Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 18
Lack of Clinical Control in COPD Patients Depending on the Target and the Therapeutic Option
Authors Soler-Cataluña JJ ![]() , Huerta A
, Huerta A ![]() , Almagro P
, Almagro P ![]() , González-Segura D
, González-Segura D ![]() , Cosío BG
, Cosío BG ![]()
Received 3 April 2023
Accepted for publication 28 June 2023
Published 6 July 2023 Volume 2023:18 Pages 1367—1376
DOI https://doi.org/10.2147/COPD.S414910
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jill Ohar
Juan José Soler-Cataluña,1,2 Arturo Huerta,3 Pere Almagro,4 Diego González-Segura,5 Borja G Cosío6 On behalf of the CLAVE Study Investigators
1Department of Pneumology, Hospital Arnau de Vilanova-Lliria, Valencia, Spain; 2Medicine Department, València University and CIBERES, Valencia, Spain; 3Pulmonary and Critical Care Division, Clínica Sagrada Família, Barcelona, Spain; 4Internal Medicine Department, Mutua Terrassa University Hospital, Terrassa, Spain; 5Medical Advisor, Chiesi SAU, Barcelona, Spain; 6Department of Pneumology, H. Universitari Son Espases Hospital-IdISBa and CIBERES, Palma de Mallorca, Spain
Correspondence: Juan José Soler-Cataluña, Department of Pneumology Arnau de Vilanova-Lliria, C/San Clemente 12, Valencia, 46015, Spain, Email [email protected]
Introduction: According to the Global Initiative for chronic obstructive lung disease (GOLD), when a treatment is not achieving an appropriate response it should be switched taking into account the predominant treatable trait to target (dyspnea or exacerbations). The objective of the present study was to investigate the lack of clinical control according to the target and medication groups.
Materials and Methods: This was a post-hoc analysis of the CLAVE study, an observational, cross-sectional, multicenter study which evaluated the clinical control, and related-factors, in a cohort of 4801 patients with severe chronic obstructive pulmonary disease (COPD). The primary endpoint was the percentage of uncontrolled patients defined as COPD Assessment Test (CAT) > 16 or presence of exacerbations in the last 3 months despite receiving long-acting beta2-agonist (LABA) and/or long-acting antimuscarinic antagonist (LAMA) with or without inhaled corticosteroids (ICS). Secondary objectives included the description of sociodemographic and clinical characteristics of patients by therapeutic group and the identification of characteristics potentially associated with the lack of control of COPD including low adherence measured by the test to adherence to inhalers (TAI).
Results: In the dyspnea pathway, lack of clinical control was of 25.0% of patients receiving LABA or LAMA in monotherapy, 29.5% by those with LABA + LAMA, 38.3% with LABA + ICS and 37.0% with triple therapy (LABA + LAMA + ICS). In the exacerbation pathway, percentages were 87.1%, 76.7%, 83.3%, and 84.1%, respectively. Low physical activity and high Charlson comorbidity index were independent factor of non-control in all therapeutic groups. Additional factors were lower post-bronchodilator FEV1 and poor adherence to inhalers.
Conclusion: There are still room for improvement in COPD control. From the pharmacological perspective, every step in treatment have a pool of uncontrolled patients in which a step-up could be considered according to a trait to target strategy.
Keywords: COPD, control, target, dyspnea, comorbidities, treatment
Introduction
Chronic obstructive pulmonary disease (COPD) is a complex and very heterogeneous disorder that presents with differential characteristics and severity.1,2 Primary goals for the management of COPD are to reduce the symptoms and prevent the exacerbations.3 Despite the efficacy of pharmacological and non-pharmacological strategies,4 a number of COPD patients experience them frequently.5 According to the Global Initiative for chronic obstructive lung disease (GOLD), an initial treatment should be maintained when achieving an appropriate response.3 Nevertheless, when not, GOLD suggests considering the predominant treatable trait to target (dyspnea or exacerbations), where the exacerbation pathway actually corresponds to the target of both dyspnea and exacerbations. Their pharmacological algorithm involves mainly 4 therapeutic options: long-acting beta2-agonist (LABA) or long-acting antimuscarinic antagonist (LAMA) in monotherapy; the combination of LABA and LAMA (LABA + LAMA); the combination of LABA and inhaled corticosteroid (ICS, LABA + ICS); and triple therapy (LABA + LAMA + ICS). Escalation or de-escalation of medications should be based on their efficacy and safety; however, the decision finally yields on healthcare provider’s perception.6 The concept of clinical control has been introduced in COPD for determining the current clinical status of the patients, and thus to improve the management of their disease.7,8 In Spain, the observational, cross-sectional, multicenter CLAVE study (`Estudio observacional transversal para Caracterizar La EPOC grAVe en España´; Severe COPD categorization in Spain) evaluated the clinical control, and related-factors, in a cohort of 4801 patients with severe COPD.9 Authors demonstrated that less than one-third of the patients receiving maintenance therapy could be considered as having the disease controlled. Available studies on the clinical control in severe COPD patients are indeed limited.6,10–12 The primary objective of the present study was to investigate the lack of clinical control according to the predominant treatable trait to target and medication groups.
Materials and Methods
Study Design
This is a post-hoc analysis of data obtained in the CLAVE study.9 Briefly, patients were males and females aged ≥40 years, active smokers or ex-smokers with a smoking history of ≥10 pack-year, who had diagnosis of COPD; post-bronchodilator forced expiratory volume in 1 second (FEV1) <50% of predicted; and were receiving a maintenance treatment. Exacerbated patients, who received oral corticosteroids or antibiotics, due to a COPD exacerbation, were not included in the study. Procedures were approved by the Research Ethics Committee of the Hospital Clinic of Barcelona (Spain) and were in accordance with the Declaration of Helsinki.
Endpoints and Variables
In the present post-hoc study, patients from CLAVE study receiving a specified inhaled therapy were included in the analysis. The primary endpoint included the percentage of uncontrolled patients receiving the main therapeutic options, and considering the target. For such aim, patients were initially classified according to the predominant treatable trait to target (dyspnea or exacerbation), following the GOLD’s pharmacological treatment algorithm. Only patients showing no exacerbations in the last 12 months were included in the dyspnea pathway; whereas the exacerbation group included patients with exacerbations in the last 12 months. An uncontrolled patient had to show a value for the Spanish version of the COPD assessment test (CATTM) >16, for the dyspnea pathway; whereas a CATTM >16 together with exacerbations in the last 3 months, for the exacerbation pathway.9 The CATTM is an 8-item questionnaire that evaluates the impact of COPD on health status; where items are scored between 0 (no limitation) and 5 (very limited).13 Secondary objectives included the description of sociodemographic and clinical characteristics in patients depending on the therapeutic group, ie LABA or LAMA in monotherapy, LABA + LAMA, LABA + ICS, and triple therapy. A last secondary objective was to identify the characteristics in patients potentially associated with the lack of control of COPD for each therapeutic group. Factors initially evaluated in the univariate analysis were: post-bronchodilator FEV1 (as percentage of predicted; mean value and categorized as <30% and ≥30%), age group (<70 and ≥70 years), place of residence (rural, semi-urban, and urban), smoking status (active smoker and ex-smoker; pack-year of smoking), physical activity (determined with the International Physical Activity Questionnaire; categorized as high, moderate, and low/inactive),14 hospital level of care (primary care and specialist), adherence to inhalers (using the adherence to inhalers questionnaire; categorized as good, intermediate, and poor),15 and Charlson comorbidity index (mean value and categorized as ≥2 and 1).16
Statistical Analyses
Qualitative variables were expressed as absolute and relative frequencies (%), whereas quantitative ones as the mean and standard deviation (SD). A backward binary logistic regression was carried out to identify patient’s features potentially associated with lack of control (Odds ratio, OR; 95% confidence interval, 95% CI). In the univariate analysis, factors showing a significance <0.1 were included in the multivariate analysis. Statistical significance was set when P <0.05. Statistical analyses were performed with SAS version 9.4.
Results
A total of 4778 patients received a specified inhaled therapy in CLAVE study. Of them, 957 patients (dyspnea pathway) showed no exacerbations in the last 12 months [636 (66.5%) being considered as controlled patients, and 321 (33.5%) as uncontrolled ones]. By contrast, 3821 patients (exacerbation pathway) did show exacerbations in the last 12 months. Of these patients, 684 (17.9%) and 3137 (82.1%) are considered as controlled and uncontrolled patients, respectively.
Clinical Control of COPD According to Different Treatment Groups
The distribution of controlled and uncontrolled patients considering the target and the treatment option is shown in Figure 1. Approximately 1% and 2% of patients were not classified in the respective dyspnea and exacerbation pathways, because having a different medication pattern. These percentages represent patients either with other monotherapies other than LABA/LAMA, with other double combinations other than LABA/LAMA or LABA/ICS or with only rescue medication, which were not included in the large groups that were studied. In the dyspnea pathway, non-clinical control was reported in 25.0% of patients receiving monotherapy, 29.5% by those with LABA + LAMA, 38.3% with LABA + ICS, and 37.0% with triple therapy. In the exacerbation pathway, percentages were 87.1%, 76.7%, 83.3%, and 84.1%, respectively.
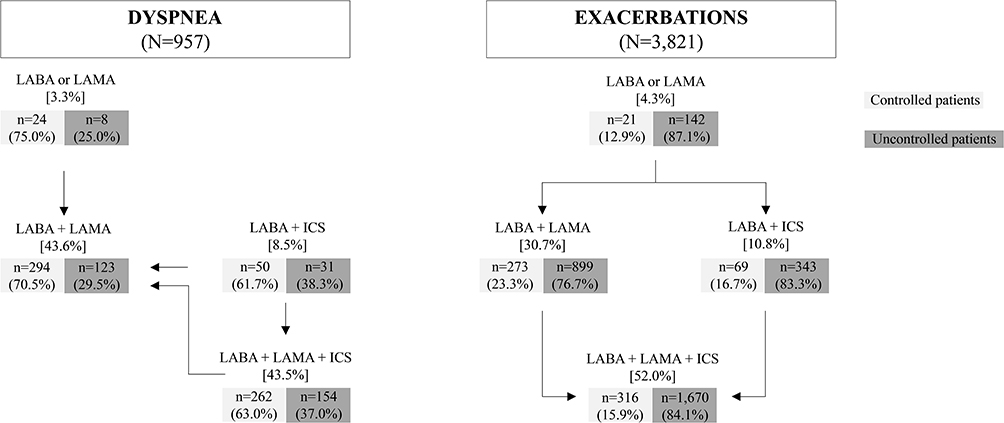 |
Figure 1 Distribution of controlled and uncontrolled patients considering the predominant treatable target and the therapeutic option (GOLD’s follow-up pharmacological treatment algorithm). Percentages in brackets represent the frequency of each treatment option in each respective pathway, whereas those in parentheses are the frequency of control and non-control for each treatment option. Approximately 1% and 2% of patients were not classified in the respective dyspnea and exacerbation pathways because having a different medication pattern. |
Characteristics of Controlled and Uncontrolled Patients
Sociodemographic and clinical characteristics of controlled and uncontrolled patients considering their therapeutic option are shown in Table 1. The mean age of all patients was 69 years (SD, 9 years). The mean age was slightly higher in uncontrolled patients than controlled ones, in all medication groups. The mean post-bronchodilator FEV1 was 39.1% of predicted (SD, 8.3%), slightly higher in controlled patients, compared with uncontrolled ones. The mean mMRC grade of dyspnea was 2.1 (SD, 1.0). The mean Charlson comorbidity index was 2.2 (SD, 1.5). Uncontrolled patients showed a higher dyspnea mean value and Charlson comorbidity index than controlled ones in all therapeutic options.
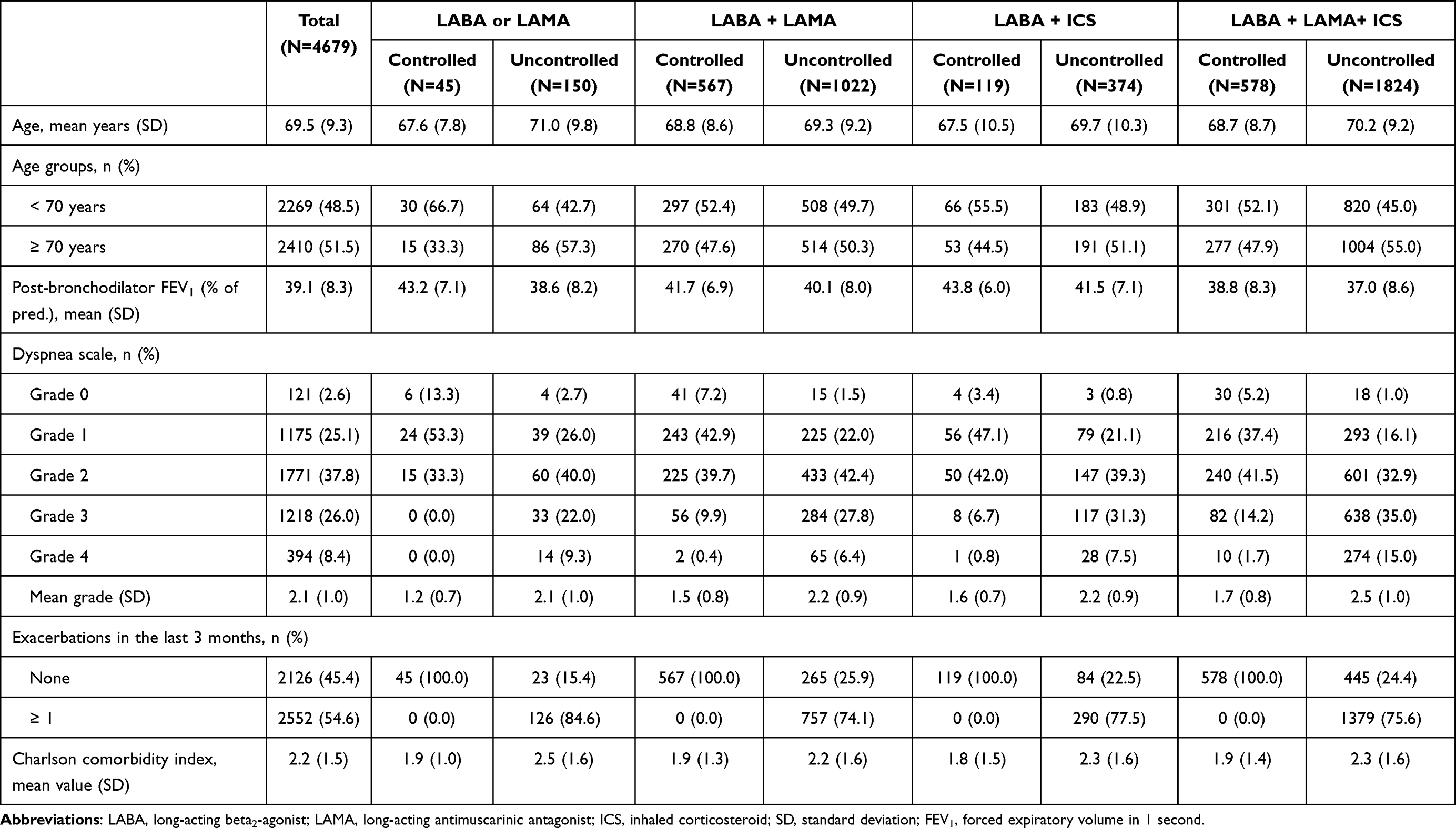 |
Table 1 Sociodemographic and Clinical Characteristics of Controlled and Uncontrolled Patients Considering Their Therapeutic Option |
Factors Associated with Lack of Clinical Control
Factors independently associated with non-control of COPD and considering the therapeutic option is shown in Table 2. Physical activity (low/inactive versus high and moderate versus high) and Charlson comorbidity index (≥2 versus 1) were independent factors of lack of control in all medication groups. Low or inactive physical activity showed higher risk of uncontrolled [OR: 8.1 (95% CI, 2.4–28.0)] than high physical activity in patients with monotherapy, OR: 4.1 (95% CI, 3.0–5.8) with LABA + LAMA, OR:1.8 (95% CI, 0.9–3.6) with LABA + ICS, and OR: 3.7 (95% CI, 2.8–4.9) with triple therapy. For Charlson comorbidity index (≥2 versus 1), ORs were: 1.5 (95% CI, 1.0–2.1), 1.5 (95% CI, 1.2–1.9), 2.2 (95% CI, 1.3–3.5), and 1.2 (95% CI, 1.0–1.5), respectively. Additional factors were post-bronchodilator FEV1 (<30% versus ≥30%), and adherence to inhalers (poor versus good) in the monotherapy group, LABA + LAMA, and triple therapy.
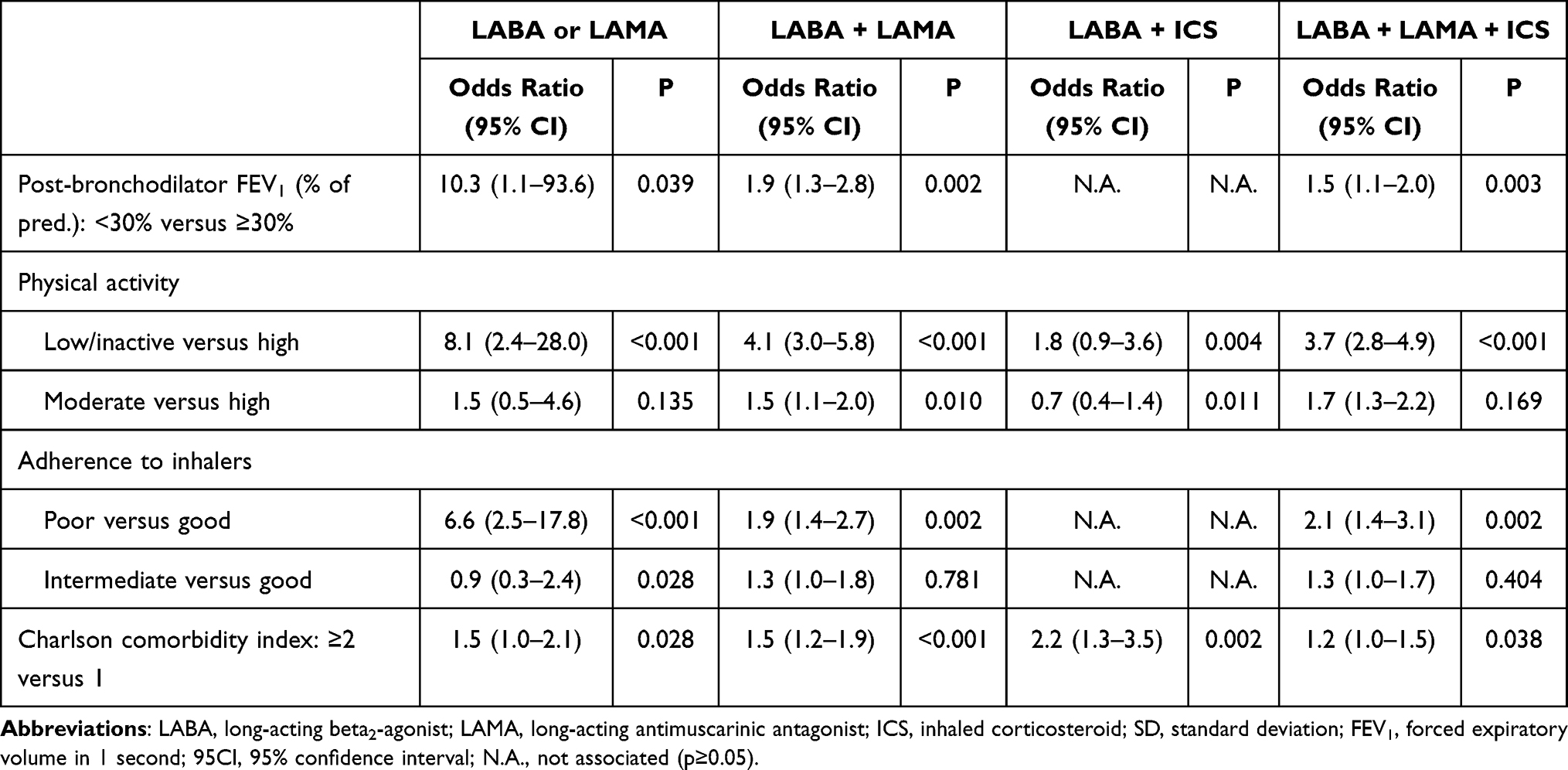 |
Table 2 Factors Independently Associated with Lack of Control of COPD Considering the Therapeutic Option |
Discussion
Clinical control in COPD is assessed to determine the clinical status of patients and optimize their treatments.6 A patient may be considered controlledif, during follow-up, show minimal or no symptoms, no acute exacerbations have occurred since the last follow-up visit, and no impairment in quality of life has been seen while receiving the current treatment.17
CATTM is a one of the most important tools used on GOLD strategy, able to determine how the disease impacts on the life of the patient.3,12 The present study aimed at complementing the information from the GOLD’s therapeutic algorithm by providing the frequency of uncontrolled patients for each therapy option, the sociodemographic and clinical profile of the patient that frequently requires each option, and the features potentially associated with non-control.
To our knowledge, this is the first study evaluating the lack of clinical control considering the target and the therapeutic option. Our study included patients from the CLAVE study,9 which involved those with severe disease. Most of them (416 in the dyspnea and 1986 in the exacerbation pathway) were receiving triple therapy. The frequency of control in the dyspnea pathway (assessed with CATTM) was higher than the non-control in all medication groups; in contrast to found in the exacerbation pathway (assessed with CATTM and exacerbations in the last 3 months), where non-control was more prevalent than control.
GOLD guidelines provide recommendations to uncontrolled patients depending on the pathway.3 In the dyspnea pathway, the combination of LABA + LAMA is recommended for patients with persistent breathlessness or exercise limitation receiving a LABA or LAMA in monotherapy. For uncontrolled patients taking LABA + ICS, the escalation to triple therapy can be considered or, if ICS was inadequate, to LABA + LAMA. Other causes of dyspnea, the inhaler technique, physical activity and the adherence should also be investigated.3 In the exacerbation pathway, the escalation to LABA + LAMA or LABA + ICS is recommended in patients with persistent exacerbations receiving monotherapy. With recurrent exacerbations on LABA + LAMA, and depending on blood eosinophils, the recommendation is to escalate to triple therapy (if eosinophils ≥100 cells/µL) or to add roflumilast or azithromycin (if <100 cells/µL). Similarly, triple therapy is recommended in patients with further exacerbation on LABA + ICS or, if inadequate response to ICS, to LABA + LAMA. Finally, an uncontrolled patient receiving triple therapy may consider one of the three following options: add roflumilast, macrolide, or stopping ICS.3 Using this step-up approach, we hope to get better control results. However, the medication was positively correlated with the number of uncontrolled patients, which might be probably explained by the severity bias from the observational nature of the study, since those patients with a more severe condition (lower FEV1, higher dyspnea score) used a more intensive treatment (triple therapy).
On the other hand, in our study, factors associated with non-control of COPD were in agreement with those proven to participate in disease severity, ie declined pulmonary function, low levels of physical activity (or inactivity), poor adherence to inhalers, and higher presence of comorbidities.18–22 Indeed, both physical activity level and Charlson comorbidity index were significant factors of non-control presented in all medication groups. Low physical activity levels have been associated with a greater lung function impairment, incidence of comorbidities (such as cardiovascular diseases, diabetes, hypertension, depression), and thus with a higher risk for all-cause mortality.20,21 In our study, the probability of non-control was up to 8.1 times higher in patients with low/intermediate activity level receiving LABA or LAMA in monotherapy, compared with those with high physical activity level. Comorbidities are frequent in COPD patients.18 They complicate the therapeutic approaches and contribute greatly to poor health outcomes.23 In our cohort of patients, when evaluating comorbidities as a continuous variable (Charlson comorbidity index ≥2 versus 1), the risk for COPD non-control was up to 2.2 times higher in patients receiving LABA + ICS. Bronchodilators represent the keystone in the COPD control, as they improve pulmonary function and reduce symptoms and exacerbations.24 However, the adherence to medications is especially poor, with non-adherence rates of 50–80%.25,26 The non-adherence of bronchodilators has been correlated with greater risk for morbimortality, higher number of hospitalizations, and impaired quality of life.19 In our study, patients receiving LABA or LAMA in monotherapy with poor adherence to the medication had 6.6 times higher probability of non-control than those with good adherence. Finally, airway obstruction (determined by FEV1) has been associated with disease progression and is indicative of poor clinical control.22 In our study, a patient receiving LABA or LAMA in monotherapy with FEV1 <30% of predicted had 10.3 times higher likelihood of non-control than those with FEV1 ≥30%. It is interesting to note that active smoking was not among factors associated with non-control, since it is one of the most important factors impacting on the natural history of the disease.27 The main limitation of the present study is its post-hoc design, not specifically designed to fulfil primary and secondary endpoints. Nevertheless, it has an exploratory nature (the correlation between therapeutic options, clinical control, and patient characteristics). Observations must be subsequently checked in further, properly designed, prospective clinical trials with large cohort of patients.
Conclusions
In conclusion, regarding the management of the disease, there are still room for improvement in the COPD control. From the pharmacological perspective, every step in treatment have a pool of uncontrolled patients in which a step-up could be considered according to the GOLD’s follow-up pharmacological treatment algorithm.
Abbreviations
COPD, Chronic obstructive pulmonary disease; GOLD, Global Initiative for chronic obstructive lung disease; CI, confidence interval; CATTM, COPD assessment test; ICS, inhaled corticosteroid; LABA, long-acting beta2-agonist; LAMA, long-acting antimuscarinic antagonist; SD, standard deviation; FEV1, forced expiratory volume in the first second.
*Participating Investigators
Abel Pallarés Sanmartín, Abel Rodríguez Canal, Abelardo Montero Saez, Ada Luz Andreu Rodriguez, Adelaida Acuña Fernandez, Africa Alcorta Mesas, Agustín Valido Morales, Ainhoa Gomez, Aizea Mardones, Alba Calderón Pecellín, Alberto Díaz De Santiago, Alberto Herrejón Silvestre, Alberto Javier Nistal Rodriguez, Alberto Levy Naon, Alberto Saura Vinuesa, Alejandra Marin Arguedas, Alejandro Veres Racamonde, Alfonso Garcia Guisado, Alfredo Candela Blanes, Alicia Pérez Rodríguez, Alicia Ruiz Martín, Alvaro Flamarique Pascual, Alvaro Perez Gomez, Amaia Atenea Iridoy Zulet, Amaia Urrutia Gajate, Amparo Lloris Bayo, Amparo Romero Plaza, Ana Boldova Loscertales, Ana Botella Gregori, Ana Bustamante Ruiz, Ana Cobas Paz, Ana Fortuna Gutierrez, Ana García Peña, Ana Isabel Enríquez Rodríguez, Ana Kersul, Ana Maria Pueyo Bastida, Ana María Rodríguez Fernández, Ana Martín Medina, Ana Paramá Fontenla, Ana Paulina Gómez-Bastero, Ana Raño, Andres Rodero, Andrés Vilas Iglesias, Angel Blanco, Anibal Manuel Hernandez Gil, Anna Soler Sendra, Annie Navarro Rolon, Antoni Riba Blanch, Antonia Fuster Gomila, Antonia Mayol Mateu, Antonia Soto Venegas, Antonio Albaladejo Dávalos, Antonio Clavo, Antonio Drusetta Llahues, Antonio Eduardo Delgado Martín, Antonio Fernández Rodríguez, Antonio Jose Madueño Caro, Antonio Manuel Pérez Pernández, Antonio Muiño Miguez, Antonio Pereira Vega, Antonio Ruiz Peña, Antonio Sancho Muñoz, Araceli Abad Fernández, Araceli Fernandez Revuelta, Armando González López, Armando Larnia Sanchez, Arturo Huerta, Astrid Crespo Lessmann, Aurelio Arnedillo Muñoz, Ayman Soudan Barakat, Bartolome Poyato Gonzalez, Beatriz Abascal Bolado, Beatriz Arias Arcos, Beatriz Morales Chacón, Begoña Fernandez Infante, Begoña Ponce Buj, Belen Lopez-Muñiz, Belen Navas Bueno, Belen Orosa Bertol, Berta Avilés Huertas, Blanca Hortal Reina, Blas Rojo Moreno-Arrones, Borja Garcia-Cosio Piqueras, Carlos Alberto Názara Otero, Carlos Disdier, Carlos Javier Carpio, Carlos José Álvarez Martínez, Carlos Leon Rodriguez, Carlos Martinez Rivera, Carlos Peñalver Mellado, Carlos Soler Portmann, Carlos Vilariño Pombo, Carme Agusti, Carmen Abeledo, Carmen Angela Centeno Clemente, Carmen Elena Calvo Rodriguez, Carmen Montero Martinez, Carmen Soria Esojo, Carmen Soto Fernandez, Carolina Puchaes Manchon, Carracedo Sevillano Martín, Catalina Balaguer Balaguer, Celia Lacarcel Bautista, César Aurelio Gutiérrez Rivera, Christian Anchorena Diaz, Christian Garcia Fadul, Christian Teijo Núñez, Chunshao Hu Yang, Concepcion Cañete Ramos, Concepción Hernández García, Coral Gonzalez Fernandez, Cristian Avon Gomez, Cristina Benito Bernáldez, Cristina Miralles Saavedra, Cristina Navarro Soriano, Cristina Represas Represas, Cristina Solé Felip, Cristobal Esteban, Damián Malia Alvarado, Daniel Mejías Hidalgo, Daniel Rey Aldana, Daniel-Ross Monserrate Mitchell, Dario Mendez Cabezudo, David Barros Casas, David De La Rosa Carrillo, David Ferrando Garcia, David Iturbe Fernández, David Morchón Simón, David Orts Giménez, Delfin Arzua Mouronte, Demetrio Gonzalez Vergara, Dita Kopecna, Domingo García Aguilar, Eduard Valverde Forcada, Eduardo Arcalá Campillo, Eduardo Marquez, Elena Castro Rodriguez, Elena Molins Millan, Eleuterio Llorca Martínez, Eliana Denise Damonte White, Elisabeth Castillo Diaz, Elsa Naval, Emma Vazquez Espinosa, Emmanuel Coloma Bazán, Enith Yojana Garcia Carrascal, Enric Hernandez Huet, Enrique Cabrerizo Cómitre, Enrique Jesus Alvarez Asensio, Enrique Temes Montes, Erick Monclou Garzón, Esteban Ciruelos Ayuso, Esteban Martin Echevarria, Esther Alonso Sastre, Esther Antón, Esther Arias Alba, Esther Rodriguez González, Eva Belen De Higes Martinez, Eva Cabrera César, Eva Farrero Muñoz, Eva Maria Rosillo Hernandez, Eva Martinez Moragon, Eva Prats, Fco. Javier Ruiz Moruno, Federico Iglesias, Felipe Nicolau Pastrie, Felix Ortiz Portal, Fernando Bonet Madurga, Fernando De Arriba Frade, Fernando Gutierrez Marcos, Fernando Iglesias Rio, Fernando Leon Marrero, Fernando Maria Navarro Ros, Fernando Molina Nieto, Fernando Muñoz Díaz, Fernando Pedraza Serrano, Fernando Sanchez-Toril Lopez, Francesc Puchades, Francisco Astudillo Martin, Francisco Beltrán Baldovi, Francisco Canales Cid, Francisco Casas Maldonado, Francisco De Pablo Cillero, Francisco Espildora Hernández, Francisco Javier Gomez De Terreros Caro, Francisco Javier Gonzalez Barcala, Francisco Linde De Luna, Francisco López García, Francisco Martín Luján, Francisco Ortega Ruiz, Frederic Tatay Soler, Germán Luis Llavador Ros, German Saez Roca, Gonzalo Segrelles Calvo, Graciliano Estrada Trigueros, Gregorio Sanchez Romero, Gustavo De Luiz Martínez, Gustavo Villegas Sanchez, Hemily Katerine Izaguirre Flores, Higinio Vazquez Galdo, Hugo Garcia Ibarra, Hugo Gomez Marquez, Ignacio Garcia-Talavera, Ignacio Javier Pérez De Diego, Ignacio Peñas, Igor Iturbe Susilla, Iker Fernandez-Navamuel, Ingrid Solanes, Inmaculada Salvador Adell, Irene Caselles González, Isaura Parente Lamelas, Ismael Ali Garcia, Ismael Francisco Aomar Millán, Iván Arroyo Fernández, J. Pablo Herrero Jarque, Jaume Joan Ferrer Sancho, Javier Barrio Soto, Javier Elvira Gonzalez, Javier Gallego Borrego, Javier Hueto Pérez De Heredia, Javier Mazo Etxaniz, Javier Morcillo Huertas, Javier Perez Pallares, Jessica Ivana Hilares Vera, Jesus Camino Buey, Jesús Fernandez Frances, Jesus Jimenez Lopez, Jesús Manuel Fernández Villar, Jesús Medina Asensio, Jesús R Hernández Hernández, Jesús Recio Iglesias, Joan Ramon Rozadilla Sacanell, Joan Sola Aznar, Joan Valldeperas, Joaquín Alfonso Megido, Joaquin Cegoñino De Sus, Joel Alejandro Varona Sanchez, Jordi Juanola Pla, Jorge Manuel Romero Requena, Jorge Pascual Bernabeu, Jose Alberto Martos Velasco, Jose Antonio Cascante Rodrigo, José Antonio Castilllo Vizuete, José Antonio Díaz Peromingo, José Antonio Marín Torrado, Jose Arnoldo Grajeda Juarez, Jose Bascuñana Morejon De Giron, Jose Bujalance Zafra, Jose Calvo Bonachera, Jose Carlos Serrano Rebollo, Jose Celdran Gil, Jose Daniel Alcazar Ramirez, José Enrique Gavela García, Jose Francisco Carboneros De La Fuente, José Ignacio De Granda-Orive, José Ignacio Herrero Herrero, José Ignacio Pardo González De Quevedo, José Ignacio Quintana González, Jose Luis Casells Hernandez, José Luis Córcoles Satorre, Jose Luis Delgado Morales, Jose Luis Diez Jarilla, Jose Luis Fernández Sánchez, Jose Luis Gutierrez Alonso, Jose Luis Rojas Box, José Luis Trujillo Castilla, Jose Luis Velasco Garrido, Jose M Marin Trigo, Jose Manuel Garcia Pazos, Jose Manuel Querol Borras, Jose Manuel Vera Aranda, Jose Manuel Villar Freire, Jose Maria Cruz Molina, Jose Martin Clos, Jose Miguel Rodriguez Gonzalez-Moro, José Miguel Seguí Ripoll, Jose Miguel Valero Perez, Jose Ramon Donado Uña, José Ramón Ferrando Gabarda, Jose Vicente Greses Giner, Jose Vicente Puchades Castelló, Jose Vicente Roig Figueroa, Josep Mª Alsina Martí, Juan Manue Diez Piña, Juan Abreu González, Juan Antonio Martinez Carbonell, Juan Antonio Santos Bermejo, Juan B. Bauza Deroulede, Juan Bautista Montagud Moncho, Juan Carlos Tapia Regidor, Juan Francisco De Vega Garcia, Juan Gonzalez Rodriguez, Juan Jose Cruz Rueda, Juan Luengo Alvarez, Juan Luis Rodriguez Hermosa, Juan Manuel Sanchez Apresa, Juan Manuel Verdeguer Miralles, Juan Marco Figueira Gonçalves, Juan Marcos Moreno Mendaña, Juan María Rubio Sánchez, Juan Ortiz De Saracho Bobo, Juan Pablo De Torres Tajes, Juan Pablo Garcia, Julia Garcia De Pedro, Julia Tabara Rodriguez, Julián Andrés Ceballos Gutiérrez, Julio Hernández Vázquez, Justo Grau Delgado, Laura Caballero Ballesteros, Laura Ovejero García, Laura Rodriguez Pons, Laureano Gomez Gonzalez, Leopoldo Damian Dominguez Perez, Leyre Serrano Fernandez, Lourdes Lázaro Asegurado, Lourdes Palomo Alameda, Lucia Diaz Cañaveral, Lucia Gil Maneu, Lucía Zamora Molina, Luis Adolfo Urrelo Cerrón, Luis Alfonso Sota Yoldi, Luis Emilio Planelles Herrero, Luis Fernando Cabañas Enriquez, Luis Fernando Cassini Gómez De Cádiz, Luis García-Giralda Ruiz, Luis Máiz, Luis Manuel Entrenas, Luis Miguel Cuadrado Gomez, Luis Miravet Sorribes, Luis Obradors, Luis Puente Maestu, Luis Rodriguez Pascual, Lyam Lamrini Hamido Laarbi, M Luisa Nieto Cabrera, M. Carmen Gallego Bermejo, Mª Carmen Bermejo Navas, Mª Del Carmen Fernandez Garcia, Mª Lourdes Ramos Casado, Mªcruz Almendros Rivas, Magdalena Serradilla Sánchez, Manuel Arenas Gordillo, Manuel F Ramirez Espinosa, Manuel Jesús Menduiña Guillén, Manuel Jesús Romero Jiménez, Manuel Lorenzo López Reboiro, Manuel Maldonado Escobar, Manuel Martínez Riaza, Manuel Mazabel Flores, Manuel Quirós Valera, Manuel Suárez Tembra, Manuel Tumbeiro Novoa, Manuel Vilà Justribó, Mar Garcia Perez, Marcel Jose Rodriguez Guzman, Mari Carmen Anton Sanz, Maria Belen Marin Martinez, Maria Carme Puy Rión, Maria Carmen Aguar Benito, Maria Carmen Morillo Dominguez, Maria Cruz Gonzalez Villaescusa, Maria De Las Nieves Jimenez Baquero, María Del Carmen García García, Maria Del Carmen Villa Corbaton, Maria Del Mar Bedia Monet, Maria Del Mar Lucena Merino, Maria Del Mar Rodriguez Alvarez, María Del Pilar Martínez Olondris, Maria Del Roser Costa Solà, Maria Dolores Corbacho Abelaira, Maria Dolores Hisado Díaz, Maria E. Barroso Medel, Maria Elia Gómez Merino, Maria Emilia Navascues Martinez, Maria Encarnación Hernández Contreras, Maria Gomez Antunez, María Gómez Peña, María González Gómez, Maria Hernandez Bonaga, Maria Hernández Roca, María Inés Prieto López, Maria Jesus Aviles Ingles, María Jesús Cazorla Martinez, María Jesús Igúzquiza Pellejero, Maria Jesus Linares Asensio, Maria Jesus Mena Rodriguez, María Jesús Moro Alvarez, María José Muñoz Martínez, María José Sánchez Pérez, Maria Luisa Lopez Diaz-Ufano, Maria Martinez Ceres, Maria Milagros Iriberri Pascual, Maria Paz Valiño Lopez, Maria Rafaela Sanchez Perez, María Ruth Herrero Mosquete, Maria Teresa Rodriguez Iglesias, María Torres - Durán, Mariano Rodríguez Porres, Mario Nicolás Albani Pérez, Marta Ballester Canelles, Marta Palop Cervera, Martín Rubianes Gonzalez, Maryam Sidahi Serrano, Maximino González Fernández, Mcarmen Juarez Morales, Mercedes Duffort Falco, Mercedes Palau Benavent, Mercedes Pallero Castillo, Michael Alwakil Olbah, Miguel Angel Ciscar Vilanova, Miguel Angel Franco Campos, Miguel Angel Martin Perez, Miguel Angel Moscardó Orenes, Miguel Angel Racionero Casero, Miguel Angel Rodriguez Rodriguez, Miguel Barrueco Ferrero, Miguel Miller Guerrero, Miguel Roman Rodriguez, Miguel Sanchez Nanclares, Milagros Gonzalez Bejar, Milko Torres De Castro, Mireia Serra Fortuny, Mohamed Kallouchi, Monica Ponce Sanchez, Monica Romero Nieto, Monica Sanchez Garcia, Muriel Sena Gutiérrez, Myriam Calle Rubio, Nagore Blanco Cid, Natividad Quilez Ruiz Rico, Noelia Cubero De Frutos, Noelia Pablos Mateos, Nuria Castejón Pina, Nuria Celorrio Jimenez, Núria Chamorro Tort, Nuria Galofré, Nuria Reina Marfil, Nuria Rodriguez Lázaro, Oscar Bernadich, Pablo Catalán Serra, Pablo Espejo Salamanca, Pablo Rubinstein, Pascual Cortes Miro, Patricia Mata Calderón, Patricia Mínguez Clemente, Patricia Sobradillo Ecenarro, Paula Rodriguez Rodriguez, Pedrito Tomas Tobaruela, Pedro Cancelo Suarez, Pedro J Romero Palacios, Pedro Jose Cordero Rodriguez, Pedro Landete Rodriguez, Pedro Luis Baños Hidalgo, Pedro Penela Penela, Pere Almagro Mena, Pere Serra Mitjà, Pilar Gil Alaña, Pilar Gispert Del Rio, Pilar Iñigo Naranjo, Pilar Marin Martinez, Póvilas Gerardo Dambrava Rodríguez, Rafael Castillo Rubio, Rafael Castrodeza Sanz, Rafael Garcia Carretero, Rafael Lama Martinez, Ramon Boixeda Viu, Ramon Magarolas Jordà, Raquel Dacal Quintas, Raquel García Sevila, Raquel Morillo Guerrero, Raquel Rodriguez Martínez, Raquel Sánchez Juez, Raul Sandoval Contreras, Ricardo Diaz-Casteleiro Romero, Ricardo Ismael Aguilar Perez Grovas, Roberto Bernabeu Mora, Roberto Chalela Rengifo, Roberto Gorgues Comas, Roberto Hurtado Garcia, Roberto Ordóñez Picón, Rocio García García, Rodolfo Álvarez-Sala, Romualdo Roncero Vidal, Rosa Malo De Molina Ruiz, Rosa Maria Folgado De La Fuente, Rosa Maria López Lisbona, Rosa Nieto, Rosario Martinez Barea, Rossana Isabel Baron Lopez, Ruben Lera Alvarez, Salud Santos Pérez, Salvador Alvarez Martin, Salvador Bello Dronda, Salvador Díaz Lobato, Santiago Balmes Estrada, Santiago Carrizo Sierra, Santiago Rubio - Félix, Segismundo Solano Reina, Sergio Alcolea Batres, Sergio Cinza Sanjurjo, Sergio Curi Chercoles, Sergio Fandos Lorente, Sergio Manuel Marti Beltran, Silvia Fernandez Huerga, Silvia Merlos Navarro, Silvia Pérez Fernández, Silvia Sánchez, Sladana Obradovic, Soledad Alonso Viteri, Sonia Martínez Sáez, Susana Filgueira Martínez, Tamara Alonso Pérez, Teresa Peña Migul, Tomas De Vega Santos, Uan Ignacio Ramos Clemente Romero, Vanessa Zorrilla Lorenzo, Vicenta Cresencio Perez, Vicente Quinzá Valero, Victor Gaya Sancho, Victor Manuel Mora Cuesta, Victoria Valeri-Busto Gonzalez, Virginia Almadana Pacheco, Walther Ivan Giron Matute, Xavier Flor, Xavier Pomares Amigó, Xavier Vila Giralte, Xoel Pena Perez, Yadira Dobarganes Sansón, Yoana Lazaro Salazar, Yussef Abu El Wafa and Zully Vasquez Gambasica. All of these authors mentioned collected data.
Data Sharing Statement
Data is available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
Procedures were approved by the Research Ethics Committee of the Hospital Clinic of Barcelona (Spain) and were in accordance with the Declaration of Helsinki. All participants provided informed consent.
Acknowledgments
The authors of this study would like to thank ADKNOMA for the editorial support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study described within the paper was sponsored by Chiesi España SAU.
Disclosure
Pere Almagro declares he has received speaking or advisory fees, or economic aid to attend congresses from Astra-Zeneca, GSK, Novartis, Chiesi, Menarini, Boehringer-Ingelheim, Ferrer, and Rovi. Borja G Cosío declares he has received speaking or advisory fees, or economic aid to attend congresses from Astra-Zeneca, GSK, Novartis, Chiesi, Mundipharma, Menarini, Sanofi, TEVA, Boehringer-Ingelheim, and Rovi. He also reports non-financial support from Separ. Juan José Soler-Cataluña has received speaker fees from AstraZeneca, Bial, Boehringer Ingelheim, Chiesi, FAES, GSK, Menarini, and consulting fees from Bial, Boehringer Ingelheim, Chiesi and GSK. Diego Gonzalez-Segura is an employee of Chiesi España SAU, the sponsor of the study. The authors report no other conflicts of interest in this work.
References
1. Agusti A, MacNee W. The COPD control panel: towards personalised medicine in COPD. Thorax. 2013;68(7):687–690. doi:10.1136/thoraxjnl-2012-202772
2. Miravitlles M, Soler-Cataluña JJ, Calle M, et al. Treatment of COPD by clinical phenotypes: putting old evidence into clinical practice. Eur Respir J. 2013;41(6):1252–1256. doi:10.1183/09031936.00118912
3. Singh D, Agusti A, Anzueto A, et al. Global strategy for the diagnosis, management, and prevention of Chronic Obstructive Lung Disease: the GOLD science committee report 2019. Eur Respir J. 2019;53(5):1900164. doi:10.1183/13993003.00164-2019
4. Ur Rehman A, Hassali MAA, Abbas S, et al. Pharmacological and non-pharmacological management of COPD; limitations and future prospects: a review of current literature. J Public Health. 2020;28(4):357–366. doi:10.1007/s10389-019-01021-3
5. Busch R, Han MK, Bowler RP, et al. Risk factors for COPD exacerbations in inhaled medication users: the COPDGene study biannual longitudinal follow-up prospective cohort. BMC Pulm Med. 2016;16(1):28. doi:10.1186/s12890-016-0191-7
6. Nibber A, Chisholm A, Soler-Cataluña JJ, et al. Validating the concept of COPD control: a real-world cohort study from the United Kingdom. COPD. 2017;14(5):504–512. doi:10.1080/15412555.2017.1350154
7. Soler-Cataluña JJ, Alcazar-Navarrete B, Miravitlles M, et al. The concept of control in COPD: a new proposal for optimising therapy. Eur Respir J. 2014;44(4):1072–1075. doi:10.1183/09031936.00064414
8. Soler-Cataluña JJ, Alcazar B, Miravitlles M. The concept of control of COPD in clinical practice. Int J Chron Obst Pulm Dis. 2014;9:1397–1405.
9. Soler-Cataluña JJ, Almagro P, Huerta A, et al. Determinants of disease control in patients with severe COPD. The CLAVE Study. Eur Resp J. 2019;54:2723.
10. Lopez-Campos JL, Bustamante V, Muñoz X, et al. Moving towards patient-centered medicine for COPD management: multidimensional approaches versus phenotype-based medicine—a critical view. COPD. 2014;11(5):591–602. doi:10.3109/15412555.2014.898035
11. Miravitlles M, Sliwinski P, Rhee CK, et al. Evaluation of criteria for clinical control in a prospective, international, multicenter study of patients with COPD. Respir Med. 2018;136:8–14. doi:10.1016/j.rmed.2018.01.019
12. Baloira A, Gonzalez-Moro JMR, Sanjuán E, et al. Degree of control of patients with chronic obstructive pulmonary disease in Spain: SINCON study. BMC Pulm Med. 2018;18(1):183. doi:10.1186/s12890-018-0749-7
13. Jones PW, Harding G, Berry P, et al. Development and first validation of the COPD Assessment Test. Eur Respir J. 2009;34(3):648–654. doi:10.1183/09031936.00102509
14. Hagströmer M, Oja P, Sjöström M. The International Physical Activity Questionnaire (IPAQ): a study of concurrent and construct validity. Public Health Nutr. 2006;9(6):755–762. doi:10.1079/PHN2005898
15. Plaza V, Fernández-Rodríguez C, Melero C, et al. Validation of the “Test of the Adherence to Inhalers” (TAI) for asthma and COPD patients. J Aerosol Med Pulm Drug Deliv. 2016;29(2):142–152. doi:10.1089/jamp.2015.1212
16. Charlson ME, Pompei P, Ales KL, et al. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. doi:10.1016/0021-9681(87)90171-8
17. Molina paris J. How can we define well-controlled chronic obstructive pulmonary disease? Expert Rev Respir Med. 2013;7(sup2):3–15. doi:10.1586/ers.13.15
18. Chatila WM, Thomashow BM, Minai OA, et al. Comorbidities in chronic obstructive pulmonary disease. Proc Am Thorac Soc. 2008;5(4):549–555. doi:10.1513/pats.200709-148ET
19. Vestbo J, Anderson JA, Calverley PM, et al. Adherence to inhaled therapy, mortality and hospital admission in COPD. Thorax. 2009;64(11):939–943. doi:10.1136/thx.2009.113662
20. Waschki B, Kirsten A, Holz O, et al. Physical activity is the strongest predictor of all-cause mortality in patients with COPD: a prospective cohort study. Chest. 2011;140(2):331–342. doi:10.1378/chest.10-2521
21. Watz H, Pitta F, Rochester CL, et al. An official European Respiratory Society statement on physical activity in COPD. Eur Respir J. 2014;44(6):1521–1537. doi:10.1183/09031936.00046814
22. Guimarães M, Bugalho A, Oliveira AS, et al. COPD control: can a consensus be found? Rev Port Pneumol. 2016;22(3):167–176. doi:10.1016/j.rppnen.2016.01.004
23. Hillas G, Perlikos F, Tsiligianni I, et al. Managing comorbidities in COPD. Int J Chron Obstruct Pulmon Dis. 2015;10:95–109. doi:10.2147/COPD.S54473
24. Miravitlles M, Baek S, Vithlani V, et al. Optimal bronchodilation for COPD patients: are all long-acting β 2 -agonist/long-acting muscarinic antagonists the same? Tuberc Respir Dis. 2018;81(3):198–215. doi:10.4046/trd.2018.0040
25. Humenberger M, Horner A, Labek A, et al. Adherence to inhaled therapy and its impact on chronic obstructive pulmonary disease (COPD). BMC Pulm Med. 2018;18(1):163. doi:10.1186/s12890-018-0724-3
26. George M. Adherence in asthma and COPD: new strategies for an old problem. Respir Care. 2018;63(6):818–831. doi:10.4187/respcare.05905
27. Bai JW, Chen XX, Liu S, et al. Smoking cessation affects the natural history of COPD. Int J Chron Obstruct Pulmon Dis. 2017;12:3323–3328. doi:10.2147/COPD.S150243
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Disease Progression and Age as Factors Underlying Multimorbidity in Patients with COPD: Results from COSYCONET
Alter P, Kahnert K, Trudzinski FC, Bals R, Watz H, Speicher T, Söhler S, Andreas S, Welte T, Rabe KF, Wouters EFM, Sassmann-Schweda A, Wirtz H, Ficker JH, Vogelmeier CF, Jörres RA
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:1703-1713
Published Date: 29 July 2022
The Microbiome in COPD: Emerging Potential for Microbiome-Targeted Interventions
Millares L, Monso E
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:1835-1845
Published Date: 12 August 2022
Impact of Cardiovascular and Metabolic Comorbidities on Long-term Outcomes of Home-based Pulmonary Rehabilitation in COPD
Grosbois JM, Détrée A, Pierache A, Bautin N, Pérez T, Wallaert B, Chenivesse C, Le Rouzic O
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:155-167
Published Date: 23 February 2023
Automated Oxygen Administration Alleviates Dyspnea in Patients Admitted with Acute Exacerbation of COPD: A Randomized Controlled Trial
Sandau C, Hansen EF, Ringbæk TJ, Kallemose T, Bove DG, Poulsen I, Nørholm V, Pedersen L, Jensen JUS, Ulrik CS
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:599-614
Published Date: 18 April 2023
Cardiovascular Events According to Inhaler Therapy and Comorbidities in Chronic Obstructive Pulmonary Disease
Kim EK, Lee E, Park JE, Lee JS, Choi HS, Park B, Sheen SS, Park KJ, Rhee CK, Lee SY, Yoo KH, Park JH
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:243-254
Published Date: 19 January 2024