")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 19
Use of Ecological Momentary Assessment to Measure Dyspnea in COPD
Authors Miller SN , Nichols M , Teufel II RJ, Silverman EP, Walentynowicz M
Received 1 November 2023
Accepted for publication 13 March 2024
Published 28 March 2024 Volume 2024:19 Pages 841—849
DOI https://doi.org/10.2147/COPD.S447660
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jill Ohar
Sarah N Miller,1 Michelle Nichols,1 Ronald J Teufel II,2 Erin P Silverman,3 Marta Walentynowicz4
1College of Nursing, Medical University of South Carolina, Charleston, South Carolina, SC, USA; 2College of Medicine, Medical University of South Carolina, Charleston, South Carolina, SC, USA; 3Division of Pulmonary, Critical Care, and Sleep Medicine, University of Florida, Gainesville, FL, USA; 4Center for the Psychology of Learning and Experimental Psychopathology, KU Leuven, Leuven, Belgium
Correspondence: Sarah N Miller, Medical University of South Carolina, College of Nursing, 99 Jonathan Lucas Street, Charleston, SC, 29425, USA, Tel +18437921692, Email [email protected]
Abstract: Dyspnea is an unpredictable and distressing symptom of chronic obstructive pulmonary disease (COPD). Dyspnea is challenging to measure due to the heterogeneity of COPD and recall bias associated with retrospective reports. Ecological Momentary Assessment (EMA) is a technique used to collect symptoms in real-time within a natural environment, useful for monitoring symptom trends and risks of exacerbation in COPD. EMA can be integrated into mobile health (mHealth) platforms for repeated data collection and used alongside physiological measures and behavioral activity monitors. The purpose of this paper is to discuss the use of mHealth and EMA for dyspnea measurement, consider clinical implications of EMA in COPD management, and identify needs for future research in this area.
Keywords: COPD, ecological momentary assessment, mobile health, dyspnea, mHealth, telehealth
Dyspnea, or the sensation of breathlessness or air hunger, is a highly unpleasant and debilitating sensation common in chronic obstructive pulmonary disease (COPD). The perception of dyspnea is highly individualized and influenced by airway pathology, individual interoceptive sensitivity, and previous exposure to dyspnea. Respiratory perception is a complex, multidimensional process that involves both the cognitive and affective evaluation of respiratory sensations.1 This two-stage process begins with the initial discriminative dimension, involving physical awareness of what one is feeling, followed by the assessment of how the sensations feel, when the individual evaluates and characterizes the sensation. The interoceptive process is unique to each person, incorporating tolerance, past experiences, and emotions alongside physiological stimuli. Measuring dyspnea presents challenges, as no diagnostic test or biomarker closely correlates with changes in dyspnea across all conditions or settings.2
Ecological momentary assessment (EMA), a technique developed within the behavioral sciences, allows researchers and clinicians to collect symptoms (eg, respiratory symptoms such as coughing), cognitions, affective state, and exposure in real-time within a natural environment.3 As the term ecological (relating to the natural living environment) indicates, short (momentary) reporting periods are used for assessment of symptoms occurring during everyday experiences. This reduces the risk of memory limitations, bias, and error.4 EMA is differentiated from other data collection methods by three main criteria: it is collected from patients in real-time, in the home or natural environment, and data elements (eg, symptoms) are repeatedly collected in brief moments over an extended period. Although the concept of collecting diary data and self-monitoring has a long history in clinical research, technological advances in the last decennia, in particular the introduction of smartphones, have led to increased use of this method in various fields, including psychopathology,5 chronic pain,6 and physical activity.7 In this commentary, we discuss the use of EMA, particularly via mobile (mHealth) technology for measurement of dyspnea, consider clinical implications for COPD management, and identify needs for future research.
Measurement of Dyspnea
Clinical measurement of dyspnea typically involves retrospective symptom recall via administration of questionnaires. Measures assess the three domains of dyspnea: sensory-perceptual, affective, and impact domains. These encompass how dyspnea feels (“the sensory-perceptual experience”), how distressing the dyspnea symptom seems (“affective distress”), and the functional, economic, quality-of-life, and health-related costs of dyspnea (“symptom impact or burden”).2 Examples include visual analog scales (VAS),2,8–10 Borg-style ratings of perceived dyspnea or exertion,11,12 numerical scales,13 and Likert-style instruments where the patient is asked to rate the intensity of a sensation or describe what that sensation feels like, typically in the moment where the patient encounters a very specific stimulus (eg, while walking normally, during exercise, breathing with a resistive load, etc.; see Table 1). While this degree of specificity may not precisely capture an individual’s clinical and day-to-day status, such measures are relatively quick to administer and carry a low burden. However, as these retrospective scales ask for recall over several days to weeks, they might be susceptible to recall bias.13,14 Affective distress is typically measured via either single- or multi-item scales that seek to determine how the patient feels about their dyspnea symptoms.8 Despite their similarities, affective and sensory-perceptual measures assess different responses to breathlessness. Ratings of intensity, level of unpleasantness, and amount of distress are examples of physical and psychological responses to an unpleasant stimulus (such as dyspnea) that are similar yet distinct.
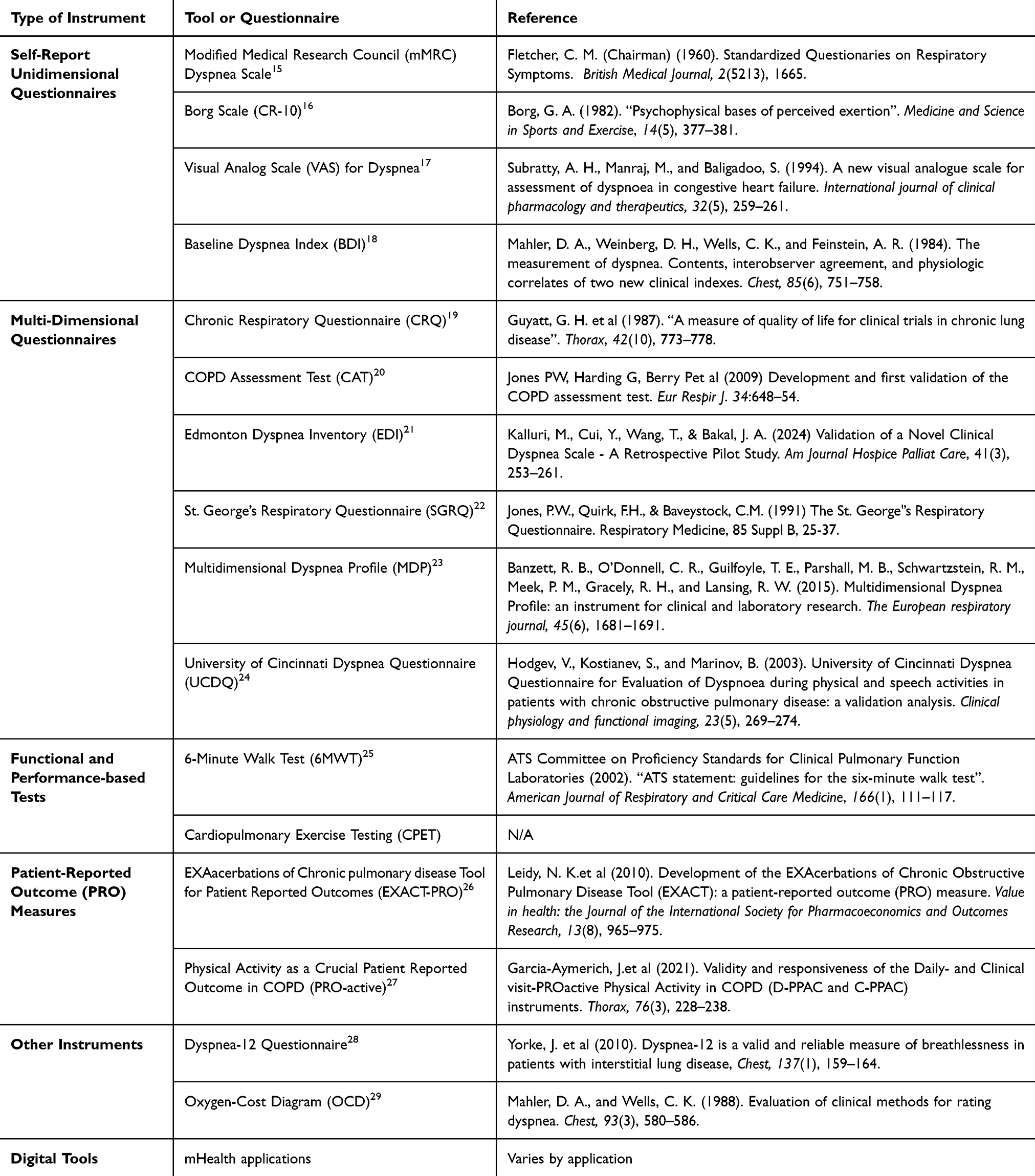 |
Table 1 Summary of Validated Tools and Questionnaires for Assessing Dyspnea |
Currently, the measurement of respiratory sensations exhibits variability concerning questionnaire wording, specific populations (patient or non-patient, patient homogeneity or heterogeneity), and the nature of the rating task (types of scales, qualitative descriptors, quantitative rates, free response options, etc.).2 The Multidimensional Dyspnea Profile (MDP)9 and the Dyspnea-1211,12 incorporate intensity ratings for sensory, quality, and affective descriptors to capture the multiple steps comprising the process of dyspnea perception. The American Thoracic Society (ATS) has emphasized the need to further validate and utilize measurement tools to facilitate comparison across dyspnea studies.2 Recognizing that no single measure comprehensively assesses all three of the core dyspnea sub-domains (sensory, affective, and impact), ATS recommends selecting measurement tools based on aspects of dyspnea that are most closely aligned with clinical or research objectives.
Limitations of Current Assessment Methods
As previously noted, most dyspnea self-report measures are retrospective and require summarizing the dyspnea experience outside of the naturalistic context. However, retrospective self-reported symptoms are susceptible to recall bias and unreliability compared to momentary assessment.13 Retrospective reports rely on memory, experience, and information processing, all of which pose a risk for bias, often resulting in retrospective misestimation of experienced symptoms. Previous studies employed paper symptom diaries to measure dyspnea and found variations in recall based on breathlessness intensity on study days.30 Written diaries have practical limitations, as they are cumbersome, easily lost, and verification of the date and time of recording is not reliable. For instance, participants might complete all diary entries in a single moment just before the control visit. While recall of breathlessness is important for clinical care,31 there remains a need to measure the patient’s current level of dyspnea and compare it to a baseline to assess symptoms or explore dyspnea variability following triggers or during certain activities. With increased confusion and memory loss more prevalent in those with COPD compared to those without,32 there is increased risk of inaccurate symptom reporting when relying on retrospective measures. Additionally, although current assessment measures allow for large-scale cross-sectional research, they are less suited to look at within-person, short-term associations. For example, few studies have measured dyspnea during acute exacerbations of COPD, leaving gaps in understanding of the prevalence and intensity of dyspnea during exacerbations.33
Ecological Momentary Assessment
EMA has been validated and useful to assess breathing (asthma and COPD) symptoms in research and clinical studies spanning from youth to adults.34–37 In a typical EMA protocol, patients are prompted to respond to brief surveys asking about their experiences in the moment or just before the prompt. By collecting data regarding momentary experiences in real-time, EMA minimizes recall bias and provides a more accurate representation of the patient’s experiences compared to traditional retrospective self-report measures. Those brief momentary surveys are delivered to the patients in their natural environment, enhancing the ecological validity of the assessment.3,5,31,38 This means that this measure is more representative of the patient’s real-world experiences, compared to the responses given in a clinical or research setting which can alter symptom experience (eg, “white coat” hypertension). Due to the large number of measurements or data points per individual, it is possible to conduct within-subject comparisons to characterize individual mean and variance.39 Self-report data from EMA surveys can be combined with behavioral and physiological data collected from wearable measurement tools (for example, activity trackers, heart rate monitors, mobile spirometry, or self-reporting inhaler devices). Such forms of data collection can be used not only for observational research but also combined with and used alongside interventions to strengthen interpretation of intervention effects, deliver personalized feedback to patients, and provide information about disease progression and status to providers to offer better quality of care.
It is important to note that while telehealth or telecare may seem similar to EMA (i.e. remote patient monitoring and communication healthcare technologies outside of traditional facilities), these are not explicitly considered EMA. Unlike EMA, which collects momentary data in real-time through brief surveys or measures in the patient’s natural environment, telehealth often relies on periodic or scheduled data collection, introducing recall or selection biases and lacking the ecological validity characteristic of EMA. Passive data collection techniques (e.g. remote patient monitoring such as self-reporting inhaler devices or activity sensors) are unable to measure the subjective and highly individual dyspnea experience. Telehealth encompasses more holistic care provision (including the consultation, diagnosis, treatment, and care management of the patient), typically with bidirectional communication between the provider and patient. However, communication technology is used to facilitate health care in telehealth, and EMA surveys can be integrated into telehealth platforms to provide real-time symptom monitoring and feedback to patients and providers.
Examples of mHealth-Enabled EMA of Dyspnea in COPD
As technology has progressed and been readily adopted, so has the ability to obtain frequent EMA with time stamps, especially via smartphones as a tool for mHealth data collection.38,40 To show that it is feasible to utilize a mHealth platform for EMA measurement of COPD-related dyspnea in the home environment, a number of recent studies will be showcased in this section.34,41–45 An initial broad-based search on PubMed helped define the scope of the literature, and the subsequent search strategy was to search abstracts for the following terms: (“copd” OR “chronic obstructive pulmonary disease”) AND (“EMA OR ecological momentary assessment”) AND (“mHealth OR mobile health”) to identify articles that reported on use of EMA via mHealth technology to measure dyspnea in patients with COPD. Studies were identified by team members through hand-searching of databases and platforms including Scopus, Healthcare Administration, PubMed and databases from EBSCOHost Platform including MEDLINE, CINAHL Complete, APA PsycInfo, Health Source: Nursing/Academic Edition, Consumer Health Complete – EBSCOhost, Psychology and Behavioral Sciences Collection.
The first study, a 2020 mHealth Prototype design pilot study, used a 3-Phase process to develop an EMA app with input from patients with COPD.44 During the first phase of the study, participants reported that symptom monitoring was important to their own COPD self-management due to difficulties recalling details and managing the complexity of COPD. Patients with COPD worked with researchers to make recommendations on symptom and medication monitoring and determined five symptoms to assess via EMA: breathlessness, coughing, mucus, tiredness, and sleep quality. During Phase 2, patients and one caregiver tested the mobile application and provided qualitative feedback on assessment measures, technology issues, and design elements (for example, a sliding graph vs a Likert scale for symptom assessment). While the Prototype study was focused on the co-design of a prototype mobile app for COPD, during rollout (Phase 3), researchers were able to capture breathlessness symptom data (n=37; n=31 with COPD) over a 4-month period. However, level of engagement was inconsistent between users. In this study, researchers tracked usage sequence and found that patients frequently entered the app to log symptoms, then viewed symptom data, which may provide value for self-monitoring and adaptation of treatment strategies for patients with COPD.
The feasibility trial (RESP-FIT) employed an EMA platform to collect symptoms in adults with COPD.34 Symptoms, including dyspnea, were assessed in real-time within the home environment using a technologically enabled mobile application (mHealth) platform and Bluetooth to track adherence. This study provides insight into dyspnea measurement using the Borg scale via EMA as dyspnea was measured using a modified Borg scale integrated into the mobile app. The Minimal Clinically Important (MCI) difference for dyspnea is typically defined as 1 unit on a modified Borg scale or 10mm on a 100mm visual analog scale.46 The modified Medical Research Council (mMRC)29,47 dyspnea measurement tool (Table 1) is a valuable discriminative instrument48 and was employed for determining eligibility as inclusion criteria. Participants used a mobile application with an integrated modified Borg scale (100mm visual analog sliding scale) to measure dyspnea through EMA. Over a 6-week data collection period, participants were prompted to daily utilize the smartphone application with Bluetooth tracking device (for adherence) to rate symptoms, including dyspnea, resulting in a total of 14,388 recorded actions in the app, encompassing various measurement points of dyspnea over time. The findings from this study explored the effects of a respiratory muscle strength training program on symptoms, including dyspnea and fatigue, and demonstrated the feasibility of collecting dyspnea ratings via mHealth technology in the home environment. It is important to note that the RESP-FIT study primarily aimed to establish feasibility and acceptability, and within-subject comparisons were not conducted, leaving room for investigation in future large-scale trials.
To explore how breathlessness memory is related to peaks or timing of the sensation, the Relating Experienced to Recalled Breathlessness (RETRO) study conducted in Sweden investigated the relationship between recalled and momentary (experienced) breathlessness.31 Researchers utilized EMA via mHealth to assess daily breathlessness and found that recalled breathlessness was significantly influenced by peak sensations of breathlessness, or the worst experiences, over a 1-week period. The authors posit this finding bears significance in clinical care when relying on recalled symptom reports. It should be considered in intervention development, as it may be optimal for interventions to target peak breathlessness rather than average breathlessness over a given period. It is worth noting that this study encompassed participants with undefined breathlessness, with only 40% self-reporting COPD. Other sources of dyspnea included conditions such as asthma, cardiovascular etiology, cancer, hypertension, and stroke. Given the comprehensive analysis of EMA to measure dyspnea or breathlessness in 34 patients with COPD, we have included it in this commentary as it provides valuable insights into this topic.
Finally, the SHINE study employed electronic “eDiaries” to assess shortness of breath in 209 patients with COPD, finding high patient compliance (81.3%) with symptom diaries over a 26-week study period.41 The diary assessments included five symptom items: cough, phlegm, shortness of breath, wheezing, and chest tightness, aiming to investigate frequency of symptom occurrence and how COPD symptoms impact the patient’s life. Patients with COPD entered their symptoms twice daily, once in the morning upon waking up and again during an evening assessment. While there was some element of recall involved in eDiary prompts (ie, ‘How many times did you wake up during the night because of your COPD?’), recall bias was mitigated due to the short recollection period and daily symptom entry. The SHINE study revealed a strong connection between shortness of breath and the overall impact of COPD (in terms of burden and activity), and notably, supported the validity and reliability of using an eDiary to measure patient-reported symptom severity and impact. An important limitation of this study was that only 33% of participants in this study were female. Given that COPD is more prevalent in and has a greater impact on women,49 future study demographics should take this into account.
Clinical Implications
The utilization of EMA for measuring dyspnea carries significant clinical implications and advantages. Firstly, EMA enhances the accuracy of data collection in a natural environment over an extended period. In a clinical context, EMA holds the potential for informed assessment, founded on real-time data collection, thereby mitigating recall bias. This reveals crucial details regarding symptoms, behaviors, and environmental triggers, facilitating context-specific considerations. EMA can be configured to capture data based on time, specific events, and/or geographical location, allowing investigation into environmental and seasonal effects on COPD. Reports generated using EMA encompass biobehavioral data and pinpoint triggers or activities that initiate or exacerbate symptoms or responses. This approach is versatile and applicable across a broad spectrum of clinical conditions and populations, especially with the increasing accessibility and prevalence of smartphone technology.
Data quality can be improved through more frequent and detailed data capture moments. Both time-based EMA (in regular intervals, for example every 4 hours or every morning) and event-based EMA (for example, when a dyspneic episode occurs or after exposure to an exacerbation trigger) provide deeper insight into the symptom experience and resulting health-related behaviors. This flexibility allows for targeted symptom reporting at specific times of the day, during events like the onset or exacerbation of symptoms, or based on location proximity to triggers that may elicit behaviors or responses. Enhanced data quality and accuracy will enable clinicians to identify trends in symptoms, assess severity of symptoms during individual events and over time, and develop personalized treatment plans. Moreover, EMA actively engages patients as integral members of their clinical care team, fostering a collaborative approach to healthcare and joint patient-provider decision-making.
EMA techniques have been used to match breathlessness with other data to provide a more holistic view of disease impact and exacerbation risks, along with physiological functioning and behavioral measures such as remote spirometry50 and activity trackers. For instance, clinicians can assess EMA dyspnea self-reports alongside data from an activity tracker to understand the impact of exercise or physical activity on dyspnea symptoms. This may provide insight into behaviors, such as activity avoidance, driven by fear of dyspnea. A validated patient-reported outcome tool such as the (PRO)active should be considered, as it captures the experience of physical activity with a strong correlation to dyspnea in patients with COPD.51
Importantly, self-reported app data can be used to predict COPD exacerbations with moderate discriminative ability. An example of this is the myCOPD mobile app, a digital momentary assessment symptom diary for patients with COPD that tracks characteristics of long-term COPD status using the COPD Assessment Test (CAT).52 A retrospective analysis of 2,374 patients using this system identified a relationship between symptom scores, CAT scores, and self-reported exacerbation events.53 An evaluation of four studies (three RCTs and one observational trial) using myCOPD identified potential cost savings in a subpopulation of AECOPD dependent upon myCOPD uptake and hospital readmissions.45 Finally, EMA in COPD may provide more robust insight into the role of adherence (medication, pulmonary rehabilitation exercises, disease management strategies) on dyspnea. While it is crucial to consider monthly average adherence and its impact on disease control, EMA analysis provides a deeper understanding of the factors linked to an individual patient’s adherence behavior. This enhanced understanding of adherence behavior can be leveraged to further customize interventions, maximize positive behavior, and mitigate disease burden.
Limitations
There are limitations to consider when recommending EMA via mHealth to measure dyspnea in COPD. Patients may feel burden due to frequent measurements or in cases where notifications prompt or remind someone to enter symptoms. Another important limitation to consider is the potential that increased monitoring may lead to burden on both the patient and the clinician with implications for increased healthcare utilization. When exploring cost per quality adjusted life year (QALY), telemonitoring may not be cost-effective54 and telehealth interventions have been associated with higher costs.55 Thus, the potential effects on healthcare utilization and cost-effectiveness should be considered when utilizing EMA in COPD. Also, age-related factors may pose a barrier to utilization of mHealth for EMA of dyspnea. While the RESP-FIT study did not find any age-related technological issues in older participants,34 Phase 2 of the Prototype study (n=5) reported that a sliding scale was not user-friendly and recommended a larger font size on mobile applications for older participants.44 Thus, digital literacy should be considered and further explored in EMA research in COPD. Finally, generation of large datasets with a complex structure leads to complicated and challenging statistical analyses. A well-designed Linear Mixed Model (LMM) or Generalized Linear Mixed Model (GLMM) can facilitate the analysis of ordinal and categorical data and accommodate inherent within-participant correlations, provided it is executed with a robust methodology based on pilot or previous data.56
Gaps and Future Research
While early reports are promising, there remains limited research on the use of EMA of dyspnea in COPD. Robust studies and randomized clinical trials are needed to explore clinical implications, environmental measurement capabilities and seasonal COPD exacerbations, and how physiological measures (i.e., remote spirometry) correlate with dyspnea in real-time. Along with digital literacy, social determinants of health (SDOH), particularly geographic location and access to resources such as food and internet, are unexplored in the EMA literature. To ensure accessibility of interventions and equal representation in future clinical trials, SDOH should be considered when considering the feasibility and acceptability of EMA techniques for patients with COPD. Additionally, qualitative research is needed to explore patient experiences, preferences, and needs as well as facilitators and barriers of EMA of dyspnea in COPD. With correct analysis, EMA can provide insights into patterns over time, individual or seasonal fluctuations, and situational variations. Future research should focus on defining systematic data collection strategies that utilize EMA to inform the development of a validated, standardized language for EMA measurement of dyspnea. This approach should not be limited to COPD but rather should be explored in other patient populations, such as those with cardiac conditions, enabling more accurate real-time measurement of dyspnea across various clinical conditions. This, in turn, will inform generalizable patient interventions and improve the clinical management of individuals with respiratory diseases.
Human Rights
No human subjects were involved in this project.
Informed Consent
No human subjects were involved in this project.
Welfare of Animals
This article does not contain any studies with animals performed by any of the authors.
Funding
This study was funded by the South Carolina Clinical & Translational Research (SCTR) Institute, with an academic home at the Medical University of South Carolina, National Institutes of Health/National Center for Advancing Translational Sciences (grant numbers KL2 TR001452 & UL1 TR001450), by the South Carolina Center for Rural and Primary Healthcare as part of the state’s rural health initiative, and by the South Carolina Telehealth Alliance (SCTA) Telehealth Translational Research Pilot Project Grant.
Disclosure
Dr Marta Walentynowicz reports grants from Research Foundation Flanders, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Davenport PW, Vovk A. Cortical and subcortical central neural pathways in respiratory sensations. Respir Physiol Neurobiol. 2009;167(1):72–86. doi:10.1016/j.resp.2008.10.001
2. Parshall MB, Schwartzstein RM, Adams L, et al. An official American thoracic society statement: update on the mechanisms, assessment, and management of dyspnea. Am J Respir Crit Care Med. 2012;185(4):435–452. doi:10.1164/rccm.201111-2042ST
3. Shiffman S, Stone AA, Hufford MR. Ecological momentary assessment. Annu Rev Clin Psychol. 2008;4:1–32. doi:10.1146/annurev.clinpsy.3.022806.091415
4. Stone AA, Schneider S, Smyth JM. Evaluation of pressing issues in ecological momentary assessment. Annu Rev Clin Psychol. 2023;19(1):107–131. doi:10.1146/annurev-clinpsy-080921-083128
5. Mestdagh M, Dejonckheere E. Ambulatory assessment in psychopathology research: current achievements and future ambitions. Curr Opin Psychol. 2021;41:1–8. doi:10.1016/j.copsyc.2021.01.004
6. May M, Junghaenel DU, Ono M, Stone AA, Schneider S. Ecological momentary assessment methodology in chronic pain research: a systematic review. J Pain. 2018;19(7):699–716. doi:10.1016/j.jpain.2018.01.006
7. Reichert M, Giurgiu M, Koch E, et al. Ambulatory assessment for physical activity research: state of the science, best practices and future directions. Psychol Sport Exerc. 2020;50:1.
8. Banzett RB, Pedersen SH, Schwartzstein RM, Lansing RW. The affective dimension of laboratory dyspnea: air hunger is more unpleasant than work/effort. Am J Respir Crit Care Med. 2008;177(12):1384–1390. doi:10.1164/rccm.200711-1675OC
9. Meek PM, Banzett R, Parsall MB, Gracely RH, Schwartzstein RM, Lansing R. Reliability and validity of the multidimensional dyspnea profile. Chest. 2012;141(6):1546–1553. doi:10.1378/chest.11-1087
10. Gift AG. Validation of a vertical visual analogue scale as a measure of clinical dyspnea. Rehabil Nurs. 1989;14(6):323–325. doi:10.1002/j.2048-7940.1989.tb01129.x
11. Yorke J, Moosavi SH, Shuldham C, Jones PW. Quantification of dyspnoea using descriptors: development and initial testing of the Dyspnoea-12. Thorax. 2010;65(1):21–26. doi:10.1136/thx.2009.118521
12. Yorke J, Russell AM, Swigris J, et al. Assessment of dyspnea in asthma: validation of the dyspnea-12. J Asthma. 2011;48(6):602–608. doi:10.3109/02770903.2011.585412
13. Van den Bergh O, Walentynowicz M. Accuracy and bias in retrospective symptom reporting. Curr Opin Psychiatry. 2016;29(5):302–308. doi:10.1097/YCO.0000000000000267
14. Walentynowicz M, Bogaerts K, Van Diest I, Raes F, Van den Bergh O. Was it so bad? The role of retrospective memory in symptom reporting. Health Psychol. 2015;34(12):1166–1174. doi:10.1037/hea0000222
15. Fletcher CM (Chairman). Standardised questionnaire on respiratory symptoms: a statement prepared and approved by the MRC Committee on the Aetiology of Chronic Bronchitis (MRC breathlessness score). Br Med J. 1960;2(5213):1665.
16. Borg GA. Psychophysical bases of perceived exertion. Med Sci Sports Exerc. 1982;14(5):377–381. doi:10.1249/00005768-198205000-00012
17. Subratty AH, Manraj M, Baligadoo S. A new visual analogue scale for assessment of dyspnoea in congestive heart failure. Int J Clin Pharmacol Ther. 1994;32(5):259–261.
18. Mahler DA, Weinberg DH, Wells CK, Feinstein AR. The measurement of dyspnea. Contents, interobserver agreement, and physiologic correlates of two new clinical indexes. Chest. 1984;85(6):751–758. doi:10.1378/chest.85.6.751
19. Guyatt GH, Berman LB, Townsend M, Pugsley SO, Chambers LW. A measure of quality of life for clinical trials in chronic lung disease. Thorax. 1987;42(10):773–778. doi:10.1136/thx.42.10.773
20. Jones PW, Harding G, Berry P, Wiklund I, Chen WH, Kline Leidy N. Development and first validation of the COPD assessment test. Eur Respir J. 2009;34(3):648–654. doi:10.1183/09031936.00102509
21. Kalluri, M., Cui, Y., Wang, T., & Bakal, J. A. Validation of a Novel Clinical Dyspnea Scale - A Retrospective Pilot Study. Am Journal Hospice Palliat Care. 2024;41(3), 253–261.
22. Jones P.W, Quirk, F.H, Baveystock, C.M. The St George’s Respiratory Questionnaire. Respiratory medicine. 1991;85(2532):1 doi:10.1016/s0954-6111(06)80166-6.
23. Banzett RB, O’Donnell CR, Guilfoyle TE, et al. Multidimensional dyspnea profile: an instrument for clinical and laboratory research. Eur Respir J. 2015;45(6):1681–1691. doi:10.1183/09031936.00038914
24. Hodgev V, Kostianev S, Marinov B. University of Cincinnati Dyspnea questionnaire for evaluation of dyspnoea during physical and speech activities in patients with chronic obstructive pulmonary disease: a validation analysis. Clin Physiol Funct Imaging. 2003;23(5):269–274. doi:10.1046/j.1475-097X.2003.00506.x
25. ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories and others. ATS statement: guidelines for the six-minute walk test. Am J Respir Crit Care Med. 2002;166(1):111–117. doi:10.1164/ajrccm.166.1.at1102
26. Leidy NK, Wilcox TK, Jones PW, Roberts L, Powers JH, Sethi S. Standardizing measurement of chronic obstructive pulmonary disease exacerbations. Reliability and validity of a patient-reported diary. Am J Respir Crit Care Med. 2011;183(3):323–329. doi:10.1164/rccm.201005-0762OC
27. Garcia-Aymerich J, Puhan MA, Corriol-Rohou S, et al. Validity and responsiveness of the Daily- and Clinical visit-PROactive Physical Activity in COPD (D-PPAC and C-PPAC) instruments. Thorax. 2021;76(3):228–238. doi:10.1136/thoraxjnl-2020-214554
28. Yorke J, Swigris J, Russell AM, et al. Dyspnea-12 is a valid and reliable measure of breathlessness in patients with interstitial lung disease. Chest. 2011;139(1):159–164. doi:10.1378/chest.10-0693
29. Mahler DA, Wells CK. Evaluation of clinical methods for rating dyspnea. Chest. 1988;93(3):580–586. doi:10.1378/chest.93.3.580
30. Meek PM, Lareau SC, Anderson D. Memory for symptoms in COPD patients: how accurate are their reports? Eur Respir J. 2001;18(3):474–481. doi:10.1183/09031936.01.00083501
31. Sandberg J, Sundh J, Anderberg P, et al. Comparing recalled versus experienced symptoms of breathlessness ratings: an ecological assessment study using mobile phone technology. Respirology. 2022;27(10):874–881. doi:10.1111/resp.14313
32. Greenlund KJ, Liu Y, Deokar AJ, Wheaton AG, Croft JB. Association of chronic obstructive pulmonary disease with increased confusion or memory loss and functional limitations among adults in 21 states, 2011 behavioral risk factor surveillance system. Prev Chronic Dis. 2016;13:E02. doi:10.5888/pcd13.150428
33. Clarke SY, Williams MT, Johnston KN, Lee AL. The prevalence and assessment of pain and dyspnoea in acute exacerbations of COPD: a systematic review. Chron Respir Dis. 2022;19:14799731221105518. doi:10.1177/14799731221105518
34. Miller S, Teufel R, Nichols M, et al. Feasibility of RESP-FIT: technology-enhanced self-management intervention for adults with COPD. Int J Chron Obstruct Pulmon Dis. 2021;16:3263–3273. doi:10.2147/COPD.S326675
35. Nichols M, Miller S, Treiber F, Ruggiero K, Dawley E, Teufel Ii R. Patient and parent perspectives on improving pediatric asthma self-management through a mobile health intervention: pilot study. JMIR Form Res. 2020;4(7):e15295. doi:10.2196/15295
36. Nichols M, Teufel R, Miller S, et al. Managing asthma and obesity related symptoms (MATADORS): an mhealth intervention to facilitate symptom self-management among youth. Int J Environ Res Public Health. 2020;17(21):7750. doi:10.3390/ijerph17217750
37. Ii RJ T, Patel SK, Shuler AB, et al. Smartphones for real-time assessment of adherence behavior and symptom exacerbation for high-risk youth with asthma: pilot study. JMIR Pediatr Parent. 2018;1(2): doi:10.2196/pediatrics.9796
38. de Vries LP, Baselmans BML, Bartels M. Smartphone-based ecological momentary assessment of well-being: a systematic review and recommendations for future studies. J Happiness Stud. 2021;22(5):2361–2408. doi:10.1007/s10902-020-00324-7
39. Hedeker D, Mermelstein RJ, Demirtas H. Modeling between-subject and within-subject variances in ecological momentary assessment data using mixed-effects location scale models. Stat Med. 2012;31(27):3328–3336. doi:10.1002/sim.5338
40. Whitehead L, Seaton P. The effectiveness of self-management mobile phone and tablet apps in long-term condition management: a systematic review. J Med Internet Res. 2016;18(5):e97. doi:10.2196/jmir.4883
41. Kulich K, Keininger DL, Tiplady B, Banerji D. Symptoms and impact of COPD assessed by an electronic diary in patients with moderate-to-severe COPD: psychometric results from the SHINE study. Int J Chron Obstruct Pulmon Dis. 2015;10:79–94. doi:10.2147/COPD.S73092
42. Miller S, Teufel R, Silverman E. Real-time symptom monitoring of dyspnea via ecological momentary assessment. Eur Respir J. 2018;52:1 doi:10.1183/13993003.congress-2018.PA1513.
43. Miller S, Layne D, Nichols M, et al. Symptom assessment in the home environment using a technology-enhanced self-management intervention in adults with COPD and dyspnea in: b18. Symp Commun Among Patient Fam. 2022;2022:A2385 doi:10.1164/ajrccm-conference.2022.205.1_MeetingAbstracts.A2385.
44. Davies A, Mueller J, Hennings J, Caress AL, Jay C. Recommendations for developing support tools with people suffering from chronic obstructive pulmonary disease: co-design and pilot testing of a mobile health prototype. JMIR Hum Factors. 2020;7(2):e16289. doi:10.2196/16289
45. Davies H, Chappell M, Wang Y, et al. myCOPD app for managing chronic obstructive pulmonary disease: a nice medical technology guidance for a digital health technology. Appl Health Econ Health Policy. 2023;21(5):689–700. doi:10.1007/s40258-023-00811-x
46. Ekström M, Johnson MJ, Huang C, Currow DC. Minimal clinically important differences in average, best, worst and current intensity and unpleasantness of chronic breathlessness. Eur Respir J. 2020;56(2):1902202. doi:10.1183/13993003.02202-2019
47. Bestall JC, Paul EA, Garrod R, Garnham R, Jones PW, Wedzicha JA. Usefulness of the medical research council (MRC) dyspnoea scale as a measure of disability in patients with chronic obstructive pulmonary disease. Thorax. 1999;54(7):581–586. doi:10.1136/thx.54.7.581
48. Sunjaya A, Poulos L, Reddel H, Jenkins C. Qualitative validation of the modified Medical Research Council (mMRC) dyspnoea scale as a patient-reported measure of breathlessness severity. Respir Med. 2022;203:106984. doi:10.1016/j.rmed.2022.106984
49. DeMeo DL, Ramagopalan S, Kavati A, et al. Women manifest more severe COPD symptoms across the life course. Int J Chron Obstruct Pulmon Dis. 2018;13:3021–3029. doi:10.2147/COPD.S160270
50. Miller S, Schooley B, Hikmet N, et al. Evaluation of remote patient monitoring app for spirometry patients. Respiratory Care. 2021;66(Suppl 10):1.
51. Rist C, Karlsson N, Necander S, Da Silva CA. Physical activity end-points in trials of chronic respiratory diseases: summary of evidence. ERJ Open Res. 2022;8(1):00541–2021. doi:10.1183/23120541.00541-2021
52. North M, Bourne S, Green B, et al. A randomised controlled feasibility trial of E-health application supported care vs usual care after exacerbation of COPD: the RESCUE trial. NPJ Digit Med. 2020;3(1):145. doi:10.1038/s41746-020-00347-7
53. Chmiel FP, Burns DK, Pickering JB, Blythin A, Wilkinson TM, Boniface MJ. Prediction of Chronic Obstructive Pulmonary Disease Exacerbation Events by Using Patient Self-reported Data in a Digital Health App: statistical Evaluation and Machine Learning Approach. JMIR Med Inform. 2022;10(3):e26499. doi:10.2196/26499
54. Stoddart A, van der Pol M, Pinnock H, et al. Telemonitoring for chronic obstructive pulmonary disease: a cost and cost-utility analysis of a randomised controlled trial. J Telemed Telecare. 2015;21(2):108–118. doi:10.1177/1357633X14566574
55. Henderson C, Knapp M, Fernández JL, et al. Cost effectiveness of telehealth for patients with long term conditions (whole systems demonstrator telehealth questionnaire study): nested economic evaluation in a pragmatic, cluster randomised controlled trial. BMJ. 2013;346:f1035.
56. Oleson JJ, Jones MA, Jorgensen EJ, Wu YH. Statistical considerations for analyzing ecological momentary assessment data. J Speech Lang Hear Res. 2022;65(1):344–360. doi:10.1044/2021_JSLHR-21-00081
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Analyzing the Effectiveness of mHealth to Manage Diabetes Mellitus Among Adults Over 50: A Systematic Literature Review
Kruse CS, Mileski M, Heinemann K, Huynh H, Leafblad A, Moreno E
Journal of Multidisciplinary Healthcare 2023, 16:101-117
Published Date: 12 January 2023
Leveraging mHealth for the Treatment and Management of PLHIV
Kruse CS, Pacheco GJ, Rosenthal N, Kopp CJ, Omorotionmwan O, Cruz JE
Risk Management and Healthcare Policy 2023, 16:677-697
Published Date: 12 April 2023
Automated Oxygen Administration Alleviates Dyspnea in Patients Admitted with Acute Exacerbation of COPD: A Randomized Controlled Trial
Sandau C, Hansen EF, Ringbæk TJ, Kallemose T, Bove DG, Poulsen I, Nørholm V, Pedersen L, Jensen JUS, Ulrik CS
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:599-614
Published Date: 18 April 2023
Lack of Clinical Control in COPD Patients Depending on the Target and the Therapeutic Option
Soler-Cataluña JJ, Huerta A, Almagro P, González-Segura D, Cosío BG
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:1367-1376
Published Date: 6 July 2023
Effects of Adherence to an mHealth Tool for Self-Management of COPD Exacerbations
Bischoff EW, Ariens N, Boer L, Vercoulen J, Akkermans RP, van den Bemt L, Schermer TR
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:2381-2389
Published Date: 1 November 2023