")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Analyzing the Effectiveness of mHealth to Manage Diabetes Mellitus Among Adults Over 50: A Systematic Literature Review
Authors Kruse CS , Mileski M , Heinemann K , Huynh H, Leafblad A, Moreno E
Received 9 October 2022
Accepted for publication 5 December 2022
Published 12 January 2023 Volume 2023:16 Pages 101—117
DOI https://doi.org/10.2147/JMDH.S392693
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Clemens Scott Kruse, Michael Mileski, Katharine Heinemann, Hung Huynh, Abigail Leafblad, Emmanuel Moreno
School of Health Administration, Texas State University, San Marcos, TX, USA
Correspondence: Michael Mileski, Texas State University, School of Health Administration, 601 University Drive, Encino Hall— 250, San Marcos, TX, 78666, USA, Tel +1 512 245 3556, Email [email protected]
Purpose: A total of 537 million suffered from diabetes mellitus in 2021, and the aging of the population will not abate this number in the future. Diabetes predisposes people to ailments and doubles the risk of COVID-19 mortality. mHealth has shown promise to help manage diabetes. The aim of this review is to objectively analyze research from the last 2.5 years to assess effectiveness where mHealth has been used as an intervention to help manage diabetes in older patients. We also analyzed patient satisfaction, quality, and barriers to adoption of mHealth to manage diabetes.
Patients and Methods: No human subjects were involved in this review. We queried four research databases for mHealth to manage diabetes in older adults. We conducted the review based on the Kruse Protocol for writing as systematic review and we reported our findings in accordance with PRISMA (2020).
Results: Thirty research articles from 11 countries were analyzed. Five interventions of mHealth were identified. Of these mHealth Short Message service (SMS) helped change behavior and encouraged self-care. mHealth SMS coupled with telemedicine for coaching showed positive effects on weight loss, BMI, diet, exercise, HbA1C, disease awareness, blood pressure, cholesterol, medication adherence, and foot care.
Conclusion: mHealth SMS coupled with telemedicine for coaching shows the greatest promise for educating, changing behavior, and realizing positive outcomes across a broad spectrum of health factors. The largest drawback is the cost of acquiring equipment and training users.
Keywords: mHealth, telemedicine, eHealth, telehealth, diabetes mellitus
Plain Language Summary
This systematic review analyzes studies published over the last 2.5 years in academic, peer-reviewed literature to identify mHealth-related interventions to manage Type 2 Diabetes Mellitus. Through data extraction on 30 articles from 11 countries, we identified five mHealth-related interventions. These interventions were found to improve symptoms of Type 2 Diabetes Mellitus, and many interventions show improvement over treatment as usual. Employing technologically-inclined interventions can help meet a preference of patients while still feeling confident about their efficacy. This study has implications for administrators, clinicians, and policy makers.
Introduction
Rationale
Telemedicine is defined as healing at a distance through the use of information and communication technologies.1 Telemedicine encompasses a wide range of clinical interventions including mHealth and eHealth. The distinction between the latter and former is that the latter involves a computer as the interface while the former involves mobile technology such as a cellular phone or tablet. mHealth and eHealth are forms of telehealth. mHealth uses mobile technology to heal at a distance and eHealth uses computer based apps to do the same. These are closely related because most computer applications can be accessed through mobile devices. Mobile devices are convenient, and they are hosting medical-related applications to help patients manage many medical conditions.
It is important to note in studying alternative modalities of care that improvements that are not statistically different from treatment as usual is usually still a significant event to report. Some patients prefer technologically inclined interventions. When an mHealth intervention shows improvement that is close to treatment as usual, it means the provider can assign this intervention to the patient because it fulfils a preference and its efficacy is sound. The advantages inherent to technological interventions such as mHealth is that they allow healing at a distance. They help avoid miles driven and time expended to travel to a medical appointment. They prevent exposure to the medical environment.
Diabetes mellitus “is a heterogeneous group of disorders characterized by hyperglycemia due to an absolute or relative deficit in insulin production or action.”2 This condition is associated with end organ damage, dysfunction, and failure of the retina, kidney, nervous system, heart, and blood vessels. The prevalence of this group of disorders is estimated by the International Diabetes Federation of 537 million in 2021 and predicted to rise to 643 million by 2030.3 About 90% of those with diabetes have Type 2 diabetes, which is lifestyle-related. This distinction is important because treatments for type 2 do not always work with type 1. Diabetes affects older people more than any other age group ranging from 22–33% of the population.4 With the aging of the population, diabetes in this age group should have priority because the prevalence will increase as the number of people entering this age bracket increases, thus causing a greater burden to the healthcare system. Diabetes doubles the risk of COVID-19 mortality to older adults.5
Type I diabetes is characterized by the destruction of the beta cells of the pancreas, leading to insulin deficiency in the patient.6 Treatment for type I diabetes includes insulin replacement therapy which meets specific glycemic targets.6 Type II diabetes is characterized by hyperglycemia, insulin resistance, and impaired insulin secretion.7 Treatment for type II diabetes includes educational measures, continuous evaluation for vascular complications, minimization of long-term risk factors, lifestyle changes, and attempts to achieve normoglycemia, often using insulin therapy.8 Resulting from the COVID-19 pandemic, those who suffered from the infection can suffer from type I or type II diabetes and are often seen with severe metabolic manifestations of diabetes which include diabetic ketoacidosis, hyperosmolar hyperglycemic states, and severe insulin resistance.8,9
Telehealth has been used as an intervention to help monitor and manage diabetes for decades. It is used for telemonitoring, glucose recording, and communication with providers.10 The telehealth intervention is associated with convenience, access, and time savings for patients.11 However, disadvantaged communities are often challenged with limited technological literacy, and telehealth in general is used less by people older than 65.12 A marked increase in the use of telehealth is evidenced post pandemic, and telehealth is expected to continue to be a frequently utilized treatment modality.13,14 Management of chronic conditions such as diabetes is increasingly being conducted via telehealth.14–16 A descriptive systematic review was published in 2017 to explore the enablers and barriers faced by adults with diabetes using two-way information technologies to support diabetes self-management.17 A team of reviewers analyzed 48 articles and identified enablers (access to reliable technology, highly automated data entry, graphical display of data with immediate feedback, and supportive healthcare professionals and family members) and barriers (poorly designed interfaces and systems that lacked functionalities valued by patients).
A systematic review was published in 2021 that explored the effectiveness of technology-based psychosocial interventions on diabetes distress and health-relevant outcomes.18 This group of reviewers analyzed 20 randomized control trials to conclude that technology-based psychosocial interventions improved diabetes distress, self-efficacy and HbA1c levels with significant and small effect sizes.
Objectives
The purpose of this review is to analyze the effectiveness of mHealth to manage Type 2 diabetes mellitus self-care among adults greater than 50 years old from literature published over the last 2.5 years in peer-reviewed academic journals.
Material and Methods
Eligibility Criteria
The eligibility criteria for this review is older adults (over the age of 50), research articles published in the last 2.5 years in peer-reviewed, academic journals, using mixed method, quantitative, and qualitative, methods to analyze the relationship between mHealth as an intervention to manage the self-care of diabetes mellitus. Two and a half years was chosen due to the plethora of articles available on this topic, and to focus on research efforts since the beginning of the pandemic. In addition, this time frame produces articles incident to COVID-19, a period when telehealth tools were used ubiquitously in medicine due to the inability to meet face-to-face. In order to avoid confounding results, other systematic reviews were not included in the analysis because systematic reviews already reported on results from studies that may also be counted in our analysis. Articles should report results of studies. Grey literature was only considered if the articles reported results.
Information Sources
Four research databases were queried: PubMed (MEDLINE), CINAHL Ultimate, Web of Science, and Science Direct. They were searched between July 1st and July 20th 2022.
Search Strategy
We created a Boolean search string to combine key terms listed in the Medical Subject Headings (MeSH) of the US Library of Medicine. We used the same search strategy in all databases. The search string was (mhealth OR ehealth OR telemedicine OR smartphone) AND (diabetes OR “diabetes control”) AND (‘older adult’ OR elderly). We used similar filter strategies, because not all databases have the same tools. MEDLINE was excluded from all databases except PubMed to eliminate duplicates.
Selection Process
In accordance with the Kruse Protocol, we searched key terms in all databases, filtered results, and screened abstracts for applicability.19 At least two reviewers screen each abstract and analyzed each study. Three consensus meetings were held to determine which articles would be analyzed, which data-extraction items were significant measurements of effectiveness, and what observations should become themes. Results were reported in accordance with the PRISMA 2020 standard.20
Data Collection Process
We used a standardized Excel spreadsheet to extract data, and we collected additional data at each step of the process. This spreadsheet was standardized in the Kruse Protocol and has developed over a decade of use to collect data useful for clinicians, administrators, and policy makers.19 We used a series of three consensus meetings to screen abstracts, identify articles for analysis, and identify themes through narrative analysis.21
Data Items
In accordance with the Kruse Protocol, we collected the following fields of data at each step: Participants, experimental intervention (mHealth), results compared with a control, medical outcomes commensurate with the intervention, study design, sample size, bias identified in the study, effect size, country of origin, statistics used, patient satisfaction, quality associated with the intervention (effectiveness), barriers to adoption, strength of evidence and quality of evidence.
Study Risk of Bias Assessment
We observed bias and assessed the quality of each study using the John’s Hopkins Nursing Evidence Based Practice tool (JHNEBP).22 We considered the instances of bias in how to interpret the results because bias can limit external validity.23
Effect Measures
Because we chose to accept mixed methods and qualitative studies, we were unable to standardize summary measures, as would be performed in a meta-analysis. We reported measures of effect in tables for those studies in which it was reported. The odds ratio was the preferred measure of effect, but we also collected measures reported as Cohen’s d. These were tabulated and reported.
Synthesis Methods
A thematic analysis was performed after data extraction was completed.21 This procedure helps makes sense of the data collected through data extraction. Although this technique is often used in qualitative research, its use in quantitative research is well established in the literature.24–26
Reporting Bias Assessment
The overall ratings of quality from the JHNEBP provide us with an assessment of the applicability of the cumulative evidence by identifying the strength and quality of evidence. Each reviewer recorded observations of bias on the standardized spreadsheet.
Additional Analyses and Certainty Assessment
We performed a narrative analysis of the observations to convert them into themes.21 We calculated frequency of occurrence and reported these in affinity matrices. The frequency does not imply importance: only the probability of occurrence in the group of articles for analysis. The reported frequency also provides confidence in the data analyzed.
Results
Study Selection
Figure 1 illustrates the article selection process, to include the inclusion and exclusion criteria from four databases plus one targeted article search. A kappa statistic was calculated based on the level of agreement between authors, (k=0.99, near perfect agreement).27,28 The initial search yielded 113,698 results. A series of filters (full text, human subjects, English language, peer-reviewed, academic journals, and exclude reviews), abstract screening, and a brief full article examination reduced the final group to 30. About 42% of those rejected were due to the age of the participants. These 30 studies generated from 11 different countries, but most were from the US (14/30, 47%), China (4/30, 13%), the UK (2/30, 7%), Korea (2/30, 7%), and Bangladesh (2/30, 7%). Eastern and Western medicines are different in their approach, but they were included to provide a comprehensive overview of interventions and their level of success.
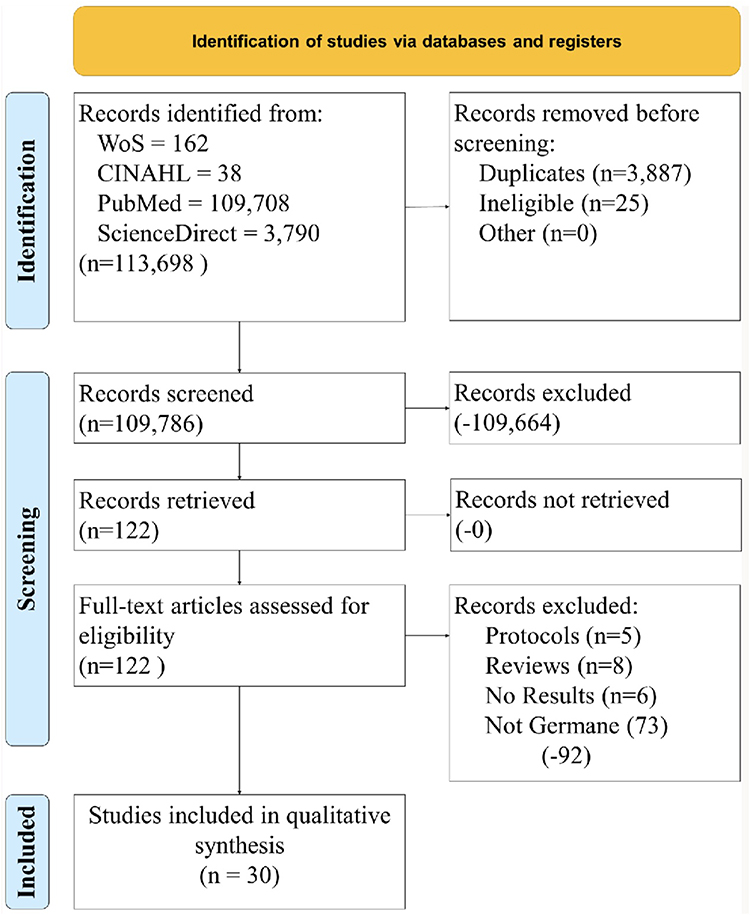 |
Figure 1 PRISMA diagram—article selection process. Notes: PRISMA figure adapted from Page MJ, McKenzie JE, Bossuyt PM et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. Creative Commons.20 |
Study Characteristics
Following the PRISMA (2020) checklist, Table 1 was created to summarize the characteristics of each article analyzed (participants, intervention, comparison, outcomes, study design, PICOS). Of the 30 articles analyzed, over the 2.5 year period, 100% were older adults over 50, 100% implemented a form of mHealth for the intervention (mHealth app 37%, mHealth Short Message Service (SMS) 27%, mHealth plus remote monitoring 17%, mHealth plus telemedicine 13%, mHealth app plus SMS 7%). Of the 30 studies, 15 (50%) were randomized control trials (RCT), 6 (20%) were qualitative, 3 (10%) were observational and 3 were quasi-experimental, 2 (7%) were true experiments, and 1 was a focus group. Slightly less than half originated in the United States (14/30, 47%). Studies are listed in chronological order and alphabetically: 2020 (n=19),29–47 2021 (n=8),48–55 2022 (n=3).56–58 For each study, we extracted the following data fields: participants, intervention, comparison (to control or other group), medical outcomes, study design, sample size, bias within study, country of origin, statistics used, patient satisfaction, quality associated with intervention, barriers to adoption, strength of evidence, and quality of evidence. This was performed as a way to summarize study characteristics in a manner established in the literature. Results varied across studies. Twenty-five out of 30 (83%) articles found an improvement in at least one area studied, (eg, HbA1C), but the improvement was not always statistically significant. While mHealth apps were effective at helping diabetes patients manage their disease, some apps required manual entry of data, which discouraged users from using it. The intervention of mHealth SMS showed consistently improvement across multiple focus areas: BMI, weight loss, exercise, diet, disease awareness, HbA1C, and healthy behaviors. Similar results were also observed with mHealth plus telemedicine coaching. Additional explanation of the results will be provided below.
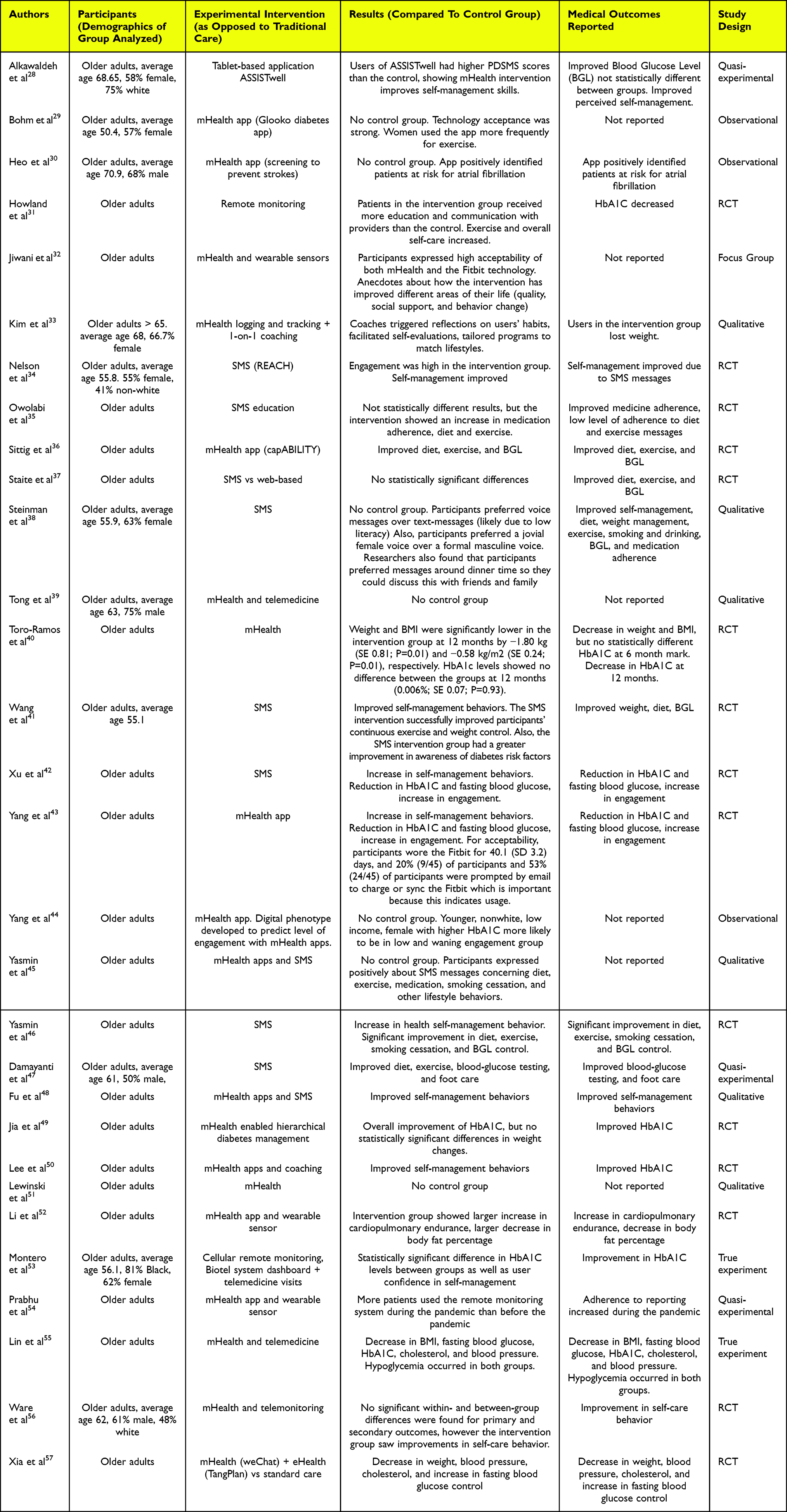 |
Table 1 PICOS |
Risk and Reporting of Bias in Studies
Reviewers used the JHNEBP quality assessment tool identified the following the strength and quality of evidence. Of the 30 articles analyzed, 18/30 (60%) were strength I (the highest rating) because they were either RCTs or true experiments. 10/30 (33%) were type III (qualitative or observational) and 2/30 (7%) were type II (quasi-experimental). Most studies used large samples (average 1022) reported consistent results with definitive conclusions, and used adequate controls, so the quality of evidence was strong, or Type A (23/30, 77%) and the remainder used smaller but adequate samples (7/30, 23%). Studies of type C or strength below III were not used for analysis. Reviewers also made note of bias within and among the studies. The most common bias was selection bias (27/30, 90%) because most studies used convenience samples in one city or country. The second most common was sample bias (8/30, 27%) because the sample was a majority of one gender or race. Selection and sample bias affect the external and internal validity of studies, respectively.
Results of Individual Studies
Reviewers independently analyzed each article and recorded independent observations commensurate with the objective statement. A thematic analysis was conducted as part of sense making.21 Each observation that occurred more than once became a theme. Themes were used to summarize the observations, but they did not always match the observation completely. A summary of the themes is tabulated in Table 2. Articles are listed in chronological order. Appendices 1A and B show an observation-to-theme match. Appendix 1c tabulates the additional data extracted from the literature. Additional analysis of the findings is provided below.
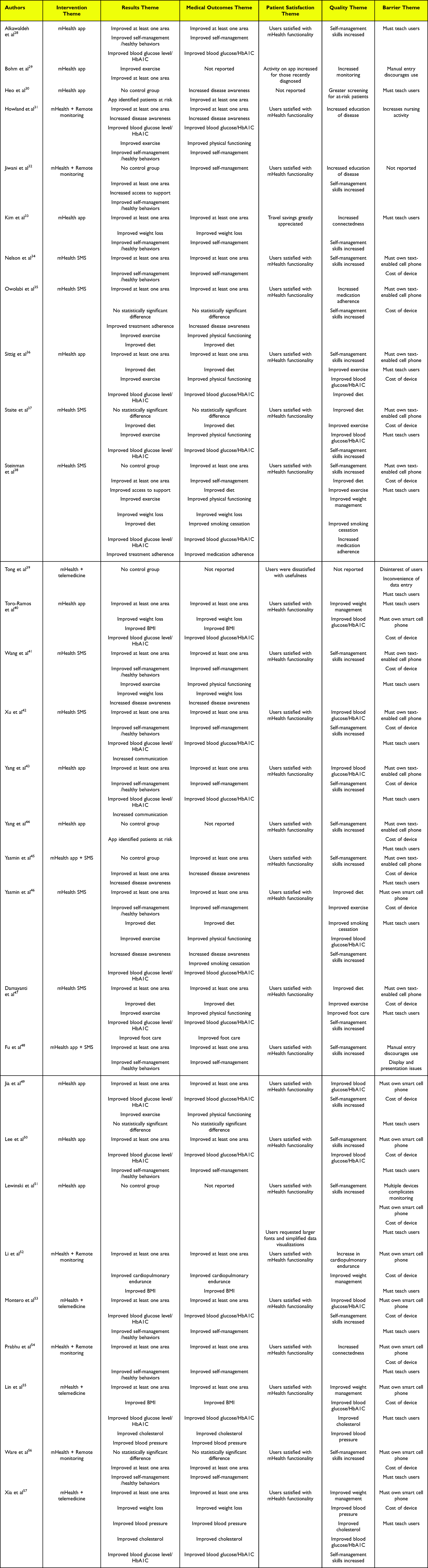 |
Table 2 Summary of Analysis, Sorted Chronologically by Author |
Results of Syntheses, Additional Analysis and Certainty of Evidence
The thematic analysis made sense of the data, and themes were tabulated into affinity matrices for analysis. While frequency does not imply importance, it does provide a probability of occurrence in the group of articles for analysis.
When mHealth apps were utilized as the intervention, the most common patient satisfaction theme was that patients were satisfied with the intervention, however, many were discouraged when the app required manual input of data. When the mHealth apps were coupled with wearable sensors, and the data from the sensors were automatically entered into the app, the observation about manual entry went away. These interventions showed improvement in at least one area of observation, but the results were not as strong as other interventions. When mHealth SMS was utilized as the intervention, patients noted that the messages helped them improve their self-care habits. The results, medical outcomes, and quality observations were strong with this intervention. However, when the mHealth SMS was coupled with telemedicine visits to offer coaching, the results were the strongest. Patients developed good self-care behavior, improved in weight loss, diet, exercise, blood glucose levels, cholesterol, blood pressure, and foot care. This intervention showed the strongest results.
Three sections of themes are similar, but they were created for different audiences. The section “results” is generic, and it includes results of studies (compared to a control group, where appropriate) that are both administrative, clinical, and patient-centered. The section “medical outcomes” is designed for the practitioner. The section “Quality” is designed for the administrator. While there are some repeats in these three sections, they are tailored for the specific audiences and some verbiage changes for them.
Results of Studies, Compared with the Control Group
Table 3 tabulates the Result themes and individual observations. Reviewers made some general observations. In 25/30 (83%) articles, an improvement in at least one area was observed, but the improvement was not always statistically significant. This accounted for 25/107 (23%) of the observed themes or observations.29,30,32–37,39,41–43,45–51,53–58 Improved self-management behaviors appeared in 14/107 (13%) of the occurrences.29,32–35,42,43,45,47,49,51,54,55,57 Patients who used mHealth as interventions in their care demonstrated improved blood glucose level (BGL)/HbA1C, included fasting blood glucose (FBG). This theme appeared in 15/107 (14%) of the occurrences.29,32,37–39,41,43,45,47,48,50,51,54,56,58 The theme “improved exercise” appeared in 10/107 (9%) of the occurrences. The themes “improved diet”36–39,47,48 and “improved weight loss”34,39,41,42,58 each appeared in 6/107 (6%) of the occurrences. The theme “increased disease awareness” appeared in 4/107 (4%) of the occurrences. Improved BMI appeared in 3/107 (3%) occurrences. The themes “increased communication”,43,45 “improved blood pressure”,56,58 “improved cholesterol”,56,58 “improved treatment adherence”,36,39 and “app identified patients at risk”,31,44 each occurred in 2/107 (2%) occurrences. The following observations could not be categorized into themes: “increased access to support”, “improved cardiopulmonary endurance”, and “improved foot care.”33,48,53
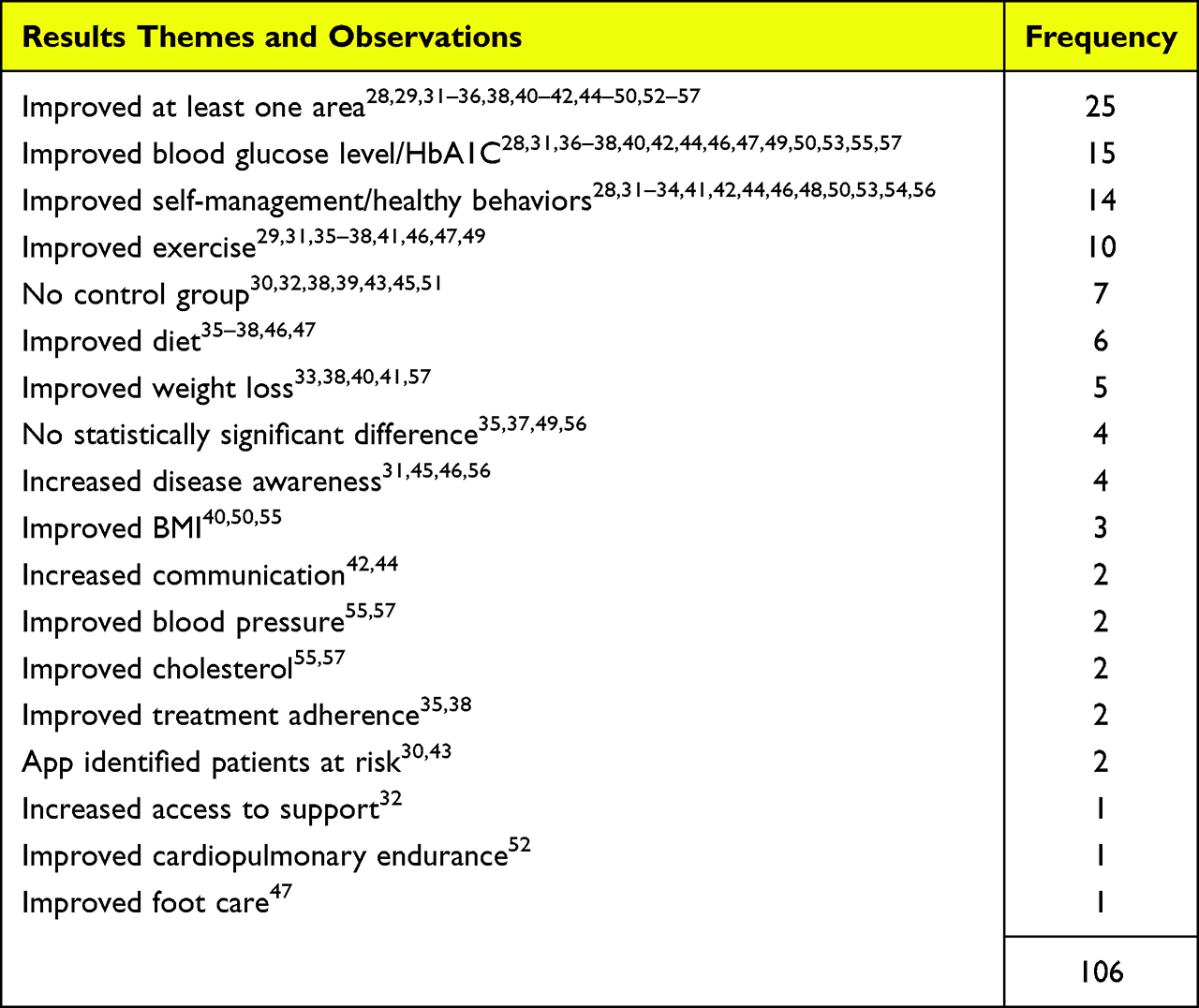 |
Table 3 Results Themes and Observations |
Medical Outcomes Commensurate with the Intervention
Table 4 tabulates the medical outcome themes and observations. Like in the results themes, reviewers made some general observations: the use of mHealth interventions showed improvements in at least one clinical area in 24/30 articles (60%),29,31,32,34–37,39,41–43,45–51,53–58 and there was an improvement in self-management in 15/30 articles (50%).29,32–35,39,42,43,45,47,49,51,54,55,57 The theme “improved blood glucose/HbA1C” appeared 15/100 (15%) of the occurrences.29,32,37–39,41,43,45,47,48,50,51,54,56,58 The theme “improved physical functioning” occurred 9/100 (9%) occurrences.32,36–39,42,47,48,50 Improved diet36–39,47,48 and increased disease awareness31,32,36,42,46,47 each appeared 6/100 (9%) occurrences. Improved weight loss occurred 5/100 (5%) of the occurrences.34,39,41,42,58 Improved BMI occurred 3/100 (3%) of the occurrences.41,53,56 The themes “improved cholesterol”,56,58 “improved smoking cessation”,39,47 and “improved blood pressure”,56,58 each occurred 2/100 (2%) of the occurrences. Finally, three observations could not be categorized into themes: “improved medication adherence”, “improved foot care”, and “improved cardiopulmonary endurance.”39,48,53
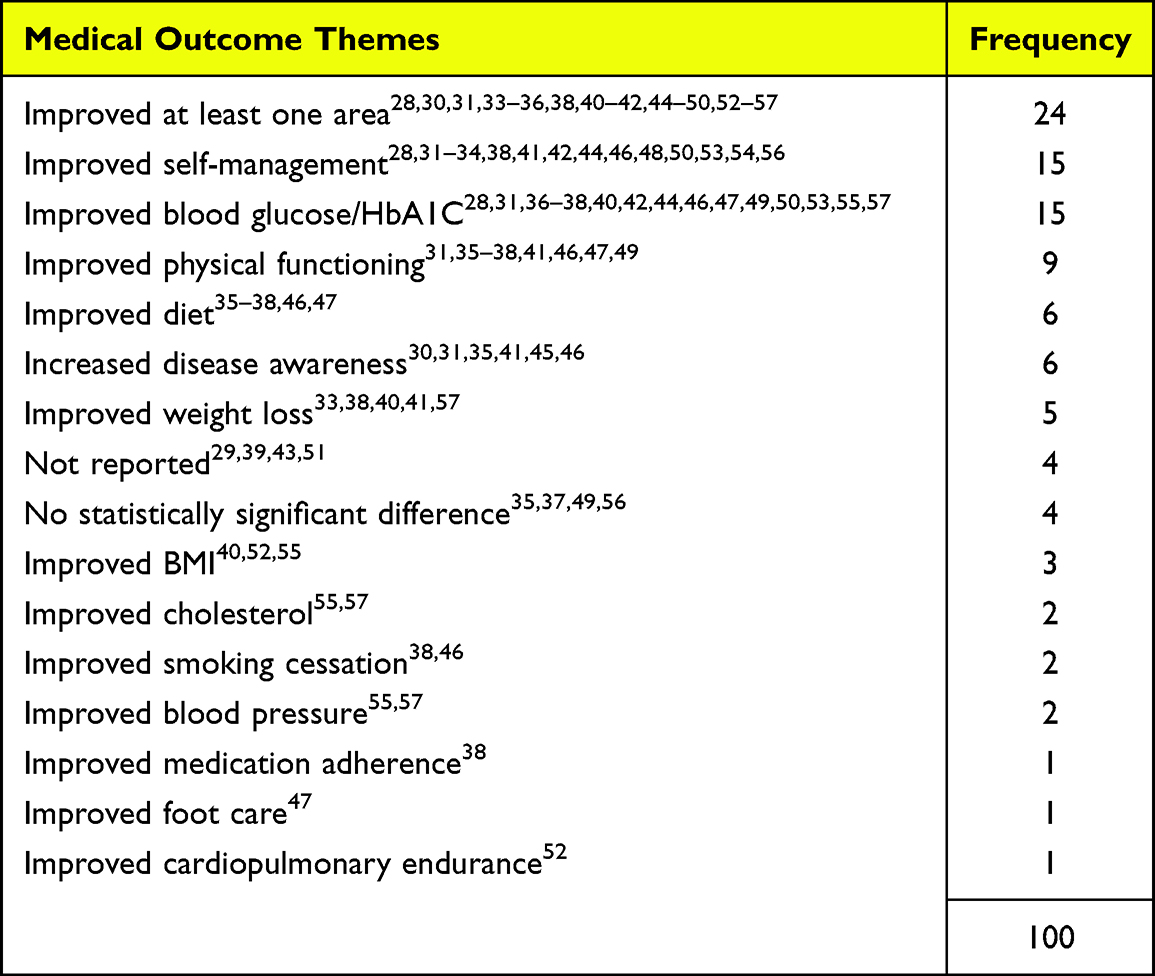 |
Table 4 Medical Outcomes Themes and Observations |
Quality Themes and Observations Commensurate with the Intervention
Table 5 tabulates the Quality themes and observations. Of these observations, the “increase in self-management skills” is the most significant, appearing 21/80 (26%) of the occurrences.29,32–39,43–46,50,51,54,55,57,58 Improved blood glucose/HbA1C appeared in 15/80 (19%) of the occurrences.29,32,37–39,41,43,45,47,48,50,51,54,56,58 Improved exercise32,36–39,42,47,48,50 appeared 9/100 (9%), and improved weight management34,39,41,42,53,56,58 appeared 8/100 (8%) of the occurrences. Improved diet36–39,47,48 appeared 6/100 (6%) and increased education of disease32,33,36,42,47 occurred 5/100 (5%) of the occurrences. The following themes each appeared 2/100 (2%) of the occurrences: “increased medication adherence”,36,39 “improved smoking cessation”,39,47 “improved blood pressure”,56,58 “improved cholesterol”,56,58 and “increased connectedness.” The following observations could not be categorized into a theme: “improved foot care”,48 “increased monitoring”, “greater screening for at-risk patients”, and “increase in cardiopulmonary endurance.”30,31,48,53
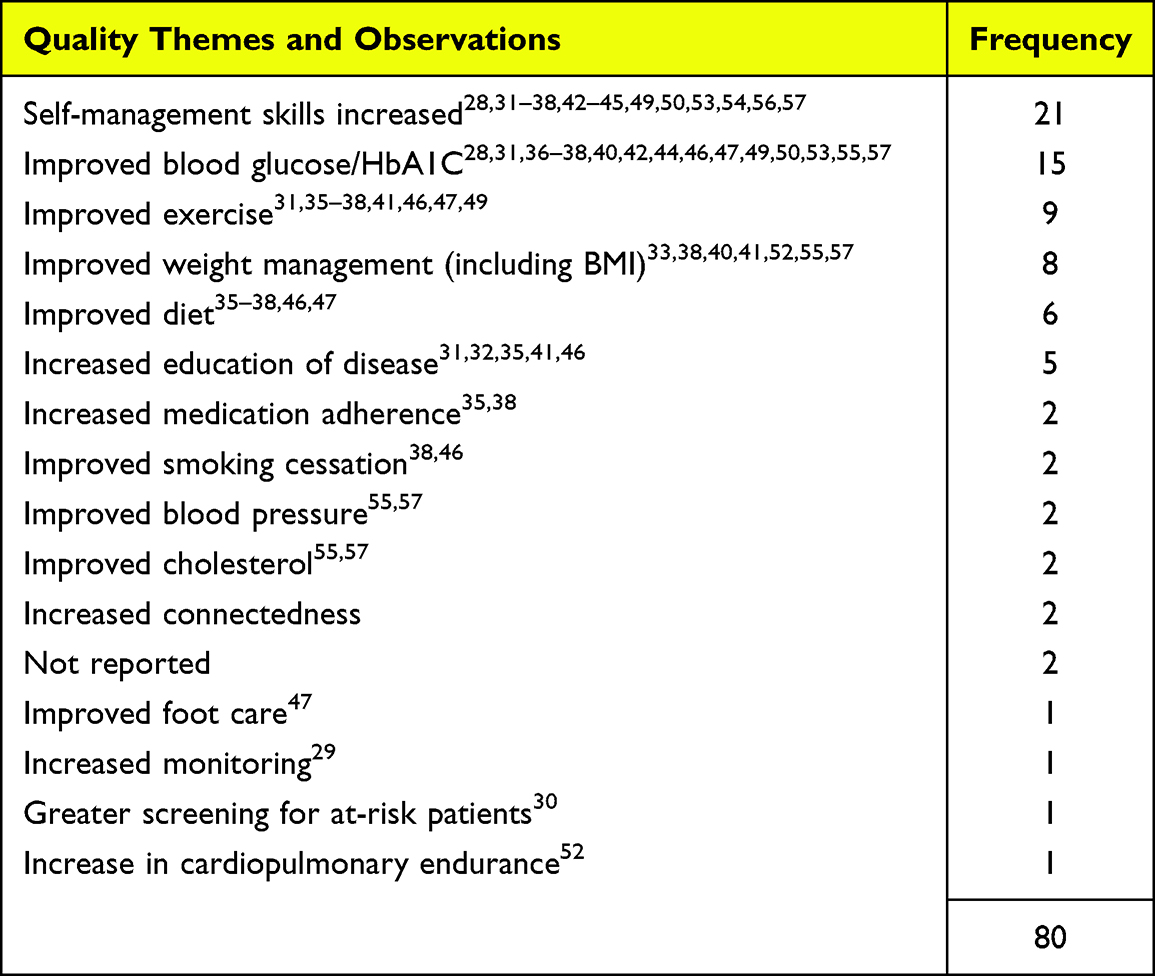 |
Table 5 Quality Themes and Observations |
The most commonly identified theme for patient satisfaction was that patients/participants were satisfied with the functionality of mHealth. This theme appeared 26/31 (84%) of the occurrences.29,32,33,35–39,41–58 Four other observations were identified, but they could not be fit into themes: “Activity on app increased for those recently diagnosed with diabetes”, “users were dissatisfied with usefulness”, “travel savings were greatly appreciated because the mHealth app prevented them from driving into the clinic”, and “users requested larger fonts and simplified data visualizations.”30,34,40,52
Table 6 tabulates the themes and observations associated with barriers to adoption of mHealth interventions for the management of diabetes. The most common themes identified were associated with the necessity to acquire a mobile device in order to use it as an intervention. This includes the cost of acquisition and the training of the users. Teaching users occurred the most often, 24/76 (32%).29,31,34,37–48,50–58 Cost of device appeared 22/76 (29%) of the occurrences.35,36,38,39,41–48,51,52,54–58 Must own a text-enabled cell phone18,35–39,42,43,45,46,48 or a smart cell phone each occurred 11/76 (14%).41,47,50–58 Manual entry of data discourages use of the app appeared 2/76 (3%) of the occurrences.30,49 The following observations could not be categorized into a theme: “Disinterest of users”, “inconvenience of data entry”, “display and presentation issues”, “multiple devices complicates monitoring”, and nursing activities increase as a result of the intervention.”32,40,49,52
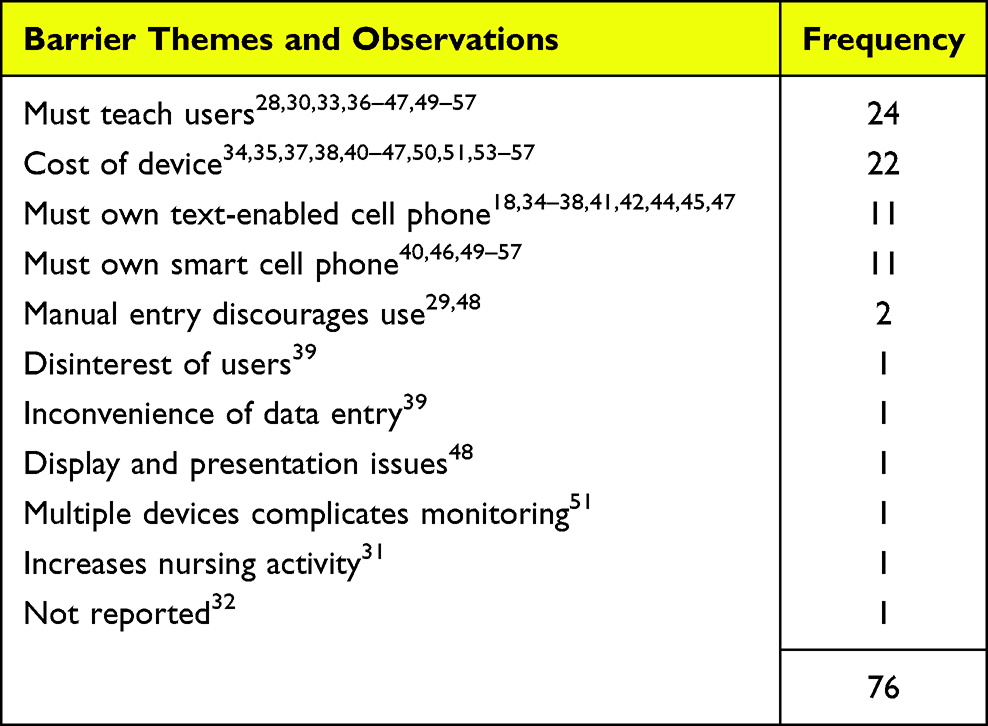 |
Table 6 Themes and Observations for Barriers to the Adoption of mHealth Interventions |
Discussion
Summary of Evidence
This research found that 83% of the articles analyzed reported a positive outcome in at least one area of focus.29,30,32–37,39,41–43,45–51,53–58 mHealth SMS helps patients develop health habits and increase their level of self-care.35,36,38,42,43,46–49,59 The most significant finding of this research is that mHealth SMS coupled with telemedicine for coaching yields positive results for BMI, weight loss, exercise, foot care, diet, and overall self-care.40,54,56,58
Healthcare providers can leverage mHealth SMS services to help diabetes patients create health habits and improve self-care for older adults. Coupled with telemedicine visits, provider teams can coach diabetes patients into long-term, self-care habits and decrease mortality incident to the disease. mHealth SMS coupled with telemedicine not only serves as a preventative for future diabetes-related ailments, but it also increases the health and longevity of patients who have suffered with diabetes for years.
Administrators can view the expense of mHealth SMS and telemedicine interventions as both preventative and ongoing maintenance of diabetes. These measures greatly increase the self-management of diabetes patients. Screening tools can be employed to identify at-risk patients and begin to change their habits early.
Developers should note the continued observations about manual entry, small fonts, and complicated data visualizations. Manual entry of data discourages users from using the app.49 mHealth applications should fully interface with the wearable sensors and transmit data to the provider team and electronic health record. Fonts must be large enough for older adults to comfortably view, and data visualizations should be simple enough to provide immediate feedback and, if necessary, compel action.52
Future research should explore mHealth combinations more thoroughly. Does mHealth apps plus telemedicine coaching yield as strong of results? Do mHealth apps, SMS, and telemedicine yield strong results? Also, cohort studies would be helpful to determine if the change in self-management is transitory or long term. This study analyzed Type 2 diabetes, instead of Type 1. Future research should focus on Type 1 diabetes. Historically, Type 1 diabetes has only comprised less than 10% of the diabetes population, but COVID-19 has caused a large surge in this population. Type 1 diabetes has always been a significant disease to study, and COVID-19 has raised its importance.
Limitations
A limitation of this review is the short time-frame chosen for publication of articles. We chose 2.5 years due to the plethora of results that occurred in our initial search using 5 or 10 years. Analyzing additional articles may have yielded new results or additional iterations of the same results. However, technology advances rapidly, and more recent articles will reflect current technology and capabilities of the same. Additionally, our search string focused on MeSH terms (with the exception of “smartphone”), which might have omitted studies not indexed with MeSH hierarchy. The term “smartphone” was used to control for this issue, however, we may still have not identified all studies.
Including grey literature may have also yielded different results. Our team chose to omit grey literature because opinions are not always based on study results. We chose to include research studies with strong designs. As a result of that decision, half of the articles analyzed in this review were RCTs.
Conclusion
The broad implication of this study is that mHealth SMS helps educate persons with diabetes and when coupled with telemedicine coaching, it yields very strong clinical and administrative results. These particular interventions are not costly, do not adversely affect patient satisfaction, and may result in fewer hospitalizations for diabetes related ailments. Most people own text-enabled phones, but not as many own smart phones. Unless mHealth apps fully interface with remote sensors and transmit data to care teams, patients will lose patience with any manual-entry and will abandon it. SMS, however, provides quick, simple education and reminders to help develop health habits and encourage self-care.
Other Information
This review is conducted in accordance with the Kruse Protocol for writing a systematic review.19 It is reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis.20 This review is registered with PROSPERO: registration number CRD42021266568.
Abbreviations
BGL, Blood glucose level; GLM, General Linear Model; JHNEBP, Johns Hopkins Nursing Evidence Based Practice (tool); PDSMS, Perceived diabetes self-management scale; PICOS, Participants, intervention, comparison (to control), outcomes (medical), and study design; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; RCT, Randomized controlled trial; SMS, Short Message Service.
Ethics Disclosure
This work was exempted from normal IRB processes, as it is a systematic review. The research was conducted in accordance with the Declaration of Helsinki.
Funding
There was no funding associated with this research.
Disclosure
The authors report no conflicts of interest or competing interests with this work.
References
1. World Health Organization. Telemedicine: Opportunities and Developments in Member States. Report on the Second Global Survey on eHealth. World Health Organization; 2010.
2. Alam U, Asghar O, Azmi S, Malik RA. General aspects of diabetes mellitus. Handb Clin Neurol. 2014;126:211–222.
3. International Diabetes Foundation. Diabetes Facts and Figures; 2022. Available from: https://www.idf.org/aboutdiabetes/what-is-diabetes/facts-figures.html.
4. Kirkman MS, Briscoe VJ, Clark N, et al. Diabetes in older adults. Diabetes Care. 2012;35(12):2650–2664.
5. Peric S, Stulnig TM. Diabetes and COVID-19. Wien Klin Wochenschr. 2020;132(13):356–361.
6. Weinstock RS. Management of Blood Glucose in Adults with Type 1 Diabetes Mellitus. UpToDate; 2019.
7. Laffel L, Svoren B. Epidemiology, Presentation, and Diagnosis of Type 2 Diabetes Mellitus in Children and Adolescents. Waltham, MA: UpToDate; 2013.
8. Wexler DJ. Initial Management of Hyperglycemia in Adults with Type 2 Diabetes Mellitus. Waltham, MA: UpToDate; 2021.
9. Pal R, Banerjee M, Yadav U, Bhattacharjee S. Clinical profile and outcomes in COVID-19 patients with diabetic ketoacidosis: a systematic review of literature. Diabetes Metab Syndrome. 2020;14(6):1563–1569.
10. Shah DA, Sall D, Peng W, Sharer R, Essary AC, Radhakrishnan P. Exploring the role of telehealth in providing equitable healthcare to the vulnerable patient population during COVID-19. J Telemed Telecare. 2022;1357633X221113711.
11. Charles BL. Telemedicine can lower costs and improve access. Healthcare Financial Management. 2000;54(4):66.
12. Weber E, Miller SJ, Astha V, Janevic T, Benn E. Characteristics of telehealth users in NYC for COVID-related care during the coronavirus pandemic. J Am Med Informatics Assoc. 2020;27(12):1949–1954.
13. Humphreys J, Schoenherr L, Elia G, et al. Rapid implementation of inpatient telepalliative medicine consultations during COVID-19 pandemic. J Pain Symptom Manage. 2020;60(1):e54–e59.
14. Ong MK, Pfeffer M, Mullur RS, Kunins L. Telemedicine for adults. UpToDate Disponível em; 2021. Available from: https://www.uptodate.com.
15. Bashshur RL, Shannon GW, Smith BR, et al. The empirical foundations of telemedicine interventions for chronic disease management. Telemedicine e-Health. 2014;20(9):769–800.
16. Lee JY, Lee SWH. Telemedicine cost–effectiveness for diabetes management: a systematic review. Diabetes Technol Ther. 2018;20(7):492–500.
17. Macdonald EM, Perrin BM, Kingsley MI. Enablers and barriers to using two-way information technology in the management of adults with diabetes: a descriptive systematic review. J Telemed Telecare. 2018;24(5):319–340.
18. Yap JM, Tantono N, Wu VX, Klainin-Yobas P. Effectiveness of technology-based psychosocial interventions on diabetes distress and health-relevant outcomes among type 2 diabetes mellitus: a systematic review and meta-analysis. J Telemed Telecare. 2021;1357633X211058329.
19. Kruse CS. Writing a Systematic Review for Publication in a Health-Related Degree Program. JMIR Res Protoc. 2019;8(10):e15490. doi:10.2196/15490
20. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372.
21. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101.
22. Newhouse R, Dearholt S, Poe S, Pugh L, White K. The Johns Hopkins Nursing Evidence-Based Practice Rating Scale. Baltimore, MD: The Johns Hopkins Hospital; 2005.
23. Pannucci CJ, Wilkins EG. Identifying and avoiding bias in research. Plast Reconstr Surg. 2010;126(2):619.
24. Kruse C, Heinemann K. Facilitators and Barriers to the Adoption of Telemedicine During the First Year of COVID-19: systematic Review. J Med Internet Res. 2022;24(1):e31752.
25. Kruse CS, Beane A. Health Information Technology Continues to Show Positive Effect on Medical Outcomes: systematic Review. J Med Internet Res. 2018;20(2):e41. doi:10.2196/jmir.8793
26. Kruse CS, Lee K, Watson JB, Lobo LG, Stoppelmoor AG, Oyibo SE. Measures of effectiveness, efficiency, and quality of telemedicine in the management of alcohol abuse, addiction, and rehabilitation: systematic review. J Med Internet Res. 2020;22(1):e13252.
27. Light RJ. Measures of response agreement for qualitative data: some generalizations and alternatives. Psychol Bull. 1971;76(5):365.
28. McHugh ML. Interrater reliability: the kappa statistic. Biochemia medica. 2012;22(3):276–282.
29. Alkawaldeh MY, Choi J, Jacelon CS. A diabetes self-management tablet-based application for older adults with type 2 diabetes: the ASSISTwell pilot study. Geriatr Nurs (Minneap). 2020;41(6):839–845. doi:10.1016/j.gerinurse.2020.05.004
30. Böhm AK, Jensen ML, Sørensen MR, Stargardt T. Real-World Evidence of User Engagement With Mobile Health for Diabetes Management: longitudinal Observational Study. JMIR Mhealth Uhealth. 2020;8(11):e22212. doi:10.2196/22212
31. Heo NJ, Rhee SY, Waalen J, Steinhubl S. Chronic kidney disease and undiagnosed atrial fibrillation in individuals with diabetes. Cardiovasc Diabetol. 2020;19(1):157. doi:10.1186/s12933-020-01128-y
32. Howland C, Despins L, Sindt J, Wakefield B, Mehr DR. Primary Care Clinic Nurse Activities with a Telehealth Monitoring System. West J Nurs Res. 2020;43(1):5–12. doi:10.1177/0193945920923082
33. Jiwani R, Dennis B, Bess C, et al. Assessing acceptability and patient experience of a behavioral lifestyle intervention using fitbit technology in older adults to manage type 2 diabetes amid COVID-19 pandemic: a focus group study. Geriatr Nurs (Minneap). 2021;42(1):57–64.
34. Kim H, Tietsort C, Posteher K, Michaelides A, Toro-Ramos T. Enabling self-management of a chronic condition through patient-centered coaching: a case of an mHealth diabetes prevention program for older adults. Health Commun. 2020;35(14):1791–1799.
35. Nelson LA, Spieker A, Greevy R, LeStourgeon LM, Wallston KA, Mayberry LS. User Engagement Among Diverse Adults in a 12-Month Text Message-Delivered Diabetes Support Intervention: results from a Randomized Controlled Trial. JMIR Mhealth Uhealth. 2020;8(7):e17534. doi:10.2196/17534
36. Owolabi EO, Ter Goon D, Ajayi AI. Impact of mobile phone text messaging intervention on adherence among patients with diabetes in a rural setting: a randomized controlled trial. Medicine. 2020;99(12):548.
37. Sittig S, Wang J, Iyengar S, Myneni S, Franklin A. Incorporating Behavioral Trigger Messages Into a Mobile Health App for Chronic Disease Management: randomized Clinical Feasibility Trial in Diabetes. JMIR Mhealth Uhealth. 2020;8(3):e15927. doi:10.2196/15927
38. Staite E, Bayley A, Al-Ozairi E, et al. A Wearable Technology Delivering a Web-Based Diabetes Prevention Program to People at High Risk of Type 2 Diabetes: randomized Controlled Trial. JMIR Mhealth Uhealth. 2020;8(7):e15448. doi:10.2196/15448
39. Steinman L, Heang H, van Pelt M, et al. Facilitators and Barriers to Chronic Disease Self-Management and Mobile Health Interventions for People Living With Diabetes and Hypertension in Cambodia: qualitative Study. JMIR Mhealth Uhealth. 2020;8(4):e13536. doi:10.2196/13536
40. Tong T, Myers AK, Bissoonauth AA, Pekmezaris R, Kozikowski A. Identifying the barriers and perceptions of non-Hispanic black and Hispanic/Latino persons with uncontrolled type 2 diabetes for participation in a home Telemonitoring feasibility study: a quantitative analysis of those who declined participation, withdrew or were non-adherent. Ethn Health. 2020;25(4):485–494. doi:10.1080/13557858.2019.1566520
41. Toro-Ramos T, Michaelides A, Anton M, et al. Mobile delivery of the diabetes prevention program in people with prediabetes: randomized controlled trial. JMIR mHealth and uHealth. 2020;8(7):e17842.
42. Wang X, Liu D, Du M, Hao R, Zheng H, Yan C. The role of text messaging intervention in Inner Mongolia among patients with type 2 diabetes mellitus: a randomized controlled trial. BMC Med Inform Decis Mak. 2020;20(1):90. doi:10.1186/s12911-020-01129-7
43. Xu R, Xing M, Javaherian K, Peters R, Ross W, Bernal-Mizrachi C. Improving HbA(1c) with Glucose Self-Monitoring in Diabetic Patients with EpxDiabetes, a Phone Call and Text Message-Based Telemedicine Platform: a Randomized Controlled Trial. Telemed J E Health. 2020;26(6):784–793. doi:10.1089/tmj.2019.0035
44. Yang Q, Hatch D, Crowley MJ, et al. Digital Phenotyping Self-Monitoring Behaviors for Individuals With Type 2 Diabetes Mellitus: observational Study Using Latent Class Growth Analysis. JMIR Mhealth Uhealth. 2020;8(6):e17730. doi:10.2196/17730
45. Yang Y, Lee EY, Kim HS, Lee SH, Yoon KH, Cho JH. Effect of a Mobile Phone-Based Glucose-Monitoring and Feedback System for Type 2 Diabetes Management in Multiple Primary Care Clinic Settings: cluster Randomized Controlled Trial. JMIR Mhealth Uhealth. 2020;8(2):e16266. doi:10.2196/16266
46. Yasmin F, Ali L, Banu B, Rasul FB, Sauerborn R, Souares A. Understanding patients’ experience living with diabetes type 2 and effective disease management: a qualitative study following a mobile health intervention in Bangladesh. BMC Health Serv Res. 2020;20(1):29. doi:10.1186/s12913-019-4811-9
47. Yasmin F, Nahar N, Banu B, Ali L, Sauerborn R, Souares A. The influence of mobile phone-based health reminders on patient adherence to medications and healthy lifestyle recommendations for effective management of diabetes type 2: a randomized control trial in Dhaka, Bangladesh. BMC Health Serv Res. 2020;20(1):520. doi:10.1186/s12913-020-05387-z
48. Damayanti MR, Antari GAA, Nopriani NLP. Effect of a Ten-Week Short Message Service-Based Intervention on Self-Management of Type-2 Diabetes Patients in Bali, Indonesia. Nurse Media J Nursing. 2021;11(2):177–186. doi:10.14710/nmjn.v11i2.35257
49. Fu HNC, Jin D, Adam TJ. Content Analysis: first-Time Patient User Challenges with Top-Rated Commercial Diabetes Apps. Telemed J E Health. 2021;27(6):663–669. doi:10.1089/tmj.2020.0128
50. Jia W, Zhang P, Zhu D, et al. Evaluation of an mHealth-enabled hierarchical diabetes management intervention in primary care in China (ROADMAP): a cluster randomized trial. PLoS Med. 2021;18(9):e1003754. doi:10.1371/journal.pmed.1003754
51. Lee MK, Lee DY, Ahn HY, Park CY. A Novel User Utility Score for Diabetes Management Using Tailored Mobile Coaching: secondary Analysis of a Randomized Controlled Trial. JMIR Mhealth Uhealth. 2021;9(2):e17573. doi:10.2196/17573
52. Lewinski AA, Vaughn J, Diane A, et al. Perceptions of Using Multiple Mobile Health Devices to Support Self‐Management Among Adults With Type 2 Diabetes: a Qualitative Descriptive Study. J Nursing Scholarship. 2021;53(5):643–652. doi:10.1111/jnu.12667
53. Li J, Wei D, Liu S, et al. Efficiency of an mHealth App and Chest-Wearable Remote Exercise Monitoring Intervention in Patients With Type 2 Diabetes: a Prospective, Multicenter Randomized Controlled Trial. JMIR Mhealth Uhealth. 2021;9(2):e23338. doi:10.2196/23338
54. Montero AR, Toro-Tobon D, Gann K, Nassar CM, Youssef GA, Magee MF. Implications of remote monitoring Technology in Optimizing Traditional Self-Monitoring of blood glucose in adults with T2DM in primary care. BMC Endocr Disord. 2021;21(1):1–8. doi:10.1186/s12902-021-00884-6
55. Prabhu Navis J, Leelarathna L, Mubita W, et al. Impact of COVID-19 lockdown on flash and real-time glucose sensor users with type 1 diabetes in England. Acta Diabetol. 2021;58(2):231–237. doi:10.1007/s00592-020-01614-5
56. Lin K, Zhang W, He F, Shen J. Evaluation of the Clinical Efficacy of the Treatment of Overweight and Obesity in Type 2 Diabetes Mellitus by the Telemedicine Management System Based on the Internet of Things Technology. Comput Intell Neurosci. 2022;2022:8149515. doi:10.1155/2022/8149515
57. Ware P, Shah A, Ross HJ, et al. Challenges of Telemonitoring Programs for Complex Chronic Conditions: randomized Controlled Trial With an Embedded Qualitative Study. J Med Internet Res. 2022;24(1):e31754. doi:10.2196/31754
58. Xia SF, Maitiniyazi G, Chen Y, et al. Web-Based TangPlan and WeChat Combination to Support Self-management for Patients With Type 2 Diabetes: randomized Controlled Trial. JMIR Mhealth Uhealth. 2022;10(3):e30571. doi:10.2196/30571
59. Suleiman N, Alkasem M, Al Amer Z, et al. Qatar Diabetes Mobile Application Trial (QDMAT): an open-label randomised controlled trial to examine the impact of using a mobile application to improve diabetes care in type 2 diabetes mellitus-a study protocol. Trials. 2022;23(1):504. doi:10.1186/s13063-022-06334-5
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.