Back to Journals » Journal of Pain Research » Volume 18
Pain Intensity and Pain Catastrophizing Among Patients with Chronic Pain: The Mediating Effect of Self-Efficacy
Authors Li J ![]() , Cui Y
, Cui Y ![]() , Jia Q, Ouyang A, Hua Y
, Jia Q, Ouyang A, Hua Y
Received 4 November 2024
Accepted for publication 5 February 2025
Published 19 March 2025 Volume 2025:18 Pages 1361—1373
DOI https://doi.org/10.2147/JPR.S504498
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jonathan Greenberg
Jiayao Li,1,* Yi Cui,1,* Qiong Jia,2,* Anping Ouyang,3,* Yan Hua1
1Department of Nursing, Air Force Medical University, Xi’an City, Shaanxi Province, People’s Republic of China; 2Department of Hepatobiliary Surgery, Xijing Hospital, Air Force Medical University, Xi’an City, Shaanxi Province, People’s Republic of China; 3Department of Military Medical Psychology, Air Force Medical University, Xi’an City, Shaanxi Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yan Hua, Department of Nursing, Air Force Medical University, Xi’an, People’s Republic of China, Email [email protected]
Aim: This study aimed to explore the mediating role of sense of self-efficacy in the relationship between pain intensity and pain catastrophizing among chronic pain patients.
Methods: A questionnaire survey was administered to patients with chronic pain at the pain intervention departments of three tertiary hospitals in Shaanxi Province between July 2023 and July 2024. The visual analogue scale, chronic pain self-efficacy scale, and pain catastrophizing scale were used to assess the patients’ pain intensity, self-efficacy, and pain catastrophizing degree, respectively. SPSS 27.0 and Mplus 8.3 software were used for statistical analysis.
Results: This study included a total of 430 patients with chronic pain. The average score for catastrophizing pain among participants was 22.76 (score range 0– 52), which is considered moderate. Pain intensity and pain catastrophizing were significantly and positively correlated, and the findings found that chronic pain self-efficacy mediated the correlation between pain intensity and pain catastrophizing after controlling for sociodemographic and disease-related variables. In addition, chronic pain self-efficacy was found to be an important mediator, accounting for 32.5% of the total effect.
Conclusion: Among patients with chronic pain, chronic pain self-efficacy explains the relationship of pain intensity and pain catastrophizing. These findings imply that interventions that decrease pain intensity and increase patients’ sense of self-efficacy are beneficial for improving pain catastrophizing in this population.
Keywords: chronic pain, pain intensity, self-efficacy, pain catastrophizing, cross-sectional study
Introduction
Chronic pain refers to pain that persists or recurs for longer than three months and is linked to direct or potential tissue damage.1 Chronic pain is considered one of the leading causes of disability-adjusted life years worldwide. Approximately 20–30% of adults are affected by chronic pain, which places a heavy burden on individuals and the economy.2 Because chronic pain patients are affected by physiological mechanisms such as inflammation and sympathetic activation, they often experience sensory and emotional responses.3 Previous studies have confirmed that pain can be explained comprehensively in terms of sensory experiences (such as the intensity and location of pain), emotional experiences (such as fear and anxiety), and cognitive experiences (such as pain catastrophizing). However, pain catastrophizing is a negative cognitive and emotional response to pain and is characterized by feelings of helplessness, rumination, and amplification of the pain experience.4 Pain catastrophizing has been shown to be correlated with increased rates of depression, PTSD, and disability in previous clinical trials. Furthermore, pain catastrophizing is a prerequisite for adverse pain outcomes.5,6 However, most recent research has focused on the current situation of patients with chronic pain or has explored the correlation between pain catastrophizing and other factors. Therefore, it is necessary to explore more paths based on the current research status and to provide a theoretical foundation to improve patients’ pain catastrophizing.
Pain intensity is usually assessed via a visual analogue scale. Accurately assessing the severity of pain among chronic pain patients can help healthcare professionals implement individualized pain management. Previous studies have shown that pain catastrophizing is a psychological factor that is closely related to chronic pain, especially increased pain intensity and interference. Moreover, the characteristics of pain in patients with chronic pain affect the relationship between pain catastrophizing and pain-related outcomes, suggesting that pain perception may be a predictor of pain catastrophizing. Since pain catastrophizing is a modifiable risk factor, it is significant to explore the path relationship between pain intensity and increased pain catastrophizing to guide behavioral interventions that reduce pain. Previous studies have confirmed a significant correlation between pain intensity and catastrophizing, but the underlying mechanism remains unclear.
Chronic pain self-efficacy is considered a positive self-belief system that is related to individuals’ confidence playing the function when they are in pain.7 Chronic pain self-efficacy mainly involves beliefs about one’s ability to control pain, regulate associated emotions, and appropriately use pain management strategies.8 Currently, chronic pain self-efficacy is widely examined in the field of pain research. The related research has suggested that improvements in pain interference may be facilitated by an increase in treatment-related self-efficacy.9 In patients with chronic musculoskeletal pain, high self-efficacy is strongly associated with pain intensity.10 A study on the management of patients with shoulder pain also confirmed that chronic pain self-efficacy can reduce patients’ pain intensity.11 In addition to its effect on pain severity, changes in self-efficacy are also predictor of disability.12 Self-efficacy is considered to mediate the relationship between pain and disability. In summary, pain self-efficacy is closely related to patients’ pain experience and health outcomes, thus suggesting whether that healthcare professionals should consider incorporating psychological interventions such as self-efficacy into their routine pain management practices.
Currently, studies on pain intensity, self-efficacy, or pain catastrophizing have received scholarly attention. Previous studies have shown that self-efficacy plays a partial mediating role in pain catastrophizing and exercise adherence in postoperative patients with total knee arthroplasty.13 Wang et al14 demonstrated that pain catastrophizing could mediate the relationship between pain sensitivity and pain intensity in patients with chronic pain. Moreover, pain catastrophizing also played a role in the relationship between depression and pain intensity in patients with chronic pain.15 In addition to the mediating effects, it has been noted that in chronic knee osteoarthritis patients, pain catastrophizing and pain intensity were significantly and positively correlated.16 In hip patients, pain worsening was associated with their pain catastrophizing and pain self-efficacy.17 Despite the partial results of pain intensity, self-efficacy or pain catastrophizing studies, most of the studies included the two variables mentioned above. However, the effects of chronic pain self-efficacy on pain catastrophizing and whether chronic pain self-efficacy plays a mediating role between pain intensity and pain catastrophizing in Chinese chronic pain patients remain unclear and the research among the three still deserves to be explored in depth. In summary, we can find that explore the mechanisms by which there is a strong correlation between pain levels and pain catastrophizing in chronic pain patients can help to develop effective measures and intervention programs that can reduce pain catastrophizing in chronic pain patients. To summarize, we can consider to explore the role of self-efficacy on the relationship between pain intensity and pain catastrophizing in chronic pain patients based on the theoretical framework.
The theoretical framework of this study is based on an extended model of fear-avoidance theory, which provides a reference for exploring the relationship between pain intensity and pain catastrophizing among patients with chronic pain.18 According to this model, when individuals experience pain, they exhibit two very different response styles: confrontation and avoidance. Some patients trigger pain catastrophizing thinking during their pain experience, thus causing them to be hypervigilant to activity or behaviors that cause pain or injury, and then, they show avoidance responses. Adverse coping methods can lead to adverse consequences such as motor function disuse and negative emotions in patients. However, these physical and psychological problems can exacerbate an individual’s experience of pain, thus creating a vicious cycle. In this model, pain experience and pain catastrophizing are affected by susceptible pain perception and psychological factors. This study is based on an extended model of fear-avoidance theory and explores the role of pain intensity and self-efficacy in pain catastrophizing from the perspectives of pain perception and psychological factors.
Although there is a theoretical basis that can link pain intensity, chronic pain self-efficacy, and pain catastrophizing, there are still obvious gaps in the literature, and the way in which pain intensity affects patients’ pain catastrophizing pathways has not been fully explored. In addition to these insights, few studies have focused on the mediating effect of chronic pain self-efficacy on the relationship between pain intensity and pain catastrophizing among patients with chronic pain. To fill this gap, this study aimed to elucidate the complex interplay between pain intensity, self-efficacy, and pain catastrophizing, thus contributing to a more nuanced understanding of how self-efficacy affects the negative psychological experiences of people with pain. Research that uses self-efficacy as a mediating factor not only fills an important gap in existing research but also facilitates the development of targeted interventions that can enhance patients’ sense of self-efficacy and improve their overall well-being and effectiveness in terms of coping with negative psychological experiences.
Based on our literature review and theoretical framework, we propose the following hypotheses:
1. Pain intensity is positively correlated with pain catastrophizing.
2. The sense of self-efficacy in patients with chronic pain mediates the relationship between pain intensity and pain catastrophizing.
Methods
Design and Participants
This study was a cross-sectional descriptive study. A convenience sampling method was used to recruit 430 hospitalized patients from the interventional pain departments of three tertiary Grade A hospitals in Shaanxi Province from July 2023 to July 2024. The inclusion criteria were as follows: 1) pain lasting more than 3 months and clinically diagnosed as chronic pain; 2) age greater than 18 years; 3) normal communication skills; and 4) voluntary participation in this study and signing an informed consent form. The exclusion criteria were as follows: 1) additional severe ailments (such as serious heart, lung, kidney, or other organ diseases); 2) acute pain associated with a single clinical operation; and 3) mental or consciousness-related disorders. The required sample size was calculated using the following formula: Z2 1-α/ 2P(1-P) / δ2. Studies have shown that the prevalence of chronic pain in China is approximately 35.9%.19 Therefore, in this study, P = 0.359, α = 0.05, Z1-α/2 = 1.96, and δ = 0.05. The sample size calculated according to this formula was 354. Considering a potential 20% nonresponse rate, the minimum sample size was estimated to be 424. A total of 445 questionnaires were distributed, and 430 valid questionnaires were returned, thus yielding a valid response rate of 96.6%. The sample collection process for this survey is shown in Figure 1.
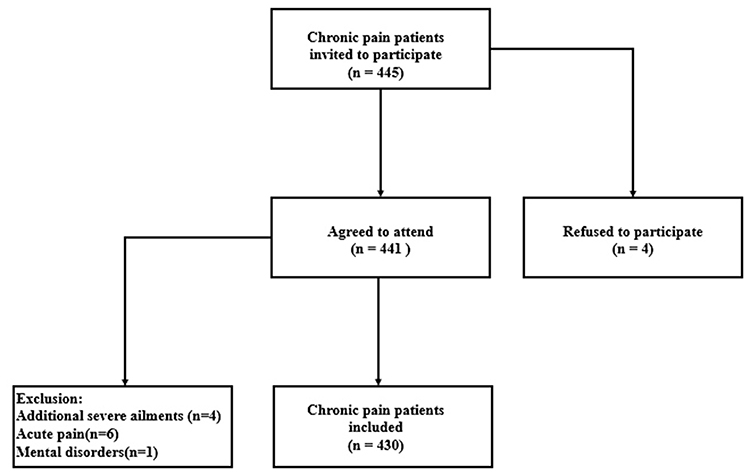 |
Figure 1 Flowchart of participant recruitment. |
Ethical Considerations
This study was approved by the Ethics Committee of the First Affiliated Hospital of Air Force Medical University (Approval No. KY20232376-F-1). All participants voluntarily participated in the study and signed an informed consent form. The research was conducted in accordance with the principles of the Declaration of Helsinki.
Measures
Questionnaire for General Information
A general data questionnaire was designed to collect patients’ demographic data and disease-related data by reviewing previous literature and consulting with pain specialists. The demographic data included age, gender, ethnicity, marital status, education, and medical payment methods. The disease-related data included pain frequency, pain duration, etc.
Visual Analogue Scale (VAS)
The Visual Analogue Scale consists of a 100-mm horizontal line. The zero end (0) of the line denoted the absence of symptoms, and the other end (100) denoted the worst possible symptoms. The meaning of the numbers on the 100-mm straight line was explained to each patient. Patients were asked to mark the point on the scale that they think describes the intensity of their pain. A ruler was used to measure the distance between this location and the starting point (0), thus yielding a millimeter-based score for pain intensity.
Chronic Pain Self-Efficacy Scale (CPSS)
The Chronic Pain Self-Efficacy Scale (CPSS) was developed by American researchers Anderson et al20 and includes 22 items (22–110 points) across three dimensions: pain management self-efficacy, somatic function self-efficacy, and symptom coping self-efficacy. Each item is scored on a 5-point Likert scale, and a higher total score indicates a higher level of self-efficacy. The scale has been shown to have acceptable psychometric properties and good reliability and validity.
Pain Catastrophizing Scale (PCS)
The Pain Catastrophizing Scale (PCS) was developed by Sullivan et al in 1995 to assess patients’ exaggerated negative attitudes toward pain.21 The PCS consists of 13 items across three dimensions: helplessness, rumination, and magnification of the pain experience. Each item is scored on a 4-point Likert scale, and the total score of the scale ranges from 0 to 52 points. The higher the score is, the higher the degree of pain catastrophizing. In this study, the Cronbach alpha coefficient of the total scale was 0.927, indicating good reliability and validity.
Data Collection
The researchers thoroughly informed the patients in the pain intervention departments of three tertiary Grade A hospitals in Shaanxi Province about the significance and goal of the survey, as well as the fact that participation in the study was voluntary and anonymous and that only approved researchers had access to the collected data. The questionnaire was administered after written consent was obtained from the participants, and the completed questionnaires were immediately collected and initially reviewed by the investigator. If any missing data were found, the patient was asked to complete the questionnaire on the spot, and the investigator checked it again. After data entry, two researchers crosschecked the data to ensure accuracy.
Pilot Study
Before the main study, a pilot survey was conducted with 20 chronic pain patients from the target hospital. They were asked to complete an assessment to test its feasibility. At the end of the evaluation, the patients provided feedback on the design and content of the evaluation, confirming that the questions were clear and unambiguous. After completing the assessment, which took approximately 10 minutes, the participants showed no signs of response fatigue.
Covariates
Based on a careful literature review, this study used the participants’ sociodemographic and disease-related characteristics as covariates, including age, gender, ethnicity, residential area, marital status, education, medical payment methods, course of disease, pain duration, pain frequency, and chronic disease comorbidity.
Data Analysis
This study used SPSS 27.0 and Mplus 8.3 software. For descriptive statistics, the mean, standard deviation, frequency and percentage are reported. Independent t tests and analysis of variance were used to examine differences in the variables. We used Pearson’s correlation analysis to analyze the correlations between variables. We used multivariate linear regression analysis to explore differences in pain catastrophizing among different sociodemographic and disease-related subgroups of chronic pain patients. Mplus 8.3 was used to establish a structural equation model (SEM) to determine the mediating role of chronic pain self-efficacy on the relationship between pain intensity and pain catastrophizing. Confidence intervals were calculated for the effect sizes; and the mediating effect was verified by bootstrapping. If the 95% confidence interval (Cl) of the indirect effect did not include 0, the mediating effect was significant. The criteria for model fit indices in this study were as follows: χ2/df ≤5, RMSEA ≤0.08, GFI ≥0.90, TLI ≥ 0.90, and SRMR≤0.08. Statistical significance was set at two-tailed p<0.05.
Results
Participants’ General Characteristics
Among all participants, scores on the PCS ranged from 0 to 52. In this study, the mean score on the PCS was 22.76, with a standard deviation of 12.01. Compared with the median value of the total score of the scale, the PCS score among chronic pain patients was at a moderate level.
Table 1 describes the characteristics of the participants (n=430). Most patients were male (58.4%, 251/186), were married (81.6%), completed secondary education (67.2%), had a disease duration of less than 5 years (75.8%).
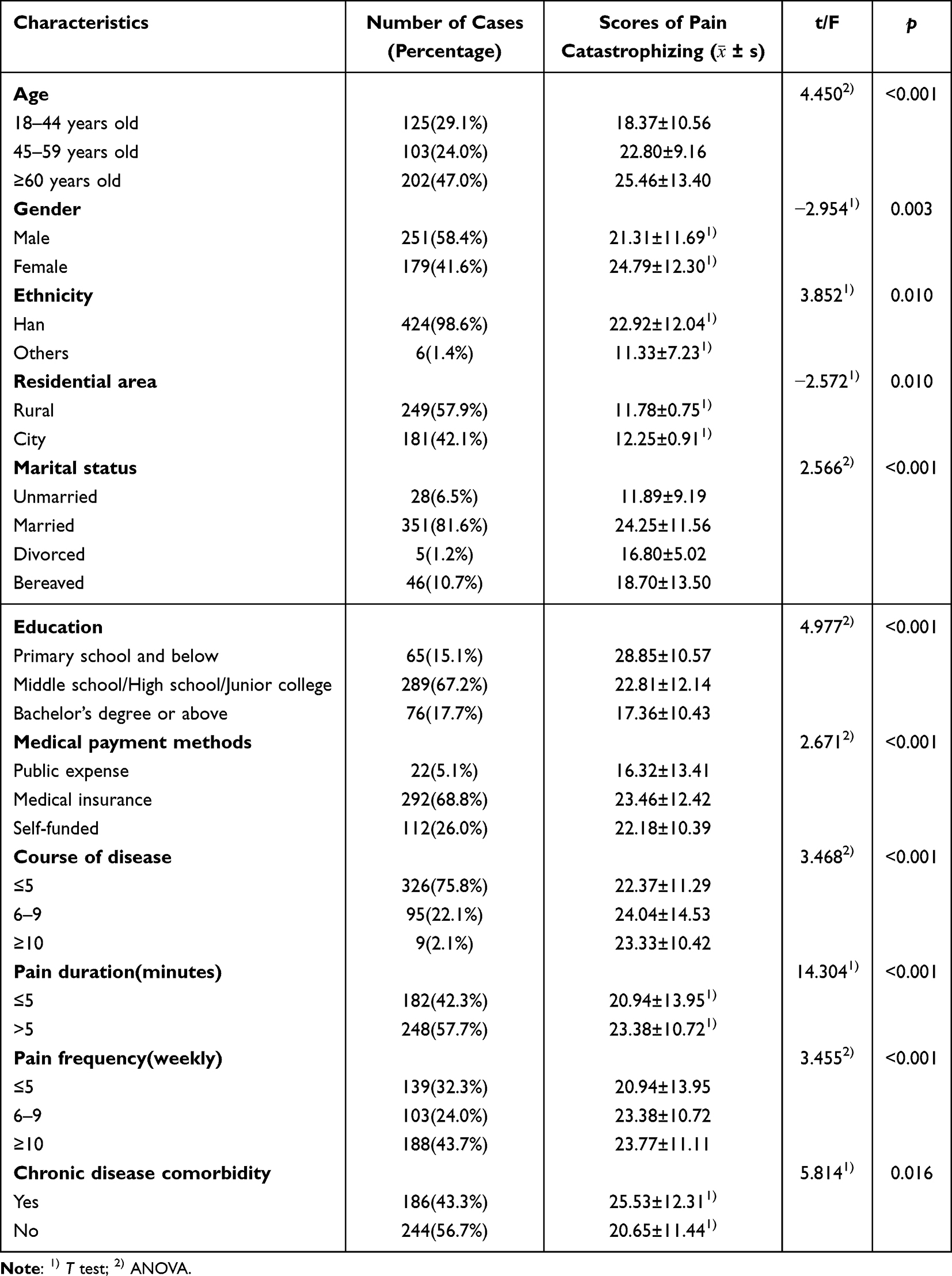 |
Table 1 Characteristics of the Participants and Univariate Analysis of Pain Catastrophizing Scores (N = 430) |
Correlations Between the Studied Variables
Table 2 lists the correlation coefficients between the variables in this study. The results of the Pearson’s correlation analysis revealed that pain intensity was positively correlated with overall pain catastrophizing (r=0.304, p<0.001) as well as the helplessness dimension (r=0.265, p<0.001), the rumination dimension (r=0.298, p<0.001), and the exaggeration dimension (r=0.305, p<0.001); pain intensity was negatively correlated with chronic pain self-efficacy (r=−0.247, p<0.001); self-efficacy was negatively correlated with overall pain catastrophizing (r=−0.454, p<0.001) as well as the helplessness dimension (r=−0.409, p<0.001), the rumination dimension (r=−0.416, p<0.001), and the exaggeration dimension (r=−0.452, p<0.001).
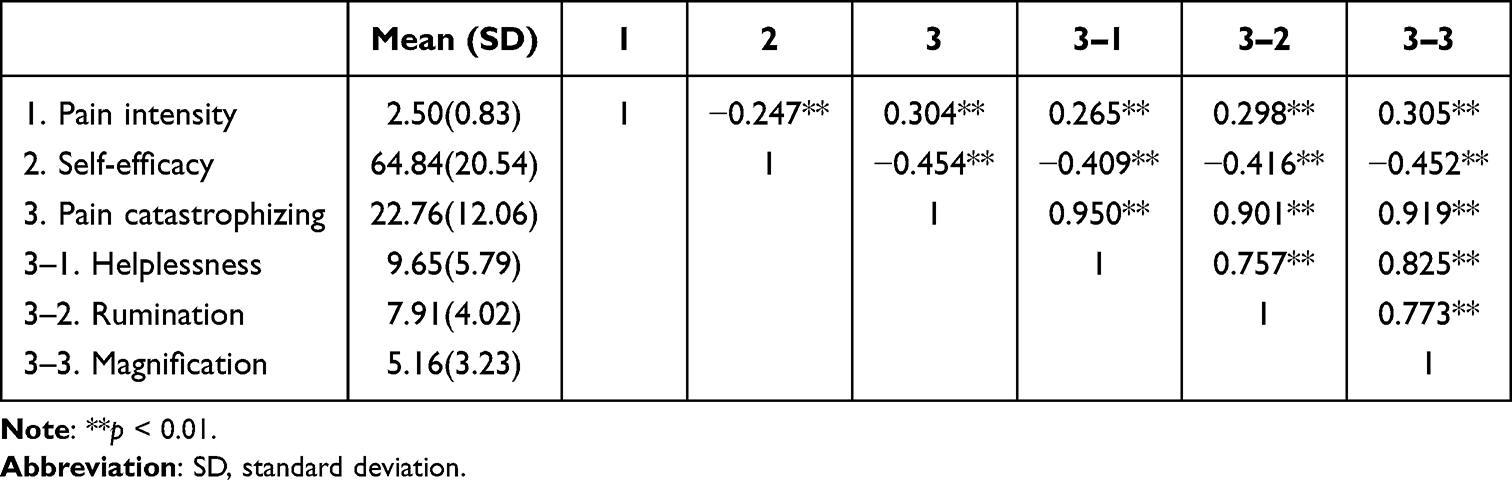 |
Table 2 Correlations of the Study Variables (N= 430) |
Multiple Linear Regression Analysis
Multiple linear regression analysis was performed with pain catastrophizing in chronic pain patients as the dependent variable and age, gender, ethnicity, residential area, marital status, pain intensity, self-efficacy, and so on as independent variables. The dependent variable in this study was a continuous variable. The results showed that pain duration, gender, pain intensity, and self-efficacy were significant differences (p<0.001) for pain catastrophizing in chronic pain patients, as shown in Table 3.
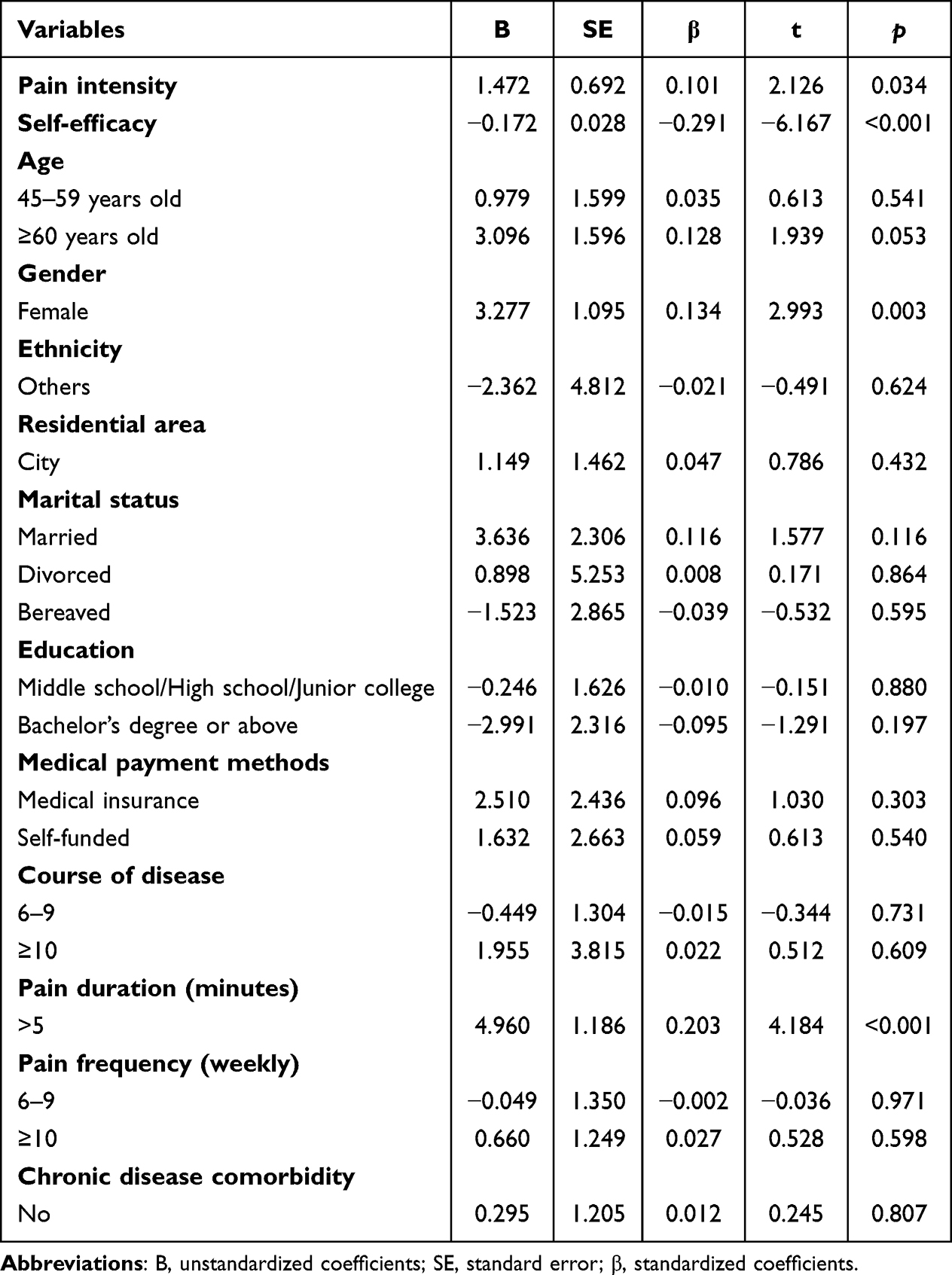 |
Table 3 Multivariate Linear Regression Analysis of Factors Influencing the Pain Catastrophizing with Chronic Pain Patients |
Mediation Model
Table 4 and Figure 2 show the paths of our mediation model. The results show that pain intensity is positively correlated with pain catastrophizing (p<0.001), and the 95% confidence interval for this effect was 0.557 to 1.346. This result provides support for Hypothesis 1.
 |
Table 4 Direct, Indirect and Total Effects Analysis of the Mediation Model (N= 430) |
 |
Figure 2 Mediating effect of self-efficacy in the relationship between pain intensity and pain catastrophizing. Note: All models were adjusted for following covariates: age, gender, ethnicity, residential area, marital status, education, medical payment methods, course of disease, pain duration, pain frequency, and chronic disease comorbidity. **p < 0.001. |
The mediated effects model fit well, and after introducing the moderator variable of self-efficacy and controlling for covariates, the relationship between pain level and pain catastrophizing was found to be partially mediated by chronic pain self-efficacy. In addition, the mediating factor (chronic pain self-efficacy) accounted for 32.5% of the total effect. Thus providing support for Hypothesis 2: “The sense of self-efficacy in patients with chronic pain mediates the relationship between pain intensity and pain catastrophizing”.
Discussion
Due to the complexity of caring for patients with chronic pain, it is important to understand the relationship between pain severity and negative patient emotions. This study investigated the mechanism underlying the relationship between pain intensity and pain catastrophizing among patients with chronic pain and elucidated the mediating role of chronic pain self-efficacy. Chronic pain self-efficacy is a positive psychological construct that has been demonstrated to be an influential form of cognitive appraisal, including pain management self-efficacy, somatic function self-efficacy, and symptom coping self-efficacy. This study aims to provide a theoretical basis for the targeted development of intervention programs to improve patients’ pain catastrophizing, mental health level, and quality of life.
This study revealed that there is a correlation between pain intensity in patients with chronic pain and on their pain catastrophizing level. This finding is consistent with previous research. For example, studies by Korkut, S and others have confirmed that pain intensity is an important predictor of pain catastrophizing in patients.22 Research by Yu Fang,23 Dinan24 has indicated that pain intensity is an antecedent to negative psychological experiences and can easily exacerbate patients’ negative emotional levels. In addition, physiological research has revealed that painful (suprathreshold) stimuli can trigger arousal and exacerbate pain catastrophizing. In summary, our study highlights the important role of pain intensity in pain catastrophizing among patients with chronic pain.
In this study, we found that in this study, pain catastrophizing was more pronounced in female patients with prolonged pain duration, which is consistent with previous studies.25,26 This may be due to the fact that the longer the pain lasts, the enhanced responsiveness of the central nervous system to normal or subthreshold afferent stimuli, ie, central sensitization. Central sensitization has strong psychometric properties and is closely related to negative emotions such as pain catastrophizing.27 According to surveys, female chronic pain patients are usually affected by fluctuations in hormone levels and tend to have lower pain thresholds than men, and are prone to negative emotional experiences.28 In summary, this suggests that healthcare professionals should focus on women who experience prolonged pain each time and take targeted interventions to promote their adoption of positive coping strategies and reduce the level of pain catastrophizing.
What’s more, we discovered chronic pain self-efficacy mediates the relationship between pain intensity and pain catastrophizing among patients with chronic pain after controlling for covariates in this study. Some studies have suggested that a patient’s pain intensity may be governed by neurobiological and neurophysiological mechanisms, which lead to a patient’s understanding of pain, especially the negative beliefs associated with chronic pain patients.29 The moderating effect of self-efficacy in patients with chronic pain suggests that there is a delicate interplay between pain intensity, self-efficacy, and pain catastrophizing. Pain self-efficacy largely determines whether patients experience pain as manageable or intolerable.30 Therefore, some studies have noted that higher levels of pain self-efficacy are associated with better physical function and pain outcomes in patients. For example, Saravanan, A et al31 confirmed that a higher level of self-efficacy can reduce pain intensity and rumination in patients with chronic low back pain. In addition, studies based on the fear-avoidance model have shown that pain self-efficacy is the only independent variable that can significantly predict avoidance behavior.32 A higher level of pain self-efficacy can lead to short-term avoidance strategies that reduce patients’ pain catastrophizing thinking.33 Therefore, by improving the sense of self-efficacy in patients with chronic pain, the negative emotions associated with pain catastrophizing, which are exacerbated by pain intensity, can be alleviated. This is highly important for maintaining the mental health of patients.
These findings may be of great significance. Specifically, our study adds to existing knowledge by revealing a strong association between pain intensity and pain catastrophizing in chronic pain patients and the study of how chronic pain self-efficacy plays a mediating role in the relationship between pain intensity and pain catastrophizing has enriched the exploration of the relationship with pain intensity and pain catastrophizing. The evidence from this study provides healthcare providers with actionable points of intervention for pain management, and targeted and effective interventions have been developed to reduce patients’ pain catastrophizing levels. Healthcare providers should first consider assessing pain severity to determine its potential role, especially in patients at high risk for chronic pain. For patients with high pain severity, pain severity reduction may influence potential pathways of pain catastrophizing. In addition, this may enhance patients’ sense of self-efficacy or motivation to achieve other goals, so that when patients have high pain intensity, they can adopt coping strategies to improve their sense of self-efficacy, thereby reducing the negative impact of pain intensity. The specific revelations and recommendations for medical staff based on the results of this study are detailed below.
Medical staff should consider reduce the pain intensity of patients with chronic pain. First, the patient’s pain intensity should be assessed during the nursing process via a combination of subjective scales and objective measurement techniques. Second, personalized care programs with varying intensities should be constructed based on the assessment results. Hypnosis is considered a state of highly focused attention that can be effectively regulated by changing the state of consciousness and the mind.34 Neuroimaging studies have shown that the basic mechanism of hypnosis involves reducing the activity of extrinsic brain networks between the environment and sensory perception, involving both cortical and subcortical regions, thereby reducing pain sensation in the participant.35 This technique has been widely used in clinical pain management. In addition, studies have shown that short-term mindfulness training can significantly activate the thalamus and insula and reduce activation in the medial prefrontal cortex, among other areas.36 These brain regions are involved in processing perception, thus regulating the perception of pain and emotional control.37 In summary, healthcare professionals can choose auxiliary relaxation training interventions that involve mindfulness in the care process of patients with chronic pain according to their pain levels to reduce their pain level, thereby alleviating patients’ negative emotions and promoting their mental health level.
What’s more, medical staff also should improve the sense of self-efficacy in patients with chronic pain. With the rise of positive psychology, self-efficacy is considered one of the key structures in behavioral science that affects mental health and psychopathology. At present, there have been studies based on self-determination theory and autonomy support theory launching randomized controlled study of empowerment education for patients with liver cirrhosis.38 In addition, some studies have used psychological techniques such as acceptance and commitment therapy and physical and occupational therapy to carry out interventional studies on patients with chronic pain.9,39 The above research results all show that the self-efficacy of patients with chronic diseases has significantly improved. In summary, clinical nursing staff can combine nursing theory with advanced psychological techniques to construct individualized and scientific intervention plans and launch randomized controlled trials or cohort studies to verify their effectiveness. The aim of these interventions is to improve patients’ sense of self-efficacy, thereby reducing negative emotions such as pain catastrophizing.
Chronic pain self-efficacy includes three dimensions: pain management self-efficacy, somatic function self-efficacy, and symptom coping self-efficacy. Research shows that patients’ sense of self-efficacy in pain management improves as their knowledge and skills in pain management increase.40 Prompting clinical medical staff should focus on strengthening patients’ degree of mastery of disease knowledge, improving their drug management capabilities and enhancing their pain relief-related skills, with the aim of improving patients’ sense of self-efficacy in pain management. In addition, according to surveys, physical activity can have a positive effect on patients’ sense of self-efficacy in terms of physical functioning to a certain extent,41 suggesting that the pain department can form a team of members, such as doctors, clinical nurse specialists, pharmacists, clinical psychologists, and physiotherapists, to develop a group-based interdisciplinary pain rehabilitation exercise plan and adopt an individualized exercise program according to the patient’s pain level. In addition, self-efficacy for coping with symptoms has been shown to influence the relationship between somatic symptoms and functional and emotional health.42 Studies have shown that social support has a positive effect on patients’ sense of self-efficacy in coping with symptoms, suggesting that healthcare workers should work with patients’ families in nursing work to improve patients’ social support capabilities. In summary, clinical medical staff can collaborate with patient families, clinical psychologists, physical therapists, and others to improve patient-related self-efficacy, thereby strengthening the cognitive and behavioral abilities of pain patients and indirectly reducing patients’ degree of pain catastrophizing.
In addition, medical staff also should identify high-risk patients prone to pain catastrophizing and actively providing individualized psychological care. Pain catastrophizing plays a crucial role in all stages of the pain experience and influences people’s subjective evaluation of pain by amplifying sensory and emotional processes.43 Therefore, pain catastrophizing should be assessed and treated as early as possible. At present, the tool used to assess pain catastrophizing among patients with chronic pain is the PCS, which lacks objective measurements. In clinical work, nursing staff can identify high-risk groups that are prone to produce pain catastrophizing emotions based on patients’ demographic and clinical characteristics. The results of this study show that gender and pain duration are all factors that influence pain catastrophizing. Therefore, caregivers should focus on the psychological experiences of patients who are female and have a prolonged pain duration.
Previous studies have shown that pain catastrophizing is a potentially important cognitive mechanism, is associated with pain-related function and changes in functional connectivity in brain regions involved in pain processing.44 In addition, there is evidence that cognitive behavioral therapy (CBT) and cognitive interviewing can improve patients’ pain catastrophizing levels.45,46 Based on the implementation of personalized cognitive‒behavioral therapy, cognitive interviews, and other psychological nursing interventions, medical staff can actively explore and influence changes in brain regions related to the level of pain catastrophizing with the help of techniques related to psychology, and targeted nursing intervention plans can be formulated in order to directly reduce the degree of pain catastrophizing among patients with chronic pain and to maintain a good psychological environment for patients.
Limitations and Future Directions
Although this study is highly important for understanding the relationship between pain intensity and pain catastrophizing among patients with chronic pain, it had several limitations. First, this study was a cross-sectional survey, and the causal relationship between variables could not be confirmed. Future research should consider conducting longitudinal studies to further verify the causal relationships between variables. Second, this study used a convenience sampling method and surveyed only chronic pain patients in Shaanxi Province. This may prevent the generalization of research results to chronic pain patients in other regions or cultural contexts. Future research should conduct a multicenter study of pain departments in Grade III A hospitals in different regions and verify our findings in groups from other cultural backgrounds or regions.
Conclusion
In summary, this study revealed that the intensity of chronic pain in the Chinese population is significantly positively correlated with patients’ level of pain catastrophizing. Women who experience longer pain duration each time may have a higher pain catastrophizing level. What’s more, chronic pain self-efficacy plays a key mediating role in the relationship between pain intensity and pain catastrophizing. No interaction effect between pain intensity and self-efficacy on pain catastrophizing was detected. These findings suggest that increasing attention to chronic pain self-efficacy may also be an important way for chronic pain patients in China to reduce pain catastrophizing.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethical Statement
This study was approved by the Ethics Committee of the First Affiliated Hospital of Air Force Medical University (Approval No. KY20232376-F-1). All participants voluntarily participated in the study and signed an informed consent form. The research was conducted in accordance with the principles of the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors have no conflicts of interest to disclose for this work.
References
1. Treede R, Rief W, Barke A, et al. Chronic pain as a symptom or a disease: the IASP classification of chronic pain for the international classification of diseases (ICD-11). Pain. 2019;160(1):19–27. doi:10.1097/j.pain.0000000000001384
2. Karimi R, Mallah N, Nedjat S, Beasley M, Takkouche B. Association between alcohol consumption and chronic pain: a systematic review and meta-analysis. Br J Anaesth. 2022;129(3):355–365. doi:10.1016/j.bja.2022.03.010
3. Rönnegård A, Nowak C, Äng B, Ärnlöv J. The association between short-term, chronic localized and chronic widespread pain and risk for cardiovascular disease in the UK biobank. Eur J Prev Cardiol. 2022;29(15):1994–2002. doi:10.1093/eurjpc/zwac127
4. Edwards R, Dworkin R, Sullivan M, Turk D, Wasan A. The role of psychosocial processes in the development and maintenance of chronic pain. J Pain. 2016;17(9):T70–T92. doi:10.1016/j.jpain.2016.01.001
5. Wideman TH, Adams H, Sullivan MJL. A prospective sequential analysis of the fear-avoidance model of pain. Pain. 2009;145(1–2):45–51. doi:10.1016/j.pain.2009.04.022
6. Gilliam WP, Schumann ME, Cunningham JL, et al. Pain catastrophizing as a treatment process variable in cognitive behavioural therapy for adults with chronic pain. Eur J Pain. 2021;25(2):339–347. doi:10.1002/ejp.1671
7. Nicholas MK. The pain self-efficacy questionnaire: taking pain into account. Eur J Pain. 2007;11(2):153–163. doi:10.1016/j.ejpain.2005.12.008
8. Miles C, Pincus T, Carnes D, Taylor S, Underwood M. Measuring pain self-efficacy. Clin J Pain. 2011;27(5):461–470. doi:10.1097/AJP.0b013e318208c8a2
9. Craner J, Lake E, Bancroft K, George L. Treatment outcomes and mechanisms for an act-based 10-week interdisciplinary chronic pain rehabilitation program. Pain Pract. 2020;20(1):44–54. doi:10.1111/papr.12824
10. Martinez-Calderon J, Zamora-Campos C, Navarro-Ledesma S, Luque-Suarez A. The role of self-efficacy on the prognosis of chronic musculoskeletal pain: a systematic review. J Pain. 2018;19(1):10–34. doi:10.1016/j.jpain.2017.08.008
11. Chester R, Jerosch-Herold C, Lewis J, Shepstone L. Psychological factors are associated with the outcome of physiotherapy for people with shoulder pain: a multicentre longitudinal cohort study. Br J Sports Med. 2018;52(4):269–275. doi:10.1136/bjsports-2016-096084
12. Meredith P, Strong J, Feeney JA. Adult attachment, anxiety, and pain self-efficacy as predictors of pain intensity and disability. Pain. 2006;123(1–2):146–154. doi:10.1016/j.pain.2006.02.025
13. Zhou Y, Gao W, Gao S, Guo X, Liu M, Cao C. Pain catastrophizing, kinesiophobia and exercise adherence in patients after total knee arthroplasty: the mediating role of exercise self-efficacy. J Pain Res. 2023;16:3993–4004. doi:10.2147/JPR.S432106
14. Wang L, Qin F, Liu H, Lu X, Zhen L, Li G. Pain sensitivity and acute postoperative pain in patients undergoing abdominal surgery: the mediating roles of pain self-efficacy and pain catastrophizing. Pain Manag Nurs. 2024;25(2):e108–e114. doi:10.1016/j.pmn.2023.12.001
15. Kim HJ, Park H, Juon H. The mediating role of pain catastrophizing on the association between depression and pain severity and interference among elderly Asian immigrants with chronic pain. J Pain Res. 2021;14:737–745. doi:10.2147/JPR.S304440
16. Odole A, Ekediegwu E, Ekechukwu END, Uchenwoke C. Correlates and predictors of pain intensity and physical function among individuals with chronic knee osteoarthritis in Nigeria. Musculoskelet Sci Pract. 2019;39:150–156. doi:10.1016/j.msksp.2018.11.014
17. Fu K, Metcalf B, Bennell KL, et al. The association between psychological factors and pain exacerbations in Hip osteoarthritis. Rheumatology. 2021;60(3):1291–1299. doi:10.1093/rheumatology/keaa494
18. Lethem J, Slade PD, Troup JD, Bentley G. Outline of a Fear-Avoidance Model of exaggerated pain perception--I. Behav Res Ther. 1983;21(4):401–408. doi:10.1016/0005-7967(83)90009-8
19. Chen B, Li L, Donovan C, et al. Prevalence and characteristics of chronic body pain in China: a national study. Springerplus. 2016;5(1):938. doi:10.1186/s40064-016-2581-y
20. Anderson KO, Dowds BN, Pelletz RE, Edwards TW, Peeters-Asdourian C. Development and initial validation of a scale to measure self-efficacy beliefs in patients with chronic pain. Pain. 1995;63(1):77–83. doi:10.1016/0304-3959(95)00021-J
21. Sullivan M, Bishop S, Pivik J. The pain catastrophizing scale: development and validation. Psychol Assess. 1995;4(7):524–532. doi:10.1037/1040-3590.7.4.524
22. Korkut S, Ülker T, Saatçi G. The power of spiritual well-being: its relationship with pain intensity, pain management, and pain catastrophizing in individuals with chronic pain. Pain Manag Nurs. 2024;25(1):62–68. doi:10.1016/j.pmn.2023.09.004
23. Fang Y, Liu M, Wu M, Liu M, Niu T, Zhang X. Pain intensity and self-perceived burden mediate the relationship between family functioning and pain catastrophizing in patients with neuropathic pain. Nurs Health Sci. 2024;26(1):e13097. doi:10.1111/nhs.13097
24. Dinan J, Hargitai I, Watson N, Smith A, Schmidt J. Pain catastrophising in the oro-facial pain population. J Oral Rehabil. 2021;48(6):643–653. doi:10.1111/joor.13166
25. Cano A. Pain catastrophizing and social support in married individuals with chronic pain: the moderating role of pain duration. Pain. 2004;110(3):656–664. doi:10.1016/j.pain.2004.05.004
26. Le LH, Brown VAV, Mol S, et al. Sex differences in pain catastrophizing and its relation to the transition from acute pain to chronic pain. BMC Anesthesiol. 2024;24(1):127. doi:10.1186/s12871-024-02496-8
27. Scerbo T, Colasurdo J, Dunn S, Unger J, Nijs J, Cook C. measurement properties of the central sensitization inventory: a systematic review. Pain Pract. 2018;18(4):544–554. doi:10.1111/papr.12636
28. Athnaiel O, Cantillo S, Paredes S, Knezevic NN. The role of sex hormones in pain-related conditions. Int J mol Sci. 2023;24(3):1866. doi:10.3390/ijms24031866
29. Louw A, Zimney K, Puentedura E, Diener I. The efficacy of pain neuroscience education on musculoskeletal pain: a systematic review of the literature. Physiother Theory Pract. 2016;32(5):332–355. doi:10.1080/09593985.2016.1194646
30. Harmell AL, Mausbach BT, Roepke SK, et al. The relationship between self-efficacy and resting blood pressure in spousal Alzheimer’s caregivers. Br J Health Psychol. 2011;16(Pt 2):317–328. doi:10.1348/135910710X504932
31. Saravanan A. Self-efficacy is inversely associated with pain rumination and pain severity in chronic low back pain. Pain Manag Nurs. 2022;23(2):241. doi:10.1016/j.pmn.2022.02.037
32. Jackson T, Wang Y, Wang Y, Fan H. Self-efficacy and chronic pain outcomes: a meta-analytic review. J Pain. 2014;15(8):800–814. doi:10.1016/j.jpain.2014.05.002
33. Varela A, Van Asselt K. The relationship between psychosocial factors and reported disability: the role of pain self-efficacy. BMC Musculoskelet Disord. 2022;23(1):21. doi:10.1186/s12891-021-04955-6
34. Császár N, Scholkmann F, Bokkon I. Implications on hypnotherapy: neuroplasticity, epigenetics and pain. Neurosci Biobehav Rev. 2021;131:755–764. doi:10.1016/j.neubiorev.2021.10.001
35. Vanhaudenhuyse A, Laureys S, Faymonville M. Neurophysiology of hypnosis. Neurophysiol Clin. 2014;44(4):343–353. doi:10.1016/j.neucli.2013.09.006
36. Zeidan F, Vago D. Mindfulness meditation-based pain relief: a mechanistic account. Ann N Y Acad Sci. 2016;1373(1):114–127. doi:10.1111/nyas.13153
37. Wielgosz J, Goldberg S, Kral T, Dunne J, Davidson R. Mindfulness meditation and psychopathology. Annu Rev Clin Psychol. 2019;15:285–316. doi:10.1146/annurev-clinpsy-021815-093423
38. Guo L, Li L, Lu Y, et al. Effects of empowerment education on the self-management and self-efficacy of liver transplant patients: a randomized controlled trial. BMC Nurs. 2023;22(1):146. doi:10.1186/s12912-023-01298-6
39. Schumann M, Coombes B, Gascho K, et al. Pain catastrophizing and pain self-efficacy mediate interdisciplinary pain rehabilitation program outcomes at posttreatment and follow-up. Pain Med. 2022;23(4):697–706. doi:10.1093/pm/pnab271
40. Macindo J, Soriano C, Gonzales H, Simbulan P, Torres G, Que J. Development and psychometric appraisal of the pain management self-efficacy questionnaire. J Adv Nurs. 2018;74(8):1993–2004. doi:10.1111/jan.13582
41. Dahlbäck A, Andréll P, Varkey E. Reliability and aspects of validity of the Swedish version of self-efficacy for exercise scale for patients with chronic pain. Physiother Theory Pract. 2023;39(1):163–173. doi:10.1080/09593985.2021.1999356
42. Shelby R, Edmond S, Wren A, et al. Self-efficacy for coping with symptoms moderates the relationship between physical symptoms and well-being in breast cancer survivors taking adjuvant endocrine therapy. Support Care Cancer. 2014;22(10):2851–2859. doi:10.1007/s00520-014-2269-1
43. Leung L. Pain catastrophizing: an updated review. Indian J Psychol Med. 2012;34(3):204–217. doi:10.4103/0253-7176.106012
44. Lazaridou A, Kim J, Cahalan C, et al. Effects of cognitive-behavioral therapy (CBT) on brain connectivity supporting catastrophizing in fibromyalgia. Clin J Pain. 2017;33(3):215–221. doi:10.1097/AJP.0000000000000422
45. Burns JW, Day MA, Thorn BE. Is reduction in pain catastrophizing a therapeutic mechanism specific to cognitive-behavioral therapy for chronic pain? Transl Behav Med. 2012;2(1):22–29. doi:10.1007/s13142-011-0086-3
46. Amtmann D, Liljenquist K, Bamer A, et al. Measuring pain catastrophizing and pain-related self-efficacy: expert panels, focus groups, and cognitive interviews. Patient. 2018;11(1):107–117. doi:10.1007/s40271-017-0269-1
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Loneliness and Pain Catastrophizing Among Individuals with Chronic Pain: The Mediating Role of Depression
Wilson JM, Colebaugh CA, Meints SM, Flowers KM, Edwards RR, Schreiber KL
Journal of Pain Research 2022, 15:2939-2948
Published Date: 16 September 2022
Association Between Pharmacotherapy and Sleep Quality in Patients with Chronic Orofacial and Chronic Body Pain: A Cross-Sectional Study
Bavia PF, Khawaja S, Hernández-Nuño de la Rosa MF, Tseng LA, Keith DA
Journal of Pain Research 2023, 16:3433-3440
Published Date: 10 October 2023
Pain Catastrophizing, Kinesiophobia and Exercise Adherence in Patients After Total Knee Arthroplasty: The Mediating Role of Exercise Self-Efficacy
Zhou Y, Gao W, Gao S, Guo X, Liu M, Cao C
Journal of Pain Research 2023, 16:3993-4004
Published Date: 21 November 2023
Network Analysis of Pain Catastrophizing, Self-Efficacy, and Kinesiophobia Among Patients After Total Knee Arthroplasty: A Cross-Sectional Study
Zhou Y, Gao W, Cao Z, Gao S, Guo X, Liu M, Cao C
Patient Preference and Adherence 2024, 18:1897-1906
Published Date: 16 September 2024
Perspectives on Pain: A Narrative Review of Pain Beliefs, Coping, and Clinical Implications

Pugh C, Snoddy K, Boyett R, Bakir H, Cawley D, Piscura MK
Journal of Pain Research 2026, 19:603074
Published Date: 23 April 2026