Back to Journals » Cancer Management and Research » Volume 18

A Predictive Model for Postoperative Metastasis in Gastric Cancer Based on Preoperative Inflammatory Markers: A Retrospective Cohort Study from Western China
Authors Chen M, Yilihamu A, Zhang B ![]()
Received 4 December 2025
Accepted for publication 1 March 2026
Published 9 March 2026 Volume 2026:18 582615
DOI https://doi.org/10.2147/CMAR.S582615
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Alessandro Rizzo
Mengjie Chen, Ailifeila Yilihamu, Bing Zhang
Anesthesia and Perioperative Center, The Affiliated Cancer Hospital of Xinjiang Medical University (Third Clinical Medical College of Xinjiang Medical University), Urumqi, 830011, People’s Republic of China
Correspondence: Bing Zhang, Email [email protected]
Background & Objective: Postoperative metastasis is the predominant cause of poor long-term survival in gastric cancer (GC), where the systemic inflammatory response plays a pivotal role. Most existing predictive models are derived from general populations, and their applicability to specific ethnic and high-risk cohorts, such as the multi-ethnic population in Western China, remains unverified. This study aimed to develop a preoperative predictive model for postoperative metastasis specifically for this population by investigating the predictive value of novel preoperative inflammatory and metabolic markers: the Systemic Immune-Inflammation Index (SII), Uric Acid-to-Albumin Ratio (UAR), and Urea-to-Hemoglobin Ratio (UHR).
Methods: Clinicopathological data from 656 GC patients who underwent surgery at Xinjiang Cancer Hospital between January 2018 and December 2023 were retrospectively collected. Based on the occurrence of postoperative metastasis, a 1:1 propensity score matching (matching factors: age, gender, BMI) was performed, resulting in 328 matched pairs (metastasis group vs non-metastasis group). Multivariable logistic regression analysis was used to identify independent predictors of postoperative metastasis, and a nomogram prediction model was constructed. The model’s discrimination, calibration, and stability were internally validated using the area under the receiver operating characteristic curve (AUC), the Hosmer–Lemeshow test, and the Bootstrap method (1000 replicates).
Results: Multivariable analysis identified SII (Q3 vs Q1: OR=1.80, P=0.009; Q4 vs Q1: OR=1.64, P=0.040), UHR (Q2 vs Q1: OR=1.84, P=0.025), T stage (T2 vs T1: OR=3.32, P< 0.001), and N stage (N2 vs N1: OR=1.73, P=0.004) as independent risk factors for postoperative metastasis. Conversely, UAR (Q2 vs Q1: OR=0.44, P=0.015) was identified as a protective factor. The nomogram prediction model demonstrated a training set AUC of 0.684 and a bootstrap-corrected AUC of 0.669 upon internal validation. The model showed good calibration (Hosmer–Lemeshow test P=0.142). At the optimal cutoff value (0.417), the model’s sensitivity was 88.1%, and the negative predictive value was 77.5%.
Conclusion: This study successfully developed and validated a predictive model for postoperative metastasis in gastric cancer that integrates preoperative inflammatory markers (SII, UAR, UHR) and clinicopathological features (T stage, N stage) for the unique multi-ethnic population of Western China. The model exhibits good calibration and moderate discrimination, is particularly effective at identifying patients with low metastatic risk (high sensitivity), and serves as a useful auxiliary tool for individualized preoperative risk assessment and clinical decision support in this region.
Keywords: gastric cancer, postoperative metastasis, inflammatory markers, predictive model, nomogram, Western China
Introduction
Gastric cancer (GC) is one of the most common malignant tumors worldwide. It has high morbidity and mortality rates, which seriously threaten human health.1 According to the latest cancer statistics, more than 1 million new cases and 769,000 deaths from gastric cancer occur each year. Gastric cancer is the fifth most common cancer and the fourth leading cause of cancer death in the world.1 Advances in surgical techniques, such as laparoscopic, minimally invasive, and robotic surgery, and the use of comprehensive treatment strategies, including neoadjuvant chemotherapy, adjuvant chemoradiotherapy, and targeted therapy, have significantly improved outcomes in operable gastric cancer. However, postoperative metastasis remains the leading cause of treatment failure and patient death.2 About 30% to 40% of patients undergoing radical surgery eventually develop local recurrence or distant metastasis. The most common sites are the liver, peritoneum, and distant lymph nodes.2 It is critical to accurately identify gastric cancer patients at high risk of metastasis before or soon after surgery. This allows for individualized adjuvant therapy, choice of treatment regimen type (such as aggressive chemotherapy or targeted/immunotherapy), and determination of close follow-up strategies. These decisions are directly related to patient quality of life and long-term survival.
In recent years, increasing evidence has demonstrated that a systemic inflammatory response is a key landmark feature of tumors, playing an indispensable role in tumor occurrence, development, invasion, and metastasis.3 Tumor-associated inflammation can promote metastasis through various mechanisms, including the promotion of angiogenesis, enhancement of the invasive ability of tumor cells, disruption of immune surveillance, and the creation of conditions for the formation of a pre-metastatic microenvironment.3 A variety of inflammatory markers derived from routine peripheral blood examinations have become key indicators in tumor prognosis research due to their low cost, high repeatability, and easy accessibility. The neutrophil-lymphocyte ratio (NLR), platelet-lymphocyte ratio (PLR), and systemic immune-inflammatory index (SII) are significantly correlated with the prognosis of various solid tumors, including gastric cancer, liver cancer, and colorectal cancer, in numerous studies.4,5 Among them, SII integrates the information of neutrophils, platelets, and lymphocytes, which is thought to reflect the host’s anti-tumor immune status and pro-tumor inflammatory environment more comprehensively.
In addition, some indicators reflecting nutritional and metabolic status are also closely related to the survival outcome of tumor patients. Serum albumin is a key indicator of nutritional status and negative regulation of systemic inflammation, and hypoalbuminemia is associated with poor survival in cancer patients.6 As an endogenous antioxidant, the uric acid level may reflect the ability of the body to cope with oxidative stress. Therefore, the uric acid/albumin ratio (UAR) may reflect oxidative stress and nutritional immunity. Similarly, urea nitrogen levels correlated with protein metabolism and nitrogen load, hemoglobin levels directly reflected anemia status, and cancer anemia correlated with tumor hypoxia microenvironment and worse prognosis. Thus, the urea/hemoglobin ratio (UHR) may be a composite indicator of both metabolic load and anemia status.7
However, despite the potential of each of these indicators, the combination of them, especially SII, UAR, and UHR, and the integration of traditional clinicopathological factors to construct a practical model specifically for predicting the risk of metastasis after gastric cancer surgery, remains to be explored. Most predictive models rely on postoperative pathological information, which limits their immediate application value in the preoperative decision-making stage.
Notably, the vast and geographically diverse Western China, particularly Xinjiang, harbors a unique multi-ethnic population with distinct genetic backgrounds and dietary habits 18 Epidemiological studies have suggested significant variations in GC incidence and clinical outcomes across different regions of China, with Western areas often facing heavier disease burdens and unique clinicopathological profiles.1–9 However, there is a conspicuous lack of high-quality, tailored prognostic research focusing on this specific population. Most existing models are built upon data from Eastern or Central Chinese cohorts, and their generalizability to Western Chinese patients is uncertain, as prediction models often suffer from performance degradation when applied to new, diverse populations.10 Therefore, developing a population-specific predictive tool is crucial for optimizing local clinical practice and addressing regional health disparities.
Therefore, this study aims to systematically evaluate the relationship between new inflammatory metabolic indicators, such as preoperative SII, UAR, and UHR, and postoperative metastasis of gastric cancer in a Western Chinese cohort, and integrate TNM staging and other classical factors to construct a simple, intuitive, and applicable nomographic prediction model before operation.
Although the value of the above inflammatory and nutritional indicators in tumor prognosis has been confirmed, there are obvious gaps in existing studies: firstly, most predictive models are highly dependent on postoperative pathological information and cannot provide effective guidance at this critical decision-making time point before surgery; secondly, related studies mostly focus on traditional inflammation ratios such as NLR and PLR, and there is no systematic evaluation of the predictive power of the combination of SII, UAR and UHR, especially their comprehensive value at the preoperative baseline level; Finally, UAR and UHR, as new composite markers reflecting oxidative stress and nutrient metabolism balance, their specific roles and mechanisms in gastric cancer metastasis are still unclear. Therefore, to fill these gaps, this study aims to systematically construct and validate, for the first time, a nomographic model integrating preoperative SII, UAR, UHR, and clinicopathological features through a large retrospective cohort study from Western China. The core innovation of this study lies in: 1. Develop a practical tool based solely on preoperative information to achieve true preoperative risk stratification for the understudied Western Chinese population. 2. To explore the independent value of UAR and UHR in predicting gastric cancer metastasis in this specific cohort. 3. Not only rigorous internal verification, but also exploratory verification of potential biological mechanisms of core indicators (UAR) through bioinformatics analysis and in vitro experiments, in an effort to advance statistical association to causal inference.
Materials and Methods
Study Subjects
This study was conducted in accordance with the Helsinki Decree and was approved by the Ethics Committee of the Third Clinical Medical College (Affiliated Cancer Hospital) of Xinjiang Medical University.
We retrospectively collected consecutive cases undergoing radical gastrectomy at the Gastrointestinal Surgery Department of Xinjiang Cancer Hospital between January 2018 and December 2023, and a total of 756 patient records were obtained from initial screening. Inclusion criteria for the study included: (1) primary gastric adenocarcinoma confirmed by postoperative histopathology; (2) radical resection of R0 for cure (standard subtotal gastrectomy or total gastrectomy + D2 lymph node dissection); (3) complete laboratory test results such as blood routine, liver and kidney function and blood lipids within 1 week before operation; (4) complete and traceable clinical pathological data (including detailed TNM staging) and postoperative follow-up data. Exclusion criteria were: (1) death during perioperative period (within 30 days after surgery); (2) presence of other primary malignancies or metastatic gastric cancer; (3) presence of acute infection, active inflammatory disease, hematological disease, or autoimmune disease, which may significantly affect the levels of inflammatory markers; and (4) absence of clinical data or loss to follow-up. Based on the criteria described above, 656 patients were eventually included in the primary analysis. Patients were divided into the metastasis group and the non-metastasis group according to whether metastasis occurred by imaging examination (such as CT, MRI, PET-CT) or pathology (including local recurrence and distant metastasis) during postoperative follow-up. To control for potential confounding bias from baseline data such as age, sex, BMI, etc, we used the 1:1 nearest neighbor method for propensity score matching, and the caliper value was set to 0.02 of the log standard deviation of the propensity score. Matching factors included age, sex, and body mass index (BMI). Finally, 328 pairs of patients (656 in total) were successfully matched and included in the final model construction and analysis.
Research Methods and Observation Indices
Basic information (age, gender, BMI), preoperative laboratory test indicators (blood routine, liver function, renal function, blood lipids, etc), and postoperative pathological characteristics (T stage, N stage) were collected. Inflammation indicators were calculated according to the formula:
Systemic Immune Inflammation Index (SII)= Platelet count × Neutrophils count/Lymphocytes count
Uric acid/albumin ratio (UAR)= uric acid (μmol/L)/albumin (g/L)
Urea/hemoglobin ratio (UHR)= urea (mmol/L)/hemoglobin (g/L)
In order to deal with the nonlinear relationship of continuous variables and facilitate clinical interpretation, all inflammatory indicators (SII, UAR, UHR) were divided into four grades according to their distribution in the whole cohort according to quartiles: Q1 (≤P25), Q2 (P25-P50), Q3 (P50-P75), and Q4 (≥P75).
Statistical Method
Statistical analysis was performed using R 4.5.0 software. Continuous variables with skewed distribution were expressed as median (interquartile range)[M (Q1, Q3)], and group comparisons were performed using the Mann–Whitney U-test; categorical variables were expressed as number (percentage)[n (%)], and group comparisons were performed using the chi-square test. Variables with P<0.05 in univariate analysis and clinically significant variables were included in multivariate Logistic regression analysis to screen independent predictors of postoperative metastasis and calculate odds ratio (OR) and 95% confidence interval (CI).
Based on the results of multivariate analysis, a nomogram model for predicting postoperative metastasis was constructed. Receiver operating characteristic curve (ROC) and area under the curve (AUC) were used to assess the discrimination of the model. The optimistically corrected AUC was calculated by internal validation with 1000 repeated samples using the Bootstrap method. The Hosmer-Lemeshow test and calibration curve were used to assess model calibration. The optimal probability cutoff value is determined by the Youden index, and the classification performance indexes such as accuracy, sensitivity, and specificity are calculated under this cutoff value. P<0.05 was statistically significant.
Results
Comparison of Baseline Data
After propensity score matching, 328 patients were enrolled in each of the metastatic and non-metastatic groups. As shown in Table 1, there was no significant difference in baseline data, such as age, gender, and BMI, between the two groups after matching (P>0.05), indicating that propensity score matching effectively balanced these potential confounding factors, and the matching effect was good.
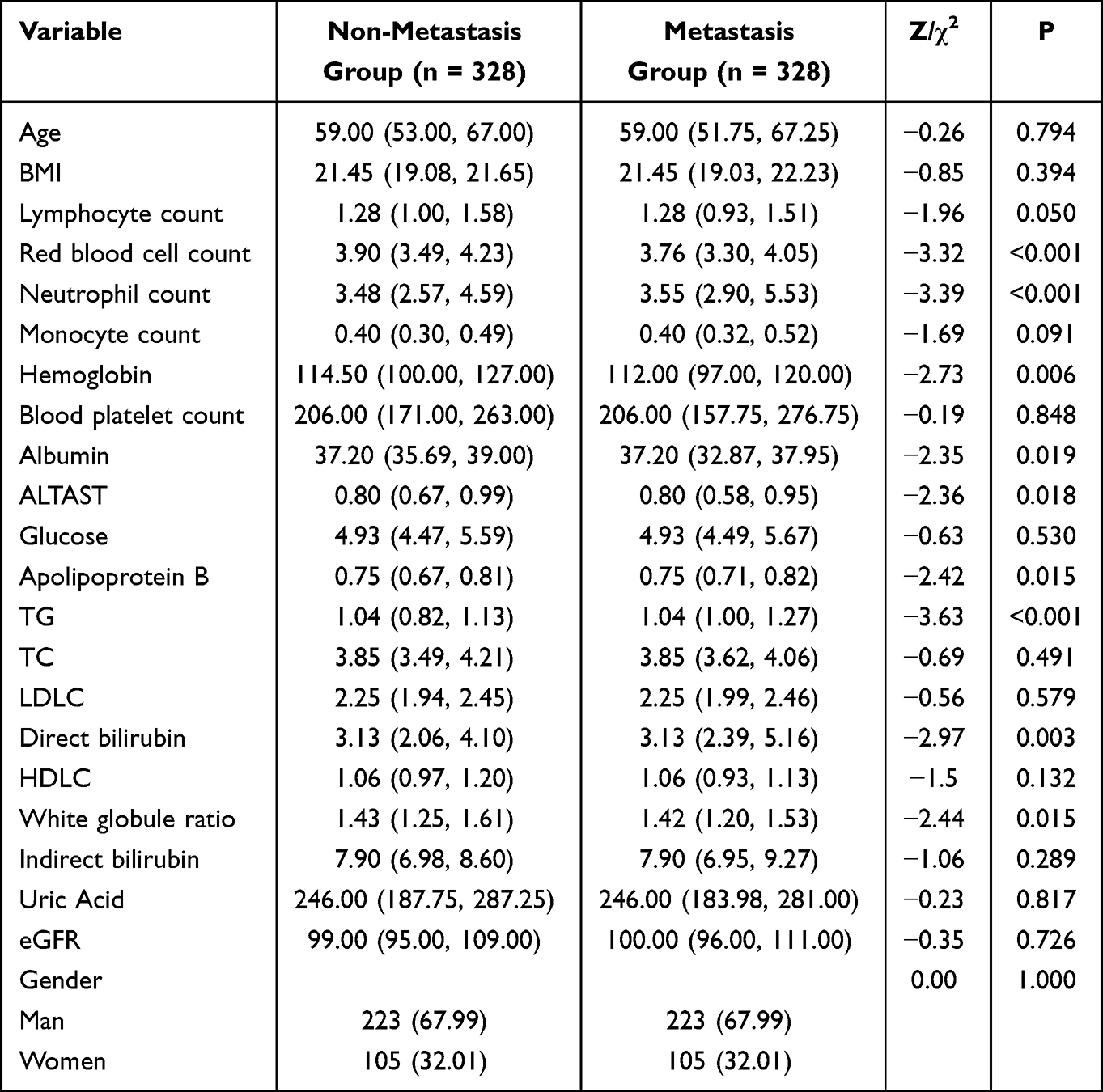 |
Table 1 Comparison of Baseline Data and Clinical Characteristics Among Tumor Metastasis Groups |
Univariate analysis showed significant differences in several laboratory parameters and pathological characteristics between metastatic and nonmetastatic patients. Red blood cell count, hemoglobin, and albumin levels were significantly lower in the metastatic group (P<0.05), which may reflect cancerous anemia and malnutrition prevalent in metastatic patients. Neutrophil count, ALT/AST ratio, apolipoprotein B, triglyceride (TG), and direct bilirubin levels were significantly higher (P<0.05), and the leukocyte ratio was significantly lower (P = 0.015) in patients with metastasis. These differences suggest that systemic inflammatory response, liver function, and lipid metabolism disorders may be associated with tumor metastasis. In terms of pathological characteristics (Table 2), the proportion of T3-T4 stage (88.72% vs 67.38%, P<0.001) and N2-N3 stage (35.37% vs 19.82%, P<0.001) in patients with metastasis was significantly higher than that in patients with non-metastasis, which is consistent with classical oncology cognition that tumor invasion depth and lymph node metastasis are the strongest predictors of distant metastasis. There was no significant difference in postoperative chemotherapy ratio between the two groups (P=0.440). See Tables 1 and 2 for specific results.
 |
Table 2 Comparison of Clinicopathological Features Among Tumor Metastasis Groups |
Distribution of Inflammatory Markers Between Groups
As shown in Table 3, although there was no difference in lymphocyte and platelet counts between the two groups after matching, there was a significant difference in the distribution of the comprehensive index SII between the two groups (χ2 = 14.93, P = 0.002). Patients in the metastatic group were more distributed in the higher quartiles of SII (Q3 and Q4), while patients in the non-metastatic group were more distributed in the lower quartile (Q1). This suggests that high preoperative SII levels are significantly associated with an increased risk of metastasis after surgery. There was no statistically significant difference in the overall distribution of UAR and UHR between the two groups (P > 0.05). However, their trend distribution plots (Figure 1) show that UARs present a complex distribution with high ends and low middle in the metastatic group, while UHRs show a trend of increasing risk with increasing quantiles in the metastatic group, which may explain why their specific quantiles show independent predictive value in multivariate analysis after controlling for other variables. The trend distribution of inflammatory markers is shown in Figure 1.
 |
Table 3 Intergroup Differences in Clinical Outcomes of Inflammatory Markers |
 |
Figure 1 Distribution trend of inflammatory markers. |
Multivariate Logistic Regression Analysis and Prediction Model Construction
Significant variables from univariate analysis were included in the multivariate Logistic regression model, and the results are shown in Table 4. SII was identified as an independent risk factor for postoperative metastasis. Patients in the Q3 and Q4 groups had an 80% and 64% increased risk of metastasis, respectively, compared with the SII-Q1 group (reference group). UAR showed a non-linear trend of protection. Compared with UAR-Q1, patients in Q2 had a significantly reduced risk of metastasis by 56% and in Q3 by 40%. UHR was an independent risk factor, and patients in Q2 and Q3 had an increased risk of metastasis by 84% and 72%, respectively, compared with UHR-Q1. Among clinicopathological factors, T stage and N stage were still strong predictors. Patients in stage T2 had a 232% increased risk of metastasis compared with stage T1. Compared with stage N1, stage N2 patients had a 73% increased risk of metastasis. Chemotherapy did not show independent predictive value in this model (P=0.235). Based on the above six independent predictors available preoperatively (SII, UAR, UHR, T stage, N stage), we constructed a nomogram model to predict the risk of metastasis after gastric cancer surgery (Figure 2). The nomogram visually shows the scores corresponding to different levels of each variable. The total score of all variable scores can be added to find the corresponding individualized transition probability on the risk axis.
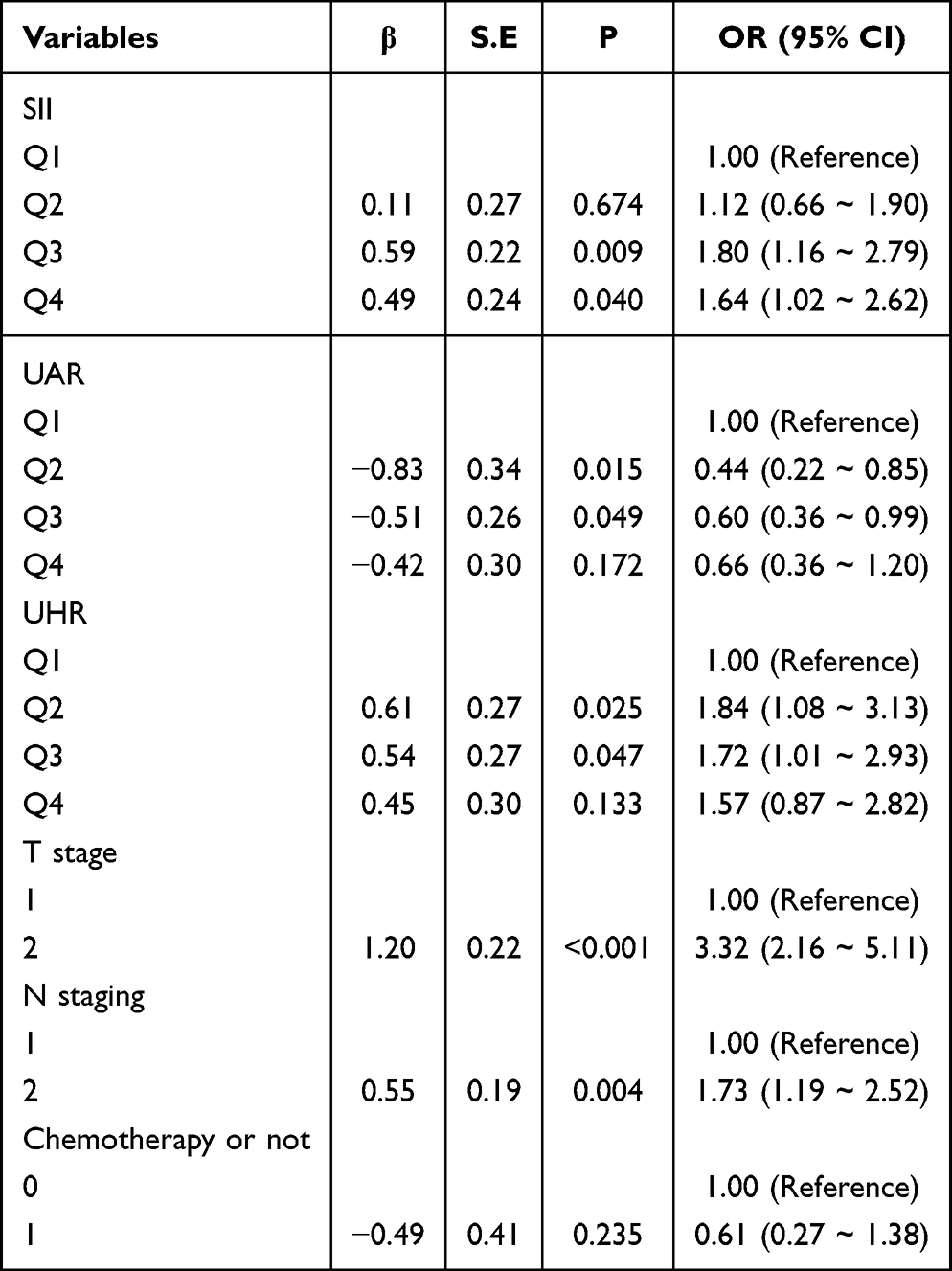 |
Table 4 Multivariate Logistic Analysis of Postoperative Metastasis |
 |
Figure 2 Nomogram for predicting postoperative metastasis risk in gastric cancer. |
Model Performance Evaluation
The ROC curve of the predictive model in the training set is shown in Figure 3, with an AUC of 0.684 (95% CI: 0.651–0.717), indicating that the model has a moderate degree of discrimination. After internal validation of the Bootstrap method with 1000 repeated samples, the calculated optimistic corrected AUC is 0.669, which is very close to the AUC of the training set, indicating that the overfitting degree of the model is slight and the stability is good. The Hosmer-Lemeshow goodness of fit test showed P=0.142, which was not statistically significant, indicating that there was no significant deviation between the predicted probability of the model and the actual observed probability. The calibration curve (Figure 4) also clearly shows that the prediction curve fits closely to the 45-degree diagonal representing perfect prediction, with mean absolute errors as low as 0.025, further confirming the excellent calibration of the model.
 |
Figure 3 ROC curve of the predictive model. |
 |
Figure 4 Calibration curve of the model. |
Model Classification Performance
In clinical application, we determined the optimal probability cutoff value of 0.417 through the Youden index. The classification performance of the model at this cutoff is shown in Table 5. The sensitivity of the model was as high as 88.1% and the negative predictive value was 77.5%. This means that the model is very effective in identifying patients with a very low risk of metastasis after surgery, with a low rate of missed diagnosis. Although the specificity was relatively low (40.9%), resulting in some false positives, the overall accuracy was 64.5%. The prediction probability distribution plot (Figure 5) visually illustrates the discriminative effect of the model: the prediction probability of patients in the non-metastatic group is more concentrated on the left side (low probability region), while the prediction probability of patients in the metastatic group is more distributed to the right side (high probability region). Although there is overlap between the two, the model does distinguish patients with different risks to some extent.
 |
Table 5 Classification Performance |
 |
Figure 5 Distribution of prediction probabilities in metastasis and non-metastasis groups. |
Discussion
Based on real data from a single large cancer center in Western China, this study successfully developed and internally validated the first preoperative nomogram for predicting postoperative metastasis of gastric cancer specifically for this unique multi-ethnic population. The core strength of the model lies in its preoperative availability and convenience, as all predictive variables (SII, UAR, UHR, T stage, N stage) are available preoperatively through routine blood tests and imaging/biopsy assessments, allowing clinicians to quantify risk stratification of patients before making surgical and postoperative adjuvant treatment strategies.
The results of this study reconfirm the critical role of systemic inflammatory response in the progression of gastric cancer. SII, as a composite index integrating neutrophils, platelets, and lymphocytes, has been proven to be an independent risk factor for postoperative metastasis, which is consistent with Hu et al’s study in liver cancer and previous reports in gastric cancer4,5. The biological mechanism may be that neutrophils promote tumor cell invasion and angiogenesis by secreting matrix metalloproteinases (MMPs) and vascular endothelial growth factor (VEGF); platelets can help tumor cells escape immune clearance and promote microthrombosis by wrapping them; and the decrease of lymphocytes (especially cytotoxic T cells and NK cells) means the weakening of anti-tumor immune response.3 High SII is the embodiment of this imbalance between “pro-tumor inflammation” and “anti-tumor immunosuppression”.
One of the findings of this study is the potential protective effect of UAR. Contrary to conventional wisdom, our results show that patients in the median quartile (Q2, Q3) of UAR have a significantly lower risk of metastasis than those in the Q1 group. This may be due to uric acid’s dual role: in cells, it is a potent antioxidant capable of scavenging free radicals and may inhibit oxidative stress-driven tumor progression to some extent.8 Albumin is not only an important nutritional index, but also a negative acute phase protein that maintains the inflammatory homeostasis of the body. Therefore, a moderate UAR value may represent a good balance between antioxidant reserves and nutritional status. Too low (Q1) may indicate insufficient antioxidant capacity, and too high (Q4) may indicate metabolic disorders associated with hyperuricemia, whose net effect may be beneficial to tumors. This nonlinear relationship reveals the complexity of UAR as a biomarker and deserves to be explored in future studies by measuring oxidative stress markers.
As a risk factor, UHR may reflect both nitrogen metabolic load and anemia status. Higher urea nitrogen levels may be associated with a high metabolic state or slightly impaired renal function, while lower hemoglobin (resulting in elevated UHR), ie, cancerous anemia, is closely associated with the hypoxic microenvironment of the tumor. Hypoxia induces HIF-1α expression, which in turn upregulates a range of genes that promote epithelial-mesenchymal transition (EMT), angiogenesis, and metastasis.9 Thus, UHR cleverly integrates metabolism and hypoxia, two key dimensions associated with malignant behavior.
In terms of model performance, the AUC value of 0.684 is at a moderately acceptable level for predictive models based on conventional clinical parameters and comparable to many similar studies.11 In particular, it is worth emphasizing that the model exhibits extremely high sensitivity (88.1%) and satisfactory negative predictive value (77.5%). This property makes it an excellent “exclusion tool” with great potential in clinical practice. That is, if the model predicts that a patient is at low risk (probability <0.417), then there is a high probability that he will not metastasize. This helps clinicians to be more confident in adopting relatively conservative adjuvant treatment strategies or relaxing follow-up intervals for these low-risk patients, thereby avoiding overtreatment, saving medical resources, and improving patient quality of life. A relatively low specificity means there are false positives, where some patients with low risk are misjudged as high risk. Therefore, this model is more suitable for screening and identification of high-risk patients, and its positive results should be regarded as a warning signal, suggesting that a comprehensive judgment should be made in combination with other clinical information, or more active intervention measures should be taken.
Compared with the existing literature, our model innovatively integrates SII, UAR, and UHR, three indicators with different pathophysiological connotations, providing a more comprehensive perspective on preoperative risk assessment. Although studies have explored the role of NLR, PLR, or CONUT nutritional indices in the prognosis of gastric cancer,7–9 few studies have included and verified the value of UAR and UHR in predicting metastasis, and none have done so specifically in a Western Chinese cohort, addressing the need for population-specific tools.10
Clinical Implications and Future Directions
The nomogram we developed holds immediate potential for clinical translation within its context. Its primary strength lies in its preoperative applicability, allowing clinicians in Western China to perform quantitative risk stratification before finalizing surgical and adjuvant therapy plans. For patients identified as low-risk (predicted probability below the 0.417 cutoff), clinicians can confidently consider less aggressive adjuvant therapy or extended follow-up intervals, thereby avoiding overtreatment, reducing patient burden, and optimizing regional healthcare resources. Conversely, high-risk predictions should serve as an alert for more vigilant surveillance, intensive adjuvant regimens, or eligibility assessment for clinical trials. Thus, this tool facilitates a shift towards more precise and personalized management of gastric cancer in this region.
Future research should focus on externally validating this model in multi-center cohorts across Western China and incorporating dynamic changes in inflammatory markers. Furthermore, the intriguing non-linear relationship of UAR warrants investigation into its underlying biological mechanisms, potentially through correlative studies with oxidative stress markers in this specific population.
Study Limitations
There are several limitations to this study:
1. Retrospective design: inherent selection bias and information bias cannot be completely avoided. Although we used PSM to balance known confounders, unknown or unmeasured confounders may still be present.
2. Single-center data: All patients come from the same hospital in Western China, and their population characteristics and diagnosis and treatment specifications may have certain particularity, which, while a strength for local applicability, limits the extrapolation of the model to other regions. The model needs validation with external data from other centers in Western China and beyond.
3. Fluctuation of inflammatory indicators: Preoperative inflammatory indicators may be affected by transient factors (such as stress and latent infection). We only used measurements at a single time point and failed to observe their dynamic changes.
4. Missing molecular information: HER2, MMR, PD-L1, and other important molecular markers are not included in the model, which is increasingly important for accurate treatment and prognosis of modern gastric cancer.
Conclusion
In conclusion, a nomogram model integrating preoperative inflammatory markers (SII, UAR, UHR) and clinicopathological features (T stage, N stage) for predicting postoperative metastasis of gastric cancer was successfully constructed and internally validated in this Western Chinese cohort. The model has good calibration and high sensitivity, especially good at identifying patients with a low risk of postoperative metastasis. As an intuitive and practical quantitative tool, this nomogram is expected to assist clinicians in Xinjiang and broader Western China in individualized preoperative risk assessment, optimize treatment decisions and follow-up strategies, and ultimately promote regional precision medical practice for gastric cancer.
Ethics Approval
This study was conducted in accordance with the Helsinki Decree and was approved by the Ethics Committee of the Third Clinical Medical College (Affiliated Cancer Hospital) of Xinjiang Medical University.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Disclosure
The authors have no relevant financial or non-financial interests to disclose.
References
1. Sung H, Ferlay J, Siegel RL. et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–12. doi:10.3322/caac.21660
2. Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2018 (5th edition). Gastric Cancer. 2021;24(1):1–21. doi:10.1007/s10120-020-01042-y
3. Grivennikov SI, Greten FR, Karin M. Immunity, inflammation, and cancer. Cell. 2010;140(6):883–899. doi:10.1016/j.cell.2010.01.025
4. Hu B, Yang XR, Xu Y, et al. Systemic immune-inflammation index predicts prognosis of patients after curative resection for hepatocellular carcinoma. Clin Cancer Res. 2014;20(23):6212–6222. doi:10.1158/1078-0432.CCR-14-0442
5. Geng Y, Zhu D, Wu C, et al. A novel systemic inflammation response index (SIRI) for predicting the survival of patients with pancreatic cancer after chemotherapy. Cancer. 2016;122(14):2158–2167. doi:10.1002/cncr.30057
6. Gupta D, Lis CG. Pretreatment serum albumin as a predictor of cancer survival: a systematic review of the epidemiological literature. Nutr J. 2010;9:69. doi:10.1186/1475-2891-9-69
7. Sun KY, Xu JB, Chen SL, et al. Novel immunological and nutritional-based prognostic index for gastric cancer. World J Gastroenterol. 2015;21(19):5961–5971. doi:10.3748/wjg.v21.i19.5961
8. Sakurai K, Tamura T, Toyokawa T, et al. Low preoperative prognostic nutritional index predicts poor survival Post-gastrectomy in elderly patients with gastric cancer. Ann Surg Oncol. 2016;23(11):3669–3676. doi:10.1245/s10434-016-5272-6
9. Chen W, Zheng R, Baade PD, et al. Cancer statistics in China, 2015. CA Cancer J Clin. 2016;66(2):115–132. doi:10.3322/caac.21338
10. Moazzen S, van der Sloot KWJ, Vonk RJ, de Bock GH, Alizadeh BZ. Diet Quality and Upper Gastrointestinal Cancers Risk: A Meta-Analysis and Critical Assessment of Evidence Quality. Nutrients. 2020;12(6):1863. doi:10.3390/nu12061863
11. Han M, Ma L, Qu Y, Tang Y. Decreased expression of the ATM gene linked to poor prognosis for gastric cancer of different nationalities in Xinjiang. Pathol Res Pract. 2017;213(8):908–914. doi:10.1016/j.prp.2017.05.012
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Development and Validation of a Predictive Nomogram with Age and Laboratory Findings for Severe COVID-19 in Hunan Province, China
Jiang J, Zhong W, Huang W, Gao Y, He Y, Li X, Liu Z, Zhou H, Fu Y, Liu R, Zhang W
Therapeutics and Clinical Risk Management 2022, 18:579-591
Published Date: 17 May 2022
Establishment and Validation of a Model for Disease-Free Survival Rate Prediction Using the Combination of microRNA-381 and Clinical Indicators in Patients with Breast Cancer
Shen J, Wang M, Li F, Yan H, Wang R, Zhou J
Breast Cancer: Targets and Therapy 2022, 14:375-389
Published Date: 30 November 2022
A Visualized Mortality Prediction Score Model in Hematological Malignancies Patients with Carbapenem-Resistant Organisms Bloodstream Infection
Qian C, Wu Q, Ruan Z, Liu F, Li W, Shi W, Ma L, Peng D, Yin H, Yao L, Li Z, Hong M, Xia L
Infection and Drug Resistance 2023, 16:201-215
Published Date: 7 January 2023
Nomogram Based on Preoperative Fibrinogen and Systemic Immune-Inflammation Index Predicting Recurrence and Prognosis of Patients with Borrmann Type III Advanced Gastric Cancer
Wang H, Yin X, Ma K, Wang Y, Fang T, Zhang Y, Xue Y
Journal of Inflammation Research 2023, 16:1059-1075
Published Date: 12 March 2023
Prognostic Model of D2 Radical Gastrectomy Combined with Neoadjuvant Chemotherapy for Gastric Cancer
Wang G, Tan Y, Jiang Y, Liu J, Su Y, Sun Z, Liu B
Risk Management and Healthcare Policy 2023, 16:1259-1271
Published Date: 10 July 2023