Back to Journals » Journal of Inflammation Research » Volume 18
A Multicenter Study of Systemic Inflammatory Biomarkers for Prognostic Evaluation in iCCA Patients
Authors Tao Y, Xu B, Tang J, Ji S, Li J
Received 3 July 2025
Accepted for publication 6 November 2025
Published 11 November 2025 Volume 2025:18 Pages 15787—15800
DOI https://doi.org/10.2147/JIR.S551284
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Felix Marsh-Wakefield
Yun Tao,1 Benjie Xu,2 Jie Tang,1 Shengjun Ji,3 Jie Li1
1Department of Intervention, Affiliated Hospital of Jiangnan University, Wuxi, Jiangsu, People’s Republic of China; 2Department of Outpatient Chemotherapy, Harbin Medical University Cancer Hospital, Harbin, Heilongjiang, People’s Republic of China; 3Department of Radiotherapy and Oncology, Suzhou Municipal Hospital, The Affiliated Suzhou Hospital of Nanjing Medical University, Gusu School, Nanjing Medical University, Suzhou, Jiangsu, People’s Republic of China
Correspondence: Jie Li, Department of Intervention, Affiliated Hospital of Jiangnan University, Wuxi, Jiangsu, 214000, People’s Republic of China, Email [email protected] Shengjun Ji, Department of Radiation and Oncology, Suzhou Municipal Hospital, The Affiliated Suzhou Hospital of Nanjing Medical University, Gusu School, Nanjing Medical University, No. 16 West Baita Road, Suzhou, 215001, People’s Republic of China, Email [email protected]
Background: The prognostic value of systemic inflammatory biomarkers in intrahepatic cholangiocarcinoma (iCCA) remains uncertain. This study aimed to compare their predictive performance and identify the most effective indicator.
Methods: We retrospectively analyzed 312 iCCA patients who underwent curative resection at three medical centers (2014– 2022). Twelve systemic inflammatory biomarkers, derived from routine blood parameters (neutrophils, lymphocytes, monocytes, platelets, albumin), were assessed for overall survival (OS) and disease-free survival (DFS). Prognostic accuracy was evaluated using the concordance index (C-index), time-dependent area under the ROC curve (time-AUC), and Brier score. Independent predictors identified by multivariate Cox regression were incorporated into nomograms to estimate survival.
Results: The median patient age was 63 years, 71.8% were male, 38.8% had stage III disease, and 37.5% had poorly differentiated tumors. Median follow-up was 24 months. Among the twelve biomarkers, the pan-immune-inflammation value (PIV) demonstrated the strongest prognostic performance. For OS, PIV achieved a C-index of 0.682, time-AUC of 0.695, and Brier score of 0.180; for DFS, C-index was 0.679, time-AUC 0.681, and Brier score 0.192. Unlike single-ratio indices, PIV integrates neutrophil, monocyte, platelet, and lymphocyte counts, providing a multidimensional view of systemic inflammation and immunity. Multivariate analysis confirmed high PIV as an independent predictor of poor OS (HR = 2.488; 95% CI: 1.745– 3.546; P < 0.001) and DFS (HR = 2.353; 95% CI: 1.701– 3.247; P < 0.001). Nomograms combining PIV with clinicopathological factors (CEA, CA19-9, perineural invasion, TNM stage) demonstrated improved discrimination and calibration at 12, 36, and 60 months.
Conclusion: PIV provides superior prognostic value compared with traditional inflammatory indices, offering a cost-effective and readily available biomarker for iCCA. While promising, these results are based on a retrospective multicenter cohort without independent validation, and should be confirmed in prospective external studies.
Keywords: intrahepatic cholangiocarcinoma, inflammation, biomarker, prognosis
Introduction
Cholangiocarcinomas (CCAs) are a rare but aggressive group of malignancies, anatomically classified as intrahepatic (iCCA) or extrahepatic (eCCA), with iCCA arising proximal to the second-order bile ducts.1,2 iCCA differs significantly from eCCA in molecular characteristics and clinical management.3 Although uncommon, iCCA has been recognized as an increasing oncologic concern due to its rising incidence and poor prognosis.4,5 These challenges underscore the need for improved prognostic strategies.
The tumor-node-metastasis (TNM) staging system remains the cornerstone of prognostic evaluation, but its discriminatory ability is limited, particularly for patients with localized disease. In recent years, increasing evidence has underscored the association between preoperative systemic inflammatory responses and clinical outcomes in iCCA.6 A variety of serum-derived biomarkers, including the neutrophil-to-lymphocyte ratio (NLR),7–10 lymphocyte-to-monocyte ratio (LMR),11–19 platelet-to-lymphocyte ratio (PLR),11–14,18–20 systemic immune-inflammation index (SII),21,22 systemic inflammation response index (SIRI),23 and systemic inflammation score (SIS),17 have been reported as prognostic indicators. Composite scores such as the Naples prognostic score24 and the advanced lung cancer inflammation index25 have also been explored. Notably, patients with advanced iCCA and evidence of systemic inflammation tend to exhibit more aggressive tumor biology and higher recurrence rates.26
However, prior studies remain inconsistent. Many biomarkers are easy to calculate but capture only a single dimension of the host immune or inflammatory response, and their prognostic utility varies across reports. For instance, ratios such as NLR and PLR are widely adopted but susceptible to confounding by infection or hepatic dysfunction, while composite indices like SII and SIRI offer broader integration yet lack standardization and external validation. Moreover, most studies have focused on one biomarker at a time, leaving their relative prognostic strengths poorly defined.
Comparative studies that systematically evaluate multiple inflammatory biomarkers in the same iCCA population are scarce. Such investigations are clinically meaningful, as they may help identify the most reliable biomarkers, improve risk stratification, and guide postoperative surveillance strategies. Moreover, the identification of an optimal biomarker could directly influence clinical decision-making, including refining patient selection for curative surgery, tailoring adjuvant therapy recommendations, and determining the intensity of follow-up schedules. Therefore, this multicenter study aimed to comprehensively compare the prognostic performance of twelve preoperative systemic inflammatory biomarkers in patients with iCCA undergoing curative resection, using robust statistical metrics such as the concordance index (C-index), time-dependent AUC, and Brier scores.
Materials and Methods
Patients Selection
This retrospective study evaluated patients with iCCA who underwent curative surgical resection between April 2014 and January 2022 at The Affiliated Hospital of Jiangnan University, The Affiliated Suzhou Hospital of Nanjing Medical University, and Harbin Medical University Cancer Hospital. Inclusion criteria were: (1) histologically confirmed iCCA; (2) curative-intent resection; (3) no evidence of extrahepatic metastasis at the time of surgery; and (4) complete baseline laboratory data. Exclusion criteria included: (1) receipt of any preoperative therapy, such as transarterial chemoembolization, radiofrequency ablation, or systemic treatment; (2) history of hematologic malignancy, autoimmune disease, or other cancers; and (3) incomplete clinical, laboratory, or follow-up records. A total of 312 patients met the eligibility criteria and were included in the final analysis (Figure S1).
Tumor staging was based on the 8th edition of the American Joint Committee on Cancer (AJCC) system. Postoperative follow-up was scheduled every 3 months for the first 2 years, every 6 months for years 3–5, and annually thereafter. Each follow-up visit included physical examination, laboratory tests (including liver function and tumor markers such as CEA and CA19-9), and imaging assessment with abdominal ultrasonography or contrast-enhanced CT/MRI. For patients unable to attend in person, structured telephone interviews were conducted to confirm survival status and disease recurrence. Follow-up was continued through January 2025. All participants provided written informed consent. The study was conducted in accordance with the Declaration of Helsinki and approved by the institutional review boards of the participating hospitals.
Data Collection and Definition of Variables
This study collected demographic and tumor-related variables, including age, gender, presence of obstructive jaundice, hepatitis B virus (HBV) infection status, serum carcinoembryonic antigen (CEA) and carbohydrate antigen 19–9 (CA19-9) levels, tumor differentiation, perineural invasion, and tumor staging according to the 8th edition of the American Joint Committee on Cancer (AJCC) TNM classification. Preoperative hematological parameters included peripheral counts of lymphocytes, neutrophils, monocytes, and platelets, as well as serum albumin levels. A total of 12 systemic immune-inflammation biomarkers were evaluated: pan-immune-inflammation value (PIV), NLR, LMR, PLR, SII, SIRI, neutrophil-to-albumin ratio (NAR), lymphocyte × albumin (LA), neutrophil × monocyte (NM), neutrophil × platelet (NP), monocyte × platelet (MP), and SIS. The formulas used to calculate these biomarkers are detailed in Table S1. The selection of the 12 systemic inflammatory biomarkers was based on both established evidence and exploratory consideration. Classical ratios such as NLR, LMR, PLR, SII, SIRI, and SIS were included given their frequent use and reported prognostic significance in hepatobiliary and gastrointestinal malignancies. Additionally, emerging composite indices such as PIV, NAR, LA, NM, NP, and MP were incorporated based on previous evidence in other cancer types, enabling a comprehensive comparison of traditional and novel inflammatory markers in iCCA. Overall survival (OS) was defined as the interval from the date of curative surgery to death or last follow-up. Disease-free survival (DFS) was defined as the time from curative surgery to either documented disease recurrence or the most recent follow-up.
Evaluation Metrics for Inflammatory Biomarkers
Multiple metrics were utilized to evaluate the prognostic performance of the twelve systemic inflammation biomarkers. Discriminative ability was assessed using Harrell’s concordance index (C-index) and the time-dependent area under the receiver operating characteristic curve (time-AUC), with higher values indicating better discriminatory power. Calibration was assessed using the time-dependent Brier score (time-Brier score), which ranges from 0 to 1, with lower scores reflecting better model calibration.
Development and Assessment of Nomogram
Independent risk factors for OS and DFS in iCCA were identified using univariate Cox regression analysis, followed by multivariate inverse stepwise Cox regression. A clinical model was constructed based on independent predictors of OS and DFS, excluding PIV. Nomogram models were then developed by incorporating PIV along with other independent prognostic factors to estimate OS and DFS. The predictive performance of the models was evaluated using time-dependent ROC survival curves, calibration plots, and decision curve analysis (DCA). Comparative prognostic accuracy among the nomogram, clinical model, and TNM staging system was assessed using net reclassification improvement (NRI) and integrated discrimination improvement (IDI) metrics.
Statistical Analysis
Continuous variables were tested for normality using the Kolmogorov–Smirnov test and reported as mean ± standard deviation (SD) or median with interquartile range (IQR), as appropriate. Group comparisons were conducted using the Student’s t-test or Mann–Whitney U-test for continuous variables, and the Chi-square test or Fisher’s exact test for categorical variables. Prognostic factors were first evaluated by univariate Cox regression analysis, with variables showing a p value < 0.05 subsequently included in a multivariate Cox regression using an inverse stepwise selection approach. To avoid collinearity among systemic inflammatory biomarkers, variance inflation factor values were calculated for all candidate variables prior to Cox regression modeling. Variables with VIF ≥ 5 were considered to indicate multicollinearity and would have been excluded; however, in this study, all included variables demonstrated VIF < 2.0, confirming no significant collinearity. All variables in this study were complete, with no missing data; therefore, imputation procedures were not required. All statistical analyses were performed using R software (version 4.2.1), and a two-sided P < 0.05 was considered statistically significant.
Results
Patient Characteristics
This multicenter study included 312 patients who underwent radical surgical resection for iCCA. The median age of the patients was 63 years (range: 31–79 years), with 88 (28.21%) females and 224 (71.79%) males. HBV infection was observed in 14.42% of patients. The median serum levels (with IQR) of CEA and CA19-9 were 2.60 ng/mL (1.73,4.16) and 99.02 U/mL (36.19,276.80), respectively. Histological analysis revealed that 37.50% of tumors were poorly differentiated, while the remaining 62.50% were well or moderately differentiated. Perineural invasion was present in 28.85% of patients. According to the 8th edition of the AJCC staging system, 61.22% of cases were classified as stage I/II, and 38.78% as stage III. Regarding systemic inflammatory and nutritional biomarkers, the median values (with interquartile ranges) were as follows: NLR, 2.63 (1.82,3.64); LMR, 3.21 (2.10,3.84); PLR, 153.94 (108.54,211.55); SII, 588.32 (379.36,928.20); SIRI, 1.33 (0.87,2.31); NAR, 1.11 (0.84,1.55); LA, 6.01 (4.86,7.81); NM, 2.30 (1.47,3.80); NP, 1014.33 (617.33,1475.54); MP, 128.48 (80.28,191.08); SIS, 2.00 (1.00,2.00); and PIV, 312.23 (190.42,505.66) (Table 1). The median follow-up period was 24 months, ranging from 2 to 84 months. The OS rates at 12, 36, and 60 months were 71.3%, 34.2%, and 15.6%, respectively. These results indicate that although most patients survived during the first postoperative year, survival rates declined sharply thereafter, reflecting the aggressive biological behavior of iCCA and the high likelihood of recurrence or progression despite curative-intent resection.
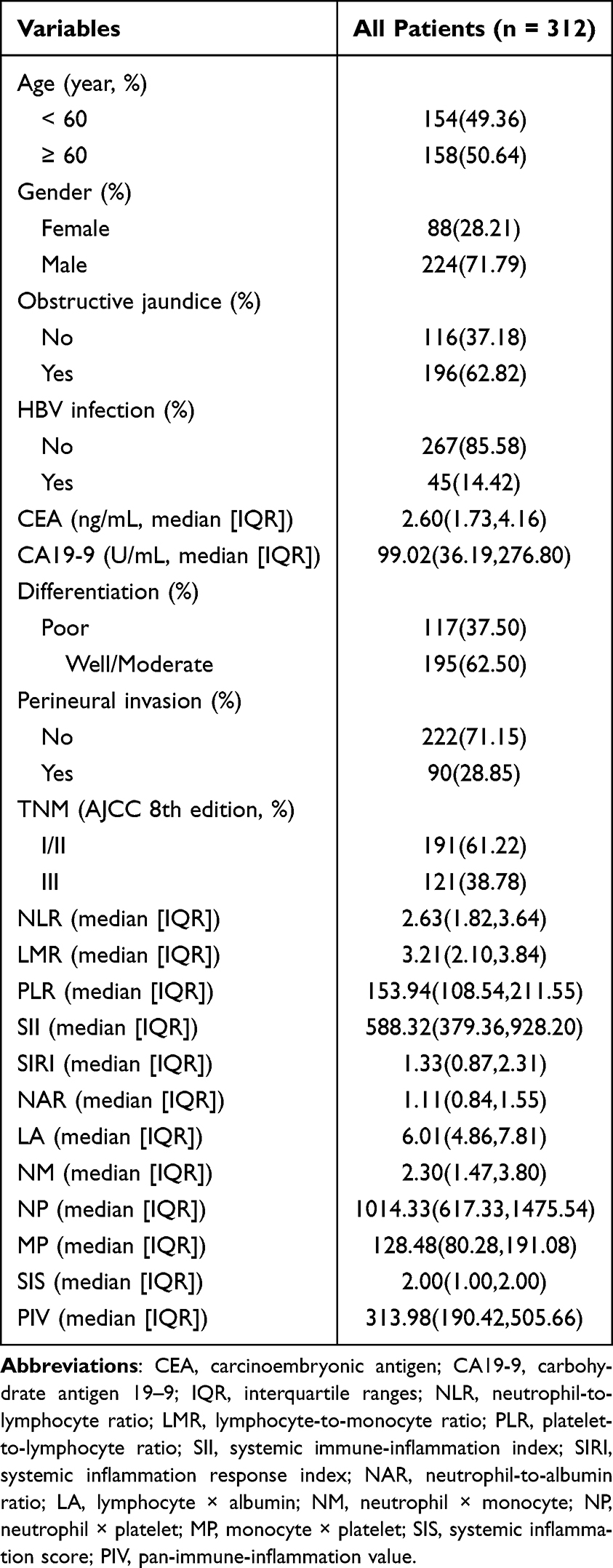 |
Table 1 Baseline Clinicopathological Characteristics of Intrahepatic Cholangiocarcinoma Patients in This Study |
Optimal Survival Prediction Inflammation Biomarkers
As shown in Figure 1 and Table 2, the prognostic performance of twelve systemic inflammatory biomarkers for OS and DFS was comprehensively evaluated. Among these biomarkers, the PIV demonstrated the best overall predictive performance. For OS, PIV yielded the highest C-index of 0.682 (95% CI: 0.637–0.727), a time-dependent AUC of 0.695 (95% CI: 0.606–0.784), and the lowest time-Brier Score of 0.180 (95% CI: 0.167–0.191). Similarly, for DFS, PIV maintained superior performance with a C-index of 0.679, time-AUC of 0.681, and a time-Brier Score of 0.192. In contrast, markers such as MP and NP exhibited lower prognostic accuracy, with MP showing the lowest C-index for OS (0.566, 95% CI: 0.517–0.615) and the highest time-Brier Score (0.192). The time-dependent AUC curves in Figure 1 further confirmed that PIV consistently maintained superior discriminatory power across 1- to 5-year time points for both OS (Figure 1A) and DFS (Figure 1B), while other biomarkers such as NLR, LMR, and PLR demonstrated moderate but inferior AUC performance.
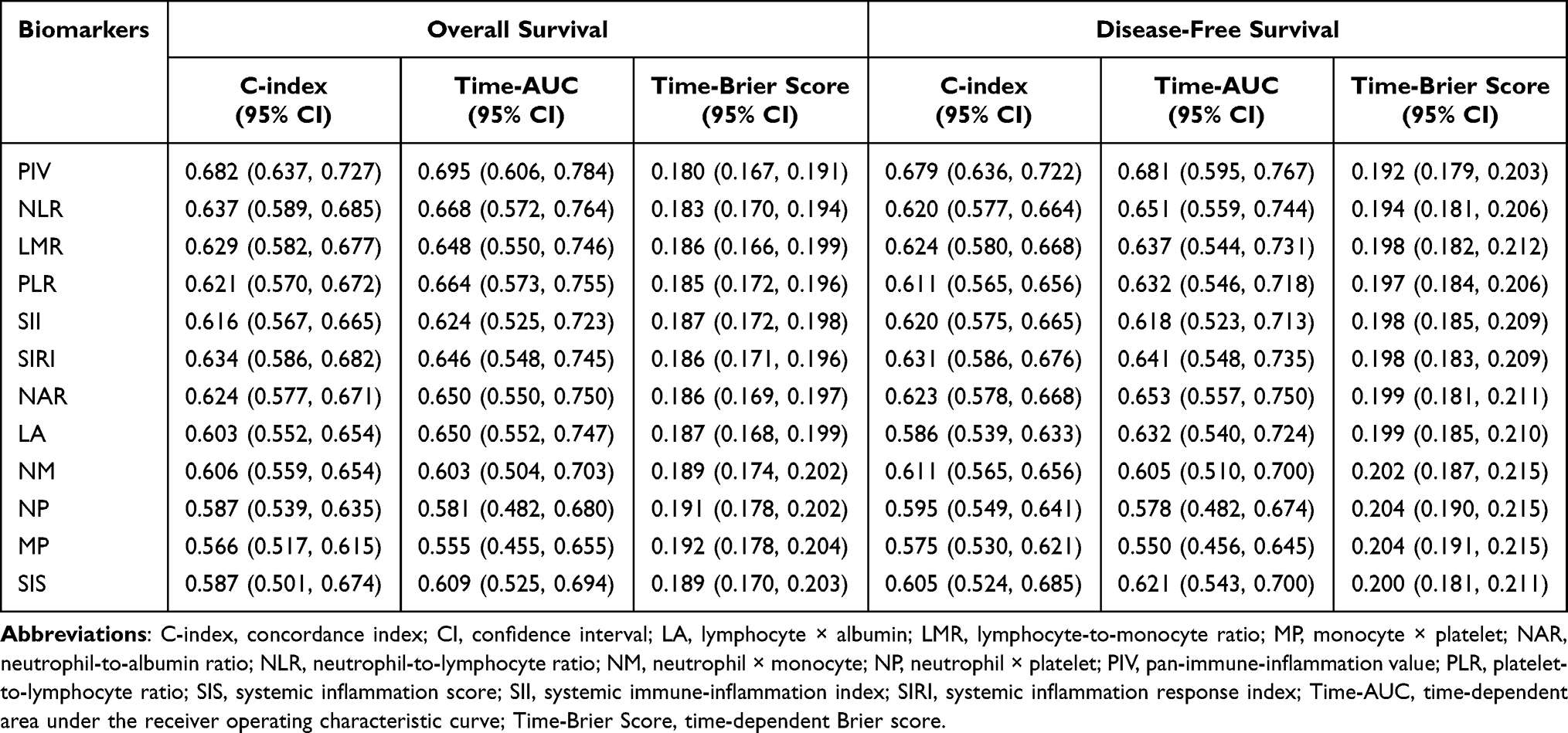 |
Table 2 Comparison of Twelve Inflammatory Biomarkers Prediction Value for Overall Survival and Disease-Free Survival |
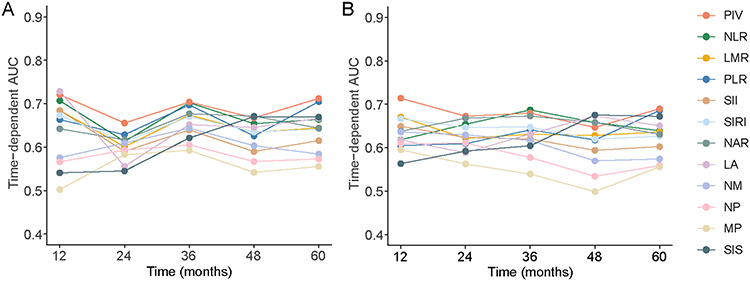 |
Figure 1 The time-dependent AUC of inflammation-based indicators for predicting overall survival (A) and disease-free survival (B) in intrahepatic cholangiocarcinoma patients. Abbreviations: AUC, area under the receiver operating characteristic curve; LA, lymphocyte × albumin; LMR, lymphocyte-to-monocyte ratio; MP, monocyte × platelet; NAR, neutrophil-to-albumin ratio; NLR, neutrophil-to-lymphocyte ratio; NM, neutrophil × monocyte; NP, neutrophil × platelet; PIV, pan-immune-inflammation value; PLR, platelet-to-lymphocyte ratio; SII, systemic immune-inflammation index; SIRI, systemic inflammation response index; SIS, systemic inflammation score. |
Characteristics and Survival Analysis of PIV
Patients were then categorized into Low PIV (< 313.98) and High PIV (≥ 313.98) groups based on the median value. As shown in Table 3, the median PIV level in the high PIV group was significantly elevated compared to the low PIV group (505.66 vs 189.96, P < 0.001). There were no significant differences in age distribution (P = 0.212), gender (P = 0.998), presence of obstructive jaundice (P = 0.911), HBV infection (P = 0.204), tumor differentiation (P = 0.642), perineural invasion (P = 0.716), or TNM stage (P = 0.253) between the two groups. However, significant differences were observed in various inflammatory and nutritional biomarkers. The high PIV group had significantly higher levels of NLR (3.40 vs 2.03), PLR (184.70 vs 116.13), SII (826.79 vs 390.71), SIRI (2.11 vs 0.97), NAR (1.31 vs 0.91), NM (3.19 vs 1.58), NP (1326.51 vs 677.43), MP (166.98 vs 91.15), and a lower LMR (2.33 vs 3.68) (all P < 0.001). LA was also significantly lower in the high PIV group (5.64 vs 6.44, P = 0.042). Notably, despite having the same median SIS value of 2.00 in both groups, the distribution difference was statistically significant (P = 0.004). No significant differences were found in CEA or CA19-9 levels between groups.
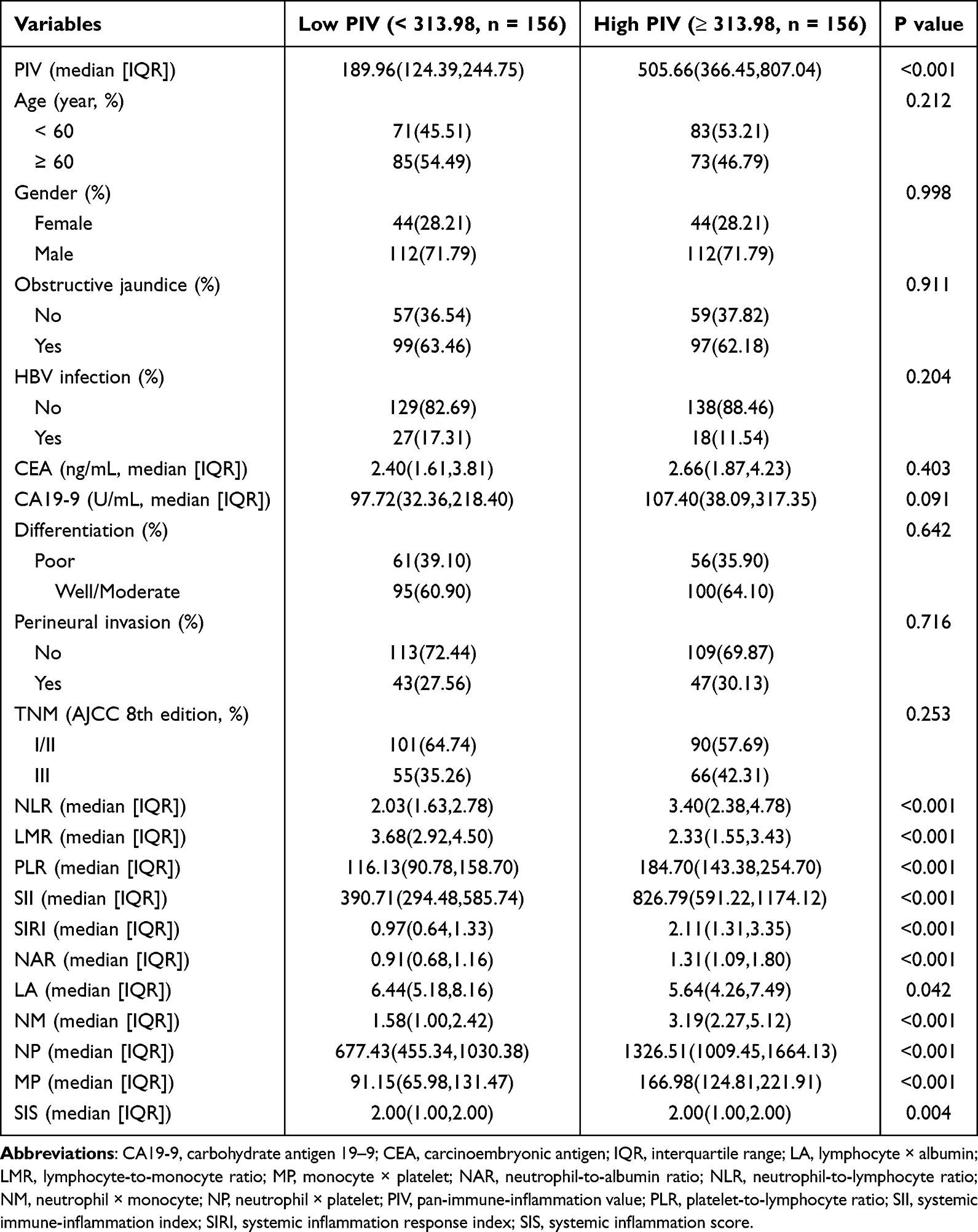 |
Table 3 Association of the PIV with Clinicopathological Characteristics in Intrahepatic Cholangiocarcinoma Patients |
Kaplan-Meier survival analysis revealed that patients with Low PIV had significantly improved OS (Figure 2A) and DFS (Figure 2B) compared to those with High PIV (all P < 0.001). Univariate and multivariate Cox regression analyses were conducted to identify independent prognostic factors for OS and DFS in patients with iCCA (Table 4). In univariate analysis, high PIV was significantly associated with worse OS (Hazard ratio [HR] = 3.077, 95% confidence interval [CI]: 2.169–4.367, P < 0.001) and DFS (HR = 2.841, 95% CI: 2.075–3.891, P < 0.001). After adjusting for other covariates in multivariate analysis, high PIV remained an independent predictor of poor OS (HR = 2.488, 95% CI: 1.745–3.546, P < 0.001) and DFS (HR = 2.353, 95% CI: 1.701–3.247, P < 0.001). Other variables that were independently associated with survival outcomes included elevated CEA (≥ 5 ng/mL) and CA19-9 (≥ 37 U/mL) levels, as well as the presence of perineural invasion. Specifically, elevated CEA was significantly associated with shorter OS (HR = 1.661, 95% CI: 1.172–2.354, P = 0.004) and DFS (HR = 1.671, 95% CI: 1.192–2.341, P = 0.003), while high CA19-9 was also linked to poor OS (HR = 1.622, P = 0.025) and DFS (HR = 1.610, P = 0.014). Perineural invasion remained a strong predictor of reduced OS (HR = 1.712, P = 0.001) and DFS (HR = 1.582, P = 0.004). Additionally, TNM stage III was independently associated with worse OS (HR = 1.462, P = 0.016), but its effect on DFS did not reach statistical significance in multivariate analysis (P = 0.095). Importantly, collinearity testing was performed by calculating variance inflation factor values for all covariates included in the Cox models. All variance inflation factor values were below 2 (Table S2), indicating no evidence of multicollinearity among the included predictors for OS and DFS.
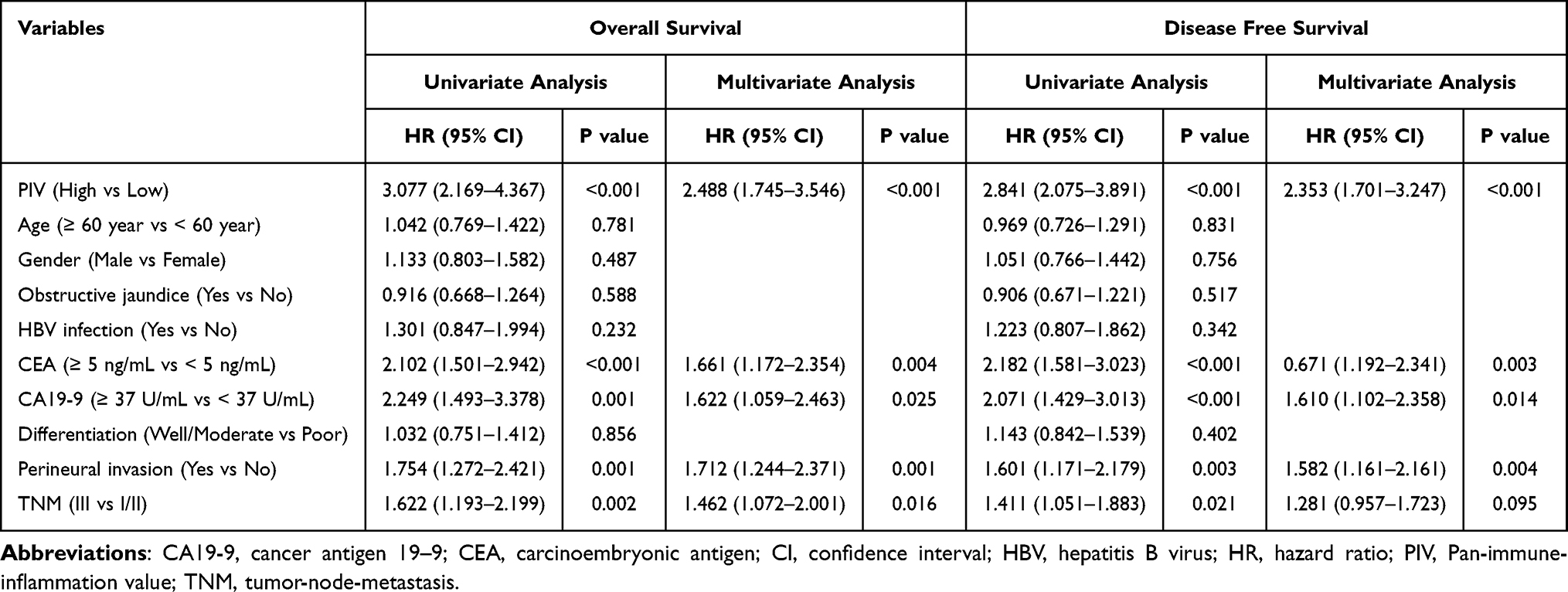 |
Table 4 Univariate and Multivariate Analyses of the Prognosis for Intrahepatic Cholangiocarcinoma |
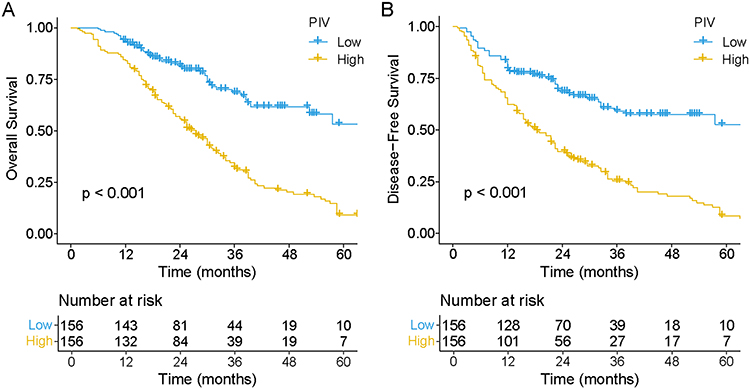 |
Figure 2 The Kaplan–Meier curves analysis of PIV for overall survival (A) and disease-free survival (B) in intrahepatic cholangiocarcinoma patients. Abbreviation: PIV, pan-immune-inflammation value. |
Across all major clinical subgroups, patients with low PIV consistently demonstrated significantly better OS and DFS compared with those with high PIV (Table S3). This prognostic advantage was independent of age, gender, HBV status, tumor markers, histological differentiation, perineural invasion, and TNM stage, underscoring the robustness of PIV as a predictor of survival in iCCA.
Development and Assessment of Nomograms
Multivariate Cox regression analysis identified PIV, CEA, CA19-9, perineural invasion, and TNM stage as independent prognostic factors for OS (Figure 3A), while PIV, CEA, CA19-9, and perineural invasion were independently associated with DFS (Figure 3B). These variables were incorporated into the construction of respective prognostic models. The nomogram models demonstrated strong predictive performance, with AUC values for OS prediction at 12, 36, and 60 months of 0.706, 0.716, and 0.762, respectively (Figure 3C), and for DFS prediction of 0.668, 0.717, and 0.734, respectively (Figure 3D). Calibration curves indicated excellent agreement between predicted and observed outcomes at 12, 36, and 60 months, confirming the models’ robust predictive accuracy for postoperative survival in patients with iCCA (Figure 4A–F).
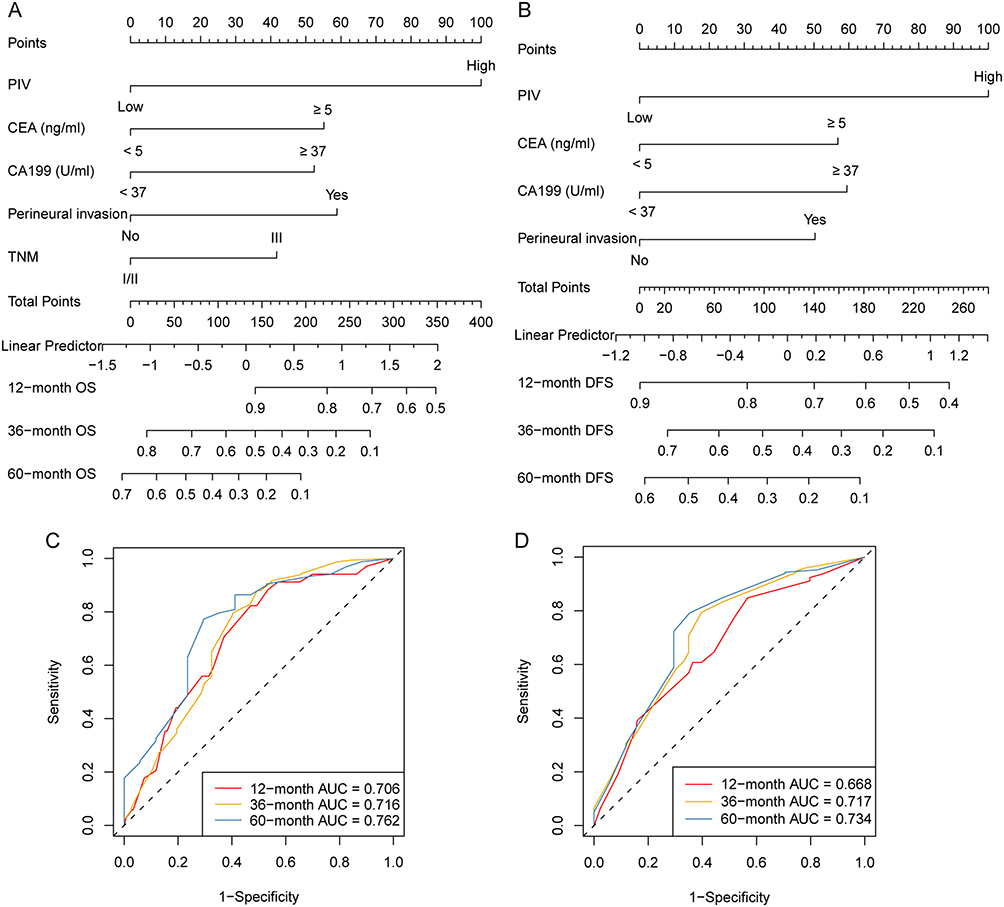 |
Figure 3 Construction of the nomograms. Nomograms incorporating the PIV and other clinicopathological parameters for predicting overall survival (A) and disease-free survival (B). ROC curves of the training set for overall survival (C) and disease-free survival (D) based on the model. Abbreviations: AUC, area under the curve; CA19-9, carbohydrate antigen 19–9; CEA, carcinoembryonic antigen; DFS, disease-free survival; OS, overall survival; PIV, pan-immune-inflammation value; ROC, receiver operating characteristic; TNM, tumor-node-metastasis. |
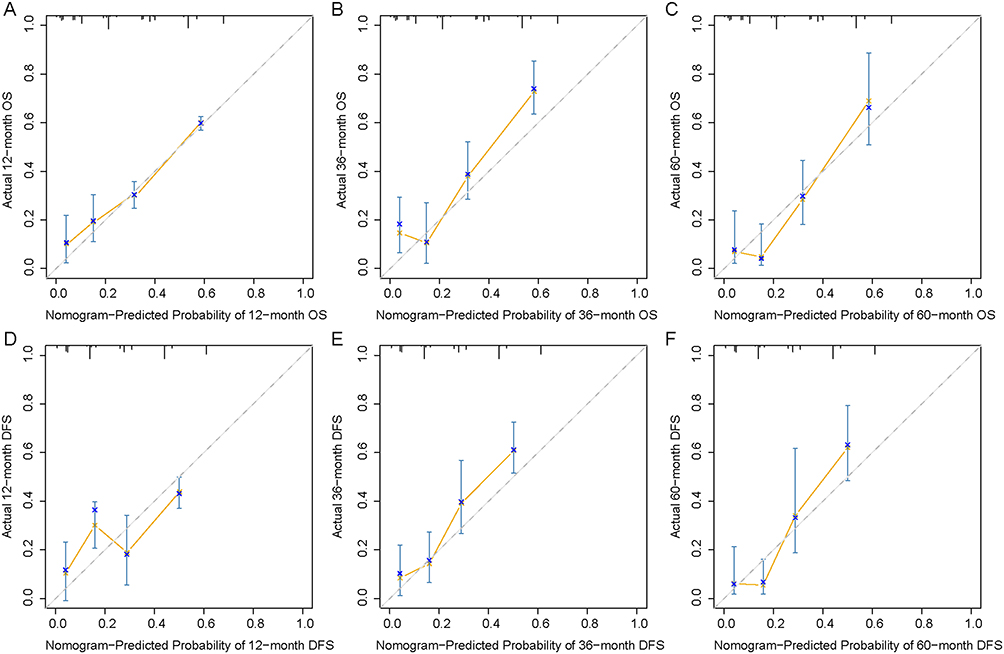 |
Figure 4 The calibration curves of the nomograms between predicted and observed 12- (A), 36- (B), and 60- (C) month OS of patients. The calibration curves of the nomograms between predicted and observed 12- (D), 36- (E), and 60- (F) month DFS of patients. Abbreviations: DFS, disease-free survival; OS, overall survival. |
Model Comparison
To evaluate the predictive performance of different prognostic models, the nomogram, TNM staging system, and clinical model were compared using C-index, IDI, and NRI metrics (Table 5). For OS, the nomogram demonstrated superior discrimination with a C-index of 0.705 (95% CI: 0.661–0.749), outperforming both the TNM system (C-index = 0.646) and the clinical model (C-index = 0.682). Compared with the clinical model, the nomogram yielded a significant IDI improvement of 0.072 (95% CI: 0.011–0.129, P = 0.003) and an NRI of 0.209 (95% CI: 0.127–0.289, P < 0.001), suggesting enhanced predictive accuracy and improved reclassification performance. In contrast, the TNM system showed inferior performance, with a significantly lower IDI (−0.052, P < 0.001) and NRI (−0.162, P < 0.001) compared to the clinical model. Similar trends were observed for DFS. The nomogram achieved the highest C-index of 0.693 (95% CI: 0.628–0.745), followed by the clinical model (0.662) and the TNM system (0.616). The nomogram showed significant improvements in IDI (0.081, P = 0.002) and NRI (0.228, P < 0.001) over the clinical model. These results suggest that the nomogram provides superior prognostic accuracy and reclassification ability for both OS and DFS compared with the TNM system and clinical model alone.
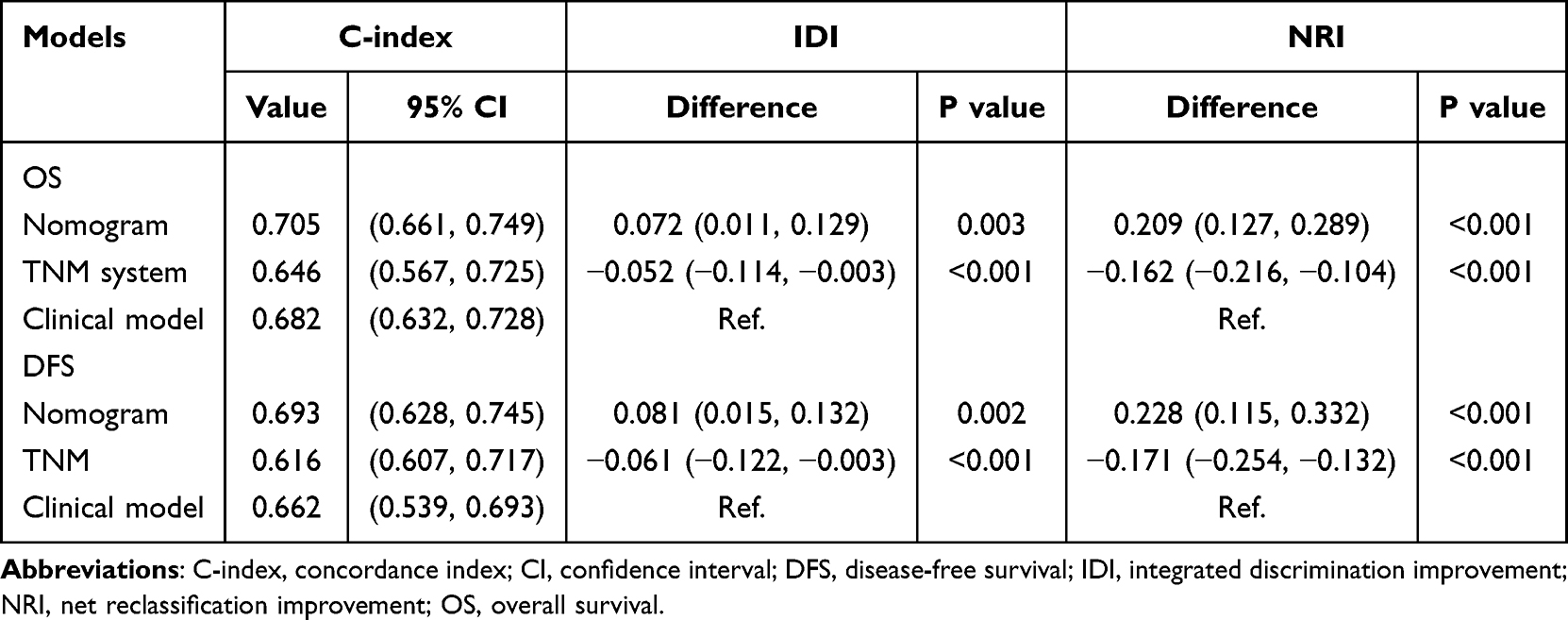 |
Table 5 The Comparison of the Predictive Value of Nomogram, TNM System and Clinical Model |
DCA was performed to assess the clinical utility of the nomogram, clinical model, and TNM staging system for predicting overall survival at 12, 36, and 60 months (Figure S2A–C), as well as disease-free survival at the same time points (Figure S2D–F). Across all time horizons, the nomogram consistently demonstrated the highest net benefit across a wide range of threshold probabilities compared to the clinical model and TNM system. In contrast, the TNM system yielded the lowest net benefit curves at nearly all threshold levels, indicating limited clinical utility when used alone. The clinical model showed moderate net benefit but was consistently outperformed by the nomogram.
Discussion
In this multicenter cohort study involving 312 patients with iCCA, we systematically compared the prognostic value of twelve preoperative systemic inflammatory biomarkers. Among them, the PIV demonstrated the highest predictive performance for both OS and DFS, with the highest C-index and lowest time-dependent Brier scores. Multivariate Cox regression confirmed high PIV as an independent risk factor for poor prognosis. Patients with high PIV levels exhibited worse survival outcomes. A prognostic nomogram incorporating PIV and other independent variables showed superior discrimination and clinical utility compared to the TNM staging system and clinical model, as evidenced by improved C-index, NRI, and IDI. Decision curve analysis further confirmed the net benefit of the nomogram across multiple time points.
Cancer-related inflammation is closely associated with tumor initiation, development, and metastasis.27 Elevated proinflammatory cytokines, including tumor necrosis factor-alpha (TNF-α), interleukin (IL)-1 and IL-6, significantly promote tumor growth by activating key intracellular signaling pathways involved in cellular proliferation and angiogenesis.28 Neutrophils play a crucial role in tumor initiation and progression by secreting reactive oxygen species, reactive nitrogen species, and matrix metalloproteinases, which collectively facilitate carcinogenesis.29 Moreover, neutrophils stimulate angiogenesis through the release of vascular endothelial growth factor A, IL-6, and transforming growth factor-beta (TGF-β).30,31 Concurrently, neutrophils mediate immunosuppression by secreting nitric oxide, arginase, and immunosuppressive cytokines, thereby impairing cytotoxic T-cell functionality.32 At metastatic sites, neutrophils further diminish CD8+ T-cell activity via inducible nitric oxide synthase and engage with regulatory B-cells to suppress natural killer cell-mediated responses.33–35 Monocytes, particularly tumor-associated macrophages (TAMs), contribute significantly to tumor progression by inducing apoptosis in anti-tumor T-cells and promoting angiogenesis through secretion of TNF-α, and IL-10.36 Increased TAM infiltration in tumor tissues correlates with poor prognosis due to their involvement in facilitating tumor cell proliferation, invasion, and immune escape mechanisms.37 Platelets are critical in promoting tumor progression and metastasis through mechanisms involving epithelial-mesenchymal transition, angiogenesis, and immune evasion.38 Platelets shield circulating tumor cells from immune recognition by forming protective thrombi. Activated platelets secrete growth factors, including TGF-β and fibroblast growth factor, further enhancing angiogenesis and metastatic potential.39 Moreover, platelets recruit neutrophils and monocytes to metastatic niches, intensifying local inflammation and facilitating distant tumor dissemination. Conversely, lymphocytes, especially cytotoxic T lymphocytes, are essential in anti-tumor immunity due to their capacity to induce tumor cell apoptosis through mechanisms involving perforin, interferon-gamma, and TNF-α.40 Elevated intratumoral lymphocyte infiltration consistently correlates with improved prognosis, underscoring their pivotal role in counteracting tumor progression and metastasis.41 Conversely, lymphopenia is persistently associated with adverse clinical outcomes, emphasizing lymphocytes’ vital function in tumor suppression.42 Peripheral blood-derived indices such as NLR, LMR, and PLR offer significant clinical advantages due to their minimal invasiveness, cost-effectiveness, and ease of monitoring through routine blood tests, effectively reflecting systemic inflammation and tumor microenvironment dynamics.7,11,20 These biomarkers have gained increasing attention in clinical oncology, overcoming limitations of traditional tissue-based markers. Integrating these indices into composite biomarkers presents a promising strategy for improving cancer prognosis and guiding personalized treatments.
The pan-immune-inflammation value (PIV), first introduced by Fucà et al in 2020, integrates neutrophil, monocyte, platelet, and lymphocyte counts into a single composite biomarker, thereby providing a multidimensional representation of the systemic inflammatory and immune status.43 By simultaneously capturing both pro-tumor (neutrophils, monocytes, platelets) and anti-tumor (lymphocytes) components, PIV enhances the accuracy of prognostic assessment compared with traditional single-dimensional indices. Previous studies have consistently demonstrated that PIV outperforms NLR, PLR, and other established inflammatory markers in predicting outcomes across several malignancies, including colorectal, breast, and lung cancers.44–48 In metastatic colorectal cancer, PIV was shown to be a superior predictor of OS and progression-free survival (PFS), surpassing NLR in multivariable models.43 Similarly, in breast cancer, PIV emerged as an independent prognostic indicator, with stronger predictive power than conventional inflammatory indices and even the TNM staging system, particularly for OS in patients with HER2-positive advanced disease undergoing first-line therapy.49 In lung cancer, a recent systematic meta-analysis further confirmed the robust prognostic utility of PIV, demonstrating that elevated PIV consistently correlated with poorer outcomes across treatment modalities such as surgery, chemoradiotherapy, and targeted therapy.48
In our current multicenter study on iCCA, PIV demonstrated superior prognostic efficacy compared to other eleven inflammatory biomarkers. Specifically, PIV yielded the highest C-index for OS and DFS, alongside time-AUC values and lowest Brier scores, underscoring its robust predictive accuracy. Multivariate Cox regression analysis further validated PIV as an independent prognostic factor for OS and DFS, with hazard ratios significantly higher for patients categorized within the high-PIV group, highlighting its strong association with adverse survival outcomes in patients undergoing curative surgery for iCCA. The nomogram model developed in our study, which incorporated PIV alongside significant clinical parameters including CEA, CA19-9, perineural invasion, and TNM staging, demonstrated enhanced prognostic accuracy compared to models relying solely on clinical factors or TNM staging. Specifically, the inclusion of PIV improved model performance as evidenced by increased IDI and NRI, thereby refining patient stratification and prognostic evaluation. Furthermore, the clinical utility of PIV was emphasized by its ease of calculation from routine blood tests, providing a non-invasive, cost-effective, and readily accessible prognostic tool suitable for dynamic longitudinal monitoring. These advantages facilitate clinical decision-making and may inform tailored therapeutic interventions aimed at improving patient outcomes. Given the biological rationale underlying PIV, reflecting complex tumor-host inflammatory interactions more comprehensively than single-dimensional biomarkers, its integration into clinical practice promises substantial enhancements in prognostic assessments and individualized patient management strategies. Exploratory subgroup analyses suggested that the prognostic utility of PIV was generally preserved across different clinical characteristics, including early- and late-stage disease, as well as among patients with or without HBV infection. This indicates that PIV may function as a robust systemic marker independent of specific clinical backgrounds. Moreover, we adopted the median value as the cut-off for PIV to ensure objectivity; however, whether this threshold is stable and generalizable across populations requires further multicenter validation.
Our study highlights several clinically meaningful implications. First, PIV can be readily calculated from routine preoperative blood tests without additional costs, making it feasible for immediate clinical use. Second, incorporating PIV into prognostic models significantly improves patient stratification beyond conventional clinicopathological factors, which may refine decisions on postoperative surveillance intensity and identify high-risk patients who could benefit from adjuvant or experimental therapies. Third, its ease of dynamic assessment suggests potential for longitudinal monitoring, though this requires further validation.
The novelty of this study lies in its comprehensive comparison of a broad panel of systemic inflammatory biomarkers in iCCA, which has not been previously performed in a multicenter cohort. The identification of PIV as the most powerful predictor highlights its potential as a practical, non-invasive, and inexpensive tool to enhance prognostic evaluation. Incorporating PIV into a nomogram with standard clinicopathological variables significantly improved prognostic discrimination, suggesting that PIV-based models may guide individualized treatment planning and follow-up strategies in clinical practice.
This study has several limitations. First, its retrospective design may introduce selection bias and limits the ability to infer causality. Retrospective studies are also prone to missing data and residual confounding, which may affect the stability of the results. Although our dataset was complete and multivariate analyses were conducted to adjust for known variables, the influence of unmeasured confounders and potential biases in patient selection or treatment allocation cannot be excluded. Second, all participating centers were located in China, which may limit the generalizability of the findings to other populations. Third, systemic inflammatory and nutritional markers were derived from a single preoperative blood test, without accounting for dynamic changes during follow-up that may provide additional prognostic insights. Last, the potential impact of postoperative adjuvant therapies (chemotherapy, targeted therapy, and immunotherapy) on systemic inflammation and survival outcomes was not systematically accounted for, as treatment strategies varied across centers and complete data were not uniformly available. This may confound the observed associations. Future prospective studies should include stratification or adjustment for adjuvant therapy to better delineate the independent prognostic role of PIV.
Conclusion
In summary, this multicenter study demonstrated that PIV is a valuable systemic inflammatory biomarker for predicting survival outcomes in patients with iCCA. Importantly, when combined with clinicopathological variables, PIV contributed to the development of a prognostic nomogram that outperformed the TNM staging system in terms of discrimination and clinical utility. These findings highlight the potential of PIV-based models to enhance individualized prognostic assessment, although prospective validation remains necessary before clinical implementation.
AI Writing Statement
No AI writing assistance was utilized in the production of this manuscript.
Abbreviations
AJCC, American Joint Committee on Cancer; AUC, Area under the receiver operating characteristic curve; CA19-9, Carbohydrate antigen 19-9; CEA, Carcinoembryonic antigen; CI, Confidence interval; DCA, Decision curve analysis; DFS, Disease-free survival; HBV, Hepatitis B virus; HR, Hazard ratio; IDI, Integrated discrimination improvement; IQR, Interquartile range; LA, Lymphocyte × albumin; LMR, Lymphocyte-to-monocyte ratio; MP, Monocyte × platelet; NAR, Neutrophil-to-albumin ratio; NLR, Neutrophil-to-lymphocyte ratio; NM, Neutrophil × monocyte; NP, Neutrophil × platelet; NRI, Net reclassification improvement; OS, Overall survival; PFS, Progression-free survival; PIV, Pan-immune-inflammation value; PLR, Platelet-to-lymphocyte ratio; ROC, Receiver operating characteristic; SD, Standard deviation; SII, Systemic immune-inflammation index; SIRI, Systemic inflammation response index; SIS, Systemic inflammation score; TNM, Tumor-node-metastasis.
Data Sharing Statement
The data that support the findings of this study are available on reasonable request from the corresponding author.
Ethics Statement
The studies involving human participants were reviewed and approved by The Ethics Committee of The Affiliated Hospital of Jiangnan University, The Affiliated Suzhou Hospital of Nanjing Medical University, and Harbin Medical University Cancer Hospital. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Health Commission Science and Technology Project of Wuxi City (M202321), Clinical Research and Translational Medicine Project of the Affiliated Hospital of Jiangnan University (CYJ202324).
Disclosure
The authors report no potential conflicts of interest in this work.
References
1. Kendall T, Verheij J, Gaudio E, et al. Anatomical, histomorphological and molecular classification of cholangiocarcinoma. Liver Int. 2019;39(Suppl 1):7–18. doi:10.1111/liv.14093
2. European Association for the Study of the Liver. EASL-ILCA clinical practice guidelines on the management of intrahepatic cholangiocarcinoma. J Hepatol. 2023;79(2):181–208. doi:10.1016/j.jhep.2023.03.010
3. Moris D, Palta M, Kim C, Allen PJ, Morse MA, Lidsky ME. Advances in the treatment of intrahepatic cholangiocarcinoma: an overview of the current and future therapeutic landscape for clinicians. CA Cancer J Clin. 2023;73(3):198–222. doi:10.3322/caac.21759
4. Javle M, Lee S, Azad NS, et al. Temporal changes in cholangiocarcinoma incidence and mortality in the United States from 2001 to 2017. Oncologist. 2022;27(11):874–883. doi:10.1093/oncolo/oyac150
5. Storandt MH, Tella SH, Wieczorek MA, et al. Projected incidence of hepatobiliary cancers and trends based on age, race, and gender in the United States. Cancers. 2024;16(3):684. doi:10.3390/cancers16040684
6. Cui H, Li Y, Li S, Liu G. Prognostic utility of preoperative inflammatory markers in patients with intrahepatic cholangiocarcinoma after hepatic resection: a systematic review and meta-analysis. Cancer Med. 2023;12(1):99–110. doi:10.1002/cam4.4935
7. Brustia R, Langella S, Kawai T, et al. Preoperative risk score for prediction of long-term outcomes after hepatectomy for intrahepatic cholangiocarcinoma: report of a collaborative, international-based, external validation study. Eur J Surg Oncol. 2020;46(4 Pt A):560–571. doi:10.1016/j.ejso.2019.10.041
8. Lin G, Liu Y, Li S, et al. Elevated neutrophil-to-lymphocyte ratio is an independent poor prognostic factor in patients with intrahepatic cholangiocarcinoma. Oncotarget. 2016;7(32):50963–50971. doi:10.18632/oncotarget.7680
9. Sasaki K, Margonis GA, Andreatos N, et al. Preoperative risk score and prediction of long-term outcomes after hepatectomy for intrahepatic cholangiocarcinoma. J Am Coll Surg. 2018;226(3):393–403. doi:10.1016/j.jamcollsurg.2017.12.011
10. Watanabe A, Harimoto N, Araki K, et al. Absolute neutrophil count predicts postoperative prognosis in mass-forming intrahepatic cholangiocarcinoma. Anticancer Res. 2019;39(2):941–947. doi:10.21873/anticanres.13197
11. Chen Q, Dai Z, Yin D, et al. Negative impact of preoperative platelet-lymphocyte ratio on outcome after hepatic resection for intrahepatic cholangiocarcinoma. Medicine. 2015;94(32):e574. doi:10.1097/MD.0000000000000574
12. Lin J, Fang T, Zhu M, et al. Comparative performance of inflammation-based prognostic scores in patients operated for intrahepatic cholangiocarcinoma. Cancer Manag Res. 2019;11:9107–9119. doi:10.2147/CMAR.S198959
13. Ma B, Meng H, Shen A, et al. Prognostic value of inflammatory and tumour markers in small-duct subtype intrahepatic cholangiocarcinoma after curative-intent resection. Gastroenterol Res Pract. 2021;2021:6616062. doi:10.1155/2021/6616062
14. Ohira M, Yoshizumi T, Yugawa K, et al. Association of inflammatory biomarkers with long-term outcomes after curative surgery for mass-forming intrahepatic cholangiocarcinoma. Surg Today. 2020;50(4):379–388. doi:10.1007/s00595-019-01905-7
15. Wang JJ, Li H, Li JX, Xu L, Wu H, Zeng Y. Preoperative gamma-glutamyltransferase to lymphocyte ratio predicts long-term outcomes in intrahepatic cholangiocarcinoma patients following hepatic resection. World J Gastroenterol. 2020;26(13):1501–1512. doi:10.3748/wjg.v26.i13.1501
16. Wu Y, Ren F, Chai Y, et al. Prognostic value of inflammation-based indexes for intrahepatic cholangiocarcinoma following curative resection. Oncol Lett. 2019;17(1):165–174. doi:10.3892/ol.2018.9618
17. Zhang Y, Shi SM, Yang H, et al. Systemic inflammation score predicts survival in patients with intrahepatic cholangiocarcinoma undergoing curative resection. J Cancer. 2019;10(2):494–503. doi:10.7150/jca.26890
18. Zhang Z, Zhou Y, Hu K, Huang Y. Investigating effects of preoperative inflammatory biomarkers on predicting survival outcomes of intrahepatic cholangiocarcinoma after curative resection. World J Surg Oncol. 2020;18(1):272. doi:10.1186/s12957-020-02053-w
19. Zhao J, Chen Y, Wang J, et al. Preoperative risk grade predicts the long-term prognosis of intrahepatic cholangiocarcinoma: a retrospective cohort analysis. BMC Surg. 2021;21(1):113. doi:10.1186/s12893-020-00954-x
20. Tsilimigras DI, Moris D, Mehta R, et al. The systemic immune-inflammation index predicts prognosis in intrahepatic cholangiocarcinoma: an international multi-institutional analysis. HPB. 2020;22(12):1667–1674. doi:10.1016/j.hpb.2020.03.011
21. Ren A, Li Z, Cheng P, Zhang X, Deng R, Ma Y. Systemic immune-inflammation index is a prognostic predictor in patients with intrahepatic cholangiocarcinoma undergoing liver transplantation. Mediators Inflamm. 2021;2021:6656996. doi:10.1155/2021/6656996
22. Li H, Wang JJ, Zhang M, et al. Prognostic significance of systemic immune-inflammation index in patients with intrahepatic cholangiocarcinoma undergoing hepatic resection. World J Gastrointest Oncol. 2020;12(5):467–482. doi:10.4251/wjgo.v12.i4.467
23. Jin B, Hu W, Su S, et al. The prognostic value of systemic inflammation response index in cholangiocarcinoma patients. Cancer Manag Res. 2021;13:6263–6277. doi:10.2147/CMAR.S317954
24. Du CF, Gao ZY, Xu ZD, et al. Prognostic value of the Naples prognostic score in patients with intrahepatic cholangiocarcinoma after hepatectomy. BMC Cancer. 2024;24(1):727. doi:10.1186/s12885-024-12502-4
25. Catalano G, Alaimo L, Chatzipanagiotou OP, et al. Prognostic value of the advanced lung cancer inflammation index in intrahepatic cholangiocarcinoma. Eur J Surg Oncol. 2024;50(6):108773. doi:10.1016/j.ejso.2024.108773
26. Maßmann M, Treckmann J, Markus P, et al. A prognostic systemic inflammation score (SIS) in patients with advanced intrahepatic cholangiocarcinoma. J Cancer Res Clin Oncol. 2023;149(16):5085–5094. doi:10.1007/s00432-022-04424-0
27. Rossi S, Basso M, Strippoli A, et al. Are markers of systemic inflammation good prognostic indicators in colorectal cancer? Clin Colorectal Cancer. 2017;16(4):264–274. doi:10.1016/j.clcc.2017.03.015
28. Pine JK, Morris E, Hutchins GG, et al. Systemic neutrophil-to-lymphocyte ratio in colorectal cancer: the relationship to patient survival, tumour biology and local lymphocytic response to tumour. Br J Cancer. 2015;113(2):204–211. doi:10.1038/bjc.2015.87
29. Deryugina EI, Zajac E, Juncker-Jensen A, Kupriyanova TA, Welter L, Quigley JP. Tissue-infiltrating neutrophils constitute the major in vivo source of angiogenesis-inducing MMP-9 in the tumor microenvironment. Neoplasia. 2014;16(10):771–788. doi:10.1016/j.neo.2014.08.013
30. Ocana A, Nieto-Jiménez C, Pandiella A, Templeton AJ. Neutrophils in cancer: prognostic role and therapeutic strategies. Mol Cancer. 2017;16(1):137. doi:10.1186/s12943-017-0707-7
31. Xiong S, Dong L, Cheng L. Neutrophils in cancer carcinogenesis and metastasis. J Hematol Oncol. 2021;14(1):173. doi:10.1186/s13045-021-01187-y
32. Jaillon S, Ponzetta A, Di Mitri D, Santoni A, Bonecchi R, Mantovani A. Neutrophil diversity and plasticity in tumour progression and therapy. Nat Rev Cancer. 2020;20(9):485–503. doi:10.1038/s41568-020-0281-y
33. Coffelt SB, Kersten K, Doornebal CW, et al. IL-17-producing γδ T cells and neutrophils conspire to promote breast cancer metastasis. Nature. 2015;522(7556):345–348. doi:10.1038/nature14282
34. Bodogai M, Moritoh K, Lee-Chang C, et al. Immunosuppressive and prometastatic functions of myeloid-derived suppressive cells rely upon education from tumor-associated B cells. Cancer Res. 2015;75(17):3456–3465. doi:10.1158/0008-5472.CAN-14-3077
35. Coffelt SB, Wellenstein MD, de Visser KE. Neutrophils in cancer: neutral no more. Nat Rev Cancer. 2016;16(7):431–446. doi:10.1038/nrc.2016.52
36. Shibutani M, Maeda K, Nagahara H, et al. The peripheral monocyte count is associated with the density of tumor-associated macrophages in the tumor microenvironment of colorectal cancer: a retrospective study. BMC Cancer. 2017;17(1):404. doi:10.1186/s12885-017-3395-1
37. Petty AJ, Yang Y. Tumor-associated macrophages: implications in cancer immunotherapy. Immunotherapy. 2017;9(3):289–302. doi:10.2217/imt-2016-0135
38. Haemmerle M, Taylor ML, Gutschner T, et al. Platelets reduce anoikis and promote metastasis by activating YAP1 signaling. Nat Commun. 2017;8(1):310. doi:10.1038/s41467-017-00411-z
39. Wan S, Lai Y, Myers RE, et al. Preoperative platelet count associates with survival and distant metastasis in surgically resected colorectal cancer patients. J Gastrointest Cancer. 2013;44(4):293–304. doi:10.1007/s12029-013-9491-9
40. Gonzalez H, Hagerling C, Werb Z. Roles of the immune system in cancer: from tumor initiation to metastatic progression. Genes Dev. 2018;32(19–20):1267–1284. doi:10.1101/gad.314617.118
41. Pang H, Zhang W, Liang X, et al. Prognostic score system using preoperative inflammatory, nutritional and tumor markers to predict prognosis for gastric cancer: a two-center cohort study. Adv Ther. 2021;38(10):4917–4934. doi:10.1007/s12325-021-01870-z
42. Li S, Yao W, Liu R, Lu Y, Zhang H, Liang X. Severe lymphopenia as a prognostic factor in rectal cancer patients receiving adjuvant chemoradiotherapy: a retrospective study. Sci Rep. 2023;13(1):7566. doi:10.1038/s41598-023-34145-4
43. Fucà G, Guarini V, Antoniotti C, et al. The pan-immune-inflammation value is a new prognostic biomarker in metastatic colorectal cancer: results from a pooled-analysis of the Valentino and TRIBE first-line trials. Br J Cancer. 2020;123(3):403–409. doi:10.1038/s41416-020-0894-7
44. Yu HJ, Shan R, Xu JQ. Prognostic significance of the pretreatment pan-immune-inflammation value in cancer patients: an updated meta-analysis of 30 studies. Front Nutr. 2023;10:1259929. doi:10.3389/fnut.2023.1259929
45. Guven DC, Sahin TK, Erul E, Kilickap S, Gambichler T, Aksoy S. The association between the pan-immune-inflammation value and cancer prognosis: a systematic review and meta-analysis. Cancers. 2022;14(11):2675. doi:10.3390/cancers14112675
46. Yang XC, Liu H, Liu DC, Tong C, Liang XW, Chen RH. Prognostic value of pan-immune-inflammation value in colorectal cancer patients: a systematic review and meta-analysis. Front Oncol. 2022;12:1036890. doi:10.3389/fonc.2022.1036890
47. Qi X, Qiao B, Song T, et al. Clinical utility of the pan-immune-inflammation value in breast cancer patients. Front Oncol. 2023;13:1223786. doi:10.3389/fonc.2023.1223786
48. Hong S, Liu J, Cheng J, Meng C, Liu B, Liao J. Pan-immune-inflammation value in lung cancer: prognostic significance and implications for therapeutic guidance—a systematic review and meta-analysis. World J Surg Oncol. 2025;23(1):250. doi:10.1186/s12957-025-03910-2
49. Lin F, Zhang LP, Xie SY, et al. Pan-immune-inflammation value: a new prognostic index in operative breast cancer. Front Oncol. 2022;12:830138. doi:10.3389/fonc.2022.830138
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Novel Risk Score (P-score) Based on a Three-Gene Signature, for Estimating the Risk of Prostate Cancer-Specific Mortality
Söderdahl F, Xu LD, Bring J, Häggman M
Research and Reports in Urology 2022, 14:203-217
Published Date: 11 May 2022
Identification of KRBA1 as a Potential Prognostic Biomarker Associated with Immune Infiltration and m6A Modification in Hepatocellular Carcinoma
Liu Y, Fu B, Yu Z, Song G, Zeng H, Gong Y, Ding Y, Huang D
Journal of Hepatocellular Carcinoma 2022, 9:497-516
Published Date: 31 May 2022
Prognostic Roles of Inflammation- and Nutrition-Based Indicators for Female Patients with Cancer
Yang M, Zhang Q, Ge Y, Tang M, Hu C, Wang Z, Zhang X, Song M, Ruan G, Zhang X, Liu T, Xie H, Zhang H, Zhang K, Li Q, Li X, Liu X, Lin S, Shi H
Journal of Inflammation Research 2022, 15:3573-3586
Published Date: 17 June 2022
Fashionable, but What is Their Real Clinical Usefulness? NLR, LMR, and PLR as a Promising Indicator in Colorectal Cancer Prognosis: A Systematic Review
Misiewicz A, Dymicka-Piekarska V
Journal of Inflammation Research 2023, 16:69-81
Published Date: 7 January 2023
NUP62CL as an Immunological and Prognostic Biomarker of Oral Squamous Cell Carcinoma
Yu X, Xu L, Zhou Y, Zhou X, Yang L, Zhou Y
Journal of Inflammation Research 2023, 16:3799-3809
Published Date: 29 August 2023