")
Back to Journals » Journal of Blood Medicine » Volume 14
Von Willebrand Disease Epidemiology, Burden of Illness and Management: A Systematic Review
Authors Du P , Bergamasco A, Moride Y, Truong Berthoz F, Özen G, Tzivelekis S
Received 16 September 2022
Accepted for publication 6 January 2023
Published 2 March 2023 Volume 2023:14 Pages 189—208
DOI https://doi.org/10.2147/JBM.S389241
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Ping Du,1 Aurore Bergamasco,2 Yola Moride,2,3 Françoise Truong Berthoz,4 Gülden Özen,1 Spiros Tzivelekis1
1Takeda Development Center Americas, Inc., Cambridge, MA, USA; 2YOLARX Consultants, Paris, France; 3Rutgers, The State University of New Jersey, New Brunswick, NJ, USA; 4Takeda Pharmaceuticals International AG, Zürich, Switzerland
Correspondence: Ping Du, Takeda Development Center Americas, Inc., 40 Landsdowne Street, Cambridge, MA, 02139, USA, Tel +1-717-307-0572, Email [email protected]
Introduction: Although hereditary von Willebrand disease (VWD) is the most common bleeding disorder, its epidemiology is not well understood. A systematic review (PROSPERO CRD42020197674/CRD42021244374) on the epidemiology/burden of illness of VWD was conducted to better understand patients’ unmet needs.
Methods: Observational studies (published January 1, 2010 to April 14, 2021) were identified in MEDLINE and Embase databases, using free-text keywords and thesaurus terms for VWD and outcomes of interest. Pragmatic web-based searches of the gray literature, including conference abstracts, were performed, and reference lists of retained publications were manually searched for additional sources. Case reports and clinical trials (phase 1– 3) were excluded. Outcomes of interest were incidence, prevalence, mortality, patient characteristics, burden of illness, and therapeutic management/treatments currently used for VWD.
Results: Of the 3095 identified sources, 168 were included in this systematic review. Reported VWD prevalence (22 sources) ranged from 108.9 to 2200 per 100,000 in population-based studies and from 0.3 to 16.5 per 100,000 in referral-based studies. Reported times between first symptom onset and diagnosis (two sources; mean 669 days; median 3 years) highlighted gaps in timely VWD diagnosis. Bleeding events reported in 72– 94% of the patients with VWD (all types; 27 sources) were mostly mucocutaneous including epistaxis, menorrhagia, and oral/gum bleeding. Poorer health-related quality of life (three sources) and greater health care resource utilization (three sources) were reported for patients with VWD than in general populations.
Conclusion: Available data suggest that patients with VWD experience high disease burden in terms of bleeding, poor quality of life, and health care resource utilization.
Keywords: disease burden, epidemiology, health-related quality of life, health care resource utilization, systematic review, von Willebrand disease
Introduction
von Willebrand disease (VWD) is an inherited bleeding disorder characterized by defects in the concentration, structure, or function of von Willebrand factor (VWF), a glycoprotein that acts as a carrier protein for factor VIII (FVIII) and facilitates platelet adhesion at vascular injury sites.1–3 There are three main types of VWD that differ according to the degree of disease severity and inheritance pattern.2 Types 1 and 3 are characterized by quantitative defects in the VWD protein: type 1 VWD is characterized by partial quantitative VWF deficiency, resulting in a mild to moderate bleeding phenotype, whereas type 3, the most severe form of VWD, results from near-complete absence of VWF.2,4 Type 2 VWD represents a group of disease phenotypes resulting from qualitative defects in VWF, affecting formation of multimers (types 2A and 2B), platelet adhesion (type 2M), or FVIII binding (type 2N).2,4 Bleeding complications in patients with VWD vary depending on the level of residual VWF activity, disease type, age, and sex.5 Patients most often experience mucocutaneous bleeding, including epistaxis, easy bruising, and heavy menstrual bleeding (HMB), as well as bleeding after surgery/trauma.4,5
VWD is considered the most common hereditary bleeding disorder,6 but information on the epidemiology of VWD is limited. This systematic review was, therefore, conducted to better understand the disease and related unmet needs for the patients. Data on the epidemiology of VWD worldwide were reviewed, including incidence, prevalence, mortality, patient characteristics, natural history, burden of illness, and therapeutic management/treatments received in the real-world clinical practice setting.
Methods
A systematic review was conducted between January 1, 2010 and April 14, 2021 (date last searched) using methods developed by the Cochrane group and the National Academy of Medicine, formerly the Institute of Medicine of the National Academy.7,8 This time period was selected to provide comprehensive search results for the outcomes of interest that were also reflective of recent trends in disease burden, epidemiology and clinical management strategies. The protocol was registered under the International Prospective Register of Systematic Reviews. The original protocol, which covered searches through to July 1, 2020, was registered on August 8, 2020 (PROSPERO CRD42020197674). An updated protocol was registered on May 12, 2021, and covered pragmatic searches from July 1, 2020 to April 14, 2021, and literature searches from July 1, 2020 to March 22, 2021, as well as from January 2010 to March 22, 2021, for publications not covered by the original protocol (ie, scientific communications without abstracts) (PROSPERO CRD42021244374).
Search Strategy and Information Sources
Comprehensive literature searches of MEDLINE and Embase were conducted to identify publications written in English. Search strategies were based on free-text keywords and thesaurus terms (ie, Medical Subject Headings [MeSH] and Emtree terms) combining the following concepts: population and data of interest. Search strategies are detailed in Supplemental Table 1. In addition, pragmatic searches were performed using Google, Google Scholar, the Cochrane Library, and websites of relevant scientific societies involved in VWD, as well as abstracts from related conferences (Supplemental Table 2). The reference lists of retained publications were manually searched for additional relevant sources (“snowballing”).
Eligibility Criteria
Observational (non-interventional) studies, literature reviews, or meta-analyses involving patients with VWD and reporting on epidemiologic, burden of illness, and management data of interest were included. Table 1 provides a complete list of inclusion and exclusion criteria.
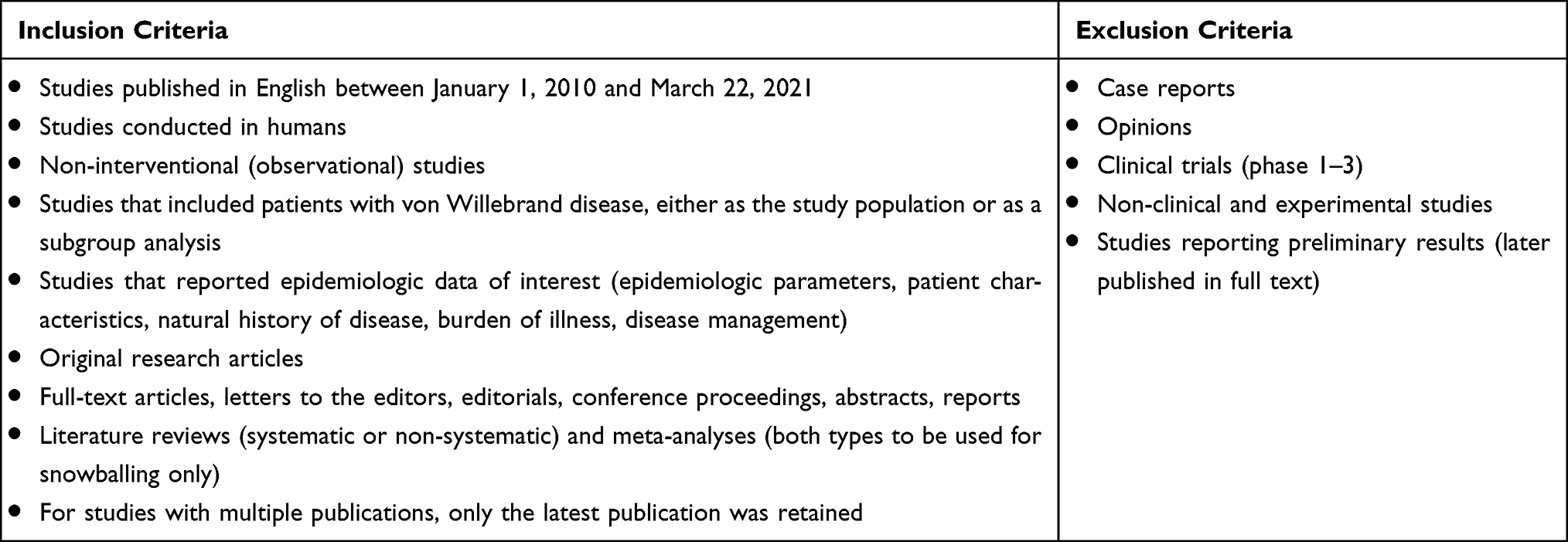 |
Table 1 Eligibility Criteria for the Selection of Sources Included in This Systematic Review |
Selection of Studies
During the first stage, titles and/or abstracts were screened using the predefined eligibility criteria by two independent reviewers, with conflicts resolved by a third assessor, and during the second stage, eligibility was confirmed by in-depth review of full texts. Reasons for exclusion at second stage were documented. For studies with multiple publications, only the most recent reporting on each outcome of interest was retained.
Data Extraction and Data Synthesis
Data from relevant publications were extracted into a standardized data extraction form and the extracted data evaluated for completeness. Data items extracted included general information (source, citation, publication type, geographical coverage); study methods (study period, study design, data source); target population (age); VWD type; study population (diagnostic criteria); number of patients with VWD; and definition of the reference population. The following study outcomes were also extracted: patient characteristics (sociodemographics and medical history), incidence/prevalence estimates, all-cause and VWD-related mortality, time from symptoms onset to diagnosis, disease severity, disease progression, bleeding events at diagnosis and during follow-up, disease management/treatment used in clinical practice, health care resource utilization (HCRU), and health-related quality of life (HRQoL).
For each study, the methodology was assessed qualitatively. Specific attention was paid to the robustness of study methods and the generalizability of findings, and these results were used to inform data synthesis. Risk-of-bias tools were not used.
Results of the systematic review were synthesized qualitatively; there was no pooling of estimates through a meta-analysis. For prevalence, incidence, and mortality, a range of estimates was reported according to country/region. Ranges of estimates were provided, and outliers identified using qualitative appraisal and reason for outlying estimates qualitatively assessed; no statistical tests were conducted. Details regarding characteristics of patients and natural history of disease were reported according to VWD type, if available. The burden of illness was described in terms of HCRU and impact of the disease on patients’ HRQoL.
Results
Study Selection
A total of 3095 references were identified through the combined search of electronic bibliographical databases (Medline n = 735, Embase n = 2360). Following removal of duplicates, titles/abstracts of 2671 unique references (Supplemental Table 1) were screened independently by two assessors and 2368 references were excluded. Of the 303 full-text articles assessed for eligibility, 136 met the eligibility criteria; a further 32 references were identified through pragmatic searches (Supplemental Table 2). Thus, 168 sources (ie, unique references) (Supplemental Table 3) were retained for this systematic review (Figure 1).
 |
Figure 1 Flow chart for the identification and selection of published sources included for this systematic review. *Independently by two assessors. |
VWD Epidemiology
Prevalence
Estimates of the prevalence of VWD (overall or by specific type) were available from 22 of the 168 sources and varied according to the method of estimation. Referral-based estimates were derived from the number of symptomatic patients attending hemophilia treatment centers or health care facilities based on national registries or surveillance studies. Population-based estimates relied on the identification of patients with VWD in cohort studies based on specific diagnostic criteria.
Multinational estimates for VWD (all types) were reported from two global sources, and a cross-sectional study conducted in Western Europe and Israel. Based on expert opinion, Orphanet reported that globally 0.6–1.3% of the general population was affected by VWD (unspecified data source and time period), and that the prevalence of symptomatic VWD was approximately 10 per 100,000.9 The 2019 annual global survey of the World Federation of Hemophilia yielded a referral-based estimate of 1.5 per 100,000 based on the number of patients (with all types of VWD) registered in hemophilia treatment centers.10 The European cross-sectional study yielded a population-based estimate of 0.05 per 100,000 for type 3 VWD.11
Country-specific prevalence estimates for VWD were reported from 17 sources: five from Europe, three from Americas, and nine from other regions (Table 2). Referral-based prevalence estimates for overall VWD ranged from 4.4 to 16.5 per 100,000 in Europe,12–16 from 0.1 to 8.8 per 100,000 in Western Pacific,17–21 and from 1.8 to 2.0 per 100,000 in Eastern Mediterranean22,23 (Table 2). Referral-based data were also available for the Czech Republic24 and the USA;25 however, as sizes of the catchment populations were not reported, prevalence could not be estimated.
 |
Table 2 Reported Country-Based Prevalence Estimates of VWD (17 Sources) |
Estimates by VWD type were available from two registries in Europe (Italy12 and the UK15) and one registry in the Western Pacific (Australia18,26). Each of these sources reported higher prevalence estimates for type 1 disease than type 2 or type 3: 2.7–7.2 per 100,000 for type 1 VWD, 0.8–2.5 per 100,000 for type 2, and 0.1–0.3 per 100,000 for type 3. Higher prevalence estimates were also reported for adults than for children in the National Register of Congenital Coagulopathies in Italy.12
Population-based estimates, which were mostly conducted in pediatric populations, were higher than referral-based estimates, varying between 800 and 1000 per 100,000 in Europe,27,28 1500 per 100,000 in Eastern Mediterranean,29 108.9 and 1300 per 100,000 in the Americas,30,31 and 2200 per 100,000 in Africa.32
Incidence
Referral-based incidence estimates of VWD according to the United Kingdom Haemophilia Centre Doctors’ Organisation (UKHCDO) report, based on the National Hemophilia Database, were 0.6 (all subtypes), 0.3 (type 1 VWD), 0.2 (type 2 VWD), and 0.01 (type 3 VWD) per 100,000.15 There were no incidence estimates found for the Americas, Eastern Mediterranean, Western Pacific, or Africa regions. The Orphanet database reported that the incidence rate of type 3 VWD varied across countries from 0.05 to 0.1 per 100,000 person-years in Europe and the USA; sources of estimates and time period were not reported.33
Patient Demographic Characteristics
Reported demographic characteristics of patients with VWD are presented in Table 3. Patients diagnosed with VWD were predominantly white, with a blood group O and a family history of VWD or other bleeding disorder. The proportion of female patients with VWD (all types) ranged from 45% to 68%.10,12,13,15,18,19,22,24,25,28–31,34–48
 |
Table 3 Reported Patient Demographic Characteristics |
Mortality and Causes of Death
Mortality rates were available from seven sources (Supplemental Table 4);15,36,41,44,46,48–51 none of the publications reported mortality according to VWD type. Based on studies conducted in Sweden and the USA, VWD does not appear to be associated with an increased risk of death compared with populations without VWD. In a cohort study including 2790 patients with VWD in Sweden, all-cause mortality over a 22-year observation period (1987–2009) was estimated at 10.8% (equivalent to 235 per 100,000 person-years), and the risk of death in patients with VWD was not statistically different from that of age- and sex-matched individuals without VWD (hazard ratio 0.90; 95% confidence interval [CI], 0.80–1.05).49 All-cause mortality in a single-center cohort study (1985–2010) conducted in the USA was 5.1% in 198 patients with VWD compared with 2.0% in 198 patients without VWD matched for age, sex, and cardiovascular comorbidities (P = 0.1).48 A lower inpatient mortality rate was reported for adult patients with VWD (7556 admissions) than for those without VWD (19,918,970 admissions) in a retrospective US cohort study (2009–2011) using inpatient discharge data (1.3% vs 2.2% [P < 0.0001]).41,46 Another retrospective cohort study (2003–2011) using the same database, and focusing on pregnant women, found similar inpatient mortality rates for women with (n = 15,258) or without VWD (n = 40,602,254; 0.03% vs 0.02%, respectively [P = 0.970]).51
Other studies have reported mortality rates for 11,120 patients with VWD newly registered at hemophilia centers in the UK (0.6% over period of April 2019 to March 2020),15 161 children aged <18 years in Turkey (1.2% over period of 1985–2017),44 and 506 pregnant women in the USA (0% over period of 2007–2011).50
Data on cause of death were limited to two publications. In a retrospective US single-center cohort study (1985–2010), among 10 deaths in 198 patients with VWD, 7 were due to cancer or cancer-related complications.48 In the UK, among 69 deaths in patients with VWD (n = 11,120) recorded in the UKHCDO (2019–2020), carcinoma (7.2%) and bacterial infection (2.9%) were the most common known cause of death; the majority (79.7%) of deaths had an unknown cause.15
Burden of Illness
In total, 36 sources were identified that described bleeding events and disease-related complications. The burden of illness was also described in eight sources that reported on HRQoL and nine that reported on the HCRU of patients with VWD.
Timing of VWD Diagnosis
The time from onset of symptoms to VWD diagnosis was poorly documented in the literature, with only two sources being identified. One source was a retrospective US cohort study, which was based on administrative claims data (N = 18,182) and estimated the mean time from the first billing claim for a bleeding event to a VWD diagnosis as 669 days (range, 2–3284 days).52 The second source was a European retrospective cohort study based on medical records for 103 patients with severe VWD from 2010 to 2013 in which the estimated median time between the first bleeding event and VWD diagnosis was 3 years (interquartile range [IQR] 0–18).38
Bleeding Events and Disease-Related Complications
Patients with VWD frequently experience bleeding events. Based on data collected from patient questionnaires or chart reviews, between 72% and 94% of the patients had a history of bleeding events.40,44,53 Bleeding events commonly occurred at mucocutaneous sites (Table 4), with epistaxis, HMB, and oral/gum bleeding being the most frequently reported events in the overall VWD population.
 |
Table 4 Reported Disease-Related Complications |
HMB occurred frequently, affecting 61–100% of the women of reproductive age with VWD.23,31,34,42,44,54–58 Lower estimates (43% and 53%) were found in studies that used medical records.47,59 Postpartum hemorrhage occurred less frequently than HMB, occurring in 5.5–12.7% of the deliveries in women with VWD.42,47,50,59–63 Miscarriages were reported in 3–29% of the pregnant women with VWD.64–66 Rates of anemia and iron deficiency in women with VWD (including pregnant women) ranged from 13% to 21.4%50,52,65 and 4.2 to 22.5%.67,68
Wound-related bleeding was also a common non-spontaneous type of bleeding event that was reported in 38–79% of the patients.28,34,37,42,54,55,57,58 Post-surgical bleeding events occurred in 2.4–71.9% of the patients with VWD,31,34,37,47,54,56,58,59 with the highest rate observed in patients aged 65–85 years in a sub-analysis of the cross-sectional von Willebrand in the Netherlands (WiN) study.37 Gastrointestinal (GI) bleeding events were reported in 3.7–24% of the overall VWD population, with studies indicating that these events occur less frequently in the pediatric population.23,34,37,42–45,47,54,56,58,59,62,69,70 The reported proportions of patients who experienced joint bleeds34,39,71–73 or hemarthrosis23,37,39,42,44,47,56,58,62,71,73 were heterogenous across the identified studies, ranging from 6.3% to 32.3% and 3.8% to 38%, respectively. Bleeding events occurring in the central nervous system were rarely reported.34,37,44,55–58,69
Bleeding Score
In total, bleeding scores (BSs) in patients with VWD (all types) were reported in eight studies.24,37,53,55,57,58,72,74 In the Dutch WiN study (N = 666), the Tosetto BS varied from 10 to 12 in patients with VWD (aged ≥16 years) (normal Tosetto BS score defined as <3).37,53,55 In a subgroup analysis of the WiN study that focused on 113 pediatric patients with VWD (aged 0–15 years), the median BS assessed according to the International Society on Thrombosis and Hemostasis Bleeding Assessment Tool (ISTH-BAT) was 9.0 (IQR 5.0–12.5) (normal range defined as <3 in children).57 In a Canadian study that included 100 pediatric patients with VWD (aged <18 years), the median (range) Pediatric Bleeding Questionnaire (PBQ) score was estimated to be 7.0 (0–29) (PBQ score of ≥2 is predictive of VWD diagnosis).74
BSs were higher/worse in patients with type 2 or 3 than in those with type 1 VWD. In the Dutch WiN study, the median (range) Tosetto BS for patients with either type 1 or type 2 VWD was 10 (−1 to 31) and 13 (0–33), respectively, compared with 19.5 (2–35) in patients with type 3 VWD.55 Similarly, in the pediatric subgroup analysis of the WiN study (aged 0–15 years), median (IQR) ISTH-BAT score was 6.5 (4.0–10.0), 10.5 (6.3–12.8), and 17.0 (11.5–25.5) for patients with type 1, 2, or 3 VWD, respectively.57 In the Canadian study, median (range) PBQ score was estimated to be 9 (2–18) for type 1 VWD, 14 (3–17) for type 2 VWD, and 12 (4–29) for type 3 VWD.74
Comorbidities
Cardiovascular-Related Comorbidities
Eight sources reported estimates of cardiovascular comorbidities in patients with VWD.37,41,46,48,50,64,69,75 The reported proportions of patients with cardiovascular disease (CVD) in the overall VWD population were 15%41,46 and 31%37 based on two sources; reported hypertension rates ranged from 20.0% to 64.8% in patients >16 years of age.37,41,46,48,64,75 In a retrospective US cohort study based on hospital discharge data, the proportion of patients with at least one CVD or hypertension was lower in patients with (7556 admissions) versus without (19,918,970 admissions) VWD (15% vs 26% [P < 0.001] and 37.4% vs 49.4% [P < 0.0001], respectively).41,46 In a US single-center case–control study involving 198 patients with VWD, atrial fibrillation was reported in 7.6% and hypertension in 37.4% of the patients.48 In the Dutch WiN study involving 536 adult patients (aged ≥16 years) with type 1 or 2 VWD (type 3 excluded), the comorbidities of hypertension, hypercholesterolemia, and history of arterial thrombotic events were reported in 21.8%, 9.5%, and 4.3% of the patients, respectively.75
Digestive System-Related Comorbidities
In a subgroup analysis of the Dutch WiN study focusing on elderly patients with VWD (aged 65–85 years, n = 71), 15.5% of the patients had GI diseases.37 In the retrospective US study based on discharge data, the proportion of patients with liver disease was higher in the population of patients with (7556 admissions) versus without (19,918,970 admissions) VWD (1.0% vs 0.8% [P = 0.0458]).41 Chronic liver disease was also reported in 1.9% of the adult patients with type 1 or 2 VWD (n = 536) in the WiN study.75
Blood-Borne Diseases
The rate of infections with hepatitis B virus in patients with VWD was 0–1.5% across the identified studies.23,24,37 Across six studies, the rate of human immunodeficiency virus (HIV) and hepatitis C virus (HCV) infections in patients with VWD were reported at 0.1–0.4% and 1.1–3.8%, respectively.10,12,16,25,41,71 In the retrospective US study, the proportion of patients with HCV was higher in patients with (7556 admissions) versus without (19,918,970 admissions) VWD (3.8% vs 1.8% [P < 0.0001]), whereas the proportion with HIV infection was lower in patients with VWD versus without VWD (0.4% vs 0.8% [P = 0.0001]).41
Metabolic and Endocrine Comorbidities
The rates of metabolic and endocrine comorbidities in patients with VWD were reported in five studies.41,46,48,50,59,69,75 Rates of hypothyroidism ranged from 2.4% in the Dutch WiN study in patients with type 1 or 2 VWD (n = 536)75 to 16.2% in the US single-center case–control study involving all types of VWD (n = 197); this latter rate was significantly higher than in patients without VWD (5.6%, P < 0.0001).48,59 In the overall VWD population, reports of diabetes mellitus in three studies ranged from 6.7% to 16.2%,41,48,50 whereas 3.7% of the patients with type 1 or 2 VWD (n = 536) had diabetes mellitus in the WiN study.75 In the retrospective US study, the proportion of patients with diabetes mellitus and obesity was lower in patients with (7556 admissions) versus without (19,918,970 admissions) VWD (13.5% vs 23.4% [P < 0.0001] and 9.2% vs 10.0% [P = 0.028], respectively).41
Other Comorbidities
Across three studies, cancer rates ranged from 4.3% (in patients aged ≥16 years with type 1 or 2 VWD) to 23.9% (in patients aged 65–85 years with all VWD types); rates based on self-reporting by patients tended to be lower than those based on medical chart review.37,75,76 Across the studies identified through the systematic review, none reported on comorbidities involving renal, skin, allergic, or hypersensitivity disorders in patients with VWD.
Health-Related Quality of Life
Eight studies assessed HRQoL in patients with VWD (Table 5).39,40,67,73,77–82 VWD was associated with lower/poorer HRQoL scores than reference or general populations in three of these studies. In children aged 0–5 years (n = 46) from the Dutch WiN study, mean (SD) scores for general health perception (70 [15] vs 79 [15]) and parental time (83 [27] vs 93 [11]) from the Infant/Toddler Quality of Life (ITQOL) questionnaire were lower than those reported in the reference population (Dutch preschool children without VWD).77 Similarly, in children aged 6–15 years (n = 87), physical functioning (96 [13] vs 99 [4]), role functioning–emotional/behavioral (95 [15] vs 98 [7]), general health perceptions (76 [20] vs 83 [13]), and physical summary (54 [8] vs 56 [6]) scores from the Child Health Questionnaire Parent Form 50 (CHQ-PF50) and Child Form 87 (CHQ-CF87) were lower than those for the reference population.77 A Swedish retrospective study (N = 29) reported significantly lower median scores in the 36-item Short Form Health Survey (SF-36) for bodily pain in women with VWD and HMB than in those women from the general population.82 In a Canadian cross-sectional study, adult patients (aged ≥18 years) with VWD (N = 102) were found to have significantly lower scores (P < 0.05) in all SF-36 domains (except role–emotional limitations), compared with age- and sex-normative data from the general population.80 The physical (PCS) and mental component summary (MCS) scores were also significantly lower (by 2.4 and 3.9 points, respectively [P < 0.0.05]) than the general population.80
 |
Table 5 Reported HRQoL Outcomes in Patients with VWD |
Data from the Dutch WiN study also showed that within the patient population with VWD (n = 804), HRQoL (based on SF-36 scores) was poorer in patients with joint bleeding than in those without these clinical symptoms/conditions (PCS, 73 vs 77 [P = 0.005]; MCS, 47 vs 50 [P = 0.006]).39 In another analysis from the WiN study, patients with VWD and joint bleeding (n = 48) had significantly higher (worse) hemophilia joint health scores (HJHS; median total score 5 [IQR 1–15] vs 1.5 [IQR 0–5]; P < 0.01) and more functional limitations on the Hemophilia Activities List (HAL) (median total score 88 [IQR 69–98] vs 100 [IQR 87–100]; P < 0.01) than patients with VWD but without joint bleeding (n = 48).79,81
Based on data from the Universal Data Collection, a surveillance system funded by the US Centers for Disease Control and Prevention, 4.3% of the children with VWD (aged 2–12 years, n = 2712) used a cane, crutches, walker, or wheelchair for mobility assistance, with this rate higher in patients with type 3 VWD than in those with type 1 or 2 (22.6% vs 3.3% or 3.5%, respectively).40
Health Care Resource Utilization
The burden of VWD on outpatient/emergency department visits and hospitalizations was reported in nine studies (Table 6). No publications reporting on admissions to intensive care units were identified. In a Swedish population-based case–control study, a twofold increase in the rate of outpatient hospital visits and hospitalizations was recorded in patients with VWD (n = 2790) compared with age- and sex-matched controls (n = 5 controls per case).83 In this study, the most common causes of outpatient visits were menorrhagia and epistaxis, and GI bleeding was the most common cause of hospitalizations. A retrospective cohort study based on US administrative claims data (N = 5058) also showed that patients with VWD and major bleeding events were significantly (P < 0.0001) more likely to be admitted to hospital (incidence rate ratio [IRR] 3.2; 95% CI, 2.8–3.8) and to have emergency department (IRR 2.0; 95% CI, 1.8–2.3) and outpatient visits (IRR 1.3; 95% CI, 1.2–1.3) than patients with VWD who had no major bleeding events.69 In another retrospective cohort study based on US administrative claims data in patients undergoing major surgery, IRRs for the patients with VWD (n = 2972) were 1.2 (95% CI, 1.1–1.2; P < 0.0001) for outpatient visits and 1.4 (95% CI, 1.3–1.6; P < 0.0001) for emergency department visits in comparison to the patients without VWD.84
 |
Table 6 Reported Outpatient Visits, Emergency Department Visits, and Hospitalizations for Patients with VWD |
VWD Disease Management
Data on VWD treatment with an unspecified indication (ie, on-demand, surgery, or prophylaxis) were available from seven sources.15,24,34,62,85,86 The main products and doses used in clinical practice are summarized by indication in Table 7. Patterns of on-demand treatment for VWD were reported in 12 sources. On-demand treatments included desmopressin, replacement therapy with VWF (including VWF/FVIII concentrates), antifibrinolytics, and blood transfusion.38,51,63,72,85,87–91 There were 17 sources reporting on the use of situational/conditional prophylaxis (ie, for surgical procedures or childbirth), and nine sources on the use of long-term prophylaxis. Treatments for situational/conditional prophylaxis included desmopressin, plasma-derived VWF and VWF/FVIII-containing concentrates (as monotherapy or in combination), recombinant VWF, and tranexamic acid.61,73,85,88,92–94 Plasma-derived VWF/FVIII and VWF concentrates were used for long-term prophylaxis (Table 7).81,91,92,95–101 The age, sex, and type of VWD of patients receiving long-term prophylaxis varied across studies: median age was 15.9–60 years;92,95,96,98,100 more than half were male;95,97,99,100 and 3.1–12.5% had VWD type 1, 17.6–46.9% type 2, and 40.6–74.5% type 3.92,95–97,99,100,102 Indications for long-term prophylaxis were reported in eight studies: joint bleeding in 13–43.8%, epistaxis or oral bleeding in 23–34.4%, and GI bleeding in 6.3–63.6% of patients with VWD in general, and HMB in 5–21.9% of the women with VWD.92,95–100,102
 |
Table 7 Disease Management in the Real-World Clinical Practice Setting |
Discussion
This systematic review shows that there are limited data available on the epidemiology of VWD, indicating the need for more research to be conducted. Prevalence data that were identified varied depending on method, region/country, VWD type, and patient age.9–23,27–32 Incidence data were limited to two sources.15,33 The systematic review also highlighted high disease burden, with a high proportion of patients with VWD reporting a history of bleeding events.23,28,31,34,37,39,42–45,47,54–63,67,68,70–73 Patients with VWD were also reported to have lower/poorer HRQoL scores versus general populations,77,80,82 as well as increased HCRU.83,84
VWD prevalence estimates varied highly according to the study populations and method of estimation. Population-based estimates were higher than referral-based estimates (108.9–2200 per 100,00027–32 vs 0.1–16.5 per 100,0009,10,12–15,17–23). This is perhaps not surprising given that the population-based studies mostly involved healthy school children or college students (aged ≤35 years) or unselected children (aged ≤18 years) attending one or more local hospitals.27–32 By contrast, the referral-based studies (with the exception of two cross-sectional studies22,23) identified symptomatic patients of all ages in national registry programs or surveillance databases.10,12–15,17–20 Therefore, the population-based studies are more likely to identify a greater number of patients with VWD, with less severe bleeding symptoms, than referral-based studies identifying symptomatic patients seeking care for VWD in specialist centers. The wide range in population-based estimates reflects variations in population size (N = 182–4592), as well as in timescale (study periods varied across a range of years from around 1985 to 2018 [exact timing not provided for study by Rodeghiero et al]).27–32 Definitions used to identify patients with VWD in the population-based studies also varied. Whereas all six population-based studies providing estimates for VWD overall27–32 included VWF levels with or without FVIII levels in the definition, the presence of bleeding symptoms was only required in three studies.28,30,31 Variations in referral-based estimates likely reflect several factors, including diagnostic facilities, physician awareness, subtype of VWD, and/or severity of bleeds.
Estimates of VWD prevalence also varied by disease type, age, and sex. Prevalence was lower in pediatric than in adult populations,12 which could reflect the accumulation of non-fatal cases or increased diagnosis in adulthood. Type 3 VWD was the rarest reported (0.1–0.3 per 100,000), followed by type 2 VWD (0.8–2.5 per 100,000), and type 1 VWD (2.7–7.2 per 100,000).12,15,18 Reports suggest that more women than men are affected by VWD globally, despite VWD having an autosomal inheritance pattern.5 This may be because VWD is diagnosed more often in women due to female-specific hemostatic challenges such as HMB and intra-/postpartum bleeding. The studies reviewed suggest that HMB occurs frequently (>60%) in patients with VWD,23,31,34,42,44,54–58 while postpartum bleeding can occur in up to 13% of women with VWD.42,47,50,59–63
This systematic review also suggests that there are important gaps in VWD diagnosis that could delay care and result in adverse health outcomes. Although the time from symptom development to diagnosis was poorly documented in the literature,38,52 the 3-year difference between median age at overt symptom onset and median age at diagnosis reported in this review38 highlights the need for improved disease awareness for both patients and health care providers. According to international guidelines for VWD diagnosis, an accurate and timely diagnosis remains a major challenge for patients with VWD, with barriers identified as difficulties in distinguishing between normal and abnormal bleeding symptoms, limited clarity regarding an appropriate diagnostic approach, and limited access to specialized laboratory testing.103 To facilitate VWD diagnosis, the multidisciplinary review panel recommended the use of bleeding-assessment tools in patients suspected of having VWD in a primary care setting to help identify patients who require laboratory testing, as well as specific diagnostic approaches for types 1 and 2 VWD.103
Patients with VWD had a high burden of bleeding events even after VWD diagnosis or if receiving VWD treatment. Bleeding was reported in 72–94% of the patients with VWD,40,44,53 with mucocutaneous bleeds such as menorrhagia, GI bleeds, epistaxis, and oral bleeds being the most frequent.23,28,31,34,37,39,42–45,47,54–63,67,68,70–73,84 Life-threatening bleeding involving critical organs (eg, central nervous system34,37,44,55,69) were also reported, although these were rare and studies have not found a difference in mortality between VWD and general populations.41,46,48,49,51 Only one study compared bleeding rates across all three VWD types.34 In this retrospective Italian study (N = 1234), GI bleeding was more common in patients with types 2A or 3, central nervous system and joint bleeding events in those with type 3, and hematomas in patients with types 2N and 3, relative to other VWD types. However, the frequency of mucosal bleeding (epistaxis, HMB, and gum bleeding) did not differ significantly across VWD types. Lower bleeding rates were reported in studies that used medical records (vs those using questionnaires) or focused on specific patient populations, which suggests that bleeding events are not always reported or captured in medical records. Only one study used a validated bleeding assessment tool (the ISTH-BAT) completed by the physician to evaluate bleeding rates.57 Bleeding assessment tools provide a standardized approach to assessment and can educate patients and physicians regarding bleeding symptoms and possible interventions.103
The reported real-world treatment patterns show a range of treatment options with respect to VWD types and severity,92,95–97,99,100,102 with only a small proportion of patients with VWD reported to be receiving long-term VWF prophylaxis in a multinational VWD Prophylaxis Network study and in the Czech National Hemophilia Programme registry (0.7% and 1.6%, respectively).24,102 Long-term prophylaxis was administered most often in patients with type 3 VWD,92,95–97,99,100,102 and mostly for joint or GI bleeding.92,95–100,102 The current VWD management guidelines conditionally recommend long-term prophylaxis for patients with VWD and a history of severe and frequent bleeds.4 The guideline panel, however, acknowledged the low certainty of evidence for a net health benefit for long-term prophylaxis in this population. Thus, future research is needed to better understand bleeding outcomes and unmet needs of patients with VWD who may benefit from long-term prophylaxis.
Findings from the identified sources also suggest that VWD is associated with poorer HRQoL scores77,80,82 as well as higher HCRU83,84 compared with general populations. A variety of measurements were used across the eight studies evaluating HRQoL, including quality-of-life measures (SF-36 in adults, and ITQOL, CHQ-PF50, and CHQ-CF87 in children), and joint health measures (HJHS and HAL).39,40,67,73,77–82 In children, scores for physical functioning, emotional/behavioral functioning, and general health perceptions were lower than in children without VWD,77 while in adults, both SF-36 PCS and MCS scores were lower than the general population.80 All nine studies reporting HCRU were observational studies,36,38,40,41,46,57,69,83,84,90 mostly retrospective cohort studies. Although not covered by this review, decreased HRQoL and increased HCRU would be expected to have a substantial economic and societal impact. Studies evaluating VWD prophylaxis continue to demonstrate reductions in HCRU, such as hospitalizations,83,104 further supporting the overall benefit of long-term prophylaxis for eligible patients.
Limitations
Large variations in outcomes reported in this review reflect the heterogeneity of bleeding phenotype in VWD, as well as variability in study populations and research methodologies. Differences in disease awareness, diagnosis, and clinical management of VWD across the large geographic areas and different time periods covered by this review will also have contributed to the heterogeneity of the data.
Some relevant sources may not be captured in this review if they were not indexed in the electronic bibliographic databases used for this literature search, not classified under the MeSH or Emtree terms, or did not contain the keywords used in the search. To mitigate this limitation, the comprehensiveness of the search strategy was verified against articles known to be pertinent for the search. Keywords were reverse generated using a sample of articles deemed relevant for the review. Furthermore, some relevant sources may not have been captured in the systematic literature search, as some sources do not publish their studies in peer-reviewed journals. To mitigate this limitation, pragmatic searches of the gray literature as well as “snowballing” were conducted. Single-entry data extraction was employed for this systematic review. However, the completeness of the data was assessed by a separate reviewer.
Summary
This systematic review highlights the limited data available on the epidemiology of VWD, as well as the high disease burden and related impact on HRQoL and HCRU for patients with VWD. More real-world studies are needed to better understand the characteristics of VWD patient populations and help inform timely VWD diagnosis and care.
Data Sharing Statement
The datasets, including the template data extraction form and data extracted from the included studies, are available upon request from corresponding author, Ping Du.
Acknowledgments
The authors thank Teigna Arredondo-Bisono who provided support in the protocol development, data extraction, and analysis. Under the direction of the authors, medical writing support was provided by Joanne Vaughan, Excel Medical Affairs (Fairfield, CT, USA), and was funded by Takeda Development Center Americas, Inc., Lexington, MA, USA.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Shire Human Genetic Therapies, Inc, a Takeda company, Lexington, MA. The sponsor was involved with the protocol development, analysis of identified sources and interpretation of findings, report development, and in the decision to submit the article for publication.
Disclosure
PD, GÖ, and ST are employees of Takeda Development Center Americas, Inc., and Takeda stockholders. AB and YM are employees of YOLARX Consultants and received fees from Shire Human Genetic Therapies, Inc., a Takeda company, for conducting this analysis. FTB is an employee of Takeda Pharmaceuticals International AG, and a Takeda stockholder. The authors report no other conflicts of interest in this work.
References
1. Gralnick HR, Williams S, McKeown L, et al. A monomeric von Willebrand factor fragment, Leu-504--Lys-728, inhibits von Willebrand factor interaction with glycoprotein Ib-IX [corrected]. Proc Natl Acad Sci U S A. 1992;89(17):7880–7884. doi:10.1073/pnas.89.17.7880
2. Sadler JE, Budde U, Eikenboom JC, et al. Update on the pathophysiology and classification of von Willebrand disease: a report of the subcommittee on von Willebrand Factor. J Thromb Haemost. 2006;4(10):2103–2114. doi:10.1111/j.1538-7836.2006.02146.x
3. Weiss HJ, Sussman II, Hoyer LW. Stabilization of factor VIII in plasma by the von Willebrand factor. Studies on posttransfusion and dissociated factor VIII and in patients with von Willebrand’s disease. J Clin Invest. 1977;60(2):390–404. doi:10.1172/JCI108788
4. Connell NT, Flood VH, Brignardello-Petersen R, et al. ASH ISTH NHF WFH 2021 guidelines on the management of von Willebrand disease. Blood Adv. 2021;5(1):301–325. doi:10.1182/bloodadvances.2020003264
5. Leebeek FWG, Eikenboom JCJ. Von Willebrand’s disease. N Engl J Med. 2016;375(21):2067–2080. doi:10.1056/NEJMra1601561
6. Bowman M, Hopman WM, Rapson D, Lillicrap D, James P. The prevalence of symptomatic von Willebrand disease in primary care practice. J Thromb Haemost. 2010;8(1):213–216. doi:10.1111/j.1538-7836.2009.03661.x
7. Cochrane group. Cochrane handbook for systematic reviews of interventions. Available from: http://training.cochrane.org/handbook.
8. Institute of Medicine (IOM). Standards for systematic reviews. Available from: https://iom.nationalacademies.org/Reports/2011/Finding-What-Works-in-Health-Care-Standards-for-Systematic-Reviews/Standards.aspx.
9. Orphanet. Von Willebrand disease. Available from: https://www.orpha.net/consor/cgi-bin/OC_Exp.php?Lng=EN&Expert=903.
10. World Federation of Hemophilia. Report on the annual global survey; 2019. Available from: http://www1.wfh.org/publications/files/pdf-1806.pdf.
11. Mannucci PM, Bloom AL, Larrieu MJ, Nilsson IM, West RR. Atherosclerosis and von Willebrand factor. I. Prevalence of severe von Willebrand’s disease in Western Europe and Israel. Br J Haematol. 1984;57(1):163–169. doi:10.1111/j.1365-2141.1984.tb02876.x
12. Abbonizio F, Hassan HJ, Riccioni R, Santagostino E, Arcieri R, Giampaolo A. New data from the Italian National Register of congenital coagulopathies, 2016 annual survey. Blood Transfus. 2020;18(1):58–66. doi:10.2450/2019.0211-18
13. FranceCoag. National statistics: von Willebrand disease. Available from: https://www.francecoag.org/SiteWebPublic/public/stats/stats_page.jsp?stat1=on&stat4=on.
14. Giampaolo A, Abbonizio F, Arcieri R. Italian national registry of congenital coagulopathies. Blood Transfus. 2020;18(3):s30.
15. United Kingdom Haemophilia Centre Doctors’ Organisation (UKHCDO). UKHCDO annual report 2020 & bleeding disorder statistics for the financial year 2019/2020; 2020.
16. Giampaolo A, Abbonizio F, Arcieri R, Hassan HJ. Italian registry of congenital bleeding disorders. J Clin Med. 2017;6(3):34. doi:10.3390/jcm6030034
17. Korea Hemophilia Foundation (KHF). Current Status. Available from: http://www.kohem.org/eng/load.asp?subPage=310.
18. National Blood Authority of Australia. Australian bleeding disorders registry: annual report 2018-19; 2019. Available from: https://www.blood.gov.au/system/files/ABDR-Annual-Report-2018-19-FINAL.pdf.
19. Tatsunami S, Kuwabara R, Akita M, Mimaya J, Shirahata A, Taki M. Number of patients with coagulation disorders in Japan’s 2010 annual report from the research committee for the national surveillance on coagulation disorders in Japan. Haemophilia. 2012;18(3):84.
20. Yoon HS, Han Y, Kim YJ, et al. Epidemiology of congenital bleeding disorders: a nationwide population-based Korean study. J Korean Med Sci. 2020;35(39):e350. doi:10.3346/jkms.2020.35.e350
21. Qu Y, Nie X, Yang Z, et al. The prevalence of hemophilia in mainland China: a systematic review and meta-analysis. Southeast Asian J Trop Med Public Health. 2014;45(2):455–466.
22. Alkaabi S, Alzadjali A, Wasifuddin M, et al. Spectrum, clinical characteristics and outcome of von Willebrand disease in Oman. Haemophilia. 2020;26(Suppl 2):142.
23. Mansouritorghabeh H, Manavifar L, Banihashem A, et al. An investigation of the spectrum of common and rare inherited coagulation disorders in north-eastern Iran. Blood Transfus. 2013;11(2):233–240. doi:10.2450/2012.0023-12
24. Blatný J, Ovesná P The status of care for persons with von Willebrand disease registered within CNHP registry annual report; 2019. Available from: https://www.cnhp.cz/res/file/vysledky/cnhp_2019_vwd_print.pdf.
25. Centers for Disease Control and Prevention. HTC population profile patient characteristics. Available from: https://www.cdc.gov/ncbddd/hemophilia/communitycounts/data-reports/2020-9/table-1-patient-characteristics-by-calendar.html.
26. The World Bank. Population, Total – Australia; 2019. Available from: https://data.worldbank.org/indicator/SP.POP.TOTL?locations=AU.
27. Rodeghiero F, Castaman G, Dini E. Epidemiological investigation of the prevalence of von Willebrand’s disease. Blood. 1987;69(2):454–459.
28. Sap F, Kavakli T, Kavakli K, Dizdarer C. The prevalence of von Willebrand disease and significance of in vitro bleeding time (PFA-100) in von Willebrand disease screening in the Izmir region. Turk J Haematol. 2013;30(1):40–47. doi:10.4274/tjh.2011.0020
29. Abu-Douleh E, Al-Numair N, Albanyan A, Alsuliman A, Bayoumi N, Owaidah T. Prevalence of von Willebrand disease among university students in Riyadh, Saudi Arabia. J Appl Hematol. 2018;9(4):136–139. doi:10.4103/joah.joah_63_18
30. Bowman M, Hopman WM, Rapson D, Lillicrap D, Silva M, James P. A prospective evaluation of the prevalence of symptomatic von Willebrand disease (VWD) in a pediatric primary care population. Pediatr Blood Cancer. 2010;55(1):171–173. doi:10.1002/pbc.22429
31. Werner EJ, Broxson EH, Tucker EL, Giroux DS, Shults J, Abshire TC. Prevalence of von Willebrand disease in children: a multiethnic study. J Pediatr. 1993;123(6):893–898. doi:10.1016/s0022-3476(05)80384-1
32. Shonde-Adebola KB, Shokunbi WA, Adebola MB. Prevalence of von Willebrand disease among Nigerian youths in Ibadan South-Western Nigeria. OALib. 2021;8:e7789. doi:10.4236/oalib.1107789
33. Orphanet. Von Willebrand disease type 3. Available from: https://www.orpha.net/consor/cgi-bin/OC_Exp.php?lng=en&Expert=166096.
34. Federici AB, Bucciarelli P, Castaman G, et al. Management of inherited von Willebrand disease in Italy: results from the retrospective study on 1234 patients. Semin Thromb Hemost. 2011;37(5):511–521. doi:10.1055/s-0031-1281037
35. Federici AB, Bucciarelli P, Castaman G, et al. The bleeding score predicts clinical outcomes and replacement therapy in adults with von Willebrand disease. Blood. 2014;123(26):4037–4044. doi:10.1182/blood-2014-02-557264
36. Holm E, Osooli M, Steen Carlsson K, Berntorp E. Cardiovascular disease-related hospitalization and mortality among persons with von Willebrand disease: a nationwide register study in Sweden. Haemophilia. 2019;25(1):109–115. doi:10.1111/hae.13642
37. Sanders YV, Giezenaar MA, Laros-van Gorkom BA, et al. von Willebrand disease and aging: an evolving phenotype. J Thromb Haemost. 2014;12(7):1066–1075. doi:10.1111/jth.12586
38. Siboni SM, Biguzzi E, Caiani V, Mistretta C, Bucciarelli P, Peyvandi F. Baseline factor VIII plasma levels and age at first bleeding in patients with severe forms of von Willebrand disease. Haemophilia. 2016;22(4):564–569. doi:10.1111/hae.12900
39. van Galen KPM, Sanders YV, Vojinovic U, et al. Joint bleeds in von Willebrand disease patients have significant impact on quality of life and joint integrity: a cross-sectional study. Haemophilia. 2015;21(3):e185–e192. doi:10.1111/hae.12670
40. Abe K, Dupervil B, O’Brien SH, et al. Higher rates of bleeding and use of treatment products among young boys compared to girls with von Willebrand disease. Am J Hematol. 2020;95(1):10–17. doi:10.1002/ajh.25656
41. Apostolova MH, Seaman CD, Comer DM, Yabes JG, Ragni MV. Prevalence and risk factors associated with hypertension in von Willebrand disease. Clin Appl Thromb Hemost. 2018;24(1):93–99. doi:10.1177/1076029616670258
42. Kumar S, Kishore R, Gupta V, Jain M, Shukla J. Prevalence and spectrum of von Willebrand disease in Eastern Uttar Pradesh. Indian J Pathol Microbiol. 2010;53(3):486–489. doi:10.4103/0377-4929.68287
43. Mokhtar GM, Tantawy AA, Adly AA, Telbany MA, El Arab SE, Ismail M. A longitudinal prospective study of bleeding diathesis in Egyptian pediatric patients: single-center experience. Blood Coagul Fibrinolysis. 2012;23(5):411–418. doi:10.1097/MBC.0b013e3283540bf8
44. Öner N, Gürsel T, Kaya Z, et al. Inherited coagulation disorders in Turkish children: a retrospective, single-center cohort study. Transfus Apher Sci. 2020;59(3):102728. doi:10.1016/j.transci.2020.102728
45. Sahoo T, Naseem S, Ahluwalia J, Marwaha RK, Trehan A, Bansal D. Inherited bleeding disorders in North Indian children: 14 years’ experience from a tertiary care center. Indian J Hematol Blood Transfus. 2020;36(2):330–336. doi:10.1007/s12288-019-01233-3
46. Seaman CD, Yabes J, Comer DM, Ragni MV. Does deficiency of von Willebrand factor protect against cardiovascular disease? Analysis of a national discharge register. J Thromb Haemost. 2015;13(11):1999–2003. doi:10.1111/jth.13142
47. Trasi S, Shetty S, Ghosh K, Mohanty D. Prevalence and spectrum of von Willebrand disease from western India. Indian J Med Res. 2005;121(5):653–658.
48. Qureshi W, Hassan S, Dabak V, Kuriakose P. Thrombosis in VonWillebrand disease. Thromb Res. 2012;130(5):e255–e258. doi:10.1016/j.thromres.2012.09.005
49. Henriksson KM, Astermark J, Nilsson J-A, Baghaei F, Holmstrom M, Berntorp E. Survival among 5118 patients with bleeding disorders compared to matched controls in Sweden: results from a cohort register study. J Thromb Haemost. 2011;9(Suppl 2):222.
50. Malec LM, Moore CG, Yabes J, Li J, Ragni MV. Postpartum haemorrhage in women with von Willebrand disease: an observational study of the Pennsylvania Health Care Cost Containment Council (PHC4) database. Haemophilia. 2015;21(5):e442–e445. doi:10.1111/hae.12739
51. Mittal V, Ahuja S, Acharya C, Palabindala V, Milner C. Obstetric and bleeding complications in pregnancy with von Willebrand disease: results from nationwide inpatient sample database 2003–2011. Blood. 2017;130(1):3373.
52. Sidonio RF, Haley KM, Fallaize D. Impact of diagnosis of von Willebrand disease on patient outcomes: analysis of medical insurance claims data. Haemophilia. 2017;23(5):743–749. doi:10.1111/hae.13292
53. Tosetto A, Rodeghiero F, Castaman G, et al. A quantitative analysis of bleeding symptoms in type 1 von Willebrand disease: results from a multicenter European study (MCMDM-1 VWD). J Thromb Haemost. 2006;4(4):766–773. doi:10.1111/j.1538-7836.2006.01847.x
54. Chen YC, Yang L, Cheng SN, Hu SH, Chao TY. von Willebrand disease: a clinical and laboratory study of sixty-five patients. Ann Hematol. 2011;90(10):1183–1190. doi:10.1007/s00277-011-1266-4
55. de Wee EM, Sanders YV, Mauser-Bunschoten EP, et al. Determinants of bleeding phenotype in adult patients with moderate or severe von Willebrand disease. Thromb Haemost. 2012;108(4):683–692. doi:10.1160/TH12-04-0244
56. Lak M, Peyvandi F, Mannucci PM. Clinical manifestations and complications of childbirth and replacement therapy in 385 Iranian patients with type 3 von Willebrand disease. Br J Haematol. 2000;111(4):1236–1239. doi:10.1046/j.1365-2141.2000.02507.x
57. Sanders YV, Fijnvandraat K, Boender J, et al. Bleeding spectrum in children with moderate or severe von Willebrand disease: relevance of pediatric-specific bleeding. Am J Hematol. 2015;90(12):1142–1148. doi:10.1002/ajh.24195
58. Tosetto A, Badiee Z, Baghaipour MR, et al. Bleeding symptoms in patients diagnosed as type 3 von Willebrand disease: results from 3WINTERS-IPS, an international and collaborative cross-sectional study. J Thromb Haemost. 2020;18(9):2145–2154. doi:10.1111/jth.14886
59. Hassan S, Qureshi W, Donthireddy V, Kuriakose P. Congenital von Willebrand’s disease and clinical hypothyroidism. Haemophilia. 2013;19(2):242–245. doi:10.1111/hae.12065
60. O’Brien SH, Stanek JR, Kaur D, McCracken K, Vesely SK. Laboratory monitoring during pregnancy and post-partum hemorrhage in women with von Willebrand disease. J Thromb Haemost. 2020;18(3):604–608. doi:10.1111/jth.14696
61. Xu Z, Dargaud Y, Chamouard V, et al. A single-centre study of management of pregnant women with von Willebrand disease. Haemophilia. 2019;25(1):e54–e57. doi:10.1111/hae.13653
62. Majluf-Cruz A, Velez-Ruelas MA, Gonzalez-Avila AI, et al. von Willebrand’s disease in Mexico: a pilot study. Haemophilia. 2013;19(2):231–235. doi:10.1111/hae.12016
63. Wilson E, Hanna F, Hyppa A, et al. Assessment of von Willebrand disease and pregnancy outcomes at regional Australian hospitals. Eur J Haematol. 2021;106(4):456–466. doi:10.1111/ejh.13562
64. Skeith L, Rydz N, O’Beirne M, Goodyear D, Li H, Poon MC. Pregnancy loss in women with von Willebrand disease: a single-center pilot study. Blood Coagul Fibrinolysis. 2017;28(5):393–397. doi:10.1097/MBC.0000000000000620
65. Sladic M, Smrkolj S. The impact of von Willebrand’s disease on pregnancy, delivery and postpartum period: a population-based study. Eur J Obstet Gynecol Reprod Biol. 2019;234:E155.
66. Yousuf S, Cohen AJ, Eris E, Astsaturov A. A single institutional study on pregnancy outcomes in patients with von Willebrand disease. Blood. 2017;130(Suppl 1):1086. doi:10.1182/blood.V130.Suppl_1.1086.1086
67. Rae C, Furlong W, Horsman J, et al. Bleeding disorders, menorrhagia and iron deficiency: impacts on health-related quality of life. Haemophilia. 2013;19(3):385–391. doi:10.1111/hae.12014
68. Kaur D, Vesely SK, Koch T, O’Brien SH. Quality and consequences of laboratory monitoring for von Willebrand disease during pregnancy. Am J Hematol. 2018;93(9):E31–E32.
69. Lu M, Oladapo A, Wu Y, Farahbakhshian S, Ewenstein B. Economic burden of major bleeding events in commercially insured patients with von Willebrand disease based on claims data from the United States. J Manag Care Spec Pharm. 2021;27(2):175–185. doi:10.18553/jmcp.2020.20327
70. Tsagianni A, Comer DM, Yabes JG, Ragni MV. Von Willebrand disease and gastrointestinal bleeding: a national inpatient sample study. Thromb Res. 2019;178:119–123. doi:10.1016/j.thromres.2019.04.017
71. Haley KM, Sidonio RF, Abraham S, Cheng D, Recht M, Kulkarni R. A cross-sectional study of women and girls with congenital bleeding disorders: the American Thrombosis and Hemostasis Network cohort. J Womens Health. 2020;29(5):670–676. doi:10.1089/jwh.2019.7930
72. van Deukeren D, Mauser-Bunschoten EP, Schutgens REG, et al. The prevalence and burden of hand and wrist bleeds in von Willebrand disease. Haemophilia. 2019;25(1):e35–e38. doi:10.1111/hae.13632
73. van Galen KPM, Meijer K, Vogely HC, et al. Joint surgery in von Willebrand disease: a multicentre cross-sectional study. Haemophilia. 2016;22(2):256–262. doi:10.1111/hae.12834
74. Biss TT, Blanchette VS, Clark DS, et al. Quantitation of bleeding symptoms in children with von Willebrand disease: use of a standardized pediatric bleeding questionnaire. J Thromb Haemost. 2010;8(5):950–956. doi:10.1111/j.1538-7836.2010.03796.x
75. Atiq F, Meijer K, Eikenboom J, et al. Comorbidities associated with higher von Willebrand factor (VWF) levels may explain the age-related increase of VWF in von Willebrand disease. Br J Haematol. 2018;182(1):93–105. doi:10.1111/bjh.15277
76. Franchini M, Di Perna C, Santoro C, et al. Cancers in patients with von Willebrand disease: a survey from the Italian Association of Haemophilia Centres. Semin Thromb Hemost. 2016;42(1):36–41. doi:10.1055/s-0035-1564844
77. de Wee EM, Fijnvandraat K, de Goede-Bolder A, et al. Impact of von Willebrand disease on health-related quality of life in a pediatric population. J Thromb Haemost. 2011;9(3):502–509. doi:10.1111/j.1538-7836.2010.04175.x
78. McLaughlin JM, Munn JE, Anderson TL, Lambing A, Tortella B, Witkop ML. Predictors of quality of life among adolescents and young adults with a bleeding disorder. Health Qual Life Outcomes. 2017;15(1):67. doi:10.1186/s12955-017-0643-7
79. van Galen KPM, de Kleijn P, Foppen W, et al. Long-term impact of joint bleeds in von Willebrand disease: a nested case-control study. Haematologica. 2017;102(9):1486–1493. doi:10.3324/haematol.2017.168617
80. Xu Y, Deforest M, Grabell J, Hopman W, James P. Relative contributions of bleeding scores and iron status on health-related quality of life in von Willebrand disease: a cross-sectional study. Haemophilia. 2017;23(1):115–121. doi:10.1111/hae.13062
81. van Galen KPM, Timmer M, de Kleijn P, et al. Long-term outcome after joint bleeds in von Willebrand disease compared to haemophilia A: a post hoc analysis. Thromb Haemost. 2018;118(10):1690–1700. doi:10.1055/s-0038-1670704
82. Govorov I, Ekelund L, Chaireti R, et al. Heavy menstrual bleeding and health-associated quality of life in women with von Willebrand’s disease. Exp Ther Med. 2016;11(5):1923–1929. doi:10.3892/etm.2016.3144
83. Holm E, Carlsson KS, Lovdahl S, Lail AE, Abshire TC, Berntorp E. Bleeding-related hospitalization in patients with von Willebrand disease and the impact of prophylaxis: results from national registers in Sweden compared with normal controls and participants in the von Willebrand Disease Prophylaxis Network. Haemophilia. 2018;24(4):628–633. doi:10.1111/hae.13473
84. Oladapo A, Wu Y, Lu M, Farahbakhshian S, Ewenstein B. Estimation of the economic burden associated with major surgery due to von Willebrand disease based on claims data from the USA. Blood. 2019;134(1):4692.
85. Boban A, Lambert CM, Hermans C. VWF-FVIII concentrates in the treatment of inherited von Willebrand disease: a single-centre retrospective study. Haemophilia. 2019;25(4):e300–e303. doi:10.1111/hae.13779
86. De Wee EM, Knol HM, Mauser-Bunschoten EP, et al. Gynaecological and obstetric bleeding in moderate and severe von Willebrand disease. Thromb Haemost. 2011;106(5):885–892. doi:10.1160/TH11-03-0180
87. Batty P, Chen YH, Bowles L, Hart DP, Platton S, Pasi KJ. Safety and efficacy of a von Willebrand factor/factor VIII concentrate (Wilate(R)): a single centre experience. Haemophilia. 2014;20(6):846–853. doi:10.1111/hae.12496
88. Howman R, Barnes C, Curtin J, et al. The clinical efficacy and safety of the FVIII/VWF concentrate, BIOSTATE(R), in children with von Willebrand disorder: a multi-centre retrospective review. Haemophilia. 2011;17(3):463–469. doi:10.1111/j.1365-2516.2010.02445.x
89. Khair K, Batty P, Riat R, et al. Wilate use in 47 children with von Willebrand disease: the North London paediatric haemophilia network experience. Haemophilia. 2015;21(1):e44–e50. doi:10.1111/hae.12497
90. Livesey K, Yealy DM, Li J, Moore CG, Ragni MV. Von Willebrand disease in the emergency department. Haemophilia. 2016;22(2):263–267. doi:10.1111/hae.12841
91. Miesbach W, Krekeler S, Wolf Z, Seifried E. Clinical use of Haemate(R) P in von Willebrand disease: a 25-year retrospective observational study. Thromb Res. 2015;135(3):479–484. doi:10.1016/j.thromres.2014.12.017
92. Goudemand J, Bridey F, Claeyssens S, et al. Management of von Willebrand disease with a factor VIII-poor von Willebrand factor concentrate: results from a prospective observational post-marketing study. J Thromb Haemost. 2020;18(8):1922–1933. doi:10.1111/jth.14928
93. Govorov I, Lofgren S, Chaireti R, Holmstrom M, Bremme K, Mints M. Postpartum hemorrhage in women with von Willebrand disease - a retrospective observational study. PLoS One. 2016;11(10):e0164683. doi:10.1371/journal.pone.0164683
94. James AH, Konkle BA, Kouides P, et al. Postpartum von Willebrand factor levels in women with and without von Willebrand disease and implications for prophylaxis. Haemophilia. 2015;21(1):81–87. doi:10.1111/hae.12568
95. Abshire TC, Federici AB, Alvarez MT, et al. Prophylaxis in severe forms of von Willebrand’s disease: results from the von Willebrand Disease Prophylaxis Network (VWD PN). Haemophilia. 2013;19(1):76–81. doi:10.1111/j.1365-2516.2012.02916.x
96. Castaman G, Coppola A, Zanon E, et al. Efficacy and safety during formulation switch of a pasteurized VWF/FVIII concentrate: results from an Italian prospective observational study in patients with von Willebrand disease. Haemophilia. 2013;19(1):82–88. doi:10.1111/hae.12005
97. Federici AB, Gianniello F, Mannucci PM. Secondary long-term prophylaxis in von Willebrand disease: an Italian cohort study. Hematology Meeting Reports. 2005;1:6. doi:10.4081/hmr.v1i6.270
98. Federici AB, Barillari G, Zanon E, et al. Efficacy and safety of highly purified, doubly virus-inactivated VWF/FVIII concentrates in inherited von Willebrand’s disease: results of an Italian cohort study on 120 patients characterized by bleeding severity score. Haemophilia. 2010;16(1):101–110. doi:10.1111/j.1365-2516.2009.02088.x
99. Holm E, Abshire TC, Bowen J, et al. Changes in bleeding patterns in von Willebrand disease after institution of long-term replacement therapy: results from the von Willebrand Disease Prophylaxis Network. Blood Coagul Fibrinolysis. 2015;26(4):383–388. doi:10.1097/MBC.0000000000000257
100. Halimeh S, Krumpel A, Rott H, et al. Long-term secondary prophylaxis in children, adolescents and young adults with von Willebrand disease. Results of a cohort study. Thromb Haemost. 2011;105(4):597–604. doi:10.1160/TH10-09-0616
101. Berntorp E. Prophylaxis and treatment of bleeding complications in von Willebrand disease type 3. Semin Thromb Hemost. 2006;32(6):621–625. doi:10.1055/s-2006-949667
102. Berntorp E, Abshire T. The von Willebrand disease prophylaxis network: exploring a treatment concept. J Thromb Haemost. 2006;4(11):2511–2512. doi:10.1111/j.1538-7836.2006.02179.x
103. James PD, Connell NT, Ameer B, et al. ASH ISTH NHF WFH 2021 guidelines on the diagnosis of von Willebrand disease. Blood Adv. 2021;5(1):280–300. doi:10.1182/bloodadvances.2020003265
104. Schinco P, Cultrera D, Valeri F, et al. Cost-consequence analysis of long-term prophylaxis in the treatment of von Willebrand disease in the Italian context. Clinicoecon Outcomes Res. 2015;7:17–25. doi:10.2147/CEOR.S71892
105. Population Estimate as of January 1, 2021. Institut national de statistique et des études économiques (INSEE); 2021. Available from: https://www.insee.fr/fr/statistiques/1893198.
106. Weiss HJ, Ball AP, Mannucci PM. Incidence of severe von Willebrand’s disease. N Engl J Med. 1982;307(2):127. doi:10.1056/NEJM198207083070222
107. The World Bank. Population, total - Japan. Available from: https://data.worldbank.org/indicator/SP.POP.TOTL?locations=JP.
108. The World Bank. Population, Total - Korea, Republic. Available from: https://data.worldbank.org/indicator/SP.POP.TOTL?locations=KR.
109. Lu M, Oladapo A, Wu Y, Farahbakhshian S, Ewenstein B. Prevalence and burden of major bleeding events in patients with von Willebrand disease based on claims data from the USA. Blood. 2018;132(Suppl 1):2222.
110. Turan O. Gynaecological problem and their management in women with moderate and severe von Willebrand disease (VWD). Haemophilia. 2020;26(Suppl 4):139–140.
111. Borel-Derlon A, Goudemand J, Boyer-Neumann C, et al. Gynecological & obstetrical events from a French post-marketing survey of a von Willebrand factor concentrate with a low factor VIII content. J Thromb Haemost. 2011;9(Suppl 2):667–668.
112. Boyer-Neumann C, Borel-Derlon A, Goudemand J, et al. Management of childbirth in Von Willebrand Disease (VWD) women: results from studies with a von Willebrand factor product with a low content of Factor VIII. Hamostaseologie. 2013;33(1):A42.
113. Desprez D, Drillaud N, Flaujac C, et al. Efficacy and safety of a recombinant Von Willebrand Factor treatment in patients with inherited Von Willebrand Disease requiring surgical procedures. Haemophilia. 2021;27(2):270–276. doi:10.1111/hae.14242
114. Auerswald G, Bade A, Haubold K, Overberg D, Masurat S, Moorthi C. No inhibitor development after continuous infusion of factor concentrates in subjects with bleeding disorders undergoing surgery: a prospective study. Haemophilia. 2013;19(3):438–444. doi:10.1111/hae.12075
115. Seaman CD, Ragni MV. Periprocedural management of von Willebrand disease: an institutional experience. Haemophilia. 2019;25(3):e199–e203. doi:10.1111/hae.13718
116. O’Connell M, Singleton E, Byrne MB, Ryan K, White B, O’Donnell J. Efficacy and safety of Wilate following an en masse switch for patients with inherited von Willebrand disease. J Thromb Haemost. 2013;11(2):550.
117. Proulle V, Trossaert M, Rugeri L, et al. Efficacy and safety of hFVIII/VWF concentrate in a large cohort of patients with von Willebrand disease (VWD) requiring surgical procedures: the French experience. Res Pract Thromb Haemost. 2019;3:389–390.
 © 2023 Takeda Pharmaceutical Company Limited. This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 Takeda Pharmaceutical Company Limited. This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.