Back to Journals » Journal of Pain Research » Volume 19
Altered Cortical Structure in Primary Dysmenorrhea: Cortical Thickness Mediates the Association Between Estradiol and Pain Catastrophizing
Authors Liu H, Xu X, Gan H, Chen Y, Chi X, Lu T, Shang M, Zhu Y, Dun W, Zhang M
Received 3 March 2026
Accepted for publication 23 June 2026
Published 9 July 2026 Volume 2026:19 606502
DOI https://doi.org/10.2147/JPR.S606502
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Rocío de la Vega
Huiping Liu,1,2 Xinyu Xu,3,4 Huiyan Gan,3 Yanran Chen,1,2 Xiaotong Chi,3 Tao Lu,1 Meiling Shang,1,2 Yi Zhu,5 Wanghuan Dun,6 Ming Zhang1
1Department of Medical Imaging, The First Affiliated Hospital of Xi’an Jiaotong University, Xi’an, Shaanxi, 710061, People’s Republic of China; 2School of Future Technology, Xi’an Jiaotong University, Xi’an, Shaanxi, 710049, People’s Republic of China; 3Health Science Center, Xi’an Jiaotong University, Xi’an, Shaanxi, 710049, People’s Republic of China; 4Department of Occupational and Environmental Health, School of Public Health, Health Science Center, Xi’an Jiaotong University, Xi’an, Shaanxi, 710049, People’s Republic of China; 5Department of Clinical and Technical Support, Philips, Beijing, People’s Republic of China; 6Rehabilitation Medicine Department, The First Affiliated Hospital of Xi’an Jiaotong University, Xi’an, Shaanxi, 710061, People’s Republic of China
Correspondence: Wanghuan Dun, Rehabilitation Medicine Department, The First Affiliated Hospital of Xi’an Jiaotong University, Xi’an, Shaanxi, 710061, People’s Republic of China, Tel +(86) 18092706568, Email [email protected] Ming Zhang, Department of Medical Imaging, the First Affiliated Hospital of Xi’an Jiaotong University, Xi’an, Shaanxi, 710061, People’s Republic of China, Tel +(86) 18991232265, Email [email protected]
Background: Primary dysmenorrhea (PDM), as a form of chronic pelvic pain, has a complex pathophysiology involving hormonal factors, central nervous system alterations, and maladaptive pain cognition. Previous neuroimaging studies have demonstrated structural brain alterations in patients with PDM. However, the relationships among hormone levels, brain structural changes, and pain catastrophizing remain poorly understood. This study aimed to investigate brain structural alterations and their associations with estradiol (E2) levels and pain catastrophizing in patients with PDM.
Methods: T1-weighted MRI scans and E2 sampling were acquired during the menstrual phase from 45 patients with PDM and 44 age-matched healthy controls. Cortical thickness, volume, and folding were compared using a general linear model. Among the regions showing significant group differences, mediation analyses focused specifically on the right postcentral gyrus to examine whether its cortical thickness mediated the relationship between E2 levels and Pain Catastrophizing Scale (PCS) magnification scores in patients with PDM. The McGill Pain Questionnaire (MPQ) was used to measure the quality and intensity of menstrual pain.
Results: The PDM group scored significantly higher on the MPQ and PCS, suggesting greater pain perception and psychologic distress. Patients with PDM exhibited alterations in cortical thickness, volume, and folding within specific brain regions. Notably, the cingulate cortex, orbitofrontal cortex, and postcentral gyrus demonstrated substantial changes. Mediation analysis revealed that E2 levels were positively correlated with PCS magnification scores (r = 0.342, p = 0.023), and this relationship was fully mediated by cortical thickness of the right postcentral gyrus (indirect effect = 0.045, p < 0.001).
Conclusion: This study identified brain structural alterations during the menstrual phase in patients with PDM and further found that cortical thickness of the right postcentral gyrus mediated the relationship between estradiol levels and pain magnification. These findings provide new insights into the complex mechanisms underlying PDM.
Keywords: brain structure, chronic pain, estradiol, pain catastrophizing, primary dysmenorrhea
Introduction
Primary dysmenorrhea (PDM) is defined as recurrent, cramping lower abdominal pain occurring during menstruation in the absence of any discernible macroscopic pelvic pathology, affecting up to 90% of women.1–4 PDM often accompanied by symptoms such as vomiting, headache, and fatigue, which affects women’s quality of life and imposes a substantial socioeconomic burden.5,6 The Chinese government has incorporated women’s reproductive health into national public health strategies and implemented policies to improve healthcare access and occupational protection for women with menstrual disorders.7,8 The pathophysiology of PDM is complex and involves the central nervous system, hormonal regulation, psychological factors, and emotional processes.2,4,9 Persistent nociceptive input to the central nervous system may lead to both functional and structural brain alterations, including central sensitization to pain.5,10–13 Previous studies suggest that continuous pain signals can induce maladaptive brain adaptations, leading to measurable structural14 and functional15,16 changes over time. Liu et al17 reported alterations in gray matter volume, cortical thickness, and white matter integrity in pain-related regions, including the prefrontal cortex, insula, and thalamus. Another study identified reduced gray matter volume in the right superior temporal gyrus and decreased thickness in the orbitofrontal cortex, postcentral gyrus, and superior occipital gyrus, along with altered functional connectivity (FC) in related regions.13 These findings highlight the impact of PDM on brain structure and function, particularly in regions involved in pain perception, emotional regulation, and cognitive control.18 Moreover, abnormalities in these structures and in FC are closely associated with PDM duration, pain severity, and onset age of PDM.13,17 However, previous studies have predominantly been conducted at the voxel level.
As a primary regulator of the menstrual cycle, hormone levels have been notably associated with increased amygdala volume in patients with PDM.19 Additionally, fluctuations in estradiol (E2) levels throughout the menstrual cycle may affect the endometrial lining and uterine contractility, thereby affecting pain perception in PDM.20 E2 has been reported to modulate dysmenorrhea symptoms,21 suggesting a link between PDM and hormonal regulation. Notably, E2 also influences brain activity. Higher E2 levels are associated with reduced limbic deactivation during psychosocial stress.22 Furthermore, previous studies have shown that E2 administration not only increases hippocampal gray matter volume23 but also affects effective connectivity within emotional processing networks.24
Anti-GABAergic effects of E2 have been observed in the rat cortex25 and hypothalamus,26 with reports suggesting that this effect may be mediated through a depressant effect on GABAergic transmission.27 Sustaining E2 levels after menopause may also help prevent stress-related neural and cognitive decline.28 This dual role of estradiol suggests that the relationship between E2 and pain in PDM may be complex, potentially involving neural mechanisms besides direct physiologic effects on the uterus. Previous studies have examined brain structural alterations and hormonal changes in PDM.19 Furthermore, the mediating role of brain structure between hormonal fluctuations and psychological outcomes has increasingly become a focus of investigation. For instance, recent research demonstrates that individual variability in E2 is significantly associated with altered cortical thickness in emotion-processing regions, and further examined whether brain structure mediated the association between E2 variability and internalizing symptoms.29 The bivariate approaches cannot clarify whether brain structure mediates the relationship between E2 levels and pain‑related psychological outcomes. Mediation analysis provides a statistical framework to examine whether cortical structural measures may partly account for the association between E2 levels and pain catastrophizing. Therefore, by integrating neuroimaging data, hormonal profiles, and clinical assessments, this study aimed to characterize abnormal brain structural alterations in patients with PDM and investigate whether specific cortical structures mediate the relationship between E2 levels and pain catastrophizing. To achieve a more comprehensive characterization of cortical morphologic alterations in PDM, we employed the FreeSurfer-based analysis approach, which enables detailed quantification of cortical thickness, surface area, and folding.30 We hypothesized that brain structural alterations are associated with E2 levels and pain catastrophizing in patients with PDM.
Materials and Methods
Participants
Potential participants were recruited from Xi’an Jiaotong University and surrounding schools between 2018 and 2022. They were initially screened through clinical interviews and gynecological history assessments conducted by clinicians at the First Affiliated Hospital of Xi’an Jiaotong University. All participants underwent structural MRI examinations. Pelvic MRI scans were reviewed to explicitly exclude organic gynecologic diseases, including endometriosis, adenomyosis, and uterine fibroids. Brain MRI scans were evaluated to rule out any structural neurologic abnormalities. The inclusion criteria for the PDM group were as follows: (1) meeting the clinical diagnostic criteria for primary dysmenorrhea as defined by the American College of Obstetricians and Gynecologists, characterized by cyclic lower abdominal pain during menstruation in the absence of identifiable pelvic pathology; (2) regular menstrual cycles lasting between 27 and 32 days (to control for neuroendocrine variability during MRI scanning);9,31–33 and (3) an average menstrual pain intensity score of ≥ 4 over the past 6 months, assessed using a visual analog scale (VAS; 0 = no pain, 10 = worst pain), indicating at least moderate pain severity.
The exclusion criteria were as follows: (1) organic brain or pelvic disorders detected by MRI; (2) use of oral contraceptives, hormonal supplements, Chinese herbal medicine, or any centrally acting medications (eg., opioids or antiepileptics) within the past 6 months; (3) a history of chronic illness, including other comorbid chronic pain conditions (eg., tension-type headache or fibromyalgia), neurologic or psychiatric disorders, or left-handedness; (4) presence of metal implants or a pacemaker; (5) pregnancy or plans for pregnancy in the near future; (6) alcoholism or substance abuse; and (7) claustrophobia. Participants were instructed to refrain from using painkillers for 24 hours prior to the study.
MRI scans were conducted during the first two days (Day 1–2) of the menstrual phase, synchronized with blood sample collection. Participants were excluded if they had used hormonal contraceptives or other hormone-related medications within the previous 6 months. Participants were also instructed to avoid alcohol, caffeine, and strenuous exercise before MRI scanning and blood collection. A total of 121 adults [58 healthy controls (HCs) and 63 patients with PDM] recruited from local colleges or universities met the inclusion criteria and underwent MRI scanning. The average intensity of menstrual pain during the current cycle was assessed on the last day of the menstrual phase using the McGill Pain Questionnaire (MPQ).34 All questionnaires [MPQ, Pain Catastrophizing Scale (PCS), Self-Rating Anxiety Scale (SAS), and Self-Rating Depression Scale (SDS)] were administered on the same day. For the PCS, participants were instructed to rate their thoughts and feelings specifically related to their menstrual experience during the current cycle. Participants’ anxiety was assessed using the SAS, which consists of 20 items rated on a 4-point Likert scale (1 = “hardly ever,” 2 = “sometimes,” 3 = “most of the time,” and 4 = “almost all of the time”).35 Participants’ depressive symptoms were assessed using the SDS, which also consists of multiple items scored similarly to the SAS.36,37 Higher scores on these scales indicate greater pain intensity, anxiety, and depressive symptoms. Pain catastrophizing, defined as an “exaggerated negative psychologic response to actual or anticipated pain,” including rumination, magnification, and helplessness, was assessed using the PCS.38
Written informed consent was obtained from all participants. The study was approved by the Ethics Review Committee of the First Affiliated Hospital of Xi’an Jiaotong University (approval number: 2017–0154) and was conducted in accordance with the Declaration of Helsinki.
Sample Size Estimation
An a priori statistical power analysis was conducted using G*Power software (version 3.1.9.7) to determine the appropriate sample size. Given that the non-normal distribution of our primary clinical and neuroimaging metrics was verified via the Shapiro–Wilk test, the non-parametric Wilcoxon-Mann–Whitney U-test was selected for between-group comparisons. Regarding the parameter settings, we established a Type I error rate of 0.05, a statistical power (1-β) of 0.80, and a 1:1 allocation ratio. We anticipated a medium-to-large effect size (Cohen’s d = 0.65) based on previously published structural neuroimaging studies in patients with PDM.17 By applying the conservative Asymptotic Relative Efficiency (ARE ≈ 0.955) adjustment for continuous data, the G*Power calculation yielded a minimum theoretical requirement of 80 valid participants (40 per group) for between-group comparisons. For the exploratory mediation analysis, sample size adequacy was further evaluated with reference to previous methodological literature on sample size requirements for detecting mediated effects. The simulation-based study estimated the sample sizes required to achieve 80% statistical power for detecting mediated effects under different combinations of path coefficients and statistical testing methods. For a medium-sized mediation effect, their results suggest that approximately 71–74 participants are required when using recommended approaches such as the bias-corrected bootstrap method.39 The final sample size of the present study (N = 89) exceeded this recommended range and was considered adequate for the planned exploratory mediation analysis of a medium-sized indirect effect.
Serologic Sampling
Serum samples were collected in strict accordance with ethical guidelines. Prior to collection, participants received detailed explanations to ensure full understanding of the study objectives and procedures. Approximately 5 mL of venous blood was drawn from the antecubital vein under aseptic conditions. Serum was separated by centrifugation at 3000 rpm for 10 minutes at 4°C and stored at −80°C until analysis. Serum estradiol levels were quantified using an automated chemiluminescence immunoassay system in the hospital’s certified clinical laboratory. The assay was performed according to standard operating procedures using clinical-grade diagnostic reagents. To ensure analytical reliability, the detection system was subject to rigorous internal quality control and periodic external quality assessment. All laboratory personnel were blinded to the clinical status of the participants.
Structural MRI Data Acquisition
MRI scans were performed during the menstrual phase at the Department of Medical Imaging, the First Affiliated Hospital of Xi’an Jiaotong University. Image data were acquired using a 3.0-T MRI scanner (GE SIGNA HDxt, WI, USA) equipped with an 8-channel phased-array head coil. For each participant, a high-resolution T1-weighted anatomical scan was obtained with the following parameters: echo time (TE) = 2.6 milliseconds, repetition time (TR) = 1900 milliseconds, flip angle = 15°, 140 slices, slice thickness = 1 mm, voxel size = 1 × 1×1 mm3, and field of view = 256×256 mm2.
MRI Preprocessing
Surface-based morphometric measures, including cortical thickness, cortical volume, and cortical folding, were obtained using FreeSurfer v6.0.0 (https://surfer.nmr.mgh.harvard.edu/).40,41 Preprocessing steps included motion correction and image averaging, removal of non-brain tissue, automated Talairach transformation, segmentation of subcortical white matter and deep gray matter volumetric structures, intensity normalization, tessellation of the gray–white matter boundary, automated topology correction, and surface deformation along intensity gradients to precisely demarcate gray–white and gray–cerebrospinal fluid boundaries, defined by the greatest intensity shift between tissue classes.42 Further data processing included surface inflation, registration to a spherical atlas based on individual cortical folding patterns to align cortical geometry across participants, and parcellation of the cerebral cortex into automatically defined units according to gyral and sulcal structures. The extracted measurements included cortical thickness, volume, and folding estimates for the 34 cortical regions per hemisphere (68 total) as defined by the Desikan-Killiany atlas.43 All reconstructed pial and white matter surfaces were visually inspected to identify potential artifacts. Only participants with accurate surface reconstructions and no visible artifacts were included in the final statistical analyses.44,45
Statistical Analysis
For demographic and clinical variables, independent 2-tailed t tests were used to compare patients with PDM and HCs [or Mann–Whitney U-tests if normality assumptions were violated; assessed by (Shapiro–Wilk/visual inspection)], with P values adjusted using false discovery rate (FDR) correction. The threshold for statistical significance was set at p < 0.05 for all analyses. Statistical analyses were performed using R version 4.4.1. Group differences in regional cortical thickness, volume, and folding were tested using general linear models with the cortical metric as the dependent variable and group (PDM vs HC) as the primary independent variable, controlling for age, intracranial volume, SDS, and SAS. First, empirical p-values at each vertex/voxel were derived through Monte Carlo permutation tests (5000 iterations).46 Subsequently, multiple comparisons across all vertices/voxels were corrected by applying the Benjamini-Hochberg procedure, controlling the false discovery rate (FDR) at a threshold of 0.05. For data visualization, statistically significant differences were plotted in R (version 4.4.1) using the “ggseg” package. Effect sizes were calculated using Cohen’s d.
To further explore the relationship among cortical structural abnormalities, serum E2 levels, and clinical scale assessments, we performed a stepwise correlation analysis. First, Spearman correlation analyses were conducted between serum E2 levels and all brain structural metrics showing significant between-group differences. Second, brain structural metrics that were significantly correlated with serum E2 levels were further correlated with clinical scale scores. Finally, only brain structural metrics that showed significant associations with both serum E2 levels and clinical scale assessments were entered into the subsequent mediation analysis as candidate mediators. Statistical significance was set at p < 0.05, with Bonferroni correction applied for multiple correlation analyses.
Based on this stepwise selection procedure, cortical thickness of the right postcentral gyrus was identified as the candidate mediator and was further examined in the mediation analysis. A regression-based framework was applied: (1) PCS scores were regressed on E2 levels (total effect, c path); (2) right postcentral gyrus thickness was regressed on E2 levels (a path); and (3) PCS scores were regressed on both E2 levels and cortical thickness (b and c paths). The significance of the indirect effect (a × b) was estimated using a bootstrapping procedure (based on the product-of-coefficients method) with 5,000 resamples to derive bias-corrected 95% confidence intervals (CIs).47 If the 95% CI did not contain zero, the mediation effect was considered statistically significant. Age, intracranial volume, and SAS and SDS scores were included as covariates in all mediation models.
Sensitivity analyses were conducted to verify the robustness of the observed correlations and mediation effects within the PDM group (n = 45). Influential data points were identified using Cook’s distance, with a threshold defined as D > 4/n (D > 0.089). Three participants exceeding this threshold were excluded to determine whether the primary results were driven by extreme values.
Results
Demographic and Clinical Characteristics
The final analysis included 45 patients with PDM and 44 HCs, after excluding 32 individuals because of blood sample loss or contamination (n = 28), primarily caused by delayed freezing (> 2 hours) or freezer malfunction leading to improper storage temperatures, and incomplete pain scale responses (n = 4). The demographic and clinical characteristics of both groups are summarized in Table 1. No significant differences were observed in age between the two groups (p = 0.197). The MPQ scores were significantly higher in the PDM group, with significant differences in MPQ sensory scores (p < 0.001, q < 0.001), MPQ affective scores (p < 0.001, q < 0.001), and MPQ total pain scores (p < 0.001, q < 0.001). The PDM group also demonstrated significantly higher PCS subscale scores [including rumination (p < 0.001, q < 0.001), magnification (p < 0.001, q < 0.001), and helplessness (p < 0.001, q < 0.001)] and a higher PCS total score (p < 0.001, q < 0.001). In addition, significant differences were observed in the SAS (p < 0.001, q < 0.001) and SDS (p < 0.001, q < 0.001) scores. Serum E2 levels were also significantly elevated in patients with PDM (p = 0.039, q = 0.041).
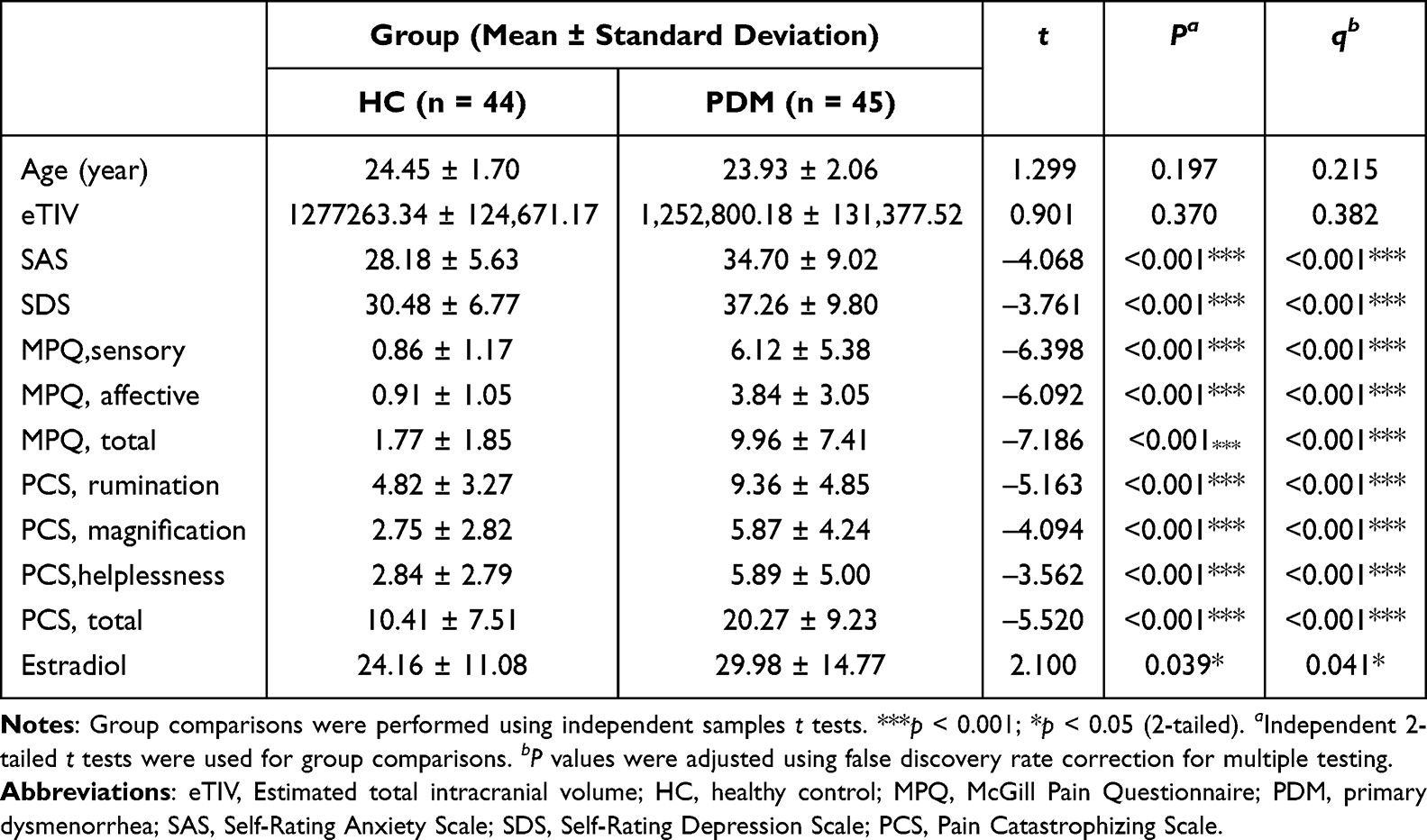 |
Table 1 Demographic and Clinical Characteristics of Healthy Controls and Patients with PDM |
Cortical Morphology
No statistically significant differences in total cortical thickness were observed between the two groups. Compared with HCs, patients with PDM exhibited increased cortical thickness in the right isthmus cingulate cortex (PFDR = 0.009, Cohen’s d = 0.503), right postcentral gyrus (PFDR = 0.031, Cohen’s d = 0.600), and right rostral middle frontal gyrus (PFDR = 0.005, Cohen’s d = 0.430) (Figure 1 and Table 2). With respect to cortical volume, patients with PDM demonstrated reduced volumes in the left posterior cingulate gyrus (PFDR = 0.032, Cohen’s d = −0.346) and left postcentral gyrus (PFDR = 0.042, Cohen’s d = −0.387), whereas increased volumes were observed in the right superior temporal gyrus (PFDR = 0.033, Cohen’s d = 0.288) and right lateral orbitofrontal cortex (PFDR = 0.002, Cohen’s d = 0.319) (Figure 2 and Table 2). Additionally, patients with PDM exhibited increased cortical folding in the right lateral orbitofrontal cortex (PFDR < 0.001, Cohen’s d = 1.172) and right posterior cingulate cortex (PFDR = 0.003, Cohen’s d = 0.305). In contrast, decreased folding was observed in the right rostral anterior cingulate cortex (PFDR < 0.001, Cohen’s d = −1.093) (Figure 3 and Table 2). Detailed results for all regional cortical thickness, volume, and folding measures are provided in Supplementary Tables 1–3.
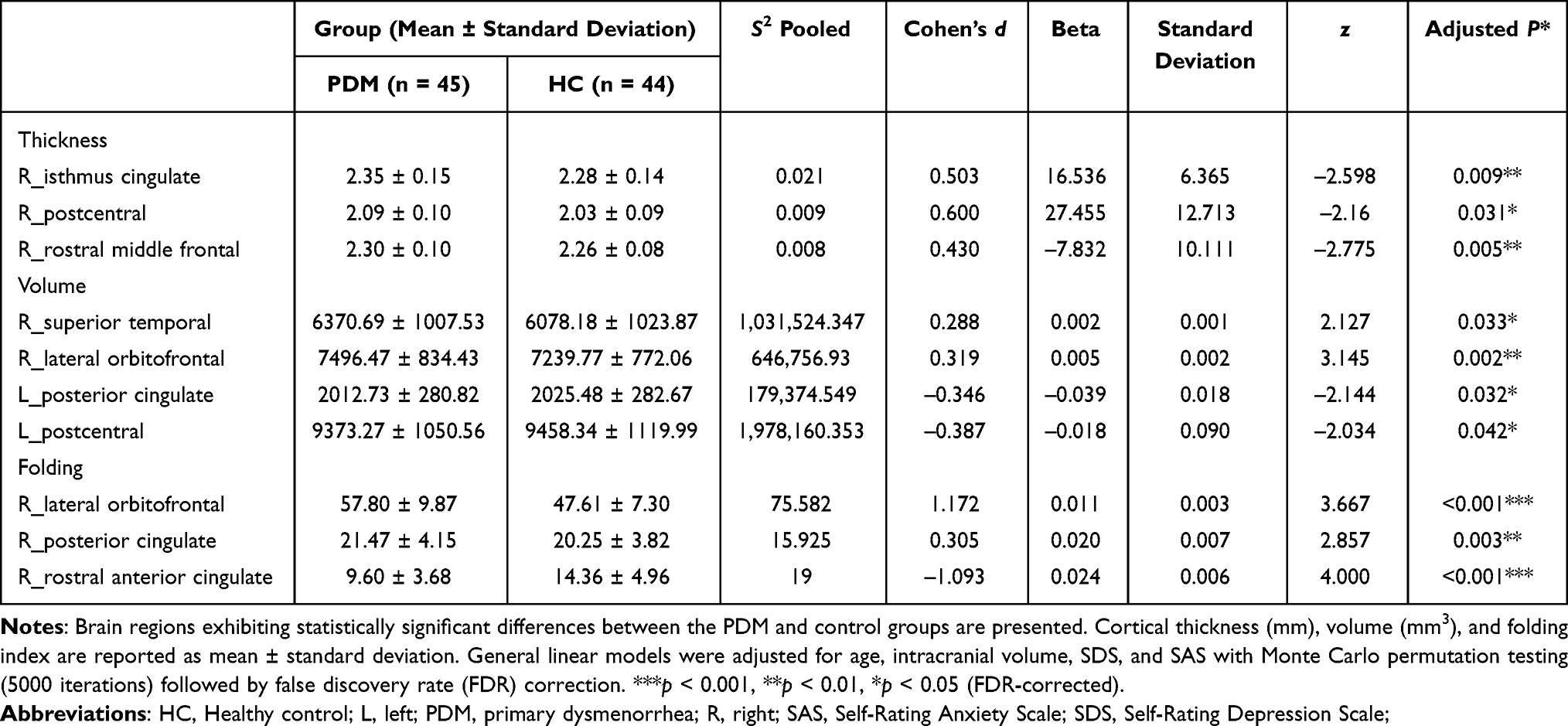 |
Table 2 Differences in Cortical Measurements (Volume, Cortical Thickness, and Folding) Between Healthy Controls and Patients with PDM |
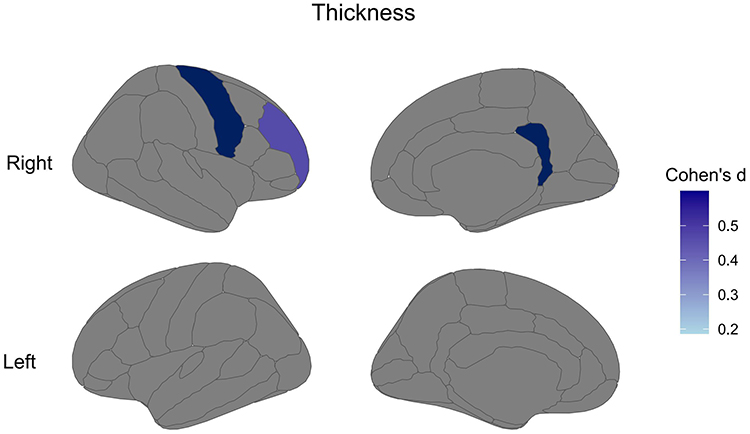 |
Figure 1 Brain regions displaying cortical thickness differences (FDR-adjusted p <0.05) after controlling for age, intracranial volume, SDS, and SAS as covariates. Color bars represent Cohen’s d effect sizes. The displayed regions correspond to the 68 cortical regions defined by the Desikan-Killiany atlas. Regions exhibiting marked group differences are listed in Supplementary Table 1. Abbreviations: FDR, False discovery rate; SAS, Self-Rating Anxiety Scale; SDS, Self-Rating Depression Scale. |
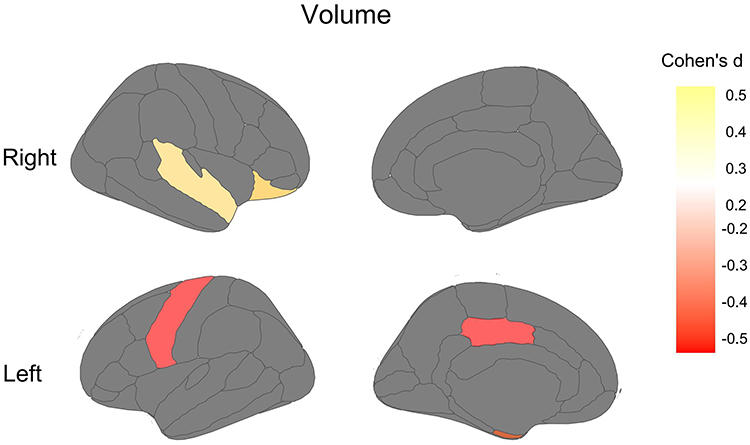 |
Figure 2 Brain regions displaying cortical volume differences (FDR-adjusted p <0.05) after controlling for age, intracranial volume, SDS, and SAS as covariates. Color bars represent Cohen’s d effect sizes. The displayed regions correspond to the 68 cortical regions defined by the Desikan-Killiany atlas. Regions exhibiting marked group differences are listed in Supplementary Table 2. Abbreviations: FDR, False discovery rate; SAS, Self-Rating Anxiety Scale; SDS, Self-Rating Depression Scale. |
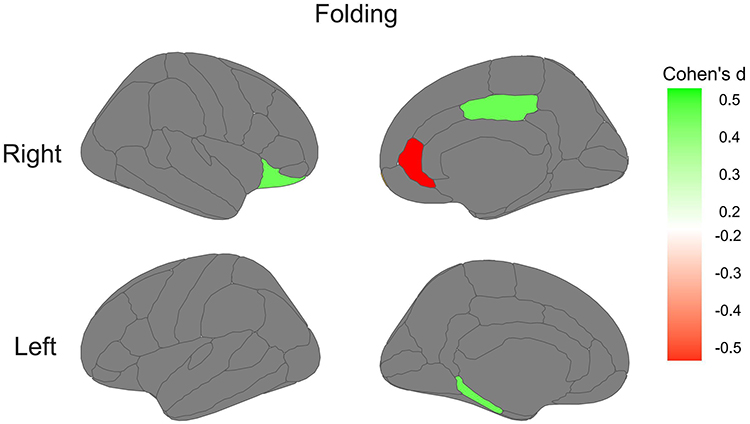 |
Figure 3 Brain regions displaying cortical folding differences (FDR-adjusted p < 0.05) after controlling for age, intracranial volume, SDS, and SAS as covariates. Color bars represent Cohen’s d effect sizes. The displayed regions correspond to the 68 cortical regions defined by the Desikan-Killiany atlas. Regions exhibiting marked group differences are listed in Supplementary Table 3. |
Correlations Among E2 Levels, Cortical Morphology, and Pain Catastrophizing
Initial inspection of the correlation matrix in patients with PDM (Supplementary Table 4) indicated that, among the PCS subcomponents, only magnification revealed a statistically significant correlation with E2 levels. Significant correlations were observed between E2 levels and PCS magnification scores (r = 0.342, P = 0.023; Supplementary Figure 1A), as well as between cortical thickness of the right postcentral gyrus and PCS magnification scores (r = 0.307, P = 0.042; Supplementary Figure 1B). Other PCS subcomponents, including rumination and helplessness, were not statistically significantly correlated with E2 levels. Among all brain metrics with significant group differences, only the cortical thickness of the right postcentral gyrus was significantly correlated with E2 levels (Supplementary Table 6). Notably, cortical thickness of the right postcentral gyrus was also significantly positively correlated with E2 levels (r = 0.415, P = 0.007; Supplementary Figure 1C). In the HC group, none of these correlations reached statistical significance (all P> 0.05; Supplementary Table 5).
Right Postcentral Gyrus Thickness Mediates the Relationship Between E2 Levels and PCS Magnification
Mediation analysis was conducted using standardized variables to examine whether right postcentral gyrus cortical thickness mediated the relationship between E2 levels and PCS magnification scores. The results demonstrated a notable mediating effect of right postcentral gyrus cortical thickness, with a standardized indirect effect of β = 0.045 (95% CI: 0.004–0.105; P < 0.001). Specifically, the effect of E2 on right postcentral gyrus cortical thickness was statistically significant (βa = 0.215, 95% CI: 0.046–0.384; P = 0.013), and the effect of right postcentral gyrus cortical thickness on PCS magnification scores was also statistically significant (βb = 0.210, 95% CI: 0.036–0.384; P = 0.018). However, no significant direct effect of E2 levels on PCS magnification scores was observed (Direct effect: β = 0.065; 95% CI: –0.026 to 0.156; P = 0.162). These findings highlight the critical mediating role of the right postcentral gyrus cortical thickness in the relationship between E2 levels and PCS magnification (Figure 4).
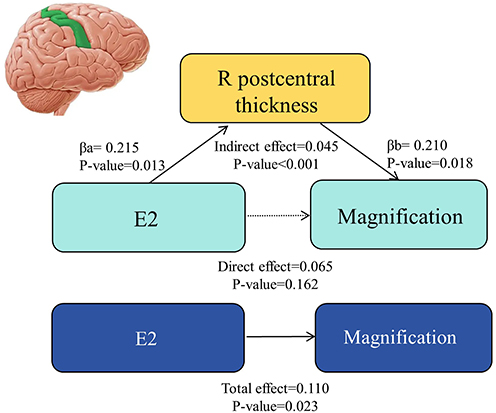 |
Figure 4 Mediation model of estradiol on magnification via right postcentral gyrus cortical thickness. Path coefficients show the relationship between estradiol levels and pain magnification scores mediated by right postcentral gyrus cortical thickness. Solid lines represent significant pathways (βa = 0.215, P = 0.013; βb = 0.210, p = 0.018). Dashed line indicates non-significant direct effect (β = 0.065, p = 0.162). The significant indirect effect (β = 0.045, p<0.001) and total effect (β = 0.110, p = 0.023) suggest mediation. All analyses controlled for age, anxiety, and depression scores. Abbreviations: CI, confidence interval. |
Sensitivity Analysis
A sensitivity analysis was conducted by excluding outliers (identified through Cook’s distance) to assess the robustness of the primary findings. The associations between E2 levels and PCS magnification scores (original r = 0.342, without outliers r = 0.325, P = 0.015), between right postcentral gyrus cortical thickness and PCS magnification scores (original r = 0.307, without outliers r = 0.324, P = 0.028), and between E2 level and right postcentral cortical gyrus thickness (original r = 0.415, without outliers r = 0.408, P = 0.004) all remained statistically significant. Furthermore, the mediation effect through the right postcentral gyrus cortical thickness remained significant after excluding outliers (original indirect effect β = 0.045; without outliers β = 0.049, 95% CI: 0.007–0.118). These results confirm that our main findings are robust and not driven by influential observations.
Discussion and Conclusion
In this study, we employed whole-brain surface-based morphometry to investigate cerebral morphologic changes in patients with PDM compared with HCs. Additionally, mediation analyses were conducted to elucidate the relationships among E2 levels, cortical morphology, and pain-related cognition, thereby advancing the understanding of the central nervous system’s role in PDM. The findings demonstrated abnormal cortical morphology in patients with PDM, including alterations in cortical thickness, volume, and folding index. Exploratory mediation analysis further suggested an indirect statistical association among hormone levels, right postcentral gyrus cortical thickness, and pain catastrophizing. This study observed that patients with PDM exhibited multidimensional structural abnormalities in the cingulate system. Specifically, they exhibited increased cortical thickness in the right isthmus cingulate cortex, reduced cortical volume in the left posterior cingulate cortex, decreased folding index in the right rostral anterior cingulate cortex, and increased folding index in the right posterior cingulate cortex. Previous studies have indicated that the cingulate gyrus comprises distinct regions and subregions.48 The anterior cingulate is involved in emotional processing, and its functional impairment may exacerbate negative emotional experiences of pain. The posterior cingulate contributes to pain memory integration and the assessment of self-related sensations, whereas the isthmus cingulate modulates imbalances in pain-related attentional allocation. These alterations may lead to abnormal transmission of pain-related information in the default mode network (DMN), salience network, and limbic system, thereby sustaining pain chronicity.48–50 The cingulate system, through brain morphologic plasticity, plays a pivotal role in the pain cognitive–affective interaction network in patients with chronic pain and PDM.51–53 Longitudinal studies on patients with fibromyalgia have reported that the cingulate gyrus is closely related to functional dissociation among DMN nodes,54 potentially reflecting functional decline in pain memory integration and visceral sensory processing.55,56 In patients with chronic lower-back pain, dysregulated coupling within the prefrontal–limbic system57,58 further indicates impairments in emotional regulation mediated by the cingulate–amygdala pathway.59 Patients with PDM also appear to exhibit abnormal reorganization of cingulate neural circuitry. Similar to observations in other chronic pain conditions, enhanced connectivity between cingulate–somatosensory and cingulate–prefrontal cortices has been reported.60 This connectivity strength was positively correlated with disease duration and negatively correlated with pain intensity, suggesting that altered FC of the cingulate cortex may underlay pain–emotion comorbidity in PDM. In addition, the lateral orbitofrontal cortex exhibited concurrent structural changes, including volume enlargement and increased folding index, along with increased cortical thickness in the right rostral middle frontal gyrus and volume expansion in the right superior temporal gyrus. An fMRI study on patients with migraine reported abnormally elevated functional hub activity (degree centrality, DC) in the anterior cingulate cortex and superior temporal gyrus, accompanied by increased FC between these regions.61 Previous studies have emphasized the role of the cingulate gyrus in chronic pain primarily from a functional perspective. However, this study identified marked structural alterations in the cingulate gyrus and right superior temporal gyrus, providing a more comprehensive characterization of neuroplastic changes following persistent pain in patients with PDM.13,62
The orbitofrontal cortex plays a vital role in decision-making, emotion, and learning.63,64 Previous studies have reported that the orbitofrontal cortex is involved in pain modulation pathways.65 In particular, the orbitofrontal cortex shows extensive functional connectivity with multiple pain-related brain regions, including the thalamus and the anterior cingulate cortex.66,67 Experimental direct activation of glutamatergic neurons in the mouse ventrolateral orbitofrontal cortex or enhancement of glutamatergic input from the ventromedial thalamic nucleus can alleviate hypersensitivity induced by peripheral neuropathic pain.68 Moreover, changes in the connectivity strength of the orbitofrontal cortex–amygdala–hippocampus network may promote the transition from acute to chronic pain. Changes in the orbitofrontal cortex observed in patients with PDM play a remarkable role in the reprocessing and evaluation of pain-related information, influencing pain perception. The rostral anterior cingulate cortex plays a central role in higher-order cognitive regulation and emotional integration of pain.69 As a primary node in the prefrontal–limbic system, this region modulates the emotional components of pain by inhibiting excessive amygdala activation.70 Structural alterations in both the orbitofrontal cortex and the cingulate cortex in patients with PDM may reflect neuroadaptive remodeling associated with chronic menstrual pain, highlighting the important role of the prefrontal–limbic system in PDM.
Our study observed that patients with PDM exhibited notable asymmetric structural changes in the postcentral gyrus, characterized by increased cortical thickness in the right postcentral gyrus and reduced volume in the left postcentral gyrus compared with HCs. As a core component of the primary somatosensory cortex, the postcentral gyrus is critical for pain processing.71,72 A neuroimaging study indicates that structural or functional alterations in this region are associated with pain in chronic prostatitis/chronic pelvic pain conditions, playing a central integrative role in pain information processing.73 Increased right postcentral gyrus thickness may reflect neuroplastic adaptations involving synaptic mechanisms.74 In contrast, the left-hemisphere volume reduction aligns with gray matter atrophy patterns reported in chronic pain conditions,75,76 potentially reflecting impaired somatic pain integration. This hemispheric asymmetry may indicate distinct adaptations in the primary somatosensory cortex, with left-sided atrophy potentially disrupting somatic pain integration and right-sided thickening representing neuroplastic adaptations to chronic nociceptive input.71 The findings of the present study are consistent with previous research, suggesting that the postcentral gyrus is one of the key brain regions involved in abnormal brain structural alterations in patients with PDM. Moreover, the left and right postcentral gyri may reflect distinct characteristics of pain-related neuroplastic alterations in patients with PDM.
Additionally, in the present study, among the brain structural metrics showing significant between-group differences, relatively larger effect sizes were observed for cortical folding in the right rostral anterior cingulate cortex and right lateral orbitofrontal cortex, as well as cortical thickness in the right postcentral gyrus and right isthmus cingulate cortex. These findings suggest that these regions may show more pronounced structural alterations in patients with PDM and may therefore deserve particular attention in understanding the central nervous system alterations associated with PDM.
The mediation analysis suggested an indirect statistical association among E2 levels, cortical thickness of the right postcentral gyrus, and PCS magnification scores in patients with PDM. Previous studies have suggested that brain structure and function are influenced by hormonal fluctuations, with changes in E2 levels potentially leading to changes in the central nervous system, resulting in increased cortical thickness in specific brain regions.77,78 Experimental evidence also indicates that estrogen-related signaling may influence synaptic plasticity and neurotransmission, providing a possible biological context for associations between estradiol and cortical morphology.79–81 Pain catastrophizing influences psychologic experience and perception of pain, and elevated levels have been reported in patients with endometriosis.82 In the present study, patients with PDM exhibited higher PCS scores and PCS magnification scores than HCs. Previous studies have linked pain catastrophizing to resting-state brain FC and gray matter morphology,18,75,83 suggesting that pain catastrophizing may be influenced by underlying brain structure and function. Notably, the mediation was identified specifically in the PDM group but not in HCs. These results suggest that the cortical thickness of right postcentral gyrus may statistically account for part of the association between estradiol levels and pain catastrophizing in patients with PDM, and the statistical mediating role may be related to the disease-specific context of PDM. Our findings suggest that PDM may be associated with complex relationships among hormonal levels, central nervous system alterations, and pain-related cognitive processes. Therefore, future therapeutic strategies for patients with PDM may need to move beyond a single-target approach and instead integrate multiple interventions, such as endocrine regulation, central nervous system modulation, and pain-related cognitive interventions, to more effectively improve clinical symptoms.
In summary, this study highlights substantial group differences in pain catastrophizing, cortical structure, and E2 level between patients with PDM and HCs. The findings suggest statistical associations among brain structure, psychologic processes, and hormonal levels in PDM, and provide additional evidence consistent with central nervous system involvement in PDM.
Limitations
This study had several notable limitations. First, the cross-sectional design relied on data collected at a single time point, which inherently limited the ability to infer causal relationships between the observed brain structural changes and the pathophysiology of dysmenorrhea. This temporal constraint also precluded longitudinal assessment of dynamic neuroplastic changes across the menstrual cycle. Second, although the sample size was statistically adequate for exploratory analyses, participants were recruited from a single medical institution. This institutional and geographic homogeneity may introduce selection bias and limit the generalizability of the findings to a broader population with diverse genetic, environmental, and socioeconomic backgrounds. Finally, specifically regarding the mediation analysis, while primary clinical variables and key covariates (such as age, intracranial volume, SAS, and SDS scores) were strictly controlled in our models, the potential subtle modulating effects of unmeasured confounders, including participants’ lifestyle factors, duration of PDM, and minor menstrual cycle variability, warrant further investigation. These limitations underscore the need for future large-scale, multicenter longitudinal studies incorporating multimodal neuroimaging, comprehensive hormonal profiling, and detailed clinical phenotyping to elucidate the temporal trajectory of neural structural adaptations and their underlying mechanisms in PDM.
Data Sharing Statement
The datasets obtained during the current study are available from the corresponding author, Ming Zhang ([email protected]), upon reasonable request.
Ethics Committee Approval
The approval for the study was obtained from The First Affiliated Hospital of Xi’an Jiaotong University Clinical Research Ethics Committee (decision number:2017-0154).
Acknowledgments
The authors thank all study participants for their time and effort devoted to this study. This work was supported by the Institutional Foundation of The First Affiliated Hospital of Xi’an Jiaotong University (2024-MS-25), the Clinical Research Project Funds for the First Affiliated Hospital of Xi’an Jiaotong University (XJTU1AF-CRF-2022-023) and the Health Research and Innovation Capacity Strengthening Platform Program of Shaanxi Province (No.2023PT-09).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that this study was conducted in the absence of any commercial or financial relationships that could be construed as potential conflicts of interest.
References
1. Kho KA, Shields JK. Diagnosis and management of primary dysmenorrhea. JAMA. 2020;323(3):268–14. doi:10.1001/jama.2019.16921
2. Ferries-Rowe E, Corey E, Archer JS. Primary dysmenorrhea: diagnosis and therapy. Obstet Gynecol. 2020;136(5):1047–1058. doi:10.1097/AOG.0000000000004096
3. Tu F, Hellman K. Primary dysmenorrhea: diagnosis and therapy. Obstet Gynecol. 2021;137(4):752. doi:10.1097/AOG.0000000000004341
4. Iacovides S, Avidon I, Baker FC. What we know about primary dysmenorrhea today: a critical review. Hum Reprod Update. 2015;21(6):762–778. doi:10.1093/humupd/dmv039
5. Li R, Li B, Kreher DA, Benjamin AR, Gubbels A, Smith SM. Association between dysmenorrhea and chronic pain: a systematic review and meta-analysis of population-based studies. Am J Obstet Gynecol. 2020;223(3):350–371. doi:10.1016/j.ajog.2020.03.002
6. MacGregor B, Allaire C, Bedaiwy MA, Yong PJ, Bougie O. Disease burden of dysmenorrhea: impact on life course potential. Int J Womens Health. 2023;15:499–509. doi:10.2147/IJWH.S380006
7. Luo Y, Liu D, Sun G, et al. The chain mediating effect of health literacy and self-care ability on the relationship between dysmenorrhea symptoms and negative emotions among chinese female college students. IJWH. 2025;17:1069–1082. doi:10.2147/IJWH.S511601
8. Yu R. Menstrual leave policies in mainland china: implementation, controversies, and future directions. Ajsr. 2024;16–19. doi:10.70251/HYJR2348.211619
9. Tu CH, Niddam DM, Chao HT, et al. Brain morphological changes associated with cyclic menstrual pain. Pain. 2010;150(3):462–468. doi:10.1016/j.pain.2010.05.026
10. Latremoliere A, Woolf CJ. Central sensitization: a generator of pain hypersensitivity by central neural plasticity. J Pain. 2009;10(9):895–926. doi:10.1016/j.jpain.2009.06.012
11. Yu S, Liu L, Chen L, et al. Classification of primary dysmenorrhea by brain effective connectivity of the amygdala: a machine learning study. Brain Imaging Behav. 2022;16(6):2517–2525. doi:10.1007/s11682-022-00707-9
12. Yu S, Xu J, Shen Z, et al. Frequency-specific alterations in brain function in patients with primary dysmenorrhea. Pain Med. 2022;23(5):902–911. doi:10.1093/pm/pnab225
13. Liu N, Huo J, Li Y, et al. Changes in brain structure and related functional connectivity during menstruation in women with primary dysmenorrhea. Quant Imaging Med Surg. 2023;13(2):1071–1082. doi:10.21037/qims-22-683
14. Rodriguez-Raecke R, Niemeier A, Ihle K, Ruether W, May A. Brain gray matter decrease in chronic pain is the consequence and not the cause of pain. J Neurosci. 2009;29(44):13746–13750. doi:10.1523/JNEUROSCI.3687-09.2009
15. Yi SJ, Chen RB, Zhong YL, Huang X. The effect of long-term menstrual pain on large-scale brain network in primary dysmenorrhea patients. JPR. 2022;15:2123–2131. doi:10.2147/JPR.S366268
16. Wang C, He J, Feng X, et al. Characteristics of pain empathic networks in healthy and primary dysmenorrhea women: an fMRI study. Brain Imaging and Behavior. 2024;18(5):1086–1099. doi:10.1007/s11682-024-00901-x
17. Liu P, Yang J, Wang G, et al. Altered regional cortical thickness and subcortical volume in women with primary dysmenorrhoea. Eur. J. Pain. 2016;20(4):512–520. doi:10.1002/ejp.753
18. Henderson LA, Akhter R, Youssef AM, et al. The effects of catastrophizing on central motor activity. Eur. J. Pain. 2016;20(4):639–651. doi:10.1002/ejp.781
19. Yang L, Dun W, Li K, et al. Altered amygdalar volume and functional connectivity in primary dysmenorrhoea during the menstrual cycle. Eur J Pain. 2019;23(5):994–1005. doi:10.1002/ejp.1368
20. Jiang J, Zhuang Y, Si S, et al. The association of reproductive hormones during the menstrual period with primary dysmenorrhea. Int J Womens Health. 2023;15:1501–1514. doi:10.2147/IJWH.S421950
21. Petraglia F, Parke S, Serrani M, Mellinger U, Römer T. Estradiol valerate plus dienogest versus ethinylestradiol plus levonorgestrel for the treatment of primary dysmenorrhea. Int J Gynaecol Obstet. 2014;125(3):270–274. doi:10.1016/j.ijgo.2013.11.017
22. Albert K, Pruessner J, Newhouse P. Estradiol levels modulate brain activity and negative responses to psychosocial stress across the menstrual cycle. Psychoneuroendocrinology. 2015;59:14–24. doi:10.1016/j.psyneuen.2015.04.022
23. Albert K, Hiscox J, Boyd B, Dumas J, Taylor W, Newhouse P. Estrogen enhances hippocampal gray-matter volume in young and older postmenopausal women: a prospective dose-response study. Neurobiol Aging. 2017;56:1–6. doi:10.1016/j.neurobiolaging.2017.03.033
24. Derntl B, Eber CH, Kogler L, Rehbein E, Sundstöm-Poromaa I, Morawetz C. Estradiol modulates changes in effective connectivity in emotion regulation networks. Psychoneuroendocrinology. 2024;167:107103. doi:10.1016/j.psyneuen.2024.107103
25. Jüptner M, Jussofie A, Hiemke C. Effects of ovariectomy and steroid replacement on GABAA receptor binding in female rat brain. J Steroid Biochem Mol Biol. 1991;38(2):141–147. doi:10.1016/0960-0760(91)90119-p
26. Herbison AE, Fénelon VS. Estrogen regulation of GABAA receptor subunit mRNA expression in preoptic area and bed nucleus of the stria terminalis of female rat brain. J Neurosci. 1995;15(3 Pt 2):2328–2337. doi:10.1523/JNEUROSCI.15-03-02328.1995
27. Murphy DD, Cole NB, Greenberger V, Segal M. Estradiol increases dendritic spine density by reducing GABA neurotransmission in hippocampal neurons. J Neurosci. 1998;18(7):2550–2559. doi:10.1523/JNEUROSCI.18-07-02550.1998
28. Ycaza Herrera A, Mather M. Actions and interactions of estradiol and glucocorticoids in cognition and the brain: implications for aging women. Neurosci Biobehav Rev. 2015;55:36–52. doi:10.1016/j.neubiorev.2015.04.005
29. Zwaan IS, Felmingham K, Vijayakumar N, et al. Estradiol variability is associated with brain structure in early adolescent females. Psychoneuroendocrinology. 2022;146:105943. doi:10.1016/j.psyneuen.2022.105943
30. De Pauw R, Coppieters I, Caeyenberghs K, et al. Associations between brain morphology and motor performance in chronic neck pain: a whole-brain surface-based morphometry approach. Hum Brain Mapp. 2019;40(14):4266–4278. doi:10.1002/hbm.24700
31. Iacovides S, Baker FC, Avidon I, Bentley A. Women with dysmenorrhea are hypersensitive to experimental deep muscle pain across the menstrual cycle. J Pain. 2013;14(10):1066–1076. doi:10.1016/j.jpain.2013.04.010
32. Chantler I, Mitchell D, Fuller A. Actigraphy quantifies reduced voluntary physical activity in women with primary dysmenorrhea. J Pain. 2009;10(1):38–46. doi:10.1016/j.jpain.2008.07.002
33. Zhang B, Xu Y, He W, et al. Intensity dependence of auditory evoked potentials in primary dysmenorrhea. J Pain. 2017;18(11):1324–1332. doi:10.1016/j.jpain.2017.06.009
34. Hawker GA, Mian S, Kendzerska T, French M. Measures of adult pain: visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS), and Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP). Arthritis Care Res. 2011;63(Suppl 11):S240–252. doi:10.1002/acr.20543
35. Zung WW. A rating instrument for anxiety disorders. Psychosomatics. 1971;12(6):371–379. doi:10.1016/S0033-3182(71)71479-0
36. Zung WW. A SELF-RATING DEPRESSION SCALE. Arch Gen Psychiatry. 1965;12:63–70. doi:10.1001/archpsyc.1965.01720310065008
37. Grandi G, Xholli A, Ferrari S, Cannoletta M, Volpe A, Cagnacci A. Intermenstrual pelvic pain, quality of life and mood. Gynecol Obstet Invest. 2013;75(2):97–100. doi:10.1159/000343997
38. Sullivan MJL, Bishop SR, Pivik J. The Pain Catastrophizing Scale: development and validation. Psychol. Assess. 1995;7(4):524–532. doi:10.1037/1040-3590.7.4.524
39. Mackinnon DP. Required Sample Size to Detect the Mediated Effect. Available from: https://www.academia.edu/19420516/Required_Sample_Size_to_Detect_the_Mediated_Effect.
40. Fischl B. FreeSurfer. Neuroimage. 2012;62(2):774–781. doi:10.1016/j.neuroimage.2012.01.021
41. Dale AM, Fischl B, Sereno MI. Cortical surface-based analysis. I. Segmentation and surface reconstruction. Neuroimage. 1999;9(2):179–194. doi:10.1006/nimg.1998.0395
42. Fischl B, van der Kouwe A, Destrieux C, et al. Automatically parcellating the human cerebral cortex. Cereb Cortex. 2004;14(1):11–22. doi:10.1093/cercor/bhg087
43. Desikan RS, Ségonne F, Fischl B, et al. An automated labeling system for subdividing the human cerebral cortex on MRI scans into gyral based regions of interest. Neuroimage. 2006;31(3):968–980. doi:10.1016/j.neuroimage.2006.01.021
44. Esteban O, Birman D, Schaer M, Koyejo OO, Poldrack RA, Gorgolewski KJ. MRIQC: advancing the automatic prediction of image quality in MRI from unseen sites. PLoS One. 2017;12(9):e0184661. doi:10.1371/journal.pone.0184661
45. Backhausen LL, Herting MM, Buse J, Roessner V, Smolka MN, Vetter NC. Quality control of structural mri images applied using freesurfer-a hands-on workflow to rate motion artifacts. Front Neurosci. 2016;10:558. doi:10.3389/fnins.2016.00558
46. Nichols TE, Holmes AP. Nonparametric permutation tests for functional neuroimaging: a primer with examples. Hum Brain Mapp. 2002;15(1):1–25. doi:10.1002/hbm.1058
47. Preacher KJ, Hayes AF. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav Res Methods. 2008;40(3):879–891. doi:10.3758/brm.40.3.879
48. Vogt BA. Pain and emotion interactions in subregions of the cingulate gyrus. Nat Rev Neurosci. 2005;6(7):533–544. doi:10.1038/nrn1704
49. Baliki MN, Petre B, Torbey S, et al. Corticostriatal functional connectivity predicts transition to chronic back pain. Nat Neurosci. 2012;15(8):1117–1119. doi:10.1038/nn.3153
50. Etkin A, Egner T, Kalisch R. Emotional processing in anterior cingulate and medial prefrontal cortex. Trends Cognit Sci. 2011;15(2):85–93. doi:10.1016/j.tics.2010.11.004
51. As-Sanie S, Harris RE, Napadow V, et al. Changes in regional gray matter volume in women with chronic pelvic pain: a voxel-based morphometry study. Pain. 2012;153(5):1006–1014. doi:10.1016/j.pain.2012.01.032
52. As-Sanie S, Kim J, Schmidt-Wilcke T, et al. Functional connectivity is associated with altered brain chemistry in women with endometriosis-associated chronic pelvic pain. J Pain. 2016;17(1):1–13. doi:10.1016/j.jpain.2015.09.008
53. Liu P, Liu Y, Wang G, et al. Changes of functional connectivity of the anterior cingulate cortex in women with primary dysmenorrhea. Brain Imaging Behav. 2018;12(3):710–717. doi:10.1007/s11682-017-9730-y
54. Mosch B, Hagena V, Herpertz S, Ruttorf M, Diers M. Neural correlates of control over pain in fibromyalgia patients. Neuroimage Clin. 2023;37:103355. doi:10.1016/j.nicl.2023.103355
55. Lin P, Yang Y, Jovicich J, et al. Static and dynamic posterior cingulate cortex nodal topology of default mode network predicts attention task performance. Brain Imaging Behav. 2016;10(1):212–225. doi:10.1007/s11682-015-9384-6
56. Neumann N, Domin M, Schmidt CO, Lotze M. Chronic pain is associated with less grey matter volume in the anterior cingulum, anterior and posterior insula and hippocampus across three different chronic pain conditions. Eur J Pain. 2023;27(10):1239–1248. doi:10.1002/ejp.2153
57. Nguyen T, Behrens M, Broscheid KC, et al. Associations between gait performance and pain intensity, psychosocial factors, executive functions as well as prefrontal cortex activity in chronic low back pain patients: a cross-sectional fNIRS study. Front Med Lausanne. 2023;10:1147907. doi:10.3389/fmed.2023.1147907
58. Li H, Song Q, Zhang R, Zhou Y, Kong Y. Enhanced temporal coupling between thalamus and dorsolateral prefrontal cortex mediates chronic low back pain and depression. Neural Plast. 2021;2021:7498714. doi:10.1155/2021/7498714
59. Kim YR, Kim SJ. Altered synaptic connections and inhibitory network of the primary somatosensory cortex in chronic pain. Korean J Physiol Pharmacol. 2022;26(2):69–75. doi:10.4196/kjpp.2022.26.2.69
60. Liu P, Wang G, Liu Y, et al. Disrupted intrinsic connectivity of the periaqueductal gray in patients with functional dyspepsia: a resting-state fMRI study. Neurogastroenterol Motil. 2017;29(8). doi:10.1111/nmo.13060
61. Chen YC, Cao ZM, Liu GY, et al. Abnormal functional hubs in migraine patients: a resting-state MRI analysis about voxel-wise degree centrality. J Oral Facial Pain Headache. 2024;38(1):52–63. doi:10.22514/jofph.2024.006
62. Liu J, Liu H, Mu J, et al. Altered white matter microarchitecture in the cingulum bundle in women with primary dysmenorrhea: a tract-based analysis study. Hum Brain Mapp. 2017;38(9):4430–4443. doi:10.1002/hbm.23670
63. Groman SM, Keistler C, Keip AJ, et al. Orbitofrontal circuits control multiple reinforcement-learning processes. Neuron. 2019;103(4):734–746.e3. doi:10.1016/j.neuron.2019.05.042
64. Rolls ET, Grabenhorst F. The orbitofrontal cortex and beyond: from affect to decision-making. Prog Neurobiol. 2008;86(3):216–244. doi:10.1016/j.pneurobio.2008.09.001
65. Mercer Lindsay N, Chen C, Gilam G, Mackey S, Scherrer G. Brain circuits for pain and its treatment. Sci Transl Med. 2021;13(619):eabj7360. doi:10.1126/scitranslmed.abj7360
66. Bliss TVP, Collingridge GL, Kaang BK, Zhuo M. Synaptic plasticity in the anterior cingulate cortex in acute and chronic pain. Nat Rev Neurosci. 2016;17(8):485–496. doi:10.1038/nrn.2016.68
67. Kringelbach ML. The human orbitofrontal cortex: linking reward to hedonic experience. Nat Rev Neurosci. 2005;6(9):691–702. doi:10.1038/nrn1747
68. Huang J, Zhang Z, Gambeta E, Chen L, Zamponi GW. An orbitofrontal cortex to midbrain projection modulates hypersensitivity after peripheral nerve injury. Cell Rep. 2021;35(4):109033. doi:10.1016/j.celrep.2021.109033
69. Kragel PA, Kano M, Van Oudenhove L, et al. Generalizable representations of pain, cognitive control, and negative emotion in medial frontal cortex. Nat Neurosci. 2018;21(2):283–289. doi:10.1038/s41593-017-0051-7
70. Etkin A, Egner T, Peraza DM, Kandel ER, Hirsch J. Resolving emotional conflict: a role for the rostral anterior cingulate cortex in modulating activity in the amygdala. Neuron. 2006;51(6):871–882. doi:10.1016/j.neuron.2006.07.029
71. Wei X, Shi G, Tu J, et al. Structural and functional asymmetry in precentral and postcentral gyrus in patients with unilateral chronic shoulder pain. Front Neurol. 2022;13:792695. doi:10.3389/fneur.2022.792695
72. Kim W, Kim SK, Nabekura J. Functional and structural plasticity in the primary somatosensory cortex associated with chronic pain. J Neurochem. 2017;141(4):499–506. doi:10.1111/jnc.14012
73. Zhao Y, Lin J, Dong Y, et al. Neuroimaging studies of chronic prostatitis/chronic pelvic pain syndrome. Pain Res Manag. 2022;2022:9448620. doi:10.1155/2022/9448620
74. Kim SK, Eto K, Nabekura J. Synaptic structure and function in the mouse somatosensory cortex during chronic pain: in vivo two-photon imaging. Neural Plast. 2012;2012:640259. doi:10.1155/2012/640259
75. Apkarian AV, Sosa Y, Sonty S, et al. Chronic back pain is associated with decreased prefrontal and thalamic gray matter density. J Neurosci. 2004;24(46):10410–10415. doi:10.1523/JNEUROSCI.2541-04.2004
76. Apkarian AV, Bushnell MC, Treede RD, Zubieta JK. Human brain mechanisms of pain perception and regulation in health and disease. Eur J Pain. 2005;9(4):463–484. doi:10.1016/j.ejpain.2004.11.001
77. Pletzer B, Kronbichler M, Aichhorn M, Bergmann J, Ladurner G, Kerschbaum HH. Menstrual cycle and hormonal contraceptive use modulate human brain structure. Brain Res. 2010;1348:55–62. doi:10.1016/j.brainres.2010.06.019
78. Petersen N, Touroutoglou A, Andreano JM, Cahill L. Oral contraceptive pill use is associated with localized decreases in cortical thickness. Hum Brain Mapp. 2015;36(7):2644–2654. doi:10.1002/hbm.22797
79. Lu Y, Sareddy GR, Wang J, et al. Neuron-derived estrogen regulates synaptic plasticity and memory. J Neurosci. 2019;39(15):2792–2809. doi:10.1523/JNEUROSCI.1970-18.2019
80. McEwen BS. Invited review: estrogens effects on the brain: multiple sites and molecular mechanisms. J Appl Physiol. 2001;91(6):2785–2801. doi:10.1152/jappl.2001.91.6.2785
81. Barth C, Villringer A, Sacher J. Sex hormones affect neurotransmitters and shape the adult female brain during hormonal transition periods. Front Neurosci. 2015;9. doi:10.3389/fnins.2015.00037
82. van Aken MAW, Oosterman JM, van Rijn CM, et al. Pain cognition versus pain intensity in patients with endometriosis: toward personalized treatment. Fertil Steril. 2017;108(4):679–686. doi:10.1016/j.fertnstert.2017.07.016
83. Giesecke T, Gracely RH, Grant MAB, et al. Evidence of augmented central pain processing in idiopathic chronic low back pain. Arthritis Rheum. 2004;50(2):613–623. doi:10.1002/art.20063
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Loneliness and Pain Catastrophizing Among Individuals with Chronic Pain: The Mediating Role of Depression
Wilson JM, Colebaugh CA, Meints SM, Flowers KM, Edwards RR, Schreiber KL
Journal of Pain Research 2022, 15:2939-2948
Published Date: 16 September 2022
Disease Burden of Dysmenorrhea: Impact on Life Course Potential
MacGregor B, Allaire C, Bedaiwy MA, Yong PJ, Bougie O
International Journal of Women's Health 2023, 15:499-509
Published Date: 3 April 2023
Pain Catastrophizing and Its Association with Military Medical Disability Among US Active Duty Service Members with Chronic Predominately Musculoskeletal Pain: A Retrospective Cohort Analysis
Schaaf S, Flynn DM, Steffen AD, Ransom J, Doorenbos A
Journal of Pain Research 2023, 16:3837-3852
Published Date: 9 November 2023
Pain Intensity and Pain Catastrophizing Among Patients with Chronic Pain: The Mediating Effect of Self-Efficacy
Li J, Cui Y, Jia Q, Ouyang A, Hua Y
Journal of Pain Research 2025, 18:1361-1373
Published Date: 19 March 2025
Perspectives on Pain: A Narrative Review of Pain Beliefs, Coping, and Clinical Implications

Pugh C, Snoddy K, Boyett R, Bakir H, Cawley D, Piscura MK
Journal of Pain Research 2026, 19:603074
Published Date: 23 April 2026