Back to Journals » Journal of Pain Research » Volume 19
Acupuncture-Based Interventions for Sleep Outcomes in Patients with Postherpetic Neuralgia: A Systematic Review and Meta-Analysis
Authors Zhang J, Zhang J, Chen J ![]() , Li Z
, Li Z ![]() , Liu X
, Liu X ![]() , Chen S
, Chen S ![]()
Received 3 April 2026
Accepted for publication 5 June 2026
Published 19 June 2026 Volume 2026:19 613776
DOI https://doi.org/10.2147/JPR.S613776
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
Jingqi Zhang,1 Jiachen Zhang,2 Jie Chen,1 Zhaohua Li,1 Xiaorong Liu,1 Shaozong Chen3
1College of Acupuncture and Massage, Shandong University of Traditional Chinese Medicine, Jinan, People’s Republic of China; 2College of Traditional Chinese Medicine, Shandong University of Traditional Chinese Medicine, Jinan, People’s Republic of China; 3Research Institution of Acupuncture and Moxibustion, Shandong University of Traditional Chinese Medicine, Jinan, People’s Republic of China
Correspondence: Shaozong Chen, Shandong University of Traditional Chinese Medicine, 4655 Daxue Road, Changqing District, Jinan, Shandong, 250355, People’s Republic of China, Email [email protected]
Background: Acupuncture therapy is currently widely used in the clinical treatment of postherpetic neuralgia, but its effectiveness in improving patients’ sleep quality remains inconclusive. This study evaluates the impact of acupuncture-related therapies on sleep quality in patients with postherpetic neuralgia through a systematic review and meta-analysis.
Methods: We searched eight databases, including PubMed, Web of Science, Embase, Cochrane Library, China National Knowledge Infrastructure (CNKI), Wanfang Data, VIP Database for Chinese Technical Periodicals (VIP), and Chinese Biomedical Literature Database (CBM), with the search period ranging from each database’s inception to October 2025. The methodological quality of included studies was assessed using the Cochrane Risk of Bias Assessment Tool 2.0 (RoB 2). Statistical analysis was performed using Stata SE 15.0. This study’s registration number is: CRD420251184715.
Results: A total of 21 studies involving 1,739 patients were included. Meta-analysis results showed that acupuncture intervention significantly improved sleep quality in patients with postherpetic neuralgia compared with conventional treatment (SMD = − 1.21, 95% CI = − 1.48 to − 0.94, p < 0.0001). Subgroup analysis by acupuncture intervention type revealed that all acupuncture methods outperformed conventional treatment in improving sleep outcomes. Furthermore, analyses of secondary outcome measures—including pain scores (VAS), anxiety scores (SAS, HAMA), depression scores (SDS, HAMD), quality of life score (SF-36, NHP), clinical effectiveness, and adverse events—also indicated that acupuncture therapy demonstrated superior efficacy in broader clinical outcomes among PHN patients.
Conclusion: Acupuncture-related therapies may improve sleep quality in patients with postherpetic neuralgia. However, high-quality RCTs with more stringent designs and broader coverage of acupuncture techniques should be conducted in the future to verify its efficacy.
Keywords: postherpetic neuralgia, acupuncture therapy, sleep quality, Traditional Chinese medicine, systematic review, meta-analysis
Introduction
Postherpetic neuralgia (PHN) refers to persistent unilateral stabbing or burning pain that occurs after an episode of herpes zoster (HZ)1 and persists for at least one month after the resolution of skin lesions;2 it is the most common long-term complication of varicella-zoster virus reactivation.3 The incidence of HZ is high; in China, for example, the combined annual incidence of HZ across all age groups is 4.28/1000 people.4 Between 5% and 30% of HZ patients are at risk of developing PHN,5 with the risk of PHN in elderly HZ patients being no less than 20%.6 Given the increasing global aging of the population, the incidence of PHN is likely to rise further.7,8 In addition to persistent pain, PHN is often compounded by sleep disturbances, anxiety, depression, and even suicidal tendencies, which significantly impact patients’ quality of life and social functioning. Among these, sleep disturbances are one of the most common and clinically significant comorbid symptoms in PHN patients. Studies indicate that approximately 50.5% of PHN patients experience insomnia to varying degrees, while 30.6% meet the clinical criteria for moderate to severe insomnia.9 Sleep disturbances are not only closely associated with pain severity,10 but they also further exacerbate anxiety, depression, and daily functional impairment, creating a vicious cycle between pain and sleep disturbances. Therefore, independently and specifically assessing and intervening in the sleep quality of PHN patients is of critical importance for improving overall prognosis.
Current treatment methods for sleep disorders in PHN patients include pharmacotherapy,11 interventional surgery,12 and neuromodulation.13 However, these approaches remain suboptimal in clinical practice: oral medications have limited efficacy, often require combination with other therapies,14 while also carrying adverse effects;15 other methods are mostly invasive, with inconsistent efficacy, and carry risks of infection and nerve damage.16 Although these treatments can alleviate clinical symptoms in PHN patients to some extent, long-term use is often limited by adverse reactions, invasive procedures, and compliance issues. Due to the limitations of traditional therapies, there is an urgent clinical need to identify a safer intervention strategy with more comprehensive regulatory effects.
Acupuncture, as a non-pharmacological and non-invasive treatment method, offers advantages such as high efficacy, minimal side effects, and a high safety profile.17 According to Traditional Chinese Medicine, stimulating specific acupoints along the meridians can promote the circulation of qi and blood, regulate organ functions, and achieve the effects of balancing yin and yang, alleviating pain, and calming the mind. Modern medical research confirms that acupuncture not only alleviates PHN-related pain but also directly or indirectly improves patients’ sleep disorders through multi-target mechanisms. For instance, it may directly modulate neurotransmitter release,18 regulate the neuroendocrine axis response,19 modulate immune function,20 and optimize autonomic nervous system balance.21
Current acupuncture therapies, including manual acupuncture,22 electroacupuncture,23 fire needling,24 and plum-blossom needling,25 have been widely used to treat sleep disorders in PHN patients.26,27 Zhou et al observed that acupuncture combined with cupping was significantly more effective than traditional oral pharmacotherapy in reducing the incidence of PHN and patients’ VAS scores;28 Cui et al further indicated that acupuncture combined with cupping and antiepileptic drugs is currently the most effective treatment regimen.29 Tang et al proposed that electroacupuncture could serve as one of the treatment options for patients with refractory PHN.30 In addition, certain specialized needling techniques, such as Wrist-ankle acupuncture, have demonstrated significant efficacy and warrant attention.31 Though multiple systematic reviews have confirmed the positive effects of acupuncture on PHN pain, these studies have primarily focused on pain relief or overall efficacy, and there remains a lack of systematic evaluations specifically addressing sleep disturbances in PHN. Furthermore, the relative efficacy of different acupuncture techniques in improving sleep remains unclear. Considering the impact of sleep quality on the prognosis and quality of life of PHN patients, this study conducts an evidence-based investigation through a systematic review and meta-analysis to assess the relative efficacy of different acupuncture techniques in improving sleep in PHN patients. Additionally, the study further evaluates their effects on pain, emotional symptoms, quality of life, and safety to provide evidence-based guidance for clinical treatment.
Methods
This study employed the latest PRISMA 2020 criteria, and we explicitly declare that the review was conducted in accordance with the PRISMA 2020 guidelines. A complete scheme for this study was registered in the Prospective Register of Systematic Reviews (PROSPERO): CRD420251184715.
Search Strategies
Two researchers independently searched eight electronic databases: PubMed, Web of Science, Embase, Cochrane Library, China National Knowledge Infrastructure (CNKI), Wanfang Data, VIP Database for Chinese Technical Periodicals (VIP), and Chinese Biomedical Literature Database (CBM). The search period covered the inception of each database through October 2025, to ensure the comprehensiveness of the search, no language or regional restrictions were imposed during the literature review process. The search strategy combined subject headings with free-text terms. The search strategy comprised two parts: (1) “postherpetic neuralgia”, “herpetic neuralgia”, “PHN”, “Herpes Zoster”, “Neuralgia”. (2) “Acupuncture”, “Acupuncture Therapy”, “Acupuncture Points”, “acupoint”, “Electroacupuncture”, “fire needling”, “acupuncture, ear”, “Wrist-Ankle Acupuncture”, “acupotomy”, “catgut embedding”, and all expressions corresponding to the aforementioned terms. The specific search strategy is detailed in Supplementary Table 1. To prevent literature omission, we manually searched the references of included studies and relevant reviews.
Inclusion Criteria
Inclusion criteria were established according to PICOS principles: (1) Population: Adult patients aged ≥18 years with a confirmed diagnosis of PHN, defined as persistent pain lasting ≥1 month after rash resolution,32 or meeting the diagnostic criteria of the original study. To account for potential variations arising from different clinical settings and ensure comparability of baseline data, we will collate, compile, and verify the specific diagnostic guidelines and definitions of PHN disease course used in each included study. (2) Intervention: The treatment group received acupuncture-related therapies as the primary approach, such as manual acupuncture, electroacupuncture, fire needling therapy, warm needling therapy, plum-blossom needling therapy, auricular acupuncture, abdominal acupuncture, wrist-ankle acupuncture, acupotomy, or catgut embedding therapy. All interventions involved transdermal insertion into specific acupoints or body regions. Variations in technique details were permitted, acupuncture can be used either as a stand-alone therapy or in combination with conventional treatment (such as conventional medications and routine nursing care), provided that the baseline characteristics and standard care between the intervention group and the control group are identical. (3) Comparator: Includes sham acupuncture, placebo, standard clinical care, and guideline-recommended conventional drug regimens for PHN,33 along with symptomatic or supportive medications used according to clinical practice based on subjects’ comorbidities or concomitant symptoms. Treatment designs can be tailored to individual subject characteristics. Comparisons between “standard treatment + acupuncture” versus “standard treatment + sham acupuncture” or “standard treatment alone” are permitted within the same standard treatment context. (4) Outcomes: Must include at least one sleep-related outcome. Primary sleep quality measures should be sleep quality scales or indices, such as the Pittsburgh Sleep Quality Index (PSQI), Insomnia Severity Index (ISI), or Athens Insomnia Scale (AIS),34 or objective sleep parameters, including sleep duration, sleep latency, and sleep efficiency. Secondary outcomes include pain scores, overall clinical effectiveness, anxiety/depression scores, quality of life scores, and adverse events. (5) Study design: Include randomized controlled trials (RCTs).
Exclusion Criteria
(1) Meta-analyses, reviews, animal experiments, case reports, etc. (2) Study participants in the acute phase of herpes zoster or with unhealed skin lesions, without a definitive diagnosis of PHN; those with comorbid conditions potentially affecting sleep, where such effects could not be distinguished or excluded in the study. (3) Interventions combining acupuncture with oral or topical Chinese herbal medicine, moxibustion, cupping, massage, or physical therapy; combining acupuncture with physical therapy, rehabilitation therapy, or specialized nursing interventions; concurrent use of two or more distinct acupuncture techniques; or use of pharmacological treatments that may significantly interfere with acupuncture efficacy, resulting in uncorrectable intergroup medication imbalances, precluding independent assessment of acupuncture intervention effects.(4) Studies with control groups involving any form of acupuncture-related treatment, traditional Chinese medicine therapies, physical therapy, surgical interventions, or the use of experimental or non-conventional drug regimens not recommended by guidelines. (5) Studies lacking reported sleep quality measures, with missing or unavailable data for quantitative or qualitative analysis. (6) Studies with unclear descriptions of intervention protocols, control measures, or research designs, preventing assessment of compliance. (7) Publications not originally published in Chinese or English.
Literature Selection and Data Collection
Jingqi Zhang and Jiachen Zhang conducted literature screening and data extraction. First, based on predefined inclusion and exclusion criteria, they independently screened the retrieved literature, removed duplicates, performed an initial screening of titles and abstracts, and obtained full texts for secondary screening of potentially eligible studies. Second, data extraction encompassed baseline characteristics including: first author, publication year, study design, intervention type, sample size, participant age, disease duration, specific diagnostic criteria (including guidelines and duration definitions), and acupuncture site. Any discrepancies or disputes during this process were resolved with assistance from Jie Chen to determine the final list of included studies.
Quality Assessment
Two independent reviewers (Jingqi Zhang, Jiachen Zhang) assessed the risk of bias using the Cochrane Risk of Bias tool version 2.0 (RoB 2.0) for randomized trials.35 Each study was rated as “low risk of bias,” “some concerns,” or “high risk of bias” across the following areas: bias arising from the randomization process; bias arising from deviation from the intended intervention; bias arising from missing outcome data; bias in outcome measurement; and bias in selection of the reported result, including bias related to protocol registration. If the risk of bias was rated “high” in one or more domains, the trial was classified as having an overall high risk of bias. If all domains were rated as “low” risk of bias, we classified the trial as overall low risk of bias. After the assessment was completed, Jingqi Zhang and Jiachen Zhang cross-checked the results. In cases of disagreement, Jie Chen assisted in resolving them.
Statistical Analysis
This meta-analysis employed StataSE 15.0. For dichotomous outcome measures, we used relative risk (RR) and its 95% confidence interval (CI) as the effect size. For continuous outcome measures, we used the mean difference (MD) and its 95% CI when studies employed the same measurement tool. Otherwise, we used the standardized mean difference (SMD) and its 95% CI if different scales were used. When data were presented as median and interquartile range, or as median (lower quartile, upper quartile), we converted them to mean ± SD for further analysis, following the methods of Luo et al (2018)36 and Wan et al (2014).37 If studies reported both baseline and final measurements, we used the change values. For scales with reverse-scoring criteria, means were multiplied by −1 to ensure directional consistency. Statistical significance was set at p < 0.05. Heterogeneity was assessed using the I2 statistic and p-value. When I2 ≤ 50% and p ≥ 0.05, low heterogeneity was assumed, employing a fixed-effects model. When I2 > 50% and p < 0.05, indicating substantial heterogeneity, a random-effects model would be adopted. If heterogeneity is significant, we will explore its sources through subgroup analyses, sensitivity analyses, or meta-regression analyses, considering both clinical and methodological characteristics. Although this study included a variety of acupuncture techniques, these interventions were all based on acupuncture theory-such as acupoint stimulation and meridian regulation—and were therefore considered sufficiently comparable for pooled analysis. This study’s subgroup analysis aims to explore potential differences in efficacy among different acupuncture techniques, rather than precisely quantifying the absolute effect size of acupuncture. Therefore, studies employing pure acupuncture and acupuncture combined with modern medicine will be analyzed together within the same acupuncture technique subgroup. For outcome measures included in ≥10 studies, we will construct funnel plots to assess publication bias and perform Egger’s linear regression test.
Results
Literature Search Results
Database searches yielded 13,069 records. After removing 6,700 duplicates, we excluded 6,278 studies based on title and abstract screening due to irrelevance to the research topic, leaving 91 records for full-text evaluation. During the full-text review stage, 70 articles were excluded for the following reasons: population did not meet inclusion criteria (1 article), intervention measures were inconsistent or unclear in design (21 articles), control measures did not meet requirements (15 articles), lack of reporting on required outcome measures (12 articles), non-randomized controlled studies (3 articles), publication of study protocols only (4 articles), and registered studies with unpublished results (14 articles). Ultimately, 21 studies38–58 met the criteria and were included in this review. The literature screening process is detailed in Figure 1.
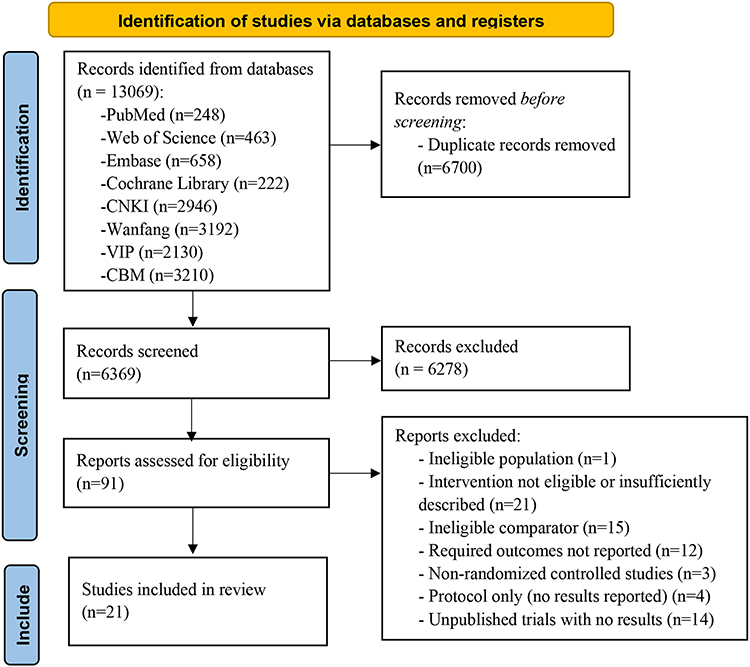 |
Figure 1 PRISMA flow diagram. |
Basic Characteristics of the Studies
This review included 21 studies published between 2018 and 2025, conducted exclusively in China. Twenty studies were single-center investigations, while one was a multi-center trial. Patients’ average age ranged from 42.58 to 69 years, and the average duration of disease ranged from 1.71 to 27.6 months. Intervention methods included: acupotomy therapy (3 studies), fire needling therapy (5 studies), manual acupuncture (6 studies), electroacupuncture (3 studies), plum-blossom needling therapy (2 studies), silver needle heat therapy (1 study), and wrist-ankle acupuncture (2 studies). Regarding treatment duration, 8 studies lasted 28 days, 4 lasted 14 days, 3 lasted 21 days, 3 lasted 42 days, 1 lasted 36 days, 1 lasted 12 days, and 1 did not report specific duration. For outcome measures, among sleep-related indicators, 15 studies used the PSQI scale, 2 used the AIS scale, and 1 used the SRSS scale. Additionally, 2 studies assessed sleep quality using sleep quality scores, and 1 used Continuous Sleep Duration. Nineteen studies used the VAS to assess pain score. For quality of life outcomes, 3 studies used the SF-36 scale and 1 used the NHP scale. Anxiety and depression levels were assessed using the SAS scale in 2 studies, the SDS scale in 2 studies, the HAMA scale in 2 studies, and the HAMD scale in 1 study. Twenty studies reported comparative clinical effectiveness results, and 9 reported adverse reaction incidence. Baseline characteristics of included studies are detailed in Table 1.
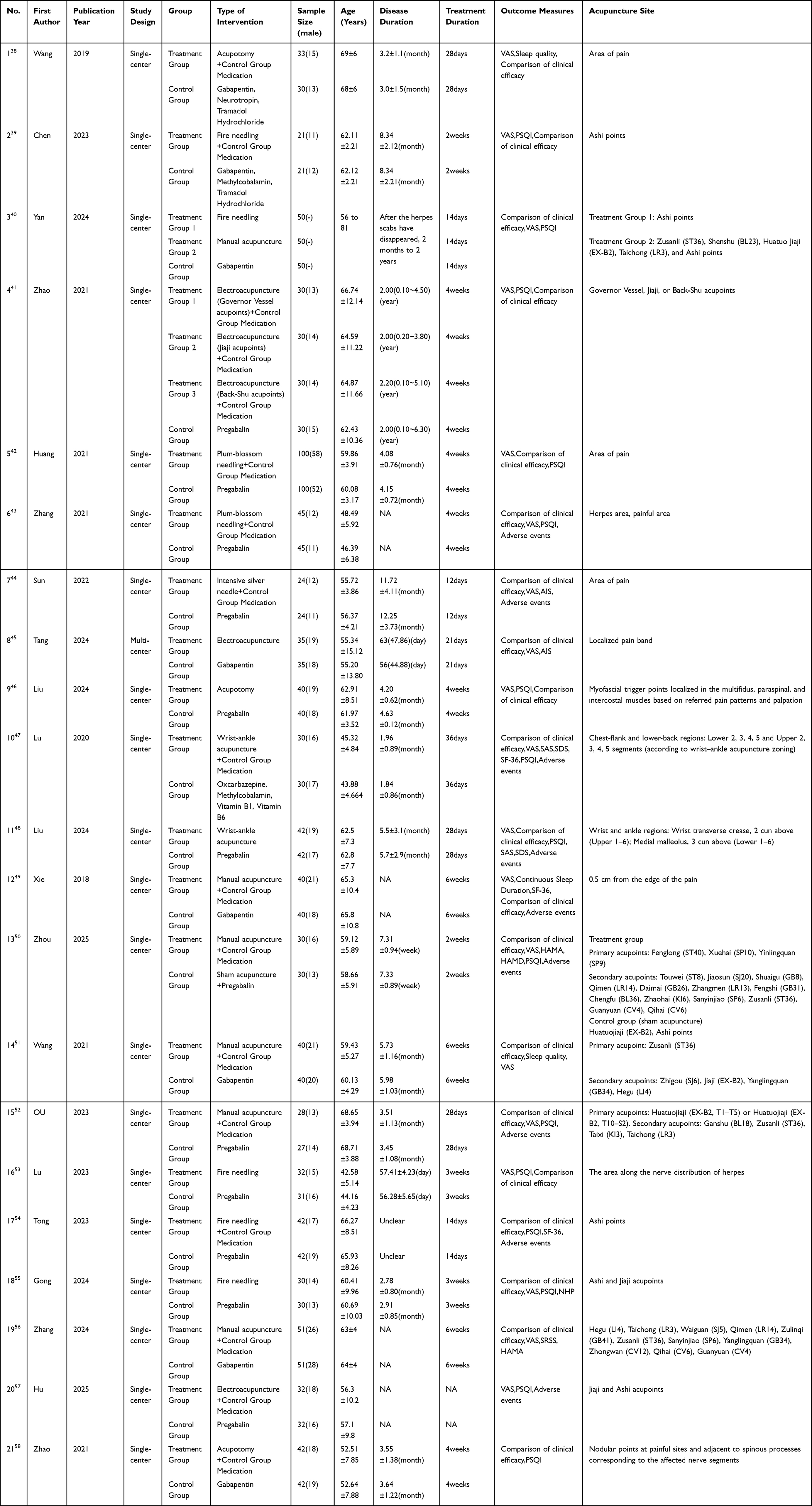 |
Table 1 Basic Information of the Included Literature |
Regarding diagnostic criteria for PHN (see Supplementary Table 2 for details), 16 studies reported specific diagnostic guidelines, with the 2016 edition of the “Chinese Expert Consensus on the Diagnosis and Treatment of Postherpetic Neuralgia” being the most frequently cited reference. The remaining 5 studies did not explicitly specify the diagnostic basis. Regarding the definition of PHN duration, most trials required that pain persist for ≥1 month after the resolution of the rash or skin lesions. However, there were slight clinical variations among studies. For example, Gong 2024 required a PHN duration of 1–6 months, while Hu 2025 adopted a stricter criterion of more than 90 days after the healing of skin lesions. Additionally, 9 studies lacked a clear operational definition of PHN duration in the main text.
Yan 2024 involved a three-arm randomized controlled trial comprising manual acupuncture, fire needling therapy, and a drug control group. To fully utilize clinical data and facilitate combined analysis with the other two arms, the statistical analysis included two independent comparisons: manual acupuncture versus the same control group, and fire needling therapy versus the same control group. We recognize that breaking down a multi-arm study into multiple independent comparisons may carry a risk of statistical double-counting; however, given that one of the core objectives of this study is to explore the differences among various acupuncture techniques, this approach allows us to preserve as much information as possible regarding specific techniques from the original study. The Zhao 2021 intervention comprised three protocols: “electroacupuncture on the Governor Vessel + control group medication,” “electroacupuncture at jiaji acupoints + control group medication,” and “electroacupuncture at beishu acupoints + control group medication.” This study focused on the overall efficacy of acupuncture-related therapies; thus, these arms were combined for analysis.
Risk of Bias Assessment
In the 21 included studies, 2 were rated as high risk of bias and 19 as having some concerns (see Figure 2A and B). Specifically, Wang 2019 and Lu 2023 were rated as high risk. Both studies reported patient withdrawals during treatment due to pain or intolerance, and neither conducted an intention-to-treat analysis, suggesting potential intervention deviation that may have influenced outcomes. Furthermore, the reasons for missing data in both studies were related to primary outcomes, yet no appropriate handling of missing data was performed, potentially leading to overestimation of efficacy. Lu 2023 exhibited a high overall missing data rate, and the control group experienced dropouts due to intolerable pain, further increasing the risk of bias. The remaining 19 studies were classified as “some concerns.” Due to the unique nature of acupuncture interventions, none of the studies could clearly confirm whether blinding was implemented during the research process, leaving some uncertainty about “bias arising from deviation from the intended intervention.” Most studies described the randomization process, but Yan 2024, Sun 2022, Wang 2021, Gong 2024, and Zhang 2024 did not specify the exact methods. None of the studies provided access to their protocols, precluding assessment of potential selective reporting regarding study design and outcome measures.
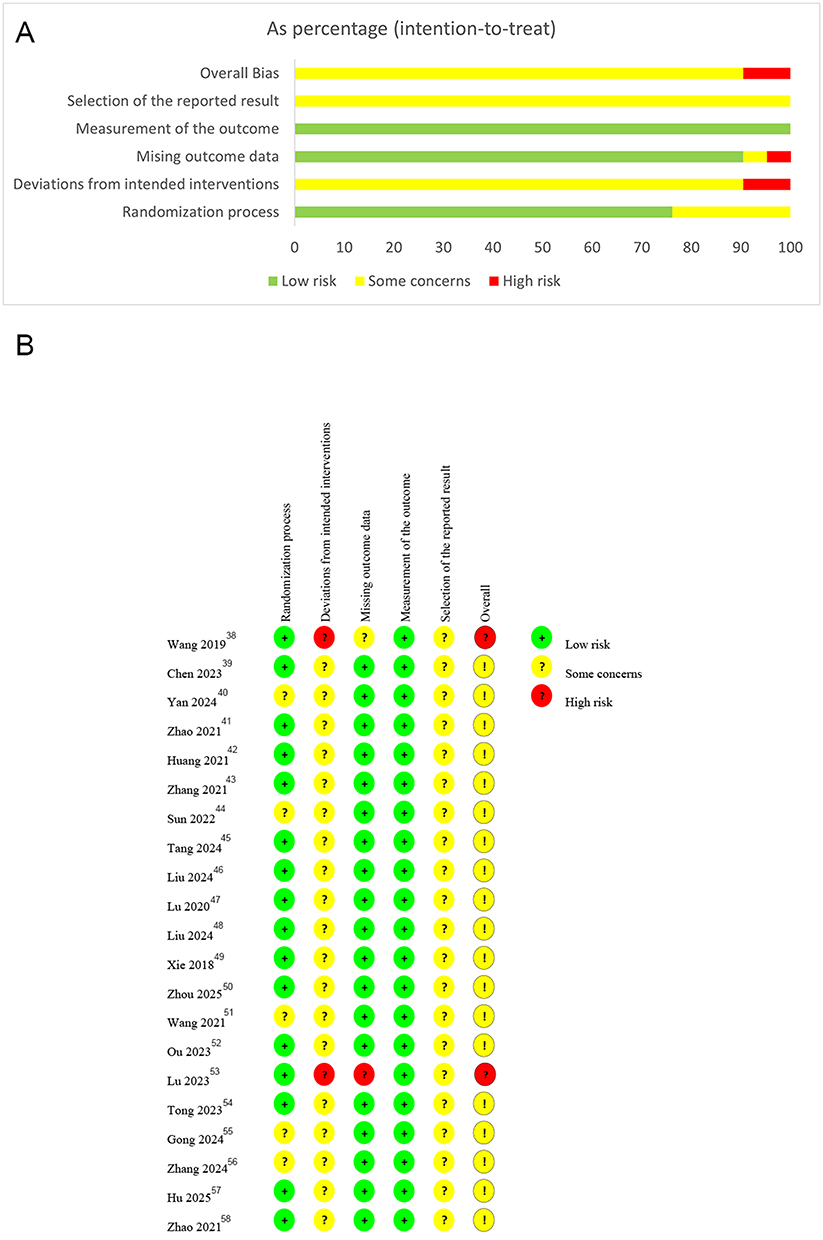 |
Figure 2 (A) and (B) Assessment of risk of bias summary. |
Analysis of Outcome Measures
Primary Outcome Measures
Twenty studies involving 1,659 participants were included. We analyzed the effects and efficacy of acupuncture on improving sleep quality in patients with PHN. Statistical analysis revealed significant heterogeneity among studies (I2 = 84.6%), warranting a random-effects model for the meta-analysis. Results demonstrated that acupuncture significantly outperformed the control group in improving sleep quality (SMD = −1.21, 95% CI: −1.48 to −0.94, p < 0.0001), implying acupuncture may help alleviate sleep disturbances and enhance sleep quality in PHN patients. Detailed findings are presented in Figure 3.
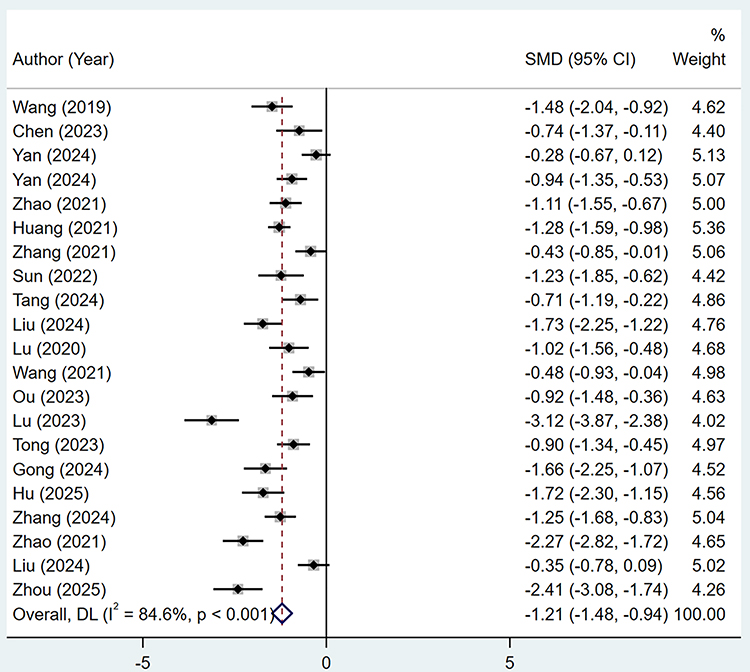 |
Figure 3 Forest plots of sleep quality. Note: Weights are from random-effects model. |
Another study (Xie 2018) analyzed the outcome of continuous sleep duration. There was no statistically significant difference in continuous sleep duration between the two groups before treatment (P>0.05). After 3 and 6 weeks of treatment, both groups showed significant increases in continuous sleep duration compared to baseline (both P<0.05). Moreover, the treatment group consistently demonstrated significantly longer continuous sleep duration than the control group (P<0.05), indicating that acupuncture therapy was superior to conventional treatment alone in prolonging continuous sleep duration.
Secondary Outcome Measures
The meta-analysis included 3 to 20 studies and summarized secondary outcome measures, including pain score, anxiety score, depression score, quality of life score, clinical effectiveness, and adverse events. Heterogeneity tests revealed significant heterogeneity for Pain score (I2=98.2%), Anxiety score (I2=91.6%), Depression score (I2=93.3%), and Quality of life score (I2=92.3%); No significant heterogeneity was observed for Clinical effectiveness (I2=0.0%) and Adverse events (I2=42.6%). Meta-analysis results revealed that the acupuncture group demonstrated statistically significant advantages over the control group in the following outcome measures: pain score, anxiety score, depression score, quality of life score, and clinical effectiveness (P<0.05). However, there was no statistically significant difference between the two groups in adverse events (P>0.05). These findings confirm that the acupuncture group demonstrated superior improvement compared to the control group in pain, anxiety, depression, quality of life, and clinical effectiveness among PHN patients. No significant differences between the two groups were observed regarding adverse reactions. Pooled effect sizes and statistical results for each outcome measure are detailed in Table 2; forest plots for individual outcomes are presented in Supplementary Figure 1–6.
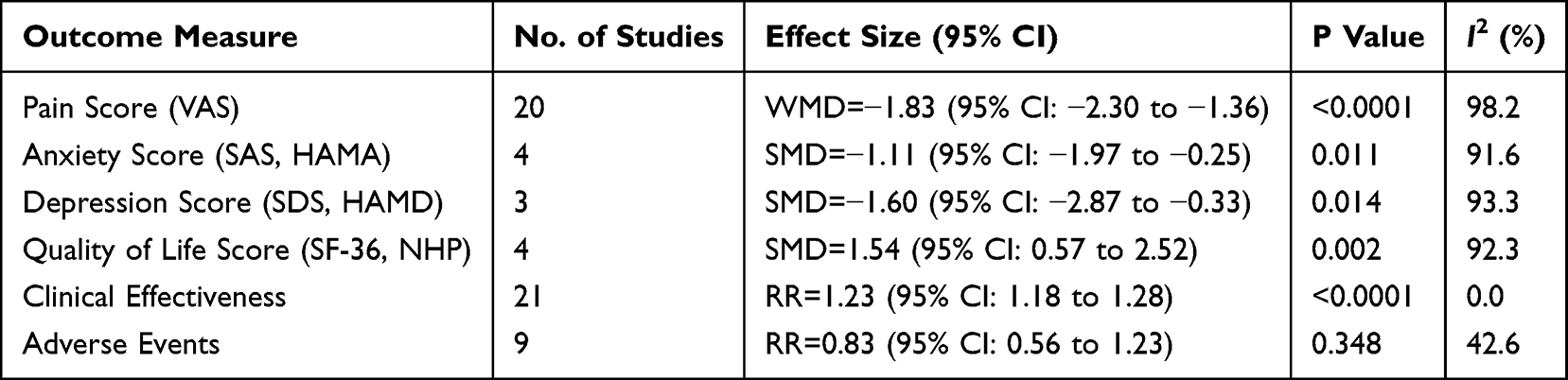 |
Table 2 Secondary Outcome Measures |
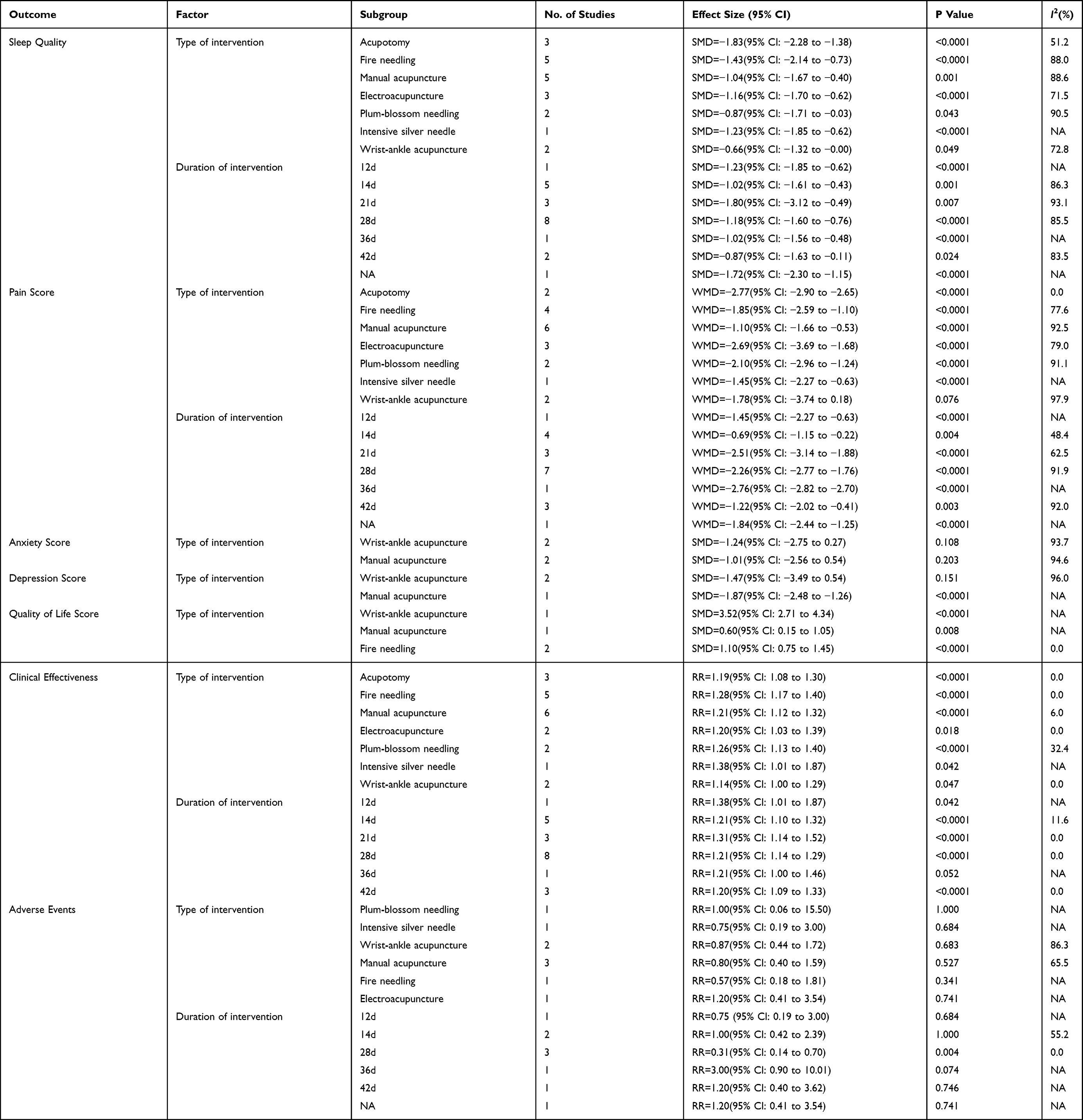 |
Table 3 Other Subgroup Analysis |
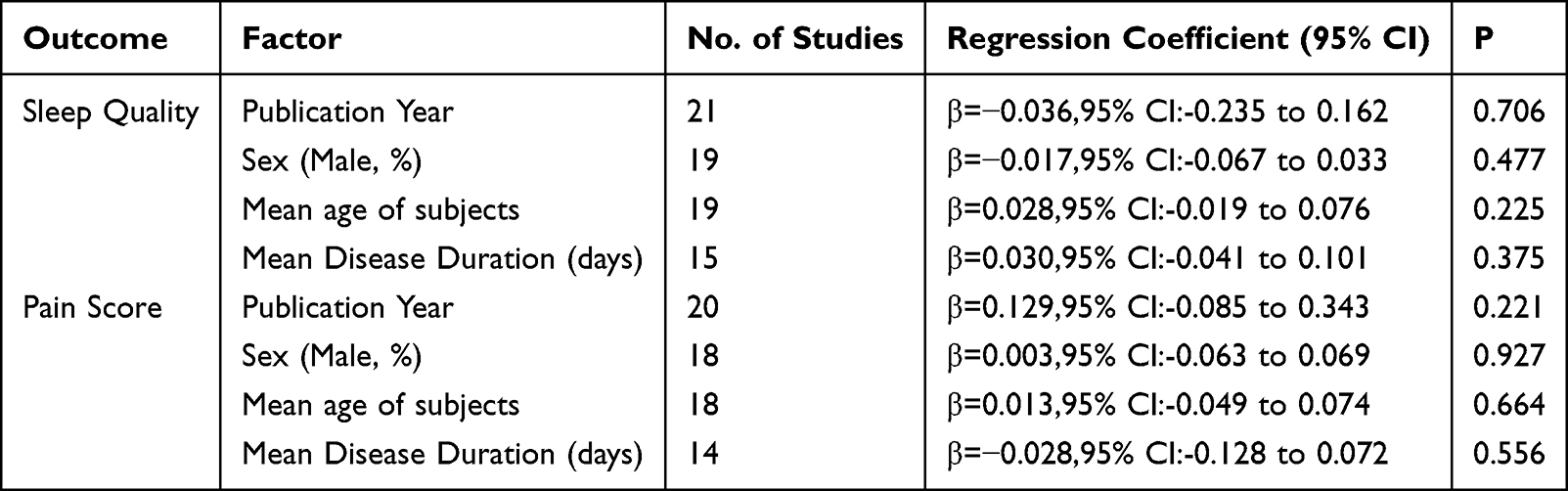 |
Table 4 Meta-Regression |
Sensitivity Analysis
We conducted a sensitivity analysis for seven outcome measures: sleep quality, pain score, anxiety score, depression score, quality of life score, clinical effectiveness, and adverse events. We sequentially excluded individual included studies, recalculated the pooled effect sizes for the remaining studies, and compared these with the original pooled results. Results showed negligible changes in pooled effect sizes for all outcomes after excluding any single study, without substantial alterations in overall direction or statistical significance, indicating robust and reliable findings. Sensitivity analysis for sleep quality is presented in Figure 4; analyses for other outcomes appear in Supplementary Figures 7–12.
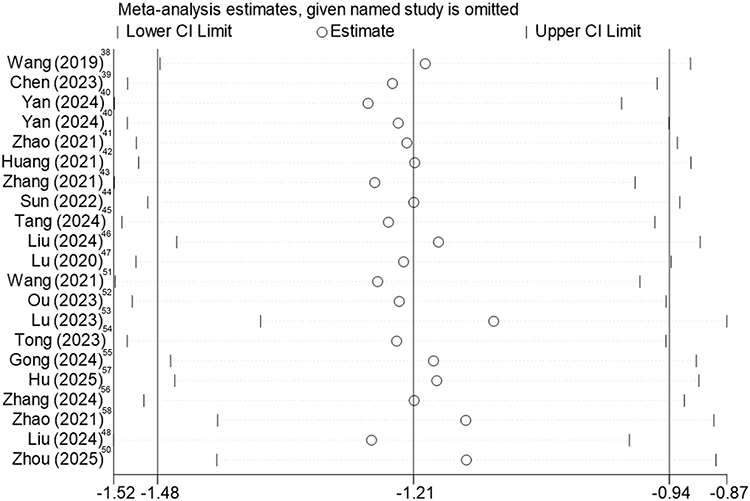 |
Figure 4 Sensitivity analysis of sleep quality. |
Assessment of Publication Bias
Initially, we visually assessed publication bias for the seven outcomes—sleep quality, pain score, anxiety score, depression score, quality of life score, clinical effectiveness, and adverse events—using funnel plots. Results indicated that the scatter plots were not perfectly symmetrical, suggesting potential publication bias. See Supplementary Figures 13–19. We further conducted quantitative analysis of funnel plot asymmetry using the Egger test. Results showed that the p-values for Pain score (p=0.084) and Adverse events (p=0.830) were both greater than 0.05, indicating no significant publication bias for these two outcome measures. The Egger test p-values for the other outcomes were as follows: Sleep quality (p=0.016), Anxiety score (p=0.001), Depression score (p=0.014), Quality of life score (p=0.025), and Clinical effectiveness (p=0.005), all of which were less than 0.05, suggesting potential publication bias for these outcomes. For Anxiety score, Depression score, and Quality of life outcomes, the limited number of included studies precluded trim-and-truncate analysis to correct for potential publication bias. The trim-and-truncate-adjusted pooled effect size for Sleep quality was −1.207 (95% CI: −1.478 to −0.936). The pooled effect size for clinical effectiveness after trim-and-fill correction was 1.190 (95% CI: 1.145 to 1.236), as shown in Supplementary Figures 20 and 21. Compared before trim-and-fill correction, the adjusted effect size showed no significant change and remained within the confidence interval of the pre-trimmed pooled effect. This implies that even if publication bias exists, its impact on the overall conclusion is limited.
Exploration of Heterogeneity
Subgroup Analysis
Given the significant heterogeneity in sleep quality assessment results, we further conducted subgroup analyses based on acupuncture type and treatment duration. The findings suggest that the type of acupuncture may be a partial source of heterogeneity, though treatment duration has not been confirmed as a significant source of heterogeneity.
Subgroup analysis by acupuncture modality (Figure 5) revealed that all acupuncture-related therapies improved sleep quality compared to the control group. The acupotomy subgroup demonstrated the numerically largest pooled effect size (SMD = −1.83, 95% CI: −2.28 to −1.38) and relatively low heterogeneity (I2 = 51.2%). The pooled effect sizes for fire needling (SMD = −1.43), electroacupuncture (SMD = −1.16), and silver needle heat conduction (SMD = −1.23) subgroups were also substantial. The pooled effect sizes for manual acupuncture (SMD = −1.04), plum-blossom needling (SMD = −0.87), and wrist-ankle acupuncture (SMD = −0.66) were relatively lower, and the pooled effect size for wrist-ankle acupuncture was also relatively small. Heterogeneity remained high within most subgroups. Statistically significant differences were not observed between different acupuncture type subgroups (p = 0.089).
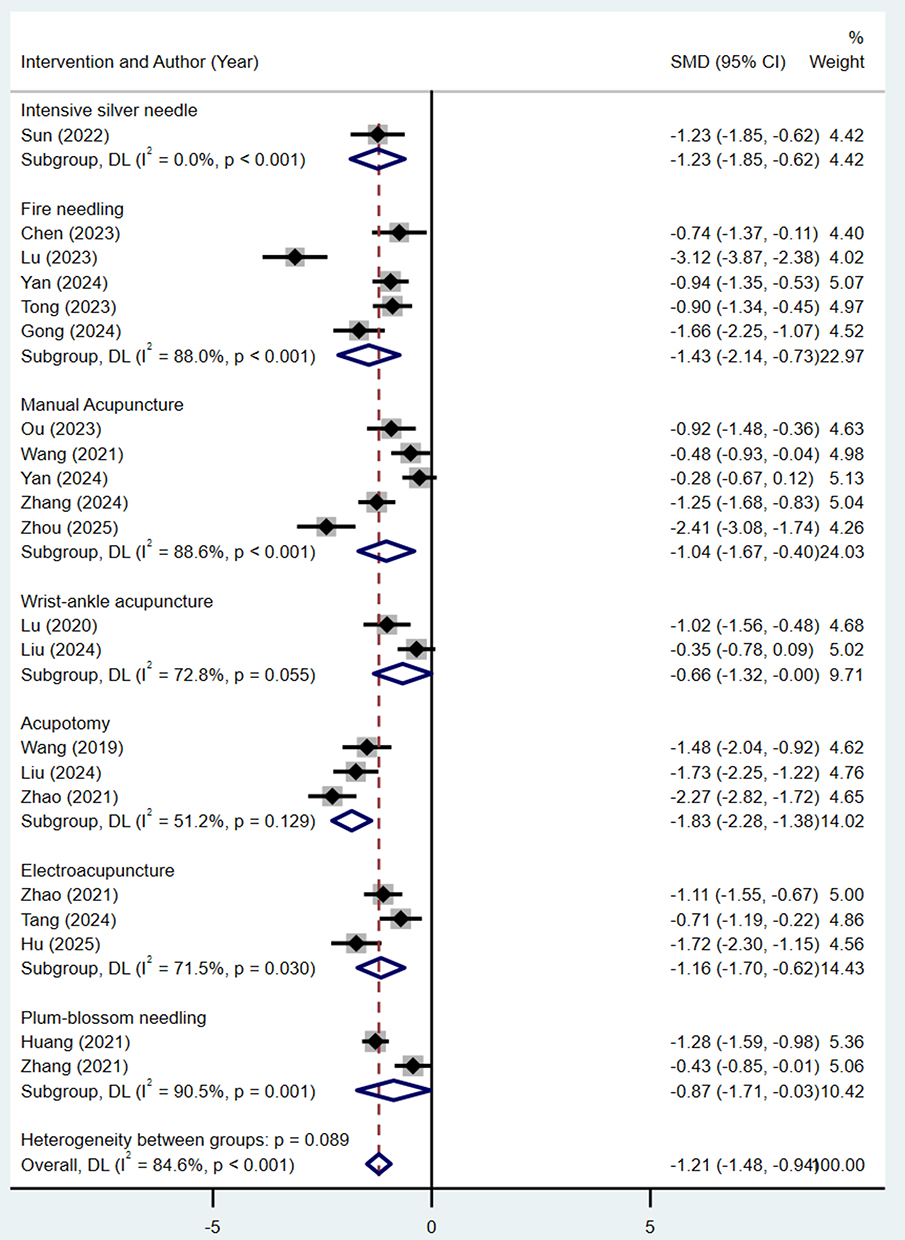 |
Figure 5 Forest plots of subgroup analysis of Treatment method. Note: Weights and between-subgroup heterogeneity test are from random-effects model. |
Analysis by treatment duration subgroups (Figure 6) indicated that acupuncture-related therapies significantly improved sleep quality in patients with postherpetic neuralgia compared to the control group across all subgroups. The pooled effect sizes were similar in the 28-day subgroup (SMD = −1.18, 95% CI: −1.60 to −0.76) and the 14-day subgroup (SMD = −1.02, 95% CI: −1.61 to −0.43). The 21-day group showed a larger effect size (SMD = −1.80), but with excessive heterogeneity (I2 = 93.1%). The 42-day group demonstrated a relatively smaller improvement (SMD = −0.87). No significant differences were observed between treatment groups (p = 0.482).
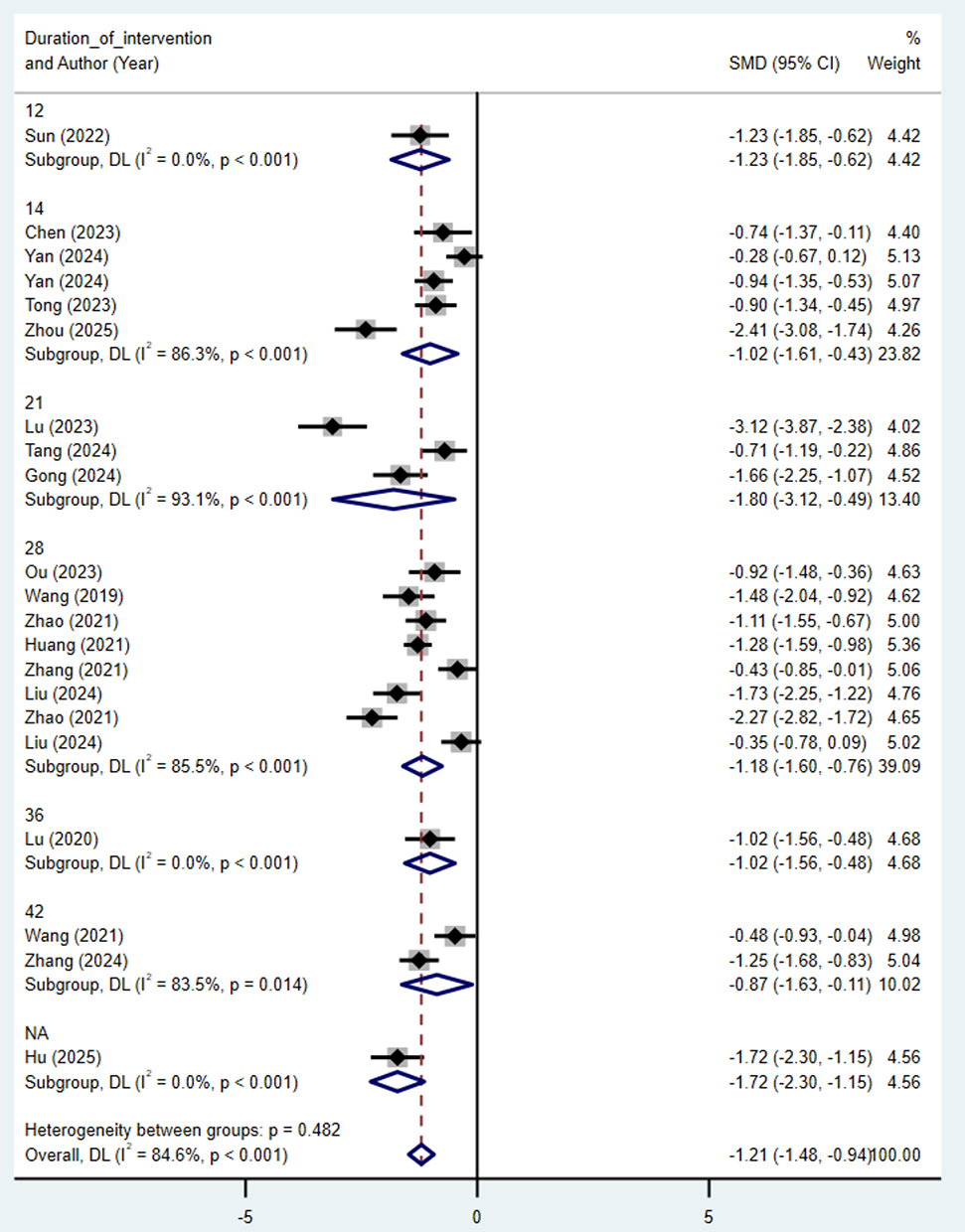 |
Figure 6 Forest plots of subgroup analysis of Course of treatment. Note: Weights and between-subgroup heterogeneity test are from random-effects model. |
Additionally, we performed subgroup analyses on pain scores, anxiety scores, depression scores, quality of life scores, clinical effectiveness, and adverse events outcome measures to explore potential sources of heterogeneity and influencing factors. Detailed results for each outcome measure appear in Table 3.
Meta-Regression Analysis
Additionally, we employed meta-regression analysis on four continuous variables—publication year, proportion of males in the intervention group, mean age, and mean disease duration—to investigate their potential influence on study heterogeneity for the two outcomes: sleep quality and pain scores. Results indicated that none of these factors showed significant associations with study heterogeneity (all P > 0.05), indicating they may not be primary sources of heterogeneity. See Table 4 for details.
Discussion
This study summarized 21 RCTs and conducted a systematic review to evaluate the effects of acupuncture-related therapies, such as manual acupuncture, electroacupuncture, fire needling, and acupotomy, on the sleep quality of patients with PHN. Results suggested that acupuncture exhibited potential advantages over conventional drug therapy in improving sleep quality. Most acupuncture treatments demonstrated a trend toward improvement; however, given the inherent heterogeneity among the included studies, these efficacy trends should be interpreted with caution. Although treatment outcomes varied across different intervention cycles, they generally favored the acupuncture groups compared to the control. Furthermore, acupuncture was associated with greater improvements in overall therapeutic efficacy, reducing pain scores, alleviating anxiety and depression, and improving quality of life, maintaining a clinically acceptable safety profile throughout.
Our findings build upon and expand the insights from previous systematic reviews and meta-analyses. Wang et al26 analyzed 7 RCTs comparing various acupuncture methods with pharmacologic therapy and found acupuncture superior for pain relief. However, they noted that evidence for sleep improvement remained inconclusive at that time due to the limited number of studies reporting this outcome. In contrast, our study confirms the definitive efficacy of acupuncture for sleep quality by incorporating a significantly larger and more recent body of evidence published between 2018 and 2025. A previous Bayesian network meta-analysis by Cui et al29 based on 29 RCTs comparing 10 acupuncture therapies combined with antiepileptics against antiepileptics alone for VAS, PSQI, and depression scores, revealed that electroacupuncture combined with antiepileptic drugs exhibited the most significant advantage in reducing patients’ PSQI scores. In our study, which updates the evidence with 21 RCTs through 2025, the acupotomy subgroup exhibited the largest pooled effect size for sleep outcomes. While differences between subgroups in our study were exploratory, this finding differs from Cui et al’s results because our inclusion of more recent, high-quality RCTs identifies acupotomy’s unique potential to improve sleep quality by releasing soft tissue adhesions. Yang et al,59 including 9 RCTs, evaluated collateral-pricking and bloodletting cupping combined with electroacupuncture against conventional drugs (eg., pregabalin or carbamazepine) or electroacupuncture alone regarding efficacy rate, VAS, and PSQI scores. They demonstrated that this combination is effective for alleviating pain and improving sleep. Our study is consistent with this trend for PSQI improvement; however, by evaluating a broader spectrum of acupuncture modalities across 21 updated RCTs, our synthesis provides more comprehensive and robust clinical guidance for managing sleep disturbances in PHN patients.
PHN is a common neuropathic pain condition, and its chronic pain often leads to psychiatric symptoms such as insomnia, anxiety, and depression,60 adversely affecting quality of life. Traditional Chinese medicine refers to HZ as “Chan Yao Huo Dan (waist-wrapping fire toxin)” or “Snake-like sores”,61 and PHN with a course of ≥3 months falls under the category of “pain after recovery from snake toxin”.62 Its pathogenesis relates to the principles of “pain due to obstruction” and “pain due to deficiency of nourishment.” Pain often arises from residual damp-heat toxins and Qi deficiency, leading to blood stasis obstructing collaterals and meridian blockage. It manifests as a pattern of qi stagnation and blood stasis with underlying deficiency and superficial excess.2,62 Prolonged pain disturbs the mind, preventing yang from entering yin, thus causing sleep disturbances.63 Traditional Chinese medicine initially focuses on clearing heat and detoxifying, promoting blood circulation and unblocking meridians,64 and later emphasizes tonifying qi, invigorating blood, protecting meridians, and relieving pain.65 Clinical studies66,67 confirm that acupuncture significantly alleviates PHN and related sleep disturbances. Traditional Chinese medicine explains this effect through stimulating acupoints to unblock meridians, harmonize qi and blood, warm and disperse nodules, restore qi and blood circulation, relieve pain, balance yin and yang, calm the spirit, and stabilize the mind—thereby improving sleep and reducing anxiety.62,68
Modern research confirms that acupuncture exhibits clear efficacy in improving sleep duration, enhancing sleep quality, and promoting mental health.69 Although the mechanisms underlying acupuncture’s improvement of PHN-related sleep disorders remain incompletely understood, current theories primarily focus on three aspects: (1) Modulation of neuropathic pain pathways: Acupuncture reduces expression of ion channels and receptors such as TRPV1 and P2X3,70 inhibits activation of microglia and astrocytes,71,72 decreases release of proinflammatory cytokines TNF-α and IL-1β,73 and elevates levels of 5-HT and NE in the spinal cord and brain. This activates central descending pain inhibitory pathways,74 alleviating pain signals that disrupt sleep. (2) Regulation of sleep-related neurotransmitters and cytokines: Restores the sleep-wake cycle by modulating 5-HT, NE, dopamine, GABA, glutamate, as well as IL-1, IL-6, TNF-α, and nitric oxide,74,75 exerting sedative and hypnotic effects. (3) Modulating autonomic nervous system and hypothalamic function: Acupuncture can suppress excessive sympathetic nervous system excitation, enhance parasympathetic activity, and downregulate the hypothalamic-pituitary-adrenal (HPA) axis stress response.76,77 This alleviates pain-related hyperarousal states and promotes both the initiation and maintenance of sleep. In summary, acupuncture improves sleep quality in PHN patients through multi-system, multi-target synergistic regulation.
Due to significant heterogeneity, we conducted subgroup analyses based on acupuncture technique and intervention duration. Sleep-related outcomes indicated that all acupuncture techniques positively influenced the alleviation of PHN-related sleep disturbances. Analysis of effect size trends suggested that the combined effect size was highest in the acupotomy subgroup, followed by the fire needling subgroup, and the combined effect of plum-blossom needling and wrist-ankle acupuncture was relatively smaller. Though subgroup variations did not reach statistical significance, these findings suggest potential differences among acupuncture treatments in improving sleep quality for PHN patients, indicating that acupotomy and fire needling may exhibit relatively superior clinical potential. However, this inference is based on indirect comparisons; it cannot be equated with evidence from direct efficacy trials. In addition, in the forest plot, some subgroups include only a single study, representing estimates from that single study rather than a pooled effect size. Acupotomy therapy occupies a middle ground between acupuncture and minimally invasive surgery. The instrument resembles a needle but features a micro-blade at its tip. After percutaneous insertion into subcutaneous tissues, fascia, ligaments, and other soft tissues, it releases scar adhesions and corrects soft tissue tension imbalances to relieve pain and restore function.78 Its improvement of PHN-related sleep disruption primarily occurs indirectly through analgesia: By releasing adhesions, reducing mechanical compression on cutaneous nerves and nerve roots, and elevating local pain thresholds, it provides sustained relief from neuropathic pain.78 Fire needling involves rapidly inserting a needle heated to red-hot into acupoints or diseased areas, combining mechanical and thermal stimulation.79 Animal studies indicate that fire needling can indirectly alleviate nocturnal pain-related awakenings and sleep onset difficulties in patients by suppressing spinal astrocyte activation, modulating inflammatory cytokines, reducing neuronal apoptosis, and promoting nerve repair. This approach enhances sleep quality in PHN patients through analgesic, anti-inflammatory, and neuro-regenerative effects.80
Classified by intervention duration, all treatment groups showed that acupuncture improved sleep quality in PHN patients. However, differences between subgroups did not reach statistical significance, and effect sizes across treatment groups did not exhibit a trend of increasing with treatment duration. This evidence is insufficient to support the claim that extending treatment duration yields linear cumulative or dose-dependent benefits. Although the 21-day group exhibited the largest effect size, its confidence interval was wide, and intra-group heterogeneity was high. The results may also be influenced by sample size, which can limit their stability. This mechanism may be related to the persistent “after-effects” of acupuncture. Improvements were maintained for several weeks after treatment completion, while long-term continuous stimulation may lead to “fatigue” of acupoint stimulation, resulting in diminishing marginal effects.81 A similar trend was observed in clinical effectiveness outcomes: effect sizes fluctuated between days 12 and 21, without showing a monotonically increasing pattern. After 28 days, the effect size stabilized around 1.20 and did not increase further at 36 or 42 days, suggesting that therapeutic efficacy may plateau around 4 weeks. Overall, no clear time-dependent enhancement trend was observed.
This study suffers from significant heterogeneity across multiple aspects. Clinically, variations in acupuncture techniques—such as point combinations, Qi-obtaining levels, manipulation methods, and stimulation intensity—along with operator experience and physician-patient interactions, may contribute to potential sources of heterogeneity. Similarly, differences in control measures, including drug dosages and combination therapies, represent additional sources of variability. On the methodological front, some studies featured small sample sizes (<30 cases per group), and most failed to clearly describe the implementation process of blinding, potentially leading to performance bias and detection biases. Additionally, inadequate reporting of dropouts may introduce non-response bias and overestimate treatment efficacy. Sleep outcomes relied predominantly on subjective measures, such as the PSQI, and lacked objective polysomnography data. Subjective assessments are susceptible to the expectancy effect, which may further increase variability in results.
This study analyzed secondary outcomes. Subgroup analysis by intervention type for pain scores revealed that the acupotomy subgroup exhibited the largest combined effect size, followed by the electroacupuncture subgroup, consistent with the effect size trends observed in sleep-related outcomes. Both acupotomy and electroacupuncture demonstrate clinical potential for the management of PHN pain. This efficacy may stem from electroacupuncture’s use of pulsed currents at specific frequencies and intensities to stimulate acupoints, enabling more stable, quantifiable stimulation that covers a broader tissue area.82 Electroacupuncture activates multiple bioactive substances through peripheral, spinal, and supraspinal mechanisms to block persistent neuropathic pain.83 Acupuncture-related therapies also significantly improved anxiety, depression, and quality of life in PHN patients. Although outcomes showed high heterogeneity (I2 > 90%), the effect direction was consistent, indicating that acupuncture has a stable positive impact on patients’ psychological state and quality of life. Sleep is closely and bidirectionally linked to anxiety, depression, and quality of life: negative emotions disrupt sleep through worry, rumination, and feelings of hopelessness, while poor sleep exacerbates emotional distress and diminishes quality of life, creating a cross-diagnostic vicious cycle.84,85
The adverse events reported in the study were primarily mild to moderate and reversible symptoms, and no serious adverse events were observed, indicating the good safety of the acupuncture intervention. Common adverse reactions in the intervention group included dizziness or vertigo, somnolence, nausea or vomiting, and pruritus, with one additional report of needle phobia. The control group predominantly experienced somnolence, dizziness or vertigo, nausea or vomiting, and xerostomia. Combined analysis showed a downward trend in the risk of adverse events with acupuncture, though it did not reach statistical significance. Regarding effect direction, acupuncture showed no clear signal of increased risk, and its safety remains clinically acceptable.
This study offers the following advantages: We focus on the improvement of sleep quality in PHN patients through acupuncture-related therapies, addressing the shortcomings of previous research that predominantly examined pain or general symptoms while neglecting sleep as a critical outcome measure. Limitations include: (1) Limited research on certain acupuncture techniques, such as wrist-ankle acupuncture and plum-blossom needling therapy, which have small sample sizes; their efficacy requires further validation through high-quality studies. (2) High heterogeneity in pooled results; despite subgroup analyses and meta-regression based on intervention type, treatment duration, age, disease duration, and gender, the sources of heterogeneity remain incompletely explained. In addition, the included trials all reported generally favorable results, while there is a lack of published negative or inconclusive studies, suggesting that the results may be overestimated. Future clinical studies require greater standardization and more detailed reporting to identify influencing factors better. (3) All included studies originated from China, leading to a certain degree of regional bias. (4) Most studies did not employ blinding methods such as sham acupuncture and failed to clearly report specific implementation details of blinding, making it difficult to rule out the influence of participant and evaluator expectations on outcomes. Only one study used a sham acupuncture control, and only one was a multi-center study. (5) When analyzing multi-arm randomized controlled trials (eg., Yan 2024), we included each intervention group as a separate comparison in the analysis to examine the efficacy of different acupuncture techniques individually. This approach facilitates detailed subgroup analysis but also results in the duplicate counting of samples within the same control group. Such duplication may artificially inflate statistical power to some extent and alter the confidence intervals of the pooled effect size. (6) Differences in the diagnostic criteria and duration of PHN across the original studies may introduce heterogeneity. Some studies did not report the diagnostic guidelines used, and several studies lacked a clear definition of the duration of PHN. This issue may affect the comparability of the baseline characteristics of the study populations.
Conclusion
In summary, the current evidence suggests that acupuncture and related therapies may offer potential clinical benefits for improving sleep disturbances in patients with PHN. However, given limitations such as the high heterogeneity of the included studies and potential publication bias, the current findings should be interpreted with caution. Different acupuncture modalities and treatment durations may influence efficacy assessments. Future research necessitates adequately powered, rigorously designed randomized controlled trials with detailed reporting of intervention specifics and population characteristics to further validate efficacy and elevate the quality of evidence.
Data Sharing Statement
All data generated or analysed during this study are included in this published article and its Supplementary Information Files.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was not supported by any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Treede RD, Rief W, Barke A. et al. Chronic pain as a symptom or a disease: the IASP Classification of Chronic Pain for the International Classification of Diseases (ICD-11). Pain. 2019;160(1):19–23. doi:10.1097/j.pain.0000000000001384
2. Dai J, Liu B, Xue K, et al. Chinese Guidelines for the Comprehensive Management of Herpes Zoster-associated Pain (2025 Edition). Chinese Journal of Pain Medicine. 2025;31(8):561–571.
3. Koshy E, Mengting L, Kumar H, Jianbo W. Epidemiology, treatment and prevention of herpes zoster: a comprehensive review. Indian J Dermatol Venereol Leprol. 2018;84(3):251–262. doi:10.4103/ijdvl.IJDVL_1021_16
4. Zhang Z, Liu X, Suo L, Zhao D, Pan J, Lu L. The incidence of herpes zoster in China: a meta-analysis and evidence quality assessment. Hum Vaccin Immunother. 2023;19(2):2228169. doi:10.1080/21645515.2023.2228169
5. Liao X, Xu S, Wang Y, Zheng B. Epidemiology and risk factors of postherpetic neuralgia worldwide: protocol for a systematic review and meta-analysis. BMJ Open. 2026;16(1):e104637. doi:10.1136/bmjopen-2025-104637
6. Chen LK, Arai H, Chen LY, et al. Looking back to move forward: a twenty-year audit of herpes zoster in Asia-Pacific. BMC Infect Dis. 2017;17(1):213. doi:10.1186/s12879-017-2198-y
7. Thompson RR, Kong CL, Porco TC, Kim E, Ebert CD, Acharya NR. Herpes Zoster and Postherpetic Neuralgia: changing Incidence Rates From 1994 to 2018 in the United States. Clin Infect Dis. 2021;73(9):e3210–e3217. doi:10.1093/cid/ciaa1185
8. MacIntyre R, Stein A, Harrison C, Britt H, Mahimbo A, Cunningham A. Increasing trends of herpes zoster in Australia. PLoS One. 2015;10(4):e0125025. doi:10.1371/journal.pone.0125025
9. Lee DH, Park JE, Yoon DM, Yoon KB, Kim K, Kim SH. Factors Associated with Increased Risk for Clinical Insomnia in Patients with Postherpetic Neuralgia: a Retrospective Cross-Sectional Study. Pain Med. 2016;17(10):1917–1922. doi:10.1093/pm/pnw066
10. Takai H, Nozaki-Taguchi N, Shono K, Sato Y, Isono S. Relationship Between Patient-reported Outcome Measures and Accelerometer-measured Physical Activity and Sleep in Patients With Postherpetic Neuralgia. Clin J Pain. 2024;40(9):520–525. doi:10.1097/ajp.0000000000001233
11. Shi Y, Song C. Effectiveness and Safety of Gabapentin versus Pregabalin in the Treatment of Postherpetic Neuralgia: a Retrospective Cohort Study. Br J Hosp Med (Lond). 2024;85(12):1–11. doi:10.12968/hmed.2024.0485
12. Wang H, Zhang D, Wang S, Wang H, Nie H. Comparison of the efficacy of pulsed radiofrequency in treating acute herpetic neuralgia and postherpetic neuralgia in the thoracic segment. Front Neurol. 2024;15:1425796. doi:10.3389/fneur.2024.1425796
13. Liu J, Zhang A, Ye X, X H, He R, Jiang Z. The effect of short-term spinal cord electrical stimulation on patients with postherpetic neuralgia and its effect on sleep quality. Neuro Endocrinol Lett. 2021;42(2):81–86.
14. Wen B, Wang Y, Zhang C, Xu W, Fu Z. Efficacy of different interventions for the treatment of postherpetic neuralgia: a Bayesian network meta-analysis. J Int Med Res. 2020;48(12):300060520977416. doi:10.1177/0300060520977416
15. Nalamachu S, Morley-Forster P. Diagnosing and managing postherpetic neuralgia. Drugs Aging. 2012;29(11):863–869. doi:10.1007/s40266-012-0014-3
16. Ki YM, Park HJ, Yi SH, Sim WS, Lee JY. Latent infection after spinal cord stimulation device implantation for complex regional pain syndrome: a case report. Medicine (Baltimore). 2023;102(19):e33750. doi:10.1097/md.0000000000033750
17. Liang X, Chen X, Li X, et al. Efficacy and safety of therapies related to acupuncture for acute herpes zoster: a PRISMA systematic review and network meta-analysis. Medicine (Baltimore). 2024;103(20):e38006. doi:10.1097/md.0000000000038006
18. Jiang J, Ji B, Jin W, et al. Clinical Efficacy and Therapeutic Mechanism of Acupuncture in the Treatment of Adolescent Depression. J Integr Neurosci. 2025;24(9):38071. doi:10.31083/jin38071
19. Xie C, Wang J, Zhao N, et al. Effects of Electroacupuncture on Sleep via the Dopamine System of the HPA Axis in Rats after Cage Change. Evid Based Complement Alternat Med. 2021;2021:5527060. doi:10.1155/2021/5527060
20. Zifeng Z, Choying WO, Hongling C, et al. Acupuncture inhibits astrocytic hyperactivationthe p38 mitogen-activated protein kinase/mitogen- and stress-activated protein kinase 1 signaling pathway in cerebral ischemia-reperfusion injury. J Tradit Chin Med. 2026;46(2):316–325. doi:10.19852/j.cnki.jtcm.2026.02.005
21. Akita T, Kurono Y, Yamada A, Hayano J, Minagawa M. Effects of Acupuncture on Autonomic Nervous Functions During Sleep: comparison with Nonacupuncture Site Stimulation Using a Crossover Design. J Integr Complement Med. 2022;28(10):791–798. doi:10.1089/jicm.2022.0526
22. Xu W, Zhang ZY, Sun D, et al. Effects of mind-regulating acupuncture on pain,negative emotion and sleep quality in patients with postherpetic neuralgia:a randomized controlled pilot trial. Acupuncture Research. 2024;49(5):499–505. doi:10.13702/j.1000-0607.20230195
23. Sun R, Li S, Ren L, et al. Efficacy of Electroacupuncture for the Treatment of Postherpetic Neuralgia: study Protocol for a Multicenter Randomized Controlled Trial. J Pain Res. 2022;15:959–968. doi:10.2147/jpr.S357435
24. Chen Q. Study on the Effects of Fire Needle Therapy on Postherpetic Neuralgia Patients and Its Impacts on Sleep Quality. World Journal of Sleep Medicine. 2025;12(2):358–360.
25. Zhou L, Teng J, Li J. Effect of plum-blossom needle tapping and cupping combined with ultra-short wave and hyperbaric oxygen therapy on pain and sleep quality in patients with herpes zoster. China Modern Medicine. 2025;32(3):43–46.
26. Wang Y, Li W, Peng W, Zhou J, Liu Z. Acupuncture for postherpetic neuralgia: systematic review and meta-analysis. Medicine (Baltimore). 2018;97(34):e11986. doi:10.1097/md.0000000000011986
27. Yu J, Tu M, Shi Y, et al. Acupuncture therapy for treating postherpetic neuralgia: a protocol for an overview of systematic reviews and meta-analysis. Medicine (Baltimore). 2020;99(47):e23283. doi:10.1097/md.0000000000023283
28. Zhou Q, Wei S, Zhu H, et al. Acupuncture and moxibustion combined with cupping for the treatment of post-herpetic neuralgia: a meta-analysis. Medicine (Baltimore). 2021;100(31):e26785. doi:10.1097/md.0000000000026785
29. Cui Y, Zhou X, Li Q, et al. Efficacy of different acupuncture therapies on postherpetic neuralgia: a Bayesian network meta-analysis. Front Neurosci. 2022;16:1056102. doi:10.3389/fnins.2022.1056102
30. Tang J, Zhang Y, Liu C, Zeng A, Song L. Therapeutic Strategies for Postherpetic Neuralgia: mechanisms, Treatments, and Perspectives. Curr Pain Headache Rep. 2023;27(9):307–319. doi:10.1007/s11916-023-01146-x
31. Wang J, Li D, Li Y, Luo X, Deng L, Pu J. Research progress on wrist-ankle acupuncture in treatment of postherpetic neuralgia. Journal of Snake. 2025;37(4):514–517.
32. Yu S, Wan Y, Wan Q, et al. Chinese Expert Consensus on the Diagnosis and Treatment of Postherpetic Neuralgia. Chinese Journal of Pain Medicine. 2016;22(03):161–167.
33. Johnson RW, Rice AS. Clinical practice. Postherpetic neuralgia. N Engl J Med. 2014;371(16):1526–1533. doi:10.1056/NEJMcp1403062
34. Fabbri M, Beracci A, Martoni M, Meneo D, Tonetti L, Natale V. Measuring Subjective Sleep Quality: a Review. Int J Environ Res Public Health. 2021;18(3):82. doi:10.3390/ijerph18031082
35. Sterne JAC, Savović J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898. doi:10.1136/bmj.l4898
36. Luo D, Wan X, Liu J, Tong T. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat Methods Med Res. 2018;27(6):1785–1805. doi:10.1177/0962280216669183
37. Wan X, Wang W, Liu J, Tong T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol. 2014;14(1):135. doi:10.1186/1471-2288-14-135
38. Wang X, Cheng S, Ma Y, et al. Efficacy of arc-edge needle with oral analgesic medicine treatment for patients with thoracodorsal postherpetic neuralgia. Chin J Painol. 2019;15(2):102–108.
39. Chen Y, Wang L, Zhou X, Chen X. Clinical Effect of Fire Acupuncture Combined with Conventional Drugs in Treatment of Postherpetic Neuralgia. Chinese Community Doctors. 2023;39(6):78–80.
40. Yan D, Pu T, Li W, Wei H, He S, Zhang Z. Observation on the clinical effect of treating postherpetic neuralgia with fire needle acupuncture. China Practical Medical. 2024;19(23):146–148.
41. Zhao H, Shen F, Zheng Q, et al. Clinical observation on the treatment of postherpetic neuralgia by neuromodulation electro-acupuncture. World Clinical Drugs. 2021;42(11):978–982,999.
42. Huang D, Zhang J. Effects of plum blossom needle tapping combined with Pregabalin in treatment of patients with postherpetic neuralgia. Medical Journal of Chinese People’s Health. 2021;33(22):119–120,123.
43. Zhang C, Guo S, Xie C, Huang J, Ruan Z. Clinical effect of herbal needle combined pregabalin in postherpetic neuralgia. Shaanxi Journal of Traditional Chinese Medicine. 2021;42(3):376–378,382.
44. Sun J, Gao Y, Yu H. The effect of intensive silver needle combined with pregabalin in the treatment of postherpetic neuralgia. Journal of Diagnosis and Therapy on Dermato-Venereology. 2022;29(6):548–552.
45. Tang W, Zhang R, Cheng X, et al. Clinical observation of row needling for postherpetic neuralgia. China’s Naturopathy. 2024;32(11):46–49.
46. Liu S, Zhang Y, Shao X, Shen S, Huang Q. On Treatment of 40 Cases of Postherpetic Neuralgia with Ultramicro Acupotomy at Myofascial Trigger Points. Henan Traditional Chinese Medicine. 2024;44(3):422–426.
47. Lu H. Clinical observation of wrist-ankle acupuncture for postherpetic neuralgia. World Latest Medicine Information. 2020;20(1): 155–156.
48. Liu W, Wei Z, Hu J, et al. Clinical observation on wrist-ankle acupuncture in treatment of postherpetic neuralgia and its influence on inflammatory factors. Chinese Journal of Pain Medicine. 2024;30(10):750–756.
49. Xie Y, Zhao J, Jiang M, et al. Clinical Study of Surround Needling Combined with Gabapentin Treating PHN. Journal of Clinical Acupuncture and Moxibustion. 2018;34(9):20–23.
50. Zhou Q, Ta N, Fu G, Zhang Y, Zhao W. Clinical effect and mechanism of yizhen therapy on post-herpetic neuralgia. Acupuncture Research. 2026; 51 (2):225–232. doi:10.13702/j.1000-0607.20241305
51. Wang X, Zhang B, Yu T. Effects of Acupuncture and Gabapentine Capsules on the Levels of Serum SP and NPY in Patients with Postherpetic Neuralgia. Western Journal of Traditional Chinese Medicine. 2021;34(8):133–135.
52. Ou C. The Effect of Acupuncture Combined with Pregabalin on Pain in Patients with Postherpetic Neuralgia. Journal of China Prescription Drug. 2023;21(10):129–132.
53. Lu C. Clinical observation on the treatment of postherpetic neuralgia with the hair-thin needle pricking method. Journal of Practical Traditional Chinese Medicine. 2023;39(6):1173–1175.
54. Tong F. Clinical Study on Filiform-Fire Needle Combined with Pregabalin for Postherpetic Neuralgia with Qi Stagnation and Blood Stasis Syndrome. Journal of New Chinese Medicine. 2023;55(14):141–145.
55. Gong Y, Peng Y. Effect of filiform fire needling on pain relief and quality of life improvement in patients with postherpetic neuralgia. Rehabilitation. 2024;(29):128–131. doi:10.3969/j.issn.1005-832X.2024.29.037
56. Zhang Y, Meng X, Zhang M, Guo H. Observation of the therapeutic effect of qi-regulating acupuncture combined with gabapentin in the treatment of postherpetic neuralgia and its effect on serumb β-EP and NK-1 levels. Shanghai Journal of Acupuncture and Moxibustion. 2024;43(3):301–306.
57. Hu X, Ye X. The effect of electroacupuncture combined with pregabalin on pain and sleep quality in patients with postherpetic neuralgia pain. The Medical Forum. 2025;29(23):73–75. doi:10.19435/j.1672-1721.2025.23.021
58. Zhao H, Yu X. The efficacy of ultramicro needle knife combined with gabapentin in the treatment of PHN. Journal of Heze Medical College. 2021;33(4):30–31,42.
59. Yang Y, Xu W, Li M, Zhou Y, Qian Y. Collateral-Pricking and Bloodletting Cupping Combined with Electroacupuncture for Postherpetic Neuralgia: a Meta-Analysis. Altern Ther Health Med. 2024;30(11):290–296.
60. Jiang X, Yan Y, Chen Z, et al. The basolateral amygdala-anterior cingulate cortex circuit contributes to postherpetic neuralgia-anxiety comorbidity. Theranostics. 2025;15(10):4614–4637. doi:10.7150/thno.111130
61. Chao Y. General Treatise on the Causes and Symptoms of Diseases. Liaoning Science and Technology Publishing House; 1997.
62. Liu S, Wang L. Research Progress on the Combined Use of Hao Fire Needle Retention and Acupuncture in the Treatment of Postherpetic Neuralgia. Traditional Chinese Medicine. 2025;14(11):5121–5126. doi:10.12677/tcm.2025.1411737
63. Lu Y, Xiao H, Chen R, Zhu Z, Gui M, Zhang W. Clinical study on acupuncture at Jiaji points combined with bloodletting cupping for postherpetic neuralgia in elderly patients. Hubei Journal of Traditional Chinese Medicine. 2019;41(12):49–51.
64. Li Y, Wang J, Sun Z, Zhang F, Cao T. Discussion on Traditional Chinese Medicine Treatment of Postherpetic Neuralgia from “Collaterals”. Journal of Traditional Chinese Medicine. 2019;60(08):653–655.
65. Xue C, Xie L, Li X, et al. Experience in treating postherpetic neuralgia with collateral theory. Shanghai Journal of Traditional Chinese Medicine. 2023;57(7):30–33.
66. Zhou X, Liu X. Application of Acupuncture Therapy Combined with Traditional Chinese Medicine Nursing for Patients with Postherpetic Neuralgia. Chinese Journal of Integrative Nursing. 2022;8(11):131–136.
67. Jin Y. Clinical Observation of Acupuncture for Thoracic Herpes Zoster Based on Meridian Sinew Theory. Liaoning University of Traditional Chinese Medicine. 2024. doi:10.27213/d.cnki.glnzc.2024.000536
68. Li Q, Zhang S. Clinical research progress on acupuncture for postherpetic neuralgia. Longevity Guide. 2021;(26):16–18.
69. Yin X, Li W, Liang T, et al. Effect of Electroacupuncture on Insomnia in Patients With Depression: a Randomized Clinical Trial. JAMA Netw Open. 2022;5(7):e2220563. doi:10.1001/jamanetworkopen.2022.20563
70. Zhang Q, Zhou M, Huo M, et al. Mechanisms of acupuncture-electroacupuncture on inflammatory pain. Mol Pain. 2023;19:17448069231202882. doi:10.1177/17448069231202882
71. Ji RR, Chamessian A, Zhang YQ. Pain regulation by non-neuronal cells and inflammation. Science. 2016;354(6312):572–577. doi:10.1126/science.aaf8924
72. Liang Y, Qiu Y, Du J, et al. Inhibition of spinal microglia and astrocytes contributes to the anti-allodynic effect of electroacupuncture in neuropathic pain induced by spinal nerve ligation. Acupunct Med. 2016;34(1):40–47. doi:10.1136/acupmed-2015-010773
73. Li Y, Fang Z, Gu N, et al. Inhibition of chemokine CX3CL1 in spinal cord mediates the electroacupuncture-induced suppression of inflammatory pain. J Pain Res. 2019;12:2663–2672. doi:10.2147/jpr.S205987
74. Ma X, Chen W, Yang NN, et al. Potential mechanisms of acupuncture for neuropathic pain based on somatosensory system. Front Neurosci. 2022;16:940343. doi:10.3389/fnins.2022.940343
75. Liu F, You J, Li Q, et al. Acupuncture for Chronic Pain-Related Insomnia: a Systematic Review and Meta-Analysis. Evid Based Complement Alternat Med. 2019;2019:5381028. doi:10.1155/2019/5381028
76. Lin JG, Kotha P, Chen YH. Understandings of acupuncture application and mechanisms. Am J Transl Res. 2022;14(3):1469–1481.
77. Zheng JY, Zhu J, Wang Y, Tian ZZ. Effects of acupuncture on hypothalamic-pituitary-adrenal axis: current status and future perspectives. J Integr Med. 2024;22(4):445–458. doi:10.1016/j.joim.2024.06.004
78. Zhao Y, Fang W, Qin WK. Thinking of therapeutic mechanism of small knife needle in treating closed myofascitis. Chinese Acupuncture & Moxibustion. 2014;34(9):907–909.
79. Lu L, Xiong J, Chen Z, et al. Efficacy and safety of fire needle vs conventional acupuncture in the treatment of postherpetic neuralgia: a protocol for systematic review and meta analysis. Medicine (Baltimore). 2020;99(41):e22563. doi:10.1097/md.0000000000022563
80. Ding Y, Cao H, Huang Y, et al. Fire Acupuncture Combined with Pulse Radiofrequency Relieves Tactile Allodynia in Rats with Postherpetic Neuralgia. Int J Gen Med. 2025;18:5699–5716. doi:10.2147/ijgm.S541807
81. Zhang X, Wang Y, Liu C, et al. The dose-effect relationship between acupuncture and its effect on primary insomnia: a systematic review and meta-analysis. Front Psychiatry. 2025;16:1501321. doi:10.3389/fpsyt.2025.1501321
82. Hahm TS. Electroacupuncture. Korean J Anesthesiol. 2009;57(1):3–7. doi:10.4097/kjae.2009.57.1.3
83. Zhang R, Lao L, Ren K, Berman BM. Mechanisms of acupuncture-electroacupuncture on persistent pain. Anesthesiology. 2014;120(2):482–503. doi:10.1097/aln.0000000000000101
84. Lee M, Choh AC, Demerath EW, et al. Sleep disturbance in relation to health-related quality of life in adults: the Fels Longitudinal Study. J Nutr Health Aging. 2009;13(6):576–583. doi:10.1007/s12603-009-0110-1
85. Nguyen VV, Zainal NH, Newman MG. Why Sleep is Key: poor Sleep Quality is a Mechanism for the Bidirectional Relationship between Major Depressive Disorder and Generalized Anxiety Disorder Across 18 Years. J Anxiety Disord. 2022;90:102601. doi:10.1016/j.janxdis.2022.102601
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Efficacy and Safety of Acupuncture for Tinnitus-Associated Insomnia: A Protocol for a Systematic Review and Meta-Analysis
Fan L, Gao Y, Zhou J, Hu H, Gao H
Journal of Pain Research 2022, 15:2957-2965
Published Date: 21 September 2022
A Systematic Review and Meta-Analysis Protocol on How Best to Use Non-Pharmacologic Therapies to Manage Chronic Low Back Pain and Associated Depression
Guo Y, Ma Q, Zhou X, Yang J, He K, Shen L, Zhao C, Chen Z, Tan CIC, Chen J
Journal of Pain Research 2022, 15:3509-3521
Published Date: 4 November 2022
Tezepelumab for Patients with Severe Uncontrolled Asthma: A Systematic Review and Meta-Analysis
Zoumot Z, Al Busaidi N, Tashkandi W, Aljohaney AA, Isse S, Vidyasagar K, Ukwaja KN
Journal of Asthma and Allergy 2022, 15:1665-1679
Published Date: 18 November 2022
Different Intensities of Evening Exercise on Sleep in Healthy Adults: A Systematic Review and Network Meta-Analysis
Yue T, Liu X, Gao Q, Wang Y
Nature and Science of Sleep 2022, 14:2157-2177
Published Date: 14 December 2022
Comparison of Balanced Crystalloids versus Normal Saline in Critically Ill Patients: A Systematic Review with Meta-Analysis and Trial Sequential Analysis of Randomized Controlled Trials
Chen Y, Gao Y
Therapeutics and Clinical Risk Management 2023, 19:783-799
Published Date: 11 October 2023