Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Acupuncture for Post-Stroke Lower Limb Dysfunction: Clinical Efficacy and Neurophysiological Mechanisms
Authors Xie W ![]() , Di Z, Shao W, Wang A, Guan L
, Di Z, Shao W, Wang A, Guan L
Received 12 September 2025
Accepted for publication 7 November 2025
Published 25 November 2025 Volume 2025:18 Pages 7691—7703
DOI https://doi.org/10.2147/JMDH.S567206
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Veronica Swallow
Wei Xie,1,* Zhong Di,2,* Wei Shao,1 Aijun Wang,1 Lihua Guan1
1Department of Acupuncture, Quzhou Hospital of Traditional Chinese Medicine, Quzhou, Zhejiang, 324000, People’s Republic of China; 2Department of Acupuncture and Moxibustion, The Third Affiliated Hospital of Zhejiang University of Traditional Chinese Medicine, Hangzhou, Zhejiang, 310005, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wei Xie, Email [email protected]
Purpose: Lower limb dysfunction is a common and debilitating consequence of stroke, significantly compromising patients’ quality of life. This mini-review synthesizes clinical research on acupuncture for post-stroke lower limb dysfunction over the past five years, integrating traditional Chinese medicine (TCM) theories and modern evidence.
Methods: The review analyzed clinical studies and TCM theoretical perspectives. TCM attributes stroke pathogenesis to Yin-Yang disharmony, Qi-blood imbalance, and complex interactions of wind, phlegm, fire, stasis, and toxin.
Results: Acupuncture therapies, including body acupuncture, electroacupuncture, abdominal acupuncture, scalp-body acupuncture, specific acupoint stimulation, moxibustion, and combined techniques, demonstrate significant efficacy in improving motor coordination, reducing muscle tone, and enhancing voluntary movement. Mechanistically, acupuncture regulates cerebral blood flow, reduces ischemic-reperfusion injury, modulates neuroinflammation, and promotes neural regeneration. Clinical studies show that these approaches effectively alleviate symptoms, with total effective rates ranging from 70% to 95.5%.
Conclusion: Acupuncture shows considerable potential for post-stroke lower limb dysfunction, likely exerting effects through modulation of cerebral blood flow, neuroinflammation, oxidative stress, and neural plasticity. However, challenges remain, including the lack of standardized acupoint selection protocols, stimulation parameters, large multicenter trials, and in-depth mechanistic research.
Keywords: stroke, lower limb dysfunction, acupuncture, traditional Chinese medicine, neurorehabilitation
Introduction
Stroke was recorded as “Piangu” (hemiplegia) and “Pianfeng” (unilateral wind) in Huangdi Neijing (Inner Canon of the Yellow Emperor). Ling Spiritual Pivot: Needling Nodes and True Evil states:
When pathogenic factors invade one side of the body deeply, they reside in the Nutritive Qi and Defensive Qi. As the Nutritive and Defensive Qi decline, the True Qi departs, leaving the pathogenic factors alone, leading to Piangu.
In Traditional Chinese Medicine (TCM), stroke is also understood in terms of “Yin–Yang disharmony”, which refers to imbalance between the body’s passive (Yin) and active (Yang) forces, and “Qi–blood imbalance”, indicating insufficient or obstructed flow of vital energy (Qi) and blood.1 These imbalances are believed to impair organ function, block meridians, and contribute to motor and sensory deficits.2 Western medicine refers to it as “stroke” or “cerebrovascular accident (CVA)”, primarily caused by sudden rupture or spasm of cerebral arterial vessels, or acute local cerebral tissue circulatory disorders and hemiplegia dominated by limb function impairment due to stenosis or obstruction.3 Lower limb dysfunction is particularly common among limb impairments, clinically characterized by disorders of motor coordination in major muscle groups and joints of the affected side, accompanied by increased muscle tone, decreased muscle strength, and impaired voluntary motor function.4 It is also a key factor contributing to reduced quality of life and aggravated family and social economic burdens after stroke.5 Numerous clinical studies have shown that body acupuncture, electro-acupuncture, abdominal acupuncture, scalp-body acupuncture, specific acupoint acupuncture, acupuncture with different manipulation techniques, moxibustion, and combined acupuncture-moxibustion demonstrate significant efficacy in treating post-stroke lower limb dysfunction, playing a crucial role in improving patients’ quality of life and reducing mortality and disability rates.6 This article summarizes the clinical research achievements of acupuncture in treating post-stroke lower limb dysfunction over the past five years.
Methods
This narrative review aimed to synthesize recent clinical research on acupuncture for post-stroke lower limb dysfunction and integrate it with TCM theories. We conducted a structured literature search in PubMed, Web of Science, CNKI, and Wanfang databases for articles published between January 2018 and December 2024. Search terms included “stroke”, “hemiplegia”, “lower limb dysfunction”, “motor impairment”, “gait disturbance”, and “acupuncture” (including electroacupuncture, scalp acupuncture, abdominal acupuncture, and moxibustion).
Inclusion Criteria
To ensure a structured and transparent selection of studies, we applied the PICOS framework to formulate the inclusion criteria as follows:
1. Population: Adult patients with post-stroke lower limb dysfunction.
2. Intervention: Acupuncture or acupuncture-based interventions, either as monotherapy or combined with conventional rehabilitation.
3. Comparator: Conventional rehabilitation, standard care, or control groups.
4. Outcomes Motor function (Fugl-Meyer Assessment), activities of daily living (Barthel Index), gait, muscle strength, or spasticity.
5. Study design: Randomized controlled trials, non-randomized trials, and observational studies.
Exclusion Criteria
Studies were excluded if they met any of the following:
- Animal or in vitro studies.
- Review articles, case reports, or conference abstracts without primary clinical data.
- Studies lacking clear outcome measures related to lower limb function.
- Duplicate publications or studies with incomplete data.
Data Extraction and Synthesis
Two authors independently screened titles and abstracts, evaluated full-text articles for eligibility, and extracted relevant information, including study design, sample size, patient characteristics, intervention protocols, acupoints used, treatment duration, and primary outcomes. Discrepancies were resolved through discussion. The included studies were qualitatively synthesized according to acupuncture modality and primary outcome measures. Given the heterogeneity in study designs and interventions, quantitative meta-analysis was not performed; instead, findings were summarized narratively to highlight overall trends and clinical efficacy.
Epidemiological Context
Stroke is a leading cause of long-term disability worldwide, with over 12 million new cases and 6 million deaths annually.7 Post-stroke lower limb dysfunction—including motor impairment, spasticity, and gait disturbances—affects a substantial proportion of survivors, significantly limiting mobility and quality of life. Patients exhibit considerable heterogeneity in age, stroke subtype, severity, comorbidities, and time since onset, all of which influence recovery and treatment outcomes.8 Conventional rehabilitation, such as physiotherapy and task-specific training, remains standard but is often constrained by residual deficits and variable adherence. This epidemiological and clinical landscape highlights the need to explore complementary interventions, such as acupuncture, to optimize functional recovery (Table 1).
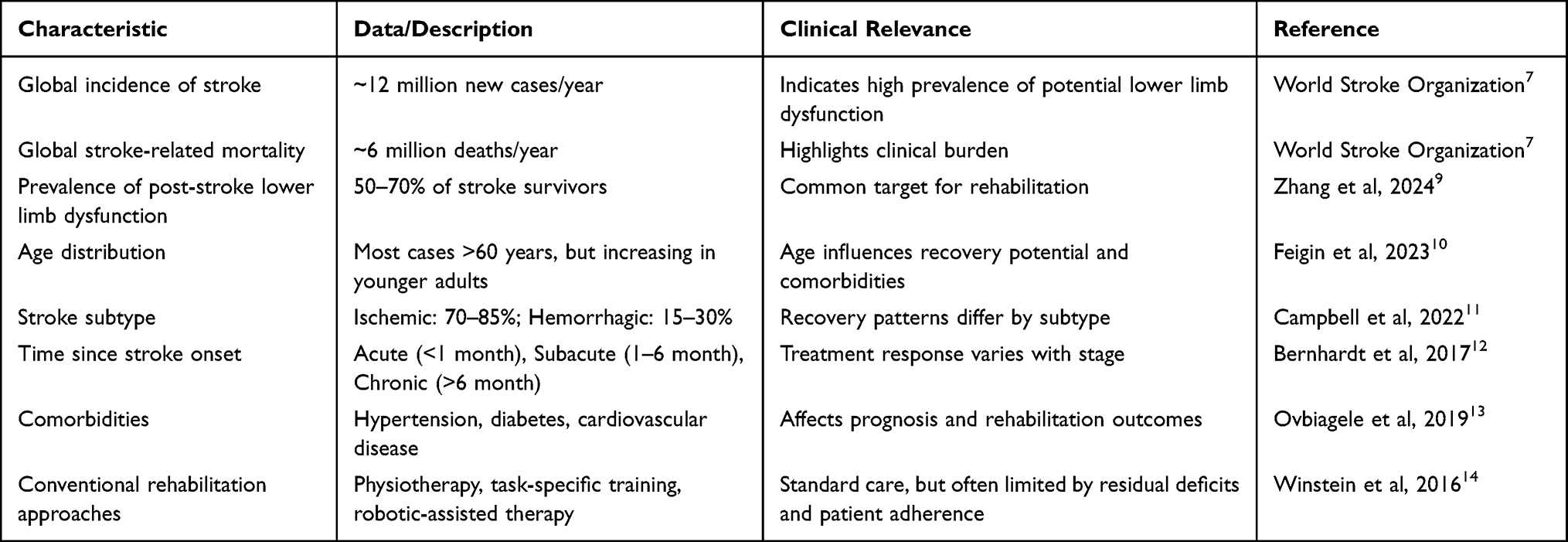 |
Table 1 Epidemiological Characteristics and Heterogeneity of Post-Stroke Lower Limb Dysfunction |
Etiology and Pathogenesis of Stroke
Traditional Chinese Medicine Perspective on Stroke
The earliest record of “stroke” appears in Plain Questions: Treatise on Wind of Huangdi Neijing, but it had a different meaning from the current concept.15 The term “stroke” was first used in Synopsis of the Golden Chamber: Syndrome and Pulse Differentiation of Stroke and Arthralgia, and its association with symptoms like hemiplegia was first documented. Analysis of etiology and pathogenesis: External causes include not only the six exogenous pathogens but also various infectious factors in Western medicine.16 Internal causes vary among individuals and are complex, with their role in pathogenesis widely acknowledged by physicians.1
Phlegm-blood stasis obstruction: Phlegm-dampness blocks the Qi movement of Zang-Fu organs, disrupts the distribution of body fluids and blood, generates blood stasis, forms phlegm-blood stasis, blocks meridians, and clouds the clear orifices.1
Phlegm-heat in the fu organs: Excessive consumption of fatty, sweet, and thick foods or alcohol impairs the spleen and stomach, leading to phlegm-heat; or emotional depression transforms into fire, consuming Qi and Yin, condensing body fluids into phlegm, with phlegm-heat clouding the clear orifices.
Blood stasis obstruction: Prolonged illness, Zheng deficiency (healthy Qi deficiency), or emotional disorders cause Qi stagnation and blood stasis; fire-heat scorching blood or Yin fluid deficiency can also lead to stasis, blocking cerebral collaterals.
Exuberant fire-toxin: Fire-toxin can be triggered by internal or external factors, generating wind, moving blood, and disturbing the mind and orifices.
Qi deficiency and blood stasis: Internal injury from overwork, prolonged illness, or congenital deficiency weakens Zheng Qi, causing poor Qi-blood circulation, blocking tendons and cerebral collaterals, and impairing mental function.
Toxin damaging brain collaterals: Long-term accumulation of exogenous six pathogens, improper diet, or emotional disorders generates toxins, which harm the brain marrow and damage brain vessels.
Liver-Kidney Yin deficiency: Aging, internal injury, or accumulated damage lead to Liver-Kidney insufficiency, Yin-blood deficiency, and wind disturbing the brain orifices.17
In summary, the pathogenesis of stroke roots in Yin-Yang disharmony of Zang-Fu organs and Qi-blood disorder, characterized by fundamental deficiency and superficial excess, with the disease location in the Liver, Spleen, and Kidney.18 It involves pathological factors such as wind (internal and external), phlegm (damp-phlegm, wind-phlegm), fire (phlegm-fire, Liver-fire), blood stasis, Qi disorder (Qi reversal, Qi sinking), deficiency (Yin deficiency, Qi-blood deficiency), and toxin (infection). The current trend of stroke occurrence and progression is the combination of multiple factors, which mutually transform and influence each other (Table 2). As summarized in Figure 1, the pathogenesis of stroke in TCM involves a complex interplay of multiple factors, including wind, phlegm, fire, blood stasis, and deficiency.
 |
Table 2 Traditional Chinese Medicine (TCM) Perspectives on Stroke Pathogenesis |
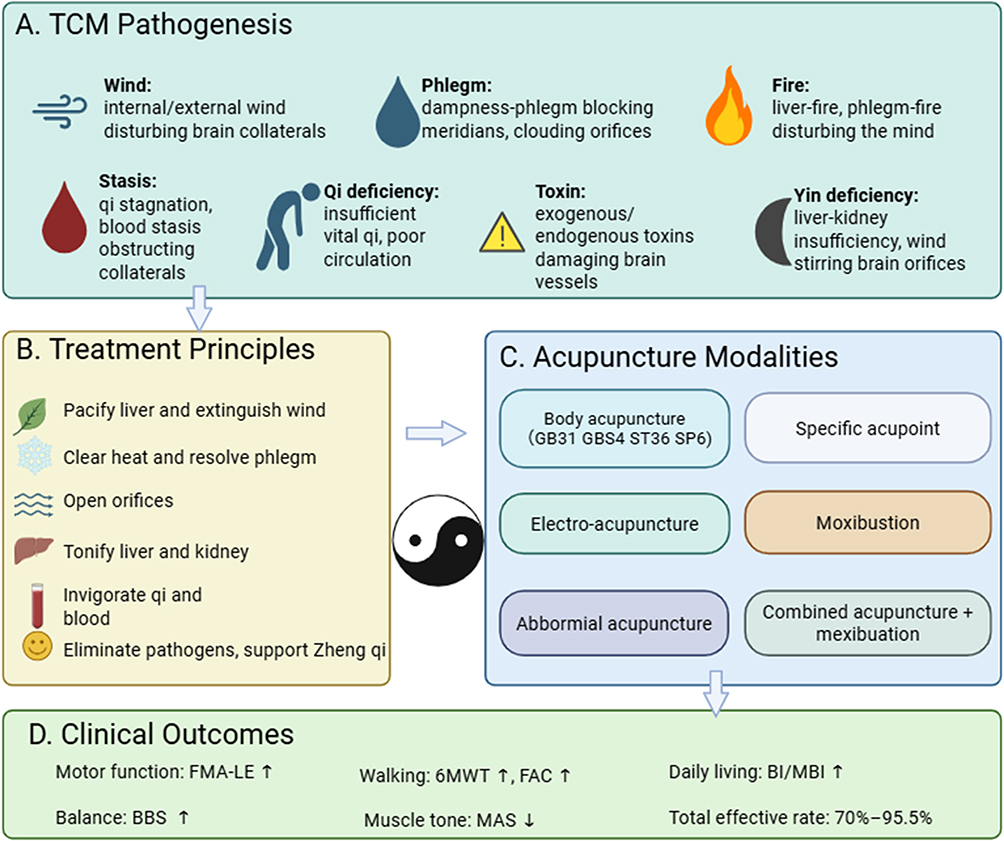 |
Figure 1 Conceptual framework illustrating TCM pathogenesis, treatment principles, acupuncture modalities, and associated clinical outcomes. (A) TCM Pathogenesis (B) Treatment Principles (C) Acupuncture Modalities (D) Clinical Outcomes. |
Guiding Principles of TCM Treatment for Post-Stroke Limb Dysfunction
The treatment principles of stroke follow “treating the branch in emergency and the root in remission”. The main therapies focus on eliminating pathogens, commonly using methods such as calming the Liver to extinguish wind, clearing heat and resolving phlegm, removing phlegm to open orifices, tonifying the Liver and Kidney, and activating blood to unblock collaterals.1 For the closed syndrome and collapse syndrome, treat them with eliminating pathogens to open orifices and resuscitate, and supporting Zheng Qi to solidify collapse, restoring Yin and Yang, respectively.23 In the recovery and sequelae stages, syndrome differentiation mainly identifies mixed deficiency-excess and pathogen excess with Zheng deficiency, requiring combined pathogen elimination and Zheng support, such as nourishing Yin to extinguish wind and invigorating Qi to activate blood. Post-stroke limb dysfunction results from tendons and vessels losing Qi-blood nourishment, requiring combined acupuncture and medication to invigorate Yuan Qi, tonify Qi-blood, activate blood, and unblock meridians for joint flexibility.24 The following reviews acupuncture therapies alone.
Acupuncture Methods
Body Acupuncture
Traditional acupuncture follows the principle of “treating flaccidity by exclusively selecting Yangming”, mainly selecting acupoints from the Hand and Foot Yangming meridians to promote Qi-blood circulation in meridians, nourish tendons, and activate blood to unblock collaterals. Li et al (2022) treated 60 patients with post-stroke lower limb dysfunction by selecting acupoints such as Weizhong (BL40), Ququan (LR8), Fengshi (GB31), Yanglingquan (GB34), Xuanzhong (GB39), Zusanli (ST36), Geshu (BL17), Sanyinjiao (SP6), Fengchi (GB20), and Xuehai (SP10) (Figure 2). The results showed 25 cures, 12 improvements, 16 marked effects, and 7 cases with no effect, with a total marked effective rate of 88.33%, indicating significant acupuncture efficacy. Scholars have proposed that effective stimulation of body acupuncture is a necessary means to treat limb dysfunction in post-stroke hemiplegic patients, often using pain sensation and limb twitching as standards to excite neural pathways, induce brain tissue excitation, and promote local brain function recovery.25 Mechanistically, body acupuncture may modulate peripheral sensory input to the central nervous system, enhancing cortical excitability and promoting neuroplasticity in motor-related regions.26 Additionally, it can influence local microcirculation, reduce oxidative stress, and facilitate neuromuscular junction recovery.27
 |
Figure 2 Anatomical localization of the primary acupuncture points used in post-stroke lower limb rehabilitation. |
Wei et al28 randomly divided 60 patients with post-stroke lower limb dysfunction into two groups (30 cases each) to study the effect of Taiyin-Yangming balanced acupuncture on post-stroke lower limb hemiplegia. Both groups selected acupoints based on syndrome differentiation. The treatment group used Taiyin-Yangming meridian balanced acupuncture, while the control group received conventional acupuncture. The results showed the total effective rate of the treatment group was significantly higher than that of the control group (93.3% > 86.1%), and the marked effective rate was also higher (76.7% > 56.7%), with a significant difference between the two groups (P<0.05). Tian et al29 divided 100 eligible patients into two groups randomly to explore the effect of Yin-Yang opposite needling combined with respiratory reinforcing-reducing method on post-stroke lower limb balance dysfunction. The control group received basic therapy without relevant rehabilitation treatment, while the acupuncture group received Yin-Yang opposite needling combined with respiratory reinforcing-reducing method in addition to basic treatment. Before and after treatment, the balance trajectory parameters, stability coefficient, and weight distribution coefficient were significantly improved in both groups (P<0.05). After treatment, the rectangular area, peripheral area, trajectory length, trajectory length per unit area, left-right offset stability, and weight distribution coefficient showed significant differences between the acupuncture group and the control group (P<0.05). Yu et al30 divided 50 eligible patients into two groups (25 cases each) to explore the efficacy of double-needle concurrent needling for increased lower limb muscle tone after stroke. The treatment group performed double-needle concurrent needling on antagonistic acupoints of the affected limb, while the control group received conventional acupuncture on the affected limb. The results showed the total effective rate of the treatment group was significantly higher than that of the control group (72% > 56%, P<0.05). These protocols likely enhance synaptic plasticity and modulate inhibitory-excitatory balance in motor circuits, promoting recovery of motor coordination and reducing spasticity.25,31,32
Electro-Acupuncture
Electro-acupuncture increases oxygen supply to the ischemic area, indirectly improves oxygen and energy metabolism in the ischemic area, thereby reducing the infarction focus, inhibiting cell apoptosis, alleviating neuronal damage, and promoting functional recovery of neurons in the ischemic penumbra.33 Mechanistically, electrical stimulation can activate Aβ and Aδ fibers, inducing long-term potentiation in motor cortex neurons and facilitating corticospinal tract reorganization.34 It also modulates neurotransmitter release (eg, glutamate, GABA) and neurotrophic factors such as BDNF to enhance neuroplasticity.35 Li et al36 randomly divided 40 eligible patients into two groups. The treatment group received conventional rehabilitation therapy and electro-acupuncture at BIguan (ST31), Liangqiu (ST34), Fengshi (GB31), Chengfu (BL36), Yinmen (BL37), etc. The control group selected Huantiao (GB30), BIguan (ST31), Futu (ST32), Fengshi (GB31), etc, using the Qi ci method (triple needling). The control group used discontinuous waves, while the treatment group used a flexor-extensor alternating stimulator with discontinuous waves. The results showed that the neurological deficit scores of both groups were significantly different from those before treatment (P<0.01), and the treatment group was also significantly different from the control group (P<0.01). The total effective rate of the treatment group was significantly better than that of the control group (90% > 55%), indicating that electro-acupuncture was more effective than flexor-extensor alternating stimulation therapy. In addition, Li et al highlighted that combining electro-acupuncture with traditional rehabilitation enhances proprioceptive function,37 improving balance and gait stability. Proprioceptive training facilitates sensorimotor integration and motor relearning,38 suggesting a synergistic effect with electro-acupuncture in restoring lower limb function. This synergistic effect likely arises from enhanced sensorimotor integration and cortical remapping induced by patterned electrical stimulation.39
Abdominal Acupuncture
Abdominal acupuncture activates the Nogo-A-mediated central nerve regeneration function, not only significantly improving the clinical efficacy of patients with cerebral ischemia-reperfusion but also playing an important role in promoting motor function recovery, reducing ischemia-reperfusion injury, and alleviating mental disorders. Zhan et al40 analyzed the efficacy of Sun’s abdominal acupuncture in treating 120 patients with post-stroke lower limb dysfunction. The patients were randomly divided into two groups: the observation group received body acupuncture combined with Sun’s abdominal acupuncture, while the control group received only body acupuncture with the same acupoints. The clinical symptoms of lower limb dysfunction, FMA scale, and the lower limb motor function component of the BI index were significantly improved in the observation group compared to the control group (P<0.05). Abdominal acupuncture may act through modulation of central nervous system plasticity, influencing motor cortex excitability and activating descending motor pathways, while also affecting autonomic regulation to improve circulation and metabolic support to ischemic tissues.41
Scalp-Body Acupuncture
The combination of scalp and body acupuncture embodies the near-far acupoint selection method, jointly maintaining the integrity of the blood-brain barrier, reducing brain edema, inflammatory response, and brain cell apoptosis, and promoting cell proliferation and DNA repair, thus improving neurological function.42,43 Researchers have pointed out that the earlier the combined use of scalp and body acupuncture in stroke treatment, the better the efficacy.44 Stimulation of scalp motor areas is believed to enhance cortical excitability, promote synaptogenesis, and facilitate reorganization of motor networks, while body acupuncture provides complementary peripheral neuromodulation.45,46 By improving local blood circulation and regulating biochemical metabolism, it not only shows significant effects in neurological deficit scale scores but also significantly improves patients’ daily living ability and quality of life when combined with functional exercise during treatment.47 To explore the efficacy of staged scalp-body acupuncture combined therapy in promoting lower limb function recovery in post-stroke patients, Song et al48 conducted an exploratory randomized controlled trial in patients with acute ischemic stroke, comparing scalp cluster acupuncture combined with constraint-induced movement therapy (CIMT) against body acupuncture with conventional rehabilitation. Both groups improved on the Fugl-Meyer scale and functional MRI outcomes, but the combined therapy group achieved greater functional recovery, highlighting the enhanced efficacy of integrating scalp acupuncture with body acupuncture and rehabilitation in lower limb function restoration. To explore the efficacy of acupuncture at the upper one-fifth of the scalp motor area in treating post-stroke lower limb dysfunction, a meta-analysis by Huang et al6 systematically evaluated randomized controlled trials investigating scalp acupuncture for post-stroke hemiplegia. The pooled results demonstrated that scalp acupuncture significantly improved motor function, as measured by the Fugl-Meyer Assessment, after both 1-month and 3-month treatment courses. Moreover, scalp acupuncture was associated with better recovery of activities of daily living compared to control interventions, indicating that conventional acupuncture combined with scalp acupuncture can significantly accelerate muscle strength recovery of the affected side.
Specific Acupoint Acupuncture
Evidence from recent systematic reviews highlights the therapeutic potential of specific scalp acupoint stimulation in post-stroke motor rehabilitation. Huang et al6 conducted a meta-analysis of randomized controlled trials and reported that scalp acupuncture significantly improved motor recovery, as reflected in Fugl-Meyer scores, and enhanced activities of daily living compared with control interventions, despite methodological limitations among the included studies. Complementing these findings, Wang et al (2023) applied Apriori algorithm-based data mining to analyze clinical literature and identified the motor area of the scalp as a core acupoint frequently used in combination therapies. Targeting specific scalp regions may optimize neuroplasticity and synaptic remodeling, improving lower limb motor function and coordination.49
Moxibustion
Moxibustion significantly improves the high-concentration, high-viscosity, coagulation, and aggregation state of blood, especially reducing high and low shear blood viscosity and whole blood viscosity.50 It obviously improves red blood cells in the microenvironment of tissues in stroke patients, significantly increases tissue cell oxygen supply, and further exerts the physiological functions of body organs. Moxibustion reduces the recurrence rate and achieves secondary prevention by decreasing inflammatory cytokines IL-1β, IL-6, and hs-CRP.51 Evidence supports the beneficial role of moxibustion in post-stroke rehabilitation. A meta-analysis by Chen et al52 included nine randomized controlled trials with 723 participants, and found that grain-sized moxibustion was significantly more effective than conventional therapy in improving neurological deficit scores (standardized mean difference [SMD] = −1.20; 95% CI: −1.71 to −0.69; P < 0.00001). The analysis further indicated superior outcomes for motor function and activities of daily living in the moxibustion group compared with controls. Nakahara et al53 conducted a controlled experimental study in 20 healthy volunteers, applying indirect moxibustion at ST36. The intervention significantly increased local skin temperature by approximately 2.5°C and decreased heart rate by about 4–5 beats per minute compared to baseline, suggesting that moxibustion can enhance peripheral blood circulation and modulate autonomic nervous activity. Mechanistically, moxibustion may promote motor recovery by modulating neuroinflammation, enhancing microvascular perfusion, reducing oxidative stress, and activating neurotrophic pathways (eg, BDNF/TrkB) to support neuroplasticity and neuronal repair, while also improving autonomic balance and tissue oxygenation.54 Collectively, these results indicate that moxibustion may not only promote motor recovery but also improve hemodynamic regulation relevant to stroke rehabilitation.
Combined Acupuncture and Moxibustion
Combined acupuncture and moxibustion can increase blood perfusion and supply in the ischemic area, improving the microcirculation of local cerebral ischemic foci.19,55 Gao et al22 conducted a systematic review and meta-analysis evaluating the effects of acupuncture plus moxibustion combined with rehabilitation training for post-stroke shoulder-hand syndrome (SHS) The pooled results showed that the combined therapy significantly outperformed rehabilitation alone in improving upper limb motor function, relieving pain, and enhancing activities of daily living, thereby highlighting the synergistic effect of integrating acupuncture and moxibustion with conventional rehabilitation. Similarly, Zhao et al (2015) reported that acupuncture combined with moxibustion, based on the theory of meridians and myofascial pathways, was not only safe but also effective in reducing pain and improving motor recovery in post-stroke shoulder-hand syndrome patients. The synergistic effects of combined acupuncture and moxibustion may involve enhanced cortical excitability, upregulation of neurotrophic factors (BDNF, NGF), modulation of inflammation, improved synaptic plasticity, and better microcirculation, collectively supporting motor recovery and functional reorganization after stroke.56 Together, these findings provide credible evidence that combined acupuncture and moxibustion interventions can enhance functional recovery and quality of life in stroke survivors (Table 3).
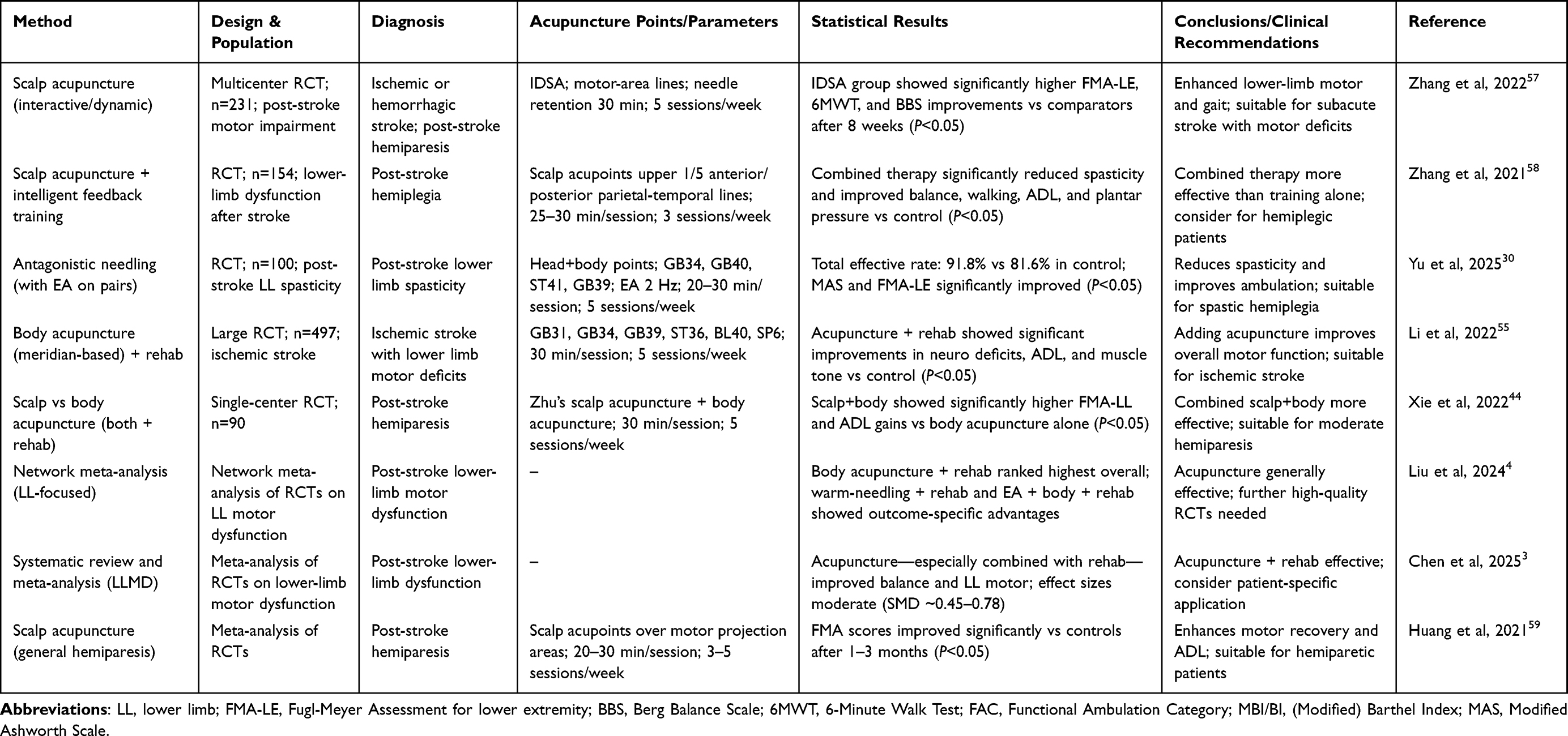 |
Table 3 Recent Clinical Studies on Acupuncture for Post-Stroke Lower-Limb Dysfunction |
Discussion
Researchers have proposed that acupuncture can reduce brain cell damage after cerebralischemia and reperfusion by influencing the functional state of the cerebral cortex;21 the warm-dredging and deficiency-tonifying effect of moxibustion can accelerate local blood circulation, improve local ischemic and hypoxic conditions, relieve muscle spasm, enhance muscle strength, and restore limb function;60 electro - acupuncture produces peripheral regulatory mechanisms through effective stimulation, generating regulatory impulses that improve abnormal bodily conditions and promote limb function recovery.61
Recent studies suggest multiple underlying mechanisms for acupuncture’s therapeutic effects on post-stroke lower limb dysfunction. Acupuncture has been shown to modulate cerebral blood flow, regulate neuroinflammation, reduce oxidative stress, and promote neurogenesis and synaptic plasticity in ischemic brain regions.62,63 Electroacupuncture can enhance motor cortex excitability and facilitate corticospinal tract reorganization,64 while scalp acupuncture targeting motor areas may optimize functional recovery through neuroplasticity.46 Moxibustion further supports microcirculation and tissue oxygenation, contributing to neural and muscular repair.65 Furthermore, although various studies demonstrate clinical efficacy, there is currently no universally accepted standardized protocol for acupoint selection, stimulation intensity, frequency, or treatment duration. Existing guidelines recommend selecting acupoints based on syndrome differentiation and targeting key meridians related to lower limb function (eg, Yangming, Taiyin), often combining local and distal points,66 but considerable variability remains across clinical practice. Standardization is essential to improve reproducibility, comparability, and integration with multimodal rehabilitation strategies.
Various acupuncture treatment methods for post-stroke lower limb dysfunction have achieved satisfactory clinical efficacy.9 They can effectively improve the ischemic and hypoxic state of the stroke - affected brain tissue,67 reduce the damage of oxygen free radicals to brain neurons during cerebral ischemia-reperfusion, accelerate brain metabolism, promote the functional recovery of damaged nerve cells, inhibit the abnormal activity of spinal motor neurons, stimulate the excitation and antagonism of neural pathways, alleviate physical pain and muscle spasm, accelerate the recovery speed of patients’ limb functions, and are of great significance for reducing disability rates and improving patients’ quality of life. However, mechanistic studies exploring the underlying biological pathways of acupuncture remain limited, and long-term follow-up data are scarce, making it difficult to fully assess the stability and persistence of therapeutic benefits. Current research still lacks large-sample, multi-center, and in-depth clinical trials that could provide more robust evidence for its efficacy.68 Future research should therefore focus on elucidating the biological mechanisms of acupuncture, establishing evidence-based standard protocols for acupoint selection and stimulation parameters, and integrating acupuncture into multimodal rehabilitation approaches to optimize functional recovery and quality of life in post-stroke patients.
Data Sharing Statement
The datasets used and analysed during the current study available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
Because this study did not involve human trials or data, it was not subject to ethical approval.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. Specifically, Wei Xie contributed to conceptualization, methodology, supervision, and drafting of the manuscript. Zhong Di, Wei Shao, Aijun Wang, and Lihua Guan contributed to data curation, formal analysis, and manuscript review and editing. Wei Xie and Zhong Di are the co-first authors.
Funding
The work was not funded by any funding.
Disclosure
The authors declared that they have no conflicts of interest regarding this work.
References
1. Zhong LLD, Kun W, Shi N, et al. Evidence-based Chinese medicine clinical practice guideline for stroke in Hong Kong. Chin Med. 2020;15(1):116. doi:10.1186/s13020-020-00397-9
2. Ren H, Yang AH, Cai YS, Qin Y, Luo TY. Study on correlation between Chinese medicine syndromes in stroke and neurological deficits during recovery phase: perspective. Medicine. 2024;103(39):e39600. doi:10.1097/MD.0000000000039600
3. Chen P, Jin X, Yu D, et al. Efficacy of acupuncture on lower limb motor dysfunction following stroke: a systematic review and meta-analysis of randomized controlled trials. PLoS One. 2025;20(5):e0312918. doi:10.1371/journal.pone.0312918
4. Liu Y, Tang Y, Wang L, et al. Optimal acupuncture methods for lower limb motor dysfunction after stroke: a systematic review and network meta-analysis. Front Neurol. 2024;15:1415792. doi:10.3389/fneur.2024.1415792
5. Xue C, Jiang C, Zhu Y, et al. Effectiveness and safety of acupuncture for post-stroke spasticity: a systematic review and meta-analysis. Front Neurol. 2022;13:2022.
6. Huang Y-J, Huang C-S, Leng K-F, Sung J-Y, Cheng S-W. Efficacy of scalp acupuncture in patients with post-stroke hemiparesis: meta-analysis of randomized controlled trials. Investig Ophthalmol Visual Sci. 2021;62(13):12–2021. doi:10.1167/iovs.62.13.12
7. Feigin VL, Brainin M, Norrving B, et al. World stroke organization: global stroke fact sheet 2025. Int J Stroke. 2025;20(2):132–144. doi:10.1177/17474930241308142
8. Alhatemi RAJ, Savaş S. A weighted ensemble approach with multiple pre-trained deep learning models for classification of stroke. Medinformatics. 2023;1(1):10–19. doi:10.47852/bonviewMEDIN32021963
9. Zhang Y, Tang Y-W, Peng Y-T, Yan Z, Zhou J, Yue Z-H. Acupuncture, an effective treatment for post-stroke neurologic dysfunction. Brain Res Bull. 2024;215:111035. doi:10.1016/j.brainresbull.2024.111035
10. Feigin VL, Owolabi MO. Pragmatic solutions to reduce the global burden of stroke: a World Stroke Organization-Lancet Neurology Commission. Lancet Neurol. 2023;22(12):1160–1206. doi:10.1016/S1474-4422(23)00277-6
11. Kelly DM, Feld J, Rothwell PM, Reinecke H, Koeppe J. Admission rates, time trends, risk factors, and outcomes of ischemic and hemorrhagic stroke from german nationwide data. Neurology. 2022;99(23):e2593–e2604. doi:10.1212/WNL.0000000000201259
12. Bernhardt J, Hayward KS, Kwakkel G, et al. Agreed definitions and a shared vision for new standards in stroke recovery research: the Stroke Recovery and Rehabilitation Roundtable taskforce. Int J Stroke. 2017;12(5):444–450. doi:10.1177/1747493017711816
13. Ovbiagele B, Goldstein LB, Higashida RT, et al. Forecasting the future of stroke in the United States: a policy statement from the American Heart Association and American Stroke Association. Stroke. 2013;44(8):2361–2375. doi:10.1161/STR.0b013e31829734f2
14. Winstein CJ, Stein J, Arena R, et al. Guidelines for adult stroke rehabilitation and recovery. Stroke. 2016;47(6):e98–e169. doi:10.1161/STR.0000000000000098
15. Zhang JL, Li YZ, Yang HY. Analyzing the Chinese medicine pathogenesis of stroke]. Zhongguo Zhong Xi Yi Jie He Za Zhi Zhongguo Zhongxiyi Jiehe Zazhi. 2012;32(1):107–110.
16. Wu S, Chen P, Zou Y, et al. Clinical relevance of Chinese syndrome factors and thromboelastography levels in patients with phlegm-heat and fu-organ excess syndrome. J Trad Chin Med Sci. 2019;6(3):211–217. doi:10.1016/j.jtcms.2019.07.002
17. Zhang S, Yang J. Factors influencing TCM syndrome types of acute cerebral infarction: a binomial logistic regression analysis. Medicine. 2023;102(46):e36080.
18. Liu T, Qin M, Xiong X, Lai X, Gao Y. Multi-omics approaches for deciphering the complexity of traditional Chinese medicine syndromes in stroke: a systematic review. Front Pharmacol. 2022;13:980650.
19. Wang L, Su XT, Cao Y, et al. Potential mechanisms of acupuncture in enhancing cerebral perfusion of ischemic stroke. Fronti Neurol. 2022;13:1030747. doi:10.3389/fneur.2022.1030747
20. Liu T, Qin M, Xiong X, Lai X, Gao Y. Multi-omics approaches for deciphering the complexity of traditional Chinese medicine syndromes in stroke: a systematic review. Front Pharmacol. 2022;13:980650. doi:10.3389/fphar.2022.980650
21. Sun X, Liu H, Sun Z, et al. Acupuncture protects against cerebral ischemia–reperfusion injury via suppressing endoplasmic reticulum stress-mediated autophagy and apoptosis. Mol Med. 2020;26(1):105. doi:10.1186/s10020-020-00236-5
22. Gao H, Li Z, Chen W, Shen F, Lu Y. Effectiveness of acupuncture and moxibustion combined with rehabilitation training for post-stroke shoulder-hand syndrome: a systematic review and meta-analysis. Front Neurol. 2025;16:1576595. doi:10.3389/fneur.2025.1576595
23. Choi TY, Jun JH, Lee HW, Yun JM, Joo MC, Lee MS. Traditional Chinese medicine interventions in the rehabilitation of cognitive and motor function in patients with stroke: an overview and evidence map. Front Neurol. 2022;13:885095. doi:10.3389/fneur.2022.885095
24. Dashtdar M, Dashtdar MR, Dashtdar B, Kardi K, Shirazi MK. The concept of wind in traditional Chinese medicine. J Pharmacopunct. 2016;19(4):293–302. doi:10.3831/KPI.2016.19.030
25. Okabe N, Wei X, Abumeri F, et al. Parvalbumin interneurons regulate rehabilitation-induced functional recovery after stroke and identify a rehabilitation drug. Nat Commun. 2025;16(1):2556. doi:10.1038/s41467-025-57860-0
26. Li D, Wang D, Zhou Y, et al. Neural effects of acupuncture on stroke patients with motor dysfunction: an activation likelihood estimation meta-analysis. Front Neurol. 2024;15:1453935. doi:10.3389/fneur.2024.1453935
27. Zhu W, Jia Q, Ferreira AC, et al. Acupuncture for ischemic stroke: where are we now? Acupuncture Herbal Med. 2024;4(1):36–55.
28. Wei NN, Pan JX, Chen YP, Chen Y. Effects of balance acupuncture combined with motor relearning for lower limb motor function of stroke patients with hemiplegia. Zhen Ci Yan Jiu. 2018;43(11):730–732. doi:10.13702/j.1000-0607.170913
29. Tian FL, Li Q, Liu GR, et al. Impacts of yin-yang meridians acupuncture with respiratory reinforcing and reducing manipulation on lower limbs balance function in stroke patients. Zhongguo Zhen jiu. 2014;34(11):1047–1050.
30. Yu T, Wang J, Jiao X, Li B, Zhang X, Zhu P. Clinical efficacy of antagonistic needling therapy on post-stroke lower limb spasticity and its effect on muscle morphology. Zhongguo Zhen jiu. 2025;45(2):139–145.
31. Dimyan MA, Cohen LG. Neuroplasticity in the context of motor rehabilitation after stroke. Nat Rev Neurol. 2011;7(2):76–85. doi:10.1038/nrneurol.2010.200
32. Campos B, Choi H, DeMarco AT, et al. Rethinking remapping: circuit mechanisms of recovery after stroke. J Neurosci. 2023;43(45):7489–7500. doi:10.1523/JNEUROSCI.1425-23.2023
33. Zheng C, Lee Y, Bin H, Jiong W. A randomized controlled trial comparing electroacupuncture with manual acupuncture for motor function recovery after ischemic stroke. Eur J Integr Med. 2018;22:76–80. doi:10.1016/j.eujim.2018.08.005
34. Li SS, Hua XY, Zheng MX, et al. Electroacupuncture treatment improves motor function and neurological outcomes after cerebral ischemia/reperfusion injury. Neural Regen Res. 2022;17(7):1545–1555. doi:10.4103/1673-5374.330617
35. Liu CH, Liao WL, Su SY, Chen WL, Hsieh CL. Electroacupuncture in the contralesional hemisphere improves neurological function involving GABA in ischemia-reperfusion injury rats. Evidence-Based Complement Altern Med. 2021;2021:5564494. doi:10.1155/2021/5564494
36. Li F, Sun Q, Shao XM, et al. Electroacupuncture combined with PNF on proprioception and motor function of lower limbs in stroke patients: a randomized controlled trial. Zhongguo Zhen Jiu. 2019;39(10):1034–1040.
37. Cho JE, Shin JH, Kim H. Does electrical stimulation synchronized with ankle movements better improve ankle proprioception and gait kinematics in chronic stroke? A randomized controlled study. NeuroRehabilitation. 2022;51(2):259–269. doi:10.3233/NRE-220018
38. Zheng K, Li L, Zhou Y, Gong X, Zheng G, Guo L. Optimal proprioceptive training combined with rehabilitation regimen for lower limb dysfunction in stroke patients: a systematic review and network meta-analysis. Front Neurol. 2024;15:1503585. doi:10.3389/fneur.2024.1503585
39. Wiśniowska-Szurlej A, Leszczak J, Brożonowicz J, Ciąpała G, Hernández-Lázaro H, Sozańska A. Effectiveness of a rehabilitation program involving functional proprioceptive stimulation for postural control and motor recovery among stroke patients: a double-blinded, randomized, controlled trial. J NeuroEng Rehab. 2025;22(1):147. doi:10.1186/s12984-025-01678-w
40. Zhan J, Ai Y, Zhan L, et al. Effect of abdominal acupuncture combined with routine rehabilitation training on shoulder-hand syndrome after stroke: a randomized controlled trial. Integr Med Res. 2022;11(2):100805. doi:10.1016/j.imr.2021.100805
41. Zhan J, Xiong B, Zhang P, et al. Abdominal acupuncture as an adjunctive therapy for the recovery of motor function after stroke: a systematic review and meta-analysis of randomized controlled trials. Front Neurol. 2021;12:705771. doi:10.3389/fneur.2021.705771
42. Jung YS, Lee S-W, Park JH, Seo HB, Choi BT, Shin HK. Electroacupuncture preconditioning reduces ROS generation with NOX4 down-regulation and ameliorates blood-brain barrier disruption after ischemic stroke. J Biomed Sci. 2016;23(1):32. doi:10.1186/s12929-016-0249-0
43. Chang QY, Lin YW, Hsieh CL. Acupuncture and neuroregeneration in ischemic stroke. Neural Regen Res. 2018;13(4):573–583. doi:10.4103/1673-5374.230272
44. Xie H, Gao Z, Fan Y, et al. Clinical observation of acupuncture combined with modern rehabilitation in the treatment of limb motor dysfunction after ischemic stroke: a randomized controlled trial. Medicine. 2022;101(45):e31703. doi:10.1097/MD.0000000000031703
45. Zhang C, Pang T, Chen Y, et al. Interactive dynamic scalp acupuncture enhances brain functional connectivity in bilateral basal ganglia ischemic stroke patients: a randomized controlled trial. Front Neurol. 2025;16:1604342. doi:10.3389/fneur.2025.1604342
46. Lin D, Gao J, Lu M, et al. Scalp acupuncture regulates functional connectivity of cerebral hemispheres in patients with hemiplegia after stroke. Front Neurol. 2023;14:1083066. doi:10.3389/fneur.2023.1083066
47. Chen L, Fang J, Ma R, et al. Additional effects of acupuncture on early comprehensive rehabilitation in patients with mild to moderate acute ischemic stroke: a multicenter randomized controlled trial. BMC Complement Alternative Med. 2016;16(1):226. doi:10.1186/s12906-016-1193-y
48. Song Y, Kang L, Dong H, Chen Y. Combined rehabilitation with scalp cluster acupuncture and constraint-induced movement therapy significantly improved functional recovery in patients with acute ischemic stroke. Int J Clin Exp Med. 2016;9(10):19797–19802.
49. Liu H, Jiang Y, Wang N, et al. Scalp acupuncture enhances local brain regions functional activities and functional connections between cerebral hemispheres in acute ischemic stroke patients. Anat Rec. 2021;304(11):2538–2551. doi:10.1002/ar.24746
50. Shin K-M, Park J-E, Liu Y, et al. Efficacy of moxibustion for pre- or stage I hypertension: study protocol for a pilot randomized controlled trial. Trials. 2012;13(1):188. doi:10.1186/1745-6215-13-188
51. Zhong Y-M, Cheng B, Zhang -L-L, Lu W-T, Shang Y-N, Zhou H-Y. Effect of moxibustion on inflammatory cytokines in animals with rheumatoid arthritis: a systematic review and meta-analysis. Evidence-Based Complem Alternative Med. 2020;2020(9):6108619. doi:10.1155/2020/6108619
52. Chen G, Huang C, Liu Y, et al. Efficacy and safety of grain moxibustion in hemiplegia: a systematic review and meta-analysis protocol. Medicine. 2019;98(17):e15215. doi:10.1097/MD.0000000000015215
53. Nakahara H, Kawai E, Miyamoto T. Acute effects of regional heat stimulation by indirect moxibustion on cardiovascular responses. J Physiol Sci. 2022;72(1):30. doi:10.1186/s12576-022-00855-z
54. Wang J, Du K, Liu C, et al. Exploring the effects of moxibustion on cognitive function in rats with multiple cerebral infarctions from the perspective of glial vascular unit repairing. Front Pharmacol. 2024;15:1428907. doi:10.3389/fphar.2024.1428907
55. Li L, Zhu W, Lin G, et al. Effects of acupuncture in ischemic stroke rehabilitation: a randomized controlled trial. Front Neurol. 2022;13. doi:10.3389/fneur.2022.897078
56. Zhu ZL, Shen TY, Sun Z, et al. Effects of zhongfeng cutong moxibustion on motor function and corticospinal tract in the patients with motor dysfunction during the recovery period of cerebral infarction. Zhongguo Zhen Jiu. 2023;43(12):1358–1362.
57. Zhang SH, Wang YL, Zhang CX, et al. Effects of interactive dynamic scalp acupuncture on motor function and gait of lower limbs after stroke: a multicenter, randomized, controlled clinical trial. Chin J Integr Med. 2022;28(6):483–491. doi:10.1007/s11655-021-3525-0
58. Zhang SH, Wang YL, Zhang CX, et al. Scalp acupuncture combined with lower-limb intelligent feedback training for lower-limb motor dysfunction after stroke: a randomized controlled trial. Zhongguo Zhen Jiu. 2021;41(5):471–477.
59. Huang YJ, Huang CS, Leng KF, Sung JY, Cheng SW. Efficacy of scalp acupuncture in patients with post-stroke hemiparesis: meta-analysis of randomized controlled trials. Front Neurol. 2021;12:746567. doi:10.3389/fneur.2021.746567
60. Cao B-Q, Tan F, Zhan J, Lai P-H. Mechanism underlying treatment of ischemic stroke using acupuncture: transmission and regulation. Neural Regen Res. 2021;16(5):944–954. doi:10.4103/1673-5374.297061
61. Liu L, Zhang Q, Li M, et al. Early post-stroke electroacupuncture promotes motor function recovery in post-ischemic rats by increasing the blood and brain irisin. Neuropsychiatric Dis Treatment. 2021;17:695–702. doi:10.2147/NDT.S290148
62. Qin S, Zhang Z, Zhao Y, et al. The impact of acupuncture on neuroplasticity after ischemic stroke: a literature review and perspectives. Front Cell Neurosci. 2022;16:817732. doi:10.3389/fncel.2022.817732
63. Kenei J, Moso J. Classification of heartbeats using convolutional neural network with range normalization. Medinformatics. 2025;2(2):120–131. doi:10.47852/bonviewMEDIN52024043
64. Zhang Y, Yin YL, Jin ZY, Hu QP, Wu XG. Electroacupuncture activates neuroplasticity in the motor cortex and corticospinal tract via the mTOR pathway in a rat P-MCAO model. BioMed Res Int. 2022;2022:3470685. doi:10.1155/2022/3470685
65. Zhu Y, Zhu X, Chen Z, et al. The efficacy of needle-warming moxibustion combined with hyperbaric oxygen therapy for ischemic stroke and its effect on neurological function. Computational Math Meth Med. 2022;2022:2204981. doi:10.1155/2022/2204981
66. Liu J, Luo X, Chen Y, et al. IDEAL-Acu: a methodological framework for evaluating the effects of acupuncture. J Evidence-Based Med. 2025;18(2):e70043. doi:10.1111/jebm.70043
67. Wang L, Su X-T, Cao Y, et al. Potential mechanisms of acupuncture in enhancing cerebral perfusion of ischemic stroke. Front Neurol. 2022;13:1030747.
68. Merdas HM. Elastic Net – MLP – SMOTE (EMS)-based model for enhancing stroke prediction. Medinformatics. 2024;1(2):73–78. doi:10.47852/bonviewMEDIN42022470
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effects of Immersive Virtual Therapy as a Method Supporting Recovery of Depressive Symptoms in Post-Stroke Rehabilitation: Randomized Controlled Trial
Kiper P, Przysiężna E, Cieślik B, Broniec-Siekaniec K, Kucińska A, Szczygieł J, Turek K, Gajda R, Szczepańska-Gieracha J
Clinical Interventions in Aging 2022, 17:1673-1685
Published Date: 23 November 2022
Influence of Acupuncture and Other Clinical Factors on the Recovery of Limb Motor Function in Patients After Stroke: A Retrospective Study
Wu B, Ding Y, Peng M, Wang X, Li Y, Cheng X
Journal of Multidisciplinary Healthcare 2023, 16:463-474
Published Date: 21 February 2023
The Role of Acupuncture and Its Related Mechanism in Treating Chronic Prostatitis/Chronic Pelvic Pain Syndrome
Wang H, Zhang J, Ma D, Zhao Z
International Journal of General Medicine 2023, 16:4039-4050
Published Date: 6 September 2023
Treatment of Allergic Rhinitis with Acupuncture Based on Pathophysiological
Dong B, Li B, Xie L, Li Y
International Journal of General Medicine 2024, 17:2741-2756
Published Date: 12 June 2024
Mechanism of Traditional Chinese Medicine in Treating Migraine: A Comprehensive Review
Chen Q, Wang M, Fu F, Nie L, Miao Q, Zhao L, Liu L, Li B
Journal of Pain Research 2024, 17:3031-3046
Published Date: 17 September 2024