Back to Journals » Therapeutics and Clinical Risk Management » Volume 19
Comparison of Balanced Crystalloids versus Normal Saline in Critically Ill Patients: A Systematic Review with Meta-Analysis and Trial Sequential Analysis of Randomized Controlled Trials
Received 18 April 2023
Accepted for publication 25 August 2023
Published 11 October 2023 Volume 2023:19 Pages 783—799
DOI https://doi.org/10.2147/TCRM.S416785
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor De Yun Wang
Yi Chen,1– 3 Yongli Gao1– 3
1Emergency Department of West China Hospital, Sichuan University/West China School of Nursing, Sichuan University, Chengdu City, Sichuan Province, People’s Republic of China; 2Institute of Disaster Medicine, Sichuan University, Chengdu City, Sichuan Province, People’s Republic of China; 3Nursing Key Laboratory of Sichuan Province, Chengdu City, Sichuan Province, People’s Republic of China
Correspondence: Yongli Gao, Emergency Department of West China Hospital, Sichuan University/West China School of Nursing, Sichuan University, No. 37 Guoxue Alley, Wuhou District, Chengdu, Sichuan Province, 610041, People’s Republic of China, Email [email protected]
Background: Fluid resuscitation is routinely needed for critically ill patients. However, the optimal choice between crystalloids and normal saline is in heat debate.
Objective: To conduct a meta-analysis comparing normal saline and balanced crystalloids in the treatment of critically ill patients with composite mortality as the primary outcome.
Methods: PubMed, Embase, Medline, Web of Science, and Cochrane Library were searched from inception up to March 2022. Studies of critically ill adult patients assigned to receive normal saline or balanced crystalloids were included. We conducted a meta-analysis using an inverse variance, random-effects model in addition to trial sequential analysis (TSA). The primary outcome was composite mortality. Subgroup analyses were also conducted.
Results: Eighteen full-text studies (n=36,224) were included. Balanced crystalloids were associated with lower mortality compared with normal saline (risk ratio [RR]=0.96; 95% confidential interval [CI] 0.93, 1; p=0.03; I2=0) and lower incidence of acute kidney injury/acute renal failure (RR =0.93; 95% CI = 0.87, 0.99; p=0.03). No significant difference was observed in other outcomes. In the sepsis patients, the balanced crystalloid showed a lower composite mortality rate compared with normal saline (RR =0.91; 95% CI = 0.85, 0.99; p=0.02). TSA analysis demonstrated that, with 80% power, the effect of balanced crystalloid is not larger than a 10% relative decrease in composite mortality compared with normal saline.
Conclusion and Relevance: This study demonstrated that balanced crystalloids could be an optimal choice over normal saline in critically ill patients to a reduced composite mortality rate. In patients with sepsis, the difference is especially significant. Nonetheless, the optimal resuscitation fluid option between saline and balanced crystalloid solutions should be investigated further with more evidence.
Keywords: balanced crystalloids, normal saline, critically ill, systematic review, meta-analysis
Introduction
Intravenous fluid resuscitation has long been recognized as a vital intervention in critically ill patients, especially in the early management of acute diseases1 such as shock and pancreatitis,2 to correct a volume deficit. Although normal saline (0.9% sodium chloride) remains the most commonly used fluid to date,3 some reports have demonstrated its demerits. A high volume of normal saline has been associated with an increased risk of hyperchloremic acidosis,4 acute kidney injury (AKI),5–8 and in some cases, mortality.9 Consequently, there is a growing consideration of the utilization of balanced crystalloids as an alternative.
Balanced crystalloid solutions (eg lactated Ringer’s, Plasma-Lyte), characterized by the substitution of chloride anions with bicarbonate or buffers,10 possess lower chloride content and stronger buffering capacity. The efficacy of balanced crystalloid solutions has been substantiated through accumulating evidence, as demonstrated by their ability to reduce the incidence of hyperchloremic acidosis11 in brain-injured patients,12 expedite the resolution of metabolic acidosis in severe diabetic ketoacidosis (DKA),13 and diminish inflammation14–16 in acute pancreatitis, etc.
In two recently published meta-analyses, critically ill patients resuscitated with balanced crystalloids have significantly lower mortality than patients with saline [(0.75, 0.99) in Hammond et al17 and (0.68, 0.95) in Nam et al].18 But in 2022, another randomized controlled trial (RCT) conducted by Finfer et al19 published an insignificant difference in the 90 days mortality rate between the Plasma-Lyte 148 group and the saline group.
The inconclusive findings have highlighted the need for further investigation. Therefore, the objective of our research is to conduct an updated systematic review with meta-analysis and trial sequential analysis of randomized controlled trials to compare the effectiveness of the balanced crystalloid solution and normal saline in critically ill patients.
Materials and Methods
This study was performed following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement.20
Search Strategy and Study Selection
We searched PubMed, Embase, Medline, Web of Science, and Cochrane Library from inception up to March 2022 without language restrictions to compare balanced crystalloids with normal saline in critically ill patients. The detailed search strategy was presented in Supplementary Material 1. Additionally, we also looked through the references of related articles.
The Included Studies Met the Following Criteria
- Population: critically ill adult patients admitted to an intensive care unit (ICU) who need fluid resuscitation;
- Intervention: balanced crystalloids, such as lactated Ringer’s solution (LRS), Plasma-Lyte A, balanced multi-electrolyte solution (BMES), isofundine, and streofundin;
- Comparison: normal saline;
- Outcome: the primary outcome was composite mortality and the secondary outcomes include the incidences of AKI and acute renal failure (ARF), requiring renal replacement therapy (RRT), hospitalization time, and mechanical ventilation–free days;
- Study design: RCT.
The exclusion criteria were as follows:
- Critically ill patients aged younger than 18;
- Patients treated with intravenous crystalloids but subsequently hospitalized outside an ICU;
- Fluids are used as maintenance instead of resuscitation;
- Meta-analyses, reviews, protocols, conference abstracts, case reports, non-English articles and repeated data;
Two researchers (GYL, CY) independently reviewed and evaluated the full text of eligible studies to decide to include the article. Any discrepancies were settled by discussing with senior researchers.
Data Extraction and Outcome Measurement
Two researchers (GYL, CY) independently collected data from the eligible articles. A third reviewer would resolve any disagreements. We developed a data extraction sheet in standardized Excel (Microsoft Corporation). The following variables were extracted: the name of the first author, publication year, the location of the study, interventions, demographic characteristics of patients, in-hospital details, and outcomes. In the case of missing data, we attempted to extract data from other meta-analyses or calculated following the Cochrane Collaboration for Systematic Reviews guidelines.21
The primary outcome was composite mortality during the hospital stay after randomization. Secondary outcomes included the incidence of AKI and ARF, requiring receipt of RRT, hospitalization time, and mechanical ventilation-free time. To acquire more data to analyze, composite mortality was defined as death at the final follow-up time in all studies. AKI was defined as Kidney Disease: Improving Global Outcomes [KDIGO] stage 2 or 3.22 ARF was consensually defined by the Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group.23 For hospitalization time, 28/30 or 90-day mortality was defined as the death at 28/30 or 90 days when the day of randomization to receive either saline solution or balanced solution was considered as day “0”. All the definitions listed were extracted from individual studies and not recreated for this analysis.
Quality Assessment
Two researchers (GYL, CY) independently assessed the risk of bias in each study by using methods from the Cochrane Collaboration24 which demand to response “low risk”, “high risk”, or ‘some concerns’ in five domains of each RCT study: (i) randomization process; (ii) deviations from intended interventions; (iii) missing outcome data; (iv) measurement of the outcome; (v) selection of the reported result. Any disagreements were dealt with by the third reviewer. We also assessed the certainty of the evidence for each outcome through the Grading Recommendations Assessment, Development, and Evaluation (GRADE) system.25 We gave a lower rating based on five domains (risk of bias, indirectness, inconsistency, imprecision, and publication bias) and a higher rating based on three domains (large magnitude of effect, adjustment for potential confounders, and dose-response gradient). Overall certainty of evidence was expressed in four categories (high, moderate, low, and very low).
Statistical Analysis
Firstly, we evaluated the transitivity assumption by comparing the distribution of potential effect modifiers (country, fluid types, patient group, mean age) for all studies. Secondly, with the Hartung-Knapp (HAKN) method or DerSimonian-Laird (DL) method,26 we measured the risk ratio (RR) with the 95% confidence intervals (CIs) for dichotomized outcome data such as mortality, while the standard mean differences (SMD) with the 95% CIs for continuous outcome data. Then we carried out I2 statistics to examine the heterogeneity between studies. The heterogeneity was considered as low (<25%), moderate (26–50%), and high (>50%) based on the I2 values.27 The fixed-effect model was used to assume that all studies are part of a homogeneous population. There were some differences in the balanced crystalloid groups that were used since the target population of the included studies was not identical. Thus, we chose the random-effects model to analyze the results.26 Leave-one-out analysis28 and GOSH test29 were applied for sensitive analysis to explore possible causes of heterogeneity.
Moreover, we also performed subgroup analyses for the mortality according to demographic characteristics like age (>60 or ≤60), country (western or non-western) ICU or hospital setting, hospitalization time (28/30 days and 90 days), the indications for fluid resuscitation (DKA, sepsis or other above-mentioned sources of ICU admission), the Acute Physiology and Chronic Health Evaluation (APACHE) II score, and study quality (low, some concerns and high risk of bias). Besides, the contour-enhanced funnel plots were illustrated to assess the publication bias.
Furthermore, to stimulate the type I or type II errors in analysis, we conducted a trial sequential analysis (TSA, TSA software: v.0.9.5.10 beta). The methods of Wetterslev et al30 and the random-effects model were adopted. The needed information size was calculated for a minimum relative risk reduction of 10%. We supposed type II error of 20% and type I error of 5% and adjusted between-study heterogeneity for sample size calculations.
All the statistical analyses and illustrations were done in R statistical software system v4.1.0. using packages: “meta31”, “metafor32”, “dmetar33”.
Results
Search results and Study Characteristics
A total of 1127 records were retrieved by the literature search strategy on the aforementioned databases. We excluded 692 duplicated studies, 188 unrelated studies, and other 219 inappropriate records. The detailed selection process was shown in Figure 1 with eighteen full-text studies left for the following meta-analysis.5,9,12–16,19,34–43 The eligible studies enrolled 36,224 patients and were published between 2001 and 2022 in 11 countries. 17,708 patients received balanced crystalloids and 18,516 patients received normal saline. The mean age of included patients ranged from 35.2 to 69.9 years old. The male proportion accounted for 59% of the entire population. The transitivity of potential effect modifiers was illustrated in Figure 2. Ten studies recorded 28/30 days mortality, 4 in 90-day mortality, 6 in ICU mortality and 10 in-hospital mortality. The detailed characteristics of eligible patients in each study were documented in Table 1.
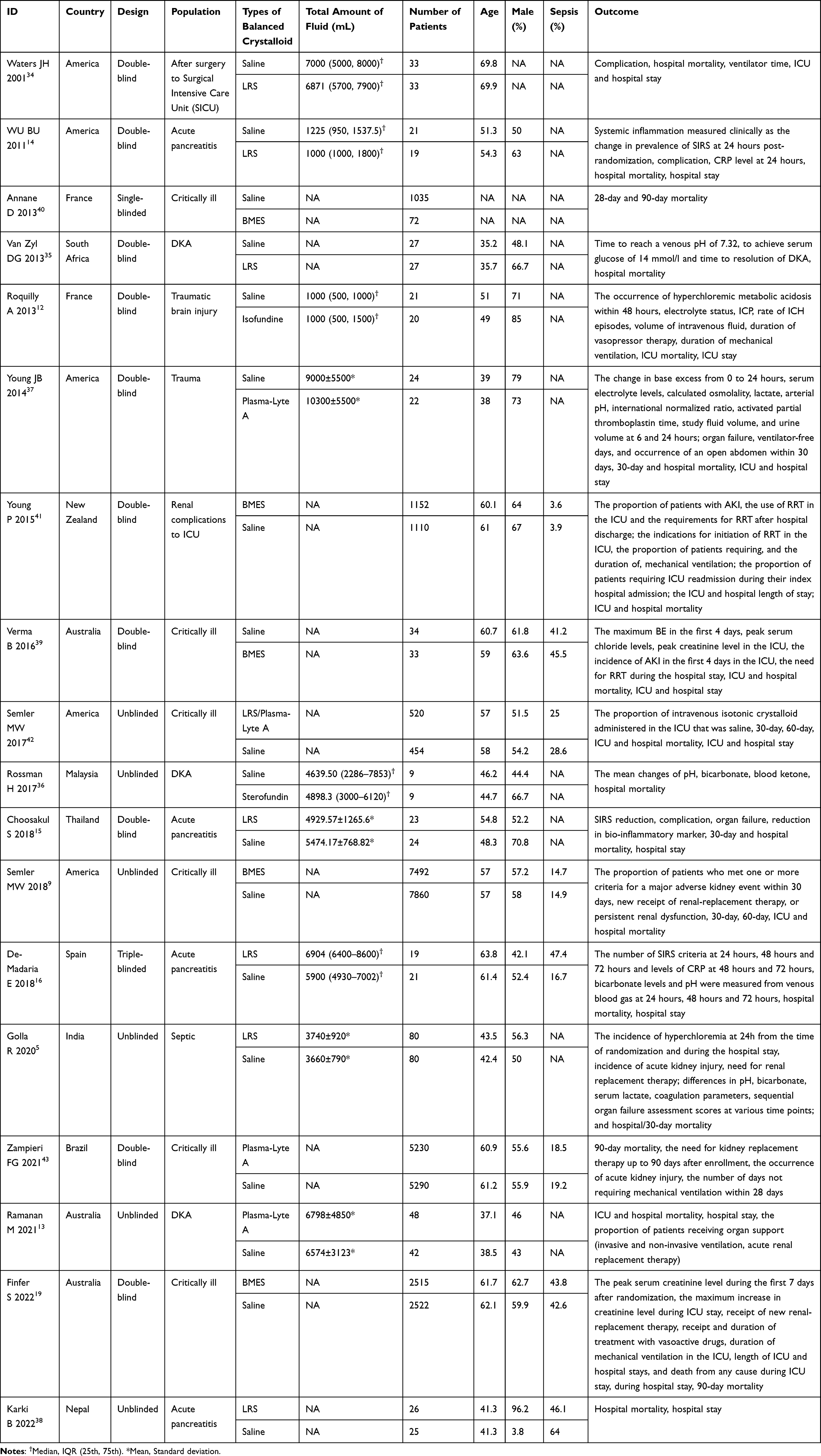 |
Table 1 The Characteristics of Included Studies |
 |
Figure 1 The flowchart for the systematic search and the selection of studies. |
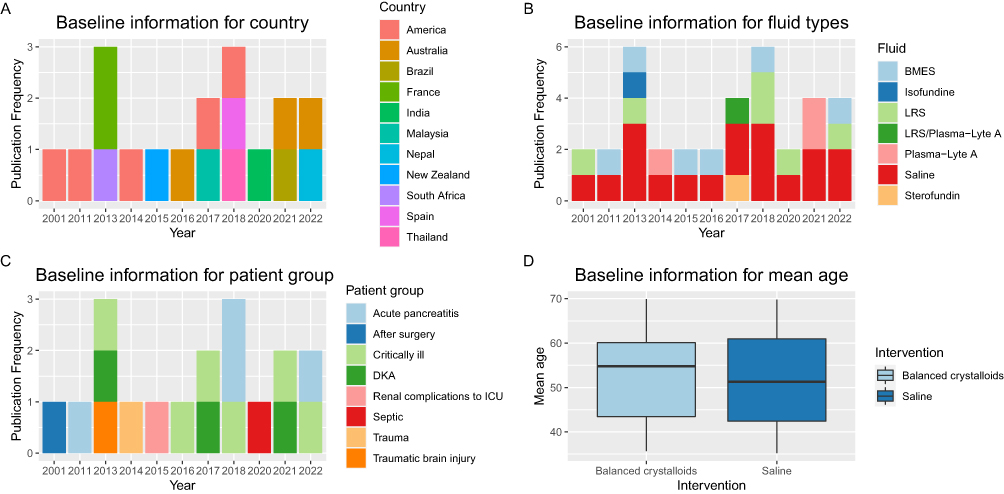 |
Figure 2 The transitivity of potential effect modifiers. (A) The geography information of all included trials. (B). The frequency of fluid types published in clinical trials. (C). The frequency of patient groups published in clinical trials. (D) The mean age of all included patients. Abbreviations: ICU, intensive care unit; DKA, diabetic ketoacidosis; BMES, balanced multi-electrolyte solution; LRS, lactated Ringer’s solution. |
Quality of Studies
The risk of bias assessment was summarized in Figure 3. We showed the results of each quality item as percentages across studies. Most studies were high-quality with a low risk of bias in all items. Two trials were at high risk in the randomization process,9,42 one showed high risk in deviations from intended interventions.5
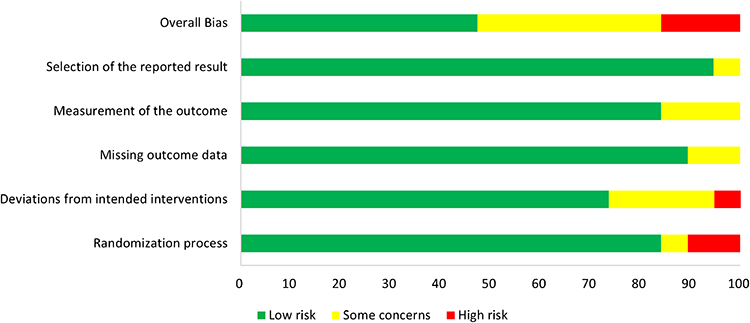 |
Figure 3 Summary of risk of bias of the included randomized controlled trials. |
Based on the GRADE system, the certainty of evidence was assessed for each outcome. Composite mortality, incidence of AKI/ARF, RRT use rate, and ventilator-free days were classified as moderate certainty. Hospitalization stay was classified as very low certainty. The detailed results were summarized in Table 2.
 |
Table 2 Summary Table of GRADE System |
Primary Outcome
As shown in Figure 4A, a total of 18 studies provided composite mortality data for 36,224 patients. The pooled estimated RR was 0.96 (95% CI 0.93, 1; p=0.03) by using the HAKN method for balanced crystalloids solutions compared with saline with low heterogeneity (I2=0). When the studies were pooled using the DL method, the estimated RR was 0.96 with low heterogeneity (95% CI 0.92, 1.01; p=0.09; I2=0).
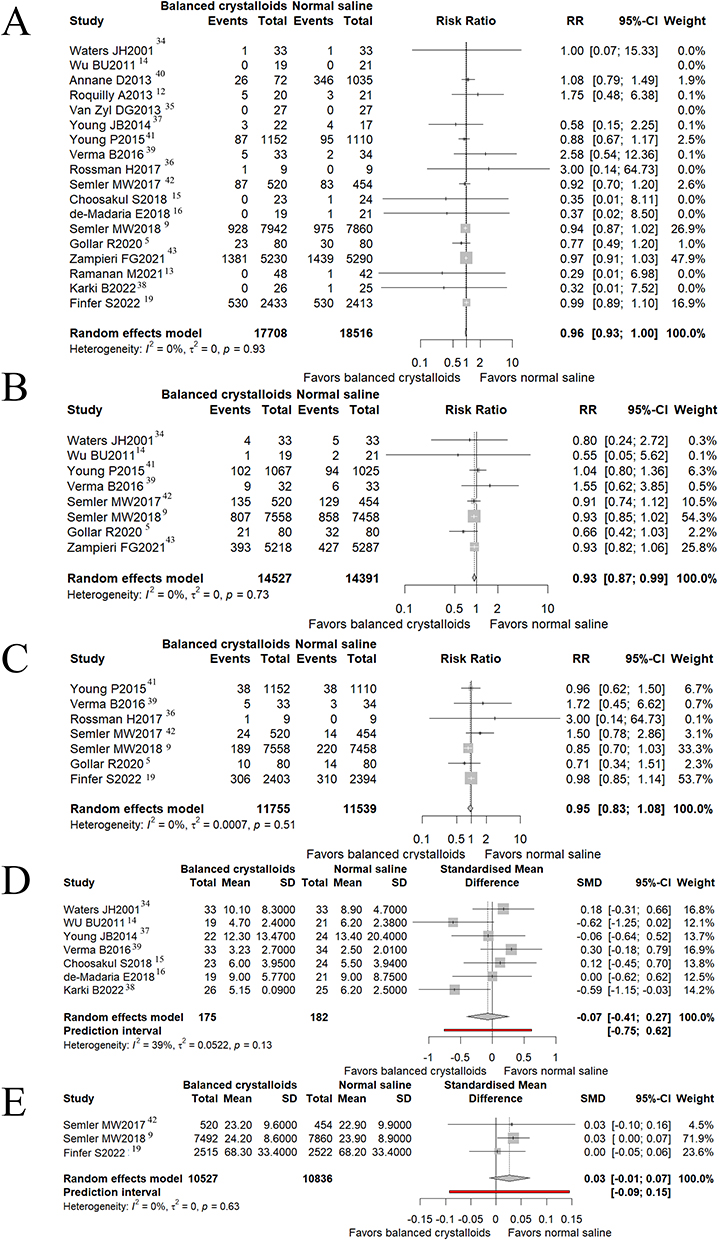 |
Figure 4 The forest plot for outcomes. (A) Composite mortality. (B) The incidence of acute kidney injury. (C) The rate of requiring renal replacement therapy. (D) The hospitalization stays (E) The ventilator-free days. |
Secondary Outcomes
Eight studies and 28,918 patients were evaluated for the incidence of AKI/ARF, and the results showed a significant decrease when applying balanced crystalloid solutions to patients, compared with normal saline, using the HAKN method (RR =0.93; 95% CI = 0.87, 0.99; p=0.03, Figure 4B). In the RRT use rate, seven studies and 23,294 patients were evaluated, there was no significant difference between balanced crystalloids and normal saline using the HAKN method (RR =0.95; 95% CI = 0.83, 1.08; p=0.34, Figure 4C). During hospitalization stay, seven studies and 357 patients were evaluated, there was no significant difference between balanced crystalloids versus saline using the HAKN method (SMD=−0.07; 95% CI, −0.41 to 0.27; p=0.64, Figure 4D). Three studies and 21,363 patients were evaluated for the ventilator-free days, there was no significant difference between those assigned to balanced crystalloids versus saline by using the HAKN method (SMD=0.03; 95% CI, −0.01 to 0.07; p=0.10, Figure 4E).
Subgroup Analysis
Regarding demographic characteristics, 11 RCTs and 6 RCTs included patients with an average age below 60 and above 60, respectively. Patients younger than 60 years old showed significantly decreased mortality comparing balanced crystalloids with saline (RR = 0.93; 95% CI = 0.87, 0.98; p=0.04, Figure 5). Furthermore, 13 RCTs RCTs were conducted in Western countries while 5 RCTs were in non-western countries. Results showed a significant difference in RCTs from Western countries (RR = 0.96; 95% CI = 0.93, 1.00; p = 0.04, Figure 5).
 |
Figure 5 The subgroup analysis of composite mortality. Abbreviations: CI, confidential interval; LRS, lactated Ringer’s solution; BMES, balanced multi-electrolyte solution; AKI, acute kidney injury; DKA, diabetic ketoacidosis; APACHE, Acute Physiology and Chronic Health Evaluation; ICU, intensive care unit. |
The ICU mortality and hospital mortality of patients involved 6 RCTs and 10 RCTs respectively. The results suggested no significant difference in ICU mortality between balanced crystalloids and saline (RR =0.97; 95% CI = 0.87, 1.08; p=0.57, Figure 5). A similar result was shown in the hospital mortality (RR =0.95; 95% CI = 0.86, 1.04; p=0.25, Figure 5). While the risk of 28/30 day mortality was significantly lower in the balanced crystalloids group than in the saline group, included in 10 studies (RR =0.94; 95% CI = 0.89, 0.99; p=0.02, Figure 5). The 90-day mortality included 4 studies, was found no significant difference between balanced crystalloids and saline (RR =0.98; 95% CI = 0.93, 1.03; p=0.35, Figure 5).
Further, we classified the patients based on indications for fluid resuscitation: sepsis, trauma, acute pancreatitis (AP), traumatic brain injury (TBI), admission to ICU after surgery, DKA, and renal complications. In 6 RCTs reporting patients with sepsis, balanced crystalloids could significantly decrease composite mortality compared with saline (RR =0.91; 95% CI = 0.85, 0.99; p=0.02, Figure 5). The difference was not statistically significant in the composite mortality of patients with trauma between balanced crystalloids and saline (RR =0.92; 95% CI = 0.74, 1.15; p=0.45, Figure 5). The RR for composite mortality of patients with TBI was higher in the balanced crystalloids group than in the saline group, but the difference was not statistically significant (RR =1.26; 95% CI = 0.93, 1.7; p=0.13, Figure 5). In 5 RCTs, patients were admitted to ICU after surgery. For these patients, the pooled estimate of the RR for patients who received balanced crystalloids compared with saline was 0.95 (95% CI = 0.87, 1.04; p=0.28, Figure 5). As for the results of patients with AKI and DKA, there were no significant differences between balanced crystalloids and saline respectively (RR =0.98; 95% CI = 0.92, 1.04; p=0.46 and RR =0.78; 95% CI = 0.24, 2.49; p=0.67, Figure 5).
Lastly, we dived the studies into three groups according to risk of bias. No significant difference was observed in low risk of bias group (8 RCTs, RR = 0.98; 95% CI = 0.92, 1.03; p = 0.30), some concerns group (7 RCTs, RR = 0.95; 95% CI = 0.88, 1.02; p = 0.14), high risk of bias group (3 RCTs, RR = 0.88; 95% CI = 0.73, 1.05; p = 0.09).
Analysis of Heterogeneity
The analysis of heterogeneity in the meta-analysis of hospitalization stay revealed a moderate level (I2 = 39%). The Leave-one-out plot demonstrated that the lowest levels of heterogeneity were observed when excluding the studies “Karki B 2022” (I2 = 13%) and “WU BU 2011” (I2 = 23%) (Supplementary Figure 1). Notably, the results showed a significant shift in the opposite direction upon exclusion of these two RCTs (omitting Karki B 2022: SMD = 0.03; 95% CI = −0.28, 0.35; p = 0.79; omitting WU BU 2011: SMD = 0.01; 95% CI = −0.32, 0.34; p = 0.93). Moreover, the GOSH test identified the studies “Kaiki B 2022” and “Verma B 2016” as contributors to the heterogeneity. After excluding these studies, the pooled effect was smaller but still in the same order of magnitude (SMD = −0.037; 95% CI = −0.41, 0.33; p = 0.79; Table 3), while the I2 of the meta-analysis decreased to be of low level (I2 = 5.70%). Overall, despite the GOSH test indicating an acceptable impact of influential studies, the leave-one-out analysis revealed fluctuations in the pooled effect, thereby undermining the stability of the results.
 |
Table 3 Sensitive Analysis for Hospitalization Stay |
Furthermore, a subgroup analysis was performed based on the quality of the studies. Four RCTs reported studies with a low risk of bias, while three RCTs reported studies with some concerns. The results showed no heterogeneity (I2 = 0) in the low risk of bias group, whereas a high level of heterogeneity (I2 = 50.10%) in the some concerns group (Table 3). These findings suggest that the heterogeneity observed is not attributable to the quality of the studies.
Publication Bias
We performed funnel plots to assess the publication bias among the included studies. No potential publication bias was observed for primary outcomes as shown in Figure 6. But the results of Karki et al38 and Semler et al9 for hospitalization time and ventilator-free days respectively have significant publication bias (p < 0.05).
 |
Figure 6 The funnel plot for primary and secondary outcomes. (A) Composite mortality. (B) The incidence of acute kidney injury and acute renal failure. (C) The rate of requiring renal replacement therapy. (D) The hospitalization stays (E) The ventilator-free days. |
TSA Analysis
Based on a risk reduction of 10%, the heterogeneity (Q = 7.68), and a 12% baseline risk of composite mortality (based on the mean mortality rate of the control group), the cumulative Z-statistic did not reach above 1.96, which corresponds to the nominal threshold for statistical significance. Additionally, it crossed below the futility boundaries, demonstrating with 80% power that the effect of balanced crystalloid is not larger than a 10% relative reduction compared with normal saline. (Figure 7).
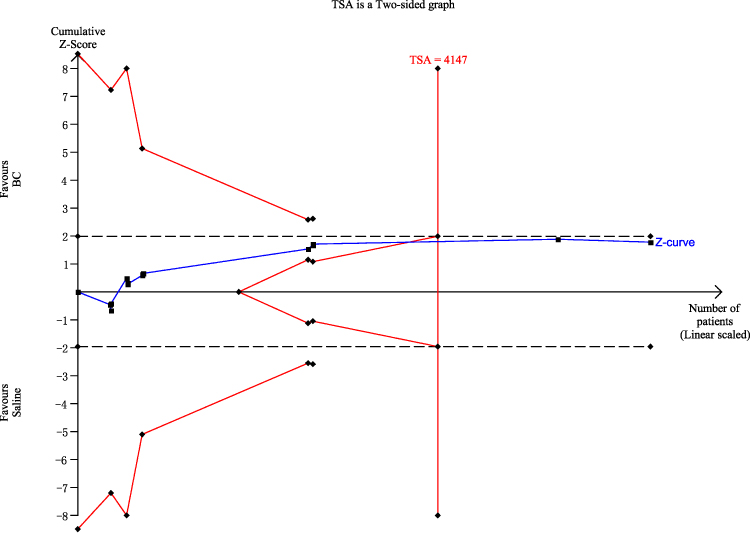 |
Figure 7 Trial sequential analysis results. The required event size to demonstrate a 10% relative decrease in composite mortality with a control group proportion of 12%, an alpha of 5% and a beta of 20% is 4147 (vertical red line). The red lines represent the trial sequential monitoring boundaries and the futility boundaries. The dashed dark lines cross the y-axis at 1.96 and −1.96, which correspond to the nominal threshold for statistical significance. The blue line is the cumulative Z-curve. |
Discussion
The present meta-analysis and systematic review assessed the efficacy and safety of balanced crystalloids versus saline for critically ill patients who required fluid resuscitation. The results of the composite mortality rate showed an 8–9% relative reduction to a 0–1% relative increase with low heterogeneity when comparing the balanced crystalloids with saline for fluid resuscitation. The balanced crystalloids showed a reduction in the incidence of AKI by 2–14% compared with saline. The protective role of balanced crystalloids was also found in patients with sepsis with a 9% reduction in composite mortality rate compared with saline.
Fluid and electrolyte management is essential in AKI patients. Continuous hemodynamic monitoring and direct supervision of the physician are necessary to prevent fluid overload and related complications.44,45 Balanced crystalloids solution, possessing a sodium and chloride content closer to that of plasma, is believed to have fewer adverse effects on acid-base balance, water regulation, and salt regulation10 compared with saline. In this study, the balanced crystalloid solution was correlated with a lower incidence of AKI significantly, consistent with Nam et al.18 However, in Hammond et al,46 including only trials with a low risk of bias, the RR was 0.96 [95% CI, 0.89, 1.02] for AKI and 0.95 [95% CI, 0.81, 1.11] for RRT with balanced crystalloid solution compared with saline. This discrepancy would originate from the number of trials included as we included 9 studies while they included only 5. Meanwhile, it is notable that our results showed that in the AKI patients, the composite mortality rate did not differ between the two groups with low heterogeneity, which suggests that the use of balanced crystalloid or saline would not influence the prognosis of patients once the diagnosis of AKI was confirmed. However, further research is necessary to account for variations in study design, population characteristics, and fluid administration protocols (including quantity and type of fluid).
On the other hand, administration of isotonic or hypertonic saline may be a suitable choice to maintain or increase serum osmolality for patients with elevated intracranial pressure. Patients with TBI would take advantage of normal saline as proved in several preliminary studies.12,37,47,48 But according to a review published in 2023 by Esteban-Zubero et al49, crystalloids and hyperosmolar fluid may be most beneficial in TBI, although the evidence is not as clear. In our results and two of the published trials,12,37 the saline did not relate to a significant decrease in composite mortality. Nevertheless, as TBI is a very special situation where low tonicity presumably increases mortality the inconsistent results could be caused by the change in ion level which did not strong enough to influence the survival results. The very small number of traumatic brain injury studies included in this meta-analysis is also not inconclusive, requiring further evaluation. While for the septic patients, the significantly lower mortality rate was confirmed not only in our results but also in Tseng et al50 and Winters et al.51
A group of researchers (Hammond et al) published a meta-analysis recently.46 The authors used both HAKN and DL random-effect models and also conducted a Bayesian meta-analysis. They searched 1779 records and summarized six low bias risk studies, in which the pooled RR of 90-day mortality of balanced crystalloid solution versus saline was 0.96 [95% CI, 0.91–1.01] in the HAKN model, 0.96 [95% CI, 0.92–1.01] in the DL model, 0.96 [95% CI, 0.88–1.04] in Bayesian meta-analysis. The interpretation of results, as they stated, will depend on an individual’s preference for a frequentist or Bayesian approach. In our results, the RR and CI between balanced crystalloid solution and saline were also slightly influenced by the statistical methods (0.96 [95% CI, 0.93–1.00] in the HAKN method, 0.96 [95% CI, 0.92–1.01] in the DL method). However, with TSA analysis, the 10% relative reduction of composite mortality when comparing balanced crystalloid with normal saline was challenged with 5% type I error and 20% type II error. The balanced crystalloid was supposed to cause fewer adverse effects on acid-base balance than saline9 based on its composition and this concept was proved by a series of studies. Firstly, in the health volunteers, saline was found to decrease renal cortical tissue perfusion compared with Plasma-Lyte through the induction of hyperchloremia.52,53 Then in observational studies and trials in the operating room, patients who were treated with balanced crystalloids also showed decreased complications.54–56 But recent RCTs failed to verify this positive effect of balanced crystalloids in critically ill patients.9,41,42 This phenomenon recalled the pendulum effect brought up by Dr. Jean-Louis Vincent,57 which means initially apparent beneficial effects have not been confirmed in later trials. To be specific, there were differences in the type and amount of fluid that were used. Buffers between different solutions like Plasma-Lyte A and LRS also differ from each other. And for 90-day mortality, it might be too far to see the significant difference of 3–4 liters of crystalloid fluid that are used on day one of admission. All these factors could influence the final result. And this should be attached to more importance when it comes to critically ill patients. With critically ill patients, even a slight difference in mortality or other outcomes may result in important clinical influence at the population level. Thus, any simple interpretation of results or irrational prejudice of choice against a specific patient should be opposed.
Limitations
This meta-analysis contains several limitations. Firstly, the amount, sequence, and types of fluid resuscitated would be an inevitable heterogeneity source in the results, whose influence should not be ignored. Secondly, as stated in the results, the definition of AKI is different between the studies. Additionally, the outcome results in subgroups were missing or the number of events was zero, resulting in the undermining of the statistical power of our results.
Conclusion
Our meta-analysis indicated that balanced crystalloids could be a more beneficial treatment for critically ill patients. But further evidence based on a large population, more robust data, and a more comprehensive view is still required. Given the importance of rapid infusion of large volumes in the early clinical practice for critically ill patients, clinicians are advised to select the most accessible method as long as they are reasonable and effective based on our experience.
Data Sharing Statement
The datasets used or analyzed during the current study are available from the corresponding author on reasonable request.
Consent to Publish Statement
The details of all images can be published and the persons providing consent have been shown the article contents to be published.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hayakawa K. Aggressive fluid management in the critically ill: pro. J Intensive Care. 2019;7(1):1–3. doi:10.1186/s40560-019-0361-9
2. Gardner TB, Vege SS, Chari ST, et al. Faster rate of initial fluid resuscitation in severe acute pancreatitis diminishes in-hospital mortality. Pancreatology. 2009;9(6):770–776. doi:10.1159/000210022
3. Finfer S, Liu B, Taylor C, Bellomo R, Myburgh J. SAFE TRIPS Investigators. Resuscitation fluid use in critically ill adults: an international cross-sectional study in 391 intensive care units. Crit Care. 2010;14(5):R185. doi:10.1186/cc9293
4. Scheingraber S, Rehm M, Sehmisch C, Finsterer U. Rapid saline infusion produces hyperchloremic acidosis in patients undergoing gynecologic surgery. Anesthesiology. 1999;90(5):1265–1270. doi:10.1097/00000542-199905000-00007
5. Golla R, Kumar S, Dhibhar DP, Bhalla A, Sharma N. 0.9% saline V/S Ringer’s lactate for fluid resuscitation in adult sepsis patients in emergency medical services: an open-label randomized controlled trial. Hong Kong J Emerg Med. 2020;2020:1024907920948983.
6. Wilcox CS. Regulation of renal blood flow by plasma chloride. J Clin Invest. 1983;71(3):726–735. doi:10.1172/JCI110820
7. Yunos NM, Bellomo R, Glassford N, Sutcliffe H, Lam Q, Bailey M. Chloride-liberal vs. chloride-restrictive intravenous fluid administration and acute kidney injury: an extended analysis. Intensive Care Med. 2015;41(2):257–264. doi:10.1007/s00134-014-3593-0
8. Bellomo R, Hegarty C, Story D, Ho L, Bailey M, Bailey M. Association between a chloride-liberal vs chloride-restrictive intravenous fluid administration strategy and kidney injury in critically ill adults. JAMA. 2012;308(15):1566–1572. doi:10.1001/jama.2012.13356
9. Semler MW, Self WH, Wanderer JP, et al. Balanced crystalloids versus saline in critically ill adults. N Engl J Med. 2018;378(9):829–839.
10. Semler MW, Kellum JA. Balanced crystalloid solutions. Am J Respir Crit Care Med. 2019;199(8):952–960. doi:10.1164/rccm.201809-1677CI
11. Soussi S, Ferry A, Chaussard M, Legrand M. Chloride toxicity in critically ill patients: what’s the evidence? Anaesth Crit Care Pain Med. 2017;36(2):125–130. doi:10.1016/j.accpm.2016.03.008
12. Roquilly A, Loutrel O, Cinotti R, et al. Balanced versus chloride-rich solutions for fluid resuscitation in brain-injured patients: a randomised double-blind pilot study. Crit Care. 2013;17(2):R77. doi:10.1186/cc12686
13. Ramanan M, Attokaran A, Murray L, et al. Sodium chloride or Plasmalyte-148 evaluation in severe diabetic ketoacidosis (SCOPE-DKA): a cluster, crossover, randomized, controlled trial. Intensive Care Med. 2021;47(11):1248–1257. doi:10.1007/s00134-021-06480-5
14. Wu BU, Hwang JQ, Gardner TH, et al. Lactated Ringer’s solution reduces systemic inflammation compared with saline in patients with acute pancreatitis. Clin Gastroenterol Hepatol. 2011;9(8):710–717. e711. doi:10.1016/j.cgh.2011.04.026
15. Choosakul S, Harinwan K, Chirapongsathorn S, et al. Comparison of normal saline versus Lactated Ringer’s solution for fluid resuscitation in patients with mild acute pancreatitis, A randomized controlled trial. Pancreatology. 2018;18(5):507–512. doi:10.1016/j.pan.2018.04.016
16. de-Madaria E, Herrera-Marante I, González-Camacho V, et al. Fluid resuscitation with lactated Ringer’s solution vs normal saline in acute pancreatitis: a triple-blind, randomized, controlled trial. United European Gastroenterol J. 2018;6(1):63–72. doi:10.1177/2050640617707864
17. Hammond DA, Lam SW, Rech MA, et al. Balanced crystalloids versus saline in critically ill adults: a systematic review and meta-analysis. Ann Pharmacother. 2020;54(1):5–13. doi:10.1177/1060028019866420
18. Jae-Hyun N. Balanced Crystalloids versus Normal Saline in Critically Ill Patients: A Systematic Review and Meta-Analysis. Hanyang University; 2022.
19. Finfer S, Micallef S, Hammond N, et al. Balanced multielectrolyte solution versus saline in critically ill adults. N Engl J Med. 2022;386(9):815–826. doi:10.1056/NEJMoa2114464
20. Moher D, Liberati A, Tetzlaff J, Altman DG; Group* P. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med. 2009;151(4):264–269. doi:10.7326/0003-4819-151-4-200908180-00135
21. Cumpston M, Li T, Page MJ, et al. Updated guidance for trusted systematic reviews: a new edition of the Cochrane Handbook for systematic reviews of interventions. Cochrane Database Syst Rev. 2019;10:Ed000142. doi:10.1002/14651858.ED000142
22. Kellum JA, Lameire N, Aspelin P, et al.; Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO clinical practice guideline for acute kidney injury. Kidney Inter Suppl. 2012;2(1):1–38.
23. Bellomo R, Ronco C, Kellum JA, Mehta RL, Palevsky P. Acute renal failure - definition, outcome measures, animal models, fluid therapy and information technology needs: the Second international consensus conference of the acute dialysis quality Initiative (ADQI) group. Crit Care. 2004;8(4):R204–212. doi:10.1186/cc2872
24. Higgins JP, Altman DG, Gøtzsche PC, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928. doi:10.1136/bmj.d5928
25. Guyatt GH, Oxman AD, Vist GE, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008;336(7650):924–926. doi:10.1136/bmj.39489.470347.AD
26. IntHout J, Ioannidis JP, Borm GF. The Hartung-Knapp-Sidik-Jonkman method for random effects meta-analysis is straightforward and considerably outperforms the standard DerSimonian-Laird method. BMC Med Res Methodol. 2014;14:25. doi:10.1186/1471-2288-14-25
27. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557–560. doi:10.1136/bmj.327.7414.557
28. Viechtbauer W, Cheung MW. Outlier and influence diagnostics for meta-analysis. Res Synth Methods. 2010;1(2):112–125. doi:10.1002/jrsm.11
29. Olkin I, Dahabreh IJ, Trikalinos TA. GOSH - a graphical display of study heterogeneity. Res Synth Methods. 2012;3(3):214–223. doi:10.1002/jrsm.1053
30. Wetterslev J, Thorlund K, Brok J, Gluud C. Trial sequential analysis may establish when firm evidence is reached in cumulative meta-analysis. J Clin Epidemiol. 2008;61(1):64–75. doi:10.1016/j.jclinepi.2007.03.013
31. Balduzzi S, Rücker G, Schwarzer G. How to perform a meta-analysis with R: a practical tutorial. Evid Based Ment Health. 2019;22(4):153–160. doi:10.1136/ebmental-2019-300117
32. Viechtbauer W. Conducting Meta-Analyses in R with the metafor Package. J Stat Softw. 2010;36(3):1–48. doi:10.18637/jss.v036.i03
33. Harrer M, Cuijpers P, Furukawa T, Ebert DD. Dmetar: companion R Package For The Guide “Doing Meta-Analysis in R”. R Package Version. 2019;9000:1.
34. Waters JH, Gottlieb A, Schoenwald P, Popovich MJ, Sprung J, Nelson DR. Normal saline versus lactated Ringer’s solution for intraoperative fluid management in patients undergoing abdominal aortic aneurysm repair: an outcome study. Anesth Analg. 2001;93(4):817–822. doi:10.1097/00000539-200110000-00004
35. Van Zyl DG, Rheeder P, Delport E. Fluid management in diabetic-acidosis--Ringer’s lactate versus normal saline: a randomized controlled trial. Qjm. 2012;105(4):337–343. doi:10.1093/qjmed/hcr226
36. Rossman H, Mahathar AW, Azlan NNM. Comparing sterofundin to 0.9% sodium chloride infusion in managing diabetic ketoacidosis: a pilot study. Med Health Kuala Lumpur. 2017;12(2):179–192.
37. Young JB, Utter GH, Schermer CR, et al. Saline versus Plasma-Lyte A in initial resuscitation of trauma patients: a randomized trial. Ann Surg. 2014;259(2):255–262. doi:10.1097/SLA.0b013e318295feba
38. Karki B, Thapa S, Khadka D, et al. Intravenous Ringers lactate versus normal saline for predominantly mild acute pancreatitis in a Nepalese Tertiary Hospital. PLoS One. 2022;17(1):e0263221. doi:10.1371/journal.pone.0263221
39. Verma B, Luethi N, Cioccari L, et al. A multicentre randomised controlled pilot study of fluid resuscitation with saline or Plasma-Lyte 148 in critically ill patients. Crit Care Resusc. 2016;18(3):205–212.
40. Annane D, Siami S, Jaber S, et al. Effects of fluid resuscitation with colloids vs crystalloids on mortality in critically ill patients presenting with hypovolemic shock: the CRISTAL randomized trial. JAMA. 2013;310(17):1809–1817. doi:10.1001/jama.2013.280502
41. Young P, Bailey M, Beasley R, et al. Effect of a buffered crystalloid solution vs saline on acute kidney injury among patients in the intensive care unit: the SPLIT randomized clinical trial. JAMA. 2015;314(16):1701–1710. doi:10.1001/jama.2015.12334
42. Semler MW, Wanderer JP, Ehrenfeld JM, et al. Balanced crystalloids versus saline in the intensive care unit. The SALT randomized trial. Am J Respir Crit Care Med. 2017;195(10):1362–1372. doi:10.1164/rccm.201607-1345OC
43. Zampieri FG, Machado FR, Biondi RS, et al. Effect of intravenous fluid treatment with a balanced solution vs 0.9% saline solution on mortality in critically ill patients: the BaSICS randomized clinical trial. JAMA. 2021;326(9):1–12. doi:10.1001/jama.2021.11684
44. Kellum JA, Romagnani P, Ashuntantang G, Ronco C, Zarbock A, Anders H-J. Acute kidney injury. Nat Rev Dis Primers. 2021;7(1):52. doi:10.1038/s41572-021-00284-z
45. Pickkers P, Darmon M, Hoste E, et al. Acute kidney injury in the critically ill: an updated review on pathophysiology and management. Intensive Care Med. 2021;47(8):835–850. doi:10.1007/s00134-021-06454-7
46. Hammond Naomi E, Zampieri Fernando G, Di Tanna Gian L, et al. Balanced crystalloids versus saline in critically ill adults — a systematic review with meta-analysis. NEJM Evid. 2022;1(2):EVIDoa2100010.
47. Rowell SE, Fair KA, Barbosa RR, et al. The impact of pre-hospital administration of lactated ringer’s solution versus normal saline in patients with traumatic brain injury. J Neurotrauma. 2016;33(11):1054–1059. doi:10.1089/neu.2014.3478
48. Hassan MH, Hassan WM, Zaini RHM, Shukeri WF, Abidin HZ, Eu CS. Balanced fluid versus saline-based fluid in post-operative severe traumatic brain injury patients: acid-base and electrolytes assessment. Malays J Med Sci. 2017;24(5):83. doi:10.21315/mjms2017.24.5.9
49. Esteban-Zubero E, García-Muro C, Alatorre-Jiménez MA. Fluid therapy and traumatic brain injury: a narrative review. Med Clin. 2023;161(1):27–32. doi:10.1016/j.medcli.2023.03.003
50. Tseng C-H, Chen -T-T, M-Y W, Chan M-C, Shih M-C, Y-K T. Resuscitation fluid types in sepsis, surgical, and trauma patients: a systematic review and sequential network meta-analyses. Crit Care. 2020;24(1):693. doi:10.1186/s13054-020-03419-y
51. Winters ME, Sherwin R, Vilke GM, Wardi G. What is the preferred resuscitation fluid for patients with severe sepsis and septic shock? J Emerg Med. 2017;928. doi:10.1016/j.jemermed.2017.08.093
52. Chowdhury AH, Cox EF, Francis ST, Lobo DN. A randomized, controlled, double-blind crossover study on the effects of 2-L infusions of 0.9% saline and plasma-lyte® 148 on renal blood flow velocity and renal cortical tissue perfusion in healthy volunteers. Ann Surg. 2012;256(1):18–24. doi:10.1097/SLA.0b013e318256be72
53. Chowdhury AH, Cox EF, Francis ST, Lobo DN. A randomized, controlled, double-blind crossover study on the effects of 1-L infusions of 6% hydroxyethyl starch suspended in 0.9% saline (voluven) and a balanced solution (Plasma Volume Redibag) on blood volume, renal blood flow velocity, and renal cortical tissue perfusion in healthy volunteers. Ann Surg. 2014;259(5):881–887. doi:10.1097/SLA.0000000000000324
54. Pfortmueller CA, Funk GC, Reiterer C, et al. Normal saline versus a balanced crystalloid for goal-directed perioperative fluid therapy in major abdominal surgery: a double-blind randomised controlled study. Br J Anaesth. 2018;120(2):274–283. doi:10.1016/j.bja.2017.11.088
55. Shaw AD, Bagshaw SM, Goldstein SL, et al. Major complications, mortality, and resource utilization after open abdominal surgery: 0.9% saline compared to Plasma-Lyte. Ann Surg. 2012;255(5):821–829. doi:10.1097/SLA.0b013e31825074f5
56. Ayebale ET, Kwizera A, Mijumbi C, Kizito S, Roche AM. Ringer’s lactate versus normal saline in urgent cesarean delivery in a resource-limited setting: a pragmatic clinical trial. Anesth Analg. 2017;125(2):533–539. doi:10.1213/ANE.0000000000002229
57. Vincent J-L. Steroids in sepsis: another swing of the pendulum in our clinical trials. Crit Care. 2008;12(2):1–2. doi:10.1186/cc6861
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Efficacy and Safety of Acupuncture for Tinnitus-Associated Insomnia: A Protocol for a Systematic Review and Meta-Analysis
Fan L, Gao Y, Zhou J, Hu H, Gao H
Journal of Pain Research 2022, 15:2957-2965
Published Date: 21 September 2022
A Systematic Review and Meta-Analysis Protocol on How Best to Use Non-Pharmacologic Therapies to Manage Chronic Low Back Pain and Associated Depression
Guo Y, Ma Q, Zhou X, Yang J, He K, Shen L, Zhao C, Chen Z, Tan CIC, Chen J
Journal of Pain Research 2022, 15:3509-3521
Published Date: 4 November 2022
Tezepelumab for Patients with Severe Uncontrolled Asthma: A Systematic Review and Meta-Analysis
Zoumot Z, Al Busaidi N, Tashkandi W, Aljohaney AA, Isse S, Vidyasagar K, Ukwaja KN
Journal of Asthma and Allergy 2022, 15:1665-1679
Published Date: 18 November 2022
Clinical Utility of Deucravacitinib for the Management of Moderate to Severe Plaque Psoriasis
Jin JQ, Spencer RK, Reddy V, Bhutani T, Liao W
Therapeutics and Clinical Risk Management 2023, 19:413-423
Published Date: 18 May 2023
The Analgesic Effect and Potential Mechanisms of Acupuncture for Migraine Rats: A Systematic Review and Meta-Analysis
Sun S, Liu L, Zhou M, Liu Y, Sun M, Zhao L
Journal of Pain Research 2023, 16:2525-2542
Published Date: 24 July 2023