Back to Journals » Journal of Hepatocellular Carcinoma » Volume 12
Adjuvant Sintilimab with or without Anti-VEGF Therapy After Resection in Hepatocellular Carcinoma with Microvascular Invasion: A Multicenter Retrospective Study
Authors Wang K, Xiang YJ ![]() , Yu HM, Cheng YQ, Zheng YT, Shan YF, Cheng SQ
, Yu HM, Cheng YQ, Zheng YT, Shan YF, Cheng SQ
Received 30 July 2025
Accepted for publication 26 November 2025
Published 16 December 2025 Volume 2025:12 Pages 2735—2744
DOI https://doi.org/10.2147/JHC.S557274
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Imam Waked
Kang Wang,1,2,* Yan-Jun Xiang,3,4,* Hong-Ming Yu,3 Yu-Qiang Cheng,3 Yi-Tao Zheng,5 Yun-Feng Shan,4 Shu-Qun Cheng1,3,4
1School of Medicine, Tongji University, Shanghai, People’s Republic of China; 2Department of Hepatic Surgery, The Oncology Center, Shanghai General Hospital, Shanghai Jiaotong University School of Medicine, Shanghai, People’s Republic of China; 3Department of Hepatic Surgery VI, Eastern Hepatobiliary Surgery Hospital, Naval Medical University, Shanghai, People’s Republic of China; 4Department of Hepatobiliary Surgery, The First Affiliated Hospital, Wenzhou Medical University, Wenzhou, People’s Republic of China; 5Department of Hepatobiliary and Pancreatic Surgery, Ningbo No.2 Hospital, Ningbo, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Shu-Qun Cheng, School of Medicine, Tongji University, 1239 Siping Road, Shanghai, 200092, People’s Republic of China, Email [email protected] Yun-Feng Shan, Department of Hepatobiliary Surgery, The First Affiliated Hospital, Wenzhou Medical University, No. 2 Fuxue Lane, Wenzhou, Zhejiang, 325015, People’s Republic of China, Email [email protected]
Background: Patients with hepatocellular carcinoma (HCC) and microvascular invasion (MVI) face high post-resection relapse risk. Whether adjuvant PD-1 alone or with anti–vascular endothelial growth factor (anti-VEGF) improves outcomes remains uncertain.
Methods: Between 1 January 2022 and 1 January 2023, 170 consecutive patients from three Chinese centers were retrospectively reviewed. After resection, 69 received observation, 46 received intravenous sintilimab, and 55 received sintilimab plus either oral lenvatinib or intravenous bevacizumab biosimilar. Recurrence-free survival (RFS) was analyzed with Kaplan–Meier estimates and Cox models.
Results: Median follow-up was 24.7 months. Recurrence or death occurred in 42/69 (60.9%) observation patients, 19/46 (41.3%) sintilimab patients, and 23/55 (41.8%) combination patients. Median RFS was 16.1 months after observation, versus 29.5 months with sintilimab (hazard ratio=0.55, 95% confidence interval=0.32– 0.95; P = 0.033) and 30.5 months with sintilimab plus anti-VEGF therapy (hazard ratio=0.55, 95% confidence interval=0.33– 0.92; P = 0.023). One- and two-year RFS rates were 58.0% and 40.0% for observation, 73.9% and 66.6% for sintilimab, and 81.8% and 63.0% for combination therapy. Overall survival analysis is immature, median overall survival has not been reached in any group.
Conclusion: Adjuvant sintilimab, with or without anti-VEGF therapy, significantly prolonged RFS compared with surgery alone in patients with MVI-positive HCC. The magnitude of benefit was comparable between monotherapy and combination therapy, indicating that routine addition of anti-VEGF therapy may not be necessary for all patients.
Keywords: microvascular invasion, adjuvant therapy, immunotherapy, PD-1 inhibitor, lenvatinib, bevacizumab
Introduction
Hepatocellular carcinoma (HCC) carries a high risk of postoperative recurrence even after curative resection, with 5-year recurrence rates on the order of 40–70%.1 This risk is especially pronounced in patients with aggressive tumor features. In particular, microvascular invasion (MVI) is a well-established predictor of early intrahepatic recurrence and poor long-term survival.2 Effective adjuvant therapy is therefore urgently needed for MVI-positive, high-risk patients to improve outcomes after surgery.
To date, however, no adjuvant treatment has been conclusively shown to reduce HCC relapse, and no standard of care exists in this setting.3 Prior approaches such as postoperative transarterial chemoembolization (TACE) or molecular targeted therapy have yielded mixed results,4–6 and the largest global Phase III trial of adjuvant sorafenib (STORM) was negative. In the STORM study, sorafenib did not significantly prolong recurrence-free survival (RFS) compared to placebo, underscoring the limitations of tyrosine kinase inhibitor (TKI) therapy alone in the adjuvant context.7 Thus, surveillance remains the current practice after resection, despite the high relapse rates in high-risk HCC patients.
In recent years, the emergence of immune checkpoint inhibitors (ICIs) and anti-angiogenic agents has revolutionized systemic therapy for advanced HCC.8,9 Immune-based treatments targeting the PD-1/PD-L1 axis have demonstrated significant survival benefits in unresectable disease, establishing a new standard first-line regimen. This success has provided a strong rationale to investigate immunotherapy and anti-angiogenic therapy in the adjuvant setting, where these modalities could potentially eradicate residual microscopic disease and suppress pro-tumor angiogenesis after resection.
Early clinical trials of adjuvant immunotherapy in HCC have yielded promising yet heterogeneous findings, fueling debate over the optimal strategy. The IMbrave050 trial recently reported that adjuvant atezolizumab plus bevacizumab significantly improved RFS in high-risk HCC patients compared to observation.10 However, in updated analysis, initial RFS benefit was not sustained.11 In contrast, a Chinese Phase II trial evaluated six months of the PD-1 inhibitor sintilimab alone versus surveillance in resected high-risk HCC.12 These divergent outcomes have raised a critical question: should adjuvant immunotherapy be given alone or in combination with VEGF-targeted therapy in order to best improve RFS13? Ongoing phase III trials are actively exploring this issue, including studies of PD-1 monotherapy (eg nivolumab in CheckMate 9DX, pembrolizumab in KEYNOTE-937) and dual immunotherapy/anti-angiogenic regimens (durvalumab ± bevacizumab in EMERALD-2). Until those results mature, the optimal adjuvant approach for MVI-positive HCC remains controversial.
Here we present a retrospective, multicenter study aimed at informing this clinical dilemma. We analyzed HCC patients with MVI who underwent curative resection, comparing postoperative adjuvant therapy with a PD-1 inhibitor (sintilimab) alone versus a combination of PD-1 inhibitor plus VEGF-targeted agents (either lenvatinib or a bevacizumab biosimilar). We evaluated the impact of these adjuvant strategies on recurrence-free survival in this high-risk population.
Methods
Study Design and Participants
This retrospective, multicenter study was conducted at Eastern Hepatobiliary Surgery Hospital, The First Affiliated Hospital of Wenzhou Medical University, and Ningbo No.2 Hospital. The study aimed to evaluate the efficacy of adjuvant sintilimab alone or in combination with anti-VEGF therapy in patients with HCC with MVI. Patients undergoing curative-intent hepatectomy between January 1, 2022, and January 1, 2023, were eligible. Inclusion criteria required pathologically confirmed HCC with documented MVI. Exclusion criteria included incomplete clinical data, administration of other postoperative adjuvant therapies (eg, TACE), macrovascular invasion, and other concurrent malignancies.
The study was approved by the institutional review boards of all participating centers and conducted following the ethical principles outlined in the Declaration of Helsinki. Due to the retrospective nature of the study, informed consent was waived.
Treatment
Patients were categorized into three groups based on their postoperative adjuvant therapy: (1) the surgery-only group (Surg-only), who received no additional postoperative therapy; (2) the PD-1 group, who received adjuvant sintilimab monotherapy; and (3) the PD-1+VEGF group, who received combined adjuvant treatment with sintilimab and anti-VEGF agents (including lenvatinib or bevacizumab biosimilars). Treatment was initiated 4–8 weeks postoperatively and continued for approximately 6–12 months. Sintilimab was administered intravenously at a fixed dose of 200 mg every 3 weeks. Lenvatinib was administered orally at a dose of 8 mg/day, and bevacizumab biosimilars were administered intravenously at a dose of 15 mg/kg every 3 weeks.
Clinical and Pathological Assessments
Patient demographic characteristics and clinical parameters collected included age, sex, hepatitis B virus infection status, liver function tests (total bilirubin, albumin, alanine aminotransferase [ALT], aspartate aminotransferase [AST]), alpha-fetoprotein (AFP), des-gamma-carboxy prothrombin (DCP), presence of liver cirrhosis, tumor size, tumor number, tumor differentiation, and MVI grade. Surgical techniques, including surgical approach (laparotomy versus laparoscopic), margin status (wide versus narrow), and resection type (anatomic versus non-anatomic), were also documented.
Outcomes
The primary outcome was RFS, defined as the time interval from surgery until documented disease recurrence or death from any cause, whichever occurred first. Secondary outcome included overall survival (OS), defined as the time from surgery to death from any cause, and post-recurrence treatment strategies.
Follow-Up and Recurrence Evaluation
Patients underwent routine postoperative follow-up every 3 months for the first year and then every 6 months thereafter. Follow-up included clinical evaluation, laboratory tests (including liver function and tumor markers), and radiological imaging (contrast-enhanced computed tomography [CT] or magnetic resonance imaging [MRI]) to detect recurrence. Radiologic recurrence was defined by standard hepatocellular carcinoma imaging features on multiphasic CT or MRI, including arterial phase hyperenhancement with portal or delayed phase washout or threshold growth on serial imaging.
Given the retrospective, multicenter design, we enhanced comparability by implementing a standardized retrospective abstraction protocol with a detailed operations manual that specified the time zero, definitions of recurrence, censoring rules, and variable coding. Source records were abstracted by trained site personnel and verified by the coordinating team.
Statistical Analysis
Continuous variables were described using means and standard deviations or medians and ranges, as appropriate. Categorical variables were summarized using frequencies and percentages. Comparisons among groups were performed using the chi-square test or Fisher’s exact test for categorical variables and the ANOVA or Kruskal–Wallis test for continuous variables, as applicable.
Kaplan-Meier curves were generated to estimate RFS and OS, with comparisons between groups performed using Log rank tests. Univariable and multivariable Cox proportional hazards models were utilized to identify independent predictors of recurrence. All statistical tests were two-sided, and a P-value <0.05 was considered statistically significant. Analyses were conducted using R software (version 4.2.2, R Foundation for Statistical Computing, Vienna, Austria).
Results
Patient Characteristics
A total of 170 patients with resected HCC at high risk of recurrence were retrospectively enrolled in this study (Figure 1). Among these patients, 69 (40.6%) received no adjuvant therapy (Surg-only group), 46 (27.1%) received adjuvant sintilimab therapy (PD-1 group), and 55 (32.4%) received combined adjuvant treatment with sintilimab and anti-VEGF agents (PD-1+VEGF group). Table 1 presents the key baseline characteristics. There were no significant differences among the groups in terms of age, sex, hepatitis B infection status, total bilirubin, AFP, cirrhosis, tumor size, tumor number, tumor differentiation, or MVI grade (all P > 0.05). The complete baseline table is available in Supplementary Table 1.
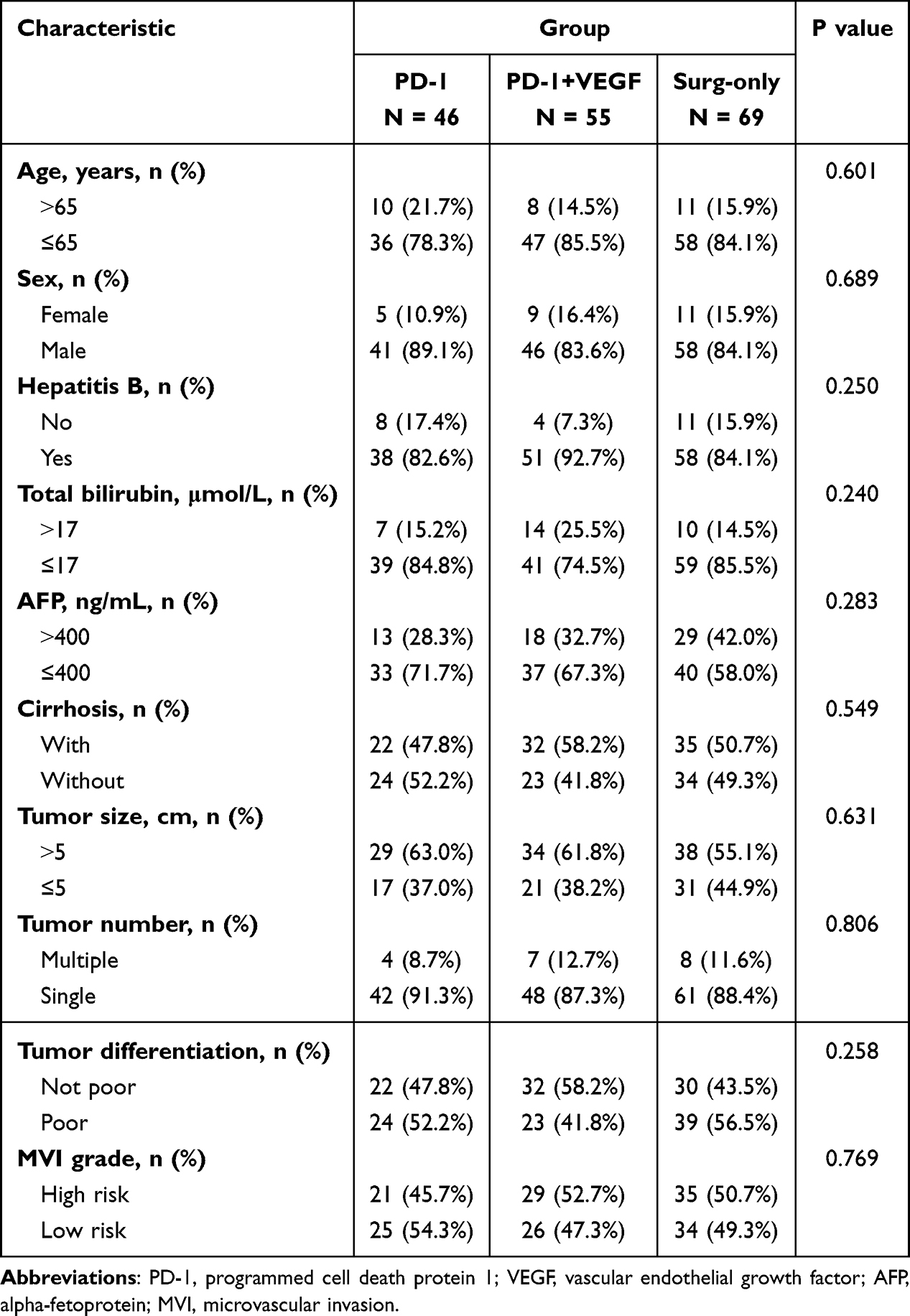 |
Table 1 Baseline Characteristics of the Study Population |
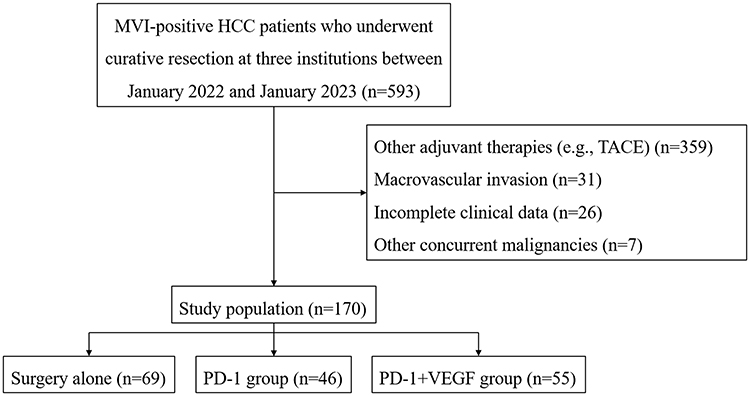 |
Figure 1 Study flowchart. Abbreviations: PD-1, programmed cell death protein 1; VEGF, vascular endothelial growth factor. |
Surgical Details
The surgical procedures predominantly involved open laparotomy, although laparoscopic approaches were employed in approximately one-quarter of patients across all groups. Most patients had wide surgical margins and underwent non-anatomic resections. There were no significant differences among groups regarding surgical approaches, margin status, or resection techniques (Supplementary Table 2).
Recurrence-Free Survival
During a median follow-up of 24.7 months, recurrence or death occurred in 42 (60.9%) patients in the Surg-only group, 19 (41.3%) patients in the PD-1 group, and 23 (41.8%) patients in the PD-1+VEGF group. Detailed information on recurrence is provided in Supplementary Table 3. Local recurrence predominated across all groups, accounting for 73.8% of events in the surgery-only group, 89.5% in the PD-1 group, and 73.9% in the PD-1+VEGF group. The median RFS was 16.1 months (95% CI=10.5-not reached) in the Surg-only group, significantly shorter than that observed in the PD-1 group (median 29.5 months, 95% CI=24.7-not reached; HR=0.55, 95% CI=0.32–0.95; P=0.033) and the PD-1+VEGF group (median 30.5 months, 95% CI=24.7-not reached; HR=0.55, 95% CI=0.33–0.92; P=0.023). The 1-year and 2-year RFS rates were 73.9% (95% CI=62.3–87.8%) and 66.6% (95% CI=54.0–82.1%), respectively, in the PD-1 group, 81.8% (95% CI=72.2–92.7%) and 63.0% (95% CI=50.8–78.1%) in the PD-1+VEGF group, and 58.0% (95% CI=47.4–70.9%) and 40.0% (95% CI=29.8–53.6%) in the Surg-only group (Figure 2A).
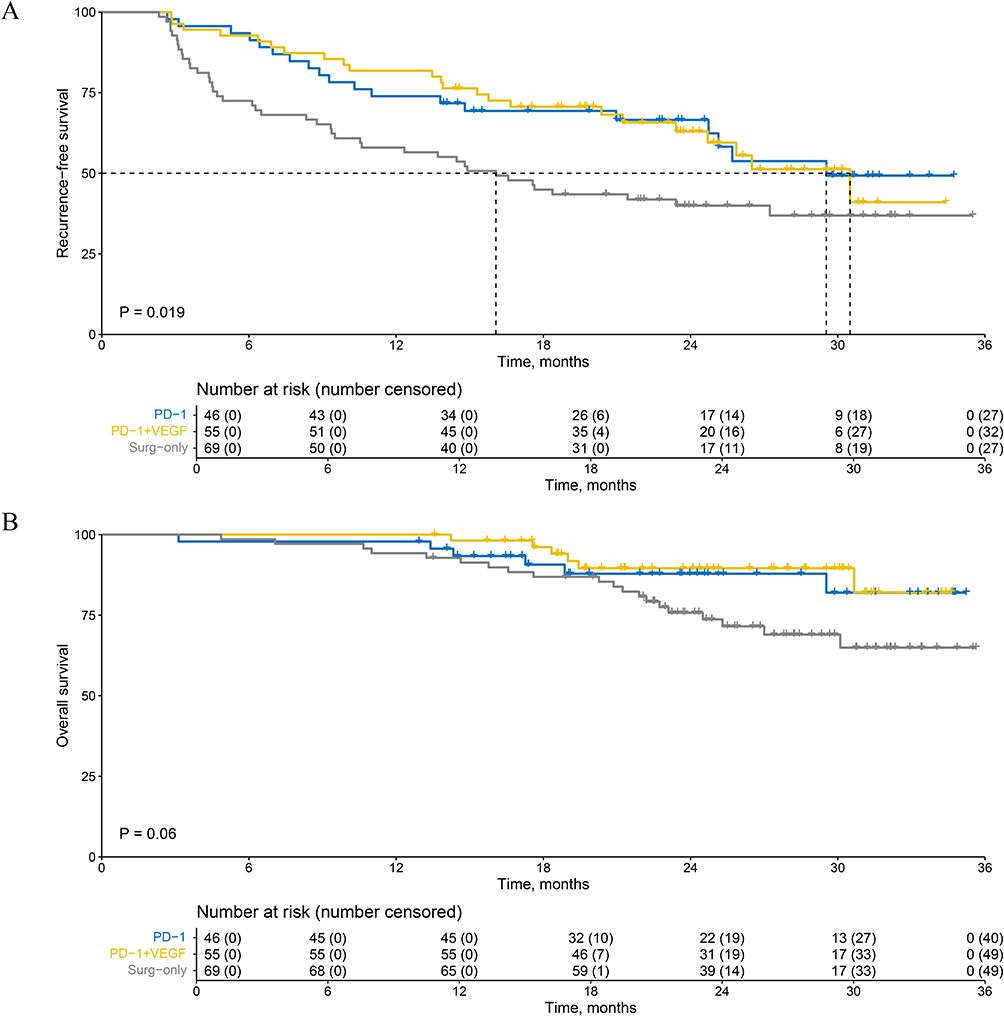 |
Figure 2 Kaplan–Meier curves of (A) recurrence-free survival and (B) overall survival for study patients. Abbreviations: PD-1, programmed cell death protein 1; VEGF, vascular endothelial growth factor. |
Multivariable Cox regression analysis adjusting for confounders demonstrated that both PD-1 (HR=0.55, 95% CI: 0.32–0.95; P=0.033) and PD-1+VEGF (HR=0.55, 95% CI: 0.33–0.92; P=0.023) treatments independently improved RFS compared to the Surg-only group (Table 2).
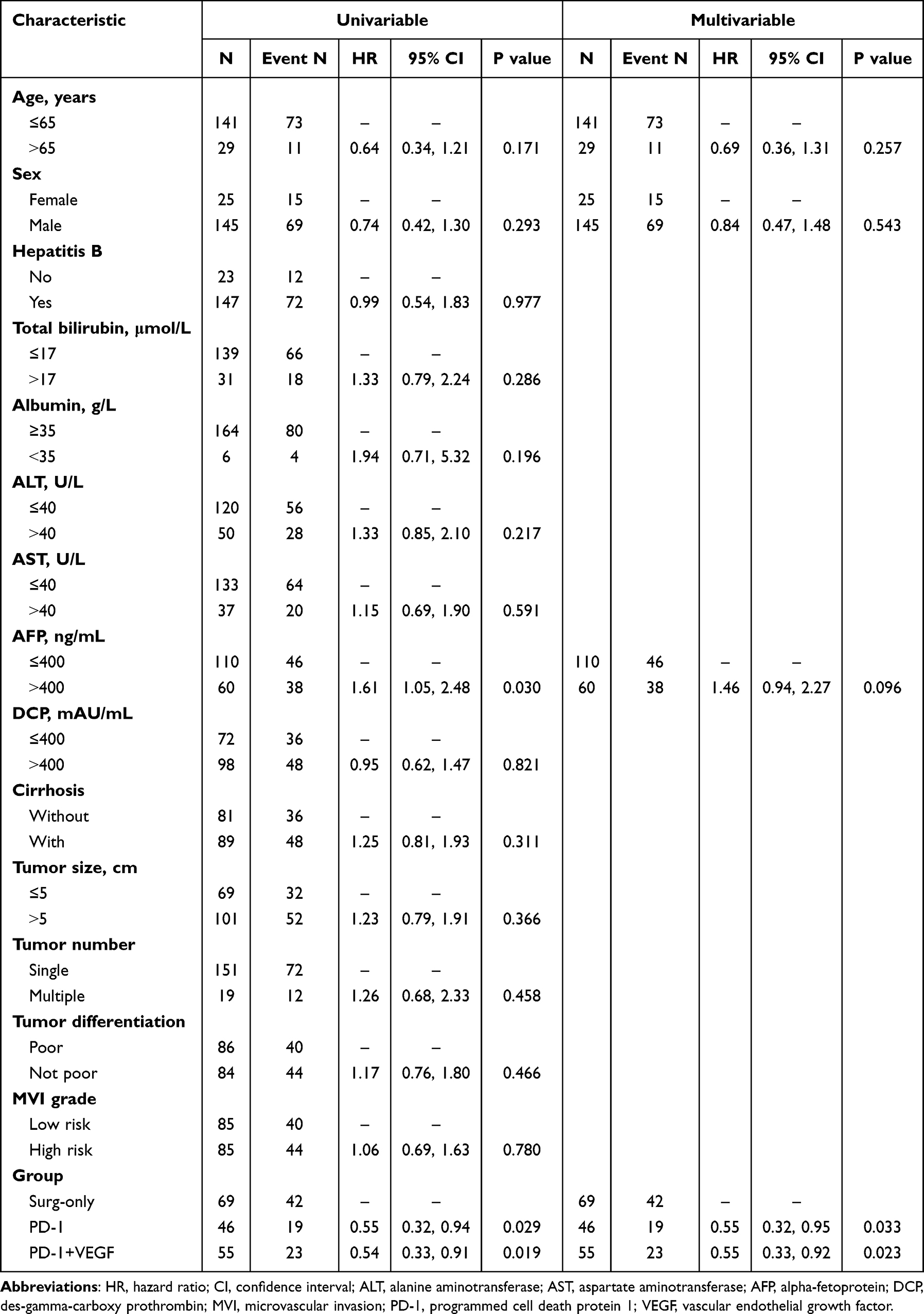 |
Table 2 Cox Regression for Recurrence-Free Survival |
Treatment After Recurrence
Of the patients experiencing recurrence, 40.5% in the Surg-only group, 58.8% in the PD-1 group, and 43.5% in the PD-1+VEGF group underwent TACE. Surgical resection or local ablation was performed in 31.0%, 35.3%, and 21.7% of patients, respectively. Additionally, systemic treatments such as tyrosine kinase inhibitors (TKIs) or PD-1+VEGF therapies were administered predominantly in the PD-1+VEGF group (Table 3).
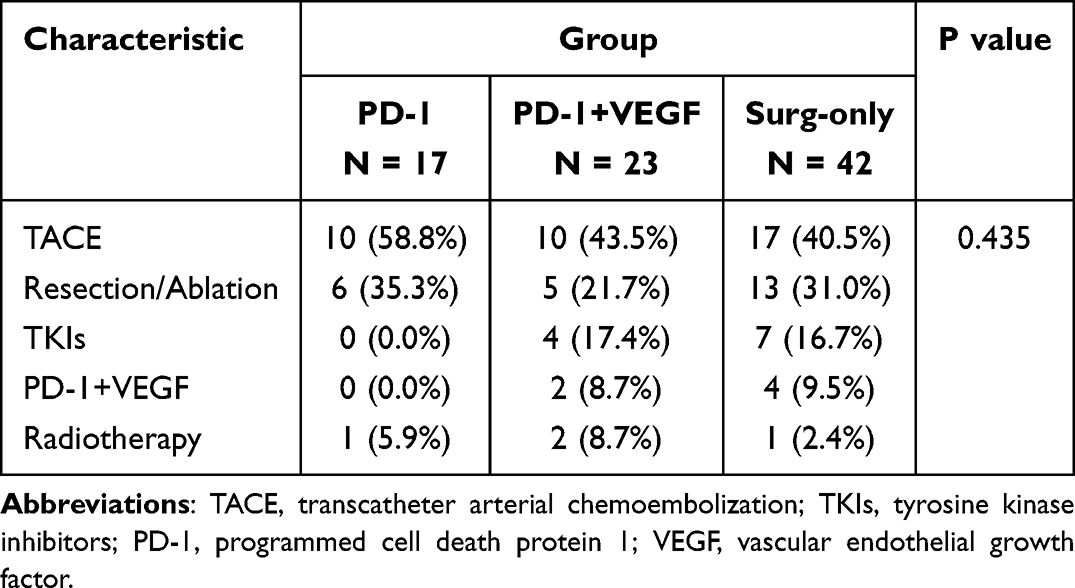 |
Table 3 Treatment After Recurrence |
Overall Survival
OS is still ongoing. At the time of data cutoff, 32 deaths were recorded. Median OS was not reached in any group. However, preliminary data suggest a favorable trend in the PD-1 and PD-1+VEGF groups compared to the Surg-only group. Longer follow-up is required to confirm these findings (Figure 2B).
Discussion
Our retrospective analysis demonstrates that adjuvant immunotherapy can improve recurrence-free survival in HCC patients with microvascular invasion, aligning with emerging evidence from recent trials. Both sintilimab monotherapy and sintilimab plus anti-VEGF therapy significantly prolonged RFS compared to surgery alone.
Despite the early RFS gains, our findings and prior studies indicate that adjuvant therapy’s benefit may diminish over time. In IMbrave050, the significant RFS advantage of atezolizumab–bevacizumab over surveillance was not maintained with longer follow-up.10 By a median of 35 months, the updated analysis showed overlapping RFS medians (33.2 vs 36.0 months) and no statistically significant difference between the arms.11 Investigators noted a convergence of the Kaplan-Meier curves around the second year of follow-up, implying that the combination merely delayed recurrence rather than preventing it. Similarly, in our study the PD-1 and PD-1+VEGF arms, which were initially separated, exhibited a narrowing gap in late follow-up. Several factors might explain this pattern. First, the benefit of VEGF inhibition could be time-limited; once therapy is stopped at 6–12 months, dormant micrometastases might eventually progress, leading to catch-up in recurrence rates. Second, differences in patient and tumor characteristics can influence late outcomes: the IMbrave050 trial included a broad “high-risk” population (tumors >5 cm, multifocal disease, MVI, etc), and it allowed certain adjunct therapies. For instance, 11% of resected patients in IMbrave050 received adjuvant TACE in addition to surgery. Such additional therapy in the active surveillance arm may have lowered recurrence rates and diluted the relative benefit of immunotherapy.
The question of whether adding anti-VEGF therapy to PD-1 blockade provides meaningful incremental benefit remains open. Our data suggest that while combination therapy produces a numerically higher early RFS, its long-term advantage over PD-1 monotherapy may be limited. It is possible that certain biological subgroups derive more sustained benefit from dual therapy. For example, patients with exceedingly angiogenic tumors or more extensive intrahepatic spread might gain more from concomitant VEGF suppression, whereas others may do just as well with immunotherapy alone. Identifying predictive biomarkers or risk features for response to combination therapy is therefore of great importance.14,15 At the same time, one must weigh the added toxicity of combination regimens. In the adjuvant IMbrave050 trial, the atezolizumab–bevacizumab arm not only had typical ICI and TKI class toxicities, but also a slight excess in severe adverse events and treatment-related deaths compared to surveillance. Although our retrospective study did not systematically capture toxicity, it is reasonable to assume that adding agents like lenvatinib or bevacizumab can increase the risk of hypertension, hepatic toxicity, and other side effects. Thus, a personalized approach — intensifying adjuvant therapy with dual ICI–antiangiogenic treatment for those most likely to relapse, and possibly sparing others the additional risk — could maximize benefit while minimizing harm.16,17 Evidence from advanced HCC suggests that PD-L1 expression and tumor mutational burden have shown variable and context-dependent predictive value, limiting immediate clinical use in the adjuvant setting.18 Genomic drivers of immune exclusion, particularly activation of the WNT and beta-catenin pathway, have been linked to resistance to immune checkpoint blockade and may identify patients less likely to benefit from PD-1 based therapy.19 Circulating biomarkers are promising for postoperative risk stratification. Postoperative alpha-fetoprotein or des-gamma-carboxy prothrombin dynamics, as well as minimal residual disease assessment using circulating tumor DNA, have been associated with early relapse and warrant evaluation as tools to guide the selection of monotherapy versus combination therapy.20–22
This study has several limitations that warrant consideration. Foremost, its retrospective, non-randomized design is subject to selection biases and unmeasured confounders. Although baseline characteristics were well balanced and multivariable Cox analysis confirmed the independent association of adjuvant therapy with improved RFS, we cannot exclude that subtle differences in tumor biology or patient fitness influenced both the choice of adjuvant treatment and the outcomes. The sample size of the PD-1 (n=46) and PD-1+VEGF (n=55) groups was modest, limiting statistical power to detect small differences between these two active regimens. Management strategies also varied across centers, including the choice of anti-VEGF agent (lenvatinib vs bevacizumab biosimilars) and the approaches to managing recurrence, which could introduce heterogeneity. Additionally, the follow-up duration remains relatively short for an HCC adjuvant study. As a result, the OS analysis is immature (only 32 total deaths were observed), and it is too early to determine whether the RFS improvement will translate into a significant OS benefit. Longer follow-up is needed, especially given that many patients received effective therapies for recurrence, which can prolong survival regardless of initial adjuvant treatment. Finally, because we excluded patients who received adjuvant TACE or other therapies, our findings specifically pertain to systemic immunotherapy-based adjuvant strategies; the results might differ in settings where multidisciplinary adjuvant approaches are combined.
Conclusions
In this multicenter cohort of patients with MVI, adjuvant PD-1 inhibitor therapy, with or without VEGF-targeted agents, was associated with a clinically meaningful delay in recurrence compared with surgery alone. The magnitude of benefit was comparable between monotherapy and combination therapy, indicating that routine addition of VEGF-targeted therapy may not be necessary for all patients.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author Shu-Qun Cheng ([email protected]) upon reasonable request.
Ethics Approval Statement
This study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki. This study was approved by the ethics committee of Eastern Hepatobiliary Surgery Hospital, The First Affiliated Hospital of Wenzhou Medical University, and Ningbo No.2 Hospital in accordance with the institutional and national guidelines and regulations governing research involving human participants.
Patient Consent Statement
Informed consent to participate was waived by the Ethics Committee due to the retrospective design of the study and the use of anonymized patient data.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China (82473487), and Shanghai Oriental Talents Program Youth Project (QNWS2024076).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Tampaki M, Papatheodoridis GV, Cholongitas E. Intrahepatic recurrence of hepatocellular carcinoma after resection: an update. Clin J Gastroenterol. 2021;14(3):699–713. doi:10.1007/s12328-021-01394-7
2. Xiang YJ, Wang K, Zheng YT, et al. Prognostic value of microvascular invasion in eight existing staging systems for hepatocellular carcinoma: a Bi-Centeric Retrospective Cohort Study. Front Oncol. 2021;11:726569. doi:10.3389/fonc.2021.726569
3. European Association for the Study of the Liver. Electronic address, European Association for the Study of the L. EASL Clinical Practice Guidelines: management of hepatocellular carcinoma. J Hepatol. 2018;69(1):182–236. doi:10.1016/j.jhep.2018.03.019
4. Sun JJ, Wang K, Zhang CZ, et al. Postoperative adjuvant transcatheter arterial chemoembolization after R0 hepatectomy improves outcomes of patients who have hepatocellular carcinoma with microvascular invasion. Ann Surg Oncol. 2016;23(4):1344–1351. doi:10.1245/s10434-015-5008-z
5. Wang XH, Zhou QF, Wang CM, et al. Adjuvant transarterial chemoembolization for intermediate-stage hepatocellular carcinoma with microvascular invasion. Br J Surg. 2022;110(8):913–916.
6. Liang L, Li C, Wang MD, et al. Development and validation of a novel online calculator for estimating survival benefit of adjuvant transcatheter arterial chemoembolization in patients undergoing surgery for hepatocellular carcinoma. J Hematol Oncol. 2021;14(1):165. doi:10.1186/s13045-021-01180-5
7. Bruix J, Takayama T, Mazzaferro V, et al. Adjuvant sorafenib for hepatocellular carcinoma after resection or ablation (STORM): a Phase 3, randomised, double-blind, placebo-controlled trial. Lancet Oncol. 2015;16(13):1344–1354. doi:10.1016/S1470-2045(15)00198-9
8. Ren Z, Xu J, Bai Y, et al. Sintilimab plus a bevacizumab biosimilar (IBI305) versus sorafenib in unresectable hepatocellular carcinoma (ORIENT-32): a randomised, open-label, Phase 2–3 study. Lancet Oncol. 2021;22(7):977–990. doi:10.1016/S1470-2045(21)00252-7
9. Finn RS, Qin S, Ikeda M, et al. Atezolizumab plus Bevacizumab in unresectable hepatocellular carcinoma. N Engl J Med. 2020;382(20):1894–1905. doi:10.1056/NEJMoa1915745
10. Qin S, Chen M, Cheng AL, et al. Atezolizumab plus bevacizumab versus active surveillance in patients with resected or ablated high-risk hepatocellular carcinoma (IMbrave050): a randomised, open-label, multicentre, phase 3 trial. Lancet. 2023;402(10415):1835–1847. doi:10.1016/S0140-6736(23)01796-8
11. Yopp A, Kudo M, Chen M, et al. LBA39 Updated efficacy and safety data from IMbrave050: phase III study of adjuvant atezolizumab (atezo) + bevacizumab (bev) vs active surveillance in patients (pts) with resected or ablated high-risk hepatocellular carcinoma (HCC). Ann Oncol. 2024;35:S1230. doi:10.1016/j.annonc.2024.08.2279
12. Wang K, Xiang Y-J, Yu H-M, et al. Adjuvant sintilimab in resected high-risk hepatocellular carcinoma: a randomized, controlled, phase 2 trial. Nature Med. 2024;30(3):708–715.
13. Pinato DJ, Fulgenzi CAM, D’Alessio A. Immunotherapy at all stages of hepatocellular carcinoma. Nature Med. 2024;30(3):640–641. doi:10.1038/s41591-024-02828-8
14. Llovet JM, Montal R, Sia D, Finn RS. Molecular therapies and precision medicine for hepatocellular carcinoma. Nat Rev Clin Oncol. 2018;15(10):599–616. doi:10.1038/s41571-018-0073-4
15. Richard C, Fumet JD, Chevrier S, et al. Exome analysis reveals genomic markers associated with better efficacy of nivolumab in lung cancer patients. Clin Cancer Res. 2019;25(3):957–966. doi:10.1158/1078-0432.CCR-18-1940
16. Kelley RK. Adjuvant sorafenib for liver cancer: wrong stage, wrong dose. Lancet Oncol. 2015;16(13):1279–1281. doi:10.1016/S1470-2045(15)00296-X
17. Kudo M, Finn RS, Qin S, et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: a randomised phase 3 non-inferiority trial. Lancet. 2018;391(10126):1163–1173. doi:10.1016/S0140-6736(18)30207-1
18. Sandi K, Xin C. Immunotherapy biomarkers for HCC: contemporary challenges and emerging opportunities. Hepatoma Res. 2022;8:32. doi:10.20517/2394-5079.2022.58
19. Pinyol R, Sia D, Llovet JM. Immune Exclusion-Wnt/CTNNB1 class predicts resistance to immunotherapies in HCC. Clin Cancer Res. 2019;25(7):2021–2023. doi:10.1158/1078-0432.CCR-18-3778
20. Kim DY, Toan BN, Tan CK, et al. Utility of combining PIVKA-II and AFP in the surveillance and monitoring of hepatocellular carcinoma in the Asia-Pacific region. Clin Mol Hepatol. 2023;29(2):277–292. doi:10.3350/cmh.2022.0212
21. Yang C, Wang H, Liu J, et al. Pre- to postoperative alpha-fetoprotein ratio-based nomogram to predict tumor recurrence in patients with hepatocellular carcinoma. Front Oncol. 2023;13:1134933. doi:10.3389/fonc.2023.1134933
22. Xu Y, Cai J, Zhong K, et al. Plasma-only circulating tumor DNA analysis detects minimal residual disease and predicts early relapse in hepatocellular carcinoma patients undergoing curative resection. Front Oncol. 2023;13:1119744. doi:10.3389/fonc.2023.1119744
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Adjuvant Therapy for High-Risk Localized Renal Cell Carcinoma: Current Landscape and Future Direction
Buller DM, Antony M, Ristau BT
OncoTargets and Therapy 2023, 16:49-64
Published Date: 24 January 2023
Safety and Efficacy of Drug-Eluting Bead Transarterial Chemoembolization Combined with Lenvatinib and Anti-PD-1 Antibodies for Unresectable Hepatocellular Carcinoma: A Retrospective Analysis
Wu SJ, Ruan DD, Wu QY, Tang Y, Zhang JH, Cai SL, Zhou YF, Luo JW, Fang ZT
Journal of Hepatocellular Carcinoma 2023, 10:807-820
Published Date: 2 June 2023
Hepatocellular Carcinoma with Radiological Progression: Lenvatinib Plus PD-1 Inhibitor Combined with Microwave Ablation and Synchronous Transarterial Chemoembolization
Shi Q, Huang P, Zhang Z, Zhang W, Liu L, Yan Z
Journal of Hepatocellular Carcinoma 2023, 10:1861-1871
Published Date: 21 October 2023
Effectiveness and Safety of the PD-1 Inhibitor Lenvatinib Plus Radiotherapy in Patients with HCC with Main PVTT: Real-World Data from a Tertiary Centre
Li G, Zhao Y, Li K, Yang S, Xiang C, Song J, Yang Y, Li G, Dong J
Journal of Hepatocellular Carcinoma 2023, 10:2037-2048
Published Date: 9 November 2023
Efficacy of Lenvatinib Combined with PD-1 Inhibitor versus Sorafenib and PD-1 Inhibitor with or Without TACE for Hepatocellular Carcinoma with Extrahepatic Metastasis
Duan WB, Wang XH, Zhang GC, He Z, Li SQ, Zhou J
ImmunoTargets and Therapy 2024, 13:247-258
Published Date: 16 May 2024