Back to Journals » Cancer Management and Research » Volume 18

A Failure Pattern Analyses in NSCLC Patients Received Immuno-Radiotherapy and a Dosimetric Feasibility Study of a Three-Ladder Radiotherapy Strategy
Authors Li Y, Ma Y, Song Z, Su J, Peng H
Received 17 November 2025
Accepted for publication 23 February 2026
Published 10 March 2026 Volume 2026:18 582081
DOI https://doi.org/10.2147/CMAR.S582081
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Bilikere Dwarakanath
Yuyi Li,1– 3 Yechen Ma,1 Zewen Song,1,4 Ju Su,1,4 Honghua Peng1,4
1Department of Oncology, the Third Xiangya Hospital of Central South University, Central South University, Changsha, People’s Republic of China; 2Graduate Collaborative Training Base of Hunan Cancer Hospital, Hengyang Medical School, University of South China, Hengyang, Hunan, People’s Republic of China; 3Department of Radiation Oncology, Hunan Cancer Hospital, the Affiliated Cancer Hospital of Xiangya School of Medicine, Central South University, Changsha, Hunan, People’s Republic of China; 4Department of Oncology, Xiangxi Autonomous Prefecture People’s Hospital, Ji Shou University, Jishou, People’s Republic of China
Correspondence: Ju Su, Email [email protected] Honghua Peng, Email [email protected]
Background: This study aimed to analyze failure patterns in stage III non-small cell lung cancer (NSCLC) patients treated with immuno-radiotherapy and to dosimetrically evaluate a novel three-ladder radiotherapy (3L-RT) strategy designed to address the observed local control deficit.
Methods: Clinical outcomes and failure patterns were retrospectively analyzed in 89 consecutive stage III NSCLC patients (2020– 2023) treated with simultaneous integrated boost intensity modulated radiotherapy (SIB-IMRT) combined with immunotherapy. Separately, a dosimetric planning study was conducted to compare the feasibility of the proposed 3L-RT strategy (prescribing 74 Gy to GTV, 60 Gy to PTV-g, and 54 Gy to PTV-c) against conventional radiotherapy (PTV-c 60 Gy) on a distinct patient cohort, with and without 4D-CT simulation.
Results: Median follow-up was 23.2 months. Median progression-free survival (PFS) and overall survival (OS) were 19.4 and 41.1 months, respectively. Immuno-neoadj independently predicted superior PFS (HR: 0.32, p < 0.001) and OS (HR: 0.25, p = 0.013). Among 43 progression events (48.3%), local failure (53.5%) predominated, driven by primary tumor progression. Distant metastases occurred in 51.2% (pulmonary, osseous, and intracranial sites most frequent). In the dosimetric comparison, the 3L-RT strategy reduced cardiopulmonary exposure versus conventional plans: lung V20 decreased from 20.2% to 19.6%, cardiac V30 from 9.55% to 8.7%, and effective dose to immune cells (EDIC) from 3.9 Gy to 3.7 Gy (p < 0.001). Dose reductions persisted with 4D-CT integration.
Conclusion: Within the studied clinical cohort, immunotherapy combined with SIB-IMRT correlates with favorable survival, yet local failure remains a predominant challenge. The proposed 3L-RT strategy is dosimetrically feasible, enabling targeted GTV dose escalation while sparing critical organs. These dosimetric findings support the rationale for future prospective clinical trials to evaluate whether this strategy can improve local control and survival outcomes.
Keywords: NSCLC, immunotherapy, failure pattern, three-ladder radiotherapy, dose escalation
Introduction
Stage III non-small cell lung cancer (NSCLC) represents a heterogeneous disease with historically poor outcomes, necessitating multimodal therapeutic approaches. The current standard of care—concurrent chemoradiotherapy (CCRT) followed by durvalumab consolidation immunotherapy—has significantly improved progression-free survival and overall survival compared to CCRT alone.1,2 However, disease progression remains a critical challenge. Noriko Kishi et al reported that after a median follow-up of 25.4 months, locoregional recurrence (LR), and LR plus distant metastases (DM) occurred in 20.6% and 8.8% of patients, respectively, following CCRT and durvalumab consolidation.3 Similarly, Michael Offin et al observed a cumulative 12-month incidence of local-regional failure in 18% (95% CI: 5.9–30%) among 62 patients (median follow-up 12 months).4 These findings underscore that suboptimal local control persists even with modern protocols. This persistent local failure may undermine the potential benefits of immunotherapy by triggering systemic immunosuppression or accelerating distant metastasis.
The persistence of local failure, particularly in bulky primary tumors, can be attributed to several biological and physical factors. Bulky tumors often harbor hypoxic regions that are radioresistant and foster an immunosuppressive microenvironment, potentially blunting the efficacy of immunotherapy.5 Furthermore, conventional radiotherapy doses may be insufficient to eradicate all clonogenic cells within large tumor volumes, especially those with intrinsic radioresistance or stem-like properties. While immunotherapy can induce systemic anti-tumor responses, its efficacy may be limited against high-burden, poorly perfused primary sites where effector T-cell infiltration is suboptimal.
A critical barrier to improving outcomes lies in the limitations of conventional radiotherapy dose escalation. While increasing radiation doses to gross tumor volume (GTV) could theoretically enhance local control, historical trials such as RTOG 0617 demonstrated unacceptable toxicity with 74 Gy compared to 60 Gy, primarily due to increased cardiopulmonary exposure.6,7 Furthermore, the advent of immunotherapy introduces new considerations: radiation-induced lymphopenia, modulated by lung and heart dose-volume parameters, has been linked to impaired immune function and worse survival.8,9 Thus, optimizing radiation strategies must balance tumor control, organ-at-risk (OAR) sparing, and preservation of systemic immunity—a tripartite challenge in the immunotherapy era.
Our previous study demonstrated that combining simultaneous integrated boost intensity modulated radiotherapy (SIB-IMRT) and/or neoadjuvant immunochemotherapy effectively reduces GTV while achieving stringent control of bilateral lung V20 parameters. This approach significantly improves survival outcomes in stage III NSCLC patients, concurrently reducing the incidence of grade ≥2 radiation pneumonitis (RP).10 Building on these findings, this study aims to analyze prognostic outcomes and failure patterns in a two-center cohort of stage III NSCLC patients treated with SIB-IMRT combined with immunotherapy, with a focus on the persistent challenge of local disease control. Further, we propose a novel three-ladder radiotherapy (3L-RT) strategy that selectively escalates radiation doses to high-risk subvolumes while adhering to organ-at-risk (OAR) constraints. The protocol prescribes 74 Gy to GTV (primary tumor), 60 Gy to the prophylactic nodal volume (PTV-g), and 54 Gy to elective nodal regions (PTV-c). This approach hypothesizes that spatially focused dose intensification might reduce primary tumor recurrence without amplifying cardiopulmonary toxicity or lymphocyte depletion.
To validate this hypothesis, we conducted a comprehensive dosimetric analysis comparing the 3L-RT strategy to conventional radiotherapy plans. Key endpoints included target coverage, dose homogeneity, and OAR parameters (eg., mean lung dose, V20 for lungs, heart V30). The present work seeks to demonstrate the dosimetric feasibility of achieving GTV dose escalation to 74 Gy while maintaining cardiopulmonary doses within established safety thresholds, thereby providing a rationale for future prospective trials evaluating the clinical efficacy of this strategy in improving locoregional control and survival outcomes for Stage III NSCLC patients.
Method
Ethics Approval and Consent to Participate
This retrospective study was conducted at two institutions, the Third Xiangya Hospital of Central South University and the Xiangxi Autonomous Prefecture People’s Hospital. The study protocol was reviewed and approved by the Ethics Committee of the Third Xiangya Hospital, Central South University (Approval No. E24412) and the Medical Ethics Committee of the Xiangxi Autonomous Prefecture People’s Hospital (Approval No. EC-LCKY2024037). The need for informed consent was waived by the ethics committees due to the retrospective nature of the study. All patient data were rigorously de-identified and anonymized prior to analysis. Confidentiality was maintained in accordance with the principles of the Declaration of Helsinki.
Patient Selection
Patients with stage III NSCLC who received immunotherapy and radical radiotherapy between January 2020 and December 2023 were identified through a hospital information system search using the keyword “lung malignant tumor.” After deduplication, patients were manually screened to ensure they met the following criteria:
- Pathologically confirmed diagnosis: Histologically verified NSCLC.
- Stage III classification: Defined by the 8th edition AJCC staging system.
- Radiotherapy requirements:
- Received SIB-IMRT with PGTV ≥ 60 Gy and PTV ≥ 50 Gy.
- Daily fractionation of 2–2.25 Gy, cumulative dose ≥ 60 Gy.
- Excluded: Patients treated with hypofractionation, 3D-CRT, or SBRT.
- Immunotherapy: At least one cycle of immunotherapy (neoadjuvant or adjuvant).
- Dosimetric data: Availability of SIB-IMRT dosimetric parameters.
- Follow-Up: Minimum 6 months post-radiotherapy.
- Imaging: Pre-treatment and 6-month post-treatment chest CT scans.
- Genetic exclusion: EGFR/ALK-positive patients excluded due to targeted therapy interference.
Clinical and demographic data, including age, gender, smoking status, pathological information, TNM staging, ECOG performance status, treatment complications, and chemotherapy/immunotherapy regimens, were extracted from the health information system (HIS). TNM staging was determined using enhanced chest CT, MRI of the head, abdominal CT/ultrasound, bone scan, or PET-CT. Radiation-related data were retrieved from the Eclipse treatment planning system (Varian Medical Systems, Palo Alto, CA), including total radiation dose, GTV, PTV-g, PTV-c, mean lung dose (MLD), lung V5 and V20, mean heart dose, heart V30 and V50, maximum spinal cord dose, and mean body dose.
4D-CT Simulation
Prior to scanning, patients received breathing instructions emphasizing diaphragmatic respiration and were positioned comfortably in a thermoplastic mask with arms elevated. Respiratory motion was monitored using the Varian Respiratory Gating for Scanners (RGSC) system. A reflective marker placed on the epigastric region tracked abdominal movement, while real-time visual feedback via the couch-mounted coaching device recorded respiratory signals. Acquired images were synchronized with respiratory data using G.E. Advantage 4D software to reconstruct ten-phase 4D-CT datasets and generate maximum intensity projection (MIP) images. These datasets were transferred to the Eclipse treatment planning system (v15.6, Varian Medical Systems) for subsequent contouring.
Target and OAR Delineation
All target volumes adhered to International Commission on Radiation Units and Measurements (ICRU) Reports 62 and 83.11,12 Organs at risk (OARs) included lungs, heart, esophagus, and spinal cord.
For 4D-CT-based planning:
- GTV Definition: The GTV was delineated on both the MIP dataset (designated IGTVMIP) and across all ten respiratory phases (GTV0–GTV90). A composite IGTV structure was created by transferring phase-specific GTV contours onto the MIP reference.
- ICTV Construction: Internal clinical target volumes (ICTV) were derived by expanding IGTV margins according to histology: 0.6 cm for squamous cell carcinoma and 0.8 cm for adenocarcinoma in primary lesions.13 Lymph node margins followed size-dependent criteria: 0.3 cm for nodes <2 cm short-axis and 0.5 cm for ≥2 cm.14 Manual adjustments were applied as described in prior protocols.15
- PTV Generation: Two planning target volumes were created: PTV-g (IGTV + 0.5 cm) and PTV-c (ICTV + 0.5 cm).
For non-4D-CT planning:
- GTV Definition: The gross tumor volume encompassed primary lesions and lymph nodes (short-axis >1 cm on CT/PET), subdivided into GTV-p (primary) and GTV-nd (nodal).
- CTV Construction: Histology-specific margins were applied: 0.6 cm (squamous) or 0.8 cm (adenocarcinoma) for primary CTV-p, and 0.3–0.5 cm for nodal CTV-nd based on size thresholds.13,14 Manual editing excluded adjacent critical structures.
- PTV Generation: Final PTVs included PTV-g (GTV + 0.5 cm) and PTV-c (CTV + 0.5 cm).
Intensity-Modulated Radiotherapy (IMRT) Treatment Plan
Two distinct IMRT strategies were designed:
- PTV-c 60Gy Plan: Prescribed 60Gy to the PTV-c in 30 fractions (2Gy/fraction).
- Three-Ladder Radiotherapy (3L-RT) Strategy: Delivered simultaneous doses of 54Gy to PTV-c, 60Gy to PTV-g, and 74Gy to GTV over 30 fractions.
All plans adhered to established clinical criteria, with the following organ-at-risk (OAR) constraints:
Lungs: V20 <30%, mean dose <20Gy
Esophagus: Max dose <64Gy, V60 <10cc
Heart: V20 <30%, V30 <40%
Spinal cord: Max dose <45Gy (preferably <40Gy)
Evaluation of Treatment Efficacy
Overall survival (OS) was measured from the date of initial diagnosis until the last follow-up (July 1, 2024), death, or loss to follow-up. Progression-free survival (PFS) was measured from diagnosis until disease progression, death, or last follow-up. Estimated radiation doses to immune cells (EDIC) for each patient were calculated were calculated using mean heart dose, mean lung dose, and integrated total dose volume (ITDV), following methodologies detailed in previous literature.9,16
Statistical Analysis
Statistical analyses were conducted using R software (v4.3.3). Normality and variance homogeneity of continuous variables were first verified. Comparative analyses employed the Kruskal–Wallis test (non-parametric) or paired t-test (parametric), while categorical variables were assessed via Chi-square tests. Survival outcomes (OS/PFS) were analyzed using Kaplan-Meier estimates with Log rank testing and visualized through the survival, survminer, survivalROC, and ggplot2 packages. Prognostic factors were identified via univariable and multivariable Cox regression (autoreg package). All tests adopted a significance threshold of p < 0.05.
Results
Study Population and Clinical Outcomes
Between January 2020 and December 2023, 89 consecutive stage III NSCLC patients undergoing definitive chemoradiation (SIB-IMRT technique) combined with immunotherapy were retrospectively analyzed. Baseline demographic and clinical characteristics are detailed in Table 1. The cohort predominantly comprised male subjects (93.3%), with a majority aged <65 years (66.3%) and exhibiting favorable performance status (ECOG 0, 66.3%). Most patients were non-COPD (93.3%), had a smoking history (76.4%), and presented with squamous cell carcinoma (77.5%). Treatment regimens included concurrent chemoradiation in 82% of cases versus sequential chemoradiation in 18%. Immunotherapy timing varied: 55.1% received neoadjuvant immunochemotherapy (Immuno-neoadj) prior to chemoradiation, while 44.9% underwent consolidative immunotherapy post-chemoradiation (Pacific-model).
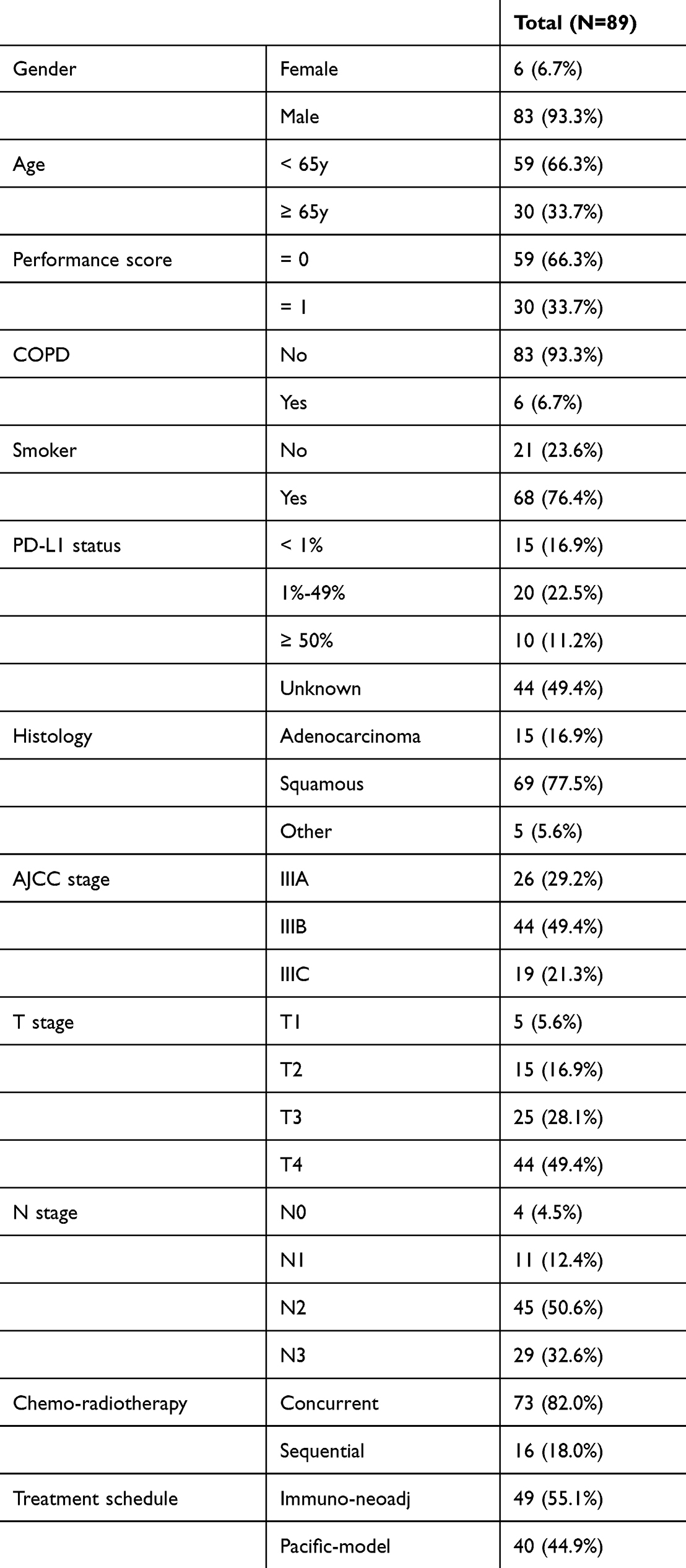 |
Table 1 Baseline Characteristics |
With a median follow-up of 23.2 months (IQR: 17.0–30.5), 45 patients experienced disease progression or death, yielding a median progression-free survival (PFS) of 19.4 months (Figure 1A, 95% CI: 16.3–NE). Overall survival (OS) analysis revealed 21 mortality events, with a median OS of 41.1 months (Figure 1B, 95% CI: 32.3–NE).
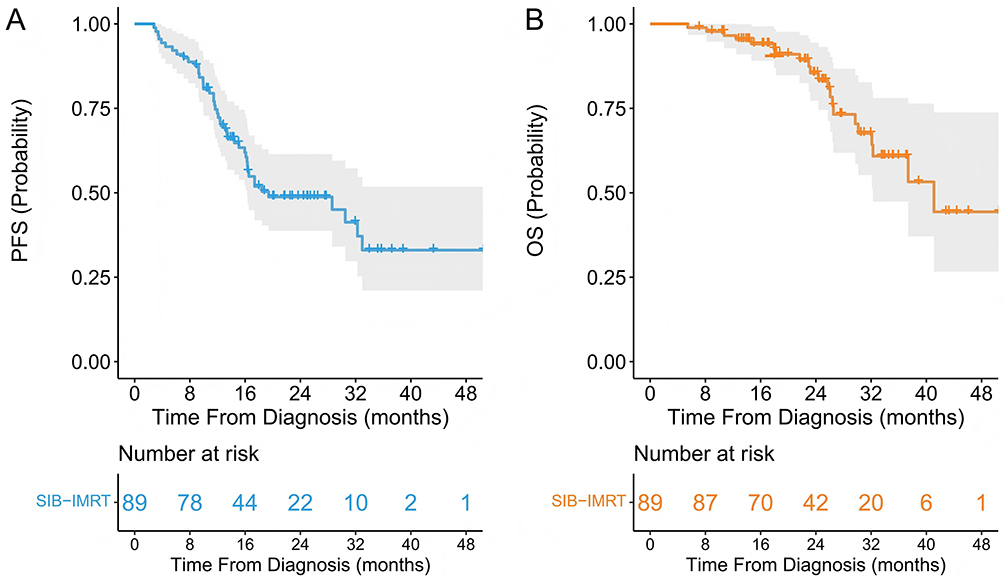 |
Figure 1 Progression-free survival (A) and overall survival (B) of stage III NSCLC patients treated with SIB-IMRT and immunotherapy. |
Univariate and multivariate Cox regression models evaluated variables with potential prognostic significance, including planning target volume (PTV) and effective radiation dose to immune cells (EDIC), previously implicated in NSCLC outcomes.9 Univariate analysis demonstrated significant associations between PFS and Immuno-neoadj therapy (Table 2, HR: 0.30, p < 0.001), AJCC IIIC staging (Table 2, HR: 3.40, p = 0.005), and elevated EDIC (Table 2, HR: 1.34, p = 0.0156). Multivariate analysis confirmed Immuno-neoadj (HR: 0.32, p < 0.001) and advanced AJCC stage (HR: 2.92, p = 0.019) as independent predictors of PFS (Table 2). For OS, univariate analysis identified Immuno-neadjuvant therapy as the sole significant prognosticator (HR: 0.25, p = 0.013; Table 2). Supplementary Figure 1A and B illustrates comparative survival outcomes between Immuno-neoadj and Pacific-model groups. Patients receiving neoadjuvant immunotherapy exhibited superior PFS (log-rank p < 0.0001) and OS (log-rank p = 0.0072) compared to those treated with the Pacific-model regimen.
 |
Table 2 Uni-Variate and Multi-Variate Cox Analyses of Factors Potentially Influencing Patient Prognosis |
Failure Pattern Analyses
Among 89 patients under surveillance, 43 (48.3%) demonstrated radiographically confirmed disease progression during follow-up. Consistent with prior investigations,17 we conducted a detailed failure pattern analysis categorizing progression into three distinct entities: local failure (persistence/growth at primary tumor site and initially involved regional lymph nodes), regional failure (new nodal involvement in ipsilateral hilar, mediastinal, or supraclavicular stations excluding previously metastatic nodes), and distant metastasis (metastatic spread beyond the above regions).
Representative cases are illustrated in Figure 2A and B. Figure 2A demonstrates local failure characterized by primary tumor enlargement, while Figure 2B exhibits regional failure manifesting as new-onset left supraclavicular LN metastasis (Supplementary Figure 1C). Among progression events, local failure occurred in 23 patients (53.5%), regional failure in 7 (16.3%), and distant metastases in 22 (51.2%), with 2 patients (4.7%) exhibiting concurrent local, regional, and distant failures (Figure 2C). Notably, primary tumor enlargement was universally observed in all local failure cases.
 |
Figure 2 Failure pattern analyses. (A) A representative case of local failure due to primary tumor enlargement. Panels show: (i) pre-treatment diagnostic chest CT; (ii) post-chemoradiotherapy response assessment CT; (iii) radiation dose distribution map of the planning target volume (PTV); (iv) follow-up CT at the time of local recurrence showing tumor progression. (B) A representative case of regional failure presenting as new-onset left supraclavicular lymph node metastasis. Panels show: (i) pre-treatment diagnostic chest CT; (ii) post-chemoradiotherapy response assessment CT; (iii) radiation dose distribution map of the PTV; (iv) follow-up CT at the time of regional recurrence revealing the new metastatic lymph node. (C) Percentage of local, regional, and distant failures in stage III NSCLC patients treated with SIB-IMRT and immunotherapy (D) Number of cases with organ-specific distant metastasis. |
Regarding distant metastases (Figure 2D), pulmonary sites predominated (n=8), followed by osseous (n = 7) and intracranial involvement (n = 6). Less frequent sites included hepatic metastases (n = 2), with isolated cases of adrenal (n = 1) and pleural metastases (n = 1).
Dosimetric Analysis of the Three-Ladder Radiotherapy Strategy
The positive correlation between radiation dose and local control has been well-established in lung cancer. Early studies, such as RTOG 73–01 and a modified Phase I/II trial from North Carolina, demonstrated that a biological effective dose (BED) ≥74 Gy significantly improves local control rates.18,19 However, traditional techniques failed to achieve safe dose escalation due to cardiopulmonary toxicity. The failure of RTOG 0617 further highlighted the risks of indiscriminate physical dose escalation (74 Gy vs. 60 Gy), which increased cardiac V40 and lymphocyte depletion, ultimately compromising survival.6,7 This underscores the critical need for organ protection and precise target delineation. Recent advances in image-guided dose escalation, such as those seen in the RTOG 1106 trial, have demonstrated that adapting the radiation dose in radiotherapy led to 2-year rates of infield and overall local regional tumor control (including isolated nodal failure) of 82% (95% CI, 62%–92%) and 62% (95% CI, 43%–77%), respectively. This supports the feasibility of selective dose delivery.20
Building on this concept and motivated by the observation of persistent local failures in our institutional cohort treated with standard SIB-IMRT and immunotherapy, we sought to design a novel escalation strategy that directly targets the primary tumor volume while minimizing collateral exposure. This led to the proposal of the “Three-Ladder Radiotherapy (3L-RT)” protocol, which prescribes a spatially focused high dose of 74 Gy to the gross tumor volume (GTV), a prophylactic dose of 60 Gy to involved nodal regions (PTV-g), and a reduced elective dose of 54 Gy to uninvolved nodal basins (PTV-c).
This approach is hypothesized to address the historical limitations in two ways: (1) by providing targeted dose intensification to the site of highest recurrence risk (the primary GTV) to potentially improve local control, and (2) by hierarchically reducing doses to adjacent elective volumes, thereby constraining integral cardiopulmonary doses (eg, lung V20, heart V30) to avoid the toxicity profile that compromised earlier escalation attempts. Importantly, this strategy aims to achieve selective intensification without relying on resource-intensive adaptive radiotherapy platforms,21 enhancing its potential applicability in broader clinical settings.
To validate this strategy, we performed a dosimetric feasibility analysis comparing 3L-RT to conventional radiotherapy (PTV-c 60 Gy) under two scenarios: with and without 4D-CT simulation to address respiratory motion errors. The study included 49 stage III NSCLC patients treated with definitive 4D-CT IMRT at Xiangxi Autonomous Prefecture People’s Hospital between Jan 1 and May 31, 2023, as reported in our previous study,22 and 50 stage III NSCLC patients treated with definitive radiotherapy at the Third Xiangya Hospital (without 4D-CT simulation) between Jan 1 and Dec 31, 2023. Without 4D-CT (Figure 3) supplementary table 1 summarized the dose coverage parameters of the two plans), the 3L-RT strategy significantly reduced cardiopulmonary exposure compared to conventional plans. Lung V5 decreased from 43.852% to 43.074%, V20 from 20.234% to 19.646%, and mean lung dose from 12.36 Gy to 11.734 Gy (Figure 3A–C). Cardiac V20 dropped from 15.914% to 14.936%, V30 from 9.55% to 8.706%, and mean heart dose from 9.026 Gy to 8.440 Gy (Figure 3D–F). Maximum spinal cord dose remained comparable (Figure 3G), but effective dose to immune cells (EDIC) decreased from 3.9 Gy to 3.694 Gy, suggesting reduced lymphocyte damage (Figure 3H, p < 0.001). With 4D-CT (Figure 4), the dose coverage parameters of the two plans were presented in supplementary table 2), the three-ladder strategy maintained significantly reduced lung doses (V5, V20, mean dose) and cardiac parameters (V20, V30, mean dose) as well as EDIC, without significant differences in spinal cord dose, demonstrating consistent organ sparing even with motion management.
 |
Figure 3 Dosimetry analyses of three-ladder radiotherapy strategy vs. conventional strategy without 4D-CT. (A) Volume of bilateral lungs receiving 5 Gy (V5). (B) Volume of bilateral lungs receiving 20 Gy (V20). (C) Mean dose to the bilateral lungs. (D) Volume of the heart receiving 20 Gy (V20). (E) Volume of the heart receiving 30 Gy (V30). (F) Mean dose to the heart. (G) Maximum dose to the spinal cord. (H) EDIC. |
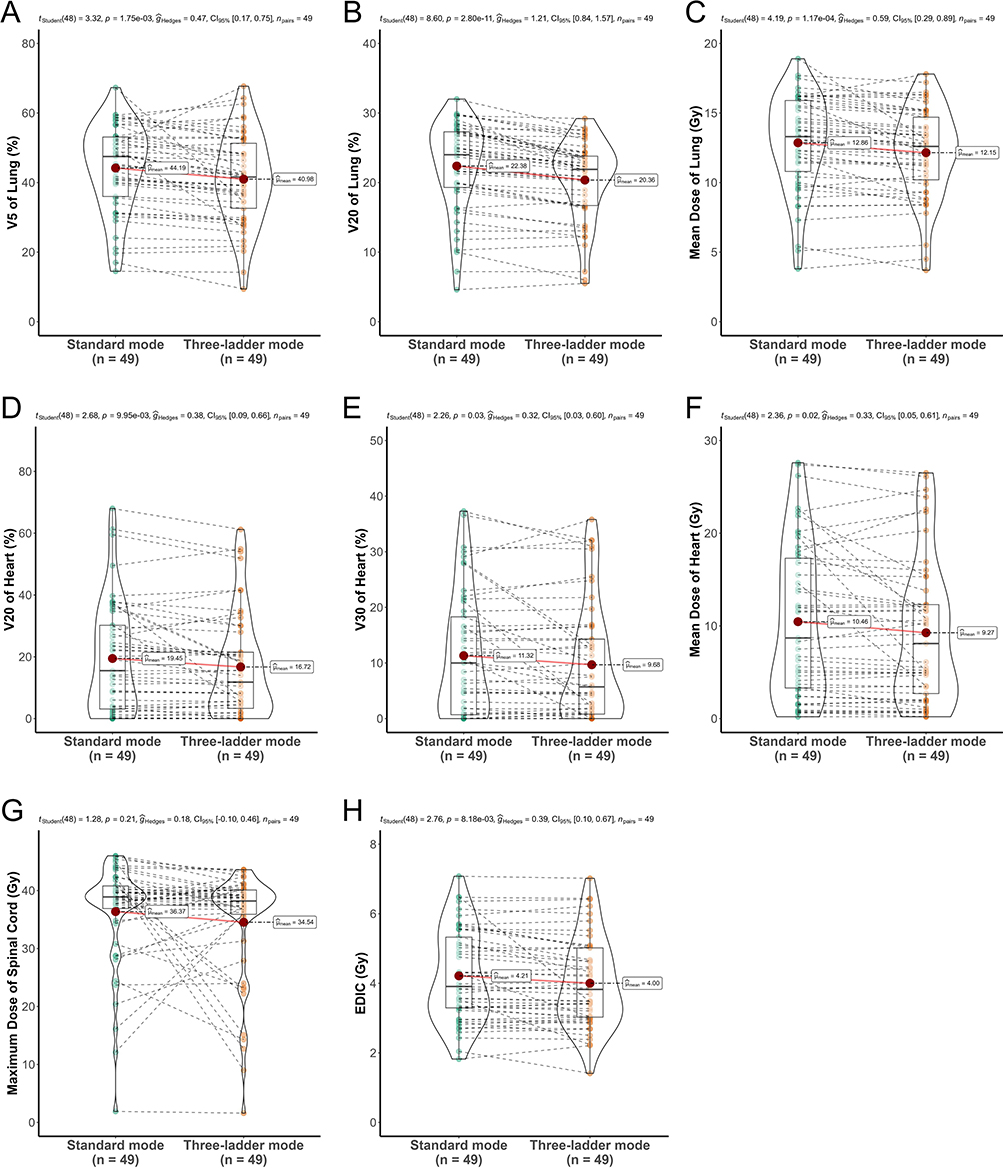 |
Figure 4 Dosimetry analyses of three-ladder radiotherapy strategy vs. conventional strategy with 4D-CT. (A) Volume of bilateral lungs receiving 5 Gy (V5). (B) Volume of bilateral lungs receiving 20 Gy (V20). (C) Mean dose to the bilateral lungs. (D) Volume of the heart receiving 20 Gy (V20). (E) Volume of the heart receiving 30 Gy (V30). (F) Mean dose to the heart. (G) Maximum dose to the spinal cord. (H) EDIC. |
Discussion
Revisiting Local Failure in the Immunotherapy Era: A Call for Radiotherapy Optimization
The integration of immunotherapy with CCRT has redefined therapeutic paradigms for stage III NSCLC, yet our analysis of 89 patients reveals a sobering reality: nearly half (48.3%, 43/89) experienced disease progression, with primary tumor enlargement constituting the dominant failure mode (25.8%, 23/89). This pattern mirrors historical cohorts treated with CCRT alone, such as the RTOG 9410 trial, where locoregional failure rates reached 35% despite dose escalation to 69.6 Gy.23 Among 100 patients with unresectable stage III A-C NSCLC treated with the PACIFIC regimen, at a median follow - up time of 18 months, 50 patients had progression, including 16 local recurrences (32%), 17 distant progressions (34%), and 17 with both (34%), respectively.24 This similar local progression rate (33 patients, 33%) underscores a critical dichotomy: while consolidation durvalumab enhances systemic control, its efficacy against macroscopic residual disease may be limited by the immunosuppressive tumor microenvironment post-radiation. Mechanistically, radiation-induced fibrosis and vascular damage may impair T-cell infiltration into bulky tumors.25 Thus, optimizing radiotherapy to achieve maximal cytoreduction before immunotherapy-induced immune exhaustion becomes paramount.
The Three-Ladder Strategy: Bridging Historical Lessons and Modern Immuno-Radiotherapy Principles
The three-ladder radiotherapy strategy (GTV 74 Gy, PTV-g 60 Gy, PTV-c 54 Gy) represents a paradigm shift from “one-size-fits-all” dose escalation to risk-adapted, spatially fractionated delivery. Our approach is grounded in three pillars:
- Selective Target Intensification: By escalating the GTV dose to 74 Gy—a threshold associated with >90% tumor control probability in hypofractionated models—we aim to eradicate radioresistant clones within the primary tumor.
- Prophylactic Volume De-escalation: Reducing PTV-g/c doses to 60 Gy/54 Gy prioritizes organ-at-risk (OAR) sparing, addressing the fatal flaw of RTOG 0617, where non-selective 74 Gy increased cardiac V40 and mortality.6,26,27 Our dosimetric data confirm that hierarchical de-escalation lowers lung V20 (19.6% vs. 20.2%) and heart V30 (8.7% vs. 9.6%), parameters independently linked to radiation pneumonitis and cardiovascular mortality.7,10
- Lymphocyte-Sparing Design: The reduction in EDIC with the three-ladder strategy may preserve systemic immunity, a factor increasingly recognized as a determinant of immunotherapy response.9,16 A recent study has shown that the recovery from lymphopenia is closely associated with an improved survival rate in patients receiving concurrent chemoradiotherapy (CCRT) and adjuvant immunotherapy. Additionally, a strong correlation between the radiation dose to large vessels and lymphopenia was observed at the conclusion of CCRT.28 This finding aligns with our EDIC results and implies that preserving lymphocytes could enhance the effectiveness of checkpoint inhibitors.
Technical and Biological Synergy with Immunotherapy
The interplay between radiotherapy dose gradients and immune activation warrants special emphasis. RT has an immunomodulating effect, stimulating the immune system via ICD-induced antigen presentation (auto-vaccination), reducing MDSCs, modifying macrophage polarization, increasing PD-1 tumor expression and stimulating vascular modification, all potentially altering the tumor microenvironment.29 However, how to reduce the dose received by vital organs at risk such as blood vessels, heart, and lungs, and better protect lymphocytes is also the key to further improving the prognosis of patients with stage III lung cancer in the era of immunotherapy.9,16,28 Our three-ladder strategy capitalizes on this duality: the 74 Gy GTV component (delivered in 2 Gy/fraction equivalents) could maximize immunogenic cell death, while lower doses to elective nodal regions minimize bystander lymphoid tissue damage. Similar studies, such as those that perform SBRT on the primary lesion and IMRT on regional lymph nodes, are also currently underway (NRG Oncology LU-008 trial). Furthermore, the strategy’s compatibility with conventional 3D-CRT or IMRT platforms (without mandating SBRT or PET-guided adaptation) enhances its applicability in resource-constrained settings, addressing a key barrier to global implementation of RTOG 1106-style protocols.21
Beyond Dosimetry: Clinical Translation and Unanswered Questions
While our dosimetric data validate the feasibility of the three-ladder approach, several translational challenges must be navigated:
- Temporal Optimization of Immunotherapy: Currently, the strategy of moving immunotherapy forward has been implemented in multiple Phase II–III clinical studies. Although Phase II studies such as KEYNOTE-799 have shown good progression-free survival (PFS) outcomes with concurrent chemoradiation therapy (CRT) and immunotherapy in stage III lung cancer,30 Phase III clinical studies represented by PACIFIC-2 (NCT03519971) did not meet the research expectations. In addition, neoadjuvant immunotherapy combined with chemotherapy followed by concurrent chemoradiation therapy has also shown better prognosis data than the PACIFIC model.10,31 Therefore, whether our strategy can achieve better prognosis outcomes with earlier immunotherapy exposure remains unknown. Moreover, preclinical data suggest that high-dose radiation concurrent with PD-1 blockade may exacerbate immune-related adverse events,32 necessitating careful toxicity monitoring in future trials.
- Biomarker-Driven Personalization: Not all patients require GTV escalation. Integrating circulating tumor DNA (ctDNA) clearance post-CCRT—a predictor of residual disease33—could refine patient selection for dose intensification.
- Long-Term Toxicity Considerations: Although our analysis focused on acute dosimetric endpoints, late effects such as cardiac dysfunction (median onset: 2–5 years post-radiation) demand longitudinal follow-up. Prospective studies should incorporate advanced cardiac imaging (eg, MRI strain analysis) to detect subclinical damage.
Limitations as Stepping Stones for Future Research
Several limitations of this study warrant consideration. First, its retrospective, two-center design limits the ability to establish causal inferences and may introduce unmeasured confounding. Second, the sample size, though consecutive, is relatively limited. This particularly constrains the statistical power and generalizability of the multivariable analyses, increasing the risk of overfitting despite our methodological precautions. Third, as treatment assignments (immuno-neoadjuvant vs. PACIFIC-model consolidation) were not randomized, selection bias between these groups cannot be fully ruled out, even after statistical adjustment. Fourth, while the 3L-RT strategy demonstrated promising dosimetric feasibility with and without 4D-CT simulation in our planning study, its clinical efficacy and safety require prospective validation in larger, more diverse cohorts. Finally, the EDIC metric serves as a planning surrogate for estimating lymphocyte radiation exposure; direct immunophenotyping in future clinical trials will be essential to elucidate the strategy’s precise immunological impact.
Conclusion
This study confirms that local failure remains the predominant pattern of recurrence following contemporary immuno-radiotherapy for stage III NSCLC. In response, we proposed a novel three-ladder radiotherapy (3L-RT) strategy for selective dose escalation. Dosimetric analysis supports its technical feasibility, achieving 74 Gy to the GTV while maintaining standard cardiopulmonary and lymphocyte dose constraints. However, the 3L-RT strategy has not been clinically tested. Its future application must consider patient selection factors (eg, tumor location, volume, cardiopulmonary function) and evaluate potential toxicity trade-offs in a prospective setting. Therefore, this work primarily provides a dosimetrically rational framework for future clinical trials to determine whether such targeted dose intensification can improve outcomes in stage III NSCLC.
Abbreviations
3L-RT, three-ladder radiotherapy; NSCLC, non-small cell lung cancer; PFS, progression-free survival; OS, overall survival; EDIC, effective dose to immune cells; CCRT, concurrent chemoradiotherapy; DM, GTV, distant metastases; gross tumor volume; SIB-IMRT, simultaneous integrated boost intensity modulated radiotherapy; OAR, organ-at-risk; iCTV, Internal clinical target volumes.
Data Sharing Statement
The raw data supporting the findings of this study are available from the corresponding author, Honghua Peng, upon reasonable request. Please use the contact information provided in the article.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work is supported by the Clinical and Medical Technology Innovation Guidance Project of Hunan Province (No. 2021SK53720).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Girard N, Bar J, Garrido P, et al. Treatment characteristics and real-world progression-free survival in patients with unresectable stage III NSCLC who received durvalumab after chemoradiotherapy: findings from the PACIFIC-R study. J Thorac Oncol. 2023;18(2):181–14. doi:10.1016/j.jtho.2022.10.003
2. Spigel DR, Faivre-Finn C, Gray JE, et al. Five-year survival outcomes from the PACIFIC trial: durvalumab after chemoradiotherapy in stage III Non–small-cell lung cancer. J Clin Oncol. 2022;40(12):1301–1311. doi:10.1200/JCO.21.01308
3. Kishi N, Matsuo Y, Shintani T, et al. Recurrence patterns and progression-free survival after chemoradiotherapy with or without consolidation durvalumab for stage III non-small cell lung cancer. J Radiat Res. 2023;64(1):142–153. doi:10.1093/jrr/rrac057
4. Offin M, Shaverdian N, Rimner A, et al. Clinical outcomes, local–regional control and the role for metastasis-directed therapies in stage III non-small cell lung cancers treated with chemoradiation and durvalumab. Radiother Oncol. 2020;149:205–211. doi:10.1016/j.radonc.2020.04.047
5. Suwa T, Kobayashi M, Nam J-M, Harada H. Tumor microenvironment and radioresistance. Exp Mol Med. 2021;53(6):1029–1035. doi:10.1038/s12276-021-00640-9
6. Bradley JD, Hu C, Komaki RR, et al. Long-term results of NRG oncology RTOG 0617: standard- versus high-dose chemoradiotherapy with or without cetuximab for unresectable stage III non–small-cell lung cancer. J Clin Oncol. 2020;38(7):706–714. doi:10.1200/JCO.19.01162
7. Chun SG, Hu C, Komaki RU, et al. Long-term prospective outcomes of intensity modulated radiotherapy for locally advanced lung cancer: a secondary analysis of a randomized clinical trial. JAMA Oncol. 2024;10(8):1111–1115. doi:10.1001/jamaoncol.2024.1841
8. Friedes C, Iocolano M, Lee SH, et al. The effective radiation dose to immune cells predicts lymphopenia and inferior cancer control in locally advanced NSCLC. Radiother Oncol. 2024;190:110030. doi:10.1016/j.radonc.2023.110030
9. McCall NS, McGinnis HS, Janopaul-Naylor JR, et al. Impact of radiation dose to the immune cells in unresectable or stage III non-small cell lung cancer in the durvalumab era. Radiother Oncol. 2022;174:133–140. doi:10.1016/j.radonc.2022.07.015
10. Song Z, Zhang X, Ma Y, Ma S, Feng Z, Liu X. Adaptive radiation strategy with V20 limitation associates with survival benefit and lower incidence of symptomatic radiation pneumonitis in stage III NSCLC patients receiving concurrent immunotherapy and thoracic radiation. Transl Oncol. 2025;51:102184. doi:10.1016/j.tranon.2024.102184
11. Morgan-Fletcher SL. Prescribing, recording and reporting photon beam therapy (supplement to ICRU report 50), ICRU report 62. ICRU, pp. ix+52, 1999 (ICRU Bethesda, MD) $65.00 ISBN 0-913394-61-0. British J Radiol. 2001;74(879):294. doi:10.1259/bjr.74.879.740294
12. Hodapp N. Der ICRU-Report 83: verordnung, Dokumentation und Kommunikation der fluenzmodulierten Photonenstrahlentherapie (IMRT). Strahlentherapie und Onkologie. 2012;188(1):97–100. doi:10.1007/s00066-011-0015-x
13. Yuan S, Meng X, Yu J, et al. Determining optimal clinical target volume margins on the basis of microscopic extracapsular extension of metastatic nodes in patients with non–small-cell lung cancer. Int J Radiat Oncol Biol Phys. 2007;67(3):727–734. doi:10.1016/j.ijrobp.2006.08.057
14. Yuan S, Sun X, Li M, et al. A randomized study of involved-field irradiation versus elective nodal irradiation in combination with concurrent chemotherapy for inoperable stage III nonsmall cell lung cancer. Am J Clin Oncol. 2007;30(3):239–244. doi:10.1097/01.coc.0000256691.27796.24
15. Xia F, Zhou L, Yang X, et al. Is a clinical target volume (CTV) necessary for locally advanced non-small cell lung cancer treated with intensity-modulated radiotherapy? —a dosimetric evaluation of three different treatment plans. J Thorac Dis. 2017;9(12):5194–5202. doi:10.21037/jtd.2017.10.147
16. Jin J-Y, Hu C, Xiao Y, et al. Higher radiation dose to the immune cells correlates with worse tumor control and overall survival in patients with stage III NSCLC: a secondary analysis of RTOG0617. Cancers. 2021;13(24):6193. doi:10.3390/cancers13246193
17. Zou L, Chu L, Xia F, et al. Is clinical target volume necessary?—a failure pattern analysis in patients with locally advanced non-small cell lung cancer treated with concurrent chemoradiotherapy using intensity-modulated radiotherapy technique. Transl Lung Cancer Res. 2020;9(5):1986–1995. doi:10.21037/tlcr-20-523
18. Perez CA, Pajak TF, Rubin P, et al. Long-term observations of the patterns of failure in patients with unresectable non-oat cell carcinoma of the lung treated with definitive radiotherapy report by the radiation therapy oncology group. Cancer. 1987;59(11):1874–1881. doi:10.1002/1097-0142(19870601)59:11<1874::AID-CNCR2820591106>3.0.CO;2-Z
19. Stinchcombe TE, Lee CB, Moore DT, et al. Long-term follow-up of a phase I/II trial of dose escalating three-dimensional conformal thoracic radiation therapy with induction and concurrent carboplatin and paclitaxel in unresectable stage IIIA/B non-small cell lung cancer. J Thorac Oncol. 2008;3(11):1279–1285. doi:10.1097/JTO.0b013e31818b1971
20. Kong F-M, Ten Haken RK, Schipper M, et al. Effect of midtreatment PET/CT-adapted radiation therapy with concurrent chemotherapy in patients with locally advanced non–small-cell lung cancer. JAMA Oncol. 2017;3(10):1358–1365. doi:10.1001/jamaoncol.2017.0982
21. Kong F-M (Spring), Hu C, Pryma DA, et al. Primary results of NRG-RTOG1106/ECOG-ACRIN 6697: a randomized phase ii trial of individualized adaptive (chemo)radiotherapy using midtreatment18 F-fluorodeoxyglucose positron emission tomography/computed tomography in stage III non–small cell lung cancer. J Clin Oncol. 2024;42(33):3935–3946. doi:10.1200/JCO.24.00022
22. Ding W, Xu T, Xiang H, et al. Is clinical target volume necessary for locally advanced non-small cell lung cancer treated with 4D-CT intensity-modulated radiation therapy. BMC Cancer. 2024;24(1):1198. doi:10.1186/s12885-024-12979-z
23. Curran WJ Jr, Paulus R, Langer CJ, et al. Sequential vs concurrent chemoradiation for stage III non-small cell lung cancer: randomized Phase III trial RTOG 9410. J Natl Cancer Inst. 2011;103(19):1452–1460. doi:10.1093/jnci/djr325
24. Filippi ARR, Saddi J, Agustoni F, et al. 123P second progression-free survival (PFS2) after first progression in patients receiving PACIFIC regimen: an exploratory analysis of the blue sky observational study. J Thoracic Oncol. 2023;18(4):S110. doi:10.1016/S1556-0864(23)00378-7
25. Barker HE, Paget JTE, Khan AA, Harrington KJ. The tumour microenvironment after radiotherapy: mechanisms of resistance and recurrence. Nat Rev Cancer. 2015;15(7):409–425. doi:10.1038/nrc3958
26. Bradley JD, Paulus R, Komaki R, et al. Standard-dose versus high-dose conformal radiotherapy with concurrent and consolidation carboplatin plus paclitaxel with or without cetuximab for patients with stage IIIA or IIIB non-small-cell lung cancer (RTOG 0617): a randomised, two-by-two factorial Phase 3 study. Lancet Oncol. 2015;16(2):187–199. doi:10.1016/S1470-2045(14)71207-0
27. Thor M, Apte A, Haq R, Iyer A, LoCastro E, Deasy JO. Using auto-segmentation to reduce contouring and dose inconsistency in clinical trials: the simulated impact on RTOG 0617. Int J Radiat Oncol Biol Phys. 2021;109(5):1619–1626. doi:10.1016/j.ijrobp.2020.11.011
28. Cho Y, Kim Y, Chamseddine I, et al. Lymphocyte dynamics during and after chemo-radiation correlate to dose and outcome in stage III NSCLC patients undergoing maintenance immunotherapy. Radiother Oncol. 2022;168:1–7. doi:10.1016/j.radonc.2022.01.007
29. Chicas-Sett R, Morales-Orue I, Castilla-Martinez J, et al. Stereotactic ablative radiotherapy combined with immune checkpoint inhibitors reboots the immune response assisted by immunotherapy in metastatic lung cancer: a systematic review. Int J Mol Sci. 2019;20(9):2173. doi:10.3390/ijms20092173
30. Jabbour SK, Lee KH, Frost N, et al. Pembrolizumab plus concurrent chemoradiation therapy in patients with unresectable, locally advanced, stage III non–small cell lung cancer. JAMA Oncol. 2021;7(9):1–9. doi:10.1001/jamaoncol.2021.2301
31. Ross HJ, Kozono D, Wang XF, et al. Atezolizumab before and after chemoradiation for unresectable stage III non–small cell lung cancer. JAMA Oncol. 2024;10(9):1212–1219. doi:10.1001/jamaoncol.2024.1897
32. Han C, Qiu J, Bai L, et al. Pneumonitis risk after chemoradiotherapy with and without immunotherapy in patients with locally advanced non-small cell lung cancer: a systematic review and meta-analysis. Int J Radiat Oncol Biol Phys. 2024;119(4):1179–1207. doi:10.1016/j.ijrobp.2024.01.217
33. Normanno N, Morabito A, Rachiglio AM, et al. Circulating tumour DNA in early stage and locally advanced NSCLC: ready for clinical implementation? Nat Rev Clin Oncol. 2025;22(3):215–231. doi:10.1038/s41571-024-00985-w
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Molecular Characteristics and the Effect of KRAS Mutation on the Prognosis of Immunotherapy in Non-Small Cell Lung Cancer in Xinjiang, China
Gu G, Yu B, Wan H, Lu S, Zhu X, Zhao Y, Fuxi Y, Liu C
OncoTargets and Therapy 2022, 15:1021-1032
Published Date: 21 September 2022
GBP5 Identifies Immuno-Hot Tumors and Predicts the Therapeutic Response to Immunotherapy in NSCLC
Fan H, Shi Y, Wang H, Li Y, Mei J, Xu J, Liu C
International Journal of General Medicine 2023, 16:1757-1769
Published Date: 10 May 2023
Clinical Significance and Molecular Annotation for PD-L1 Negative Advanced Non-Small Cell Lung Cancer with Sensitivity to Responsive to Dual PD-1/CTLA-4 Blockade
Wang L, Liu L, Zhao J, Yu X, Su C
ImmunoTargets and Therapy 2024, 13:435-445
Published Date: 6 September 2024
Effectiveness and Safety of Anlotinib-Related Therapeutic Regimens in Patients with Previously Immune Checkpoint Inhibitors-Treated Advanced NSCLC: A Real-World Exploratory Study
Fang XS, Zhang TS, Li SJ, Zhao YL, Li JB, Xia H, Wang RT
Drug Design, Development and Therapy 2025, 19:7527-7540
Published Date: 29 August 2025
Emerging Predictive Biomarkers of Immunotherapy Sensitivity in Patients with Non-Small Cell Lung Cancer
Gariazzo E, Colamartini F, Ubaldi M, Santo V, Brunetti L, Tomarelli C, Ognissanti D, Nassar J, Costabile S, Romano L, De Vita E, Scorpiniti I, Macrì M, Porreca R, Currà MF, Cortellini A, Ricciuti B, Metro G
ImmunoTargets and Therapy 2026, 15:567238
Published Date: 2 February 2026