")
Back to Journals » Journal of Pain Research » Volume 15
The Efficacy and Safety of Acupuncture for Tinnitus-Associated Insomnia: A Protocol for a Systematic Review and Meta-Analysis
Authors Fan L , Gao Y, Zhou J, Hu H , Gao H
Received 2 August 2022
Accepted for publication 7 September 2022
Published 21 September 2022 Volume 2022:15 Pages 2957—2965
DOI https://doi.org/10.2147/JPR.S383968
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
Lijuan Fan,1,* Yiqi Gao,2,* Jie Zhou,3 Hantong Hu,3 Hong Gao3
1The Third Clinical College, Zhejiang Chinese Medical University, Hangzhou City, People’s Republic of China; 2Department of Traditional Therapy Centre, The Third Affiliated Hospital of Zhejiang Chinese Medical University, Hangzhou City, People’s Republic of China; 3Department of Acupuncture and Moxibustion, The Third Affiliated Hospital of Zhejiang Chinese Medical University, Hangzhou City, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hantong Hu; Hong Gao, Department of Acupuncture and Moxibustion, The Third Affiliated Hospital of Zhejiang Chinese Medical University, No. 219 Moganshan Road, Xihu District, Hangzhou City, People’s Republic of China, Email [email protected]; [email protected]
Background: Tinnitus accounts for a significant proportion of the factors that cause insomnia, and insomnia, in turn, aggravates tinnitus. Given that tinnitus and insomnia have a bidirectional relationship, tinnitus-associated insomnia is prevalent. Nonetheless, current treatments including medication and psychological therapies for tinnitus-associated insomnia do not yield satisfactory efficacy, thereby making it challenging to manage. Although acupuncture is a potentially effective treatment option, the current evidence on the efficacy and safety of acupuncture for tinnitus-associated insomnia remains inconclusive. Therefore, this systematic review and analysis protocol aims to investigate whether acupuncture is beneficial for tinnitus-associated insomnia with an acceptable safety profile.
Methods: Nine mainstream English-language and Chinese-language databases will be searched to include qualified RCTs and meta-analyses will be conducted by combining extracted data using RevMan 5.3. The risk of bias 2.0 tool recommended by Cochrane will be adopted to evaluate the methodological quality of the included RCTs. The Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) approach will be utilized to appraise the strength and certainty of evidence. Where available, we will also perform sensitivity analyses, publication bias and subgroup analysis.
Discussion: Expected results from our systematic review and meta-analysis will verify the efficacy and safety of acupuncture in tinnitus-associated insomnia. The evidence generated by this review will help patients and clinicians make informed treatment decisions.
Keywords: systematic review, meta-analysis, acupuncture, tinnitus, insomnia
Introduction
Rationale
Insomnia is characterized by impairment of the ability to initiate, maintain, or obtain quality sleep. Among the adult population, there is an annual prevalence of between 35 and 50% of insomnia symptoms and 12–20% of insomnia disorders.1 One of the common causes of insomnia is tinnitus, which describes the perception of hearing noise without a corresponding external stimulus. The proportion of tinnitus patients who seek help for sleep disorders is fairly high, and is reported to range from 50% to 77%.2–6 Insomnia associated with tinnitus can impair patients’ concentration and result in mood disorders such as anger and frustration,7–9 which lead to poor quality of life.
The close relationship between tinnitus and insomnia has been explored for decades.6 However, the mechanisms and modifying factors that lead to insomnia in tinnitus patients remain inconclusive.6 Wallhäusser-Franke et al hypothesized that tinnitus and sleep disturbances may share similar physiological mechanisms, which involve increased sympathetic nervous system activation-induced hyper-arousal.10 Other scholars concluded that insomnia and tinnitus are maintained by dysfunctional beliefs and negative emotion.11,12 And what seems to be well recognized, is that the two react to each other.12,13 A large amount of tinnitus patients with insomnia tend to blame their sleep problems on tinnitus noise, despite the lack of convincing evidence of a direct connection. Severe sleep disturbances are often accompanied by an increase in the loudness of tinnitus, which in turn leads to worse sleep quality.10,13
Currently, tinnitus-associated insomnia is mainly treated with sedative-hypnotic medication. In recent years, with the emphasis being placed on the use of psychotherapy for treating tinnitus-associated insomnia, cognitive behavioral therapy (CBT) has also started to gain popularity. Other alternative therapies are also emerging, such as bee-humming respiratory training.14 Nonetheless, not all patients respond to medication and adverse drug reactions such as nausea, sleepiness and excessive fatigue can limit the use of pharmacotherapy. In addition, although psychological therapies like CBT are useful, they remain difficult to popularize allover the world due to the limitation of high cost and the difficulty of finding skilled psychotherapists in some areas. As a result, complementary and alternative medicine (CAM) are likely to provide optional treatment approaches for patients with tinnitus-associated insomnia.
Acupuncture therapy is an important element of CAM. Various types of acupuncture, such as auricular acupuncture (AA), electroacupuncture (EA), manual acupuncture (MA), have been widely used for treating both tinnitus15 and insomnia in clinical trials and scientific research. There are also multiple related systematic reviews and meta-analyses. However, all of them16–19 merely focus on the effect of acupuncture on insomnia, irrespective of tinnitus-associated insomnia. And the bulk of these published systematic reviews and meta-analyses20–22 simply concentrate on the effect of acupuncture on tinnitus, irrespective of its frequent comorbid conditions like insomnia. However, owing to the fact that tinnitus and insomnia have a bidirectional correlation and tinnitus-associated insomnia is fairly common in clinical settings, it is important to clarify whether acupuncture is beneficial and safe for tinnitus-associated insomnia. Nonetheless, the overwhelming majority of published studies just concentrate on the effect of acupuncture on either tinnitus or insomnia. To date, the investigation of acupuncture for treating tinnitus-associated insomnia has been rather inadequate, thereby resulting in a lack of definite evidence. As far as we are concerned, no prior studies have attempted the well-regarded approach of conducting a systematic review and meta-analysis to determine the efficacy and safety of acupuncture for tinnitus-associated insomnia. Therefore, we report this protocol for a systematic review and meta-analysis that focuses on this important clinical question.
The feasibility of conducting our study is elucidated as follows. First, insomnia-related outcomes are major components of the reported outcomes in trials involving acupuncture for tinnitus.23–25 In addition, tinnitus-associated insomnia is very common in clinical practice, so it is likely to include sufficient quantity of qualified trials for conducting a systematic review and meta-analysis that targets the evidence synthesis of acupuncture in tinnitus-associated insomnia. Second, there are some relevant published RCTs5 or systematic reviews/meta-analyses26,27 that focus on the effect of a specified therapy in insomnia associated with other diseases (eg, tinnitus, depression), so we can refer to such studies to guide the methodology and implementation procedures (eg, eligibility criteria for the included trials, outcome measures of interest) for our present study protocol.
Taken together, it is significant and feasible to conduct our present systematic review and meta-analysis protocol that aims to clarify whether acupuncture is beneficial for treating tinnitus-associated insomnia with an acceptable safety profile.
Objective
The objective of this systematic review and meta-analysis protocol is to evaluate the evidence of the efficacy and safety of acupuncture in tinnitus-associated insomnia.
Methods
We referred to the universally validated checklist of the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P, as shown in Supplementary Table 1)28 while developing this systematic review and meta-analysis protocol. Additionally, in order to increase research openness, we also registered our protocol with the registration number CRD42022349718 in the International Prospective Register of Systematic Reviews (PROSPERO).
Eligibility Criteria
The widely accepted PICOS components for conducting a systematic review and meta-analysis will be used to determine the trials’ eligibility, which are displayed in detail as follows.
Study Designs
Regardless of publication language, the eligible study type for our systematic review and meta-analysis is planned to be restricted to randomized controlled trials (RCTs) that seek to investigate the effectiveness of acupuncture therapy for tinnitus-associated insomnia. Notably, if the main purpose of the original RCT is to evaluate the efficacy of acupuncture in tinnitus but specific insomnia-associated outcome measure is also one component of the main outcomes of the study, such an RCT will also be eligible to be included. Additionally, for crossover RCTs that are enrolled, we will only include the initial results of the two groups prior to crossover in the meta-analysis by referring to similar studies.29 Non-RCTs, case series, reviews, or other ineligible study categories will not be considered in this systematic review and meta-analysis.
Participants
Participants have definitive diagnosis of tinnitus, meanwhile, they have clinically significant insomnia caused by tinnitus, which was evaluated by validated insomnia-related scales (eg, the Insomnia Severity Index (ISI) and Pittsburgh Sleep Quality Index (PSQI)) and/or polysomnography. Standard diagnostic criteria of insomnia will also be referred to, to assist in the confirmation of participants’ eligibility, such as the Diagnostic and Statistical Manual of Mental Disorders (Fourth Edition (DSM-IV),30 or Fifth Edition (DSM-5),31 and the Third version of the International Classification of Sleep Disorders (ICSD-3).32 Participants diagnosed with primary insomnia, organic sleep disorders or insomnia caused by non-tinnitus related diseases will be excluded. No restrictions will be imposed on the age, gender, and nationality of participants.
Interventions in the Experimental Group
The experimental group should use acupuncture therapy. The experimental group may employ acupuncture alone or in conjunction with specific positive treatments that are identical to those used in the control arm. Notably, the acupuncture therapy is prospectively defined as those acupuncture modalities requiring the insertion of acupuncture needles in our study, such as MA, EA, warming-needle moxibustion, and auricular acupuncture. This prospective definition of acupuncture therapy will contribute to decreasing clinical heterogeneity across the included studies. In such a scenario, studies adopting non-penetrating acupuncture techniques (eg, laser acupuncture, acupressure) are not allowed to be included.
Interventions in the Control Group
- Active treatments proposed by guidelines,33–35 such as pharmacological treatment, CBT, music therapy, and sleep hygiene.
- Placebo controls such as sham acupuncture.
- Waiting list control.
- No treatment.
Outcome Measures
We use comparable studies26,27 to identify the outcomes of interest in our protocol. Accordingly, at least one of the following outcome measures must be present in original trials that will be screened for eligibility.
Primary Outcome Measures
Sleep quality evaluated by self-reported scales with proven validity and reliability, such as Insomnia Severity Index (ISI) and Pittsburgh Sleep Quality Index (PSQI), and/or objective sleep variables assessed by sleep detection devices, such as total sleep time, sleep onset latency, and sleep efficiency (ie, the proportion of sleep time relative to the time spent in bed).
Secondary Outcome Measures
- Tinnitus-related scales with proven validity and reliability, such as the Visual Analog Scale VAS), tinnitus Handicap Inventory (THI), Tinnitus Questionnaire (TQ), Tinnitus Functional Index (TFI), and Tinnitus Handicap Questionnaire (THQ).
- Anxiety-related questionnaires with acknowledged soundness, such as Hamilton Anxiety Scale (HAMA).
- Depression-related scales with proven validity and reliability, such as Hamilton Depression Scale (HAMD) and Beck Depression Inventory (BDI).
- Quality of life (QOL) evaluated using questionnaires with acknowledged validity and reliability.
- Adverse events.
Sources for Trial Retrieval
A total of 9 representative databases will be subjected to a systematic search, including 5 databases using English language (PubMed, Web of Science, EMBASE, Cochrane Central Register of Controlled Trials, and Physiotherapy Evidence Database (PEDro)) and 4 databases using Chinese language (Chinese Biomedical Literature Database, Chinese National Knowledge Infrastructure, Wangfang database, and VIP Database for Chinese Technical Periodicals). We will search each database for potentially eligible RCTs from inception to April 2023.
Retrieval Strategies
The retrieval strategies mainly comprise 3 elements: 1) study type (eg, RCT, randomized clinical trial), 2) subjects (eg, tinnitus-associated insomnia, tinnitus-related insomnia, comorbid tinnitus and insomnia), and 3) interventions (eg, auricular acupuncture, electroacupuncture, manual acupuncture, warming-needle moxibustion). All appropriate terms related to these 3 components will be utilized to search the database. In English language databases, individual or combined search terms in English will be utilized. Respective search terms in Chinese will be utilized in Chinese language databases. In order to get the best level of retrieval sensitivity and comprehensiveness, our search strategies will combine both free text terms and subject terms (eg, Medical Subject Headings [MeSH] in PubMed). Table 1 represents the search strategies for PubMed, which can be adapted for the remaining databases by substituting MeSH with relevant subject terms (when available) and keeping the same free text terms.
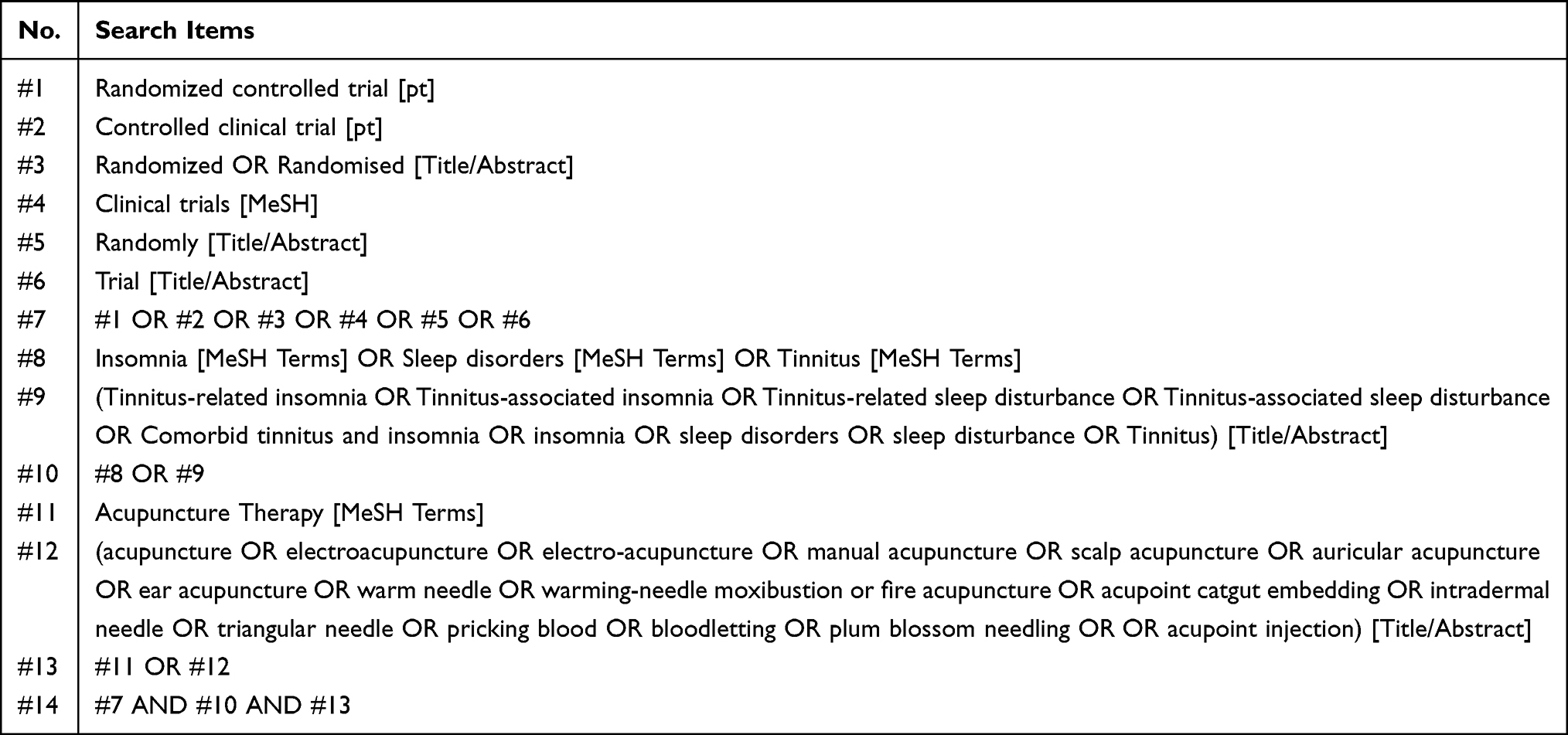 |
Table 1 Search Strategies for PubMed |
To prevent the potential omission of RCTs that are eligible, we will also carefully scan the references of previous related systematic reviews and meta-analyses in this field. In case of future updates of this systematic review, the Clinical Trials Registry (https://clinicaltrials.gov/), the World Health Organization’s International Clinical Trials Registry Platform (https://www.who.int/clinical-trials-registry-platform), and the Chinese Clinical Trial Registry (http://www.chictr.org.cn) will also be searched to find pertinent ongoing trials.
Study Selection Process
To eliminate duplicate retrieval records, the total retrieved records produced by all databases will be exported into EndNote (X9 version, Clarivate, USA) to remove the duplicate studies. In the first step of literature screening, two reviewers (L.F. and H.H.) will read the titles and abstracts of the imported publications independently to identify any possible RCTs that will meet the aforementioned eligibility criteria and exclude apparently irrelevant studies. In the second step of literature screening, the full text of all possible qualifying publications will be read to ultimately validate validity. If there is a dispute about whether to include a specific trial among the reviewers, it will be discussed with the third referee (H.G). Figure 1 summarizes the study selection process.
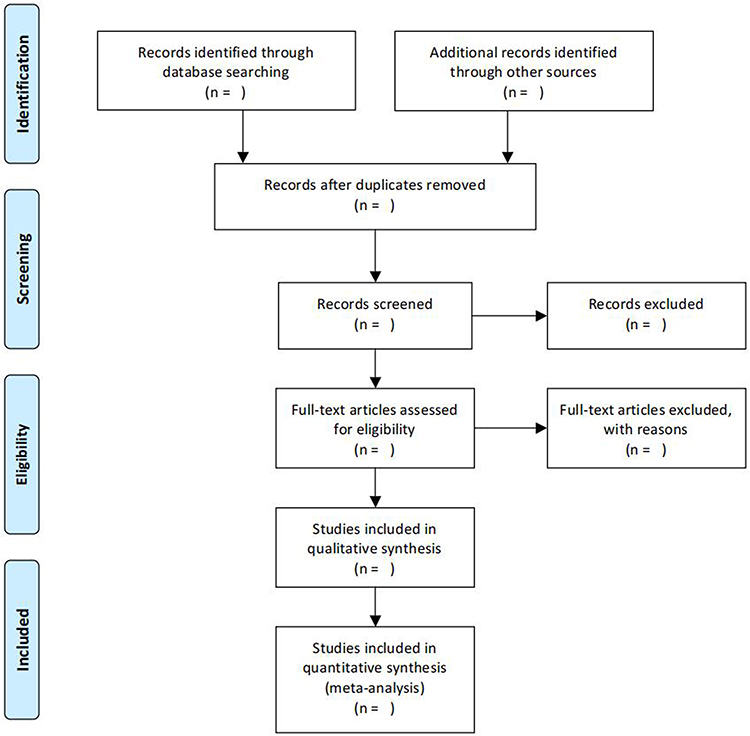 |
Figure 1 Flow diagram of study selection. |
Data Extraction and Data Items
Two impartial reviewers (J.F and Y.G) will use a predefined form (as shown in Supplementary Table 2) to collect pertinent information data of the included trial, such as publication years, author names, study designs, sample sizes, participant characteristics, interventions in the experimental group and the control arm, the number of intervention sessions, intervention duration, and outcome measures. After all eligible RCTs have been determined, for continuous data, means as well as standard deviations (SDs) will be collected. The Cochrane Handbook for Systematic Reviews of Interventions36 recommends that continuous data be transformed to means (SDs) in situations where they are presented in other ways (eg, median [interquartile range]). In regard to dichotomous data, each group’s total number of participants and respondents will be extracted. In addition, reviewers will email the respective authors to request missing data if related data are absent from the original publications. Any disputes between the two reviewers (J.F and Y.G) will be settled by referring to the third referee (H.G).
By extracting data for 12 randomly selected studies before fully extracting data for all included trials, the inter-rater agreements on the accuracy of data extraction will be evaluated using Kappa coefficients. Reviewers will get additional data extraction training if inter-rater consistency and accuracy are lacking.
Evaluation of the Methodological Quality
The methodological quality of each enrolled RCT will be evaluated by two raters (H.H. and L.F) independently with the risk of bias 2.0 (RoB 2.0) tool recommended by the Cochrane Collaboration.37 Five crucial domains will be used to evaluate each included study’s risk of bias: 1) the randomization method; 2) deviations from intended interventions; 3) missing outcome data; 4) measurement of outcomes; and 5) the selection of the reported result. A grade of “low”, “some concerns”, or “high” will be assigned to each domain. Additionally, reviewers will assign each trial’s overall ROB a rating of “low” (meaning low ROB in all domains), “some concerns” (meaning some concerns in at least one domain), or “high” (meaning high ROB in at least one domain, or some concerns in various domains). Arbitration with the referee (H.G) will be performed to settle any disagreements among the two raters.
Data Synthesis and Statistical Analysis
The effect size and its 95% CI will be calculated using the RevMan program (Version 5.30, Cochrane Collaboration, England) for the meta-analysis of pooled trials with extracted data. Meta-analyses will be undertaken using the random effects model due to the expected heterogeneity among the included studies arising from the probably diverse acupuncture protocols across each trial. The I2 statistic value is used by the χ2 test to measure heterogeneity across all included trials, and an I2 value more than 50% is regarded as significantly heterogeneous. Statistical significance is defined as two-sided P value less than 0.05 when analyzing pooled effects. Additionally, the reliability of meta-analysis results will be assessed by sensitivity analyses using the leave-one-out approach.
Subgroup Analysis
We will perform subgroup analyses based on the following criteria when they are available.
- Different acupuncture techniques (eg, MA, EA).
- The control arm’s different characteristics (eg, sham controls, active controls).
- Different assessment points of main outcomes.
Assessment of Evidence Strength and Certainty
The strength and certainty of the evidence will be assessed using Cochrane’s Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) approach. In detail, a general “confidence of evidence” rating that is split into 4 categories (ie, high, moderate, low, and extremely low) will be used to characterize the strength and certainty of the evidence.38
Publication Bias
Funnel plots and the Egger test will be used to investigate publication bias if 10 or more trials are present in the meta-analysis.
Ethics-Related Issues
This study does not need ethical approval because it will not incorporate any personal data.
Discussion
Acupuncture is the treasure of traditional Chinese medicine and has been used to treat both tinnitus and insomnia for a long time. Although the relevant mechanisms underlying acupuncture for treating tinnitus remain unclear, there are a few approaches in which acupuncture plays its role in relieving tinnitus: 1) affecting the olive cochlear nucleus; 2) stabilizing bilateral cochlear capillary blood flow; 3) activating cochlear hair cells.39 And research offers laboratory-based proof that acupuncture can alter the sleep-wake cycle by interfering with several levels of neurotransmitters and cytokines linked to insomnia, thereby improving sleep.40
The advantages of the current study will be discussed in the following manner. Firstly, all previous pertinent systematic reviews and meta-analyses16,19,41 in this field have exclusively focused on the effect of acupuncture on insomnia, irrespective of tinnitus-associated insomnia. Furthermore, the overwhelming majority of previous systematic reviews and meta-analyses have exclusively focused on the effectiveness of acupuncture for tinnitus,20–22 but omitting its effect on tinnitus-associated insomnia, which is a common comorbid condition of tinnitus. However, owing to the fact that tinnitus and insomnia have a bidirectional relationship, tinnitus-associated insomnia is a common and challenging disorder in real-world clinical settings and it deserves more attention and intensive investigation. As far as we are concerned, this is the first systematic review and meta-analysis that will focus on the efficacy and safety of acupuncture in tinnitus-associated insomnia. Expected results from this study will draw a firm conclusion and provide robust evidence in this field. Additionally, it may enrich the treatment approaches for tinnitus-associated insomnia by confirming a valid therapy for the treatment of tinnitus-associated insomnia.
Secondly, our systematic review and meta-analysis protocol will be thoroughly performed by referring to the PRISMA-P guideline.28 In order to include all eligible RCTs as far as possible, our study will undertake a thorough search that examines 9 mainstream English language and Chinese language databases. In addition, the GRADE method, which is advised by the Cochrane Collaboration, will be used to to appraise the strength and certainty of generated evidence. Sensitivity analysis, publication bias, and subgroup analysis will also be undertaken when they are available.
However, our study has several limitations. First of all, the bulk of the enrolled RCTs are anticipated to be carried out in China. Since publication bias appears to be more common in the field of CAM and China has a much higher percentage of published acupuncture RCTs with positive results than Western countries,42 publication bias may be present in our subsequent systematic review and meta-analysis, thereby reducing the robustness of subsequent results. Second, there is a chance that some qualified trials may not be included since just 9 mainstream English and Chinese databases will be searched.
Conclusion
In conclusion, this protocol lays out the rationale and intended methodology of a planned systematic review and meta-analysis that seeks to assess the evidence concerning the efficacy and safety of acupuncture for tinnitus-associated insomnia. Expected results and findings of this study will help patients and clinicians make informed treatment decisions based on evidence.
Ethical Statement
Given that a systematic review and meta-analysis will not involve private information of individuals, ethical approval is not required.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The work was supported by Zhejiang Provincial Famous Traditional Chinese Medicine Experts Inheritance Studio Construction Project (grant number: GZS2021027), the hospital project of the Third Affiliated Hospital of Zhejiang Chinese Medical University (grant number: ZS21ZA01), and the 2021 Special Project for Modernization of Chinese Medicine in Zhejiang Province (grant number: 2021ZX010).
Disclosure
The authors declare that they have no competing interests.
References
1. Buysse DJ. Insomnia. JAMA. 2013;309(7):706–716. doi:10.1001/jama.2013.193
2. Aazh H, Moore BCJ. Tinnitus loudness and the severity of insomnia: a mediation analysis. Int J Audiol. 2019;58(4):208–212. doi:10.1080/14992027.2018.1537524
3. Lasisi AO, Gureje O. Prevalence of insomnia and impact on quality of life among community elderly subjects with tinnitus. Ann Otol Rhinol Laryngol. 2011;120(4):226–230. doi:10.1177/000348941112000402
4. Tyler RS, Baker LJ. Difficulties experienced by tinnitus sufferers. J Speech Hear Disord. 1983;48(2):150–154. doi:10.1044/jshd.4802.150
5. Marks E, Hallsworth C, Vogt F, et al. Cognitive behavioural therapy for insomnia (CBTi) as a treatment for tinnitus-related insomnia: a randomised controlled trial. Cogn Behav Ther;2022:1–19. doi:10.1080/16506073.2022.2084155
6. Crönlein T, Langguth B, Pregler M, et al. Insomnia in patients with chronic tinnitus: cognitive and emotional distress as moderator variables. J Psychosom Res. 2016;83:65–68. doi:10.1016/j.jpsychores.2016.03.001
7. Koning HM. Sleep disturbances associated with tinnitus: reduce the maximal intensity of tinnitus. Int Tinnitus J. 2019;23(1):64–68. doi:10.5935/0946-5448.20190012
8. Wakabayashi S, Saito H, Oishi N, et al. Effects of tinnitus treatments on sleep disorders in patients with tinnitus. Int J Audiol. 2018;57(2):110–114. doi:10.1080/14992027.2017.1374565
9. Tunkel DE, Bauer CA, Sun GH, et al. Clinical practice guideline: tinnitus. Otolaryngol Head Neck Surg. 2014;151(2 Suppl):S1–s40. doi:10.1177/0194599814545325
10. Wallhäusser-Franke E, Schredl M, Delb W. Tinnitus and insomnia: is hyperarousal the common denominator? Sleep Med Rev. 2013;17(1):65–74. doi:10.1016/j.smrv.2012.04.003
11. Crönlein T, Langguth B, Geisler P, et al. Tinnitus and insomnia [M]. Tinnitus. 2007;166:227–233.
12. Richter K, Zimni M, Tomova I, et al. Insomnia associated with tinnitus and gender differences. Int J Environ Res Public Health. 2021;18(6):3209. doi:10.3390/ijerph18063209
13. Aazh H, Baguley DM, Moore BCJ. Factors related to insomnia in adult patients with tinnitus and/or hyperacusis: an exploratory analysis. J Am Acad Audiol. 2020;30(09):802–809.
14. Ismail AMA, Ali SM, Ghuiba K, et al. Autonomic functions, tinnitus annoyance and loudness, and quality of life: randomized-controlled responses to bee-humming (vibrational) respiratory training in tinnitus elderly. Complement Ther Clin Pract. 2022;48:101611. doi:10.1016/j.ctcp.2022.101611
15. Ismail AMA, Aly ME, Elfahl AA. Effect of acupuncture on tinnitus severity index in the elderly with nonpulsating tinnitus. Physiother Q. 2022;30(1):57–60.
16. Kim SA, Lee SH, Kim JH, et al. Efficacy of acupuncture for insomnia: a systematic review and meta-analysis. Am J Chin Med. 2021;49(5):1135–1150. doi:10.1142/S0192415X21500543
17. Cheuk DK, Yeung WF, Chung KF, et al. Acupuncture for insomnia. Cochrane Database Syst Rev. 2012;2012(9):Cd005472.
18. Zhao FY, Fu QQ, Kennedy GA, et al. Can acupuncture improve objective sleep indices in patients with primary insomnia? A systematic review and meta-analysis. Sleep Med. 2021;80:244–259. doi:10.1016/j.sleep.2021.01.053
19. Liu C, Xi H, Wu W, et al. Placebo effect of acupuncture on insomnia: a systematic review and meta-analysis. Ann Palliat Med. 2020;9(1):19–29. doi:10.21037/apm.2019.11.15
20. Liu F, Han X, Li Y, et al. Acupuncture in the treatment of tinnitus: a systematic review and meta-analysis. Eur Arch Otorhinolaryngol. 2016;273(2):285–294. doi:10.1007/s00405-014-3341-7
21. Huang K, Liang S, Chen L, et al. Acupuncture for tinnitus: a systematic review and meta-analysis of randomized controlled trials. Acupunct Med. 2021;39(4):264–271. doi:10.1177/0964528420938380
22. He M, Li X, Liu Y, et al. Electroacupuncture for tinnitus: a systematic review. PLoS One. 2016;11(3):e0150600. doi:10.1371/journal.pone.0150600
23. Su Q, Shi X, Zhang J, et al. Intervention of the syndrome-position point selection method on idiopathic tinnitus of phlegm-fire stagnation pattern: a randomized controlled study. J Healthc Eng. 2022;2022:9664078. doi:10.1155/2022/9664078
24. Jackson A, Macpherson H, Hahn S. Acupuncture for tinnitus: a series of six n = 1 controlled trials. Complement Ther Med. 2006;14(1):39–46. doi:10.1016/j.ctim.2005.07.005
25. Jeon SW, Kim KS, Nam HJ. Long-term effect of acupuncture for treatment of tinnitus: a randomized, patient- and assessor-blind, sham-acupuncture-controlled, pilot trial. J Altern Complement Med. 2012;18(7):693–699. doi:10.1089/acm.2011.0378
26. Dong B, Chen Z, Yin X, et al. The efficacy of acupuncture for treating depression-related insomnia compared with a control group: a systematic review and meta-analysis. Biomed Res Int. 2017;2017:9614810. doi:10.1155/2017/9614810
27. Hu H, Li Z, Cheng Y, et al. The efficacy and safety of acupuncture for depression-related insomnia: protocol for a systematic review and meta-analysis. J Pain Res. 2022;15:1939–1947. doi:10.2147/JPR.S370476
28. Moher D, Shamseer L, Clarke M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. 2015;4(1):1. doi:10.1186/2046-4053-4-1
29. Lee CJ, Iyer G, Liu Y, et al. The effect of vitamin D supplementation on glucose metabolism in type 2 diabetes mellitus: a systematic review and meta-analysis of intervention studies. J Diabetes Complications. 2017;31(7):1115–1126. doi:10.1016/j.jdiacomp.2017.04.019
30. ASSOCIATION A P. Diagnostic and Statistical Manual of Mental Disorders (DSM-IV).
31. ASSOCIATION A P. Diagnostic and Statistical Manual of Mental Disorders.
32. Medicine A A O S. ICSD-3 (International Classification of Sleep ICSD-3 Disorders) [M]. Dartmouth, Illinois: Association of Sleep Medicine; 2014.
33. Edinger JD, Arnedt JT, Bertisch SM, et al. Behavioral and psychological treatments for chronic insomnia disorder in adults: an American Academy of Sleep Medicine clinical practice guideline. J Clin Sleep Med. 2021;17(2):255–262. doi:10.5664/jcsm.8986
34. Riemann D, Baglioni C, Bassetti C, et al. European guideline for the diagnosis and treatment of insomnia. J Sleep Res. 2017;26(6):675–700. doi:10.1111/jsr.12594
35. Davidson JR. Major depressive disorder treatment guidelines in America and Europe. J Clin Psychiatry. 2010;71(Suppl E1):e04. doi:10.4088/JCP.9058se1c.04gry
36. Higgins. J, Thomas. J. Cochrane Handbook for Systematic Reviews of Interventions [M]. Chichester: Cochrane Collaboration; 2011.
37. Flemyng E, Dwan K, Moore TH, et al. Risk of bias 2 in Cochrane reviews: a phased approach for the introduction of new methodology. Cochrane Database Syst Rev. 2020;10:Ed000148. doi:10.1002/14651858.ED000148
38. Brozek JL, Akl EA, Alonso-Coello P, et al. Grading quality of evidence and strength of recommendations in clinical practice guidelines. Part 1 of 3. An overview of the GRADE approach and grading quality of evidence about interventions. Allergy. 2009;64(5):669–677. doi:10.1111/j.1398-9995.2009.01973.x
39. Luetzenberg FS, Babu S, Seidman MD. Alternative treatments of tinnitus: alternative medicine. Otolaryngol Clin North Am. 2020;53(4):637–650. doi:10.1016/j.otc.2020.03.011
40. Liu F, You J, Li Q, et al. Acupuncture for chronic pain-related insomnia: a systematic review and meta-analysis. eCAM. 2019;2019:5381028. doi:10.1155/2019/5381028
41. Liu FG, Tan AH, Peng CQ, et al. Efficacy and safety of scalp acupuncture for insomnia: a systematic review and meta-analysis. eCAM. 2021;2021:6621993. doi:10.1155/2021/6621993
42. Gang WJ, Gong CZ, Jing XH. Acupuncture randomized controlled trials: comparing China-based vs Western-based studies. Zhongguo Zhen Jiu. 2022;42(1):3–7. doi:10.13703/j.0255-2930.20201224-k0001
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.