DOI https://doi.org/10.2147/CLEP.S361840
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Eyal Cohen
Helle Jørgensen,1– 3 Erzsébet Horváth-Puhó,2 Kristina Laugesen,2 Sigrid K Braekkan,1,3 John-Bjarne Hansen,1,3 Henrik Toft Sørensen2
1Thrombosis Research Center (TREC), Department of Clinical Medicine, UiT, The Arctic University of Norway, Tromsø, Norway; 2Department of Clinical Epidemiology, Department of Clinical Medicine, Aarhus University Hospital and Aarhus University, Aarhus, Denmark; 3Division of Internal Medicine, University Hospital of North Norway, Tromsø, Norway
Correspondence: Helle Jørgensen, Email [email protected]
Background: Venous thromboembolism (VTE) is associated with increased risk of disability pension. How socioeconomic status (SES) impacts the risk of disability pension after a VTE is unknown. The aim of this nationwide population based cohort study to investigate the interaction between SES and incident VTE on the risk of subsequent disability pension.
Methods: Using Danish national medical and administrative databases, we established a nationwide cohort of 41,781 individuals aged 25– 65 years with incident VTE during 1995– 2016 and a comparison cohort (n=208,905) from the general population matched on year of birth, sex, and calendar year of VTE. We computed incidence rates (IRs) as the number of disability pension events per 1000 person-years at risk and measured the interaction between VTE and levels of SES (high, medium, low) on an additive scale by calculating interaction contrasts (difference in IR difference).
Results: Among individuals with high SES, the disability pension IR per 1000 person-years was 5.4 (95% CI: 4.8– 6.1) in the VTE cohort and 1.6 (95% CI: 1.5– 1.7) in the comparison cohort (IR difference 3.8). The corresponding disability pension IR in individuals with low SES was 55.1 (95% CI: 52.1– 58.1) in the VTE cohort and 26.1 (95% CI: 25.1– 27.1) in the comparison cohort (IR difference 24.0). An interaction contrast of 25.1 indicated that interaction accounted for 45.6% (25.1/55.1) of the disability pension IR in individuals with VTE and low SES.
Conclusion: SES and VTE interact to increase the risk of disability pension after VTE beyond their independent effects.
Keywords: education, employment, income, deep-vein thrombosis, pulmonary embolism, burden of illness
Introduction
Venous thromboembolism (VTE), encompassing deep vein thrombosis (DVT) and pulmonary embolism (PE), is a leading cause of lost disability-adjusted life-years worldwide.1 VTE is common in the working-age population,2 and as the workforce is ageing, more individuals will be faced with chronic diseases causing health problems that may hamper the ability to maintain employment.3 Even though effective treatments enable patients to continue working after a VTE,2 the risk of losing a substantial number of years in paid employment remains high among individuals with VTE.1
Recent studies have shown that individuals with VTE have an increased risk of work-related disability pension compared to the general population.4,5 Also, socioeconomic inequalities have been found to be associated with risk of VTE.6–10 However, it remains unclear whether the impact of socioeconomic status (SES) on the risk of disability pension among individuals with VTE is due to SES and VTE separately, or whether an interaction exists.
To prevent early exit from the labour market among individuals with VTE, a better understanding is needed not only of the risk factors, but also of the interaction between factors that affect the risk of disability pension beyond the factors’ independent effects. Therefore, the aim of this nationwide population-based cohort study was to investigate the interaction between incident VTE and categories of SES on the risk of subsequent disability pension.
Methods
Setting and Data Sources
All Danish residents have free and equal access to universal tax-funded health care and education.11 The Danish Civil Registration System (CRS) assigns a unique personal identifier (CPR number) to all Danish residents upon birth or immigration and this number enables linkage of information between nationwide health and administrative registers.11
We used the Danish National Patient Registry (DNPR) to collect data on VTE and comorbidities and the Danish Psychiatric Central Research Register (DPCCR) to collect data on psychiatric diagnoses.11 The DNPR contains records of all Danish hospital discharges since 1977 and emergency room and outpatient visits from 1995 onwards. Records include CPR number, admission and discharge dates, one primary diagnosis and one or more secondary diagnoses coded according to ICD-8 codes (from 1977 until 1994) or ICD-10 codes (from 1994 onwards).11 Information on demography, vital status, and migration was collected from the CRS, while disability pensions, income, and employment status was collected from the Integrated Database for Labour Market Research (IDA), and educational level was collected from the Educational Attainment Register.11
Study Population
We identified 41,781 hospital or outpatient clinic patients with a primary or secondary discharge diagnosis of DVT and/or PE from January 1, 1995 through December 31, 2016. We defined the VTE date as the date of the first hospital admission/outpatient visit (Supplementary Table 1). For DNPR data, positive predictive values of 86% for DVT and 90% for PE have been reported.12 VTEs reported solely in emergency room departments were not included due to a high proportion of clinical misclassification.13 If a DVT and PE occurred concurrently, we registered the event as a PE due to its higher mortality rate.14 We classified VTE events as provoked or unprovoked according to the presence of provoking factors at the time of diagnosis, such as a preexisting cancer diagnosis, fracture, trauma, surgery, and/or pregnancy within 90 days prior to VTE diagnosis (Supplementary Table 1).15
For each individual with VTE, we used the CRS to match five individuals, with replacement,16 from the general working-age population by sex, year of birth, and calendar year of VTE. The date of VTE was used as the index date for the matched comparison cohort members (n=208,905). Comparison cohort members subsequently experiencing a VTE were censored on the date of the event.
Individuals with a VTE diagnosis before 1995 were excluded. To avoid potential bias and ensure that the VTE was the cause and not a consequence of another condition leading to disability pension, we also excluded individuals already receiving a disability pension and those receiving a disability pension in the same year as the VTE. Further, individuals aged <25 years or ˃65 years at study inclusion were excluded as they would either likely still be in school/university and lack a stable income or employment, or be retired from work due to advanced age, and therefore not meet the requirements for disability pension.
Socioeconomic Status
We defined SES as the combined measure of educational level, employment status, and annual income. Information on the highest level of completed education was extracted the year prior to the VTE/index date and categorized as low, medium, or high according to the distribution of education in age-specific groups (Supplementary Tables 2 and 3). To account for salary changes over calendar years and avoid the impact of inflation, income values were re-calculated using the new gross domestic product deflators downloaded from the World Bank's website (www.worldbank.org). Based on the deflated income values of the study population, we calculated income quartiles and merged the two middle quartiles to get three categories (ie high, medium, and low income). We measured employment status the year prior to the VTE/index date and categorized employment status as high (ie employed), medium (ie outside the workforce) and low (ie unemployed), where persons included in an educational program, those in early retirement, and those receiving other types of public support were considered being outside the workforce.
Based on the categorical distribution “low, medium, and high” described above, we established a score of 1–3 for each of the SES indicators education, income, and employment status. These scores were then combined in a composite SES score with values ranging from 3 to 9. Based on the distribution in the composite SES score, we calculated tertiles of low SES (scores of 3 and 4), medium SES (scores of 5, 6, and 7), and high SES (scores of 8 and 9).
Disability Pension
The outcome was receipt of disability pension. In Denmark, persons with permanent Danish residency who have lived in the country for at least three years since their 15th birthday until receipt of disability pension or public retirement age, can be granted disability pension if her/his work capacity is reduced permanently or to such a degree that he/she is incapable of providing for himself/herself through regular or flexible work.17
For each year, we identified disability pension yearly at the end of November and set the disability pension date as January 1 that year. Direct transition from work to disability pension is rare as most persons experience a period of sick leave prior to receipt of disability pension. Furthermore, Danish regulations require that measures to improve the working ability must be performed before disability pension can be granted.17
Covariates
Diagnoses of comorbidities prior to the VTE were obtained from the DNPR and the DPCCR using ICD-8 and ICD-10 codes for cancer, obesity, coronary heart disease (including atrial fibrillation, myocardial infarction, and heart failure), mental diseases, diabetes, stroke, chronic obstructive pulmonary disease (COPD), acute kidney failure, and chronic kidney disease, and remaining diseases included in the Charlson Comorbidity Index.18 In addition, we retrieved information on surgery, pregnancy, and trauma/fractures three months prior to the VTE/index date. ICD codes are provided in Supplementary Table 1.
Statistical Analysis
We followed the study population from the VTE/index date until receipt of disability pension, turning 66 years of age, emigration, death, or December 31, 2016, whichever came first. Within categories of SES score (low, medium, high), we conducted a complete case analysis where we estimated incidence rates (IRs) per 1000 person-years with 95% confidence intervals (CIs) for disability pension.
We examined the presence of interaction between VTE and SES on disability pension by calculating interaction contrast (IC) using individuals with no VTE and high SES as the reference category. As previously described,19,20 the IC measures the difference in IR differences indicating the excess or deficit disability pension IR beyond or below the baseline IR among individuals with no VTE and high SES, the individual effect of SES on the disability pension IR and the effect of VTE on the disability pension IR (Figure 1). We calculated the attributable proportion of the disability pension IR that could be explained by interaction by dividing IC with the disability pension IR among individuals with VTE with low SES.
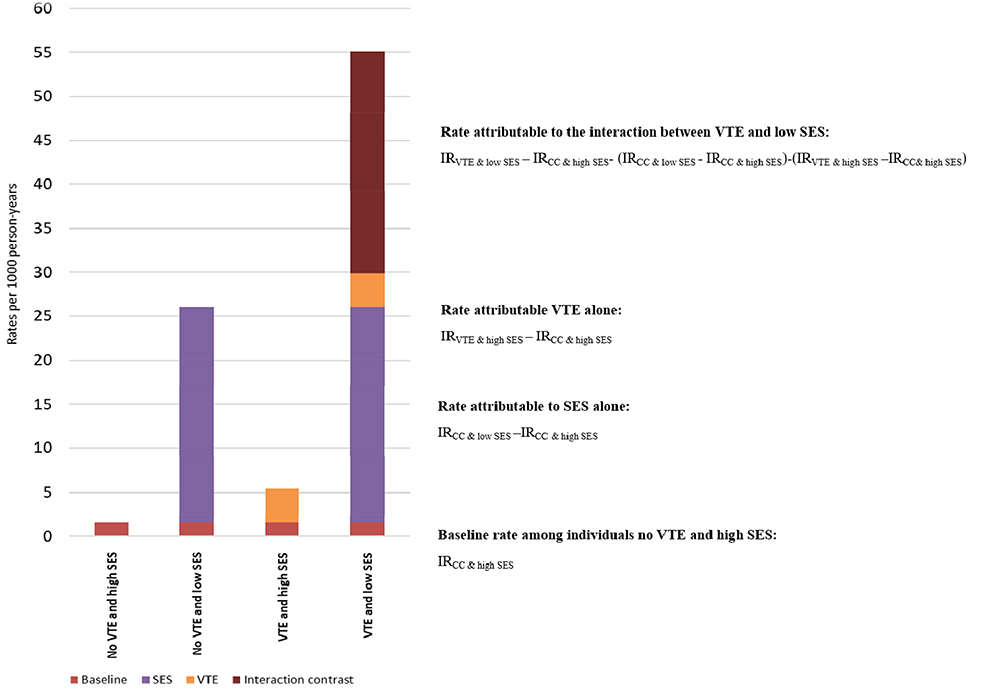 |
Figure 1 Proportion of the total disability pension incidence rate attributable to venous thromboembolism, low socioeconomic status, and their interaction. Abbreviations: SES, socioeconomic status; VTE, venous thromboembolism; IR, incidence rate. |
We used the Cox proportional hazards regression model to compute hazard ratios (HRs) as estimates of the combined effect conferred by VTE and SES using individuals with no VTE and high SES as the reference category. We tested the proportional hazards assumption using log-log plots and found no violation of this assumption. HRs were adjusted for a priori defined potential confounders by two different models. Model 1 was the unadjusted model controlling for matching factors by study design (age as a continuous variable, sex in the analyses not stratified by sex, and calendar year of VTE); Model 2 also included prior cancer, obesity, coronary heart disease (atrial fibrillation, myocardial infarction, and heart failure), mental diseases, diabetes, stroke, COPD, acute kidney failure and chronic kidney disease, and other diseases included in the Charlson Comorbidity Index, as well as surgery and trauma/fractures three months prior to the VTE/index date.
The analyses described above were conducted in the overall cohort and within strata of age (age groups 25–34 years, 35–44 years, 45–54 years, and 55–65 years on the date of inclusion) and sex.
To examine the significance of VTE subtypes and the underlying causes of VTE, we performed subgroup analyses with PE, DVT, unprovoked VTE, and provoked VTE as exposure variables. As comorbidities may be more prevalent in individuals with VTE than in the general population comparison cohort, we also performed analyses stratified by Charlson Comorbidity Index score of 0 and of ≥1.
To account for a potential overestimation of disability pension IRs due to competing risk of death, cumulative incidence functions were estimated by the methods proposed by Fine and Gray21 and visualized according to VTE/no VTE and level of SES score.
Statistical analyses were conducted using SAS version 9.4 (SAS Institute, Cary, NC).
Ethics Declaration and Accordance Statement
According to Danish legislation, studies based entirely on registry data do not require patient consent or approval from an ethics review board. The study was approved by the Danish Data Protection Agency, record number 2016-051-000001-811. All methods were performed in accordance with relevant guidelines and regulations.
Results
Characteristics
Baseline characteristics of the study participants (46.2% women) are presented in Table 1. We identified 41,781 individuals with VTE and 208,905 matched individuals from the general population. A subsequent disability pension was granted to 4203 (10.1%) individuals in the VTE cohort and 8637 (4.1%) individuals in the comparison cohort during a median follow-up of 4.4 years for the VTE cohort and 6.0 years for the comparison cohort (Table 2). The proportion of individuals with low SES was higher in the VTE cohort than in the comparison cohort (12% vs 8%), while the proportion of individuals with high SES was lower in the VTE cohort (21% vs 25%). There were 1215 (2.9%) individuals with missing SES in the VTE cohort and 5740 (2.7%) individuals with missing SES in the comparison cohort (Table 1). Individuals with VTE also had a higher prevalence of comorbidities such as surgery 3 months prior to the VTE date, history of cancer, mental disorders, and coronary heart disease, compared to the comparison cohort (Table 1). Baseline characteristics according to VTE and SES are shown in Supplementary Table 4.
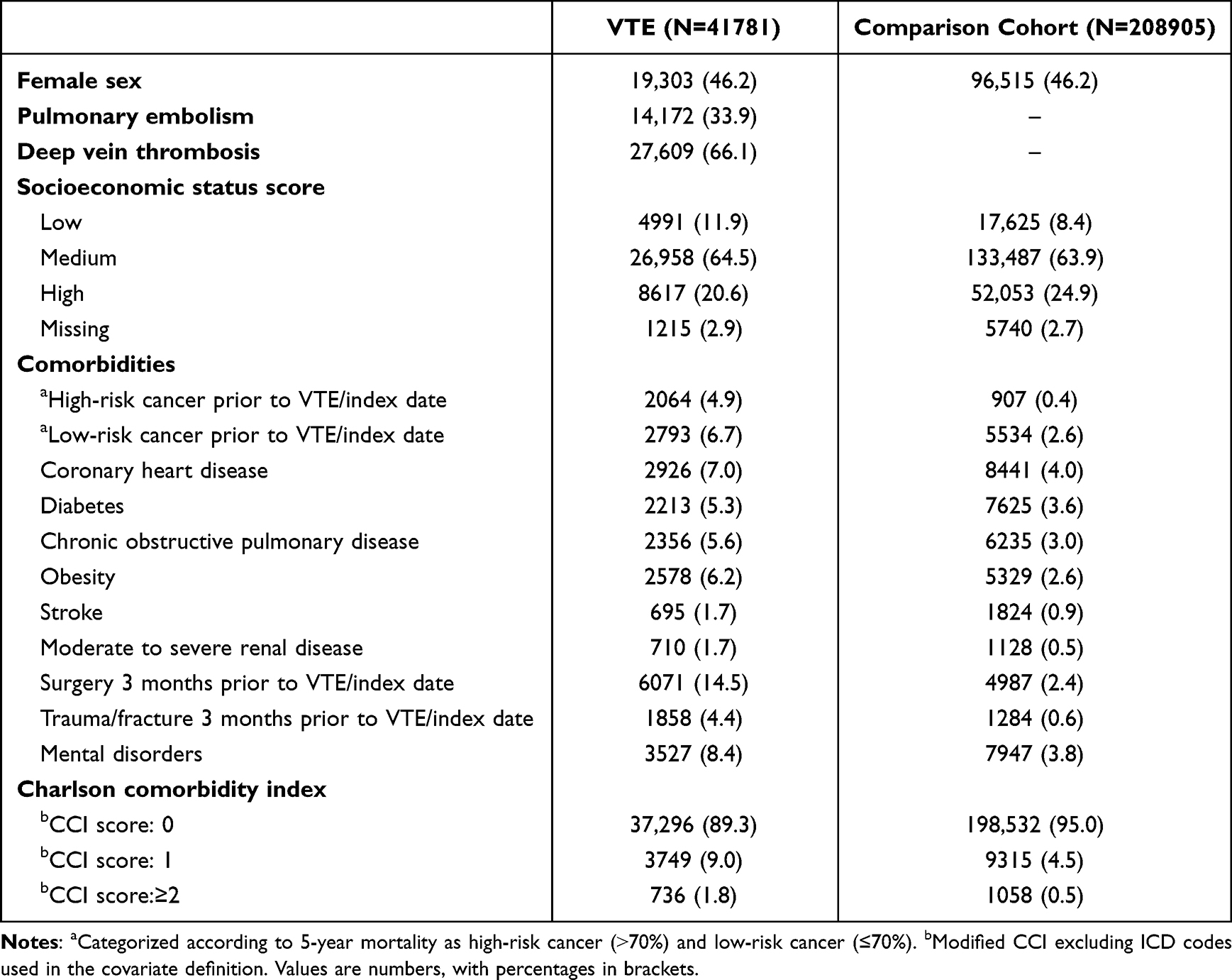 |
Table 1 Baseline Characteristics of Individuals with Venous Thromboembolism (VTE) and Members of the General Population Comparison Cohort |
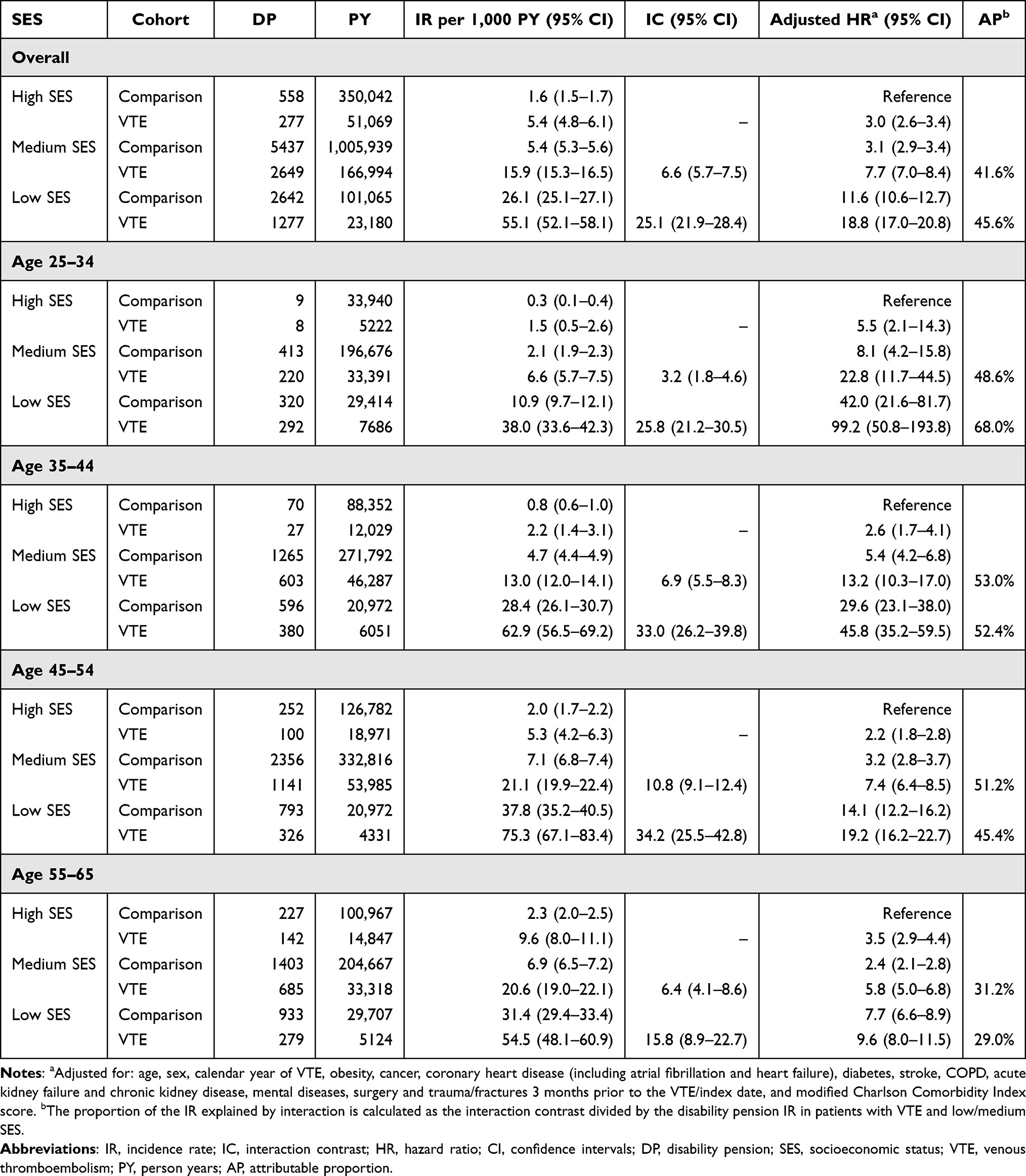 |
Table 2 Incidence Rates, Interaction Contrast, and Hazard Ratios with 95% Confidence Intervals of Work-Related Disability Pension According to Combined Categories of Socioeconomic Status Score and Venous Thromboembolism Status |
Interaction Between Venous Thromboembolism and Socioeconomic Status
The IR of disability pension per 1000 person-years among individuals with VTE and high SES was 5.4 (95% CI: 4.8–6.1) compared to 1.6 (95% CI: 1.5–1.7) in individuals with no VTE and high SES, compromising a IR difference of 3.8 (Table 2, Figure 1). The corresponding IR of disability pension in individuals with VTE and low SES was 55.1 (95% CI: 52.1–58.1) and 26.1 (95% CI: 25.1–27.1) in individuals with no VTE and low SES (IR difference of 24.0 (Table 2, Figure 1). In individuals with VTE and low SES an IC of 25.1 (95% CI: 21.9–28.4) corresponded to an attributable proportion of 45.6% of the total disability pension IR being explained by interaction between VTE and SES (Table 2). The disability pension IR in individuals with VTE and medium SES was 15.9 (95% CI: 15.3–16.5) and 5.4 (95% CI: 5.3–5.6) in individuals with no VTE and medium SES (IR difference of 10.5) (Table 2). For individuals with VTE and medium SES the attributable proportion of the disability pension IR explained by interaction was 41.6% [IC 6.6 (96% CI 5.7–7.5)] (Table 2).
The interaction was generally higher for DVT where the attributable proportion explained by interaction between DVT and low SES was 47.8% compared to 38.8% for PE and low SES (Table 3, Figure 2). In subcategories of provoked and unprovoked VTE, the attributable proportion explained by interaction between VTE and low SES was 37.8% for provoked VTE and 47.2% for unprovoked VTE (Table 3, Figure 2).
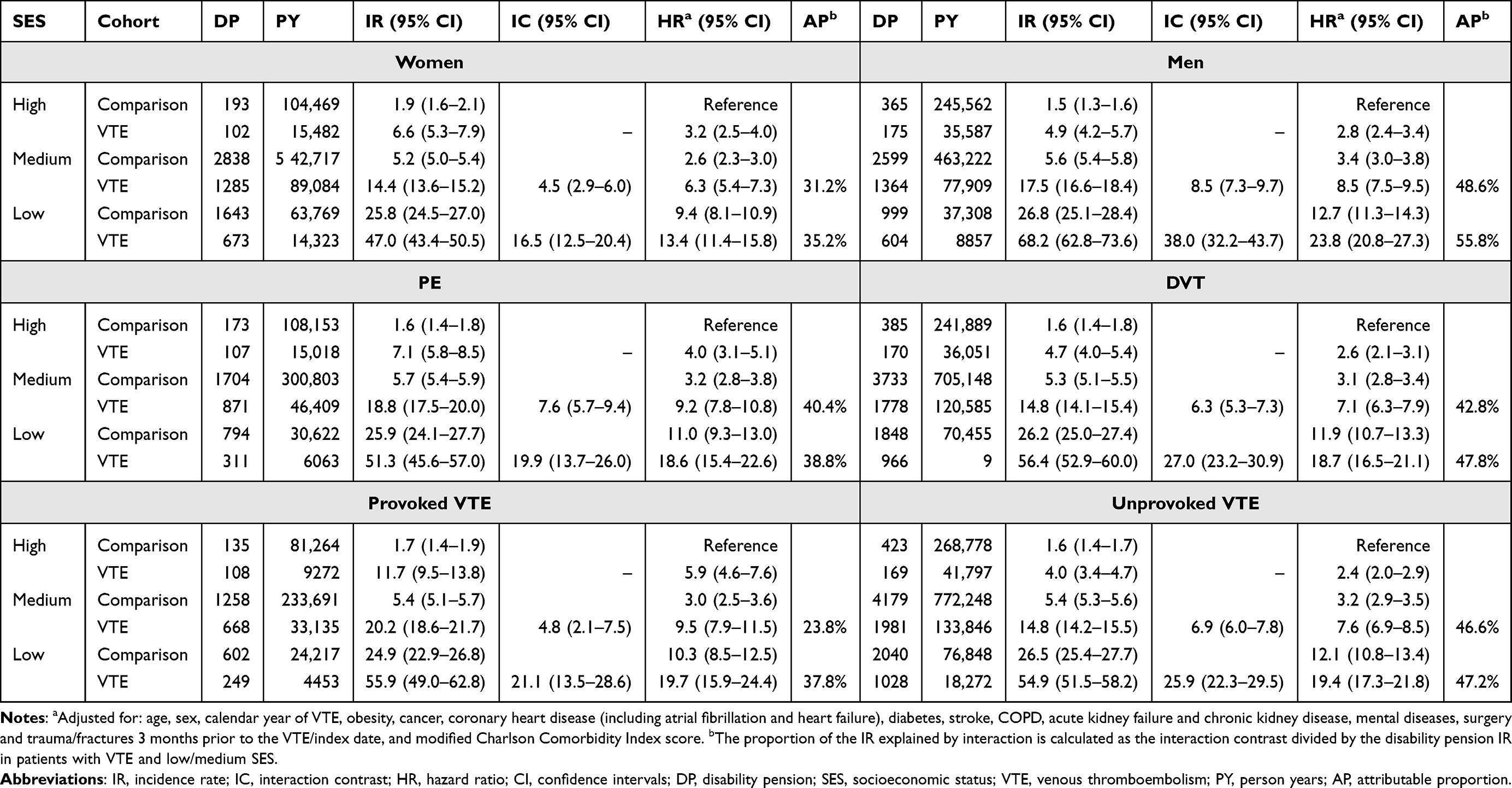 |
Table 3 Incidence Rates, Interaction Contrasts and Hazard Ratios with 95% Confidence Intervals of Work-Related Disability Pension According to Combined Categories of Socioeconomic Status Score and Venous Thromboembolism Status Stratified by Sex and Type of Venous Thromboembolism |
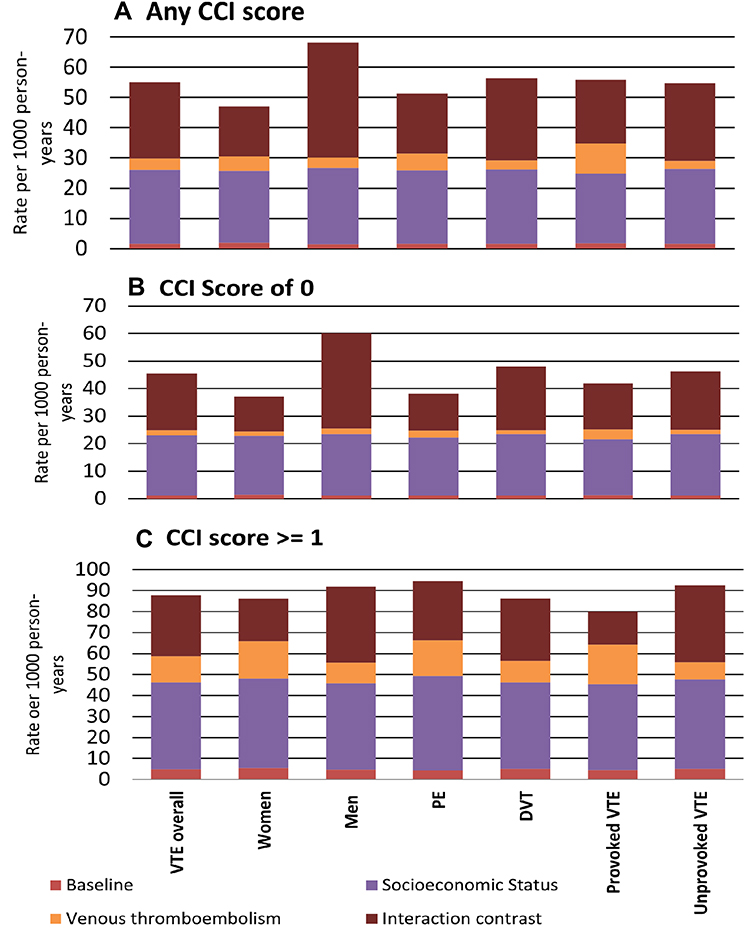 |
Figure 2 Proportion of the total disability pension rate attributable to venous thromboembolism, low socioeconomic status and their interaction in relation to men, women, pulmonary embolism, deep vein thrombosis, provoked and unprovoked venous thromboembolism in (A) main analysis, (B) analysis restricted to a Charlson Comorbidity Index score of zero, and (C) analysis restricted to a Charlson Comorbidity Index score of one or more. Abbreviations: SES, socioeconomic status; VTE, venous thromboembolism; PE, pulmonary embolism; DVT, deep vein thrombosis; CCI, Charlson comoribity index. |
The interaction was lowest in the highest age group of 55–65 years and was higher in men than in women (Tables 2 and 3, Figure 3). The attributable proportion of the disability pension IR explained by interaction between VTE and low SES was 68.0% [IC 25.8 (95% CI 21.2–30.5)] in the age group 25–34 years and 29.0% [IC 15.8 (95% CI 8.9–22.7)] in the age group 55–65 years (Table 2, Figure 3). For individuals with VTE and low SES, the attributable proportion of the disability pension IR explained by interaction was 55.8% of in men and 35.2% in women. (Table 3, Figure 3). This sex difference was particularly pronounced in the youngest and oldest age groups with interaction explaining 78.6% of the disability pension IR in men aged 25–34 and 46.6% of the disability pension IR in men aged 55–65, while the corresponding attributable proportions were 59.8% and 8.2% in women, respectively (Supplementary Table 5, Figure 3).
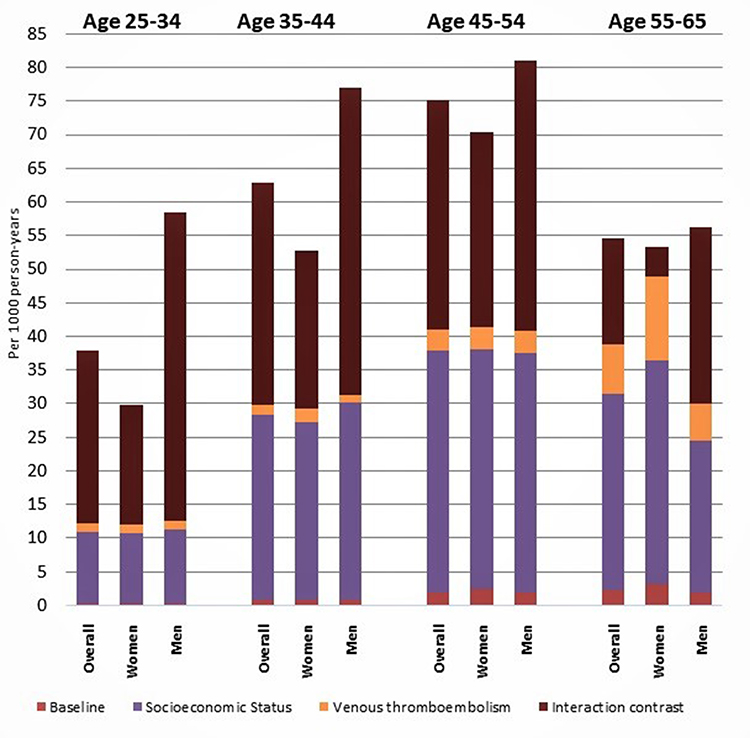 |
Figure 3 Proportion of the total disability pension incidence rate attributable to venous thromboembolism, low socioeconomic status, and their interaction by age and sex. |
In an analysis stratified on Charlson Comorbidity Index score, the interaction for those with a Charlson Comorbidity score of 0 remained essentially similar to that observed in the main analysis, while it was somewhat divergent for those with a Charlson Comorbidity score of ≥1. (Supplementary Table 6, Figure 2).
In individuals with VTE and low SES, the cumulative incidence of disability pension, after taking competing risk of death into account, was 18.7% (95% CI 17.6–19.9%) after three years, 25.6% (95% CI 24.2–26.9%) after six years, and 35.0% (95% CI 33.3–36.8%) after 12 years (Supplementary Figure 1). In the adjusted Cox proportional hazards regression model, VTE combined with low SES was associated with a HR of 18.8 (95% CI: 17.0–20.8) for disability pension, while VTE combined with medium SES yielded an adjusted HR of 7.7 (95% CI: 7.0–8.4) when compared with individuals with no VTE and high SES. (Table 2).
Discussion
In this nationwide population-based cohort study we found a large interaction on the additive scale between SES and VTE on the risk of disability pension. Even though the individual effects of lower SES and VTE increased the risk of disability pension, interaction accounted for 45.6% of the disability pension IR in individuals with low SES and VTE. The interaction between SES and VTE was present in both sexes, all age groups, and for all subtypes of VTE. Competing risk of death analyses and analyses within the strata of Charlson Comorbidity Index score suggested that VTE-related comorbidities or increased mortality in individuals with VTE might only explain a minor part of the observed interaction.
Our results confirmed those of previous reports on associations between SES and VTE,6–10 VTE and disability pension,4,5 and SES and disability pension.22–24 However, data on the interaction between VTE and socioeconomic gradient on the risk of disability pension have been lacking previously. A few studies have investigated the joint effect of occupational status and arterial cardiovascular disease on disability pension.24,25 A prospective cohort study of 44,516 survey respondents from the Finnish Public Sector found that the combination of low occupational status and cardiovascular disease were associated with a 4.5-fold increased risk of disability pension compared to high occupational class without cardiovascular disease. The combination of low occupational class and cardiovascular disease gave a Synergy Index of 1.55 suggesting a greater than additive effect.25 Another Finnish registry based study on 258,428 individuals of working age reported IRs per 1000 person-years of disability due to cardiovascular diseases of 3.3 in male manual workers aged 35–54 years and 2.4 in male manual workers aged 55–64 years.24 The reported incidence was somewhat lower for women.24
We found an interaction between low SES and incident VTE on the risk of disability pension. However, the observed interaction between VTE and SES was much stronger than the previously reported interaction with cardiovascular disease.24,25 Several factors may explain the large interaction observed in the current study. We measured SES by combining the SES indicators education, income and employment status in a composite SES score, and we measured SES close to the VTE. Our inclusion of multiple SES indicators is supported by several studies arguing that SES is innately multidimensional and therefore should be measured by more than one single indicator.26,27 The interaction between VTE and SES likely influences the risk of disability pension through several factors such as physical capacity, access to healthcare, legislation, lifestyle, labour market possibilities, work characteristics and psychosocial work environment.28,29 Therefore, a composite SES score enabled us to include a broader aspect of the socioeconomic dimension and capture both the different ways SES indicators influence each other and the temporal causation among the indicators. Moreover, by measuring SES close to the VTE, we lowered the chance of misclassifications and spurious associations that might dilute the findings. Low education and low income might imply reduced working possibilities and flexibility at work. Work-related stress, less control and decision latitude are factors that are known to generate both health problems and problems retaining employment.3,30 Furthermore, unfavorable working conditions through unfavorable psychosocial and physical work demands have been found to be more prevalent in individuals with low levels of education.30,31 Moreover, as individuals with VTE often suffer from reduced physical functioning due to recurrences, the post-thrombotic syndrome and the post PE-syndrome,32–34 typical industrial professions, or occupations with manual and tedious tasks, might be challenging to retain. In contrast, a high educational level and income might provide less physically stressful and more flexible life- and working conditions, making it easier to stay in employment despite reduced physical function.3,30
The interaction was especially pronounced in young men. Our findings are in line with previous data indicating that socioeconomic factors are strong determinants of disability among the young.10,22,35 Moreover, men have a higher risk of recurrence, post-thrombotic syndrome, and the post-PE syndrome32,33,36 and they are more prone to engage in behaviours leading to higher rates of injury and disease.37,38 These factors might contribute to the elevated risk of disability in male individuals with VTE.
Our study has several strengths. We used a large population-based cohort consisting of the entire general working-age Danish population, with highly accurate and validated data for exposures, outcome and comorbidities.12 Furthermore, we conducted the study in a setting with government-funded and free of charge education and health care services for all residents, thus reducing selection and referral bias. This allowed a detailed interpretation of the interaction between VTE and SES on the risk of disability pension, including the measurement of several SES indicators jointly and analysis stratified on age and sex.
The study also had some limitations. Disability can vary in duration and severity, and not necessarily lead to a permanent exit from work life. With receipt of permanent disability pension as the outcome, (and not including periods of sick leave etc.) we might have underestimated the actual incidence of disability pension related to VTE and SES. We also excluded individuals with missing SES values which might have somewhat biased our results.
Further, disability pension schemes vary between countries and time-periods. The transferability of our results to other countries may therefore be limited to countries with a similar generous tax-financed social benefit, - and health care system, such as in the Nordic region.
As the study was based on information available from medical and administrative registers, we lacked information relevant to receipt of a disability pension such as categories of occupation, life-style factors, like physical activity and body mass index, quality and outcome of post-VTE care, and workplace factors. Neither did we have information on the incidence of recurrence, the post-thrombotic syndrome, or the post-PE syndrome in our individuals with VTE during follow-up.
In conclusion, low SES interacts with VTE to increase the risk of disability pension beyond what could be explained by the additive effect of SES and VTE as separate components. Consequently, SES influences disability pension risk after VTE to a substantial proportion. Our results emphasise SES as a risk factor for disability pension in individuals with VTE and can help occupational and healthcare professionals to identify individuals at risk of an early exit from the workforce after a VTE.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Raskob GE, Angchaisuksiri P, Blanco AN, et al. Thrombosis: a major contributor to global disease burden. Arterioscler Thromb Vasc Biol. 2014;34(11):2363–2371. doi:10.1161/ATVBAHA.114.304488
2. White RH. The epidemiology of venous thromboembolism. Circulation. 2003;107(23 Suppl 1):I4–8. doi:10.1161/01.CIR.0000078468.11849.66
3. van Rijn RM, Robroek SJ, Brouwer S, Burdorf A. Influence of poor health on exit from paid employment: a systematic review. Occup Environ Med. 2014;71(4):295–301. doi:10.1080/09581596.2018.1469730
4. Braekkan SK, Grosse SD, Okoroh EM, et al. Venous thromboembolism and subsequent permanent work-related disability. J Thromb Haemost. 2016;14(10):1978–1987. doi:10.1111/jth.13411
5. Jørgensen H, Horváth-Puhó E, Laugesen K, Brækkan S, Hansen JB, Sørensen HT. Risk of a permanent work-related disability pension after incident venous thromboembolism in Denmark: a population-based cohort study. PLoS Med. 2021;18(8):e1003770. doi:10.1371/journal.pmed.1003770
6. Zoller B, Li X, Sundquist J, Sundquist K. Socioeconomic and occupational risk factors for venous thromboembolism in Sweden: a nationwide epidemiological study. Thromb Res. 2012;129(5):577–582. doi:10.1016/j.thromres.2011.07.050
7. Isma N, Merlo J, Ohlsson H, Svensson PJ, Lindblad B, Gottsater A. Socioeconomic factors and concomitant diseases are related to the risk for venous thromboembolism during long time follow-up. J Thromb Thrombolysis. 2013;36(1):58–64. doi:10.1007/s11239-012-0858-8
8. Rosengren A, Freden M, Hansson PO, Wilhelmsen L, Wedel H, Eriksson H. Psychosocial factors and venous thromboembolism: a long-term follow-up study of Swedish men. J Thromb Haemost. 2008;6(4):558–564. doi:10.1111/j.1538-7836.2007.02857.x
9. Holst AG, Jensen G, Prescott E. Risk factors for venous thromboembolism: results from the Copenhagen City Heart Study. Circulation. 2010;121(17):1896–1903. doi:10.1161/CIRCULATIONAHA.109.921460
10. Jørgensen H, Horváth-Puhó E, Laugesen K, Brækkan S, Hansen J-B, Sørensen HT. Socioeconomic status and risk of incident venous thromboembolism. J Thromb Haemost. 2021;19(12):3051–3061. doi:10.1111/jth.15523
11. Schmidt M, Schmidt SAJ, Adelborg K, et al. The Danish health care system and epidemiological research: from health care contacts to database records. Clin Epidemiol. 2019;11:563–591. doi:10.2147/CLEP.S179083
12. Sundbøll J, Adelborg K, Munch T, et al. Positive predictive value of cardiovascular diagnoses in the Danish National Patient Registry: a validation study. BMJ Open. 2016;6(11):e012832. doi:10.1136/bmjopen-2016-012832
13. Adelborg K, Corraini P, Darvalics B, et al. Risk of thromboembolic and bleeding outcomes following hematological cancers: a Danish population-based cohort study. J Thromb Haemost. 2019;17(8):1305–1318. doi:10.1111/jth.14475
14. Sogaard KK, Schmidt M, Pedersen L, Horvath-Puho E, Sorensen HT. 30-year mortality after venous thromboembolism: a population-based cohort study. Circulation. 2014;130(10):829–836. doi:10.1161/CIRCULATIONAHA.114.009107
15. Kearon C, Ageno W, Cannegieter SC, Cosmi B, Geersing GJ, Kyrle PA. Categorization of patients as having provoked or unprovoked venous thromboembolism: guidance from the SSC of ISTH. J Thromb Haemost. 2016;14(7):1480–1483. doi:10.1111/jth.13336
16. Heide-Jorgensen U, Adelborg K, Kahlert J, Sorensen HT, Pedersen L. Sampling strategies for selecting general population comparison cohorts. Clin Epidemiol. 2018;10:1325–1337. doi:10.2147/CLEP.S164456
17. Directorate-General for Employment SAaI, The European Comission. Your social security rights in Denmark; 2019.
18. Thygesen SK, Christiansen CF, Christensen S, Lash TL, Sørensen HT. The predictive value of ICD-10 diagnostic coding used to assess Charlson comorbidity index conditions in the population-based Danish National Registry of Patients. BMC Med Res Methodol. 2011;11(1):83. doi:10.1186/1471-2288-11-83
19. Schmidt M, Horváth-Puhó E, Ording AG, Bøtker HE, Lash TL, Sørensen HT. The interaction effect of cardiac and non-cardiac comorbidity on myocardial infarction mortality: a nationwide cohort study. Int J Cardiol. 2020;308:1–8. doi:10.1016/j.ijcard.2020.01.059
20. Bonnesen K, Schmidt M, Horváth-Puhó E, Sørensen HT. The interaction effect between comorbidity burden and venous thromboembolism on mortality: a nationwide cohort study. Thromb Haemost. 2021. doi:10.1055/a-1527-6215
21. Fine JP, Gray RJ. A proportional hazards model for the subdistribution of a competing risk. J Am Stat Assoc. 1999;94(446):496–509. doi:10.1080/01621459.1999.10474144
22. Krokstad S, Johnsen R, Westin S. Social determinants of disability pension: a 10-year follow-up of 62 000 people in a Norwegian county population. Int J Epidemiol. 2002;31(6):1183–1191. doi:10.1093/ije/31.6.1183
23. Brun C, Boggild H, Eshoj P. [Socioeconomic risk indicators for disability pension within the Danish workforce. A registry-based cohort study of the period 1994–1998]. Ugeskr Laeger. 2003;165(35):3315–3319. Danish.
24. Polvinen A, Laaksonen M, Gould R, Lahelma E, Martikainen P. The contribution of major diagnostic causes to socioeconomic differences in disability retirement. Scand J Work Environ Health. 2014;40(4):353–360. doi:10.5271/sjweh.3411
25. Virtanen M, Lallukka T, Ervasti J, et al. The joint contribution of cardiovascular disease and socioeconomic status to disability retirement: a register linkage study. Int J Cardiol. 2017;230:222–227. doi:10.1016/j.ijcard.2016.12.166
26. Geyer S, Hemström Ö, Peter R, Vågerö D. Education, income, and occupational class cannot be used interchangeably in social epidemiology. Empirical evidence against a common practice. J Epidemiol Community Health. 2006;60(9):804–810. doi:10.1136/jech.2005.041319
27. Galobardes B, Lynch J, Smith GD. Measuring socioeconomic position in health research. Br Med Bull. 2007;81–82(1):21–37. doi:10.1093/bmb/ldm001
28. Leka S, Jain A, World Health O. Health Impact of Psychosocial Hazards at Work: An Overview. Geneva: World Health Organization; 2010.
29. Levesque JF, Harris MF, Russell G. Patient-centred access to health care: conceptualising access at the interface of health systems and populations. Int J Equity Health. 2013;12(1):18. doi:10.1186/1475-9276-12-18
30. Bruusgaard D, Smeby L, Claussen B. Education and disability pension: a stronger association than previously found. Scand J Public Health. 2010;38(7):686–690. doi:10.1177/1403494810378916
31. Robroek SJ, Rongen A, Arts CH, Otten FW, Burdorf A, Schuring M. Educational Inequalities in Exit from paid employment among Dutch workers: the influence of health, lifestyle and work. PLoS One. 2015;10(8):e0134867. doi:10.1371/journal.pone.0134867
32. Stain M, Schönauer V, Minar E, et al. The post-thrombotic syndrome: risk factors and impact on the course of thrombotic disease. J Thromb Haemost. 2005;3(12):2671–2676. doi:10.1111/j.1538-7836.2005.01648.x
33. Kyrle PA, Minar E, Bialonczyk C, Hirschl M, Weltermann A, Eichinger S. The risk of recurrent venous thromboembolism in men and women. N Engl J Med. 2004;350(25):2558–2563. doi:10.1056/NEJMoa032959
34. Kahn SR, Hirsch A, Shrier I. Effect of postthrombotic syndrome on health-related quality of life after deep venous thrombosis. Arch Intern Med. 2002;162(10):1144–1148. doi:10.1001/archinte.162.10.1144
35. Haukenes I, Löve J, Hensing G, et al. Inequity in disability pension: an intersectional analysis of the co-constitution of gender, education and age. The Hordaland Health Study. Crit Public Health. 2019;29(3):302–313.
36. McRae S, Tran H, Schulman S, Ginsberg J, Kearon C. Effect of patient’s sex on risk of recurrent venous thromboembolism: a meta-analysis. Lancet. 2006;368(9533):371–378. doi:10.1016/S0140-6736(06)69110-1
37. Hoffmann R, Kröger H, Tarkiainen L, Martikainen P. Dimensions of Social Stratification and their relation to mortality: a comparison across gender and life course periods in Finland. Soc Indic Res. 2019;145(1):349–365. doi:10.1007/s11205-019-02078-z
38. McDonough P, Williams DR, House JS, Duncan GJ. Gender and the socioeconomic gradient in mortality. J Health Soc Behav. 1999;40(1):17–31. doi:10.2307/2676376
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Socioeconomic Status Related to Prescription of Triple Therapy and Anticholinergic Monotherapy in Patients with Chronic Obstructive Pulmonary Disease (COPD) in Sweden - A Retrospective National Registry Study
Larsson K, Betnér S, Fuchs B, Vanfleteren LEGW, Stridsman C
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:3597-3606
Published Date: 7 November 2025
Prevalence of and Factors Associated with Cognitive Impairment Among Adults in Central Sudan: A Community-Based Cross-Sectional Study
Omar SM, Alwabili AA, Alotaibi EA, Adam I
International Journal of General Medicine 2026, 19:573913
Published Date: 6 January 2026