Back to Journals » Journal of Pain Research » Volume 15
Loneliness and Pain Catastrophizing Among Individuals with Chronic Pain: The Mediating Role of Depression
Authors Wilson JM, Colebaugh CA, Meints SM, Flowers KM, Edwards RR, Schreiber KL ![]()
Received 8 June 2022
Accepted for publication 11 August 2022
Published 16 September 2022 Volume 2022:15 Pages 2939—2948
DOI https://doi.org/10.2147/JPR.S377789
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jonathan Greenberg
Jenna M Wilson, Carin A Colebaugh, Samantha M Meints, K Mikayla Flowers, Robert R Edwards, Kristin L Schreiber
Department of Anesthesiology, Perioperative, and Pain Medicine, Brigham & Women’s Hospital, Harvard Medical School, Boston, MA, USA
Correspondence: Jenna M Wilson, Brigham and Women’s Hospital, Harvard Medical School, 45 Francis St, Boston, MA, 02115, USA, Tel +1 7813673972, Email [email protected]
Purpose: Loneliness increased during the COVID-19 pandemic and social distancing guidelines, potentially exacerbating negative cognitions about pain. The present study investigated the longitudinal relationship between loneliness, assessed during the early weeks of the pandemic, and pain catastrophizing, assessed after living in the pandemic for approximately 1 year, among chronic pain patients. We also examined whether severity of depressive symptoms mediated this association.
Methods: This prospective longitudinal study recruited individuals with chronic pain (N=93) from Massachusetts using an online convenience sampling method via the platform Rally. Participants completed an initial survey early after the onset of social distancing (4/28/20– 6/17/20; Time 1) and a follow-up survey 1 year later (5/21/21– 6/7/21; Time 2). Participants completed validated assessments of loneliness (T1), pain catastrophizing (T2), and depression (T2). Spearman correlations and Mann–Whitney U-tests were used to explore associations among psychosocial, pain, and participant characteristics. A mediation analysis was conducted to test whether the association between loneliness and pain catastrophizing was mediated by depression.
Results: Participants had a mean age of 40.6 years and were majority female (80%) and White (82%). Greater loneliness was associated with subsequent higher pain catastrophizing (b=1.23, 95% CI [0.03, 2.44]). Mediation analysis showed a significant indirect effect (b=0.57, 95% CI [0.10, 1.18) of loneliness (T1) on catastrophizing (T2) through depression (T2) while accounting for several important covariates. The direct effect of loneliness on catastrophizing was no longer significant when depression was included in the model (b=0.66, 95% CI [− 0.54, 1.87]).
Conclusion: Findings suggest that greater loneliness during the pandemic was associated with higher pain catastrophizing 1 year later, and severity of depression after living in the pandemic mediated this association. As loneliness, depression, and catastrophizing can all be modified with behavioral interventions, understanding the temporal associations among these variables is important for the employment of future empirically supported treatments.
Keywords: loneliness, pain catastrophizing, depression, chronic pain, COVID-19
Introduction
The COVID-19 pandemic and social distancing guidelines had widespread physical and mental health consequences among adults in the U.S.,1–3 with studies also showing increased levels of loneliness.4–6 Individuals with chronic pain may have been particularly at risk of social and physical isolation as a result of social distancing guidelines, which could consequently exacerbate pain.7 Indeed, one study showed that patients with chronic pain reported higher levels of loneliness, pain severity, pain catastrophizing, and depression compared to healthy adults.8 Despite the fact that many states have now relaxed social distancing guidelines, a lasting impact of prolonged isolation persists, making it critical to understand the long-term impact in the current recovery and to also help plan for potential future waves of social distancing.
The biopsychosocial model of pain acknowledges the contribution of social and psychological factors to the pain experience.9 Pain catastrophizing (ruminating about, magnification of, and feelings of helplessness in the face of pain) is a psychological factor associated with greater pain intensity and interference.10,11 Because pain catastrophizing is a modifiable risk factor,12 it is important to explore what is associated with increased catastrophizing to inform behavioral interventions for reducing pain. Pre-pandemic, one study showed that loneliness predicted greater pain-related catastrophic thoughts.13 Due to social distancing guidelines during the pandemic, it is plausible that loneliness among individuals with chronic pain may longitudinally be associated with higher catastrophizing, although this has yet to be demonstrated.
Further, it is unknown what may explain the association between loneliness and catastrophizing, but one such factor may be depression. Loneliness is related to worse overall mental health,14 as well as increased depression during the pandemic.5,15,16 Theoretically, while loneliness refers to an individual’s feelings about their social relationships, and depression refers to how an individual feels more generally, loneliness and depression are separate constructs that may be importantly linked.17 Several longitudinal studies, conducted pre-pandemic, showed that loneliness predicted increased depressive symptomology, but this has yet to be tested within the context of heightened social isolation, which occurred as a result of the social distancing guidelines.18,19 Chronic pain is often comorbid with depression,20,21 and among individuals with chronic pain, depression is associated with greater pain catastrophizing.22–24 Importantly, depression and catastrophizing are considered conceptually distinct constructs, as depression refers to a more general mood disorder.25 Therefore, depression may link loneliness and pain catastrophizing, potentially mediating their association. Identifying depression as a link between loneliness and pain catastrophizing has important clinical implications, including early identification of at-risk patients to facilitate behavioral interventions and address depressive symptomology. Early treatment of depressive symptoms may simultaneously prevent worsened pain catastrophizing among chronic pain patients during times of increased isolation.
This prospective cohort study investigated the longitudinal relationship between loneliness experienced by individuals with chronic pain, assessed during the early weeks of the COVID-19 pandemic, and pain catastrophizing assessed after living in the pandemic for approximately 1 year. Further, we examined whether severity of depressive symptoms, after living in the pandemic for 1 year, mediated the association between loneliness and pain catastrophizing.
Materials and Methods
Participants and Procedure
This study recruited adults with chronic pain from Massachusetts and was approved by the Partners Human Research Committee/Institutional Review Board. Due to the conditions of the COVID-19 pandemic (eg, social distancing restrictions), we used an online survey to recruit a convenience sample. Participants were recruited using an online platform (Rally) that connects the public to research studies that they may be eligible to participate in. We also contacted participants from our previous pain cohorts (eg, mastectomy, total knee replacement, fibromyalgia, back pain) via email. Eligibility criteria included being at least 18 years of age, a Massachusetts resident, English speaking, and having self-reported persistent pain for ≥3 months. The survey was only open to residents of MA to try and control for discrepancies between ongoing state-ordered social distancing mandates at the time of the survey. After confirming that each participant met our eligibility criteria, they were emailed a separate link to REDCap, which is a secure data entry system, to participate in the survey. All participants provided electronic informed consent before participating in the study.
The first survey (Time 1; T1) was sent out to participants during the early weeks of the pandemic, from April 28-June 17, 2020. A total of 150 participants completed the survey at T1 (Figure 1). All participants were asked whether they were willing to be contacted for future studies, and 147 indicated that they were. All 147 participants who were willing to be contacted for future studies were invited to participate in a follow-up survey (Time 2; T2), which was completed approximately 1 year later from May 21 to June 7, 2021. The second survey (T2) was sent out to participants when social distancing mandates were beginning to be lifted after more people were vaccinated (see Figure 1). Ninety-four participants (63% response rate) completed the follow-up survey. One participant did not complete the UCLA loneliness scale (T1) and was excluded from analyses. For each survey participants completed, they were compensated with a $20 Amazon electronic gift code. Surveys took approximately 30–45 minutes to complete.
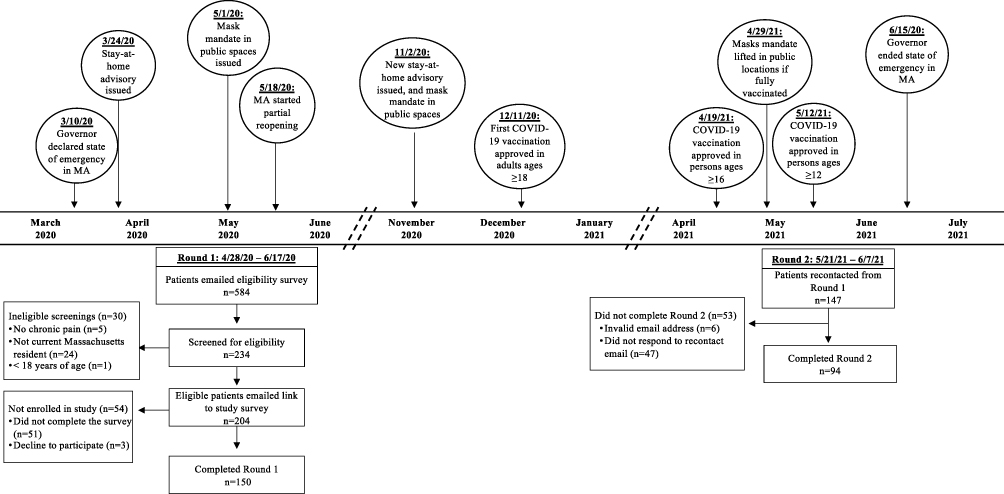 |
Figure 1 Study timeline in relation to the COVID-19 pandemic in Massachusetts. The timeline includes key dates relevant to social distancing mandates in Massachusetts around the time of survey administrations. |
Measures
Loneliness
During the early weeks of the pandemic (T1), the 3-item UCLA Loneliness Scale Version 326 was used to assess loneliness. Items (eg, “How often do you feel that you lack companionship?”) were rated on a scale from 1 (hardly ever) to 3 (often) and summed for a total score (α=0.76). Scores range from 3 to 9, and higher scores indicate greater feelings of loneliness. This scale has shown convergent and discriminant validity and demonstrated adequate internal reliability (α=0.72) in prior work.26 In prior research, scores ≥6 have been used as a cut-off point for significant loneliness.27,28
Pain Catastrophizing
The 13-item Pain Catastrophizing Scale29 was used to assess negative, maladaptive cognitions associated with pain at T1 and T2. Items (eg, “I worry all the time about whether the pain will end”) were rated on a scale from 0 (not at all) to 4 (all the time). Total scores were computed separately for T1 and T2 by summing all items, with a total possible score of 52 (αs=0.96–0.97). Higher scores reflect greater pain catastrophizing. The PCS has shown acceptable internal reliability (α=0.87) and concurrent and discriminant validity in pain and control populations.29,30 In prior research, a PCS score ≥ 16 has been used to represent clinically relevant levels of catastrophizing.31,32
Depression
The 8-item depression short form from the Patient Reported Outcome Measurement Information System (PROMIS)33 was used to measure depressive symptoms at T2. All items (eg, “I felt unhappy”; “I felt worthless”) were rated on a scale from 1 (never) to 5 (always), and items were summed for a total score (α=0.96). Scores range from 8 to 40, and higher scores indicate greater severity of depression. The PROMIS depression short form has shown acceptable internal reliability (α=0.95) and construct validity in prior work.33 Per the standard scoring, scores ranging from 8 to 16 are considered to be “None to slight” depressive symptoms; 17 to 22 are considered to be “Mild” depressive symptoms; 23 to 32 are considered to be “Moderate” depressive symptoms; and scores ≥33 are considered to be “Severe” depressive symptoms.
Potential Covariates
At T1, participants answered several questions related to their chronic pain. These variables were explored as potential covariates to examine the unique effect of loneliness on pain catastrophizing. Additionally, these pain variables were chosen because prior research has shown that they are related to pain catastrophizing,10,34,35 as well as to loneliness.36,37 One item from the Brief Pain Inventory38 (BPI) assessed participants’ pain severity (ie, “Rate your pain on average”) on a scale from 0 (no pain) to 10 (worst pain imaginable). Seven items from the BPI assessed how much pain interfered with participants’ daily activities (eg, “How has your pain interfered with your walking ability?”) on a scale from 0 (my pain did not interfere) to 10 (my pain completely interfered). The seven items were summed for a total pain interference score (range: 0–70, α=0.91). The BPI has shown high internal reliability (αs= 0.89–0.92) and construct validity in chronic pain samples.38,39 Participants were also asked “Do you typically take any medications for your pain?”. Response options were “yes” or “no”. If participants selected “yes”, then they were asked about their use of over-the-counter medications (eg, Ibuprofen), opioids (eg, Morphine), non-opioids (eg, Gabapentin), and marijuana. Participants also reported their age, education, race, income, and marital status.
Analytic Approach
Non-parametric tests were used to report basic descriptive statistics and explore associations between loneliness, pain catastrophizing, depression, and potential covariates (Table 1). Spearman correlations were conducted to explore the association of pain catastrophizing with continuous variables and Mann–Whitney U-tests were used to explore the association of pain catastrophizing with categorical variables. Mediation analysis was conducted using the PROCESS macro for SPSS. PROCESS is a regression path analysis modeling tool used to estimate direct and indirect effects of mediator models.40 The mediation model used 5000 bootstrapped samples to test the total exposure–outcome effect, and that the association between loneliness (T1) and pain catastrophizing (T2) was mediated by severity of depression (T2) (Figure 2). Participant characteristics that were significantly related to pain catastrophizing (dependent variable) were included in the model as covariates. A post-hoc power analysis indicated that a sample of 68 participants was necessary to detect a medium-sized effect (f 2=0.15) of a predictor in a multiple linear regression (eg, mediation analysis), assuming power is 0.80 and α = 0.05.41
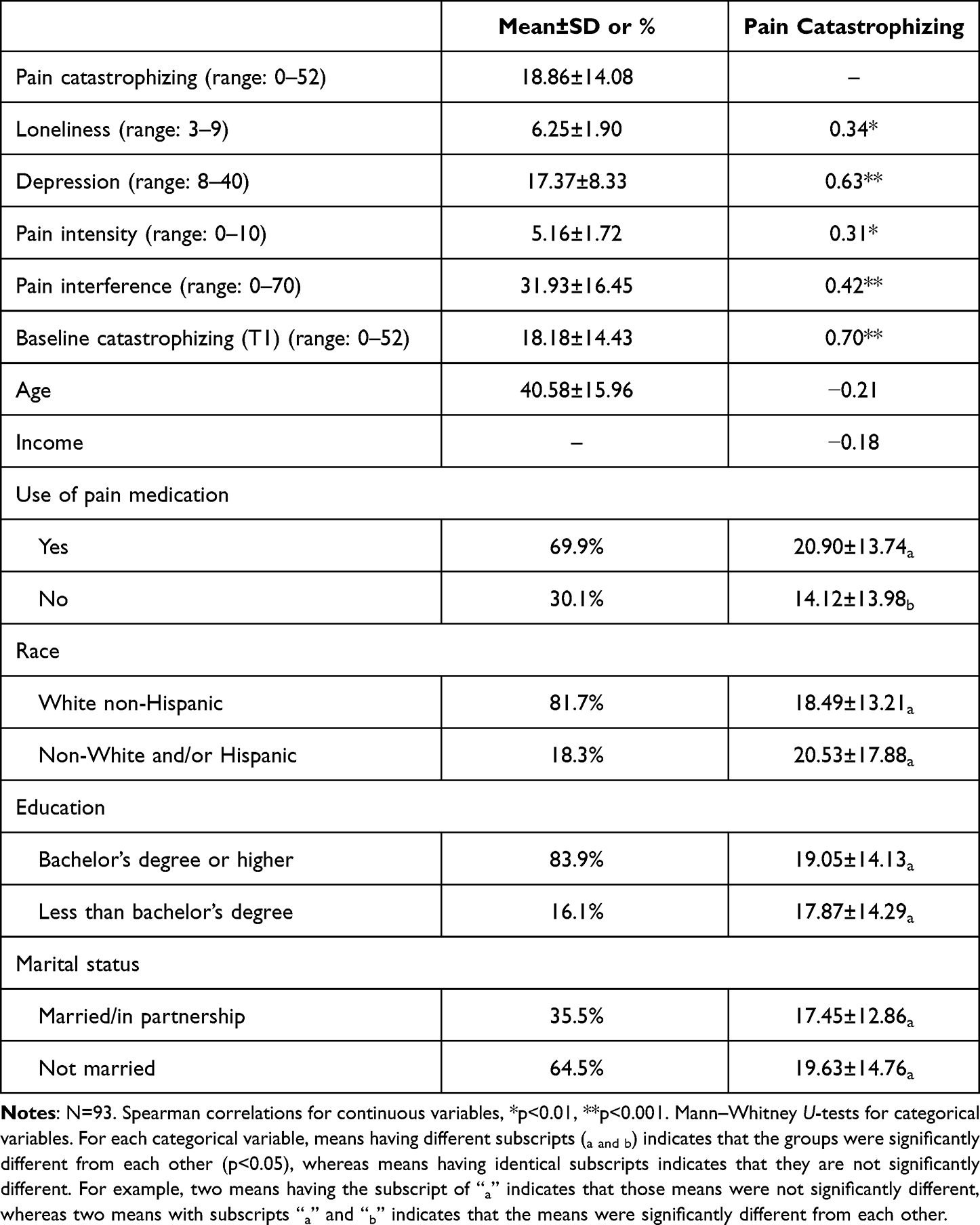 |
Table 1 Associations Among Participant Characteristics (T1) and Pain Catastrophizing (T2) |
 |
Figure 2 Causal mediation model testing the total exposure–outcome effect. |
Results
Sample Characteristics
Overall, this sample of participants (n=93) with chronic pain had a mean age of 40.6 years (SD = 16.0) and was majority female (80%), White (82%), and self-reported having a college degree or higher (84%). The majority of participants also reported being married/in a partnership (36%). Participants self-reported the nature of their chronic pain with approximately 59% reporting back pain, 24% fibromyalgia, 7% postsurgical pain, and 63% of the participants indicated other sources (eg, arthritis, knee pain) of chronic pain. On average, participants reported a pain severity score of 5.2 (SD = 1.7) and pain interference score of 31.9 (SD = 16.5). Use of any pain medication was common (70%), with approximately 58% taking over the counter medication, 15% taking opioids, and 22% using marijuana.
Based on prior research using the UCLA Loneliness Scale Version 3 with a cut-off point of ≥6,27,28 the prevalence of loneliness, assessed during the early weeks of the pandemic (T1), was 66%. Using a cut-off point of scores ≥16 on the PCS,31,32 52% of the sample reported high levels of pain catastrophizing after living in the pandemic for 1 year (T2). Based on established cut-off categories for depression,33 after living in the pandemic for 1 year (T2), 56% of the sample reported “none to slight” depressive symptoms, 17% reported “mild” depressive symptoms, 24% reported “moderate” depressive symptoms, and 3% reported “severe” depressive symptoms.
Chi-square and Mann–Whitney U-tests revealed that participants who did not complete the follow-up survey at T2 did not significantly (n=56, 37%) differ from those who did complete the follow-up survey based on any demographic characteristics (ie, age, gender, race, education, income, or marital status), or on T1 scores of loneliness, depression, and pain catastrophizing (ps>0.05).
Variables Associated with Pain Catastrophizing After 1 Pandemic Year
Spearman correlations and Mann–Whitney U-tests were conducted to assess associations among pain catastrophizing, loneliness, depression, and potential covariates (Table 1), with a focus on the relation of variables to pain catastrophizing. Loneliness was significantly correlated with pain catastrophizing, such that greater feelings of loneliness were associated with higher levels of pain catastrophizing. Depression was also significantly correlated with pain catastrophizing, such that greater severity of depression was associated with higher levels of pain catastrophizing. Pain catastrophizing was associated with greater pain severity, greater pain interference, and use of pain medications. Participants’ demographic characteristics were not significantly associated with pain catastrophizing.
Mediation Analysis
A mediation analysis tested whether the association between loneliness (T1) and pain catastrophizing (T2) was mediated by depression (T2). Loneliness was entered as the predictor variable (x variable), depression was entered as a mediator (m variable), and pain catastrophizing was entered as the outcome variable (y variable) (Figure 3). Pain severity and interference, and use of pain medications at T1 were included as covariates. Additionally, T1 catastrophizing was included as a covariate to adjust for how catastrophizing may have changed over time.
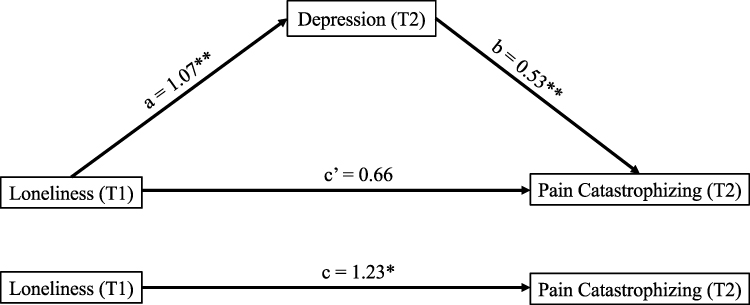 |
Figure 3 The mediating effect of depression after living in the pandemic for 1 year (T2) on the association between loneliness during the early weeks of the pandemic (T1) and pain catastrophizing after living in the pandemic for 1 year (T2), controlling for T1 pain intensity, pain interference, pain medication use, and baseline catastrophizing. *p<0.05, **p<0.01. |
The model predicting T2 pain catastrophizing was significant, F(6, 85)=18.19, p<0.001, R2=0.562. The direct effect of loneliness on pain catastrophizing, while controlling for covariates, was significant (b=1.23, 95% CI [0.03, 2.44]). Loneliness was also significantly associated with greater severity of depression (b=1.07, 95% CI [0.34, 1.80]), and depression was significantly associated with higher levels of pain catastrophizing (b=0.53, 95% CI [0.19, 0.87]). There was a significant indirect effect of loneliness on pain catastrophizing through depression (b=0.57, 95% CI [0.10, 1.18]), and the direct effect of loneliness on pain catastrophizing was no longer significant when depression was included in the model (b=0.66, 95% CI [−0.54, 1.87]). This finding suggests that loneliness during the early weeks of the pandemic was associated with higher levels of pain catastrophizing after living in the pandemic for 1 year, and greater severity of depression after living in the pandemic for 1 year mediated this relationship. We also conducted the mediation model without covariates, to test whether the associations and mediational pattern and significance may be altered by the inclusion of our control variables. When covariates were not included in the mediation model, the pattern and significance of findings remained the same.
Discussion
The recent period of mandated social distancing allowed a unique opportunity to examine the longer-term impact of social isolation among individuals with chronic pain. The present longitudinal study showed that greater feelings of loneliness during the early weeks of the pandemic were associated with subsequent higher levels of pain catastrophizing 1 year later. Further, the association between loneliness and pain catastrophizing was mediated by greater severity of depression.
Participants in this sample reported a mean score on the UCLA loneliness measure that was above the cut-off point for significant loneliness, and also somewhat higher than loneliness reported in other samples of individuals with chronic medical conditions (eg cardiovascular, autoimmune, metabolic) during the pandemic.4 This suggests that these individuals with chronic pain may have experienced heightened levels of loneliness and emphasizes the importance of understanding the long-term effects of social distancing among those with chronic pain. Our sample also exhibited relatively high levels of depression after living in the pandemic for 1 year, with approximately 26% of the sample reporting moderate-to-severe depressive symptoms. This finding is in line with other research conducted during the pandemic.42,43 The mean score of pain catastrophizing after living in the pandemic for 1 year in the present study was higher than pain catastrophizing reported in some samples of individuals with chronic pain pre-pandemic,44 but lower than pain catastrophizing scores among other chronic pain samples pre- and during the pandemic.8,31 Importantly, we did not assess pre-pandemic levels of loneliness, depression, or pain catastrophizing, and therefore we are unable to attribute scores on these variables to the COVID-19 pandemic.
The prospective, longitudinal design of our study showed that loneliness was associated with higher pain catastrophizing 1 year later. This finding expands upon prior work13 by demonstrating this association during a time of heightened social isolation, over a longer timeframe, and while accounting for participants’ pain experiences and medication use. The present study also gives insight into this association by showing that depression may serve as a mediator, such that feeling lonely may contribute to depressed mood (hopelessness, helplessness), leading to more catastrophic cognitions about pain. Notably, an alternative mediation model tested whether depression during the early weeks of the pandemic contributed to greater feelings of loneliness 1 year later, contributing to more catastrophizing (Supplemental Material). This alternative model showed that loneliness did not serve as a significant mediator, providing further support for the temporal ordering of loneliness preceding depressive symptomology.18,19
Our findings provide potentially important clinical implications, suggesting that loneliness may influence catastrophic pain-related thoughts through depression, providing a viable point of intervention in the management of pain symptoms. Importantly, depression can be modified with behavioral interventions, such as cognitive behavioral therapy.45–47 Interventions targeting depressive symptomology among chronic pain patients may reduce catastrophizing pain-related thinking and may be particularly essential during times of heightened social isolation, such as the COVID-19 pandemic (eg, self-quarantining). Because prior work suggests that reducing catastrophic pain-related cognitions improves pain management,45 targeting depressive symptoms may be one strategy by which pain catastrophizing decreases and pain management improves. Future studies may benefit from investigating the temporal associations among loneliness, depression, and catastrophizing over the course of empirically supported treatments in patients with chronic pain.
Our findings should be interpreted within the context of certain limitations. First, due to the method of convenience sampling required to obtain responses expediently during the timeframe after onset of social distancing, the sample was demographically skewed, with the majority of participants identifying as female, White, and with more formal education. Thus, the generalizability of the findings may be limited. For example, some research has shown that females report more frequent pain-related catastrophic thoughts than men,48 whereas other studies indicate no sex differences.49 It is important that future studies recruit a more demographically diverse sample from different geographic locations to further understand associations among these variables, as well as to replicate our findings to test generalizability. Second, due to the conditions of the pandemic and the online sampling strategy used, we compensated participants with an Amazon electronic gift code which may have impacted participants’ decision to complete our follow-up survey at T2 (63% response rate). Although Amazon gift codes are commonly used as an incentive to participate in online surveys, some research suggests that providing participants with cash may lead to a higher response rate.50 Third, our analysis was fundamentally based on associations between variables, and did not randomize participants to certain conditions, which limits the ability to draw causal associations. However, we demonstrated the temporal ordering of the independent variable (loneliness) and mediator (depression) by assessing the mediator at T2 instead of T1, which is a common approach when only having access to two time points of data.51,52
Conclusion
The present study demonstrated how loneliness during the early weeks of social distancing was associated with greater pain catastrophizing after living in the pandemic for approximately 1 year. Further, this association was mediated by severity of depression after living in the pandemic for 1 year. By studying the association between depression and pain catastrophizing within the context of a historically steep increase in isolation, this study afforded an opportunity to detect the relation more sensitively between isolation and negative cognitions about pain. Further, studying these associations and the mediational role of depression in this sample of patients with chronic pain is clinically important, in that it provides novel insights into how we may prioritize the employment of behavioral interventions to help individuals.
Ethics Approval
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Partners Human Research Committee (PHRC)/Institutional Review Board (IRB).
Consent to Participate
All participants provided electronic informed consent before participating in the study.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author upon request.
Funding
The conduct of this study was supported by a grant from the NIH/NIGMS: R35 GM128691.
Disclosure
There were no relevant conflicts of interests for any of the authors.
References
1. Daly M, Sutin AR, Robinson E. Longitudinal changes in mental health and the COVID-19 pandemic: evidence from the UK Household Longitudinal Study. Psychol Med. 2020;1–10. doi:10.1017/S0033291720004432
2. Pierce M, Hope H, Ford T, et al. Mental health before and during the COVID-19 pandemic: a longitudinal probability sample survey of the UK population. Lancet Psychiatry. 2020;7(10):883–892. doi:10.1016/S2215-0366(20)30308-4
3. Torales J, O’Higgins M, Castaldelli-Maia JM, Ventriglio A. The outbreak of COVID-19 coronavirus and its impact on global mental health. Int J Soc Psychiatry. 2020;66(4):317–320. doi:10.1177/0020764020915212
4. Elran-Barak R, Mozeikov M. One month into the reinforcement of social distancing due to the COVID-19 outbreak: subjective health, health behaviors, and loneliness among people with chronic medical conditions. Int J Environ Res Public Health. 2020;17(15):5403. doi:10.3390/ijerph17155403
5. Killgore WD, Cloonan SA, Taylor EC, Miller MA, Dailey NS. Three months of loneliness during the COVID-19 lockdown. Psychiatry Res. 2020;293:113392. doi:10.1016/j.psychres.2020.113392
6. Killgore WD, Cloonan SA, Taylor EC, Lucas DA, Dailey NS. Loneliness during the first half-year of COVID-19 lockdowns. Psychiatry Res. 2020;294:113551. doi:10.1016/j.psychres.2020.113551
7. Karos K, McParland JL, Bunzli S, et al. The social threats of COVID-19 for people with chronic pain. Pain. 2020;161(10):2229. doi:10.1097/j.pain.0000000000002004
8. Fallon N, Brown C, Twiddy H, et al. Adverse effects of COVID-19-related lockdown on pain, physical activity and psychological well-being in people with chronic pain. Br J Pain. 2021;15(3):357–368. doi:10.1177/2049463720973703
9. Gatchel RJ, Peng YB, Peters ML, Fuchs PN, Turk DC. The biopsychosocial approach to chronic pain: scientific advances and future directions. Psychol Bull. 2007;133(4):581. doi:10.1037/0033-2909.133.4.581
10. Quartana PJ, Campbell CM, Edwards RR. Pain catastrophizing: a critical review. Expert Rev Neurother. 2009;9(5):745–758. doi:10.1586/ern.09.34
11. Hruschak V, Flowers KM, Azizoddin DR, Jamison RN, Edwards RR, Schreiber KL. Cross-sectional study of psychosocial and pain-related variables among patients with chronic pain during a time of social distancing imposed by the coronavirus disease 2019 pandemic. Pain. 2021;162(2):619. doi:10.1097/j.pain.0000000000002128
12. Schütze R, Rees C, Smith A, Slater H, Campbell JM, O’Sullivan P. How can we best reduce pain catastrophizing in adults with chronic noncancer pain? A systematic review and meta-analysis. J Pain. 2018;19(3):233–256. doi:10.1016/j.jpain.2017.09.010
13. Wolf LD, Davis MC, Yeung EW, Tennen HA. The within-day relation between lonely episodes and subsequent clinical pain in individuals with fibromyalgia: mediating role of pain cognitions. J Psychosom Res. 2015;79(3):202–206. doi:10.1016/j.jpsychores.2014.12.018
14. Leigh-Hunt N, Bagguley D, Bash K, et al. An overview of systematic reviews on the public health consequences of social isolation and loneliness. Public Health. 2017;152:157–171. doi:10.1016/j.puhe.2017.07.035
15. Benke C, Autenrieth LK, Asselmann E, Pané-Farré CA. Lockdown, quarantine measures, and social distancing: associations with depression, anxiety and distress at the beginning of the COVID-19 pandemic among adults from Germany. Psychiatry Res. 2020;293:113462. doi:10.1016/j.psychres.2020.113462
16. Palgi Y, Shrira A, Ring L, et al. The loneliness pandemic: loneliness and other concomitants of depression, anxiety and their comorbidity during the COVID-19 outbreak. J Affect Disord. 2020;275:109. doi:10.1016/j.jad.2020.06.036
17. Weiss R. Loneliness: The Experience of Emotional and Social Isolation. Cambridge, MA: MIT Press; 1973.
18. Cacioppo JT, Hawkley LC, Thisted RA. Perceived social isolation makes me sad: 5-year cross-lagged analyses of loneliness and depressive symptomatology in the Chicago health, aging, and social relations study. Psychol Aging. 2010;25(2):453. doi:10.1037/a0017216
19. Cacioppo JT, Hughes ME, Waite LJ, Hawkley LC, Thisted RA. Loneliness as a specific risk factor for depressive symptoms: cross-sectional and longitudinal analyses. Psychol Aging. 2006;21(1):140. doi:10.1037/0882-7974.21.1.140
20. Dersh J, Polatin PB, Gatchel RJ. Chronic pain and psychopathology: research findings and theoretical considerations. Psychosom Med. 2002;64(5):773–786. doi:10.1097/01.psy.0000024232.11538.54
21. Fishbain DA. Approaches to treatment decisions for psychiatric comorbidity in the management of the chronic pain patient. Med Clin North Am. 1999;83(3):737–760. doi:10.1016/S0025-7125(05)70132-2
22. Elvery N, Jensen MP, Ehde DM, Day MA. Pain catastrophizing, mindfulness, and pain acceptance. Clin J Pain. 2017;33(6):485–495. doi:10.1097/AJP.0000000000000430
23. Keskindag B, Karaaziz M, Cirhinlioğlu FG. Dispositional pain catastrophising in non-clinical sample: the role of depression, perceived stress and social support. Curr Psychol. 2020;41:4457–4465.
24. Poulin PA, Romanow HC, Rahbari N, et al. The relationship between mindfulness, pain intensity, pain catastrophizing, depression, and quality of life among cancer survivors living with chronic neuropathic pain. Support Care Cancer. 2016;24(10):4167–4175. doi:10.1007/s00520-016-3243-x
25. Edwards RR, Cahalan C, Mensing G, Smith M, Haythornthwaite JA. Pain, catastrophizing, and depression in the rheumatic diseases. Nat Rev Rheumatol. 2011;7(4):216–224. doi:10.1038/nrrheum.2011.2
26. Hughes ME, Waite LJ, Hawkley LC, Cacioppo JT. A short scale for measuring loneliness in large surveys: results from two population-based studies. Res Aging. 2004;26(6):655–672. doi:10.1177/0164027504268574
27. Groarke JM, McGlinchey E, McKenna-Plumley PE, Berry E, Graham-Wisener L, Armour C. Examining temporal interactions between loneliness and depressive symptoms and the mediating role of emotion regulation difficulties among UK residents during the COVID-19 lockdown: longitudinal results from the COVID-19 psychological wellbeing study. J Affect Disord. 2021;285:1–9. doi:10.1016/j.jad.2021.02.033
28. Mullen RA, Tong S, Sabo RT, et al. Loneliness in primary care patients: a prevalence study. Ann Fam Med. 2019;17(2):108–115. doi:10.1370/afm.2358
29. Sullivan MJ, Bishop SR, Pivik J. The pain catastrophizing scale: development and validation. Psychol Assess. 1995;7(4):524. doi:10.1037/1040-3590.7.4.524
30. Van Damme S, Crombez G, Bijttebier P, Goubert L, Van Houdenhove B. A confirmatory factor analysis of the pain catastrophizing scale: invariant factor structure across clinical and non-clinical populations. Pain. 2002;96(3):319–324. doi:10.1016/S0304-3959(01)00463-8
31. Lazaridou A, Koulouris A, Devine JK, et al. Impact of daily yoga-based exercise on pain, catastrophizing, and sleep amongst individuals with fibromyalgia. J Pain Res. 2019;12:2915. doi:10.2147/JPR.S210653
32. Riddle DL, Wade JB, Jiranek WA, Kong X. Preoperative pain catastrophizing predicts pain outcome after knee arthroplasty. Clin Orthop Relat Res. 2010;468(3):798–806. doi:10.1007/s11999-009-0963-y
33. Cella D, Riley W, Stone A, et al. Initial adult health item banks and first wave testing of the patient-reported outcomes measurement information system (PROMIS™) network: 2005–2008. J Clin Epidemiol. 2010;63(11):1179. doi:10.1016/j.jclinepi.2010.04.011
34. Papaioannou M, Skapinakis P, Damigos D, Mavreas V, Broumas G, Palgimesi A. The role of catastrophizing in the prediction of postoperative pain. Pain Med. 2009;10(8):1452–1459. doi:10.1111/j.1526-4637.2009.00730.x
35. Sharifzadeh Y, Kao M-C, Sturgeon JA, Rico TJ, Mackey S, Darnall BD. Pain catastrophizing moderates relationships between pain intensity and opioid prescription: nonlinear sex differences revealed using a learning health system. Anesthesiology. 2017;127(1):136–146. doi:10.1097/ALN.0000000000001656
36. Boggero IA, Sturgeon JA, Arewasikporn A, Castro SA, King CD, Segerstrom SC. Associations of pain intensity and frequency with loneliness, hostility, and social functioning: cross-sectional, longitudinal, and within-person relationships. Int J Behav Med. 2019;26(2):217–229. doi:10.1007/s12529-019-09776-5
37. Karayannis NV, Baumann I, Sturgeon JA, Melloh M, Mackey SC. The impact of social isolation on pain interference: a longitudinal study. Ann Behav Med. 2019;53(1):65–74. doi:10.1093/abm/kay017
38. Cleeland C, Ryan K. Pain Assessment: Global Use of the Brief Pain Inventory. Singapore: Annals, academy of medicine; 1994.
39. Tan G, Jensen MP, Thornby JI, Shanti BF. Validation of the brief pain inventory for chronic nonmalignant pain. J Pain. 2004;5(2):133–137. doi:10.1016/j.jpain.2003.12.005
40. Hayes A. The PROCESS macro for SPSS and SAS (version 2.13)[Software]; 2013.
41. Erdfelder E, Faul F, Buchner A. GPOWER: a general power analysis program. Behav Res Methods Instrum Comput. 1996;28(1):1–11. doi:10.3758/BF03203630
42. Ettman CK, Abdalla SM, Cohen GH, Sampson L, Vivier PM, Galea S. Prevalence of depression symptoms in US adults before and during the COVID-19 pandemic. JAMA Netw open. 2020;3(9):e2019686–e2019686. doi:10.1001/jamanetworkopen.2020.19686
43. Wilson JM, Lee J, Fitzgerald HN, Oosterhoff B, Sevi B, Shook NJ. Job insecurity and financial concern during the COVID-19 pandemic are associated with worse mental health. J Occup Environ Med. 2020;62(9):686–691. doi:10.1097/JOM.0000000000001962
44. Lazaridou A, Martel MO, Cornelius M, et al. The association between daily physical activity and pain among patients with knee osteoarthritis: the moderating role of pain catastrophizing. Pain Med. 2019;20(5):916–924. doi:10.1093/pm/pny129
45. Burns JW, Day MA, Thorn BE. Is reduction in pain catastrophizing a therapeutic mechanism specific to cognitive-behavioral therapy for chronic pain? Transl Behav Med. 2012;2(1):22–29. doi:10.1007/s13142-011-0086-3
46. Käll A, Backlund U, Shafran R, Andersson G. Lonesome no more? A two-year follow-up of internet-administered cognitive behavioral therapy for loneliness. Internet Interv. 2020;19:100301. doi:10.1016/j.invent.2019.100301
47. Williams A, Eccleston C, Morley S. Psychological therapies for the management of chronic pain (excluding headache) in adults. Cochrane Database Syst Rev. 2012;11. doi:10.1002/14651858.CD007407.pub3
48. Sullivan MJ, Thorn B, Haythornthwaite JA, et al. Theoretical perspectives on the relation between catastrophizing and pain. Clin J Pain. 2001;17(1):52–64. doi:10.1097/00002508-200103000-00008
49. Edwards R, Augustson EM, Fillingim R. Sex-specific effects of pain-related anxiety on adjustment to chronic pain. Clin J Pain. 2000;16(1):46–53. doi:10.1097/00002508-200003000-00008
50. Birnholtz JP, Horn DB, Finholt TA, Bae SJ. The effects of cash, electronic, and paper gift certificates as respondent incentives for a web-based survey of technologically sophisticated respondents. Soc Sci Comput Rev. 2004;22(3):355–362. doi:10.1177/0894439304263147
51. Petrocchi N, Ottaviani C. Mindfulness facets distinctively predict depressive symptoms after two years: the mediating role of rumination. Pers Individ Dif. 2016;93:92–96. doi:10.1016/j.paid.2015.08.017
52. Biggs BK, Nelson JM, Sampilo ML. Peer relations in the anxiety–depression link: test of a mediation model. Anxiety Stress Coping. 2010;23(4):431–447. doi:10.1080/10615800903406543
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Factors Affecting the Psychological Well-Being of Health Care Workers During the COVID-19 Crisis
Alharthi MH, Alshomrani AT, Bazaid K, Sonpol HMA, Ibrahim IAE, Alashkar AM
Psychology Research and Behavior Management 2022, 15:1931-1942
Published Date: 28 July 2022
Subjective Sleep Disruption and Mood Disorders are Associated with the Risk of Chronic Pain in Patients with Obstructive Sleep Apnea
Liu L, Li X, Xue P, Wu M, Zeng S, Dai Y, Zhou J
Nature and Science of Sleep 2022, 14:2023-2032
Published Date: 7 November 2022
Pre- and Post-Pandemic (COVID-19) Mental Health of International Students: Data from a Longitudinal Study
Jamshaid S, Bahadar N, Jamshed K, Rashid M, Imran Afzal M, Tian L, Umar M, Feng X, Khan I, Zong M
Psychology Research and Behavior Management 2023, 16:431-446
Published Date: 15 February 2023
The Interconnection Between Social Support and Emotional Distress Among Individuals with Chronic Pain: A Narrative Review
Franqueiro AR, Yoon J, Crago MA, Curiel M, Wilson JM
Psychology Research and Behavior Management 2023, 16:4389-4399
Published Date: 27 October 2023
Longitudinal Problematic Social Media Use in Students and Its Association with Negative Mental Health Outcomes
Shannon H, Bush K, Shvetz C, Paquin V, Morency J, Hellemans KGC, Guimond S
Psychology Research and Behavior Management 2024, 17:1551-1560
Published Date: 8 April 2024