Back to Journals » Neuropsychiatric Disease and Treatment » Volume 19
Associations Between Adult Attention-Deficit/Hyperactivity Disorder (ADHD) Traits and Sociodemographic Characteristics in Japanese Workers
Authors Suzuki T ![]() , Wada K, Nakazato M, Ohtani T, Yamazaki M, Ikeda S
, Wada K, Nakazato M, Ohtani T, Yamazaki M, Ikeda S
Received 2 December 2022
Accepted for publication 23 February 2023
Published 5 April 2023 Volume 2023:19 Pages 759—773
DOI https://doi.org/10.2147/NDT.S398478
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 6
Editor who approved publication: Professor Taro Kishi
Tomoko Suzuki,1 Koji Wada,1,2 Michiko Nakazato,3 Toshiyuki Ohtani,4 Michiko Yamazaki,2 Shunya Ikeda1,2
1Department of Public Health, School of Medicine, International University of Health and Welfare, Narita, Japan; 2Department of Social Medical Sciences, Graduate School of Medicine, International University of Health and Welfare, Tokyo, Japan; 3Department of Psychiatry, School of Medicine, International University of Health and Welfare, Narita, Japan; 4Safety and Health Organization, Chiba University, Chiba, Japan
Correspondence: Tomoko Suzuki, Department of Public Health, School of Medicine, International University of Health and Welfare, 4-3 Kozunomori, Narita, Chiba, 286-8686, Japan, Tel +81-476-20-7701, Fax +81-476- 28-1188, Email [email protected]; [email protected]
Purpose: Most previous studies that described associations between adult attention-deficit/hyperactivity disorder (ADHD) and sociodemographic characteristics were focused on individuals diagnosed with ADHD, and few studies investigated ADHD traits in the general population. Additionally, some workers, who experienced no problems while at university and successfully graduated from university, developed ADHD traits after finding employment. This study described associations between ADHD traits and sociodemographic characteristics among Japanese workers who were university graduates.
Patients and Methods: Participants were randomly selected workers (n=1240) from across Japan who completed a self-administered online survey. ADHD traits were measured using an adult ADHD Self-report Scale, with scoring rules applied to reflect the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition criteria. Information was collected on sociodemographic characteristics including sex, age, socioeconomic status, working time, and health-related behaviors. We performed partial correlation analysis to estimate trend associations and used analysis of covariance to compare adjusted averages. This model was adjusted for all variables.
Results: Males had higher levels of ADHD traits than females (p = 0.001), and younger age was associated with higher levels of ADHD traits (p < 0.001). Workers with low incomes had higher levels of ADHD traits than workers with high incomes (p = 0.009). More frequent consumption of midnight meals was associated with higher levels of ADHD traits (p < 0.001), although there were no differences for breakfast, lunch, and dinner. Those who did not get enough rest from sleep had higher levels of ADHD traits (p = 0.007).
Conclusion: Results for high levels of ADHD traits among workers were consistent with previous studies for adults diagnosed with ADHD, even though all participants had successfully graduated from university. Assessment of these ADHD traits may support prevention of health deterioration related to these ADHD traits.
Keywords: ADHD traits, eating habits, income, lifestyle habits, sleep, socioeconomic status
Introduction
Attention-deficit/hyperactivity disorder (ADHD) is a chronic neuropsychiatric disorder defined by symptoms of inattention, hyperactivity, and impulsivity, and causes severe impairment and morbidity.1 ADHD symptoms have many negative life impacts. For example, ADHD in adults is frequently associated with comorbid psychiatric diseases, including depression2–4 and bipolar disorder,5 as well as with substance abuse and suicide attempts.6 Although ADHD diagnoses are defined categorically, ADHD traits are continuously distributed in the general population, and individuals with ADHD exist at the extreme ends of the continuum of ADHD traits.7–9 Significant differences have been found between healthy individuals with high and low levels of ADHD traits.7 For example, sickness presenteeism was significantly associated with high levels of ADHD traits among Japanese university students.10
Previous studies have investigated associations between adult ADHD traits and sociodemographic characteristics. Adult ADHD was more common among males than females,1,4,11–13 and younger adults had a higher prevalence of ADHD than older age groups.4,14 Studies that explored socioeconomic status (SES) found adults with ADHD were less likely to work than those without ADHD.15–17 Adult ADHD was also associated with a decline in work performance11,15,18,19 and low education levels.12 These studies also suggested that adult ADHD was associated with low SES. Furthermore, adults with higher levels of ADHD traits were more likely to eat snacks than those without such traits.20 Some studies that targeted children with ADHD reported similar results to those for adults with ADHD.21,22 In addition, previous reviews indicated that most adults with ADHD have sleep problems such as insomnia and daytime sleepiness.23,24 The potential for ADHD has also been suggested to be an early warning sign for secondary prevention of health deterioration,19 as adults with high levels of ADHD traits are more likely to lead unhealthy lifestyles.20 Moreover, intergenerational trauma has been implicated in ADHD, where the exposure of parents to trauma can have a negative impact on the mental health of their children.25 Parenting behavior influences the psychiatric outcomes of children, where negative behavior is a risk factor for ADHD.26
Most previous studies that described associations between ADHD and sociodemographic characteristics were focused on individuals diagnosed with ADHD, and few studies investigated ADHD traits in the general population. However, it is likely that associations between ADHD traits and sociodemographic characteristics in the general adult population will be consistent with previous studies of adults with ADHD. Additionally, some workers, who experienced no problems while at university and successfully graduated from university, developed ADHD traits after finding employment. Despite this being an important issue, few studies have targeted university graduate workers. This study aimed to describe the associations between adult ADHD traits and sociodemographic characteristics among Japanese workers. The sociodemographic characteristics associated with adult ADHD traits are a core element of ADHD traits and may provide insight into providing support for those with ADHD traits. We targeted university graduates because even among working adults who had successfully graduated from university, it is likely that associations between ADHD traits and sociodemographic characteristics would be similar to previous results for adults with ADHD.
Materials and Methods
Participants
Participants were 1240 workers from different regions of Japan who had graduated from university. Data were collected using an Internet-based questionnaire survey that was conducted in March 2019. The study profile has previously been described in detail.27 As part of a larger program of research on the influence of lifestyle factors on work and health, this study aimed to examine the relationships among mental health (with a focus on ADHD and autistic traits), lifestyle, and the work environment. The goal was to identify effective ways to prevent or reduce mental health problems in the workplace. The subjects were recruited from among approximately 1.2 million individuals, residing in all prefectures in Japan, registered with a Japanese online survey company (Macromill Inc., Tokyo, Japan). In total, 86,880 of approximately 450,000 workers aged 20–69 years were randomly selected and invited to participate in the study via e-mail. Screening was conducted to ensure that participants met the study eligibility criteria; we screened individuals aged 20–69 years who were university graduates and regular staff not currently on leave. The questionnaire was designed to end automatically once all responses had been provided. We eliminated sex bias using a sex ratio of 1:1, and age bias by including the same number of participants in all age groups (20–29, 30–39, 40–49, 50–59, and 60–69 years).
Sociodemographic Characteristics
The workers surveyed in this study completed a self-administered questionnaire that collected data on sociodemographic characteristics including sex, age, SES (ie, annual household income and occupational position), working time, and health-related behaviors (ie, smoking habits, drinking habits, leisure-time physical activity, eating habits, sleeping hours, and rest in sleep). Age was categorized into five groups (20–29, 30–39, 40–49, 50–59, and 60–69 years). Annual household income was classified into six categories: less than 4 million yen, 4–6 million yen, 6–8 million yen, 8–10 million yen, 10–12 million yen, and 12 million yen or more (100 Japanese yen equals approximately 1 USD). Occupational position was divided into four groups (president or executive level, chief director level, section chief or chief clerk level, and non-executive position). Working hours per week were classified into three categories (≤40, 41–50, and ≥51 hours). Drinking habits were categorized into three groups (almost every day, sometimes, and rarely) and smoking habits were categorized into three groups (current smoking, quit smoking, and no smoking). Leisure-time physical activity was divided into four groups: no activity, light physical activity one or more times per week, intense physical activity one or two times a week, and intense physical activity three or more times a week. Weekly intake frequencies of breakfast, lunch, dinner, snacks, and midnight meals were classified into four categories, 0–2 days, 3–4 days, 5–6 days, and 7 days (every day). A snack was defined as a light meal eaten between breakfast and lunch or between lunch and dinner, and a midnight meal was defined as a simple meal eaten late at night after dinner. Sleeping hours per day were classified into four categories: less than 5 hours, 5–6 hours, 6–7 hours, and 7 hours or more. Finally, enough rest from sleep was classified into four categories: enough rest, decent rest, not rest much, and no rest.
ADHD Traits
The adult ADHD Self-Report Scale (ASRS)28 was used to determine participants’ ADHD traits. The ASRS is an 18-item self-report scale covering the 18 symptoms of adult ADHD from the Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV).29 The ASRS Screener is a short version of the ASRS that includes 6 of the 18 ASRS questions. The six questions pertain to four inattention symptoms and two impulsivity/hyperactivity symptoms that characterize ADHD.28 In this study, ASRS subtypes were distinguished on the basis of the ASRS Screener results. Each ASRS question asks how often a particular ADHD symptom has occurred over the past 6 months. The response scale is as follows: 0, never; 1, rarely; 2, sometimes; 3, often; and 4, very often. Higher scores denote higher levels of ADHD traits. The Japanese version of the ASRS was used in this study.30 Data obtained using the DSM-IV ASRS screening scale can also be assessed in terms of their association with ADHD traits according to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) criteria,1 by following scoring rules developed for consistency with the DSM-5.10,31,32 The lowest and highest possible scores are 0 and 20, respectively.
Statistical Analyses
To examine the associations between ADHD traits and sociodemographic characteristics, adjusted ASRS and ASRS subtype scores were calculated and subjected to partial correlation analysis, analysis of covariance, and nonparametric analysis. Averages of the ASRS and ASRS subtype scores were adjusted for age and sex, or for all variables (sex, age, annual household income, occupational position, working time, drinking habits, smoking habits, leisure-time physical activity, weekly intake frequency of breakfast, lunch, dinner, snacks, and midnight meals, sleeping hours/day, and enough rest from sleep). Partial correlation analysis was performed to estimate the trend association between ASRS or ASRS subtype scores and sociodemographic characteristics by assigning ordinal numbers for each sociodemographic characteristic when these characteristics were ordinal variables. Analysis of covariance was performed to compare the adjusted averages of the ASRS and ASRS subtype scores for each sociodemographic characteristic when these characteristics were not ordinal variables. This model was adjusted for age and sex as well for all variables. The nonparametric tests performed in this study included the Mann–Whitney U-test (for comparison between two groups), Kruskal–Wallis test (for comparison among three groups), and Spearman’s rank correlation. The level of significance was 0.05 (two-tailed). Statistical analyses were conducted using SPSS software (version 24 for Windows, IBM Corp., Armonk, NY, USA).
Ethics Statement
The Ethics Committee of the International University of Health and Welfare reviewed and approved this study (No. 18-Im-017), which was conducted in accordance with the standards specified in the 1964 Declaration of Helsinki. Responding to the questionnaire implied voluntary consent to participate in the study. Individuals who agreed to participate responded directly to an anonymous online questionnaire. The Ethics Committee of the International University of Health and Welfare waived the need for written informed consent from participants.
Results
Participant Sociodemographic Characteristics
In total, 11,898 workers answered the screening questions, of whom 2658 met the eligibility criteria; 1934 of those workers were randomly selected and granted access to the self-report questionnaire. The survey was closed when 1284 workers had completed the questionnaire (1240 of whom were provided by the survey company). Therefore, the final analysis target was 1240 participants. Participant demographics are displayed in Table 1. In total, 1240 workers participated in this study. About one-quarter of the participants had an annual household income of 4–6 million yen, about two-thirds held non-executive positions, and approximately 40% worked 41–50 hours per week.
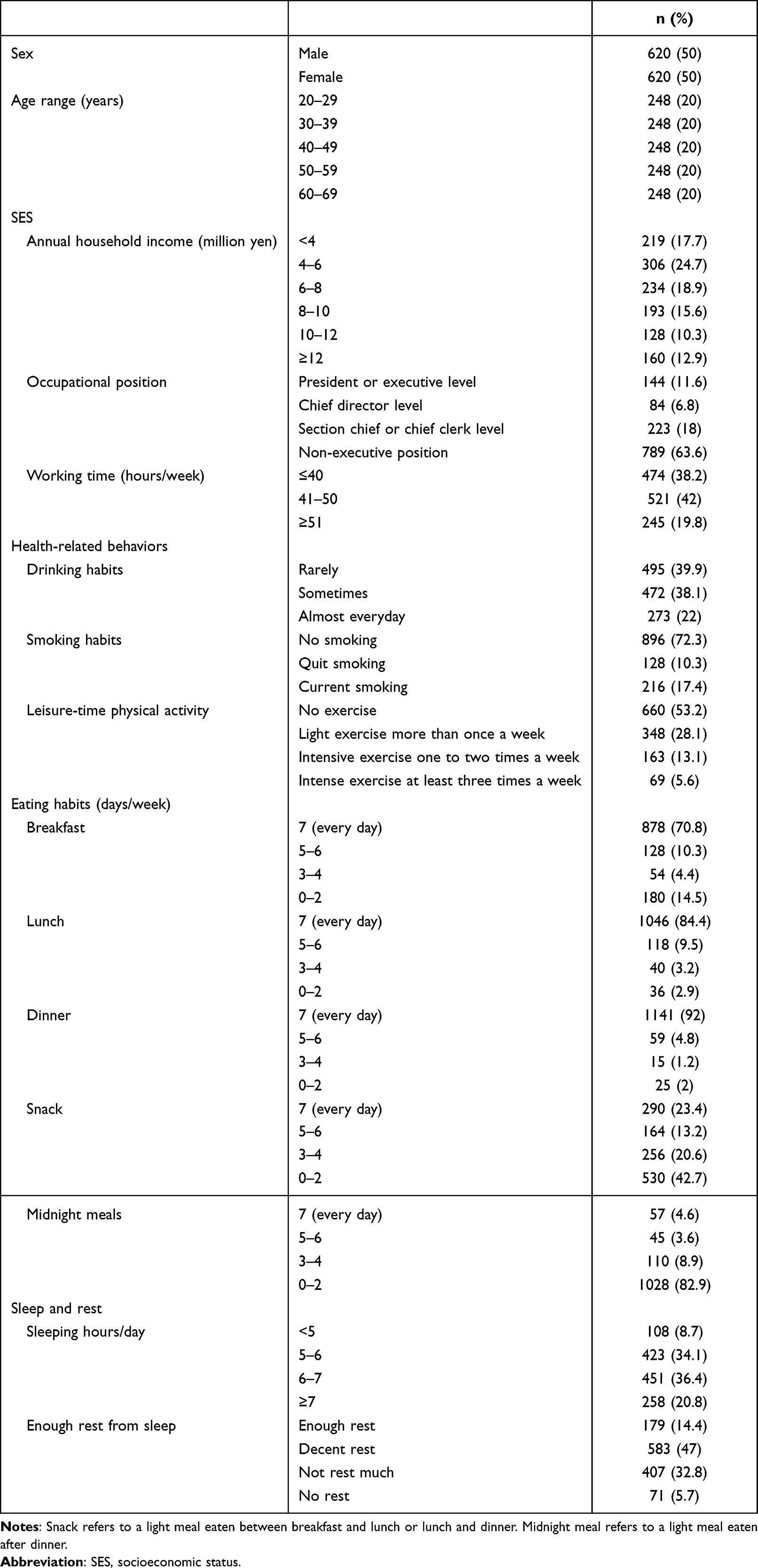 |
Table 1 Participants’ Sociodemographic Characteristics (N = 1240) |
Association Between Sociodemographic Characteristics and ADHD Traits (ASRS) Scores
Table 2 shows the association between sociodemographic characteristics and ADHD traits (ASRS) scores. After adjustment for sex and age, the results showed that males had significantly higher ASRS scores than females (p = 0.001), and a younger age was associated with higher ASRS scores (p < 0.001). Workers from a low-income background had significantly higher ASRS scores than workers from a high-income background (p = 0.009). Workers in lower occupational positions tended to have higher ASRS scores than those in higher occupational positions, although the difference was not significant. In addition, higher weekly working hours were associated with higher ASRS scores (p = 0.035). No significant differences were found in ASRS scores based on drinking habits, smoking habits, or leisure-time physical activity. In addition, no significant differences were found in ASRS scores based on the frequency of consuming breakfast, lunch, or dinner. However, a higher frequency of snacks and midnight meals was associated with higher ASRS scores (p = 0.003 and p < 0.001, respectively). Finally, those who had a short sleep duration or that did not get enough rest from sleep had higher ASRS scores that those with long sleep duration or sufficient rest from sleep (p = 0.004 and p < 0.001, respectively). After adjusting for all variables, the variables that remained significantly associated were sex (p = 0.001), age (p < 0.001), annual household income (p = 0.009), frequency of midnight meals (p < 0.001), and enough rest from sleep (p = 0.007). The variables of working time, snack, and sleep duration became non-significant. The results of the nonparametric analyses were generally consistent with those of the fully adjusted parametric analyses. However, occupational position (p = 0.007) was a significant factor only in the nonparametric analyses, while working time (p < 0.001) and sleeping hours (p = 0.021) were significant in the sex- and age-adjusted multivariate analyses and nonparametric analyses, but not in the fully adjusted multivariate analyses.
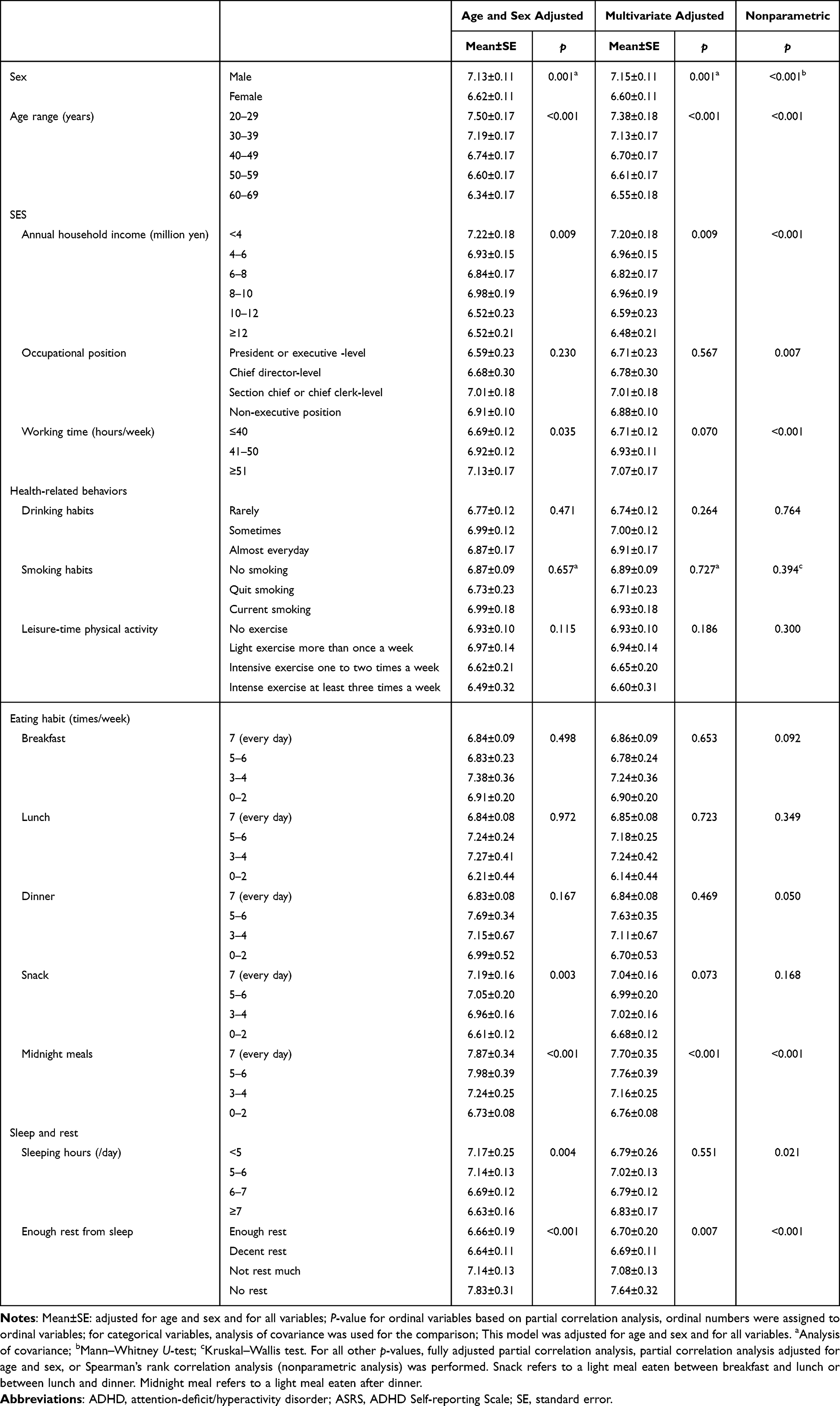 |
Table 2 Association Between Sociodemographic Characteristics and ADHD Traits (ASRS Scores) Scores (N = 1240) |
Association Between Sociodemographic Characteristics and ADHD Subtype Traits (ASRS Subtype) Scores
The results of ASRS subtype scores after adjustment for sex and age, which was different from the ASRS scores are presented in Table 3. No significant difference was found in Inattention scores based on sex. No significant difference was found in Hyperactivity-Impulsivity scores by annual household income or weekly working hours. However, lower occupational positions were associated with higher Hyperactivity-Impulsivity scores (p = 0.031). Finally, less leisure-time physical activity was associated with higher Inattention scores (p = 0.004). After adjusting for all variables, the variables that no longer showed a significant difference were occupational position in Hyperactivity-Impulsivity trait scores, snack and sleep duration in both ADHD subtype trait scores, midnight meals in Inattention trait scores, and enough rest from sleep in Hyperactivity-Impulsivity trait scores. The results of the parametric and nonparametric analyses were generally consistent, although the frequency of consuming breakfast (p = 0.030; Inattention trait), and annual household income and working time (p = 0.006 and p = 0.004, respectively; Hyperactivity-Impulsivity traits) were significant only in the latter analyses. Furthermore, the frequency of midnight meals and sleeping hours (p = 0.004 and p = 0.027, respectively; Inattention traits), and occupational position and enough rest from sleep (p = 0.008 and p = 0.046, respectively; Hyperactivity-Impulsivity trait scores) were significant in the sex- and age-adjusted multivariate and nonparametric analyses, but not in the fully adjusted multivariate analysis.
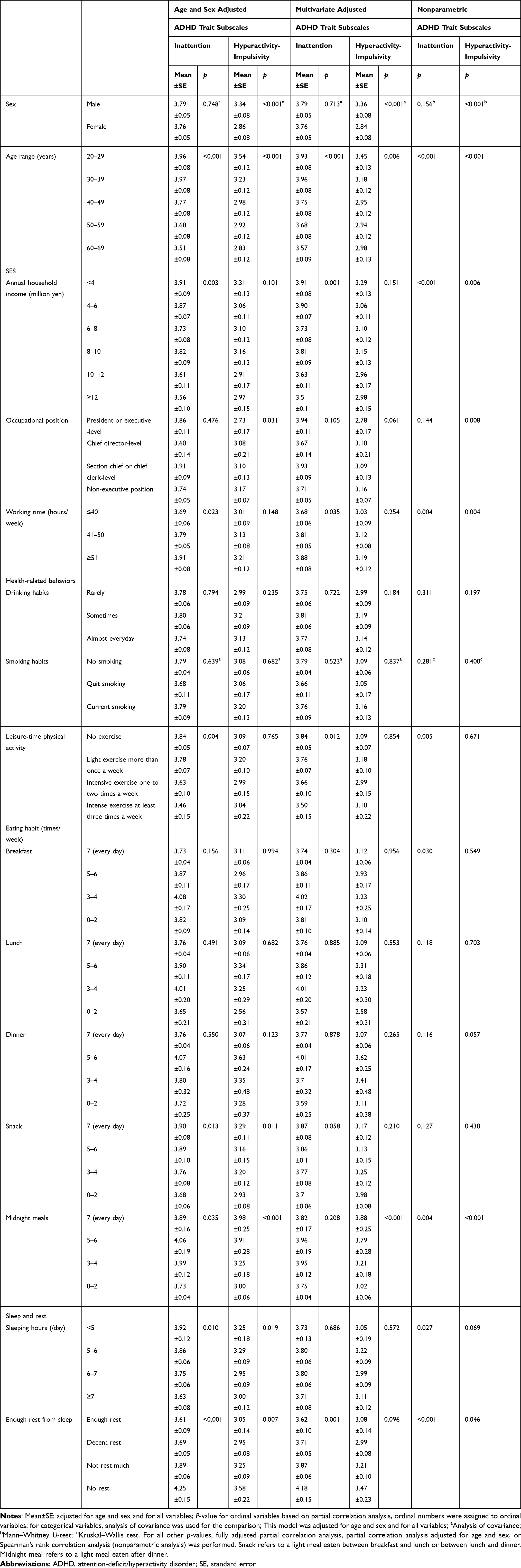 |
Table 3 Association Between Sociodemographic Characteristics and ADHD Subtype Traits Scores (N = 1240) |
Discussion
We examined associations between ADHD traits and sociodemographic characteristics among 1240 Japanese workers. Participants were sampled from across Japan, had a university education or higher, and were not a patient population. Our results for workers with high level of ADHD traits in this group were roughly consistent with previous studies for adults diagnosed with ADHD. Males had significantly higher levels of ADHD traits than females, and a younger age was associated with higher levels of ADHD traits. Workers with low incomes had higher level of ADHD traits than workers with high incomes, even though all participants were university graduates. Those that more frequently consumed midnight meals had higher levels of ADHD traits, although there were no differences based on the frequency of breakfast, lunch, and dinner. Those who did not get enough rest from sleep also had higher levels of ADHD traits than other participants.
Our results for SES showed that workers with low annual household income had higher levels of ADHD or Inattention traits than workers with a high annual household income. This highlighted that workers with a low SES had higher levels of ADHD traits than workers with a high SES, even though all participants were university graduates. Previous studies have shown that ADHD among adults is associated with factors that lead to low SES, such as frequent job changes,33 unemployment,15–17 underachievement at work,11 low performance and reduced productivity at work,11,15,18,19 and low education.12 ADHD has also been found to be less common among professionals than other workers.11 Our results are consistent with previous studies that showed that individuals with strong ADHD traits have low SES. However, despite previous studies reporting an association between low performance and ADHD traits,11,18 which affects occupational position, we found no significant differences in ADHD traits among various occupational positions in multivariate-adjusted analyses. However, in nonparametric analyses, ADHD and Hyperactivity-Impulsivity trait scores showed inverse associations with occupational position. Our study targeted workers who had graduated from university; therefore, our results suggested that workers with high level of ADHD traits can have difficulty working and adapting to society despite successfully graduating from university, which may lead to a decline in SES. Previously, it was reported that the association between ADHD symptoms and academic performance among university students was partially mediated by depressive symptoms.34 We suggest that supporting students with depressive symptoms, which are common, may improve academic achievement and, by extension, SES.
Our results showed an association between a higher frequency of snacks/midnight meals and a higher level of ADHD traits, although frequency of snacks was not significant after adjusting for multiple variables. However, there were no differences based on the frequency of breakfast, lunch, and dinner. No previous studies on the relationship between ADHD and dietary frequency were available. However, studies on the relationship between ADHD and dietary patterns suggested that adults with high levels of ADHD traits reported frequent snacking on sweets.20 Studies involving children found that individuals with ADHD symptoms also consumed more snack food21,22 and were more likely to overeat22,35 than those without these symptoms. Such eating behavior may lead to obesity, and many studies have explored the relationship between ADHD and obesity. Two meta-analyses showed similar results of a significant association between ADHD and obesity among adults, with odds ratios of 1.5536 and 1.37.37 Our results support these findings.
Regarding sleep and rest, we found that workers who had shorter sleep duration or that did not get enough rest from sleep had higher levels of ADHD traits than those with longer sleep duration or sufficient rest, although sleep duration was not significant following adjustment for multiple variables. This was consistent with previous studies that found higher levels of ADHD traits among individuals with shorter sleep duration compared with longer sleep duration. Previous reviews showed bedtime resistance, difficulty with morning awakenings, sleep onset difficulties, and insomnia among individuals with ADHD.23,24 A population-based study suggested that ADHD symptoms were linked to shorter sleep duration, long sleep latency, nocturnal wake time, and sleep deficiency in adolescents.38 These sleep problems result in reduced sleep time and daytime sleepiness.39 Many studies have reported daytime sleepiness in individuals with ADHD.23,24 These studies supported our finding of higher levels of ADHD traits among workers who did not get enough rest from sleep. In terms of subtypes of ADHD traits of our study, workers did not get enough rest from sleep showed higher levels of Inattention traits. In a previous study, Inattention traits were strongly correlated with insomnia.40 The most common sleep disorder is delayed circadian rhythm, which is seen in the majority of adults with ADHD.41 In one report, melatonin treatment advanced the circadian rhythm, although the reduction of ADHD symptoms seen in that study was not attributed to the change in circadian rhythm.42 Sleep disorders are more frequent and severe in adults with ADHD compared with other psychiatric outpatients, and it has been suggested that sleep disturbances are an intrinsic feature of adult ADHD rather than a consequence of comorbid psychiatric conditions.43
Our results showed that males had significantly higher levels of ADHD traits than females, which was consistent with most previous studies that found adult ADHD was more common among males than females.1,4,11–13 We also found that a younger age was associated with higher levels of ADHD traits, which was also consistent with previous studies that reported a higher prevalence of ADHD among younger adults.4,14 We found no significant differences in ASRS scores by drinking habits, smoking habits, or leisure-time physical activity, although less leisure-time physical activity was associated with higher Inattention trait scores. Our results for smoking and drinking were inconsistent with previous studies that found ADHD was associated with smoking,19 and ADHD symptoms were associated with frequency of drinking in college students.44 Differences in the way we assessed drinking and smoking habits may be one reason for the discrepancy between our results and those of previous studies. It has previously been reported that smokers with ADHD experience withdrawal symptoms more severely than do smokers without ADHD.45 In this study, we only asked participants about whether they were currently smokers and not necessarily heavy smokers with withdrawal symptoms. For drinking, we asked participants whether they consumed alcohol almost every day, sometimes, or rarely, and did not evaluate the level of excessive alcohol consumption as assessed in a previous study.44 Although no studies related to ADHD and exercise were available, some studies that investigated exercise as a treatment found physical exercise had potential benefits as an alternative or additional treatment option for ADHD.46 Our ASRS subtype results were roughly the same as our ASRS results. Previous studies suggested the inattention subtype was most prevalent in adults with ADHD.47,48 A population-based study reported inattentive symptoms were the most strongly associated with clinical impairment.49
The target population of our study was university graduate workers, who differ from university students in several ways. Firstly, university students have individual freedoms, and their daily lives are less structured than those of workers, which are regulated by the workplace. Thus, university students with ADHD symptoms have irregular lifestyles, such as irregular sleeping hours, lower sleep quality, and irregular eating habits, such as binge eating.50,51 In contrast, workers must follow workplace systems; therefore, they are less likely than university students to follow an irregular lifestyle during working hours. Secondly, there are differences between our target university graduate workers and general workers. Both our and previous results showed that workers with strong ADHD traits had low SES. However, the type of SES differed between studies. In our study, low income was significantly associated with ADHD traits, but occupational position was not, whereas in previous reports, poor work performance, which affects occupational position, was associated with ADHD.11,15,18,19
Implications
There are important implications from the findings of our study. In our study, several sociodemographic characteristics, especially SES, were associated with high level of ADHD traits for workers, despite those participants having successfully graduated from university. Thus, certain sociodemographic characteristics may predict high ADHD traits. Workers with such traits should be assisted accordingly.
Although it is important to include young people in studies on the genetic determinants of mental illness, this population is currently underrepresented in psychiatric research52 However, this was not the case in our study; we included equal numbers of participants in all age groups.
Limitations
This study had some limitations that warrant consideration. First, we used an online questionnaire and our sample might have been biased toward individuals who were more familiar with Internet use. Second, the DSM-IV ASRS Screener with revised scoring based on the DSM-5 criteria reported by Ustun et al31 that was used to evaluate ADHD in this study, was less accurate relative to the new DSM-5 ASRS Screener.31 However, the DSM-IV ASRS Screener with revised scoring detects most DSM-5 cases (sensitivity 84.2% and specificity 89.5%) at a threshold of maximum area under the curve.31 Third, a previous report found that self-reported evaluations may underestimate ADHD traits.53 However, high agreement between self-ratings and observer ratings for ADHD diagnoses in adults has been reported.54 Nevertheless, it will be important to replicate the present results in studies performing more detailed assessments of ADHD symptoms through validated clinical interviews.
Conclusions
We examined associations between ADHD traits and sociodemographic characteristics among 1240 Japanese workers. Participants were sampled from across Japan, had a university education or higher, and were not a patient population. Our results for characteristics associated with high levels of ADHD traits among these workers were consistent with previous studies for adults diagnosed with ADHD, even though all participants had successfully graduated from university. Males had significantly higher levels of ADHD traits than females, and a younger the age was associated with a higher level of ADHD traits. The following findings are of particular importance. Workers with a low income had higher level of ADHD traits than workers with a high income, even though they were all university graduates. Assessment of lifestyle habits showed a higher frequency of midnight meals was associated with a higher level of ADHD traits, although there were no differences based on the frequency of breakfast, lunch, and dinner. Those who did not get enough rest from sleep also had higher levels of ADHD traits. Assessment of these ADHD traits may support prevention of health deterioration related to these ADHD traits.
Abbreviations
ADHD, Attention-deficit/hyperactivity disorder; ASRS, adult ADHD Self-Report Scale; DSM-IV, Diagnostic and Statistical Manual of Mental Disorders, fourth edition; DSM-5, Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition; SES, socioeconomic status.
Acknowledgments
This work was supported by the Japan Society for the Promotion of Science (JSPS) KAKENHI (grant numbers JP16K09105 [Chief: Dr. Tomoko Suzuki] and JP21K10453 [Chief: Dr. Tomoko Suzuki]) and IUHW Research Grants (Chief: Dr. Tomoko Suzuki), Japan.
We thank Audrey Holmes, MA, Sarina Iwabuchi, PhD, and Michael Irvine, PhD, from Edanz (https://jp.edanz.com/ac) for editing a draft of this manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. American Psychiatric Association, DSM-5 Task Force. Diagnostic and Statistical Manual of Mental Disorders: DSM-5.
2. Kessler RC, Adler L, Barkley R, et al. The prevalence and correlates of adult ADHD in the United States: results from the national comorbidity survey replication. Am J Psychiatry. 2006;163(4):716–723. doi:10.1176/ajp.2006.163.4.716
3. Meinzer MC, Lewinsohn PM, Pettit JW, et al. Attention-deficit/hyperactivity disorder in adolescence predicts onset of major depressive disorder through early adulthood. Depress Anxiety. 2013;30(6):546–553. doi:10.1002/da.22082
4. Chung W, Jiang SF, Paksarian D, et al. Trends in the prevalence and incidence of attention-deficit/hyperactivity disorder among adults and children of different racial and ethnic groups. JAMA Netw Open. 2019;2(11):e1914344. doi:10.1001/jamanetworkopen.2019.14344
5. Bartoli F, Callovini T, Cavaleri D, et al. Clinical correlates of comorbid attention deficit hyperactivity disorder in adults suffering from bipolar disorder: a meta-analysis. Aust NZJ Psychiatry. 2023;57(1):34–48. doi:10.1177/00048674221106669
6. Valsecchi P, Nibbio G, Rosa J, et al. Adult ADHD: prevalence and clinical correlates in a sample of italian psychiatric outpatients. J Atten Disord. 2021;25(4):530–539. doi:10.1177/1087054718819824
7. Panagiotidi M, Overton PG, Stafford T. The relationship between ADHD traits and sensory sensitivity in the general population. Compr Psychiatry. 2018;80:179–185. doi:10.1016/j.comppsych.2017.10.008
8. Panagiotidi M, Overton PG, Stafford T. Co-occurrence of ASD and ADHD traits in an adult population. J Atten Disord. 2019;23(12):1407–1415. doi:10.1177/1087054717720720
9. McLennan JD. Understanding attention deficit hyperactivity disorder as a continuum. Can Fam Physician. 2016;62(12):979–982.
10. Suzuki T, Wada K, Muzembo B, Ngatu N, Yoshii S, Ikeda S. Autistic and attention deficit/hyperactivity disorder traits are associated with suboptimal performance among Japanese university students. JMA J. 2020;3(3):216–231.
11. de Graaf R, Kessler RC, Fayyad J, et al. The prevalence and effects of adult attention-deficit/hyperactivity disorder (ADHD) on the performance of workers: results from the WHO world mental health survey initiative. Occup Environ Med. 2008;65(12):835–842. doi:10.1136/oem.2007.038448
12. Fayyad J, Sampson NA, Hwang I, et al. The descriptive epidemiology of DSM-IV adult ADHD in the world health organization world mental health surveys. Atten Defic Hyperact Disord. 2017;9(1):47–65. doi:10.1007/s12402-016-0208-3
13. Mirza H, Al-Huseini S, Al-Jamoodi S, et al. Socio-demographic and clinical profiles of adult attention deficit hyperactivity disorder patients in a university hospital in Oman. Sultan Qaboos Univ Med J. 2022;22(2):206–211. doi:10.18295/squmj.5.2021.104
14. Simon V, Czobor P, Balint S, Meszaros A, Bitter I. Prevalence and correlates of adult attention-deficit hyperactivity disorder: meta-analysis. Br J Psychiatry. 2009;194(3):204–211. doi:10.1192/bjp.bp.107.048827
15. Kupper T, Haavik J, Drexler H, et al. The negative impact of attention-deficit/hyperactivity disorder on occupational health in adults and adolescents. Int Arch Occup Environ Health. 2012;85(8):837–847. doi:10.1007/s00420-012-0794-0
16. Gjervan B, Torgersen T, Nordahl HM, Rasmussen K. Functional impairment and occupational outcome in adults with ADHD. J Atten Disord. 2012;16(7):544–552. doi:10.1177/1087054711413074
17. Halmoy A, Fasmer OB, Gillberg C, Haavik J. Occupational outcome in adult ADHD: impact of symptom profile, comorbid psychiatric problems, and treatment: a cross-sectional study of 414 clinically diagnosed adult ADHD patients. J Atten Disord. 2009;13(2):175–187. doi:10.1177/1087054708329777
18. Kessler RC, Lane M, Stang PE, Van Brunt DL. The prevalence and workplace costs of adult attention deficit hyperactivity disorder in a large manufacturing firm. Psychol Med. 2009;39(1):137–147. doi:10.1017/S0033291708003309
19. Nigg JT. Attention-deficit/hyperactivity disorder and adverse health outcomes. Clin Psychol Rev. 2013;33(2):215–228. doi:10.1016/j.cpr.2012.11.005
20. Weissenberger S, Ptacek R, Vnukova M, et al. ADHD and lifestyle habits in Czech adults, a national sample. Neuropsychiatr Dis Treat. 2018;14:293–299. doi:10.2147/NDT.S148921
21. Yan S, Cao H, Gu C, et al. Dietary patterns are associated with attention-deficit/hyperactivity disorder (ADHD) symptoms among preschoolers in mainland China. Eur J Clin Nutr. 2018;72(11):1517–1523. doi:10.1038/s41430-018-0131-0
22. Hartmann AS, Rief W, Hilbert A. Laboratory snack food intake, negative mood, and impulsivity in youth with ADHD symptoms and episodes of loss of control eating. Where is the missing link? Appetite. 2012;58(2):672–678. doi:10.1016/j.appet.2012.01.006
23. Yoon SY, Jain U, Shapiro C. Sleep in attention-deficit/hyperactivity disorder in children and adults: past, present, and future. Sleep Med Rev. 2012;16(4):371–388. doi:10.1016/j.smrv.2011.07.001
24. Hvolby A. Associations of sleep disturbance with ADHD: implications for treatment. Atten Defic Hyperact Disord. 2015;7(1):1–18. doi:10.1007/s12402-014-0151-0
25. Duarte CS, Monk C, Weissman MM, Posner J. Intergenerational psychiatry: a new look at a powerful perspective. World Psychiatry. 2020;19(2):175–176. doi:10.1002/wps.20733
26. Bush NR, Wakschlag LS, LeWinn KZ, et al. Family environment, neurodevelopmental risk, and the Environmental Influences on Child Health Outcomes (ECHO) initiative: looking back and moving forward. Front Psychiatry. 2020;11:547. doi:10.3389/fpsyt.2020.00547
27. Suzuki T, Wada K, Nakazato M, et al. Depressive symptoms in workers with high autistic trait scores according to job stress type. Ind Health. 2022;60(6):578–588. doi:10.2486/indhealth.2021-0253
28. Kessler RC, Adler L, Ames M, et al. The World Health Organization adult ADHD Self-Report Scale (ASRS): a short screening scale for use in the general population. Psychol Med. 2005;35(2):245–256. doi:10.1017/S0033291704002892
29. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders.
30. Iwanami A. Depression and Developmental Disabilities. Seishun Publishing Co.,Ltd.; 2019.
31. Ustun B, Adler LA, Rudin C, et al. The World Health Organization adult attention-deficit/hyperactivity disorder self-report screening scale for DSM-5. JAMA Psychiatry. 2017;74(5):520–527. doi:10.1001/jamapsychiatry.2017.0298
32. Kessler R. To: users of the ASRS screening scale. In: Updates Based on the DSM-5 Version of the Screening Scale. Harvard Medical School; 2017. Available from: https://www.hcp.med.harvard.edu/ncs/ftpdir/adhd/ASRS-5_Guidelines_2-23-2018.pdf.
33. Fredriksen M, Dahl AA, Martinsen EW, Klungsoyr O, Faraone SV, Peleikis DE. Childhood and persistent ADHD symptoms associated with educational failure and long-term occupational disability in adult ADHD. Atten Defic Hyperact Disord. 2014;6(2):87–99. doi:10.1007/s12402-014-0126-1
34. Riboldi I, Crocamo C, Callovini T, et al. Testing the impact of depressive and anxiety features on the association between attention-deficit/hyperactivity disorder symptoms and academic performance among university students: a mediation analysis. Brain Sci. 2022;12:9. doi:10.3390/brainsci12091155
35. Tong L, Shi H, Li X. Associations among ADHD, abnormal eating and overweight in a non-clinical sample of Asian children. Sci Rep. 2017;7(1):2844. doi:10.1038/s41598-017-03074-4
36. Cortese S, Moreira-Maia CR, St Fleur D, Morcillo-Penalver C, Rohde LA, Faraone SV. Association between ADHD and obesity: a systematic review and meta-analysis. Am J Psychiatry. 2016;173(1):34–43. doi:10.1176/appi.ajp.2015.15020266
37. Nigg JT, Johnstone JM, Musser ED, Long HG, Willoughby MT, Shannon J. Attention-deficit/hyperactivity disorder (ADHD) and being overweight/obesity: new data and meta-analysis. Clin Psychol Rev. 2016;43:67–79. doi:10.1016/j.cpr.2015.11.005
38. Hysing M, Lundervold AJ, Posserud MB, Sivertsen B. Association between sleep problems and symptoms of attention deficit hyperactivity disorder in adolescence: results from a large population-based study. Behav Sleep Med. 2016;14(5):550–564. doi:10.1080/15402002.2015.1048448
39. Gradisar M, Gardner G, Dohnt H. Recent worldwide sleep patterns and problems during adolescence: a review and meta-analysis of age, region, and sleep. Sleep Med. 2011;12(2):110–118. doi:10.1016/j.sleep.2010.11.008
40. Brevik EJ, Lundervold AJ, Halmoy A, et al. Prevalence and clinical correlates of insomnia in adults with attention-deficit hyperactivity disorder. Acta Psychiatr Scand. 2017;136(2):220–227. doi:10.1111/acps.12756
41. Van Veen MM, Kooij JJ, Boonstra AM, Gordijn MC, Van Someren EJ. Delayed circadian rhythm in adults with attention-deficit/hyperactivity disorder and chronic sleep-onset insomnia. Biol Psychiatry. 2010;67(11):1091–1096. doi:10.1016/j.biopsych.2009.12.032
42. van Andel E, Bijlenga D, Vogel SWN, Beekman ATF, Kooij JJS. Effects of chronotherapy on circadian rhythm and ADHD symptoms in adults with attention-deficit/hyperactivity disorder and delayed sleep phase syndrome: a randomized clinical trial. Chronobiol Int. 2021;38(2):260–269. doi:10.1080/07420528.2020.1835943
43. Valsecchi P, Nibbio G, Rosa J, Vita A. Adult ADHD and sleep disorders: prevalence, severity and predictors of sleep disorders in a sample of Italian psychiatric outpatients. Psychiatry Res. 2022;310:114447. doi:10.1016/j.psychres.2022.114447
44. Garcia M, Rouchy E, Galera C, Tzourio C, Michel G. The relation between ADHD symptoms, perceived stress and binge drinking in college students. Psychiatry Res. 2020;284:112689. doi:10.1016/j.psychres.2019.112689
45. McClernon FJ, Kollins SH, Lutz AM, et al. Effects of smoking abstinence on adult smokers with and without attention deficit hyperactivity disorder: results of a preliminary study. Psychopharmacology. 2008;197(1):95–105. doi:10.1007/s00213-007-1009-3
46. Den Heijer AE, Groen Y, Tucha L, et al. Sweat it out? The effects of physical exercise on cognition and behavior in children and adults with ADHD: a systematic literature review. J Neural Transm. 2017;124(Suppl 1):3–26. doi:10.1007/s00702-016-1593-7
47. Wilens TE, Biederman J, Faraone SV, Martelon M, Westerberg D, Spencer TJ. Presenting ADHD symptoms, subtypes, and comorbid disorders in clinically referred adults with ADHD. J Clin Psychiatry. 2009;70(11):1557–1562. doi:10.4088/JCP.08m04785pur
48. Millstein R, Wilens T, Biederman J, Spencer T. Presenting ADHD symptoms and subtypes in clinically referred adults with ADHD. J Affect Disord. 1997;2:159–166.
49. Das D, Cherbuin N, Butterworth P, Anstey KJ, Easteal S. A population-based study of attention deficit/hyperactivity disorder symptoms and associated impairment in middle-aged adults. PLoS One. 2012;7(2):e31500. doi:10.1371/journal.pone.0031500
50. Kwon SJ, Kim Y, Kwak Y. Difficulties faced by university students with self-reported symptoms of attention-deficit hyperactivity disorder: a qualitative study. Child Adolesc Psychiatry Ment Health. 2018;12:12. doi:10.1186/s13034-018-0218-3
51. Meaux JB, Green A, Broussard L. ADHD in the college student: a block in the road. J Psychiatr Ment Health Nurs. 2009;16(3):248–256. doi:10.1111/j.1365-2850.2008.01349.x
52. Posner J, Biezonski D, Pieper S, Duarte CS. Genetic studies of mental illness: are children being left behind? J Am Acad Child Adolesc Psychiatry. 2021;60(6):672–674. doi:10.1016/j.jaac.2020.12.031
53. Barkley RA, Fischer M, Smallish L, Fletcher K. The persistence of attention-deficit/hyperactivity disorder into young adulthood as a function of reporting source and definition of disorder. J Abnorm Psychol. 2002;111(2):279–289. doi:10.1037/0021-843X.111.2.279
54. Murphy P, Schachar R. Use of self-ratings in the assessment of symptoms of attention deficit hyperactivity disorder in adults. Am J Psychiatry. 2000;157(7):1156–1159. doi:10.1176/appi.ajp.157.7.1156
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Cardiovascular Disease in China: Socioeconomic Status Variation in Prevalence
Zhang C, Shen Y, Wang A, Wang D, Cao L, Yue W
Risk Management and Healthcare Policy 2023, 16:2077-2084
Published Date: 9 October 2023
Socioeconomic Status Related to Prescription of Triple Therapy and Anticholinergic Monotherapy in Patients with Chronic Obstructive Pulmonary Disease (COPD) in Sweden - A Retrospective National Registry Study
Larsson K, Betnér S, Fuchs B, Vanfleteren LEGW, Stridsman C
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:3597-3606
Published Date: 7 November 2025