")
Back to Journals » Journal of Pain Research » Volume 16
Pain Catastrophizing and Its Association with Military Medical Disability Among US Active Duty Service Members with Chronic Predominately Musculoskeletal Pain: A Retrospective Cohort Analysis
Authors Schaaf S, Flynn DM , Steffen AD, Ransom J, Doorenbos A
Received 5 December 2022
Accepted for publication 6 July 2023
Published 9 November 2023 Volume 2023:16 Pages 3837—3852
DOI https://doi.org/10.2147/JPR.S400313
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Jonathan Greenberg
Sherrill Schaaf,1,* Diane M Flynn,2,* Alana D Steffen,3 Jeffrey Ransom,2 Ardith Doorenbos3,4
1School of Health Sciences, A.T. Still University, Mesa, AZ, USA; 2Interdisciplinary Pain Management Center, Madigan Army Medical Center, Tacoma, WA, USA; 3College of Nursing, University of Illinois Chicago, Chicago, IL, USA; 4Department of Anesthesiology and Pain Medicine, University of Washington School of Medicine, Seattle, WA, USA
*These authors contributed equally to this work
Correspondence: Diane M Flynn, Physical Performance Service Line, Madigan Army Medical Center, Tacoma, WA, 98431, USA, Tel +1-253-968-0618, Fax +1-253-968-0469, Email [email protected]
Context: Pain catastrophizing is characterized by negative emotional and cognitive responses to pain and is a predictor of work-related disability. Its association with military medical disability has not been studied.
Objective: To (1) identify the pain catastrophizing scale (PCS) score cut point most strongly associated with military medical disability, (2) measure the difference in rate of disability between service members with baseline PCS scores above versus below the cut point, and (3) determine if improvement in PCS score during pain specialty care is associated with decreased likelihood of disability.
Methods: This was a retrospective cohort analysis comparing PCS scores collected from US Army active duty service members at time of initial visit to an interdisciplinary pain management center and periodically during pain treatment. Outcome was determination during the following year of a military service-disqualifying disability.
Results: Receiver operating characteristic (ROC) curves determined that a PCS score of 20 was the single cut point most closely associated with subsequent disability. Kaplan–Meier curves showed significantly higher disability rate during the following year among those with baseline PCS scores ≥ 20 (52%) compared to those with lower scores (26%). Scheffe-adjusted contrasts showed that service members with PCS scores ≥ 20 whose scores improved to < 20 at follow-up were significantly less likely to have a medical disability (42.6%; 95% CI, 0.07– 0.58) than those whose PCS score remained ≥ 20 (76.3%; 95% CI, 68.0%– 84.7%).
Conclusion: A PCS score cut point of 20 distinguishes between high versus low likelihood of disability among service members. Those with high baseline PCS score had twice the likelihood of disability than those with low scores. Service members who decreased their PCS score from high to low during pain specialty care had lower likelihood of disability. Prospective research is needed to determine if treatments that lower pain catastrophizing yield reduced likelihood of subsequent disability.
Plain Language Summary: Pain catastrophizing is a persistent tendency to have distressing thoughts and emotions related to pain and worsens work-related outcomes. This study examined the association between pain catastrophizing and military medical disability in a population of active duty US Army service members. The pain catastrophizing scale (PCS) scale is a 13-item questionnaire with a range of 0 (lowest catastrophizing) to 52 (highest catastrophizing). The aims of the study were to (1) identify the PCS score cut point most strongly associated with later military medical disability, (2) measure the difference in rate of disability between service members with baseline PCS scores above versus below the cut point, and (3) determine if improvement in PCS score during pain specialty care is associated with a decreased likelihood of disability. The study found that service members with high PCS scores were twice as likely to have medical disability than those with low scores. Additionally, those who reduced their PCS score were less likely to be medically disabled later. This study showed that PCS score may help to identify service members at increased risk of disability so that they may be offered therapies that reduce pain catastrophizing. The main limitation of this study is its retrospective design; we cannot be certain if improvement in PCS resulted in lower disability rates or if inherently more disabling conditions resulted in greater catastrophizing.
Keywords: pain catastrophizing, chronic pain, interdisciplinary, disability, military
Introduction
Pain catastrophizing is characterized by negative emotional and cognitive responses to actual or anticipated pain and has been shown in clinical trials to have an adverse impact on pain intensity, response to treatment, and self-rated disability.1,2 However, research addressing the impact of pain catastrophizing on occupational disability is limited, and its impact on military medical disability is unknown.
Chronic pain can adversely impact the ability of military service members to perform their duties, thereby degrading military capability.3 Chronic pain is common in military service members. Among 297,120 US Army service members who were not deployed during fiscal year 2012, medical coding data revealed that 31% sought care for at least one chronic pain condition during a one-year period.4 Data collected from medical encounter records suggest that the incidence of chronic pain among US service members is increasing. During the 2009–2018 period, medical encounters related to chronic pain increased from 85.5 to 261.1 per 10,000 person-years.5 Although the increase may be related to changes in demographics, reporting practices and willingness to seek pain care, the increase is likely partially explained by an increase in combat deployments.5 Among service members returning from combat deployments, up to 44% report chronic pain.6 As in non-military populations, musculoskeletal pain, particularly related to joint and spine disorders, is the most common type of chronic pain in US service members.4,7 Among the categories of conditions leading to disability discharges from the military, musculoskeletal is the most common.8
Military service members are a unique population due to the stringent health screening required for entry to military service and fitness and health standards that must be met to remain on active duty.9 Service members undergo annual health screenings and semi-annual physical fitness tests for various measures of aerobic fitness and strength. In addition, service members are distinct from most other workers due to the possibility of deployment to austere and often hazardous environments, including combat zones. The demographic characteristics of the approximately 474,000 active duty Army service members are different from the non-military US workforce. For example, 77% of Army service members are under the age of 35 years, compared to 33% of the US workforce; 85% are men compared to 53% of the US workforce; and 21% are black or African American compared to 12% of the US workforce.10
The aims of this study were to (1) identify the pain catastrophizing scale (PCS) score cut point most strongly associated with subsequent military medical disability, (2) measure the difference in rates of subsequent military medical disability between service members with baseline PCS scores above versus below the cut point, and (3) determine if improvement in PCS score from the high to low range is associated with a decreased likelihood of subsequent military medical disability. The overall objective was to identify modifiable risk factors that increase the likelihood of military disability so that service members at risk can be offered therapies that may favorably impact their fitness for continued service.
Materials and Methods
Study Design and Participants
The study protocol complies with the Declaration of Helsinki and was approved by the Madigan Army Medical Center (MAMC) Institutional Review Board. The study design was a retrospective cohort analysis of PCS scores collected from active duty service members as standard clinical practice at the time of referral to the MAMC Interdisciplinary Pain Management Center (IPMC). MAMC, located on Joint Base Lewis-McChord, supports an active duty population of more than 25,000 service members. The study population comprised of all active duty Army service members referred to the IPMC between June 2018 and May 2020 for chronic pain treatment.
Determination of Military Medical Disability
The determination of military medical disability is based on whether or not service members have the physical stamina and strength to perform the tasks of their military-specific occupations as well as general tasks required of all service members. When Army service members develop chronic conditions that render them unable to perform these tasks, they are determined to be unfit for continued military service and are referred to the Integrated Disability Evaluation System (IDES) to begin the process of medical discharge from the military.11 During this process, service members undergo a separate evaluation in conjunction with the Veterans Health Administration to determine the percentage of disability compensation to which they are entitled. Researchers had access to data on when service members were referred to the IDES and determined to be unfit for continued service but did not have access to information on the percentage of disability. Service members who were referred to IDES during the one year following initial IPMC visit defined the subgroup with military medical disability. Service members were excluded from analysis if they 1) were referred to IDES prior to initial IPMC visit; 2) referred to IDES solely for hearing and/or vision-related condition(s); or 3) if they did not remain assigned to the MAMC catchment area during the full one-year follow-up period.
For the subset used for our third aim to determine if a decrease in PCS score would be associated with a lower likelihood of military medical disability, we excluded service members who completed their first follow-up PCS more than 180 days after baseline PCS. We designed this exclusion to standardize the posttreatment effects on PCS to the short-term (1 to 6 months) time period.
Measures
The PCS is a 13-item questionnaire with a score range of 0 (lowest catastrophizing) to 52 (highest catastrophizing) that assesses the 3 components of pain catastrophizing: rumination, magnification, and helplessness.12 The PCS is widely used. A 2019 meta-analysis to assess its psychometric properties identified 220 studies of various designs published between 1997 and 2015 that mentioned PCS in the abstract. Across 70 studies assessed to be of low risk for bias in this review, the PCS demonstrated good internal and test–retest reliability.13
Demographic characteristics collected in this study included sex, age, level of education, and military rank. Pain type was determined by the ICD-9 or 10 code for the primary diagnosis at the initial medical visit to the IPMC. Service members’ military medical disability status was accessed through a data sharing agreement with the Office of the US Army Surgeon General.
The PCS is one of the battery of electronic, web-based assessments of psychological, physical, and social functioning included in the Pain Assessment Screening Tool and Outcomes Registry (PASTOR),14 which is the standard pain assessment tool in pain specialty clinics in the US Military Health System. PASTOR is completed by all IPMC patients at their initial visit and periodically during pain care. Other PASTOR measures include 7-day average pain intensity as measured by the 0–10 Defense and Veterans Pain Rating Scale,15 and the National Institutes of Health (NIH) Patient Reported Outcomes Measurement Information System (PROMIS) measures of depression, anxiety, pain interference and physical function.16–18 PROMIS-based T-scores range from 0 to 100 and are normed to the general US population. Scores within normal limits are any scores better than or equal to the mean score and up to half a standard deviation worse than the mean.19 Cut points for mild, moderate, and severe are 1, 2 and 3 standard deviations worse than the mean, respectively. PASTOR also includes the 5-item primary care posttraumatic stress disorder (PC-PTSD) screen for which 3 or more positive responses are considered a positive screen.20
Procedures and Exposure
As part of usual clinic care, all service members in the study population underwent a comprehensive initial evaluation by a physician, physician assistant or nurse practitioner who developed a treatment plan. Treatment was individualized to each service member and may have included medications; therapeutic injections; and/or psychological, physical, occupational, chiropractic, acupuncture, yoga, and/or massage therapies. The first follow-up PCS score collected between 30 and 180 days after initial visit was used to compute change in PCS score.
Deidentified data were aggregated from PASTOR data, military medical disability data, and medical appointment data files to identify a sample with PCS measures completed between 30 and 180 days after initial IPMC visit, medical disability determination after referral but within 1 year, and military status 1 year after baseline.
Statistical Analyses
Chi-square analysis was conducted to compare demographic, clinical and disability categorical variables for the total population and subset. Receiver operating characteristic (ROC) curves21 were used to determine the baseline and follow-up PCS score cut points that were most strongly associated with subsequent military medical disability. Change in PCS score was computed by using the difference between baseline and first follow-up PCS score collected between 30 and 180 days after baseline (follow-up minus baseline).
Kaplan–Meier curves were used to display the survival functions for groups with high and low baseline PCS scores to estimate the proportion determined to have a military medical disability during the following year. Disability determination was the event of interest; lack of disability and discontinuation of military service in the MAMC catchment area for any other reason were considered right-censored cases. Log rank test and Cox regression with adjustment for age, sex, military rank and education were also conducted. Chi-square analysis and logistic regression with adjustment for age, sex, military rank, education, and number of days between baseline and follow-up PCS were used to examine the association between change in PCS score during treatment and subsequent disability. A Scheffe adjustment was used for pairwise comparisons of groups to control for type I errors.
Results
The study population included 812 active duty Army service members. Over 60% of the study patients were under the age of 34, with the largest group (41%) between the ages of 25 and 34 (Table 1). Men outnumbered women by more than 3 to 1 (77% vs 23%), and nearly half (48%) were senior enlisted members (military ranks E-5 to E-9), followed closely by junior enlisted members (ranks E-1 to E-4) at 36%. Officers (O-1 to O-9) and warrant officers (W-1 to W-5) made up less than 23% of participants. Most service members had some college, a technical degree, or associate degree, and all but one had a minimum of high school education or high school equivalency diploma. About 22% of the study population had a bachelor’s degree, and 12% had advanced degrees. There were no statistically significant differences in the distributions of demographic variables between the total population and subset. Table 1 presents these descriptive demographic statistics separately for the total population and for the subset of patients who completed a second PCS measure 30–180 days after baseline. Table 2 provides descriptive data on the clinical characteristics of the study populations. Musculoskeletal pain was the predominant pain type, present in more than 85% of the total population and subset. In both the total and subpopulations, most reported baseline pain intensity, pain interference and physical functional impairment in the moderate range. About half of the total population and subset had depression and anxiety scores in the normal range. Among those whose scores were consistent with depression or anxiety, the majority were in the moderate range with smaller proportions in the mild range and lowest proportion in the severe range. PC-PTSD screen was positive in 38% and 37% of the total population and subset, respectively. The subset population had a lower proportion who reported pain intensity in the moderate and severe ranges and a higher proportion who reported physical impairment in the moderate and severe ranges than the total population. There were no statistically significant differences in the distributions of pain type, PCS score, pain interference, depression, anxiety or PC-PTSD screen between the total population and subset.
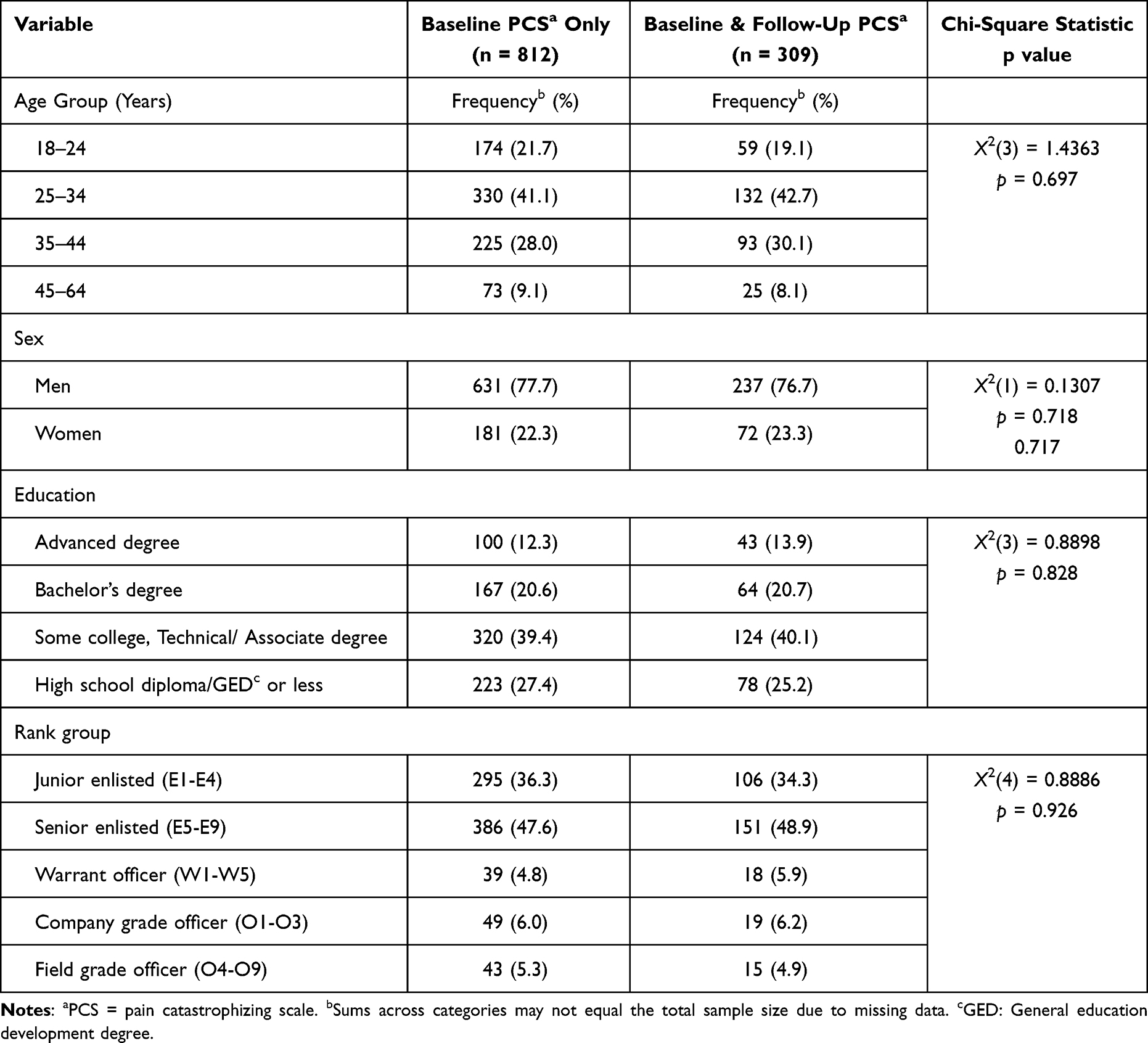 |
Table 1 Demographic Characteristics of Study Populations |
 |
Table 2 Clinical Characteristics of Study Populations |
Over a third of the total study population and over half of the subset with follow-up PCS score were determined to have a military medical disability during the one-year follow-up period (Table 3). Musculoskeletal conditions were the most common source of disability comprising more than three-quarters of disabilities in both the full study population and subset. The distribution of baseline PCS score was symmetrical (mean 22, median 20, skewness 0.3, standard deviation 13.9) (Figure 1). For the subset with 2 or more PCS scores, 95% had a second assessment within 180 days.
 |
Table 3 Frequency of Disabling Conditions Among Study Populations |
 |
Figure 1 Distribution of baseline pain catastrophizing scale scores. n = 812; mean = 22.3, median = 20.0, standard deviation 13.9. |
ROC curves revealed that a baseline PCS score cut point of 21 and a follow-up cut point of 19 had the strongest association with subsequent medical disability during the following year (area under the curve 0.81, Figure 2). Curves using a cut point of 20 for both baseline and follow-up had nearly the same strength of association with future disability (area under the curve 0.81). Given the comparability of both sets of baseline and follow-up cut points and greater usability of a single cut point, we used a cut point of 20 to discriminate between high and low for both baseline and follow-up PCS scores.
 |
Figure 2 Receiver operating characteristic (ROC) analysis determined which pre- and post-treatment PCS cutoffs maximized both sensitivity and 1 minus specificity, ie, area under the curve (AUC) for predicting medical disability. |
We used survival analysis to examine our second aim to measure the difference in rates of subsequent military medical disability between service members with baseline PCS scores above versus below the cut point. The Kaplan–Meier curves were parallel, showing consistently higher disability rates during the 1-year follow-up period among those with baseline PCS score ≥20 (estimated disability 28% and 52% at 6 and 12 months, respectively) compared to those with a PCS score <20 (13% and 26% at 6 and 12 months, respectively), as shown in Figure 3. This association was also supported by the log-rank (X2[1] = 47.4, P < 0.001) and Cox regression (high PCS compared to low: hazard ratio = 2.1 [SE = 0.28], z = 5.57, P < 0.001) with adjustments for age, sex, military rank and educational level. Across the entire sample, there was a direct relationship between baseline PCS score and subsequent disability rates (Figure 4).
 |
Figure 3 Kaplan-Meier survival curves. A comparison of the proportion of active-duty service members with baseline PCS score ≥20 vs <20 who were determined to have a military medical disability during the following year. PCS = pain catastrophizing scale. |
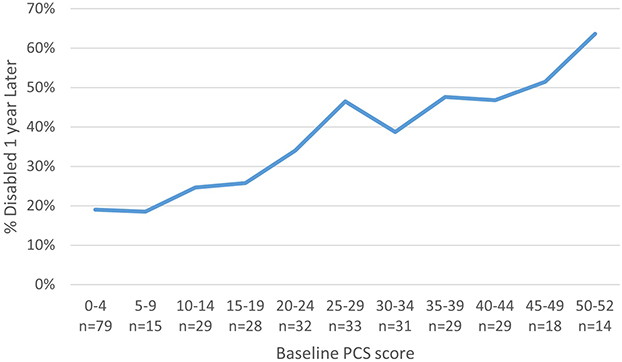 |
Figure 4 Percentage and number of service members in each PCS range who were disabled 1 year later. |
Our third aim was to examine if a decrease in PCS score during the course of pain care would be associated with a lower likelihood of subsequent military medical disability. This analysis was restricted to the subset of 309 participants who completed both baseline PCS and a follow-up PCS within the following 30–180 days.
Based on participants’ baseline and follow-up PCS scores, 4 groups were identified (Table 4). The 2 largest groups were service members who remained in the same PCS group: they started with a low (<20) PCS score and remained low (118, 38.2%) or started high (≥20) and remained high (117, 37.9%). The next largest group (50, 16.2%) were those who showed improvement by moving from the high to the low PCS range. The remaining service members (24, 7.8%) moved from the low to the high PCS range. Overall, the average PCS score change among the 309 participants was an improvement of 2.3 points. The middle 2 quartiles of PCS score change spanned 6 to 13 points across groups, and the full range of PCS score change groups was −37 to 24 points (Figure 5).
 |
Table 4 Percentage of Service Members Determined to Be Medically Disabled Within 1 Year Following Referral for Pain Specialty Care, by Group |
 |
Figure 5 Distribution of PCS score changes in each PCS subgroup. Negative numbers indicate improvement in PCS score; positive numbers indicate worsening in PCS score. Boxes show median change and limits of second and third quartiles; whiskers show maximum decrease and increase for each group; dots show outliers; Xs show mean change for each group. PCS = pain catastrophizing scale. Low PCS <20; High PCS ≥20. |
PCS subgroup showed a significant association with subsequent disability (Χ2[3] = 44.6, P < 0.001). After controlling for age, sex, rank, educational level, and number of days between baseline and follow-up PCS score, this association persisted (X2 [10] = 98.7 P < 0.001). Figure 6 displays the adjusted rates of disability for the PCS subgroups. Scheffe-adjusted contrasts showed that among service members with baseline PCS scores in the high range, those whose scores improved to the low range at follow-up were significantly less likely to have a future determination of military medical disability (42.6%; 95% CI, 0.07–0.58) than those whose PCS score remained high (76.3%; 95% CI, 68.0–84.7%). The change in PCS score and disability rates for the entire sample are shown in Figure 7. Most change score ranges had disability rates between 50% and 60%, but those whose score improved by 5–9 points had the lowest disability rate of 40% and those whose score worsened by 10–14 points had a disability rate of more than 70%.
 |
Figure 6 Adjusted rates of medical disability for PCS subgroups with 95% confidence limits. PCS = pain catastrophizing scale; Low = PCS score <20; High = PCS score ≥20. |
 |
Figure 7 Percentage of service members in each PCS change range who were disabled 1 year later. |
Discussion
To our knowledge, this is the first study to examine the association between pain catastrophizing and subsequent military medical disability. Active duty service members comprise a unique population due in part to the younger age, preponderance of men, and stringent health standards that must be maintained to remain on active duty. The key findings were that 1) 20 is a clinically meaningful PCS score cut point for assessing likelihood of future military medical disability; 2) baseline PCS scores equal to or above 20 versus below 20 were associated with twice the rate of subsequent medical disability; and 3) improvement in PCS score from high to low range during pain specialty care was associated with a significantly lower rate of subsequent disability compared with those whose PCS score remained high. Understanding of the cut point for clinically meaningful PCS scores has evolved since the introduction of the PCS tool in 1995. The PCS scoring manual was based on a population of 861 injured Nova Scotian workers with a mean age of 42 and equal sex distribution who had been off from work for a mean of 6.9 months, and reported 50th and 75th percentile scores of 20 and 30, respectively.22 Among the group whose PCS score was ≥30, 70% remained out of work 1 year later and 70% considered themselves totally disabled for occupationally related activities. Other PCS cut points proposed in the medical literature range from 20 to 30 and are based on a variety of outcome measures, including self-rated disability, and returning to work following work-related disability. The PCS score cut point of ≥20 identified in this study is consistent with the findings of Schütze and associates23 based on their meta-analysis of 79 studies with a combined population of 9914 participants designed to determine treatments that reduce pain catastrophizing. However, Pierobon and associates24 found that a slightly higher PCS score of ≥23 accounted for 20% of variance in self-rated disability. Scott and associates, determined that a pretreatment PCS score of ≥24 and posttreatment score of >15 best predicted poor return to work 1 year later among a population of occupationally disabled workers with subacute whiplash pain treated in a multidisciplinary pain rehabilitation program.25 The Initiatives on Methods, Measurement, Opportunities, and Networks (IMMPACT) recommendations regarding clinical trials of chronic pain include conducting responder analysis to determine the proportion of study subjects who meet or exceed the minimal clinically important difference (MCID) for each outcome.26 There are few published studies regarding the MCID for the PCS. In a clinical trial to study the impact of pain education on self-rated disability in a population with acute low back pain, Cashin et al found that the education intervention would have to result in a 21 point decrease in PCS score in order to result in a 2 point decrease in the (0–24) Roland-Morris disability questionnaire.27 Interestingly, the relationship we observed between the magnitude of PCS score change and disability rate across the study population was not consistent. Those with greatest improvement in PCS score of at least 10 points had disability rates no different from those with no change in PCS score, while those with more modest improvements of 5–9 points had the lowest disability rates. The most likely explanation for the inconsistency in this relationship is that those with the greatest improvement in PCS score likely had the highest baseline PCS scores. For example, those with baseline PCS scores greater than 40 may have had a decrease in PCS of more than 15 points yet still have high degrees of catastrophizing. Therefore, the MCID for in PCS regarding disability may be greater for higher baseline scores than for lower baseline scores. This is supported by the research of Monticone and associates, who used a combination of distribution- and anchor-based methods in an Italian population with non-specific low back pain, and estimated that the MCID in PCS to produce patient-perceived global improvement is a decrease of 11 points among those with baseline PCS >30 and 8 points for those with baseline score of <30.28 Future research is needed to evaluate the reproducibility of these MCIDs in other populations and for other outcomes.
Considering previous research evaluating the relationship between pain catastrophizing on work-related outcomes, the current study is most comparable to studies that evaluated staying at work (ie, remaining at work with less than 5% sick leave over a 12-month period) as the primary outcome. Our findings are consistent with the cross-sectional study conducted by de Vries et al, who found that workers with chronic musculoskeletal pain who remained at work despite pain (n = 119) had lower pain catastrophizing than those who remained on sick leave following vocational rehabilitation (n = 122).29 Conversely, a systematic review of factors associated with staying at work among workers with chronic musculoskeletal pain found that pain catastrophizing was not a determinant.30 Among workers off from work due to injury, pain catastrophizing was associated with reduced likelihood of returning to work22,25,31 and lower likelihood of maintaining improvements in pain intensity one year following multidisciplinary pain rehabilitation.32 In addition to studies of work-related outcomes, our findings are consistent with a large systematic review involving more than 2000 patients with chronic low back pain showing an association between pain catastrophizing and self-rated disability.1 Our findings are also consistent with cross-sectional studies showing direct and/or mediating effects of pain catastrophizing on pain interference33 and self-rated functional disability,34 and with prospective observational research showing an association between pain catastrophizing and self-rated disability35 among populations with chronic pain.
Among service members who were found to be medically disabled, 78% were disabled due to musculoskeletal conditions. One mechanism by which pain catastrophizing may lead to musculoskeletal disability is through its potential contribution to physical deconditioning associated with pain interference (ie, extent to which pain hinders engagement with social, cognitive, emotional, physical, and recreational activities). The fear avoidance model of chronic pain is one of the most widely accepted constructs to explain the role of psychological processes in the transition from acute pain to chronic pain and associated disability. The model posits that pain has a bidirectional relationship with pain catastrophizing and negative affect, which may worsen fear of pain and negative emotions, which may lead to avoidant behaviors and associated activity limitations, which increase the risk of physical deconditioning and disability.36 It is noteworthy that 15% of disability determinations were for psychological disorders. Given the relationship between pain catastrophizing and affective disorders, it is plausible that pain catastrophizing contributed to these determinations as well.
Importantly, pain catastrophizing is modifiable. The meta-analysis conducted by Schütze and associates concluded that most psychological, physical and pharmacological pain interventions studied produce at least medium strength effect size on pain catastrophizing, but the beneficial effects were larger and more consistent in studies of interventions that specifically targeted catastrophizing.18 In all studies included in the Schütze et al review, the strongest effect size on pain catastrophizing was produced by multimodal treatments, defined as those including both psychological and physical treatments. Among the subset of studies in the meta-analysis that targeted high pain catastrophizing, cognitive behavioral therapy had the best evidence for reducing catastrophizing.23 Murphy and associates analyzed outcomes of 931 US military veterans who engaged in multidisciplinary pain rehabilitation care that included psychological approaches, physical therapy, and pharmacotherapy at five Veterans Health Administration pain clinics. In that study among three core outcome measures, including PCS, insomnia symptom inventory, and the Pain Outcomes Questionnaire for Veterans score (a 0–100 composite score of pain intensity, pain interference, negative affect, pain-related fear and vitality), PCS score was the outcome measure most responsive to treatment. The study population had a mean baseline PCS score of 28, and an average post-treatment PCS score reduction of 31% was observed.37
The degree to which pain catastrophizing has a direct effect on military medical disability is unclear. It is possible that catastrophizing mediates the effects of therapy on disability, or it may be associated with other clinical, psychological, or occupational factors that are more strongly associated with subsequent disability. In a mediator analysis of factors associated with disability following a cognitive-behaviorally informed multidisciplinary pain program in a population with chronic low back pain, Cassidy et al found that pain catastrophizing completely mediated the effects of mindfulness on disability suggesting that the mechanism by which greater mindfulness is associated with lower disability is through its impact on catastrophizing.38 Other research has reported that pain catastrophizing mediates the effect between exercise engagement and disability in a community sample of people with chronic low back pain.39 Future mediator studies are needed to clarify the relative role of each of these potential relationships between pain catastrophizing and military medical disability.
Determining the optimal cut point for pain catastrophizing has research implications for comparing studies that examine the associations between pain catastrophizing and pain outcomes. Future research studies using military medical disability as an outcome may use a PCS score of ≥20 as a cut point for higher risk. Given the inconsistent relationship between change in PCS and disability, this study also has research implications for responder analyses of therapies that target pain catastrophizing. The threshold of 20 may be a more meaningful measure of treatment success than use of a MCID. Additionally, given that only 30% of service members with high baseline PCS score reported improvement to the low range during pain specialty care, future research should be directed at identifying other therapeutic approaches targeted at improving pain catastrophizing.
This study contributes to the research foundation for further exploration of the mechanisms by which pain catastrophizing may lead to military medical disability and occupational disability in other populations. Network analysis has shown that pain self-efficacy, fear avoidance and perceived disability are key constructs in the relationship between pain and affective disorder symptoms.40 Future network analyses that include pain catastrophizing in the models would aid in the determination of which factors are most strongly correlated with medical disability and related outcomes. Ultimately, longitudinal analyses are recommended to explore causal relationships between these interrelated factors.
This study has important clinical implications. In clinical practice, a PCS score of ≥20 in service members may be considered a positive screen for higher risk of future disability. Identifying this high-risk population earlier in the course of their pain care may help with planning early interventions that may change the disability trajectory. The Military Health System endorses a “Stepped Care Model” of pain management, which includes screening for pain at primary care visits and enhanced access to rehabilitation specialists and psychologists.41 Psychologists imbedded in military primary care clinics undergo training in brief cognitive behavioral therapy for chronic pain. The Stepped Care Model could be leveraged by measuring pain catastrophizing in service members with acute and chronic pain who do not respond to first-line therapies. Service members with high pain catastrophizing should be offered cognitive behavioral and rehabilitative therapies within the primary care setting. Those whose scores remain high despite these approaches could then be referred to military pain specialty clinics for more intensive multimodal approaches. PCS may also be used to identify patients who may benefit from treatments that target pain catastrophizing prior to engagement in intensive pain rehabilitation programs, ie, programs involving at least 20 hours per week or at least 80 total hours of therapy by a coordinated team drawn from at least two disciplines that include psychological and exercise therapies. Secondary analysis of data collected during a randomized clinical trial of service members who engaged in an intensive pain rehabilitation program at the same clinic as the present study, lower baseline pain catastrophizing was found to be a predictor of sustained improvement in functional performance up to 6 months following treatment.42 Thus, offering treatments that target pain catastrophizing to those with high baseline pain catastrophizing prior to intensive pain rehabilitation may enhance functional outcomes. For example, at the study site, six weekly group sessions of a cognitive behavioral therapy for chronic pain are now a prerequisite for participation in an intensive pain rehabilitation program.
Limitations
The primary limitation of the study is that due to the retrospective study design, we cannot be certain whether high levels of pain catastrophizing cause a higher risk of disability or if pain conditions and comorbidities that are inherently more disabling cause more pain catastrophizing. While it is likely that therapies offered by the clinic, such as cognitive behavioral therapy, physical treatments, medications18 and interventional therapies contributed to any observed PCS improvement, it is possible that improvement in PCS may have been the result rather than the cause of stabilization or improvement of the pain condition and reduced disability.
We did not have data on the distribution of military occupational specialties between groups, which could have had confounding effects. Service members in military occupations requiring the most rigorous functional conditioning, such as infantrymen, have higher functional thresholds than others to remain on active duty. Likewise, we did not have data on combat history which is likely to play a role in the development of pain catastrophizing. Moreover, we did not adjust for symptoms of other psychological conditions such as depression, anxiety and posttraumatic stress disorder, which may also have had confounding effects on subsequent disability. In addition, the subpopulation who completed follow-up PCS allowing calculation of change in PCS scores had a higher proportion with moderate or severe self-reported functional impairment and higher rate of disability than the total population. This is likely because service members with pain conditions that were more disabling had a greater number of follow-up visits to the IPMC and therefore more requests from clinic staff to complete PASTOR (and hence PCS) reassessments. Therefore, the impact of PCS score on disability observed in the subset population may not be representative of the overall population of Army service members referred for pain specialty care. Also, because we studied a population of service members referred to an IPMC, our results may not be representative of service members or non-military populations with chronic pain who are managed in primary care practices. Lastly, because the study team did not have access to disability data for Navy, Air Force, Marine Corps and Coast Guard service members, we cannot extrapolate our findings to other branches of the US Armed Forces.
Conclusions
Pain catastrophizing is a modifiable correlate of occupational disability. This study found a correlation between pain catastrophizing and military disability but was limited by retrospective design and limited or lack of data on other factors that may contribute to this relationship, such as combat history and military occupation. Future prospective research that includes analysis of these factors is warranted to determine if treatments that lower pain catastrophizing, such as cognitive behavioral, physical, and pharmacological therapies,23 improve work-related outcomes in military populations.
Abbreviations
AUC, area under the curve; CBT, cognitive behavioral therapy; IDES, Integrated Disability Evaluation System; IPMC, interdisciplinary pain management center; MAMC, Madigan Army Medical Center; MCID, minimal clinically important difference; NIH, National Institutes of Health; PCS, Pain catastrophizing scale; PROMIS, Patient reported outcomes measurement information system; ROC, receiver operating characteristic; US, United States.
Data Sharing Statement
The data sharing agreement with the Defense Health Agency who provided data for this analysis to the research team does not authorize release of data used for this analysis. Requests for data access may be directed to the corresponding author, who will request authorization of release from the Defense Health Agency.
Ethics Approval and Informed Consent
The study protocol was determined to meet the revised Common Rule by the MAMC Human Research Protections Office, complies with the Declaration of Helsinki, and was approved by the MAMC Institutional Review Board, protocol number 218052. The study involved retrospective analysis of de-identified data; therefore, informed consent was waived.
Acknowledgments
The authors wish to extend their appreciation to Norma Bowling of Kennell and Associates in support of the Defense Health Agency Enterprise Intelligence and Data Solutions Program Management Office for her data management support. Tandem Editing LLC provided professional editing support.
The views expressed are those of the authors and do not reflect the policy or position of the Department of the Army, Department of Defense, the NIH or its HEAL Initiative or the US Government. The content is solely the responsibility of the authors. The investigators adhered to the policies for protection of human subjects as prescribed in 45 CFR 46. No nonhuman animal species were used in the conduct of this research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Institutes of Health (NIH) through the NIH HEAL Initiative under award number K24AT011995.
Disclosure
All the authors report no financial relationships or other conflicts of interests related to this work.
References
1. Wertli MM, Burgstaller JM, Weiser S, Steurer J, Kofmehl R, Held U. Influence of catastrophizing on treatment outcome in patients with nonspecific low back pain: a systematic review. Spine. 2014;39(3):263–273. doi:10.1097/BRS.0000000000000110
2. Schumann ME, Coombes BJ, Gascho KE, et al. Pain catastrophizing and pain self-efficacy mediate interdisciplinary pain rehabilitation program outcomes at posttreatment and follow-up. Pain Med Malden Mass. 2022;23(4):697–706. doi:10.1093/pm/pnab271
3. Mollow JM, Pendergrass TL, Lee IE, Chervak MC, Hauret KG, Rhon DI. Musculoskeletal injuries and United States Army readiness, part I: overview of injuries and their strategic impact. Mil Med. 2020;185(9–10):e1461–31471. doi:10.1093/milmed/usaa027
4. Reif S, Adams RS, Ritter GA, Williams TV, Larson MJ. Prevalence of pain diagnoses and burden of pain among active duty soldiers, FY2012. Mil Med. 2018;183(9–10):e330–e337 . doi:10.1093/milmed/usx200
5. Smith HJ, Taubman SB, Clark LL. Characterizing the contribution of chronic pain diagnoses to the neurologic burden of disease, active component, U.S. Armed Forces, 2009–2018. MSMR US Army Cent Health Promot Prev Med Exec Commun Div. 2020;27(10):2–7.
6. Toblin RL, Quartana PJ, Riviere LA, Walper KC, Hoge CW. Chronic pain and opioid use in US soldiers after combat deployment. JAMA Intern Med. 2014;174(8):1400–1401. doi:10.1001/jamainternmed.2014.2726
7. Skelly AC, Chou R, Dettori JR, et al. AHRQ Comparative Effectiveness Review, no. 227. Noninvasive nonpharmacological treatment for chronic pain: a systematic review update; 2020. Available from: https://www.ncbi.nlm.nih.gov/books/NBK556229/.
8. Weber N, Egbert J, Kelly A, et al. Disability evaluation system analysis and research (DESAR) 2022 annual report. Available from: https://apps.dtic.mil/sti/pdfs/AD1190001.pdf.
9. Headquarters Department of the Army. Army regulation 40-501. Standards of medical fitness. Headquarters department of the army; 2019. Available from: https://armypubs.army.mil/ProductMaps/PubForm/Details.aspx?PUB_ID=1004688.
10. US Army Public Health Center. Health of the Force: create a Healthier Force for Tomorrow. Aberdeen Proving Ground; 2021. Available from: https://phc.amedd.army.mil/topics/campaigns/hof/Pages/default.aspx.
11. Headquarters Department of the Army. Army Regulation 40-502. Medical Readiness. Headquarters department of the army; 2019. Available from: https://armypubs.army.mil/epubs/DR_pubs/DR_a/ARN37126-AR_40-502-001-WEB-3.pdf.
12. Sullivan MJL, Bishop SR, Pivik J. The pain catastrophizing scale: development and validation. Psychol Assess. 1995;7:524–532. doi:10.1037/1040-3590.7.4.524
13. Wheeler CHB, Williams ACC, Morley SJ. Meta-analysis of the psychometric properties of the pain catastrophizing scale and associations with participant characteristics. Pain. 2019;160(9):1946–1953. doi:10.1097/j.pain.0000000000001494
14. Cook KF, Kallen MA, Buckenmaier C, et al. Evaluation of the validity and response burden of patient self‐report measures of the pain assessment screening tool and outcomes registry (PASTOR). Mil Med. 2017;182(7/8):
15. Buckenmaier CC, Galloway KT, Polomano RC, McDuffie M, Kwon N, Gallagher RM. Preliminary validation of the Defense and Veterans Pain Rating Scale (DVPRS) in a military population. Pain Med. 2013;14(1):110–123. doi:10.1111/j.1526-4637.2012.01516.x
16. Pilkonis PA, Choi SW, Reise SP, et al. Item banks for measuring emotional distress from the patient-reported outcomes measurement information System (PROMIS®): depression, anxiety, and anger. Assessment. 2011;18(3):263–283. doi:10.1177/1073191111411667
17. Amtmann D, Cook KF, Jensen MP, et al. Development of a PROMIS item bank to measure pain interference. Pain. 2010;150(1):173–182. doi:10.1016/j.pain.2010.04.025
18. Hays RD, Bjorner JB, Revicki DA, Spritzer KL, Cella D. Development of physical and mental health summary scores from the patient-reported outcomes measurement information system (PROMIS) global items. Qual Life Res. 2009;18(7):873–880. doi:10.1007/s11136-009-9496-9
19. Northwestern University. PROMIS score cut points. HealthMeasures. Northwestern University. Available from: https://staging.healthmeasures.net/score-and-interpret/interpret-scores/promis/promis-score-cut-points.
20. Prins A, Bovin MJ, Smolenski DJ, et al. The primary care PTSD screen for DSM-5 (PCPTSD-5): development and evaluation within a veteran primary care sample. J Gen Intern Med. 2016;31(10):1206–1211. doi:10.1007/s11606-016-3703-5
21. Liu X. Classification accuracy and cut point selection. Stat Med. 2012;31(23):2676–2686. doi:10.1002/sim.4509
22. Sullivan MJL. Pain Catastrophizing Scale Manual; 2019. Available from: https://dokumen.tips/documents/pain-catastrophizing-scale-manual-sullivan.html.
23. Schütze R, Rees C, Smith A, Slater H, Campbell JM, O’Sullivan P. How can we best reduce pain catastrophizing in adults with chronic noncancer pain? A systematic review and meta-analysis. J Pain. 2018;19(3):233–256. doi:10.1016/j.jpain.2017.09.010
24. Pierobon A, Raguzzi I, Soliño S, et al. Disability is associated with catastrophizing and not with pain intensity in patients with low back pain: a retrospective study. Physiother Res Int J Res Clin Phys Ther. 2020;25(4):e1867. doi:10.1002/pri.1867
25. Scott W, Wideman TH, Sullivan MJL. Clinically meaningful scores on pain catastrophizing before and after multidisciplinary rehabilitation: a prospective study of individuals with subacute pain after whiplash injury. Clin J Pain. 2014;30(3):183–190. doi:10.1097/AJP.0b013e31828eee6c
26. Smith SM, Dworkin RH, Turk DC, et al. Interpretation of chronic pain clinical trial outcomes: IMMPACT recommended considerations. Pain. 2020;161(11):2446–2461. doi:10.1097/j.pain.0000000000001952
27. Cashin AG, Lee H, Traeger AC, et al. Producing clinically meaningful reductions in disability: a causal mediation analysis of a patient education intervention. J Pain. 2022;23(2):236–247. doi:10.1016/j.jpain.2021.07.007
28. Monticone M, Portoghese I, Rocca B, Giordano A, Campagna M, Franchignoni F. Responsiveness and minimal important change of the pain catastrophizing scale in people with chronic low back pain undergoing multidisciplinary rehabilitation. Eur J Phys Rehabil Med. 2022;58(1):68–75. doi:10.23736/S1973-9087.21.06729-0
29. de Vries HJ, Reneman MF, Groothoff JW, Geertzen JHB, Brouwer S. Workers who stay at work despite chronic nonspecific musculoskeletal pain: do they differ from workers with sick leave? J Occup Rehabil. 2012;22(4):489–502. doi:10.1007/s10926-012-9360-6
30. de Vries HJ, Reneman MF, Groothoff JW, Geertzen JHB, Brouwer S. Factors promoting staying at work in people with chronic nonspecific musculoskeletal pain: a systematic review. Disabil Rehabil. 2012;34(6):443–458. doi:10.3109/09638288.2011.607551
31. Carriere JS, Thibault P, Milioto M, Sullivan MJL. Expectancies mediate the relations among pain catastrophizing, fear of movement, and return to work outcomes after whiplash injury. J Pain. 2015;16(12):1280–1287. doi:10.1016/j.jpain.2015.09.001
32. Moore E, Thibault P, Adams H, Sullivan MJL. Catastrophizing and pain-related fear predict failure to maintain treatment gains following participation in a pain rehabilitation program. Pain Rep. 2016;1(2):e567. doi:10.1097/PR9.0000000000000567
33. Gilliam WP, Craner JR, Morrison EJ, Sperry JA. The mediating effects of the different dimensions of pain catastrophizing on outcomes in an interdisciplinary pain rehabilitation program. Clin J Pain. 2017;33(5):443–451. doi:10.1097/AJP.0000000000000419
34. López-Bravo MD, Zamarrón-Cassinello MD, Touche RL, Muñoz-Plata R, Cuenca-Martínez F, Ramos-Toro M. Psychological factors associated with functional disability in patients with hip and knee osteoarthritis. Behav Med Wash DC. 2021;47(4):285–295. doi:10.1080/08964289.2020.1813682
35. Lazaridou A, Franceschelli O, Buliteanu A, Cornelius M, Edwards RR, Jamison RN. Influence of catastrophizing on pain intensity, disability, side effects, and opioid misuse among pain patients in primary care. J Appl Biobehav Res. 2017;22(1):e12081. doi:10.1111/jabr.12081
36. Hooten MW. chronic pain and mental health disorders: shared neural mechanisms, epidemiology, and treatment. Mayo Clin Proc. 2016;91(7):955–970. doi:10.1016/j.mayocp.2016.04.029
37. Murphy JL, Palyo SA, Schmidt ZS, et al. The resurrection of interdisciplinary pain rehabilitation: outcomes across a veterans affairs collaborative. Pain Med Malden Mass. 2021;22(2):430–443. doi:10.1093/pm/pnaa417
38. Cassidy EL, Atherton RJ, Robertson N, Walsh DA, Gillett R. Mindfulness, functioning and catastrophizing after multidisciplinary pain management for chronic low back pain. Pain. 2012;153(3):644–650. doi:10.1016/j.pain.2011.11.027
39. Marshall PW, Morrison NMV, Gibbs M, Schabrun SM. The effect of exercise engagement on low back disability at 12-months is mediated by pain and catastrophizing in a community sample of people with chronic low back pain. Behav Res Ther. 2022;159:104205. doi:10.1016/j.brat.2022.104205
40. Thompson EL, Broadbent J, Fuller-Tyszkiewicz M, Bertino M, Staiger PK. A network analysis of the links between chronic pain symptoms and affective disorder symptoms. Int J Behav Med. 2019;26:59–68. doi:10.1007/s12529-018-9754-8
41. Defense Health Agency Administrative Instruction 6025.08. Pain management and opioid safety in military medical treatment facilities, February 8, 2023; 2023. Available from: https://health.mil/Reference-Center/DHA-Publications/2023/02/08/DHA-AI-6025-08.
42. Flynn DM, Burke LA, Ransom JC, et al. Predictors of sustained response to functional restoration in a military population. Military Medicine; 2022.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.