")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Influence of Acupuncture and Other Clinical Factors on the Recovery of Limb Motor Function in Patients After Stroke: A Retrospective Study
Authors Wu B, Ding Y , Peng M , Wang X, Li Y , Cheng X
Received 18 November 2022
Accepted for publication 16 February 2023
Published 21 February 2023 Volume 2023:16 Pages 463—474
DOI https://doi.org/10.2147/JMDH.S398202
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Bangqi Wu,1,* Yi Ding,1,2,* Maohan Peng,1,2,* Xuhui Wang,1 Yibing Li,1,2 Xinyue Cheng1,2
1First Teaching Hospital of Tianjin University of Traditional Chinese Medicine, National Clinical Research Center for Chinese Medicine Acupuncture and Moxibustion, Tianjin, 300381, People’s Republic of China; 2Tianjin University of Traditional Chinese Medicine, Tianjin, 301617, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Bangqi Wu, First Teaching Hospital of Tianjin University of Traditional Chinese Medicine, No. 88, Changling Road, Xiqing District, Tianjin, 300381, People’s Republic of China, Tel +8613622026323, Fax +86-022-27982908, Email [email protected]
Background: Limb motor disorders after stroke are very common, and the clinical related factors of improving limb motor function are still unclear. As a part of comprehensive rehabilitation strategy, acupuncture has been widely used in rehabilitation after stroke in China. But more evidence is needed for the influence of acupuncture and some other clinical factors on post-stroke motor disorders.
Patients and Methods: A retrospective study was conducted using the database of patients with post-stroke motor disorders admitted to the Neurological Rehabilitation Unit of the First Teaching Hospital of Tianjin University of Traditional Chinese Medicine. The included patients were grouped according to whether NIHSS improved or muscle strength improved. The positive logistic regression was used to analyze the influencing factors of possible NIHSS improvement. Combined with the influencing factors of NIHSS improvement and muscle strength improvement, the influencing factors of limb motor function recovery after stroke were obtained.
Results: When analyzing the baseline of the included patients, it was found that patients with NIHSS improvement had earlier acupuncture intervention time (M, (IQR):13.5 (14), OR=0.716, 95% CI [0.591– 0.869], p=0.001), more cumulative acupuncture treatment times (M,(IQR):29 (12), OR=0.744, 95% CI [0.608– 0.910], p=0.004), and less hypertension history (OR=0.256, 95% CI [0.082– 0.801], p=0.019). Smoking history only has positive significance in univariate and multivariate analysis of NIHSS, not muscle strength (OR=0.274, 95% CI [0.097– 0.779], p=0.015).
Conclusion: The earlier acupuncture intervention and the more cumulative acupuncture treatment times are, the more beneficial the limb function of stroke patients with motor disorders will be. The previous history of hypertension is the influencing factor of limb motor function not improving in patients with limb motor disorder after a stroke. The effect of smoking history on limb movement function of patients with limb motor disorder after stroke needs further study.
Keywords: acupuncture, stroke, limb motor disorder, retrospective study, influencing factors
Introduction
The Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) 2017 shows stroke is the third leading cause of the five major causes of DALYs (measured by disability-adjusted life-years) worldwide and the second leading cause of death in the world in 2017. In 2019, stroke remained the second leading cause of death and the third leading cause of disability in the world.1–3 In china, due to the aging population, increased risk factors (hypertension, etc.), significant regional differences in access and quality of stroke care, and unreasonable allocation of medical resources, the prevalence and incidence rate of stroke have increased significantly and become the first leading cause of death.4,5 More than half of stroke survivors have neurological deficit symptoms,6 and the most common injury is motor disorder, such as contralateral limb hemiplegia,7 which seriously affects their physical and mental health and quality of life. The burden on patients increases significantly,3 which also leads to the continuous growth of demand for stroke rehabilitation services.8 Therefore, a better understanding of the influencing factors of motor function improvement in stroke patients with motor disorders may lead to more timely and effective prevention and intervention measures to prevent disease progression, improve the quality of life of patients and reduce disability rates.
A 1987 study on ‘Recovery from physical disability after stroke: normal patterns as a basis for evaluation’ showed that limb rehabilitation after stroke will be affected by many factors, such as age, stroke type, onset time, social and psychological variables.9 The onset time often represents the time when rehabilitation begins to intervene. When should rehabilitation begin after stroke be beneficial to the prognosis of patients? There is still no clear answer to this question. A retrospective cohort study showed that the earlier stroke patients were admitted to a rehabilitation hospital (IRH), the better their function improved.10 Strategies for improving motor function after stroke include rehabilitation physiotherapy and drugs, acupuncture as part of a comprehensive rehabilitation strategy is widely used in post-stroke rehabilitation in China.11 Some evidence suggests that acupuncture improves motor function in patients after stroke,12–15 and is a beneficial intervention factor for improving motor function in stroke patients with motor disorders. For stroke patients, ancient Chinese suggested early intervention with acupuncture,16 modern studies have shown that acupuncture at the early stage of stroke can improve recovery and reduce mortality,17 Before the active muscles of hemiplegic limbs do not have spasms, acupuncture can effectively reduce the occurrence of limb spasms after stroke.18 On the intervention time of acupuncture in rehabilitation after stroke, the current research conclusions are not consistent. A meta-analysis showed that the best time of acupuncture intervention for stroke was within 48 hours after stroke and lasted for 15 days;19 In a study of 2523 stroke patients (including 1922 cases of ischemic stroke and 601 cases of hemorrhagic stroke) treated by acupuncture, Shi et al20 showed that the cure rate in the group within 10 days of onset was significantly higher than that in the group within 11–20 days of onset, 21–120 days of onset and 4–12 months of onset, but there was no significant difference among the three groups within 10 days (≤48 h, 49–72 h and 4–10 days). However, it has also been reported that the promising good trend of early rehabilitation intervention after stroke is mostly reflected in small, single-center, and other pilot experiments,21 in a large-scale and confident Phase III trial conducted by AVERT investigators, the effectiveness of very early mobilization intervention was not proved.22 But there is no research showing that early acupuncture intervention after stroke has no good effect or even has the opposite effect, which is generally the dispute of intervention time. At present, other factors affecting the improvement of limb motor function after stroke need to be further studied.
Therefore, we designed this retrospective study to explore the influence of acupuncture and other clinical factors on the limb motor function of stroke patients, and the results are expected to save more health resources, hoping to provide an evidence-based reference for clinicians and researchers.
Materials and Methods
Study Design and Population
The First Teaching Hospital of Tianjin University of Traditional Chinese Medicine is the National Clinical Research Center for Chinese Medicine Acupuncture and Moxibustion, which integrates medicine, teaching, and research. The neurological rehabilitation unit is mainly to diagnose and treat neurological diseases, of which stroke accounts for more than 95%. Here we conducted a retrospective study on influencing factors of functional improvement in stroke patients with limb motor disorders. At least 5000 stroke patients are discharged from the neurological rehabilitation unit every year. The hospital has a broad professional foundation and provides advanced diagnostic procedures (such as MRI diagnosis). In this retrospective study, we screened and analyzed the electronic medical records of 5046 patients with post-stroke limb motor disorder hospitalized in the neurological rehabilitation unit of the First Affiliated Hospital of Tianjin University of Traditional Chinese Medicine from January 1, 2020, to January 1, 2022.
Definition
The course of disease = time from onset to treatment + hospital stay. Acupuncture intervention time is counted in days, which refers to the time from the onset of the disease to the beginning of acupuncture intervention. Acupuncture treatment times is counted in days, the patients are treated with acupuncture once a day from admission to discharge, the number of times of acupuncture treatment is approximately equal to the number of days in the hospital, and the cumulative number of times of acupuncture treatment is the total number of days in the hospital. The improvement of motor function in this study was evaluated by NIHSS score and Improvement of muscle strength. NIHSS score is a comprehensive score of the nervous system, including the score of limb motor function. In this study, improved NIHSS (One of the three scales for early prediction of stroke recovery23) is defined as the difference between admission NIHSS and discharge NIHSS>0, Not Improved NIHSS is defined as the difference between admission NIHSS and discharge NIHSS≤0. The improvement of muscle strength means that the patient’s muscle strength at the time of discharge is higher than that at the time of admission. The improvement of NIHSS and muscle strength means that the motor function of stroke limbs can be restored to a certain extent. Limb muscle strength ≤ IV: Muscle strength is divided into six levels from 0 to 5, the higher the muscle strength, the more normal, the fourth level of muscle strength means that the limbs can resist some resistance and gravity, but it is worse than normal people.
Inclusion Criteria
(1) Patients with first attack of stroke who had a definite diagnosis of bleeding or ischemic lesions by MRI or CT examination (Include patients with first stroke to reduce the impact of confounding factors) (2) Stroke patients with a course of disease between 40 and 50 days, age, gender not limited (3) Stroke patients with limb motor disorders (at least one limb muscle strength ≤ IV) (4) NIHSS score at admission ranged from 7 to 14 (5) The patient has not received any form of acupuncture treatment from the onset to hospitalization (The reason for choosing the course of disease of 40–50 days and NIHSS score of 7–14 is that there is no statistical difference in the baseline level of NIHSS of hospitalized patients within this range, and the NIHSS improved group is comparable with the non-improved group.)
Exclusion Criteria
(1) Patients with stroke motor disorder who refused acupuncture treatment after admission (2) Persons who are participating in or have participated in other trials for less than 3 months (3) Patients with a motor disorder caused by other reasons except for stroke (4) Severe medical disease, cancer or bleeding tendency (5) Incomplete electronic medical records.
See Figure 1 for the study flowchart.
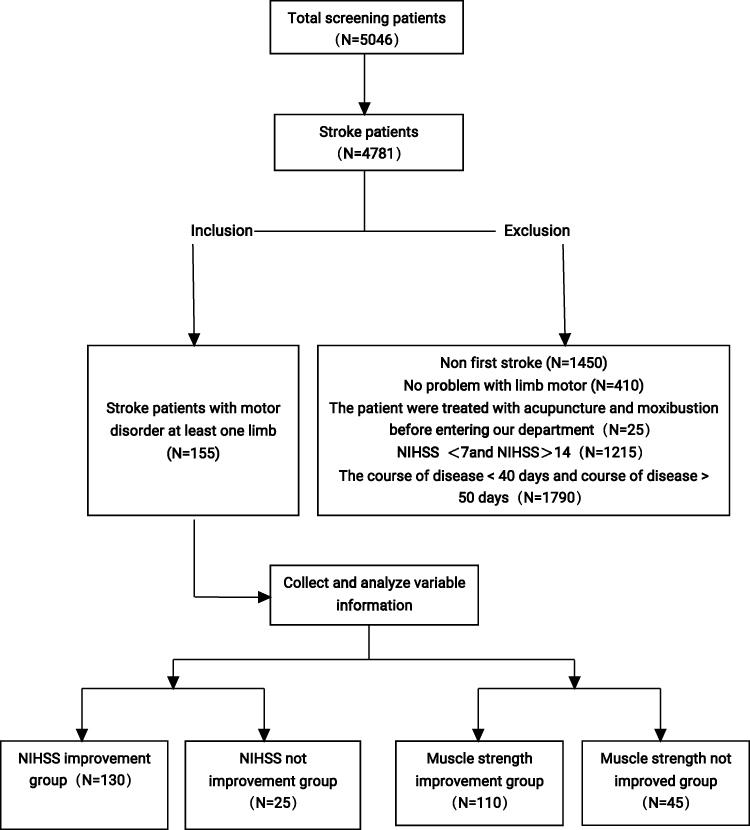 |
Figure 1 Study flowchart. |
Data Collection
First Teaching Hospital of Tianjin University of Traditional Chinese Medicine of Electronic Medical Record System is a Multimedia Electronic Medical Record Management System in Donghua-DHC-EMR, all medical records consist of a basic unit, composite unit, data template, and interface template, using the efficient indexing ability of cache database, data can be retrieved with high performance and complexity. In the electronic medical record system, the target patient population is determined according to the above Inclusion criteria. The medical records of this part of the population are retrieved by specially trained doctors (skilled in operating the electronic medical record hospitalization system), and the following variable information is extracted:
(1) Baseline characteristics: age, gender, hospital stay, smoking history, drinking history, past history, and family history (2) Motor function improvement assessment: neurological examination and clinical severity assessment, using the National Institutes of Health Stroke Scale (NIHSS) (scores from 0 to 42, the higher the score indicates greater neurological deficits); Muscle strength at admission and discharge (3) Acupuncture intervention time(days) and accumulated times of acupuncture treatment (number of times) (4) Complications.
Treatment
Patients with post-stroke motor disorders were given corresponding basic treatment, and blood pressure, blood glucose, water-electrolyte balance, nutritional support, active prevention, and treatment of complications were controlled. Antiplatelet drugs, anticoagulant drugs, lipid-lowering, fiber-lowering, nerve protection, and other symptomatic treatment were used. Routine rehabilitation guidance training for all patients. The patient received acupuncture treatment every day from the date of admission to discharge (Cases who refused to accept acupuncture treatment were not included in this study, and the treatment course is the days of hospitalization of the patient, that is, the patient receive acupuncture treatment every day during the period of hospitalization, and the treatment intensity is based on the patient’s tolerance). Acupuncture clinicians were trained by standard operating procedures, and the “sharpening mind and inducing consciousness”24 acupuncture method established by Academician Shi Xuemin was adopted.
Statistical Analysis
The data was extracted and exported from the platform in the form of Excel form. After export, the data was summarized and processed in Excel software. The processed data was imported into IBM SPSS (Statistical Product and Service Solutions) Statistics 25.0 (Hereinafter referred to as SPSS) analysis software for further screening and processing. SPSS is the earliest statistical analysis software in the world. It was developed by Norman H. Nie, C Hadlai (Tex) Hull, and Dale H. Bent and succeeded in research and development in 1968. At the same time, they established the SPSS Company. In 1975, they established a corporate organization and established SPSS headquarters in Chicago. On July 28, 2009, IBM announced that it would purchase SPSS, a statistical analysis software provider, with $1.2 billion in cash. The non-normally distributed numerical variables and grade data were analyzed with a non-parametric test (Mann–Whitney U-test). Count data are analyzed by chi-square test. Frequency (percentage) was used for categorical variables. Non-normal variables use median (Interquartile range, IQR). A value of p < 0.05 was considered statistically significant. A binary logistic regression model was used to analyze each explanatory variable, interpreted as odds ratio, 95% CI, and p-value. Whether they have hypertension history, or smoking history, were assigned values: yes 1, no 0.
Results
General Characteristics of Stroke Patients with Limb Motor Disorder
A total of 5046 patients with stroke were admitted to the First Teaching Hospital of Tianjin University of Traditional Chinese Medicine from January 1, 2020, to January 1, 2022. There were 745 cases of non-first stroke, 410 cases of normal limb muscle strength, 265 cases of non-stroke, 705 cases of stroke sequelae, and 25 cases of acupuncture after the onset, a total of 1215 patients were admitted with NIHSS less than 7 or NIHSS greater than 14, the course of the disease was less than 50 days and more than 40 days, a total of 1790 cases. A total of 155 cases met the inclusion criteria, including 130 cases in the NIHSS improvement group and 25 cases in the non-improvement group (Table 1).
 |
Table 1 Baseline of Stroke Patients with Motor Disorder |
Factors Affecting the Improvement of Motor Function in Patients with Stroke and Multivariate Analysis
According to the difference between admission NIHSS and discharge NIHSS, the patients were divided into two groups (improved group and non-improved group). Smoking, hypertension, and hyperhomocysteinemia in the non-improved group were significantly higher than those in the improved group (p < 0.05). The acupuncture intervention time in the non-improved group was longer and the number of acupuncture treatments were less (p < 0.05) (Table 2).
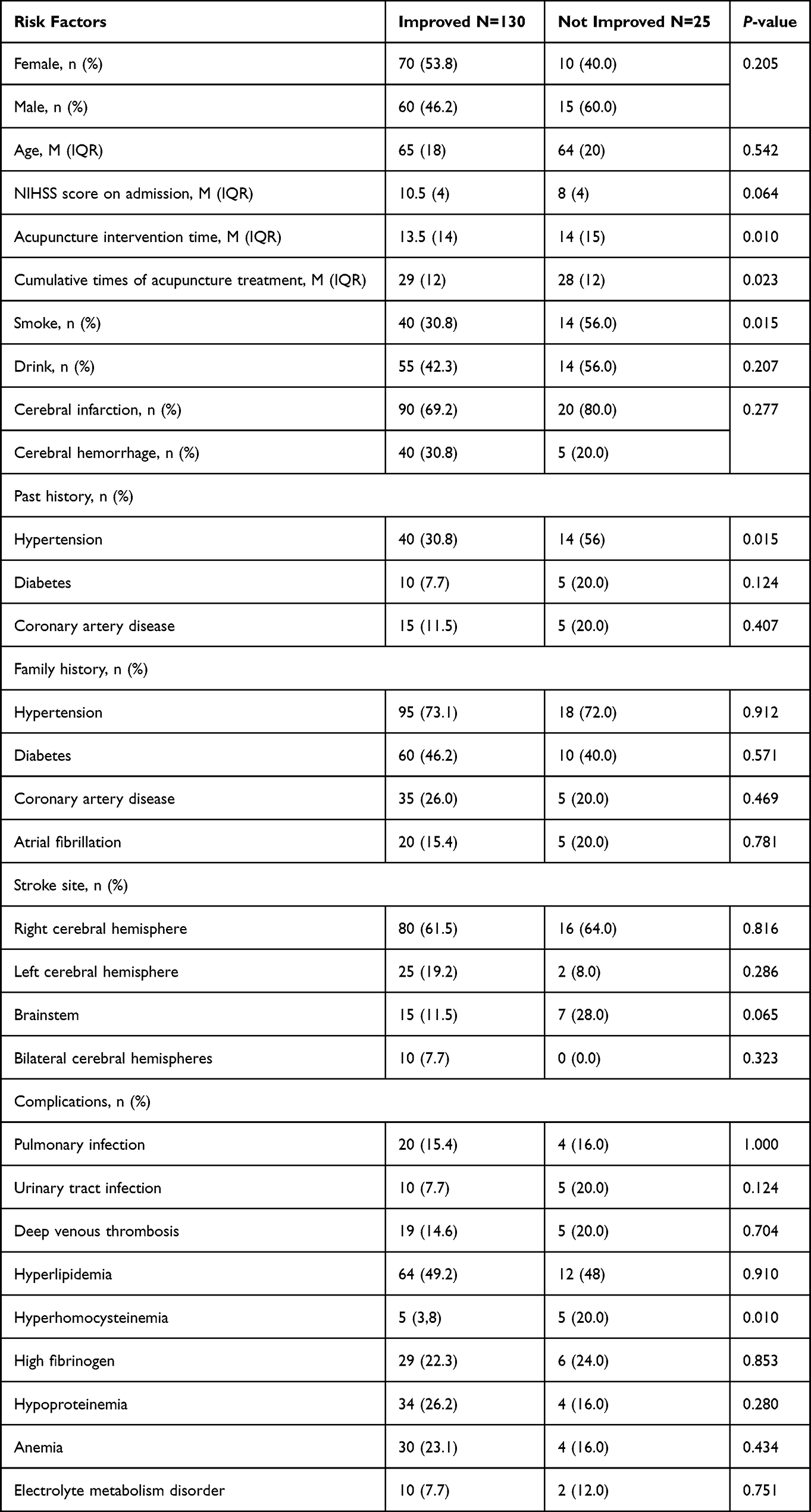 |
Table 2 Differences of Related Factors Between NIHSS Improvement Group and NIHSS No Improvement Group |
According to the difference between the muscle strength at admission and that at discharge, the patients were divided into two groups (muscle strength improvement group and muscle strength non-improvement group). The past history of hypertension in the improvement group was significantly lower than that in the non-improvement group (p<0.05), the acupuncture intervention time in the improvement group was earlier and the cumulative number of acupuncture was more (Table 3).
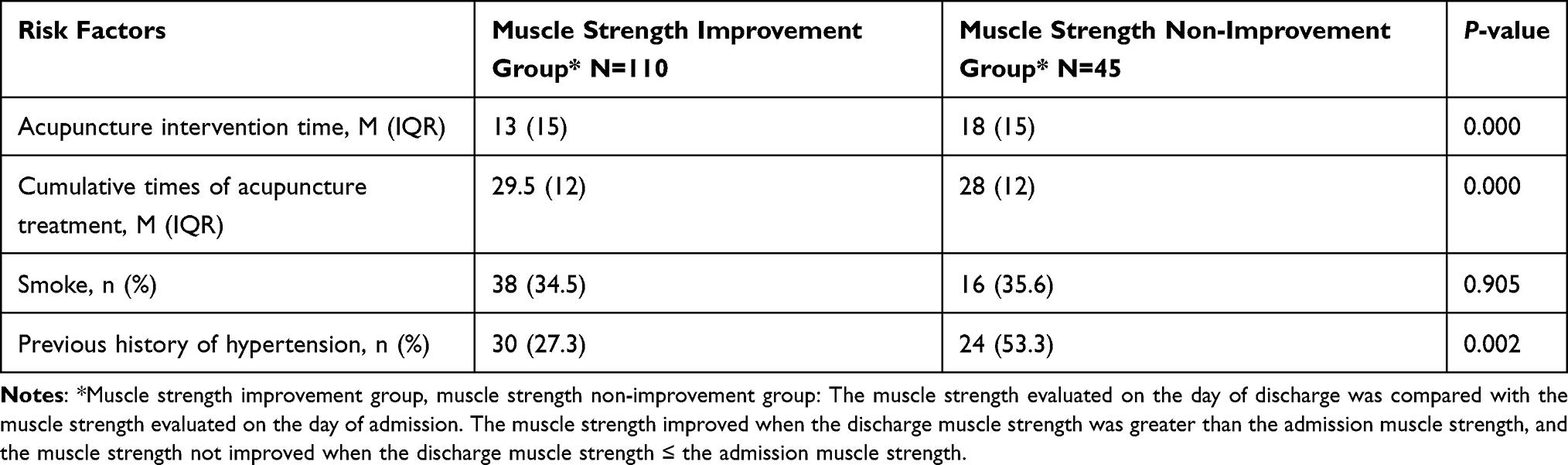 |
Table 3 Difference of Related Factors Between Muscle Strength Improvement Group and Muscle Strength Non-Improvement Group |
The influencing factors related to NIHSS improvement in univariate analysis were smoking, hypertension, hyperhomocysteinemia, acupuncture intervention time, and acupuncture treatment times (p < 0.05). In multivariate analysis, combined with the above-influencing factors, smoking (OR = 0.274, 95% CI [0.097–0.779], p < 0.05), hypertension (OR = 0.256, 95% CI [0.082–0.801], p < 0.05), acupuncture intervention time (OR = 0.716, 95% CI [0.591–0.869], p < 0.05), acupuncture treatment times (OR = 0.744, 95% CI [0.608–0.910], p < 0.05) were important predictors of NIHSS improvement in patients with stroke limb motor disorders. The possibility of non-improvement of NIHSS in smokers was 0.274 times that in non-smokers. The possibility of no improvement in NIHSS in patients with hypertension was 0.256 times that in patients without hypertension. The possibility of no improvement of NIHSS in patients with late acupuncture intervention is 0.716 times that in patients with early acupuncture intervention. The possibility of no improvement of NIHSS in patients with less cumulative acupuncture treatment is 0.744 times that in patients with more cumulative acupuncture treatment (Table 4).
 |
Table 4 Univariate and Multivariate Analysis of NIHSS Improvement and Clinical Characteristics of Stroke Patients with Motor Disorders |
It can be further discussed that smoking is significant in the group with NIHSS improved in Table 2, but not in the group with muscle strength improved in Table 3.
Discussion
Post-stroke limb movement disorder brings heavy economic and psychological burdens to patients, families, and society, leading to a substantial increase in demand for rehabilitation services. Therefore, understanding the influencing factors of functional improvement in patients with post-stroke limb motor disorders may produce more effective prevention and intervention methods for patients with post-stroke motor disorders. Here, we demonstrate that acupuncture intervention time, cumulative acupuncture treatment times, and hypertension history are the influence factors for improving limb function of stroke patients with motor disorders. Among them, the earlier the acupuncture intervention time is, the more times the accumulated acupuncture treatment is, the more beneficial to the improvement of limb function of stroke patients with motor disorders. A past history of hypertension is an unfavorable factor for the recovery of limb motor function of patients with stroke motor disorder. The effect of smoking on the limb motor function of patients with stroke motor disorder is effective for further study.
Whether acupuncture should be applied as soon as possible remains controversial in previous studies and guidelines on stroke, some studies25,26 have shown that the timing of acupuncture intervention is an independent factor affecting the disability status and degree of limb motor dysfunction in patients with limb dysfunction in cerebral infarction, early intervention may be better than late intervention, acupuncture intervention at the super early stage (within 6 hours) of stroke has obvious clinical value in terms of clinical efficacy, neurological function score, and muscle strength recovery. This study proposes that the earlier acupuncture intervention showed a better effect on motor dysfunction after stroke. It is reported that acupuncture can promote cell and neurogenesis in the injured area, and the regulation of neurochemicals induced by acupuncture is considered to be the main therapeutic mechanism.27 Ni et al believed that the curative effect, superoxide dismutase (SOD) activity, and malondialdehyde(MDA) content of early acupuncture intervention were better than those of stable acupuncture intervention in patients with cerebral infarction, early acupuncture treatment is more beneficial to improve the curative effect and anti-free radical ability of patients with cerebral infarction.28,29 Acupuncture is an alternative passive rehabilitation method, combined with active functional exercise that can better promote the recovery of motor function and daily life activities.29 In addition, based on the plasticity and functional reorganization of the nervous system, early acupuncture intervention can accelerate the establishment of cerebral collateral circulation, increase cerebral blood flow, improve cerebral oxygen metabolism, protect central neurons, reduce neuronal apoptosis, and promote the reorganization and compensation of surrounding tissues or healthy brain cells.29–33
However, due to the influence of non-therapeutic factors such as natural recovery rate within 3 weeks, the conclusion of early intervention remains to be discussed,25 and most of the studies ignore the different acupuncture cumulative amount with different acupuncture intervention time, which should also be considered as one of the factors.25 This study concluded that the more times cumulative acupuncture treatment is, the more beneficial to the improvement of limb motor function. The number of acupuncture times was a component of the cumulative amount of acupuncture treatment. In addition, it also included the cumulative acupuncture time. Many researchers believe that early rehabilitation is very important for maximum recovery from stroke, and the correlation between better results and early rehabilitation is recorded.34 In published reports, the increased time between stroke onset and rehabilitation onset is associated with poor prognosis. However, when other variables are adjusted, the time after stroke onset has little effect on the outcome before entering the rehabilitation facility.35 In summary, although acupuncture therapy has been widely used in acute stroke, the relationship between the specific intervention time and the benefit of motor function recovery needs to be further confirmed by more high-quality randomized controlled trials.
Smoking remains a major risk factor for stroke, and the dose-response relationship between smoking duration and stroke risk nearly doubles stroke risk.36,37 Compared with some unchangeable risk factors, such as age, gender, and family history, stroke prevention usually focuses on changeable risk factors. Lifestyle and behavioral changes, such as quitting smoking, can reduce not only the risk of stroke but also other cardiovascular diseases.38 Studies have shown that the risk of stroke in people who smoke only one cigarette per day is half that in people who smoke 20 cigarettes per day, much higher than expected.39 Smoking also harms the prognosis of motor function,40 smokers should aim at quitting smoking rather than reducing smoking, to reduce the risk of stroke and improve the prognosis. In the results in Table 2 and Table 4, smoking is an adverse factor affecting the recovery of limb motor function after stroke, but in Table 3, although the smoking rate in the muscle strength improvement group is 34.5%, and the smoking rate in the muscle strength non-improvement group is 35.6%, there is no statistical significance (p≥0.05), which may require further research.
The risk of stroke is closely related to blood pressure control,41 according to the latest evidence from clinical studies and randomized controlled trials (RCTs), the decline in stroke mortality observed over the past 50 years is partly due to improvements in control strategies and treatment for hypertension (BP).42 However, the effect of hypertension on the improvement of stroke motor function needs further high-quality clinical RCT studies to verify.
In the future, the optimal time for rehabilitation after a stroke may need to better understand the molecular mechanism of early physical activity induced by ischemic tissue, and provide the biological basis for selecting an intervention time window.22 Another challenge in early rehabilitation studies comes from the inherent heterogeneity of stroke patients, as other experts have observed.21 Developing biomarkers and other tools, the benefits of interventions that can be detected by reliable stratification of patients in the early stages of stroke according to their recovery potential are not visible in other undifferentiated populations. In addition, it is necessary to better understand the neurobiological mechanisms of spontaneous recovery and treatment-induced recovery in human subjects and understand the phenotype of stroke recovery,43 and avoid controllable human risk factors. In the future, whether to use a higher level of specificity scale score to evaluate the improvement of stroke motor function, or to collect and record only items about limb motor score in NIHSS score alone are factors that need to be reconsidered.
Limitations
This study has several limitations. Firstly, this retrospective study is a single-center design, which may be affected by bias. Second, according to the previous study,44 we can complete the screening of influencing factors for the improvement of the function of stroke patients with the motor disorder, but increasing the sample size may make the results more stable and reliable.
Conclusion
Acupuncture intervention time, cumulative times of acupuncture treatment, smoking, and hypertension have an impact on the improvement of NIHSS in patients with post-stroke motor disorders, that is, it has a certain impact on the recovery of limb motor function in patients with post-stroke motor disorders. Among them, receiving acupuncture treatment as soon as possible and persisting in acupuncture treatment for as long as possible may have a positive effect on the recovery of motor function of patients with post-stroke limb motor dysfunction, while patients with post-stroke motor dysfunction who have a history of hypertension may be more difficult to recover their limb motor function. The effect of smoking history on the recovery of limb motor function in patients with post-stroke motor disorder needs further discussion. Therefore, early acupuncture intervention, more accumulated times of acupuncture treatment, and no hypertension history may be the influencing factors of NIHSS improvement, that is, the beneficial factors for the recovery of limb motor function in patients with post-stroke motor disorders.
Data Sharing Statement
The database is publicly available within the hospital and allows unlimited reuse through open licensing.
Ethics Statement
This study has been approved by the IRB of The First Teaching Hospital of Tianjin University of TCM within which this study was undertaken. And that it conforms to the provisions of the Declaration of Helsinki. This clinical study is a retrospective study, which only collects the clinical data of patients, does not interfere with the treatment plan of patients, and will not bring risks to the physiology of patients. The data obtained remain anonymous. The collection of research data complies with national laws, regulations, and social ethics. The authors receive the approval of the institutional review board: The patients consent to review the medical records in this research was not required because the study design of this research is a retrospective study, it only collects the patient’s clinical data, does not interfere with the patient’s treatment plan, and will not bring risks to the patient’s physiology, has no harm to patients and no conflict of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Disclosure
The authors declare that there is no conflict of interest regarding the publication of this article.
References
1. Krishnamurthi RV, Ikeda T, Feigin VL. Global, regional and country-specific burden of ischaemic stroke, intracerebral haemorrhage and subarachnoid haemorrhage: a systematic analysis of the global burden of disease study 2017. Neuroepidemiology. 2020;54(Suppl. 2):171–179. doi:10.1159/000506396
2. Kyu HH, Abate D, Abate KH, et al. Global, regional, and national disability-adjusted life-years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1859–1922.
3. Stark BA, Roth GA, Adebayo OM, et al. Global, regional, and national burden of stroke and its risk factors, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021;20(10):795–820. doi:10.1016/S1474-4422(21)00252-0
4. Zhou M, Wang H, Zhu J, et al. Cause-specific mortality for 240 causes in China during 1990–2013: a systematic subnational analysis for the Global Burden of Disease Study 2013. Lancet. 2016;387(10015):251–272. doi:10.1016/S0140-6736(15)00551-6
5. Wu S, Wu B, Liu M, et al. Stroke in China: advances and challenges in epidemiology, prevention, and management. Lancet Neurol. 2019;18(4):394–405.
6. Di Carlo A. Human and economic burden of stroke. Age Ageing. 2008;38(1):4–5.
7. Lee KB, Lim SH, Kim KH, et al. Six-month functional recovery of stroke patients. Int J Rehabil Res. 2015;38(2):173–180.
8. Stinear CM, Lang CE, Zeiler S, Byblow WD. Advances and challenges in stroke rehabilitation. Lancet Neurol. 2020;19(4):348–360.
9. Partridge CJ. Recovery from physical disability after stroke: normal patterns as a basis for evaluation. Lancet. 1987;1(8529):373–375.
10. Wang H, Camicia M, Terdiman J, Hung Y, Sandel ME. Time to inpatient rehabilitation hospital admission and functional outcomes of stroke patients. Pm&R. 2011;3(4):296–304. doi:10.1016/j.pmrj.2010.12.018
11. Chen L, Fang J, Ma R, et al. Additional effects of acupuncture on early comprehensive rehabilitation in patients with mild to moderate acute ischemic stroke: a multicenter randomized controlled trial. Bmc Complem Altern M. 2016;16(1):226.
12. Zhu Y, Yang Y, Li J. Does acupuncture help patients with spasticity? A narrative review. Ann Phys Rehabil Med. 2019;62(4):297–301. Chinese. doi:10.1016/j.rehab.2018.09.010
13. Zhang S, Wu B, Liu M, et al. Acupuncture efficacy on ischemic stroke recovery. Stroke. 2015;46(5):1301–1306. doi:10.1161/STROKEAHA.114.007659
14. Gosman-Hedström G, Claesson L, Klingenstierna U, et al. Effects of acupuncture treatment on daily life activities and quality of life: a controlled, prospective, and randomized study of acute stroke patients. Stroke. 1998;10(29):2100–2108. doi:10.1161/01.STR.29.10.2100
15. Cao Y, Sun N, Yang J, et al. Does acupuncture ameliorate motor impairment after stroke? An assessment using the CatWalk gait system. Neurochem Int. 2017;107:198–203. doi:10.1016/j.neuint.2016.10.014
16. Ying Y, Yuan X, Yi G. 针灸早期介入在急救中的研究进展[Research progress of acupuncture intervening at early stage of first aid]. Guid J Tradit Chin Med. 2017;23(21):60–62.
17. Wu Z. 针灸治疗急性脑梗塞的疗效观察[Observation on the therapeutic effect of acupuncture and moxibustion on acute cerebral infarction]. J ClinAcupunMoxibus. 2007;07:27–28. Chinese.
18. Guo W, Wang Y, Bai Z. 针灸早期介入对脑梗塞后痉挛的影响[Effect of early acupuncture intervention on spasticity after cerebral infarction]. Chin J Trauma Disabil Medi. 2006;(04):37. Chinese.
19. Zhuo Y, Xu M, Deng S, et al. Efficacy and safety of dissimilar acupuncture intervention time-points in treating stroke: a systematic review and network meta-analysis. Ann Palliat Med. 2021;10(10):10196–10212. doi:10.21037/apm-21-1127
20. Shi X, Li J, Yan L, Li Y, Wu D. 针刺治疗中风病的临床研究[Clinical study on acupuncture treatment of apoplexy]. Shanghai J Acupun Moxibust. 1992;(04):4–7. Chinese.
21. Coleman ER, Moudgal R, Lang K, et al. Early rehabilitation after stroke: a narrative review. Curr Atheroscler Rep. 2017;19:12. doi:10.1007/s11883-017-0686-6
22. Group ATC. Efficacy and safety of very early mobilisation within 24 h of stroke onset (AVERT): a randomised controlled trial. Lancet. 2015;386(9988):46–55. doi:10.1016/S0140-6736(15)60690-0
23. Baird AE, Dambrosia J, Janket S, et al. A three-item scale for the early prediction of stroke recovery. Lancet. 2001;357(9274):2095–2099. doi:10.1016/S0140-6736(00)05183-7
24. Shi X. 醒脑开窍”针刺法治疗中风病9005例临床研究[Clinical Research on the Treatment of 9005 Cases of Apoplexy With the Acupuncture Method of Sharpening Mind and Inducing Consciousness]. Guiding J TCM. 2005;1:3–5. Chinese.
25. Li R, Wang R, Xiao L, et al. 针刺介入时机对脑梗死肢体功能障碍的影响:多中心前瞻性队列研究[Effect of timing of acupuncture on limb dysfunction in patients with cerebral infarction: a multicenter prospective cohort pilot study]. Chin Acupun Moxibust. 2021;41(03):257–262. Chinese.
26. Xiong J, Tao M, Zhang G, Lu M, Li L, Shi X. 应用醒脑开窍针刺法对急性脑梗死超早期患者神经功能缺损的影响[Effect of Xingnao Kaiqiao Acupuncture on Nerve Function Deficit in Patients with Acute Cerebral Infarction at Ultra early Stage]. TCM Clin Rehab. 2005;(37):4–5. Chinese.
27. Chavez L, Huang S, MacDonald I, Lin J, Lee Y, Chen Y. Mechanisms of acupuncture therapy in ischemic stroke rehabilitation: a literature review of basic studies. Int J Mol Sci. 2017;18(11):2270. doi:10.3390/ijms18112270
28. Lu H, Wang Z, Gan Y, Zhang C. Study on timing and dosage of acupuncture in stroke treatment. World J Acupun Moxibus. 2018;28(2):121–124. doi:10.1016/j.wjam.2018.06.007
29. Liu H, Chen L, Zhang G, et al. Scalp acupuncture enhances the functional connectivity of visual and cognitive-motor function network of patients with acute ischemic stroke. Evid-Based Compl Alt. 2020;2020:1–11.
30. Wu Q, Chen J, Yue J, et al. Electroacupuncture improves neuronal plasticity through the A2AR/cAMP/PKA signaling pathway in SNL rats. Neurochem Int. 2021;145:104983. doi:10.1016/j.neuint.2021.104983
31. Belskaya GN, Stepanova SB, Makarova LD, Sergienko DA, Krylova LG, Antimonova KV. Akupunktura v profilaktike i lechenii insul'ta: obzor zarubezhnykh issledovanii [Acupuncture in the prevention and treatment of stroke: a review of foreign studies]. Vopr Kurortol Fizioter Lech Fiz Kult. 2020;97(2):68–77. Russian. doi:10.17116/kurort20209702168
32. Wu Y, Hu R, Zhong X, et al. Electric acupuncture treatment promotes angiogenesis in rats with middle cerebral artery occlusion through EphB4/EphrinB2 mediated Src/PI3K signal pathway. J Stroke Cerebrovasc Dis. 2021;30(3):105165. doi:10.1016/j.jstrokecerebrovasdis.2020.105165
33. Li D, Chen Q, Zou W, et al. Acupuncture promotes functional recovery after cerebral hemorrhage by upregulating neurotrophic factor expression. Neural Regen Res. 2020;15(8):1510–1517. doi:10.4103/1673-5374.257532
34. Johnston MV, Keister M. Early rehabilitation for stroke patients: a new look. Arch Phys Med Rehabil. 1984;65(8):437–441.
35. Novack TA, Satterfield WT, Lyons K, Kolski G, Hackmeyer L, Connor M. Stroke onset and rehabilitation: time lag as a factor in treatment outcome. Arch Phys Med Rehabil. 1984;65(6):316–319.
36. Wolf P, D’Agostino R, Belanger A, Kannel W. Probability of stroke: a risk profile from the Framingham study. Stroke. 1991;22(3):312–318. doi:10.1161/01.STR.22.3.312
37. Bhat V, Cole J, Sorkin J, et al. Dose-response relationship between cigarette smoking and risk of ischemic stroke in young women. Stroke. 2008;39(9):2439–2443. doi:10.1161/STROKEAHA.107.510073
38. Boehme AK, Esenwa C, Elkind MSV. Stroke risk factors, genetics, and prevention. Circ Res. 2017;120(3):472–495. doi:10.1161/CIRCRESAHA.116.308398
39. Hackshaw A, Morris JK, Boniface S, Tang J, Milenković D. Low cigarette consumption and risk of coronary heart disease and stroke: meta-analysis of 141 cohort studies in 55 study reports. BMJ. 2018;360:j5855. doi:10.1136/bmj.j5855
40. Caglar NS, Akin T, Erdem IH, et al. Where are we in terms of poststroke functional outcomes and risk factors. Neurorehabilitation. 2014;34(3):391–399. doi:10.3233/NRE-141060
41. Lackland DT, Carey RM, Conforto AB, Rosendorff C, Whelton PK, Gorelick PB. Implications of recent clinical trials and hypertension guidelines on stroke and future cerebrovascular research. Stroke. 2018;49(3):772–779. doi:10.1161/STROKEAHA.117.019379
42. Lackland DT, Roccella EJ, Deutsch AF, et al. Factors influencing the decline in stroke mortality. Stroke. 2014;45(1):315–353. doi:10.1161/01.str.0000437068.30550.cf
43. Bernhardt J, Hayward KS, Kwakkel G, et al. Agreed definitions and a shared vision for new standards in stroke recovery research: the stroke recovery and rehabilitation roundtable taskforce. Int J Stroke. 2017;12(5):444–450.
44. Norman G, Monteiro S, Salama S. Sample size calculations: should the emperor’s clothes be off the peg or made to measure? BMJ. 2012;345:e5278.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.