Back to Journals » Risk Management and Healthcare Policy » Volume 16
Cardiovascular Disease in China: Socioeconomic Status Variation in Prevalence
Authors Zhang C, Shen Y, Wang A, Wang D, Cao L, Yue W ![]()
Received 28 July 2023
Accepted for publication 3 October 2023
Published 9 October 2023 Volume 2023:16 Pages 2077—2084
DOI https://doi.org/10.2147/RMHP.S429224
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Chao Zhang,1 Ying Shen,2 Anxin Wang,3 Da Wang,4 Lei Cao,5 Wei Yue1,4
1Department of Neurology, Tianjin Key Laboratory of Cerebral Vascular and Neurodegenerative Diseases, Tianjin Huanhu Hospital, Clinical College of Neurology, Neurosurgery, and Neurorehabilitation, Tianjin Medical University, Tianjin University, Tianjin, People’s Republic of China; 2Department of Traditional Chinese Medicine, Beijing Xuanwu Hospital, Capital Medical University, Beijing, People’s Republic of China; 3Department of Epidemiology, National Clinical Research Center for Neurological Diseases, Beijing TianTan Hospital, Capital Medical University, Beijing, People’s Republic of China; 4Department of Medical Administration, Tianjin Key Laboratory of Cerebral Vascular and Neurodegenerative Diseases, Tianjin Huanhu Hospital, Tianjin, People’s Republic of China; 5Department of Neurology, Nation Project Office of Stroke Prevention and Control, Beijing, People’s Republic of China
Correspondence: Wei Yue, Department of Neurology, Tianjin Huanhu Hospital, 6 Jizhao Road, Tianjin, 300350, People’s Republic of China, Tel +8613752686958, Fax +86 022 59065662, Email [email protected]
Introduction: Cardiovascular disease is the single largest contributor to global mortality and the leading cause of both death and premature death in China. Data on the association between cardiovascular disease and socioeconomic status are sparse, especially for Asian countries. Our study collected data to describe the socioeconomic status variation across cardiovascular disease using a large nationwide cross-sectional study.
Methods: We chose participants using the cluster sampling method, prepared a face-to-face questionnaire interview for the selected community residents, and collected information on health conditions, socioeconomic status, demographics, and comorbidities. All collected data were reported as frequencies and corresponding percentages. Linear regression and simple and multivariable logistic regression were performed to identify the prevalence variation. All statistical analyses were performed using SPSS version 26 software.
Results: Socioeconomic information was available for 394,688 participants (covering most provincial districts). The prevalence of cardiovascular disease was 7.9%. The prevalence was higher in rural areas than that in urban areas (rural, 8.4%; urban, 7.5%). There was a negative relationship between urbanization and cardiovascular disease prevalence. Furthermore, cardiovascular disease prevalence had a negative relationship with average earnings.
Conclusion: This cross-sectional analysis of socioeconomic status variation in the prevalence of cardiovascular disease in China showed a significant negative relationship between regional and individual socioeconomic status and cardiovascular disease. The results imply that governments would benefit communities by focusing on effective and targeted interventions for prevention, screening, and treatment in individuals who may be in the socioeconomic status with a high risk for cardiovascular disease.
Plain Language Summary: Benefits from the inclusion of many provinces, and large sample size, this study provided important new viewpoints on the prevalence of CVD. We described the current CVD status in China and the socioeconomic status variation on cardiovascular disease in the prevalence. In our study, significant differences were observed in iSES and CVD. And we identified the rSES in CVD prevalence disparities among provincial districts based on large administrative data sets. These results are essential for the government to put the target prevention programs and effective public health to those in status with a high risk to reduce prevalence. Besides, the English language in our manuscript had been proofread and revised by professional editing service in Editage.
Keywords: cardiovascular disease, prevalence, socioeconomic status, urbanization, income
Introduction
Along with the aging social population, cardiovascular disease (CVD), a type of chronic disease, has been the largest single contributor to global mortality and the leading cause of both death and premature death (accounting for more than 40%) in China.1–4 Although the World Health Organization (WHO) provides a simple protocol for the assessment and management of CVD, the prevalence is still growing, and inequalities continue to persist over space and time.5 Previous studies have shown differences in socioeconomic status (SES) risk factors.6,7 Therefore, it is important to assess regional and individual SES variations when studying disparities in the prevalence of CVD. However, research on this topic is sparse, especially for Asian countries.8,9 We sought to describe the socioeconomic variation across CVD by investigating data using a large nationwide cross-sectional study. Results could provide evidence as a basis for developing suitable interventions.
Methods
Study Design and Population
This community-based cross-sectional study was conducted in 2016 and was based on the China National Stroke Screening and Prevention Project (CNSSPP) launched by the Chinese Ministry of Health, which covered most provincial districts (30 out of 32). And this project is a nationwide program which is a cardiovascular disease surveillance program conducted annually, instituted by the Chinese government from 2011. The data were extracted from “the Big Database Platform for Cerebrovascular Disease” of the Chinese Stroke Center, and we obtained the use consent of the data. We scheduled a face-to-face questionnaire interview with community residents to identify SES variation in the prevalence of CVD. The participants were selected using the cluster sampling method. Based on the community, random sampling was selected proportionally across the local population size; this strategy was used in every primary sampling unit. All residents aged 40 years or older (born before December 31, 1976) who were long-time residents in the selected community (for longer than 6 months) were invited to participate in this study. Participants completed the questionnaire administered by the professional researchers of this project in nearby community hospitals or health stations. Further details of the sampling study design and methods of CCSP have been reported previously.10
Definition of Confounders and Intermediary Variables
Trained workers administered the questionnaire on health conditions, SES, lifestyle, and comorbidities. The explanatory variables were regional SES (rSES, according to living conditions [urban or rural] and provincial urbanization) and individual SES (iSES, according to the annual average income per year). Urbanization was calculated in provincial administrative units (participants from 22 provinces [excluding Taiwan province], four municipalities, four autonomous regions [excluding the Xizang autonomous region], and 30 provincial administrative units). This calculation refers to the percentage of participants living in urban areas.11 Concerned information was collected and categorized as follows: age (three groups); marital status (married or others); body mass index (BMI) (three groups distributed by Asian standards, normal: <23.0, overweight: 23.0–24.9, obesity: ≥25.0); smoking status (yes, passive, or no); drinking status (yes or no); regular physical activity (yes or no); hypertension and diabetes (yes or no). The endpoints were CVD prevalence, confirmed stroke (ischemic stroke, hemorrhagic stroke, subarachnoid hemorrhage, transient cerebral ischemia [TIA]), and heart diseases (defined as a series of nonfatal cardiac vascular diseases such as nonfatal myocardial infarction, angiographically defined coronary heart disease, coronary artery bypass grafting, percutaneous transluminal coronary angioplasty, angina, atrial fibrillation, or valvular heart disease). These diseases were defined by the disease diagnosis guidelines and judged by professional clinical doctors. Diagnoses were confirmed based on the individual providing their medical history and diagnoses and the evidentiary materials (medical records and auxiliary inspection reports).
Statistical Analysis
All collected data were analyzed as categorical variables and reported as frequencies and corresponding percentages using contingency tables and chi-square tests (X2 statistics). Differences in categorical variables between participants with and without CVD were examined using the X2 test. A linear association was used to examine the rSES variation. To identify the prevalence variation from rSES and iSES, the simple and multivariable logistic regression models were fitted in two different models: (i) a model that included only one characteristic, SES (urban or rural and iSES), and (ii) a model that included all confounders and intermediary characteristics (including basic information: sex, age, marital status, BMI, smoking, drinking, and physical activity; and comorbidities: hypertension and diabetes), to evaluate their contribution to CVD. All statistical analyses were performed using SPSS version 26, and statistical significance was set at P < 0.05.
Results
We obtained 423,603 individuals over 40 years of age from community general practices as previously mentioned. Participants with missing information with the status of CVD (28,484 [6.7%]) and average earnings of $431 (4.7%) were excluded from this analysis. Following these exclusions, 394,688 participants were included for analysis of the SES variation in CVD prevalence. The population distribution was similar to that of the seventh national census in China (Figure 1). The details of the seventh national census are available via open access from the website, http://www.stats.gov.cn/. Participation in population size and area breadth promised to maximize socioeconomic diversity. Among the 394,688 individuals enrolled in the CCSP Study, 206,666 (52.4%) lived in urban areas. Average earnings were 30.2% of individuals with ≤ $721, 17.5% with $721-1443, 15.3% with $1443–2885, and 37.1% with ≥ $2885. A total of 99,118 (25.1%) participants had hypertension and 29,592 (7.5%) had diabetes. The demographic characteristics are shown in Table 1. The details of the distribution of community residents in the 30 provincial districts and missing data for different variables are shown in Supplementary Figure 1 and Supplementary Table 1.
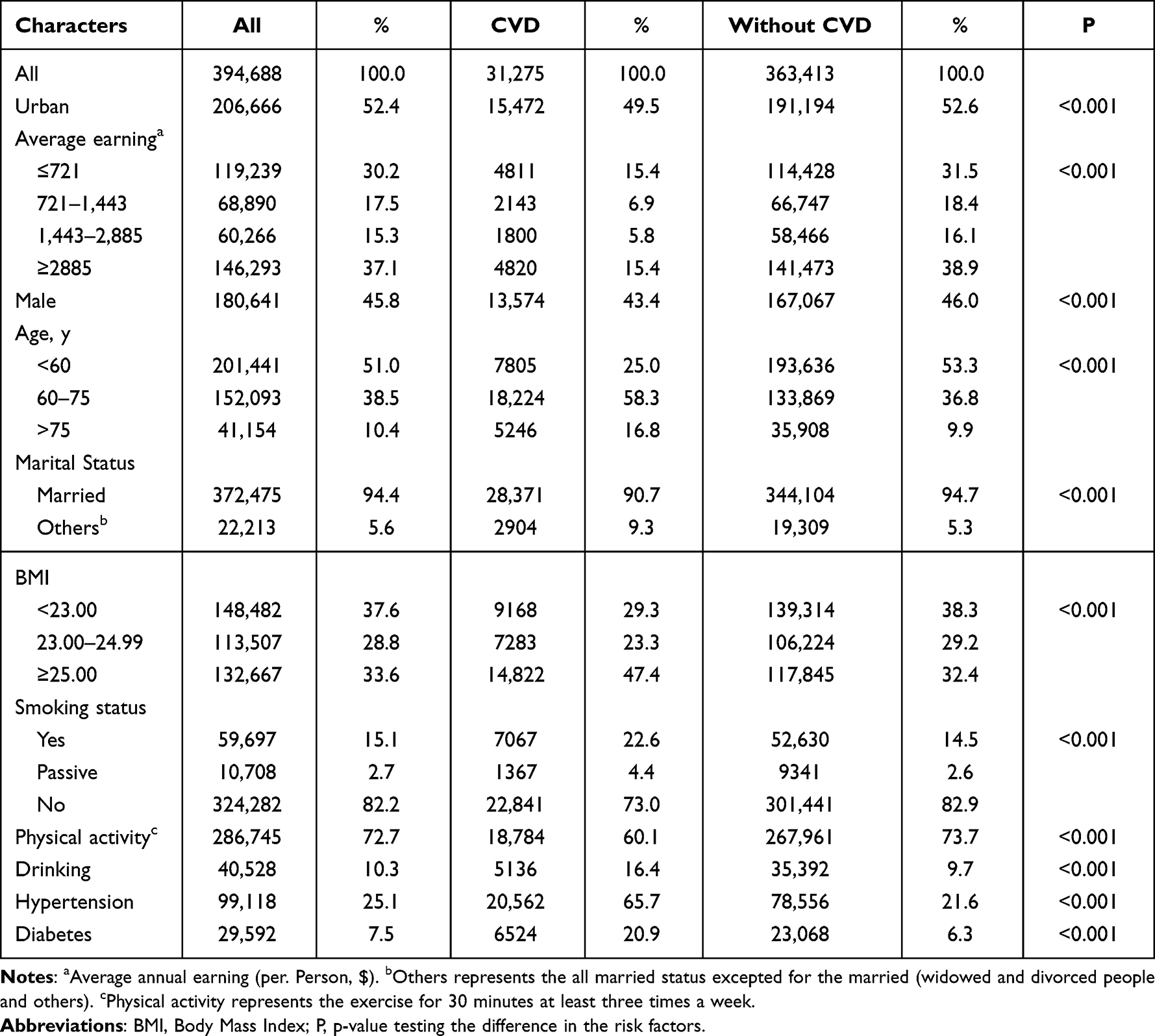 |
Table 1 The Characteristics of the Study Population and the Group with Cardiovascular Disease |
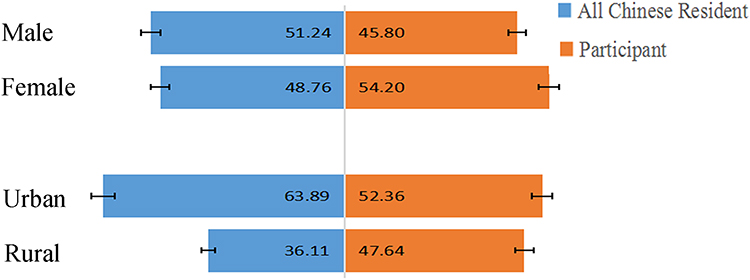 |
Figure 1 China’s population distribution on the basis of regions. |
The prevalence of CVD in the participants was 7.9% (ranging from 2.9% to 13.6% in different provincial districts); individuals with CVD were predominantly older (>75y), and overweight (Table 1). The prevalence of the CVD varied among different provincial administrative units (Supplementary Table 2) and was higher in rural areas than that in urban areas (urban, 7.5%; rural, 8.4%). There was no significant linear correlation between rSES and urbanization (P=0.353, R2 =0.030, 95% confidence interval [CI]: −0.074–0.027); however, there was a negative relationship. Simple logistic regression analysis revealed a lower CVD prevalence (odds ratio [OR], 0.882; 95% CI, 0.853–0.911) of residents in urban regions than that in rural regions (Figure 2 and Table 2).
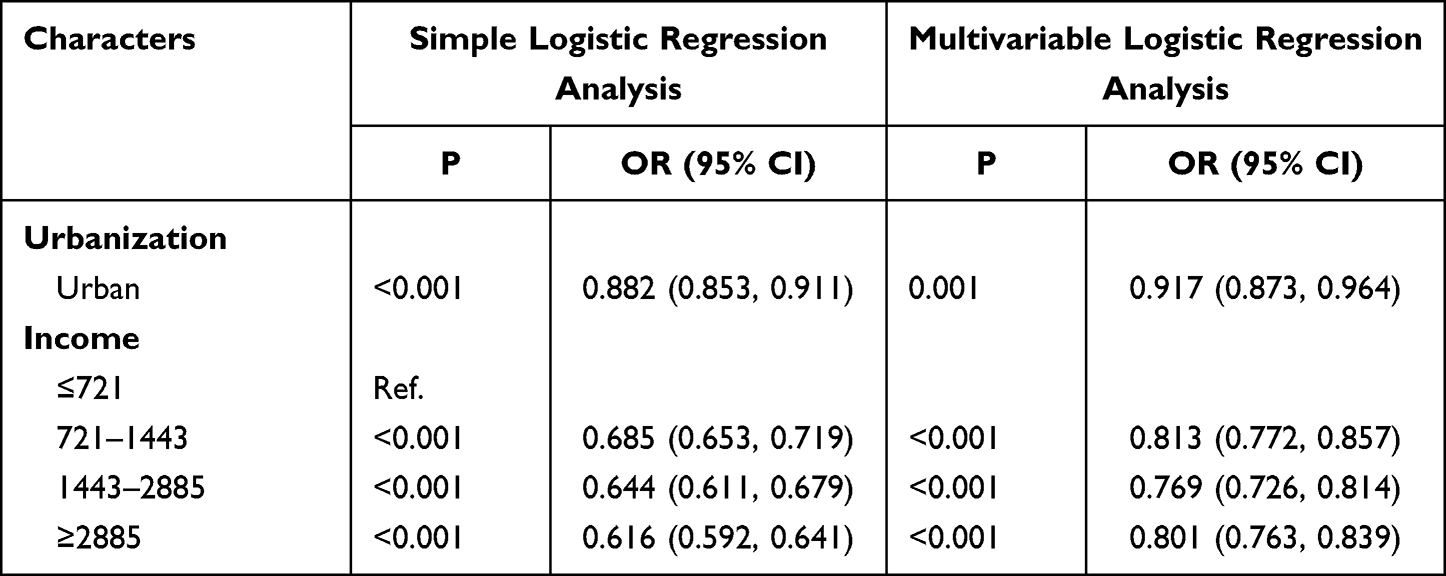 |
Table 2 The Simple and Multivariable Logistic Regression Analysis of the Socioeconomic Variation |
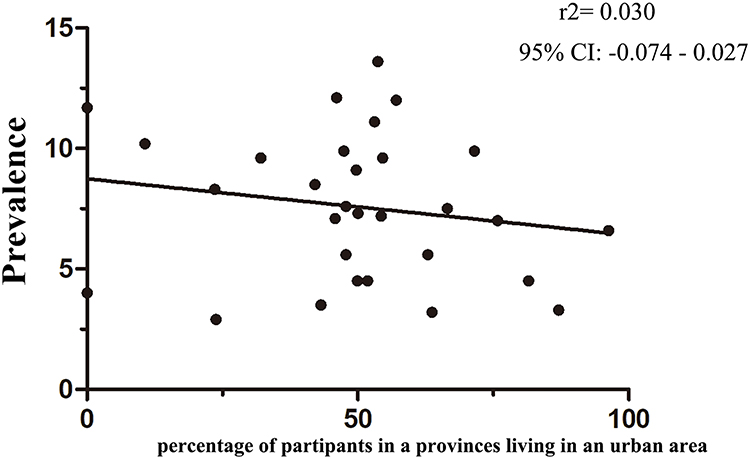 |
Figure 2 Association between cardiovascular disease and urbanization. (Urbanization refers to the district-level percentage of adults in our sample who were living in an urban area. The grey line was fitted using linear regression with each data point in the plot having the same weight). |
In terms of iSES, the prevalence of higher-income groups was significantly lower than that of low-income groups (9.9% vs 7.0% vs 6.6% vs 5.5%, Table 1). The same result of simple and multivariable logistic regression analyses showed that higher income was associated with a lower CVD prevalence, indicating that the prevalence of CVD had a negative relationship with average earnings (OR, 0.801; 95% CI, 0.763–0.839; Table 2).
Discussion
This study expanded the association between SES and CVD in China. China, a middle-income country with enormous socioeconomic and cultural diversity, is the most populous country (>1.36 billion in 2014) and has the second largest economy in the world.7 To clarify the role of regional and individual SES, more specifically socioeconomic degree or urbanization and income, on individual-level health outcomes, we collected and analyzed data on the prevalence of CVD in 394,688 adults across China. The main strengths of our study are the inclusion of many provinces, a standardized and systematic approach to data collection with the same enforcement regulation, and the use of personal income and living environment as markers of SES. We found significant differences between iSES and CVD and identified rSES variation in CVD prevalence among provincial districts based on large administrative datasets.
Socioeconomic variation in CVD has been confirmed in previous studies.12–14 The Coronary Artery Risk Development in Young Adults Study in America proved that volatility and decreases of income during a 15-year period of formative earning years were independently associated with a nearly two-fold risk of CVD and all-cause mortality.15 A 2017 meta-analysis concluded that low/medium income increased the risk of CVD worldwide.8 A previous Chinese study indicated an inverse trend between the prevalence of total CVD and socioeconomic distribution.16 That study was grouped by provinces, and the socioeconomic variation was defined by national criteria of provinces, including the high-, middle-, and low-income regions.
The present study aimed to derive individual-level health outcomes and extend this work to include regional and individual SES for CVD risk.17,18 We found a negative association between iSES and the prevalence of CVD in China. Same with our result, the study in Russia stressed that financial constraints are the key factors defining cardiovascular health behaviors.19 Various factors can explain this association. First, individuals with lower-income may more easily be involved in behavioral and lifestyle risk factors, such as poor diet (lower fruit and vegetable consumption), smoking, alcohol consumption, and restricted physical activity, all of which increase the risk of CVD.20–22 In addition, living in lower-income-stressful environments is associated with individual-level health, and previous studies have emphasized the psychophysiological pathway linking income inequality and health.23,24 Individuals with higher incomes may have certain coping strategies for stress (ie, greater material resources, attention, and information processing ability), which could increase their mental and physical resilience to external stressors.25,26 Those with higher incomes may pay more attention to the control and treatment of basic diseases (hypertension, diabetes, etc.), have an earlier recognition and response to warning symptoms, and seek or have greater access to more health services (ie, experienced physicians, evidence-based treatment, and adherence to medication).20,27,28 Individuals with lower incomes may not be able to afford necessary health care or periodic physical examinations, particularly in rural areas without universal health insurance coverage.
Although we found no significant linear regression between socioeconomic degree or urbanization and CVD, the negative correlation was absolute. Similarly, previous meta-analyses and studies indicated that a higher neighborhood disadvantage was associated with a higher CVD risk.17,29–31 There are several potential explanations for this finding. Patient care, such as that provided through The China Stroke Emergence Green Channel or China Chest Pain Center, is patchy and fragmented in lower-rSES provinces.31 The strategic allocation of financial resources for healthcare, according to disease priorities in each province, is different, which may lead to insufficient financial support for CVD in provinces with lower rSES.32 Furthermore, previous research has demonstrated that populations of rural and lower rSES face social or geographic ‘barriers’ that are likely to contribute to a higher CVD prevalence, such as shortages of healthcare professionals, lack of comprehensive understanding of health-related information, limited access and later presentation, transportation difficulties, and geographic distance.21,33 Therefore, we found that living in more impoverished rSES neighborhoods had an adverse effect on individual-level health. These results are useful for both epidemiological research and healthcare service planning and emphasize the need to improve primary and secondary prevention and to prioritize resources for residents with the greatest risk of major adverse end points. Long-time prospective studies are needed to further clarify and consolidate the association of socioeconomic status variation and CVD in China.
However, this study had limitations which could impact the application of the results. This study was retrospective, and the endpoint was self-provided. Inaccurate recording or reporting may have affected the estimates, which is a source of potential bias. And it still needs further validation with larger studies and long-time prospective studies to clarified and consolidated the association of SES and CVD in China. Although the study was based on random samples of the population, the sampling was at the provincial district level, and this project was implemented separately by the personnel in charge of each province. We devoted much effort to communicating enforcement regulations to ensure balance among the personnel, and the result was matched with the seventh nationwide population census; however, there may still be errors. Moreover, information on occupational categorization and education was not available to estimate these interaction factors.17 Hence, these errors should not bias conclusions regarding the negative relationship between the prevalence of CVD and SES.
Even considering the aforementioned limitations, our study benefited from the inclusion of many provinces, a systematic approach to data collection, and a large sample size. The results provide important new viewpoints on the prevalence of CVD. We concluded that the observed differences in the prevalence among individual or regional SES characteristics are alarming. Although our government has proposed a series of policies to respond to the huge burden of CVD and the differentiation of access to health care (such as The New Rural Cooperative Medical Scheme or the National Essential Drugs List), the prevention and treatment of CVD remain challenging for the Chinese and Chinese governments.34 This calls for different SES specific effective prevention programs. Governments should develop target public health policies and improve the strategic allocation of resources to meet the health care needs in different provinces and reduce CVD prevalence and disease burden.
Ethical Approval and Consent to Participate
Our study is a face-to-face questionnaire interview with the community. This research involving human participants, and the ethics approval have been performed in accordance with the Declaration of Helsinki and approved by The Rocket Force Special Medical Center Ethics Committee. The verbal informed consent was obtained from all participants when we called and invited people to the screening program. And the written one was got when we conducted the questionnaire.
Acknowledgments
We all appreciated the IT Professional Xiaoyan Wang and Junfeng Niu for our data processing. Furthermore, we would like thanks to all participants of CCSP.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Funded by Tianjin Key Medical Discipline (Specialty) Construction Project (No. TJYXZDXK-052B).
Disclosure
All authors declare that they have no conflicts of interest for this work.
References
1. Kreatsoulas C, Anand SS. The impact of social determinants on cardiovascular disease. Can J Cardiol. 2010;26(Suppl C):8c–13c. doi:10.1016/S0828-282X(10)71075-8
2. Yang G, Wang Y, Zeng Y, et al. Rapid health transition in China, 1990–2010: findings from the global burden of disease study 2010. Lancet. 2013;381(9882):1987–2015. doi:10.1016/S0140-6736(13)61097-1
3. Sacco RL, Roth GA, Reddy KS, et al. The heart of 25 by 25: achieving the goal of reducing global and regional premature deaths from cardiovascular diseases and stroke: a modeling study from the American heart association and world heart federation. Glob Heart. 2016;11(2):251–264. doi:10.1016/j.gheart.2016.04.002
4. Zhou M, Wang H, Zhu J, et al. Cause-specific mortality for 240 causes in China during 1990–2013: a systematic subnational analysis for the global burden of disease study 2013. Lancet. 2016;387(10015):251–272. doi:10.1016/S0140-6736(15)00551-6
5. Mendis S, Johnston SC, Fan W, Oladapo O, Cameron A, Faramawi MF. Cardiovascular risk management and its impact on hypertension control in primary care in low-resource settings: a cluster-randomized trial. Bull World Health Organ. 2010;88(6):412–419. doi:10.2471/BLT.08.062364
6. Zhao D, Liu J, Wang M, Zhang X, Zhou M. Epidemiology of cardiovascular disease in China: current features and implications. Nat Rev Cardiol. 2019;16(4):203–212. doi:10.1038/s41569-018-0119-4
7. Wu Y, Benjamin EJ, MacMahon S. Prevention and control of cardiovascular disease in the rapidly changing economy of China. Circulation. 2016;133(24):2545–2560. doi:10.1161/CIRCULATIONAHA.115.008728
8. Khaing W, Vallibhakara SA, Attia J, McEvoy M, Thakkinstian A. Effects of education and income on cardiovascular outcomes: a systematic review and meta-analysis. Eur J Prev Cardiol. 2017;24(10):1032–1042. doi:10.1177/2047487317705916
9. Subramanian SV, Corsi DJ, Subramanyam MA, Smith GD. Jumping the gun: the problematic discourse on socioeconomic status and cardiovascular health in India. Int J Epidemiol. 2013;42(5):1410–1426. doi:10.1093/ije/dyt017
10. Xia X, Yue W, Chao B, et al. Prevalence and risk factors of stroke in the elderly in Northern China: data from the national stroke screening survey. J Neurol. 2019;266(6):1449–1458. doi:10.1007/s00415-019-09281-5
11. Geldsetzer P, Manne-Goehler J, Theilmann M, et al. Geographic and sociodemographic variation of cardiovascular disease risk in India: a cross-sectional study of 797,540 adults. PLoS Med. 2018;15(6):e1002581. doi:10.1371/journal.pmed.1002581
12. Waenerlund AK, Mosquera PA, Gustafsson PE, San Sebastián M. Trends in educational and income inequalities in cardiovascular morbidity in middle age in Northern Sweden 1993–2010. Scand J Public Health. 2019;47(7):713–721. doi:10.1177/1403494818790406
13. Rosengren A, Smyth A, Rangarajan S, et al. Socioeconomic status and risk of cardiovascular disease in 20 low-income, middle-income, and high-income countries: the Prospective Urban Rural Epidemiologic (PURE) study. Lancet Global Health. 2019;7(6):e748–e60. doi:10.1016/S2214-109X(19)30045-2
14. Dalstra JA, Kunst AE, Borrell C, et al. Socioeconomic differences in the prevalence of common chronic diseases: an overview of eight European countries. Int J Epidemiol. 2005;34(2):316–326. doi:10.1093/ije/dyh386
15. Elfassy T, Swift SL, Glymour MM, et al. Associations of income volatility with incident cardiovascular disease and all-cause mortality in a US cohort. Circulation. 2019;139(7):850–859. doi:10.1161/CIRCULATIONAHA.118.035521
16. Yan R, Li W, Yin L, Wang Y, Bo J. Cardiovascular diseases and risk-factor burden in urban and rural communities in high-, middle-, and low-income regions of china: a large community-based epidemiological study. J Am Heart Assoc. 2017;6(2). doi:10.1161/JAHA.116.004445
17. Kim Y, Twardzik E, Judd SE, Colabianchi N. Neighborhood socioeconomic status and stroke incidence: a systematic review. Neurology. 2021;96(19):897–907. doi:10.1212/WNL.0000000000011892
18. Besser LM, McDonald NC, Song Y, Kukull WA, Rodriguez DA. Neighborhood environment and cognition in older adults: a systematic review. Am J Prev Med. 2017;53(2):241–251. doi:10.1016/j.amepre.2017.02.013
19. Kaneva M, Jakovljevic M. Socioeconomic and behavioral determinants of cardiovascular risk in Russia: a structural equation modeling approach. Risk Manag Healthc Policy. 2023;16:585–605. doi:10.2147/RMHP.S388873
20. Malaeb D, Hallit S, Dia N, et al. Effects of sociodemographic and socioeconomic factors on stroke development in Lebanese patients with atrial fibrillation: a cross-sectional study. F1000Research. 2021;10:793. doi:10.12688/f1000research.54236.1
21. Kee CC, Jamaiyah H, Noor Safiza MN, et al. Abdominal obesity in Malaysian adults: national health and morbidity survey III (NHMS III, 2006). Malays J Nutr. 2008;14(2):125–135.
22. Yusuf S, Joseph P, Rangarajan S, et al. Modifiable risk factors, cardiovascular disease, and mortality in 155 722 individuals from 21 high-income, middle-income, and low-income countries (PURE): a prospective cohort study. Lancet. 2020;395(10226):795–808. doi:10.1016/S0140-6736(19)32008-2
23. Raffington L, Prindle J, Keresztes A, Binder J, Heim C, Shing YL. Blunted cortisol stress reactivity in low-income children relates to lower memory function. Psychoneuroendocrinology. 2018;90:110–121. doi:10.1016/j.psyneuen.2018.02.002
24. Ryan M, Gallagher S, Jetten J, Muldoon OT. State level income inequality affects cardiovascular stress responses: evidence from the midlife in the United States (MIDUS) study. Soc Sci Med. 2022;311:115359. doi:10.1016/j.socscimed.2022.115359
25. Lazzarino AI, Hamer M, Stamatakis E, Steptoe A. Low socioeconomic status and psychological distress as synergistic predictors of mortality from stroke and coronary heart disease. Psychosom Med. 2013;75(3):311–316. doi:10.1097/PSY.0b013e3182898e6d
26. Theorell T. Psychosocial stressors in psychosomatic cardiology: a narrative review. Heart Mind. 2022;6(4):211–218. doi:10.4103/hm.hm_26_22
27. Hyldgård VB, Johnsen SP, Støvring H, Søgaard R. Socioeconomic status and acute stroke care: has the inequality gap been closed? Clin Epidemiol. 2019;11:933–941. doi:10.2147/CLEP.S218322
28. Kilpi F, Konttinen H, Silventoinen K, Martikainen P. Living arrangements as determinants of myocardial infarction incidence and survival: a prospective register study of over 300,000 Finnish men and women. Soc Sci Med. 2015;133:93–100. doi:10.1016/j.socscimed.2015.03.054
29. El Hadidi S, Samir Bazan N, Byrne S, Darweesh E, Bermingham M. heart failure prescribing quality at discharge from a critical care unit in Egypt: the impact of multidisciplinary care. Pharmacy. 2020;8(3). doi:10.3390/pharmacy8030159
30. Zhan Y, Yu J, Chen R, et al. Socioeconomic status and metabolic syndrome in the general population of China: a cross-sectional study. BMC Public Health. 2012;12:921. doi:10.1186/1471-2458-12-921
31. Gao B, Zhang L, Wang H. Clustering of major cardiovascular risk factors and the association with unhealthy lifestyles in the Chinese adult population. PLoS One. 2013;8(6):e66780. doi:10.1371/journal.pone.0066780
32. Marinho F, de Azeredo Passos VM, Malta DC, et al. Burden of disease in Brazil, 1990–2016: a systematic subnational analysis for the global burden of disease study 2016. Lancet. 2018;392(10149):760–775. doi:10.1016/S0140-6736(18)31221-2
33. Dobson A, McLaughlin D, Vagenas D, Wong KY. Why are death rates higher in rural areas? Evidence from the Australian longitudinal study on women’s health. Aust N Z J Public Health. 2010;34(6):624–628.
34. Sun J, Lyu X, Yang F. The effect of new rural cooperative medical scheme on the socioeconomic inequality in inpatient service utilization among the elderly in China. Risk Manag Healthc Policy. 2020;13:1383–1390. doi:10.2147/RMHP.S252336
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Associations Between Adult Attention-Deficit/Hyperactivity Disorder (ADHD) Traits and Sociodemographic Characteristics in Japanese Workers
Suzuki T, Wada K, Nakazato M, Ohtani T, Yamazaki M, Ikeda S
Neuropsychiatric Disease and Treatment 2023, 19:759-773
Published Date: 5 April 2023
Patterns of Non-Communicable Disease, Multimorbidity, and Population Awareness in Bahir Dar, Northwest Ethiopia: A Cross-Sectional Study
Alamnia TT, Sargent GM, Kelly M
International Journal of General Medicine 2023, 16:3013-3031
Published Date: 13 July 2023
Metabolic Syndrome and Socioeconomic Status in Association with Chronic Kidney Disease: A Cross-Sectional Study in Ningbo, China
Huang S, Yao X, Chen X, Chen X, Li Y, Kanwar Y, Chan FKS, Ye P, Zhan M
Diabetes, Metabolic Syndrome and Obesity 2024, 17:3891-3901
Published Date: 21 October 2024
Socioeconomic Status Related to Prescription of Triple Therapy and Anticholinergic Monotherapy in Patients with Chronic Obstructive Pulmonary Disease (COPD) in Sweden - A Retrospective National Registry Study
Larsson K, Betnér S, Fuchs B, Vanfleteren LEGW, Stridsman C
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:3597-3606
Published Date: 7 November 2025
Cardiovascular Disease in Advanced Chronic Kidney Disease in a Tertiary Institution, Johannesburg, South Africa
Mbenya Z, Nqebelele U, Adamu UG, Mpanya D, Tsabedze N, Mashabane M
International Journal of Nephrology and Renovascular Disease 2026, 19:595470
Published Date: 25 June 2026