Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
A Multicenter Cross-Sectional Study on Clinical Characteristics and Disease Burden of 1010 Patients with Moderate to Severe Atopic Dermatitis in Chinese Tertiary Hospitals
Authors Sun Y, Ma S, Wang Z, Cao H, Jiang G ![]()
Received 1 December 2025
Accepted for publication 24 February 2026
Published 10 March 2026 Volume 2026:19 431875
DOI https://doi.org/10.2147/CCID.S431875
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Anne-Claire Fougerousse
Yao Sun,1,* Shixi Ma,2,* Zixuan Wang,3 Handan Cao,1 Guan Jiang1
1Department of Dermatology, Affiliated Hospital of Xuzhou Medical University, Xuzhou, Jiangsu, People’s Republic of China; 2Department of General Outpatient Services, Ganyu District Center for Disease Control and Prevention, Lianyungang, Jiangsu, People’s Republic of China; 3Department of Dermatology, Xuzhou Medical University, Xuzhou, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Guan Jiang, Department of Dermatology, Affiliated Hospital of Xuzhou Medical University, Xuzhou, Jiangsu, 221002, People’s Republic of China, Tel +86 18168777336, Email [email protected]
Purpose: To investigate the clinical characteristics of patients with moderate to severe atopic dermatitis (AD) visiting tertiary hospitals in China.
Study Design: A multicenter cross-sectional survey was conducted on 1010 patients with moderate to severe AD. Their demographic characteristics, history of allergic diseases, inducing factors, treatment, disease assessment scales, and disease burden were analyzed.
Place & Duration of the Study: The survey was conducted in 7 tertiary hospitals from October 2022 to October 2023, including Affiliated Hospital of Xuzhou Medical University, Yancheng First People’s Hospital, Huai’an First People’s Hospital, Lianyungang First People’s Hospital, Lianyungang Second People’s Hospital, Suqian Hospital of Nanjing Drum Tower Hospital Group and Xuzhou First People’s Hospital.
Results: Among the 1010 patients, the median age was 55.5 years, and 59.5% had severe AD. Female patients exhibited higher clinician-assessed SCORAD scores than male patients (P=0.016), although multivariate analysis identified age, personal allergic history, and smoking as independent risk factors for severity, with gender not retaining statistical significance. 50.7% had a personal history of allergic diseases, 26.9% had a family history, and allergic rhinitis was the most common. Season, skin moisturizing after bathing, smoking, and drinking were related to the disease. Treatment was mainly oral antihistamines and topical glucocorticoids. The SCORAD score was significantly positively correlated with the DLQI/CDLQI, POEM, NRS, and ADCT scores (P< 0.01). Spearman correlation analysis demonstrated significant positive correlations between SCORAD and DLQI/CDLQI, POEM, NRS, and ADCT scores. The medical expenses of severe patients were higher than those of moderate patients (P< 0.05).
Conclusion: This study delineates the clinical profile and substantial burden of moderate-to-severe AD in Chinese tertiary hospitals, identifying older age, personal allergic history and smoking as independent risk factors for disease severity. These findings provide a basis for targeted management and informed clinical decision-making for this patient population.
Keywords: atopic dermatitis, epidemiology, cross-sectional study, clinical characteristics, disease burden, influencing factors
Introduction
Atopic dermatitis (AD) is a chronic, recurrent inflammatory skin disease characterized by eczematous lesions, dry skin, and pruritus, often accompanied by allergic diseases such as allergic rhinitis and asthma.1,2 The prevalence of AD is increasing globally, and the incidence rate in China has been rising in recent years, seriously affecting patients’ quality of life and socioeconomic status.3
Several epidemiological studies on AD have been conducted both domestically and internationally. A systematic review including 27 countries showed that the prevalence of AD ranged from 4.1% to 25.7%.4 A cross-sectional survey in China found that the prevalence of AD in 5967 infants was 30.48%.5 A study on adult AD in the United States reported a prevalence of 7.3%,6 with an increasing trend over the past decade. These studies indicate that AD has a significant prevalence trend in different countries and regions, with moderate to severe cases being predominant.
While several international studies have described AD epidemiology, there remains a paucity of large-scale, real-world data specifically characterizing moderate-to-severe AD patients managed in Chinese tertiary hospitals. The unique healthcare-seeking behavior in China, where patients with severe diseases are preferentially channeled to tertiary centers, creates a distinct patient population with potentially different clinical profiles, treatment accessibility, and economic burden. Moreover, the integration of traditional Chinese medicine (TCM) in mainstream dermatology practice and the rapid adoption of biologics like dupilumab in recent years warrant systematic documentation. Therefore, this multicenter study aims to fill these gaps by providing a comprehensive snapshot of demographic characteristics, comorbid allergic patterns, treatment modalities, patient-reported outcomes, and economic burden in this specific healthcare context.
Methods
This study included moderate to severe AD patients who visited the dermatology departments of 7 tertiary hospitals in different geographical regions from October 2022 to October 2023. The 7 hospitals were: Affiliated Hospital of Xuzhou Medical University, Xuzhou First People’s Hospital, Lianyungang First Hospital, Lianyungang Second People’s Hospital, Yancheng First People’s Hospital, Huai’an First People’s Hospital, and Suqian Hospital of Nanjing Drum Tower Hospital Group. All participating centers were tertiary hospitals located within Jiangsu Province, reflecting a geographically concentrated but socioeconomically diverse catchment area including both urban and semi-urban populations. This study has been approved by the Medical Ethics Committee of the Affiliated Hospital of Xuzhou Medical University, with the approval number [XYFY2021-KL247-01]. All procedures involving human participants were conducted in accordance with the ethical standards of the institutional research committee and with the Declaration of Helsinki. Written informed consent was obtained from all participants prior to enrollment.
All participants signed the informed consent. A total of 1050 patients signed the informed consent, of which 40 patients failed to meet the inclusion criteria, and 1010 patients were finally included in the study. The patient enrollment process is shown in Figure S1.
Inclusion Criteria
(1) Age ≥12 years; (2) Meeting the diagnostic criteria of the 2020 Chinese Guidelines for Diagnosis and Treatment of Atopic Dermatitis;7 (3) Moderate to severe AD defined by SCORAD score; (4) Patients or their guardians agreed to participate in the study and signed informed consent.
Exclusion Criteria
(1) Comorbid with other severe chronic skin diseases (such as psoriasis, erythroderma, etc).; (2) Suffering from severe systemic diseases (such as malignant tumors, autoimmune diseases, etc).; (3) Participated in AD-related clinical trials within 1 year; (4) Patients unable to understand or complete the questionnaire survey.
The sample size for this study was estimated based on parameters such as the prevalence of AD in China, confidence level, and allowable error. According to literature reports, the prevalence of AD in China is about 12.94%. Taking α=0.05, β=0.10, δ=0.10p, the sample size n=(μα+μβ)2 p(1-p)/δ2=(1.96+1.28)2 ×0.1294×(1–0.1294)/0.012942≈865 cases. Considering a non-response and information loss rate of no more than 20%, the final sample size was determined to be 1010 moderate to severe AD patients.
A unified questionnaire was used to collect information on patients’ demographic characteristics, treatment status, history of allergic diseases, family history of AD, AD triggers or exacerbating factors, disease assessment scales, and disease burden.
The Scoring Atopic Dermatitis index (SCORAD),8 Dermatology Life Quality Index (DLQI)/Children’s Dermatology Life Quality Index (CDLQI),9 Patient-Oriented Eczema Measure (POEM),10 Numerical Rating Scale (NRS) for peak pruritus,11 and Atopic Dermatitis Control Tool (ADCT)12 were used to assess the condition of AD patients. SCORAD was used to determine the severity of AD, assessing the extent of skin lesions (A), severity of lesions (B), and subjective symptoms of pruritus and sleep disturbance (C). The SCORAD calculation result is A/5+7B/2+C, with a score range of 0–103 points. Based on the score, the disease severity is classified as: mild (0–24 points), moderate (25–50 points), and severe (>50 points). DLQI/CDLQI was used to evaluate the impact of skin disease on daily life over the past week, using 10 questions scored 0–3 points each, with a total score of 30 points. Higher scores indicate a greater impact of the disease on the patient’s quality of life. POEM is a patient’s subjective assessment of disease severity, using 7 questions to score the frequency of itching, sleep disturbance, bleeding, oozing, cracking, skin peeling, and dryness over the past week. Each item is scored 0–4 points based on frequency, with a total score of 28 points. Higher scores indicate more severe disease. NRS was used to evaluate the patient’s subjective sensation of itching, using numbers between 0 and 10 to self-assess the degree of itching in the past 24 hours, where 0 represents no itching and 10 represents the most severe itching imaginable. ADCT was used to assess disease control over the past week, using 6 questions scored 0–4 points each, with a total score of 24 points. Higher scores indicate poorer AD control, with an ADCT score ≥7 considered as poor disease control.
Patient assessments were performed by experienced and professionally trained dermatologists and research nurses. All assessors received uniform training before the start of the study to ensure consistency and accuracy of the assessment.
SPSS 26.0 statistical software was used for data analysis. Normally distributed measurement data were expressed as mean ± standard deviation, and t-test was used for comparison between two groups. Data not conforming to normal distribution were expressed as median (interquartile range) [M(Q1, Q3)], and Mann–Whitney U-test was used for comparison between two groups. Kruskal–Wallis H-test was used for comparison among multiple groups, and Kruskal–Wallis H-test with Bonferroni correction was used for pairwise comparisons. Count data were expressed as number of cases (%), and Pearson’s χ2 test was used for comparison between groups. When the theoretical frequency n>40 and 1≤T<5, continuity-corrected chi-square test was used; when n≤40 or T<1, Fisher’s exact probability method was used. Correlation analysis used Spearman correlation coefficient. Binary multivariate logistic regression analysis was used for factors influencing AD severity. Two-sided tests were used with a significance level of α=0.05.
Data Quality and Missing Data
The study utilized an electronic questionnaire system where all items were set as mandatory. Only 3 cases had missing BMI data and 2 cases had missing education level data, resulting in a total missing proportion of <0.5%. Therefore, we employed a complete-case analysis and did not perform multiple imputation.
Result
This study included 1010 AD patients, comprising 602 males (59.6%) and 408 females (40.4%), with a male-to-female ratio of 1.48:1. The age range was 12 to 96 years, with a median age of 55.5 (36.7, 70.5) years. Middle-aged and elderly AD patients ≥45 years old accounted for the highest proportion at 42.2%. According to SCORAD index analysis, moderate and severe AD patients accounted for 40.5% and 59.5%, respectively. Regarding patients’ residence and marital status, urban residents and married patients accounted for high proportions of 83.7% and 81.8%, respectively. Additionally, the average body mass index (BMI) of patients was 23.5 (21.3, 25.7) kg/m2. In terms of occupation, retired/unemployed patients accounted for the highest proportion at 44.0% (444 cases). Regarding education level, patients with secondary school and vocational school education were the most numerous, accounting for 47.4% (479 cases) of the total. There were significant statistical differences between moderate and severe AD patients in terms of gender, age, marital status, occupation type, and education level (P<0.05).
In this study, we conducted a detailed survey of allergic disease history among 1010 AD patients. The results showed that 512 patients (50.7%) had a personal history of allergic diseases, while 272 patients (26.9%) had a family history of allergic diseases. Additionally, 231 patients (22.9%) had both personal and family histories of allergies. Regarding personal history of allergic diseases, allergic rhinitis was the most common, affecting 252 patients (25.0%). Further analysis revealed that moderate AD patients had a higher personal history of asthma, food allergies, urticaria, excessive insect bite reactions, and eczema compared to severe patients, with statistically significant differences (P<0.05). In terms of family history of allergic diseases, allergic rhinitis was also the most common, affecting 142 patients (14.1%). For severe AD patients, the family history of allergic rhinitis, asthma, allergic conjunctivitis, food allergies, urticaria, excessive insect bite reactions, and eczema was significantly higher than that of moderate AD patients, with statistically significant differences (P<0.05).
In this survey of 1010 AD patients, 37.0% reported symptom exacerbation in specific seasons, most notably in summer (17.1%), followed by winter (10.9%). Moderate AD patients were most affected by summer. Additionally, disease severity was associated with patients’ skin moisturizing after bathing, smoking, and drinking behaviors.
All 1010 patients had received treatment, with topical glucocorticoids and moisturizers being the main local treatments, accounting for 47.9% and 25.2%, respectively. Among oral medications, antihistamines had the highest usage rate at 64.7%, followed by Chinese herbal medicine and systemic glucocorticoids. In terms of targeted therapy, dupilumab had the highest application rate at 25.1%. Moderate patients had a higher use of topical calcineurin inhibitors compared to severe patients (P<0.05); severe patients had higher use of dupilumab, systemic glucocorticoids, compound glycyrrhizin tablets, and Chinese herbal medicine treatments compared to moderate patients (P<0.05). See Table 1 for details.
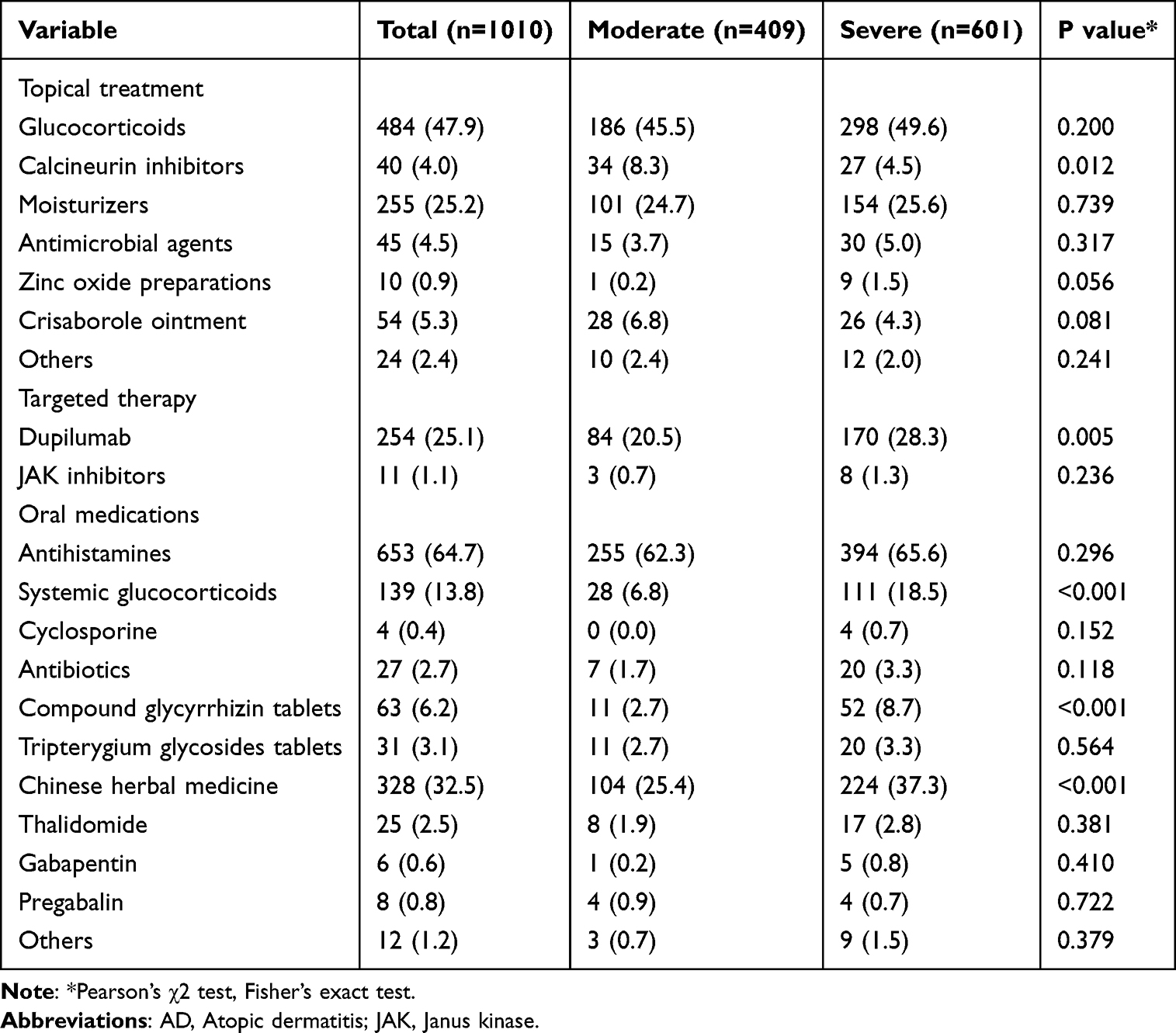 |
Table 1 Distribution of AD Patients’ Related Treatments [n (%)] |
A total of 1010 patients participated in the disease assessment scale recording. The results showed no significant differences between male and female patients in DLQI/CDLQI, POEM, NRS, and ADCT scores (all P>0.05), but female patients had higher SCORAD scores than male patients (P=0.016), suggesting more severe disease in females. There were significant differences in SCORAD, POEM, NRS, and ADCT scores among different age groups (all P<0.05). Pairwise comparisons showed statistical differences in SCORAD, POEM, and ADCT scores between the <18 years and ≥45 years groups, and between the 18–44 years and ≥45 years groups (all P<0.05). NRS scores showed statistical differences between all age groups (all P<0.05). See Table 2 for details. Spearman correlation analysis demonstrated significant positive correlations between SCORAD and DLQI/CDLQI, POEM, NRS, and ADCT scores (all P < 0.001) (Figure S2).
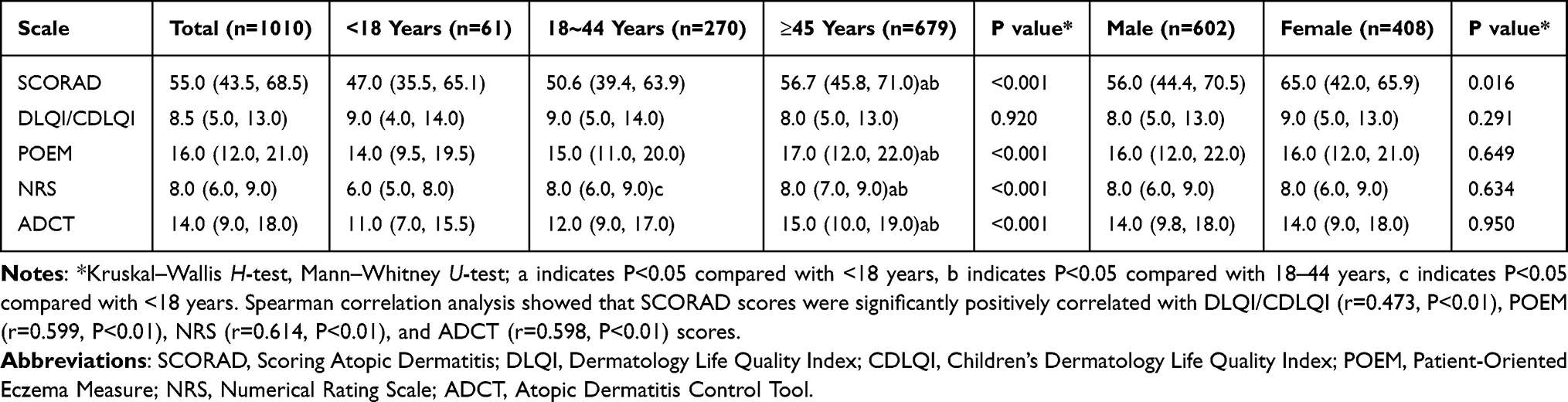 |
Table 2 Differences in Disease Assessment Scales Across Age Groups and Genders [Score, M(Q1,Q3)] |
A total of 1004 patients participated in the survey on health economic burden over the past year. Among them, 37 patients required hospitalization due to their condition, with an average cost of 5000 (4000, 9000) yuan per hospitalization and a total hospitalization medical cost of 6000 (5000, 12000) yuan. Additionally, 769 patients chose outpatient treatment, with an average medical cost of 300 (100, 500) yuan per visit and a total outpatient medical cost of 600 (100, 2000) yuan. Furthermore, 228 patients incurred other types of expenses, such as skincare products, medical cosmetics, and medicinal baths, with an average cost of 335 (200, 1000) yuan. The survey also found that 168 patients experienced absenteeism from work or school, with an average of 5.0 (2.0, 10.0) times per person. Compared to moderate AD patients, severe patients had higher average outpatient medical costs, total outpatient medical costs, and other expenses (P<0.05).
This study used SCORAD score-defined moderate and severe cases as the dependent variable. Based on the previous analysis results and clinical experience, we selected age, gender, BMI, personal history of allergic diseases, family history of allergic diseases, smoking history, drinking history, seasonal exacerbation, and other factors as independent variables, and then conducted binary multivariate logistic regression analysis. In the logistic regression model, χ2=66.659, P<0.001, indicating that the model was statistically significant. The regression results showed that age, personal history of allergic diseases, and smoking were risk factors for AD severity. See Table 3 for details.
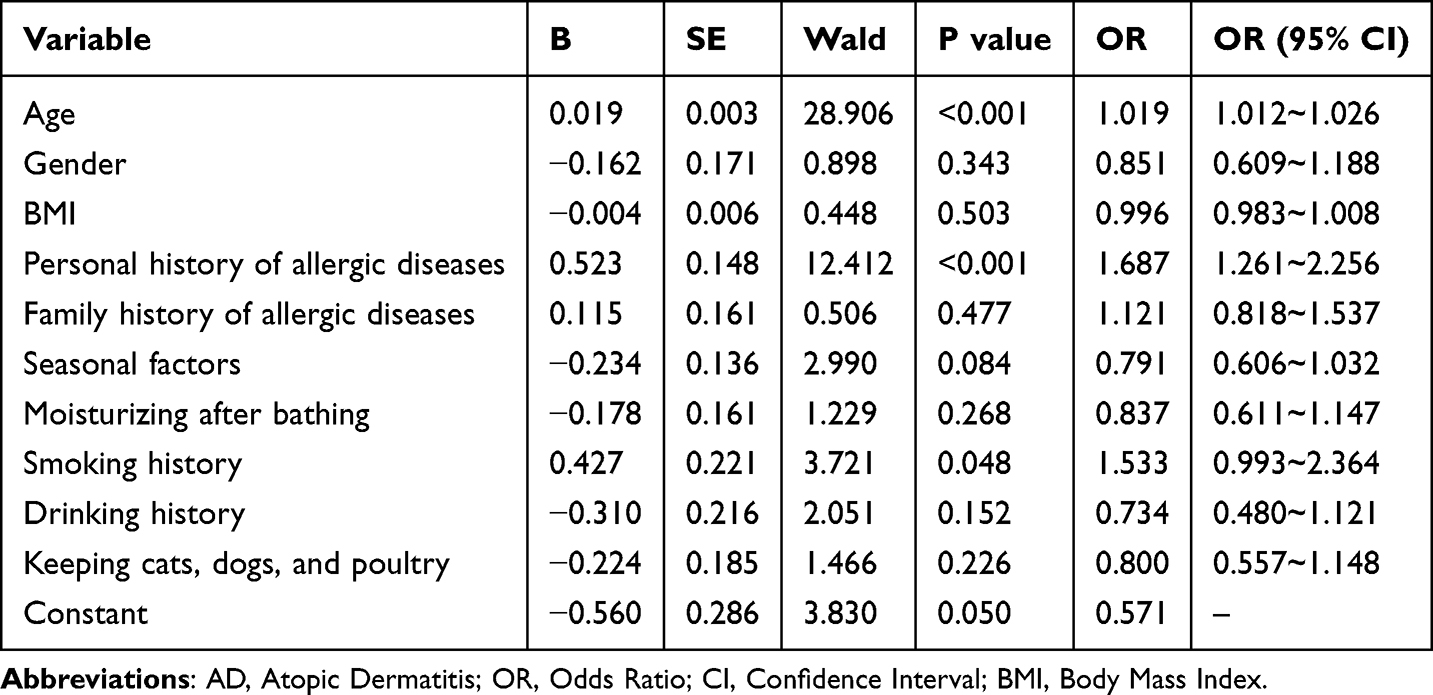 |
Table 3 Binary Multivariate Logistic Regression Analysis of Factors Influencing AD Severity |
Discussion
AD is a common chronic disease in dermatology outpatient clinics, typically characterized by recurrent eczematous lesions and pruritus. Currently, the incidence of AD varies among different countries and regions, but overall studies indicate an increasing trend, especially in Asia.13 Multiple studies both domestically and internationally have shown that moderate to severe AD is predominant across all age groups, with patients often experiencing severe recurrent pruritus that significantly affects their quality of life and imposes substantial family and social economic burdens.14
Our study results show that male patients outnumber female patients, but female patients have more severe disease (SCORAD score significantly higher than males). This is different from the results of the study in Madagascar by Sendrasoa et al,15 which found a higher proportion of female adult AD patients but no gender difference in disease severity. This discrepancy may reflect characteristics of AD patients across different ethnicities and regions. Kowalska-Olędzka et al’s study showed that European AD patients are mainly concentrated in children and young adults,16 while our study found that patients aged ≥45 years account for the highest proportion (42.2%) of Chinese AD patients. This difference may be related to China’s aging population trend and changes in environmental factors. Additionally, we found that AD severity increases with patient age. This may be due to skin aging, immune imbalance, cumulative damage, and environmental stress, which weaken the skin’s defense and repair capabilities as patients age.
The observation that female patients had higher clinician-assessed SCORAD scores (driven primarily by greater lesion extent and erythema) without corresponding differences in patient-reported outcomes (PROs) warrants careful interpretation. This divergence may reflect: (1) Physiological differences: Hormonal influences on skin barrier function and immune modulation may manifest as more visible inflammation; (2) Reporting behavior: Female patients may have higher thresholds for reporting quality-of-life impact or pruritus severity; or (3) Assessment bias: The SCORAD’s objective components (extent/erythema) may capture gender-specific dermatological manifestations that do not directly translate to differential PRO burden. Importantly, this finding underscores the necessity of integrating both objective and subjective measures in AD trials, as they capture complementary yet distinct disease dimensions. It also highlights that severity determinants may differ between observable pathology and lived experience.
Our study found that 50.7% of AD patients had at least one other allergic disease, 26.9% had a family history of allergic diseases, and 22.9% had both personal and family allergic histories. The most common personal or family history of allergic disease was allergic rhinitis, consistent with a Korean study.17 Notably, having a personal history of allergic diseases is a risk factor for AD severity. This may be because these patients have inherent immune system abnormalities, are prone to excessive immune responses, and may have more fragile skin barrier function, leading to easier exacerbation and spread of inflammation. Furthermore, most AD patients showed seasonal variations in their condition. In our study, 37.0% of AD patients experienced exacerbation in a particular season, with summer and winter being the most common periods of worsening. This result is inconsistent with previous studies,18 possibly due to differences in ethnicity and geography. Additionally, smoking is a risk factor for AD severity, consistent with Alturki et al’s study in Saudi Arabia,19 suggesting that smoking may damage the skin barrier and immune balance in multiple ways, triggering or exacerbating the condition.
Different countries and regions have developed corresponding AD diagnosis and treatment guidelines, but due to economic, cultural, and geographical factors, there are some differences in AD treatment concepts and methods.20 In our study, the main treatment methods used by patients included oral antihistamines (64.7%) and topical glucocorticoids (47.9%). Additionally, Chinese herbal medicine treatment (32.5%) was also widely used, which is a unique feature of AD treatment in China. In contrast, studies in Western countries rarely report the use of Chinese herbal medicine. For example, Armario-Hita et al’s review mainly discussed Western medical treatment plans without mentioning traditional Chinese medicine treatments.21 Our study found that the use of treatment methods recommended in international treatment guidelines was relatively low in this study population, such as cyclosporine, calcineurin inhibitors, systemic glucocorticoids, dupilumab, and phototherapy. This may be related to the accessibility of medical resources and patients’ treatment preferences.
The high dupilumab utilization (25.1%) likely reflects selection bias towards severe, refractory cases referred to tertiary centers, exceeding reported national averages (8–12%). The clinical takeaway is that while biologics are increasingly accessible in specialized settings, real-world effectiveness and long-term safety monitoring remain imperative. Our data reflect access patterns, not outcomes. Similarly, the prevalent use of traditional Chinese herbal medicine (32.5%) reflects culturally embedded treatment preferences and TCM integration in China’s dermatology practice. However, the absence of standardized efficacy/safety documentation precludes endorsement. The key message for readers is that these patterns highlight sociocultural determinants of treatment choice and the need for rigorous, prospective studies evaluating both conventional and traditional therapies in Chinese AD populations. Clinicians should engage patients in shared decision-making, acknowledging these preferences while emphasizing evidence-based core therapies.
In this study, we observed significant differences in SCORAD, DLQI/CDLQI, POEM, NRS, and ADCT scores when assessing AD patients’ conditions, consistent with previous research results.22 Our study found that the SCORAD assessment score was 55.0, indicating the extensiveness and severity of patients’ conditions; the DLQI/CDLQI assessment score was 8.5, revealing a moderate impact of the disease on patients’ quality of life; the POEM assessment score was 16.0, indicating a moderate impact of the disease on patients; the NRS assessment score was 8.0, indicating severe distress from itching; and the ADCT assessment score was 14.0, with 91.2% of patients having poor disease control. Our study also found that AD patients in the ≥45 years age group had the highest scores on all assessment scales, suggesting that patients in this age group have more severe conditions and require close attention to the occurrence and development of AD. Additionally, SCORAD scores were significantly positively correlated with DLQI/CDLQI, POEM, NRS, and ADCT scores, indicating that higher disease severity is associated with greater impact on patients’ quality of life, more pronounced symptom perception, and poorer disease control.
This study also investigated the disease burden of AD patients. Consistent with previous studies, patients with moderate to severe AD bear a huge economic burden.23 Firstly, from the perspective of hospitalization and outpatient costs, the disease brings enormous economic pressure to patients. Among hospitalized patients, the highest total hospitalization cost in the past year reached 50,000 yuan. Although outpatient costs are relatively lower, frequent visits can lead to significant cumulative expenses. In the past year, 15.5% of patients had total outpatient costs exceeding 5000 yuan, with the highest reaching 32,000 yuan. Moreover, in addition to direct medical expenses, the disease may lead to other related costs (such as skincare products, medical cosmetics, medicinal baths, etc)., with total other expenses in the past year ranging from 50 to 30,000 yuan. Furthermore, the disease has had a profound impact on patients’ lives and work.24 Our results show that 16.7% of patients experienced absenteeism or missed classes due to the disease, which not only affected their normal work and study but may also lead to reduced income or academic setbacks. Notably, severe patients had significantly higher medical expenses and other related costs compared to moderate patients, consistent with previous studies.25 This indicates that disease severity not only affects patients’ health status but also directly relates to the magnitude of economic burden. Therefore, for patients, early detection and treatment of the disease to prevent further deterioration can not only help restore physical health but also alleviate economic pressure to some extent.
The substantial economic burden observed among patients with severe AD in this study highlights the importance of early, proactive, and effective therapeutic interventions. In particular, innovative treatments targeting severe cases—such as dupilumab—though associated with higher initial costs, may prove more cost-effective in the long term by reducing complications, decreasing outpatient visits, and minimizing indirect economic losses.
While our descriptive findings align with global AD literature, this study’s value lies in its context-specific real-world evidence from Chinese tertiary care—a setting where disease concentration, treatment accessibility, and healthcare practices differ substantially from Western cohorts. The integration of comprehensive PROs and economic burden data within this unique healthcare ecosystem provides a contemporary benchmark for policy-makers and clinicians managing AD in similar resource-structured environments.
It must be acknowledged that the sample for this study was sourced from tertiary hospitals, which may overestimate the proportion and severity of AD cases. A key limitation is that all seven centers were located within Jiangsu Province. While this ensured standardized data collection and quality control, the findings may not fully represent the heterogeneity of AD patients across China’s different climatic zones, ethnicities, and healthcare systems (eg, Pearl River Delta vs Northwest regions). Future nationwide studies should validate these findings across multiple provinces. According to 2023 data from the National Center for Quality Control of Dermatological Diseases, the proportion of moderate-to-severe AD among outpatients is approximately 65% in tertiary hospitals, but only 35% in community hospitals. This suggests that the results of this study reflect the characteristics of patients seeking specialist care (referral bias) and should be interpreted with caution when extrapolating to the general, unselected population.
Limitations
This study has several limitations. First, its cross-sectional design restricts the ability to infer causal relationships between risk factors and AD severity, meaning the observed associations (such as with smoking and allergic history) are hypothesis-generating, not causal inferences. Second, all participants were recruited from tertiary hospitals, introducing a “referral filter” bias that systematically overestimates the proportion of moderate-to-severe AD cases. Consequently, the findings primarily reflect the specialized care population and may not be generalizable to community-based populations, which mainly consist of mild cases. Third, some variables (eg, seasonal exacerbation, post-bathing moisturization) relied on patients’ retrospective self-reports, potentially introducing information bias (recall bias) and social desirability bias. Future studies could use real-time ecological momentary assessment (EMA) or objective diary cards for validation. Furthermore, the absence of objective biomarkers, such as serum total IgE, TARC, filaggrin gene mutations, TEWL and skin microbiome assessments, limits a deeper exploration of AD disease mechanisms and endophenotypes. Despite these limitations, this is the first large-sample study to systematically describe the clinical characteristics and disease burden of moderate-to-severe AD patients in Chinese tertiary hospitals, providing an important foundation for future community-based research. We are currently planning a multi-center prospective cohort design to systematically integrate objective biomarkers, skin physiological parameters, and digital phenotyping to further validate and extend these findings. Future research is recommended to build upon these findings through multi-level population studies, community cohorts, or longitudinal follow-up.
Conclusion
In conclusion, this large-scale study reveals the distinctive epidemiological characteristics and substantial burden of moderate-to-severe AD in Chinese tertiary hospitals. Key findings—such as increased severity in older patients, high comorbid allergic burden, and the identification of age, smoking, and personal allergic history as independent risk factors—provide a foundation for targeted management. The divergence between objective severity and patient-reported impact, along with unique treatment patterns, underscores the need for personalized, biopsychosocial approaches in this healthcare context.
Patient Consent
All adult participants provided written informed consent. For adolescent participants (12–17 years), written informed consent was obtained from their parents or legal guardians. All participants’ privacy and confidentiality were strictly protected.
Acknowledgment
The authors would like to thank the following institutions and investigators for their invaluable contribution to patient recruitment and data collection: Lianyungang First People’s Hospital (Hong Ren), Lianyungang Second People’s Hospital (Ying Liu), Suqian Hospital of Nanjing Drum Tower Hospital Group (Jing Wang), Xuzhou First People’s Hospital (Jianbin Zhao), Huai’an First People’s Hospital (Weiguo Sun), and Yancheng First People’s Hospital (Dong Lü).
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study had no funding source.
Disclosure
The authors declared no potential conflicts of interest with respect to the research, authorship and publication of this article.
References
1. Frazier W, Bhardwaj N. Atopic dermatitis: diagnosis and treatment. Am Fam Physician. 2020;101(10):590–9.
2. Torres T, Ferreira EO, Gonçalo M, Mendes-Bastos P, Selores M, Filipe P. Update on atopic dermatitis. Acta Med Port. 2019;32(9):606–613. doi:10.20344/amp.11963
3. Lee EM, Cho YT, Chan TC, Shen D, Chu CY, Tang CH. Economic burden of atopic dermatitis in Taiwan. Acta Derm Venereol. 2023;103:adv00866. doi:10.2340/actadv.v103.4556
4. Hadi HA, Tarmizi AI, Khalid KA, Gajdács M, Aslam A, Jamshed S. The epidemiology and global burden of atopic dermatitis: a narrative review. Life. 2021;11(9). doi:10.3390/life11090936
5. Guo Y, Zhang H, Liu Q, et al. Phenotypic analysis of atopic dermatitis in children aged 1-12 months: elaboration of novel diagnostic criteria for infants in China and estimation of prevalence. J Eur Acad Dermatol Venereol. 2019;33(8):1569–1576. doi:10.1111/jdv.15618
6. Chiesa Fuxench ZC, Block JK, Boguniewicz M, et al. Atopic dermatitis in America study: a cross-sectional study examining the prevalence and disease burden of atopic dermatitis in the US adult population. J Invest Dermatol. 2019;139(3):583–590. doi:10.1016/j.jid.2018.08.028
7. Atopic Dermatitis Working Group IG. Chinese Society of Dermatology. Guideline for diagnosis and treatment of atopic dermatitis in China (2020). Chin Jl of Dermatol. 2020;53(2):81–88. doi:10.35541/cjd.20191000
8. Lacour JP. Les scores d’évaluation de la dermatite atopique: outcome measures for atopic dermatitis [Les scores d’évaluation de la dermatite atopique: outcome measures for atopic dermatitis]. Ann Dermatol Venereol. 2020;147(11s1):11s12–11s18. doi:10.1016/s0151-9638(20)31083-8
9. Rencz F, Gergely LH, Wikonkál N, et al. Dermatology life quality index (DLQI) score bands are applicable to DLQI-Relevant (DLQI-R) scoring. J Eur Acad Dermatol Venereol. 2020;34(9):e484–e486. doi:10.1111/jdv.16398
10. Silverberg JI, Lei D, Yousaf M, et al. Comparison of patient-oriented eczema measure and patient-oriented scoring atopic dermatitis vs eczema area and severity index and other measures of atopic dermatitis: a validation study. Ann Allergy Asthma Immunol. 2020;125(1):78–83. doi:10.1016/j.anai.2020.03.006
11. Yosipovitch G, Reaney M, Mastey V, et al. Peak pruritus numerical rating scale: psychometric validation and responder definition for assessing itch in moderate-to-severe atopic dermatitis. Br J Dermatol. 2019;181(4):761–769. doi:10.1111/bjd.17744
12. Kido-Nakahara M, Yokote G, Yoshida M, Furue M, Nakahara T. Atopic dermatitis control tool (ADCT): a useful tool for self-evaluation in patients with atopic dermatitis. J Dermatol. 2021;48(12):1951–1952. doi:10.1111/1346-8138.16176
13. Lim JJ, Reginald K, Say YH, Liu MH, Chew FT. A dietary pattern of frequent plant-based foods intake reduced the associated risks for atopic dermatitis exacerbation: insights from the Singapore/Malaysia cross-sectional genetics epidemiology cohort. BMC Public Health. 2023;23(1):1818. doi:10.1186/s12889-023-16736-y
14. Augustin M, Misery L, von Kobyletzski L, et al. Systematic literature review assessing the overall costs and societal impacts of moderate-to-severe atopic dermatitis in Europe. J Eur Acad Dermatol Venereol. 2022;36(12):2316–2324. doi:10.1111/jdv.18481
15. Sendrasoa FA, Ramily SL, Razafimaharo TI, et al. Atopic dermatitis in adults: a cross-sectional study in the department of dermatology, Antananarivo, Madagascar. JAAD Int. 2021;4:28–31. doi:10.1016/j.jdin.2021.04.001
16. Kowalska-Olędzka E, Czarnecka M, Baran A. Epidemiology of atopic dermatitis in Europe. J Drug Assess. 2019;8(1):126–128. doi:10.1080/21556660.2019.1619570
17. Jeon YH, Ahn K, Kim J, et al. Clinical characteristics of atopic dermatitis in Korean school-aged children and adolescents according to onset age and severity. J Korean Med Sci. 2022;37(4):e30. doi:10.3346/jkms.2022.37.e30
18. Dunlop JH, Keller JP, Peng RD, Keet CA. The effect of season of birth on atopic dermatitis and food allergy. Ann Allergy Asthma Immunol. 2020;125(2):221–223.e2. doi:10.1016/j.anai.2020.04.034
19. Alturki BA, Almutairi R, Al-Mutairi AG, Alrajhi D, Binyousef FH, Alzamil F. The effects of smoking on the severity of atopic dermatitis in Saudi Arabia. Cureus. 2023;15(12):e50315. doi:10.7759/cureus.50315
20. LePoidevin LM, Lee DE, Shi VY. A comparison of international management guidelines for atopic dermatitis. Pediatr Dermatol. 2019;36(1):36–65. doi:10.1111/pde.13678
21. Armario-Hita JC, Galán-Gutiérrez M, Dodero-Anillo JM, Carrascosa JM, Ruiz-Villaverde R. Updated review on treatment of atopic dermatitis. J Investig Allergol Clin Immunol. 2023;33(3):158–167. doi:10.18176/jiaci.0906
22. Eyerich K, Gooderham MJ, Silvestre JF, et al. Real-world clinical, psychosocial and economic burden of atopic dermatitis: results from a multicountry study. J Eur Acad Dermatol Venereol. 2024;38(2):340–353. doi:10.1111/jdv.19500
23. Mäkelä K, Salava A, Remitz A. Economic burden and quality of life of patients with moderate to severe atopic dermatitis in a tertiary care hospital in Helsinki, Finland: a survey-based study. Cutis. 2023;112(1):E44–e51. doi:10.12788/cutis.0831
24. Sanclemente G, Hernandez N, Chaparro D, Tamayo L, Lopez A. Epidemiologic features and burden of atopic dermatitis in adolescent and adult patients: a cross-sectional multicenter study. World Allergy Organ J. 2021;14(12):100611. doi:10.1016/j.waojou.2021.100611
25. Girolomoni G, Luger T, Nosbaum A, et al. The economic and psychosocial comorbidity burden among adults with moderate-to-severe atopic dermatitis in Europe: analysis of a cross-sectional survey. Dermatol Ther. 2021;11(1):117–130. doi:10.1007/s13555-020-00459-8
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Burden of Metabolic Syndrome Among a Low-Income Population in China: A Population-Based Cross-Sectional Study
Bao J, Wang L, Hu P, Liu J, Tu J, Wang J, Li J, Ning X
Diabetes, Metabolic Syndrome and Obesity 2022, 15:2713-2723
Published Date: 3 September 2022
Clinical Features of Human Brucellosis and Risk Factors for Focal Complications: A Retrospective Analysis in a Tertiary-Care Hospital in Beijing, China
Zhang Z, Zhang X, Chen X, Cui X, Cai M, Yang L, Zhang Y
International Journal of General Medicine 2022, 15:7373-7382
Published Date: 19 September 2022
Von Willebrand Disease Epidemiology, Burden of Illness and Management: A Systematic Review
Du P, Bergamasco A, Moride Y, Truong Berthoz F, Özen G, Tzivelekis S
Journal of Blood Medicine 2023, 14:189-208
Published Date: 2 March 2023
Epidemiology and Clinical Characteristics of Seasonal Human Coronaviruses in Children Hospitalized in Hebei Province, China Before and During the COVID-19 Pandemic
Zhao MC, Wen C, Sun L, Duan SX, Zang KX, Wang L, Cui XW
Risk Management and Healthcare Policy 2023, 16:1801-1807
Published Date: 8 September 2023
Adult ADHD Positive Screening and Sibship, Birth Order and Academic Achievement: Implications for Epidemiologists and Physicians in the Kingdom of Saudi Arabia
AlOmar RS, AlShamlan NA, Al-Johani WM, Almayyad AH, Alotaibi HK, Alsamin SI, Alfrayyan NY, Boubshait LA, Alghamdi LM, Al-Shammari MA
Psychology Research and Behavior Management 2023, 16:4069-4081
Published Date: 5 October 2023