Back to Journals » Psychology Research and Behavior Management » Volume 16
Adult ADHD Positive Screening and Sibship, Birth Order and Academic Achievement: Implications for Epidemiologists and Physicians in the Kingdom of Saudi Arabia
Authors AlOmar RS ![]() , AlShamlan NA
, AlShamlan NA ![]() , Al-Johani WM
, Al-Johani WM ![]() , Almayyad AH, Alotaibi HK, Alsamin SI, Alfrayyan NY, Boubshait LA, Alghamdi LM
, Almayyad AH, Alotaibi HK, Alsamin SI, Alfrayyan NY, Boubshait LA, Alghamdi LM ![]() , Al-Shammari MA
, Al-Shammari MA ![]()
Received 21 July 2023
Accepted for publication 22 September 2023
Published 5 October 2023 Volume 2023:16 Pages 4069—4081
DOI https://doi.org/10.2147/PRBM.S426715
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Reem S AlOmar,1 Nouf A AlShamlan,1 Wejdan M Al-Johani,1 Ali H Almayyad,1 Hadeel K Alotaibi,1 Sarah I Alsamin,1 Naif Y Alfrayyan,2 Leila A Boubshait,1 Layla M Alghamdi,1 Malak A Al-Shammari1
1Department of Family and Community Medicine, College of Medicine, Imam Abdulrahman Bin Faisal University, Dammam, Kingdom of Saudi Arabia; 2Internal Medicine Department, Psychiatry Division, Security Forces Hospital, Riyadh, Kingdom of Saudi Arabia
Correspondence: Reem S AlOmar, Email [email protected]
Background: Attention deficit hyperactivity disorder (ADHD) among the youth and university students differs internationally. This study aims to assess the prevalence of ADHD positivity from a validated screening test among medical students across the Kingdom of Saudi Arabia (KSA) and its associated sociodemographic and family-related factors and the impact of ADHD on students’ academic performance. Also, to highlight the implications of the current findings on epidemiologists and family physicians in the region.
Methods: This cross-sectional study utilised the Adult ADHD Self-Report Scale (ASRS) symptom checklist along with several questions on sociodemographic, siblings and personal academic achievement. Multivariable logistic regression models were performed to obtain the Odds Ratios (ORs) of risk of ADHD screening positivity and their 95% confidence intervals (CIs) against potential predictors.
Results: The overall prevalence of positively screened medical students was 38.86%. After adjustment, a statistically significant increased risk of ADHD positivity was observed for students who had one sibling (OR = 1.70, 95% CI = 1.09– 2.64). Also, upon examination of birth order, a significant increased risk was observed for students who were firstborn (OR = 1.22, 95% CI = 1.02– 1.47). With regard to academic achievement, both before and after adjustment, students who screened positive had a 14% increased risk of obtaining an F GPA (OR = 1.14, 95% CI = 0.99– 1.30).
Conclusion: A considerable number of medical students are potentially positive for ADHD. Albeit not diagnostically confirmed – this indicates that a substantial number of people have displayed symptoms akin to ADHD, but were not clinically diagnosed. Research into ADHD in the region is still in its infancy, and epidemiologists would benefit from high-quality databases to address this condition. Also, primary care physicians should develop skills in detecting and managing ADHD in children at an earlier age to improve symptoms in adulthood.
Keywords: attention deficit hyperactivity disorder, epidemiology, family physicians, cross-sectional study, Kingdom of Saudi Arabia
Background
Attention-deficit hyperactivity disorder (ADHD) is a common heterogeneous neurodevelopmental syndrome that is characterized by the presence of persistent, developmentally excessive, and impairing levels of overactivity, inattention, and impulsivity.1 ADHD is one of the most frequent childhood psychiatric disorders, where systematic reviews have revealed that the global prevalence of ADHD among children and adolescents is around 7.2%.2 It was previously considered a childhood disorder that gradually diminishes with increasing age. However, this hypothesis was challenged by follow-up studies that noticed the persistence of ADHD into adulthood.3 Epidemiological studies have found that the estimated prevalence of adult ADHD is around 2.58% among the general population.4
ADHD in adults has a profound impact on multiple life aspects, impairing functional and psychosocial abilities, which leads to serious personal and societal costs. Its characteristic feature is attentional dysfunction, characterized by impairment in focused and sustained attention.5 In addition to symptoms of excessive talking or fidgeting, difficulty organizing tasks, inability to relax, overworking, forgetfulness, and easy distraction are also common. Furthermore, people diagnosed with ADHD are more prone to develop disrupted interpersonal relationships, academic underachievement, lower educational attainment, poor work performance, and criminality.6 Moreover, around 80% of adults with ADHD have associated psychiatric comorbidities, such as major depressive disorder, generalized anxiety disorder, alcohol or substance abuse, bipolar disorder, and various personality disorders.7,8
The aetiology of ADHD is multifactorial and influenced mainly by multiple genetic factors. Although efforts have been made to identify potential biological markers for this condition, only modest differences were observed between children affected with ADHD compared with their non-affected peers.9 Furthermore, adverse childhood experiences have been found to be implicated in ADHD increased risk, especially with inattentive presentation and vice versa.10 Also, environmental factors related to family structure, such as birth order and the number of siblings, may play a role in the aetiology of ADHD.11,12 Interestingly, several studies have examined the relationship between birth order and ADHD and found an increased risk of firstborn children for ADHD as compared to children with other birth orders.13,14
Due to the negative impact of ADHD on attention and concentration, it has been assumed that its prevalence is unremarkable in higher educational institutions. However, several studies have suggested that ADHD symptoms are relatively common among college students. The condition has been reported among students of high demanding specialties such as medicine with prevalence rates reaching 27.2% in Japan.15 In the Kingdom of Saudi Arabia (KSA), there is a paucity of studies examining ADHD in adult populations. Only two studies based on single institutions have looked at ADHD in college students in general reporting rates between 10% and 12%.16,17 The King Salman Centre for Disability Research published in its Saudi national mental health report in 2019 a prevalence of 8% among the 4004 adults aged between 15 and 65 years old.18 In the same report, the authors recommended that research specific to youth and young adults at schools and universities is needed in order to highlight the status of mental health in this vital specific age group. The objectives of this study are two-fold. We identify factors associated with an ADHD positivity screening and determine whether positive screening had a detrimental effect on academic achievement of medical students.
Materials and Methods
Study Design and Participants
This cross-sectional study included medical undergraduate students across governmental and private universities in the KSA. Students who had already been diagnosed with ADHD were excluded from the study. Ethical approval to conduct the study was obtained from Imam Abdulrahman Bin Faisal’s Institutional Review Board (IRB-2022-01-114). The study complied with the principles of the Declaration of Helsinki.
Sample Size
According to the Ministry of Health’s (MoH) statistical yearbook of 2022, the number of medical students in local universities was 23,758.19 The minimum required sample size was calculated to be 897 students using Epiinfo V.5.5.9. The 10.9% prevalence of positive ADHD medical students used to derive the sample size was from a study reported in a single institution in Riyadh.16 This prevalence, along with an alpha level of 0.05 and a precision of 2% were also parameters used in the calculation. Assuming 20% non-respondents, the minimum sample size was therefore 1077 students.
Data Collection Tool and Process
Data were collected through self-administered questionnaires. A cover letter that had described the main purpose of the study was attached along with the voluntary nature of participation and the principal author’s contact information. The cover letter further stated that the student’s participation and submission of their response was considered as consent. Participants were encouraged to contact the principal author to clarify any queries that may arise. None was received.
Data collectors who were leaders of their respective groups were approached and assigned at each university, whether private or governmental. These leaders had access to their colleagues’ phone numbers and thus were sent the link to the questionnaire for distribution among their peers. The QuestionPro online software was used for the design and distribution of the questionnaire.20
The questionnaire was made up of five main sections. The first section measured the main sociodemographic characteristics which included questions on age (numerical), sex (male, female), marital status (single, married, divorced, widowed). The second section was on family and birth order and included questions on the number of siblings (single child, one sibling, two or more siblings) and birth order of children (single child, firstborn, middle born, youngest born). The third section included health-related questions such as height and weight to form a body mass index (BMI) variable using the kg/m2 formula (underweight, normal weight, overweight, obese), any personal history of mood disorders, anxiety disorder (yes/no), and a family history of ADHD, mood disorders and anxiety disorders (yes/no). The fourth question looked at the academic characteristics of the students and included questions on the last known grade point average (GPA) (A, B, C, D, F) and whether the student had previously failed (yes/no). The last section was taken from the Adult ADHD Self-Report Scale v1.1 symptom checklist (ASRS-v1.1).21 This is a checklist which originally consists of 18 questions derived from the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-TR) criteria for ADHD and is made up of two parts, part A and part B. Part A consists of six questions, most commonly known as the ASRS screener and once scored, are the most indicative of the presence of ADHD. The response to these questions varies between never to very often. These questions are scored by checking whether four or more marks appear in the dark shaded boxes, if so then that participant has symptoms that are highly indicative of ADHD (Figure 1). For the purposes of this research, only part A was used.
 |
Figure 1 Part A of the Adult ADHD Self-Report Scale (ASRS-v1.1) symptom checklist by Kesslar et al, 2005. Note: A participant who scores four or more of the dark shaded boxes is considered to have symptoms indicative of ADHD. Reproduced from Kessler RC, Adler L, Ames M, et al. The World Health Organization adult ADHD self-report scale (ASRS). Psychological Medicine. 2005;35(2):245-256.21 |
To avoid duplicate responses, the URL did not accept more than one response from the same student. Only complete responses were analysed. A pilot study was made on 50 students prior to the final distribution to assess the clarity and estimate the average time it took to fill out the questionnaire. No modifications were made, and the average time in minutes was 4.
Statistical Analysis
This study had two main outcomes. The first was whether medical students screened positive for ADHD symptoms according to the Adult ASRS (yes/no). The second was the academic achievement of students with vs without ADHD positive screening (GPA). Descriptive analyses were measured through counts and percentages for categorical variables and means ± standard deviations for continuous ones. Bivariate associations were assessed through T-tests, ANOVA and Chi-squared tests where appropriate. For the first outcome, a series of unadjusted and adjusted binary logistic regression models were used, whereas for the second outcome, the unadjusted and adjusted ordinal logistic regression models were used after verification that the proportional odds assumptions were held. Choice of variables for inclusion into the models was based on Directed Acyclic Graphs and was not solely based on significance in bivariate analyses. Models with the best fit were chosen. The level of significance was set to 0.05 throughout. All analyses were performed in Stata statistical software version 15.0.22
Results
A total of 3219 students (13.55% of the target population) participated in this study, of which 1251 (38.86%) were found to screen positive for ADHD.
Sociodemographic, Family, Health, and Academic Characteristics of Students
The overall mean age of students was 22.18 ± 1.84 years. The sample consisted of 42.22% males compared to 57.78% females. The majority of students were single. Regarding the number of siblings, 15 students (0.47%) had no siblings, whereas 96.92% had two or more siblings. Also, 25.07% of the total sample was firstborn, followed by 31.90% who were middle born and 42.56% who were the youngest in their families. Over 15% had a history of mood disorders, and a similar percentage is seen for a previous diagnosis of anxiety disorders. A positive family history for ADHD was reported in 6.77% of the sample, and 9.72% reported a family history of mood disorders. Most students reported a high GPA grade of A, and 16.93% reported to have previously been failed (Table 1).
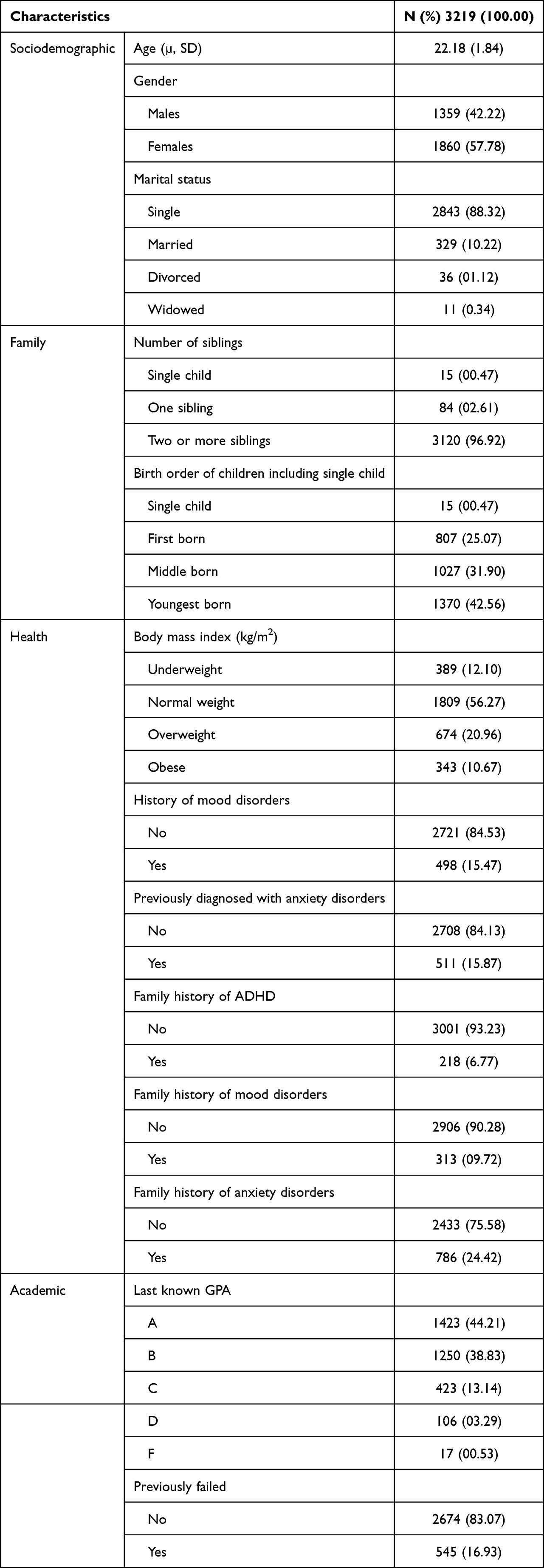 |
Table 1 Sociodemographic, Family, Health and Academic Characteristics of Study Participants |
Predictors for ADHD in Unadjusted and Adjusted Models
Table 2 presents unadjusted Odds Ratios (ORs) of risk of a positive ADHD screening and their 95% confidence intervals (CIs). The results show that there is an inverse association with age (OR = 0.93, 95% CI = 0.90–0.97). Both having a personal history of mood disorders and anxiety disorders were associated with an increase in risk of ADHD positivity. Also, a family history of mood disorders was associated with a 34% increase in risk (95% CI = 1.14–1.58) and a family history of anxiety disorders was associated with a 60% increase in risk (95% CI = 1.33–1.93). A family history of ADHD was not a significant predictor in this sample.
 |
Table 2 Univariable Binary Logistic Regression Analyses for the Relevant Control Variables Predicting ADHD |
Table 3 presents the results of the different models for risk of ADHD positive screening while accounting for all confounders from Table 3. Model 1 examines the number of siblings as the main predictor. The results show that being a single child is associated with a non-significant decreased risk of ADHD positive screening, whereas having one sibling was statistically significantly associated with a 70% increase in risk when compared to students who had two or more siblings (95% CI = 1.09–2.64). Model 2 examines the model with the main predictor being students who have no students compared to students who have one or more siblings. Similar to model 1, students who have no siblings are less likely to have ADHD positive screening tests, albeit non-significant. Model 3 looks at birth order as the main predictor. The results show that students who were the oldest among their siblings were more likely to have an ADHD positive screening (OR = 1.22, 95% CI = 1.02–1.44). Model 4 also examines birth order but without including students who have no siblings, and the association remains the same for firstborn students.
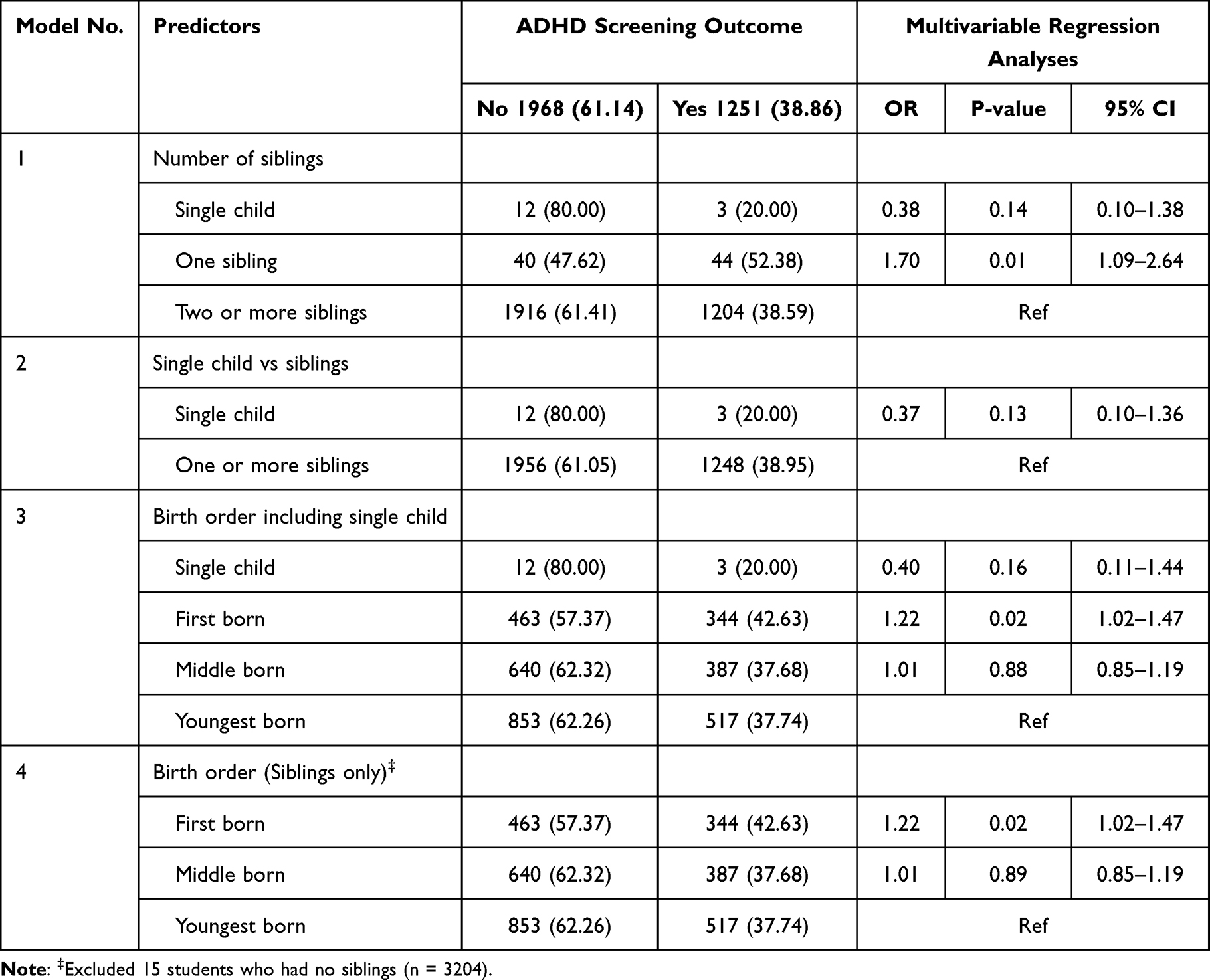 |
Table 3 Multivariable Binary Logistic Regression Analyses for Number of Siblings and Birth Order Predicting ADHD, Controlled for Age, Sex, Personal and Family History of Mood Disorders and Anxiety Disorders |
ADHD and Academic Achievement
Bivariate associations between the different sociodemographic, family and health-related variables and students’ GPA are shown in Table 4. Both age and sex were significantly associated with GPA. Students who had a personal history of mood disorders and anxiety disorders were also more likely to have lower GPAs such as C, D and F (P < 0.001). More importantly, a significant association can be seen between ADHD screening and GPA, where students who screened positive reported lower GPA more than those who screened negative (P = 0.04).
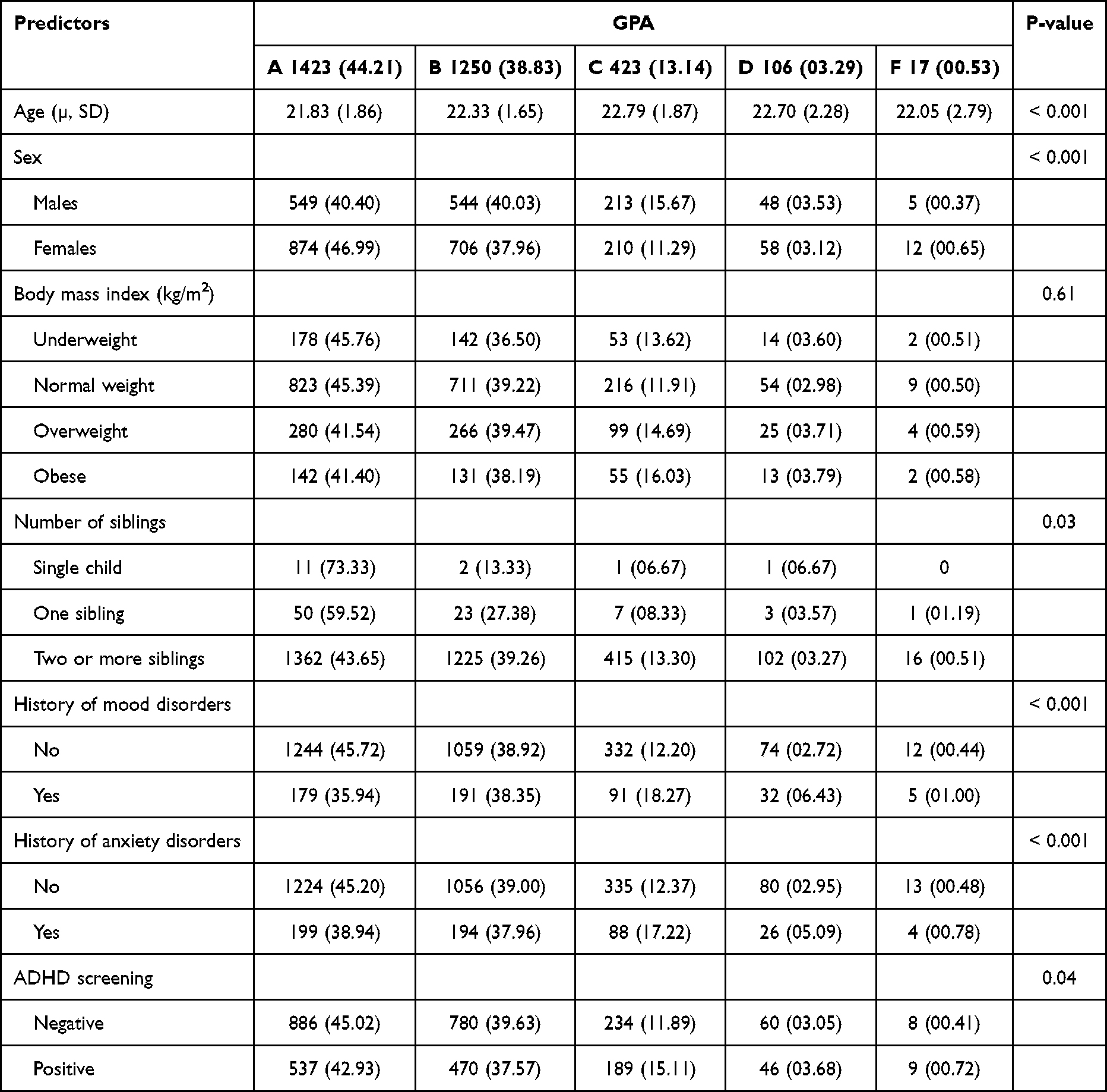 |
Table 4 Bivariate Associations of Sociodemographic, Family, Health and Academic Characteristics and GPA of Study Participants |
Further multivariable analyses have shown that both in the unadjusted and adjusted ordinal logistic regression models, students screening positive had a higher risk of a lower GPA (Unadjusted OR = 1.15, 95% CI = 1.01–1.31 and adjusted OR = 1.14, 95% CI = 0.99–1.30) holding all other variables constant (Table 5).
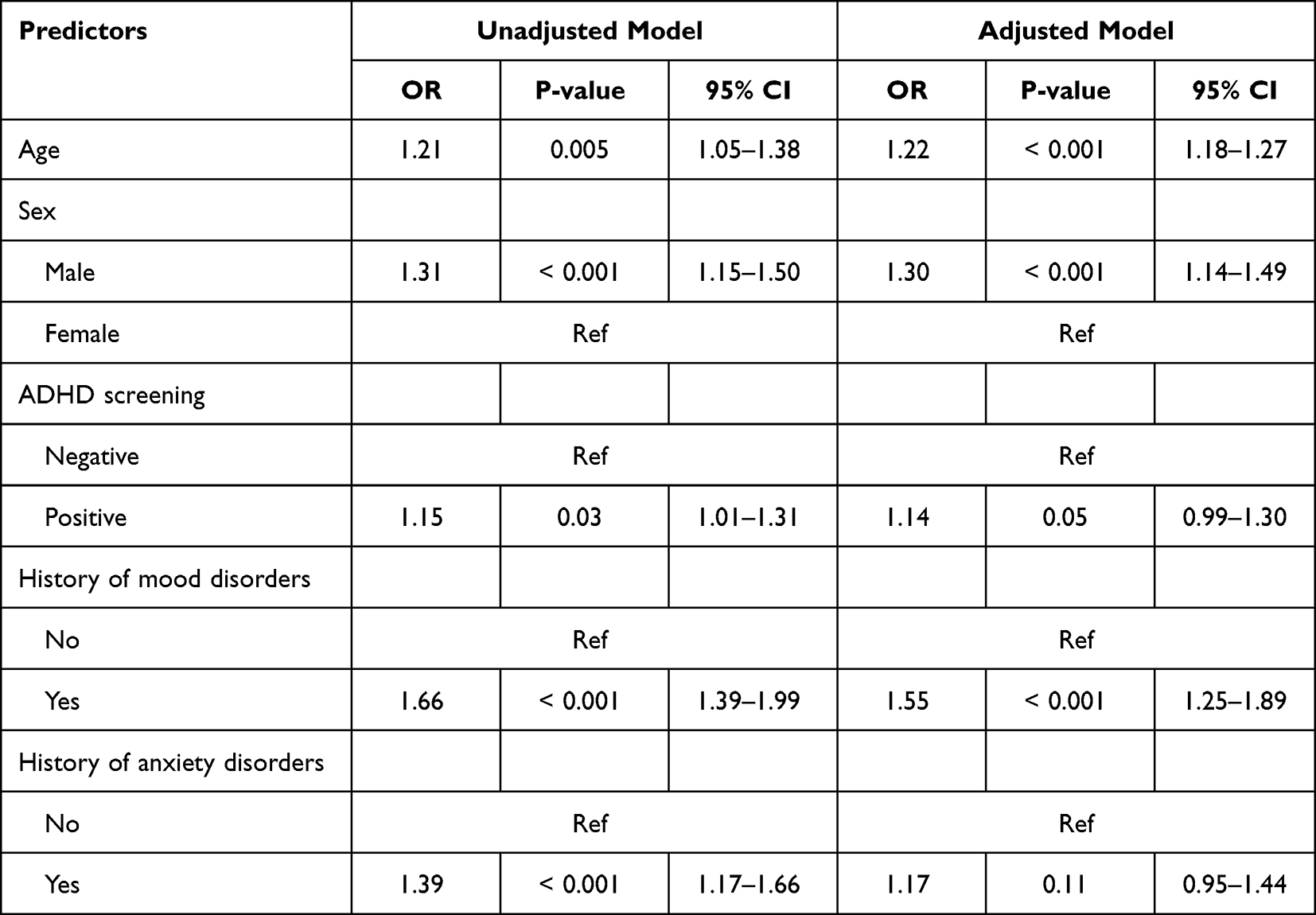 |
Table 5 Univariable and Multivariable Ordinal Logistic Regression Analysis for Positive ADHD Screening Predicting Academic Achievement in Medical Students |
Discussion
This study aimed at estimating the prevalence of positive screening for ADHD in a large sample of students, as well as to examine whether birth order and having siblings were predictors of ADHD and finally to study the effect that ADHD – albeit not diagnostically confirmed – has on students’ academic achievement. We found that among the 3219 students who have participated, 38.86% screened positive for ADHD through the use of the ASRS-v1.1 symptom checklist. We also found that having one sibling was a significant predictor for ADHD positivity. Additionally, our results show that students who screened positive had a higher risk of having lower GPAs.
In terms of the high prevalence, our findings are in line with other studies. For example, a Kenyan study found that 23.7% of medical students had screened positive for ADHD.23 In Japan, a prevalence of 27.2% of college students was reported.15 Both studies utilised the same ASRS v.1. symptom checklist. Nonetheless, others have reported lower rates, for example locally in the KSA, and a prevalence of 10.9% and 11.9% was both reported in Riyadh and Jeddah, respectively.16,17
According to a systematic review and a meta regression analysis of worldwide data, the pooled prevalence of ADHD was 5.29%.24 This same study reported that the meta regression had statistically significant variability of these rates that was due to diagnostic criteria, source of information, and geographic region. It may also be that different methodologies inherent between studies, especially in the choice of the population, have played a role in that variability. Both local studies in Riyadh and Jeddah were restricted to a single university within those cities, whilst this study was based on data from all regions of the country.
Predictors of ADHD
Males were more likely to screen positive for ADHD than females in our sample, and this was found to be consistent with the current literature. In a large systematic review that aimed to primarily examine gender differences in ADHD, studies that have utilised the symptom checklist reported an overall 2.2:1 ratio of male to female prevalence.25 It may be that females are undetected or underdiagnosed, or that the condition is expressed differently between the two genders. Indeed, studies that have looked further into the subscales of ADHD have found that males tended to express hyperactivity and impulsivity whilst females were more likely to be inattentive. Impulsiveness and hyperactivity – unlike inattentiveness – tend to diminish over time which may further contribute to adult ADHD differences between the two sexes.26
The notion that an association between ADHD and mental disorders exists has been extensively examined using population-based data internationally.27,28 Research has suggested that due to the fact that in children, a diagnosis of an ADHD may be missed unless symptoms start to show prior to the age of 7 years would naturally mean that some mental disorders are temporally secondary to adult ADHD. Additionally, evidence has shown that early detection and management of ADHD in children would subsequently reduce mental disorders. The literature also suggests that mental disorders are associated with specific subtypes of ADHD. For example, in a study of 100 adults with ADHD in Oman, it was found that certain mental conditions such as personality disorders and major depressive disorders were very highly associated with an increased risk of the inattentive subtype of ADHD.29 Our results are indicative of this association and are similar to previous studies where students who had a previous diagnosis of mood disorders and anxiety disorders were more likely to screen positive for ADHD.
This study also closely examined the association between the number of siblings, birth order and adult ADHD screening. With regard to the number of siblings, the literature varies in its findings. In the UK, in a study that utilised a dataset of over 2 million people registered with a general practitioner, they found that for every unit increase in the number of children in the household, a 27.6% increased risk of a later diagnosis of ADHD would be made.30 The authors have suggested that a large number of children in the household may hinder parental recognition of symptoms. This may have been the case in our sample, where a possibility of a missed diagnosis in childhood may have contributed to a high prevalence in adulthood. Furthermore, in Germany, and similar to our findings, firstborn children were found to be at a greater risk for ADHD positivity compared to those who had no siblings.14 This suggests that the number of children in the family may moderate the effects of birth order, as is the case in some disorders such as asthma and allergies.31 However, in the same German study, no significant association was found when comparing those with vs those without siblings.
Similar to our results, firstborn children were found to be at a higher risk for ADHD in Germany, Spain, and Taiwan.13,14,32 Firstborns tend to shoulder more responsibility in many aspects including responsibility for their younger siblings, especially in a country like the KSA where males are entrusted with a higher degree of responsibility within the family. Hence, it may be safe to assume that the birth of a younger sibling may require more emotional adjustment and competition for parental care. Furthermore, parenting skills are refined with the birth of each additional child, so it may be that the younger siblings benefit from a better parenting style. These factors may have been a deterrent to a child’s personality development.
ADHD and Academic Achievement
We found that students who screened positive for ADHD had a higher odds of acquiring a lower GPA. In a very recent study published in 2022 which primarily focused on self-reporting of ADHD using Conner’s Adult ADHD Rating Scale (CAAR), the authors found that having inattention symptoms was a significant predictor of a lower final GPA. The article also found that men had higher odds of having inattention symptoms, both of which are statistically significant as is the case here.33 Some studies on high schoolers suggested students with ADHD had a higher drop rate and were more at risk of being years behind their peers in subjects like maths and languages.34,35 Findings across the literature have not been consistent. For example, Gray et al did not associate students’ academic performance with ADHD. Also, Lewandowski et al reported that academic success was not correlated with an ADHD diagnosis in post-secondary education.36,37 It should be noted, however, that those two studies used an actual diagnosis of ADHD rather than screening.
This study was the first to assess family-related characteristics and its associations with ADHD of a large adult population in the KSA. However, we must acknowledge that the ASRS symptoms checklist is merely a screening tool where those who have screened positive should require further investigations. Also, the cross-sectional design and the method of sampling have probably impacted the generalisability and causality of our findings.
Implications for Epidemiologists and Family Physicians
Research on ADHD has gained much attention, especially since it is often missed during childhood and persists into adulthood.38 Epidemiologists and healthcare professionals continue to face challenges when attempting to study ADHD and other psychiatric illnesses in the KSA. One very clear challenge is the absence of population-based data that would take into account health-related variables. One very good opportunity for improvement is the Saudi census data. The most recent census in 2022 has included more questions on health, focusing on chronic illnesses such as diabetes, cancer, and heart disease. The census also asks about the presence of “mental disorders” in general without a requirement of stating the type of mental disorder and also asks about autism.39 It may be prudent to examine more closely specific disorders such as ADHD to be able to estimate its prevalence and study its correlates on a national level. The Saudi national health survey initiative is an initial step towards achieving this goal, however incorporating the methods of the survey into the census data would be an incredible opportunity for epidemiologists and healthcare researchers in the KSA to examine risk factors and correlates of such mental illnesses.
Without doubt, the burden falls primarily upon primary care and family physicians for the detection and treatment of ADHD. It has been previously reported that ADHD is very common among children reaching a prevalence of 12% in some populations and that it was one of the three most common chronic conditions seen in primary care, where the other two were otitis media and asthma.40 Primary care physicians should improve competency in the diagnosis, treatment, and proper follow-up of ADHD in children at an earlier age. It is often that parents may face stigma within the community regarding ADHD, but physicians must present parents with up-to-date evidence-based information to develop a long-term plan for the management of this disorder, since evidence shows that psychotropic and psychostimulant medications and behavioural modification therapy can positively affect the developmental trajectory of most children and lead to better outcomes.40,41
Conclusion
This study aimed to estimate the prevalence of a positive screening for ADHD using a validated screening tool, as well as identifying potential correlates and assess whether a positive screening of ADHD had impacted the academic achievement of the sampled medical students. ADHD was potentially found in 38.86% of our students. Predictors in this sample were age, being male, presence of a personal history of mood and anxiety disorders, as well as a family history of mood and anxiety disorders. We also found that poor academic achievement was highly associated with ADHD. Earlier detection and treatment of ADHD is crucial to control for and positively redirect developmental trajectory of individuals at an earlier age.
Abbreviations
ADHD, Attention deficit hyperactivity disorder; KSA, Kingdom of Saudi Arabia; MoH, Ministry of Health; BMI, Body mass index; GPA, Grade point average; ASRS-v1.1, Adult ADHD Self-Report Scale v1.1 symptom checklist.
Data Sharing Statement
The dataset used during the current study is available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
Approval was obtained from Imam Abdulrahman Bin Faisal’s Institutional Review Board prior to the implementation of this study (IRB-2022-01-114). A cover letter with an informed consent of participation was given prior to answering the questionnaire.
Acknowledgments
The authors would like to thank all medical students who have kindly agreed to participate in this study.
Author Contributions
All authors have made a significant contribution to the work reported here, whether it be in the conceptualisation, design of the study, acquisition of the data, analyses and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was not funded.
Disclosure
The authors have no relevant financial or non-financial interests to disclose.
References
1. Sayal K, Prasad V, Daley D, Ford T, Coghill D. ADHD in children and young people: prevalence, care pathways, and service provision. Lancet Psychiatry. 2018;5(2):175–186. doi:10.1016/S2215-0366(17)30167-0
2. Thomas R, Sanders S, Doust J, Beller E, Glasziou P. Prevalence of attention-deficit/hyperactivity disorder: a systematic review and meta-analysis. Pediatrics. 2015;135(4):e994–1001. PMID: 25733754. doi:10.1542/peds.2014-3482
3. Sibley MH, Mitchell JT, Becker SP. Method of adult diagnosis influences estimated persistence of childhood ADHD: a systematic review of longitudinal studies. Lancet Psychiatry. 2016;3(12):1157–1165. PMID: 27745869. doi:10.1016/s2215-0366(16)30190-0
4. Song P, Zha M, Yang Q, Zhang Y, Li X, Rudan I. The prevalence of adult attention-deficit hyperactivity disorder: a global systematic review and meta-analysis. J Glob Health. 2021;11:04009. PMID: 33692893; PMCID: PMCPMC7916320. doi:10.7189/jogh.11.04009
5. Bálint S, Czobor P, Komlósi S, Mészáros A, Simon V, Bitter I. Attention deficit hyperactivity disorder (ADHD): gender- and age-related differences in neurocognition. Psychol Med. 2009;39(8):1337–1345. PMID: 18713489. doi:10.1017/s0033291708004236
6. Willoughby MT. Developmental course of ADHD symptomatology during the transition from childhood to adolescence: a review with recommendations. J Child Psychol Psychiatry. 2003;44(1):88–106. PMID: 12553414. doi:10.1111/1469-7610.t01-1-00104
7. Sobanski E, Brüggemann D, Alm B, et al. Psychiatric comorbidity and functional impairment in a clinically referred sample of adults with attention-deficit/hyperactivity disorder (ADHD). Eur Arch Psychiatry Clin Neurosci. 2007;257(7):371–377. PMID: 17902010. doi:10.1007/s00406-007-0712-8
8. Klassen LJ, Katzman MA, Chokka P. Adult ADHD and its comorbidities, with a focus on bipolar disorder. J Affect Disord. 2010;124(1–2):1–8. PMID: 19683348. doi:10.1016/j.jad.2009.06.036
9. Bernanke J, Luna A, Chang L, Bruno E, Dworkin J, Posner J. Structural brain measures among children with and without ADHD in the adolescent brain and cognitive development study cohort: a cross-sectional US population-based study. Lancet Psychiatry. 2022;9(3):222–231. doi:10.1016/S2215-0366(21)00505-8
10. Lugo-Candelas C, Corbeil T, Wall M, et al. ADHD and risk for subsequent adverse childhood experiences: understanding the cycle of adversity. J Child Psychol Psychiatry. 2021;62(8):971–978. doi:10.1111/jcpp.13352
11. Faraone SV, Perlis RH, Doyle AE, et al. Molecular genetics of attention-deficit/hyperactivity disorder. Biol Psychiatry. 2005;57(11):1313–1323. PMID: 15950004. doi:10.1016/j.biopsych.2004.11.024
12. Banerjee TD, Middleton F, Faraone SV. Environmental risk factors for attention-deficit hyperactivity disorder. Acta Paediatr. 2007;96(9):1269–1274. PMID: 17718779. doi:10.1111/j.1651-2227.2007.00430.x
13. Marín AM, Seco FL, Serrano SM, García SA, Gaviria Gómez AM, Ney I. Do firstborn children have an increased risk of ADHD? J Atten Disord. 2012;18(7):594–597. doi:10.1177/1087054712445066
14. Reimelt C, Wolff N, Hölling H, et al. Siblings and birth order—are they important for the occurrence of ADHD? J Atten Disord. 2018;25(1):81–90. doi:10.1177/1087054718770020
15. Takahashi K, Miyatake N, Kurato R, Takahashi N. Prevalence of attention deficit hyperactivity disorder and/or autism spectrum disorder and its relation to lifestyle in female college students. Environ Health Prev Med. 2016;21(6):455–459. PMID: 27350055; PMCID: PMCPMC5112192. doi:10.1007/s12199-016-0548-9
16. Alrahili N, Aldakheel A, Alubied A, et al. Prevalence of adult attention deficit hyperactivity disorder among medical students in Riyadh City. Int J Med Dev Ctries. 2019:1. doi:10.24911/IJMDC.51-1543855405
17. Alghamdi WA, Alzaben FN, Alhashemi HH, et al. Prevalence and correlates of attention deficit hyperactivity disorder among college students in Jeddah, Saudi Arabia. Saudi J Med Med Sci. 2022;10(2):131–138. PMID: 35602395; PMCID: PMCPMC9121697. doi:10.4103/sjmms.sjmms_654_21
18. AlTwaijri Y, Al-Subaie A, Al-Habeeb A. Saudi national mental health survey technical report. King Salman Centre for Disability Research; 2019.
19. MoH. Statistical yearbook; 2022.
20. QuestionPro. QuestionPro 2022; 2022. Available from: https://www.questionpro.com/.
21. Kessler RC, Adler L, Ames M et al. Psychological Medicine . The World Health Organisation Adult ADHD self-report scale (ASRS). 2005; 35(2):245-256
22. StataCorp. Stata Statistical Software: Release 15. College Station, TX: StataCorp LLC; 2017.
23. Atwoli L, Owiti P, Manguro G, Ndambuki D. Attention deficit hyperactivity disorder symptom self-report among medical students in Eldoret, Kenya. Afr J Psychiatry. 2011;14(4):286–289. PMID: 22038426. doi:10.4314/ajpsy.v14i4.5
24. Polanczyk G, De lima MS, Horta BL, Biederman J, Rohde LA. The worldwide prevalence of ADHD: a systematic review and metaregression analysis. Am J Psychiatry. 2007;164(6):942–948. PMID: 17541055. doi:10.1176/ajp.2007.164.6.942
25. Willcutt EG. The prevalence of DSM-IV attention-deficit/hyperactivity disorder: a meta-analytic review. Neurotherapeutics. 2012;9(3):490–499. PMID: 22976615; PMCID: PMCPMC3441936. doi:10.1007/s13311-012-0135-8
26. Stibbe T, Huang J, Paucke M, Ulke C, Strauss M. Gender differences in adult ADHD: cognitive function assessed by the test of attentional performance. PLoS One. 2020;15(10):e0240810. PMID: 33057383; PMCID: PMCPMC7561166. doi:10.1371/journal.pone.0240810
27. Kessler RC, Adler L, Barkley R, et al. The prevalence and correlates of adult ADHD in the United States: results from the national comorbidity survey replication. Am J Psychiatry. 2006;163(4):716–723. PMID: 16585449; PMCID: PMCPMC2859678. doi:10.1176/ajp.2006.163.4.716
28. Jensen PS, Hinshaw SP, Swanson JM, et al. Findings from the NIMH multimodal treatment study of ADHD (MTA): implications and applications for primary care providers. J Dev Behav Pediatr. 2001;22(1):60–73. PMID: 11265923. doi:10.1097/00004703-200102000-00008
29. Mirza H, Al-Huseini S, Al-Jamoodi S, et al. Socio-demographic and clinical profiles of adult attention deficit hyperactivity disorder patients in a university hospital in Oman. Sultan Qaboos Univ Med J. 2022;22(2):206–211. doi:10.18295/squmj.5.2021.104
30. Hoang U, James AC, Liyanage H, et al. Determinants of inter-practice variation in ADHD diagnosis and stimulant prescribing: cross-sectional database study of a national surveillance network. BMJ Evid Based Med. 2019;24(4):155–161. PMID: 30765384; PMCID: PMCPMC6678046. doi:10.1136/bmjebm-2018-111133
31. Bernsen RM, de Jongste JC, van der Wouden JC. Birth order and sibship size as independent risk factors for asthma, allergy, and eczema. Pediatr Allergy Immunol. 2003;14(6):464–469. PMID: 14675474. doi:10.1046/j.0905-6157.2003.00108.x
32. Hsu YC, Chen CT, Yang HJ, Chou P. Family structure, birth order, and aggressive behaviors among school-aged boys with attention deficit hyperactivity disorder (ADHD). Soc Psychiatry Psychiatr Epidemiol. 2019;54(6):661–670. PMID: 30535676. doi:10.1007/s00127-018-1624-9
33. Henning C, Summerfeldt LJ, Parker JDA. ADHD and academic success in university students: the important role of impaired attention. J Atten Disord. 2021;26(6):893–901. doi:10.1177/10870547211036758
34. Kent KM, Pelham WE, Molina BSG, et al. The academic experience of male high school students with ADHD. J Abnorm Child Psychol. 2011;39(3):451–462. doi:10.1007/s10802-010-9472-4
35. Lawrence D, Houghton S, Dawson V, Sawyer M, Carroll A. Trajectories of academic achievement for students with attention-deficit/hyperactivity disorder. Br J Educ Psychol. 2021;91(2):e12392. doi:10.1111/bjep.12392
36. Gray SA, Fettes P, Woltering S, Mawjee K, Tannock R. Symptom manifestation and impairments in college students with ADHD. J Learn Disabil. 2015;49(6):616–630. doi:10.1177/0022219415576523
37. Lewandowski LJ, Lovett BJ, Codding RS, Gordon M. Symptoms of ADHD and academic concerns in college students with and without ADHD diagnoses. J Atten Disord. 2008;12(2):156–161. doi:10.1177/1087054707310882
38. Ginsberg Y, Quintero J, Anand E, Casillas M, Upadhyaya HP. Underdiagnosis of attention-deficit/hyperactivity disorder in adult patients: a review of the literature. Prim Care Companion CNS Disord. 2014;16(3). PMID: 25317367; PMCID: PMCPMC4195639. doi:10.4088/PCC.13r01600
39. GAS. Census questionnaire - 2022. General Authority for Statistics; 2022.
40. Leslie LK. The role of primary care physicians in attention-deficit/hyperactivity disorder. Pediatr Ann. 2002;31(8):475–484. PMID: 12174762; PMCID: PMCPMC1647398. doi:10.3928/0090-4481-20020801-07
41. Wang Y, Kessel E, Lee S, et al. Causal effects of psychostimulants on neural connectivity: a mechanistic, randomized clinical trial. J Child Psychol Psychiatry. 2022;63(11):1381–1391. doi:10.1111/jcpp.13585
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Burden of Metabolic Syndrome Among a Low-Income Population in China: A Population-Based Cross-Sectional Study
Bao J, Wang L, Hu P, Liu J, Tu J, Wang J, Li J, Ning X
Diabetes, Metabolic Syndrome and Obesity 2022, 15:2713-2723
Published Date: 3 September 2022
Association Between Carbapenem-Resistant Enterobacterales (CRE) Colonization Status at Time of Hospital Admission and the Subsequent Development of CRE Infection and Mortality in High-Risk Patients
Alraddadi BM, Heaphy ELG, Alzahrani MS, Alqadi M, Qashqari MS, Alhuthali MS, Al Hroub MK, Hefni L, Alshukairi AN, Aldabbagh Y, Qutub M
Infection and Drug Resistance 2024, 17:4655-4664
Published Date: 25 October 2024
The Possible Association of Burnout and Neuropathic Low Back Pain Among Hungarian Postal Workers: A Cross-Sectional Study
Balajti L, Horvath L, Fejes E, Tibold A, Kobolka I, Zadori I, Berke G, Banko Z, Springó Z, Feher G
Journal of Multidisciplinary Healthcare 2024, 17:5237-5250
Published Date: 15 November 2024
Family Physicians’ Knowledge and Perceived Confidence with Clinical Ophthalmology
Othman S, Alasmari A, Showail M
Advances in Medical Education and Practice 2024, 15:1175-1183
Published Date: 28 November 2024
Epidemiology and Antifungal Susceptibility Trends of Candidemia: A 5-Year Retrospective Study at King Abdulaziz University Hospital
Abdalal SA, Attallah DM, Mokhtar JA, Kaki RM, Niyazi HA, Niyazi HA, Aldarmasi MA
Infection and Drug Resistance 2025, 18:5905-5915
Published Date: 11 November 2025