Back to Journals » Journal of Pain Research » Volume 19
Updated Evidence of Acupuncture for Trigeminal Neuralgia: A Systematic Review and Meta-Analysis with GRADE Assessment
Authors Xu Y, Zhang L, Jiang Y, Sun J, Fang J, Li R ![]()
Received 23 February 2026
Accepted for publication 15 May 2026
Published 30 May 2026 Volume 2026:19 604548
DOI https://doi.org/10.2147/JPR.S604548
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Houman Danesh
Yaxuan Xu,1,* Lingyu Zhang,1,* Yurong Jiang,1 Jing Sun,1,2 Jianqiao Fang,1,2 Rongrong Li1,2
1The Third Clinical Medical College of Zhejiang Chinese Medical University, Hangzhou, Zhejiang, People’s Republic of China; 2Acupuncture and Moxibustion Department, The Third Affiliated Hospital of Zhejiang Chinese Medical University, Hangzhou, Zhejiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jianqiao Fang, The Third Affiliated Hospital of Zhejiang Chinese Medical University, 219 Moganshan Road, Hangzhou, Zhejiang, 310000, People’s Republic of China, Email [email protected] Rongrong Li, The Third Affiliated Hospital of Zhejiang Chinese Medical University, 219 Moganshan Road, Hangzhou, Zhejiang, 310000, People’s Republic of China, Email [email protected]
Background: Trigeminal neuralgia (TN) is a clinically intractable disorder characterized by episodes of severe pain that often significantly impairs patients’ quality of life. Although previous studies suggest that acupuncture may alleviate pain, it is particularly important to conduct an updated meta-analysis to confirm the effectiveness and safety of acupuncture in light of updated clinical evidence in recent years.
Methods: A systematic search was conducted across eight databases: four English−language (PubMed, Cochrane Library, Embase, and Web of Science) and four Chinese−language (Wanfang Data, China National Knowledge Infrastructure, China Science and Technology Journal Database, and China Biomedical Literature Service System). The search period for each database spans from its inception to 19 December 2025. Meta−analysis was conducted by using Stata 17.0.
Results: A total of 38 randomized controlled trials involving 2836 patients with TN were included. Meta−analysis results showed that compared with the control group, the acupuncture group demonstrated significant differences in the following indicators: higher overall response rate (RR = 1.14, 95% CI 1.11– 1.18), and lower visual analog scale scores (SMD = − 1.19, 95% CI − 1.62 to − 0.76), frequency of pain episodes (SMD = − 1.31, 95% CI − 2.18 to − 0.44), adverse events (RR 0.28, 95% CI: 0.16– 0.50), and BPI−facial pain score (SMD = − 0.53, 95% CI − 0.96 to − 0.09) were reduced.
Conclusion: Acupuncture combined with medication may improve efficacy and reduce adverse events compared with monotherapy. However, the quality of existing evidence is low due to methodological limitations. Rigorous, multicenter randomized controlled trials with standardized protocols are needed to confirm the role of acupuncture for TN management.
Keywords: trigeminal neuralgia, acupuncture, efficacy, meta-analysis, pain, grade
Introduction
Trigeminal neuralgia (TN) is a disorder characterized by recurrent episodes of unilateral, electric shock-like pain within the distribution of the trigeminal nerve,1,2 with an overall prevalence of approximately 0.03% to 0.3%.3 The incidence rate in women is approximately twice that in men.4 Approximately 90% of cases occur after the age of 40, with the incidence gradually increasing with age.5 The frequency and intensity of TN attacks progressively worsen with disease progression, ultimately evolving into a chronic course,6 severely impairing patients’ quality of daily life.7 It frequently induces comorbid emotional disorders such as anxiety and depression,8 with their severity showing a significant positive correlation with pain scores and disease duration.9,10
Carbamazepine (CBZ) as a first-line treatment for TN provides some analgesic effect.11,12 However, it often leads to adverse reactions such as cognitive impairment, drowsiness, dizziness, gastrointestinal discomfort, and mood swings.13,14 Surgical interventions such as microvascular decompression (MVD), pulsed radiofrequency, gamma knife, and balloon compression may either preserve neural function through decompression or achieve pain relief by controllably disrupting trigeminal sensory function.15–17 However, these approaches carry risks of high recurrence rates, sensory deficits, and severe complications including hearing loss and intracranial hemorrhage.18–20 Against this backdrop, acupuncture—as a well-established non-pharmacological analgesic therapy—offers a new potential avenue for addressing this clinical challenge. Research indicates that acupuncture not only significantly reduces pain intensity and NRS scores in TN patients,21–23 decreases attack frequency24 but also lowers the risk of developing psychiatric disorders.25
Systematic synthesis of high-quality evidence for acupuncture in treating TN remains insufficient. Previous systematic reviews have been constrained by both methodological limitations (eg, narrow inclusion criteria focusing primarily on manual acupuncture) and incomplete outcome assessment (often excluding important endpoints like quality of life or long-term effects). Consequently, the existing evidence base has not been fully utilized to inform clinical practice. Although previous studies have suggested that acupuncture may have analgesic effects on TN, such as Hu et al indicating that acupuncture has some positive effects on PTN, the quality of evidence remains low;25 Yin et al found that multiple acupuncture techniques outperformed CBZ in alleviating pain, though the assessment metrics were relatively limited.23 Lin et al and Li et al both indicated that acupuncture demonstrated superior efficacy compared to CBZ. However, the types of controls included in these studies were limited, resulting in a narrow reference range.22,26 Recent methodological advancements have yielded an expanding body of high-quality randomized controlled trials (RCTs) investigating acupuncture for TN. While existing evidence suggests potential analgesic benefits, the recent availability of more rigorous RCTs—featuring improved blinding techniques, standardized pain assessment protocols, and longer-term follow-ups—necessitates an updated systematic evaluation. This study will employ the GRADE framework to conduct a comprehensive meta-analysis that specifically addresses three critical knowledge gaps: (1) quantifying the strength of evidence amidst heterogeneity in study methodologies, (2) determining the precision and consistency of therapeutic outcomes across different acupuncture modalities, and (3) evaluating comparative efficacy relative to first-line pharmacological treatments. By synthesizing this contemporary evidence base, our findings will provide clinicians and policymakers with a current, methodologically robust assessment of acupuncture’s therapeutic profile in TN management.
Methods
This study protocol is registered with PROSPERO (registration number: CRD420251269307). This systematic review was conducted according to the Cochrane Handbook and reported in accordance with the PRISMA 2020 statement (Appendix 1).27,28
Literature Search Strategy
We performed a systematic literature search across eight databases from their inception to December 19, 2025, with no restrictions on language: PubMed, the Cochrane Library, Embase, Web of Science, Wanfang Data, China National Knowledge Infrastructure (CNKI), Chinese Scientific Journal Database (VIP), and China Biomedical Literature Service System (SinoMed). The search strategy comprehensively employs Medical Subject Headings (MeSH) and free−text terms, covering acupuncture, TN, and RCTs. Additionally, studies potentially meeting the inclusion criteria were identified by tracing the references cited in the included studies and consulting subject matter experts. The specific search strategies for each database are detailed in eTable 1.
Inclusion and Exclusion Criteria
Inclusion Criteria
We included studies that met the following criteria:
- Study design: RCTs;
- Participants: Patients clinically diagnosed with TN, with no restrictions on age, gender, ethnicity, or disease duration;
- Interventions: The intervention for the experimental group consists of acupuncture therapy (including manual acupuncture (MA), electroacupuncture (EA), fire acupuncture (FA), acupuncture and moxibustion (AM), etc.), which may be combined with or without other therapies identical to those in the control group. Specific restrictions are not imposed on acupuncture techniques, point selection, or treatment duration. The control group may include patients receiving Western medication, those awaiting consultation, sham acupuncture/placebo acupuncture or other treatment modalities.
- Outcome measures:
- Visual Analogue Scale (VAS);
- Frequency of pain episodes;
- Response rate:
Cured: pain absent, normal facial sensorimotor function, no trigger point pain, no recurrence ≥1 month;
Markedly effective: pain reduced ≥50% in frequency or VAS, facial function basically normal, daily life unaffected;
Effective: pain reduced 25–50% in frequency or VAS, partial facial function improvement, occasional induced pain;
Ineffective: pain unchanged/worsened, reduction <25%, no functional improvement; Total response rate = (Cured + Markedly effective + Effective)/Total × 100%;
- Brief Pain Inventory (BPI);
- Incidence of adverse events (AEs).
Exclusion Criteria
This study excluded relevant literature based on the following criteria:
- Studies that could not be retrieved in full text after systematic searching;
- Research where key data cannot be obtained through means such as contacting the author;
- Non−RCTs, as well as non−clinical research types such as reviews, conference abstracts, and animal studies;
- For duplicated studies, only the version with the most complete data should be retained.
- Research that struggles to distinguish the individual effects of acupuncture from those of other medical combination therapies.
Research Screening and Data Extraction
Two reviewers independently conducted literature searches and screening based on the retrieval strategy. After importing the retrieved documents into EndNote X9 (Clarivate Analytics) and removing duplicate records, they first performed an initial screening based on titles and abstracts, followed by a further evaluation through reading the full texts. For studies meeting the inclusion criteria, both parties independently extracted relevant information, including authors, publication year, number of RCTs, sample size, intervention measures, outcome measures, risk assessment tools, adverse reactions, and conclusions, and recorded these using standardized forms. After extraction is complete, cross−check the data. Any discrepancies shall be resolved by a third reviewer.
Risk of Bias Assessment
This study employed the Cochrane risk of bias assessment tool ROB 2.0 to evaluate the methodological quality of the included RCTs. The assessment encompassed five domains: randomization process, deviation from the specified intervention, missing outcome data, outcome measurement, and selection of outcome reporting. Each area is classified as “low risk,” “some concerns,” or “high risk” based on the clarity and appropriateness of the method description and implementation. All assessments were conducted independently by two researchers. In cases of disagreement, a third researcher was consulted to facilitate discussion and reach a consensus.
Statistical Analysis Methods
This study employed Stata 17.0 (StataCorp LLC) for the meta−analysis. For binary outcomes, effect sizes are expressed as relative risk or odds ratio. For continuous outcomes, the mean difference is used when measurement tools are identical across studies; otherwise, the standardized mean difference is employed. All effect sizes are reported as point estimates with 95% confidence intervals.
Heterogeneity among studies was assessed using the I2 statistic and interpreted in conjunction with the P−value. If I2 < 50% and P > 0.1, indicating low heterogeneity, the analysis was performed using a fixed−effects model. If I2 ≥ 50% or P ≤ 0.1, indicating significant heterogeneity, then a random−effects model is used. Simultaneously, subgroup analyses will be conducted to explore sources of heterogeneity. When ≥10 studies are included for a specific outcome, funnel plots will be generated to assess potential publication bias. Additionally, sensitivity analyses will be conducted by sequentially excluding individual studies to assess the impact of each study on the stability of the pooled results. The significance level for all analyses is set at α=0.05.
Grading of Evidence Quality
We will use the GRADE approach to systematically assess the quality of evidence for each outcome measure. Evidence quality will be categorized into four levels: high, medium, low, or extremely low. The assessment process is based on consideration of the following five factors that may reduce the quality of evidence: risk of bias, inconsistency of results, indirect evidence, imprecise data, and publication bias. The initial quality of evidence from RCTs is rated as “high.” It is downgraded by one level if serious concerns exist, and by two levels if very serious concerns exist. The final GRADE assessment results and specific downgrade reasons will be summarized and presented in a table.
Results
Study Selection
Through systematic retrieval of eight databases, we initially obtained 937 literature records. After removing duplicate references using EndNote X9, 545 articles remained. Based on the titles and abstracts, an initial screening was conducted to exclude 400 papers that were clearly irrelevant to the topic. Ultimately, 145 full−text papers were obtained for further evaluation. During the full−text assessment phase, the following studies were excluded for failing to meet the inclusion criteria: 8 non−randomized controlled trial designs, 2 conference abstracts or unpublished reports, 30 studies lacking randomized procedures, 11 studies with inadequately defined control groups, 54 studies failing to clearly describe randomization methods, and 2 studies for which full−text access was unavailable. A total of 38 RCTs were ultimately included for data analysis. The specific literature screening process is shown in Figure 1.
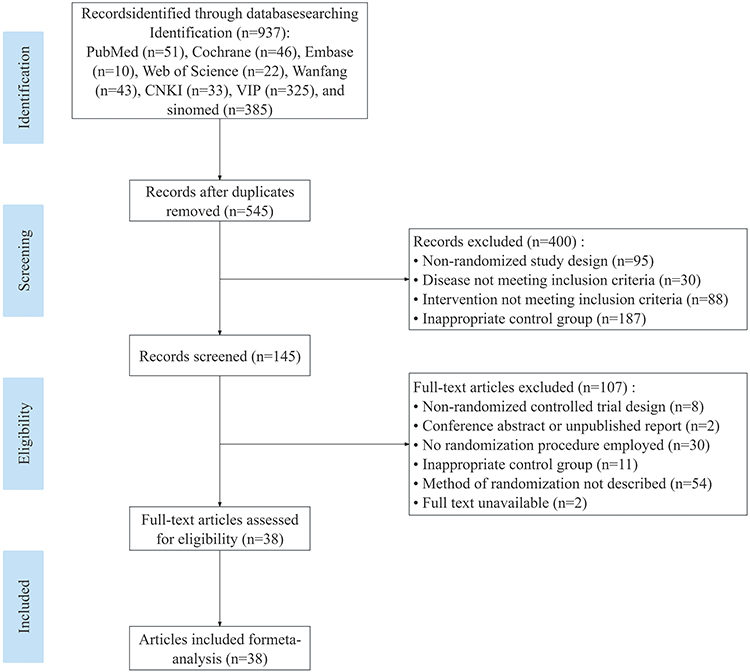 |
Figure 1 Experimental Selection Flowchart. |
Study Characteristics
This study included a total of 38 RCTs, of which 37 were published in Chinese and 1 in English.21,29–65 These studies, published between 2009 and 2024, involved a total of 2836 patients with TN. In studies reporting gender, 1196 participants were male and 1517 were female (two additional studies did not report gender). The age range of patients was broad, with a mean age of approximately 53.4 years (distribution range approximately 42 to 62 years). Treatment regimens ranged from 7 to 90 days. Regarding intervention methods, the acupuncture techniques employed in the experimental groups across 38 studies included: MA (28 studies), EA (7 studies), AM (2 studies), and FA (1 study). Fourteen studies reported AEs, with a cumulative total of 160 cases: 32 in the acupuncture group and 128 in the control group. The baseline characteristics of the included studies are detailed in Table 1.
 |
Table 1 Main Characteristics of Included RCTs |
Assessment of Methodological Quality
We assessed the risk of bias of the included RCTs using the RoB 2 tool. Of the 38 included studies, 34 studies (89.5%) were rated as having some concerns or high risk of bias for the randomization process, while only 4 studies (10.5%) met the criteria for low risk. Regarding deviations from intended interventions, only one study (2.6%) adequately documented blinding implementation and adherence and was rated as low risk. The remaining 37 studies (97.4%) were rated as having some concerns or high risk of bias. Regarding missing outcome data, the majority of studies (31/38, 81.6%) were rated as low risk due to low dropout rates or appropriate handling of missing data. However, 7 studies (18.4%) raised concerns because they failed to report dropout information and were rated as having some concerns. Regarding outcome measurement, only one study (2.6%) was rated as low risk due to the use of objective measurements or assessor blinding. The remaining 37 studies (97.4%) were rated as having some concerns or high risk of bias due to the use of subjective pain scales and unclear assessor blinding. Of the 38 studies, 37 studies (97.4%) with non−pre−registered protocols were judged to have some concerns for selective reporting, while one registered study was assessed as low risk. Overall, the included RCTs had notable methodological limitations, particularly in randomization, blinding, and selective reporting. Only a few trials were rated as having a low risk of bias. This raises concerns that the pooled effect estimate may be overestimated. Detailed risk of bias assessments are presented in Figures 2 and 3.
 |
Figure 2 Summary of risk of bias in included randomized controlled trials. |
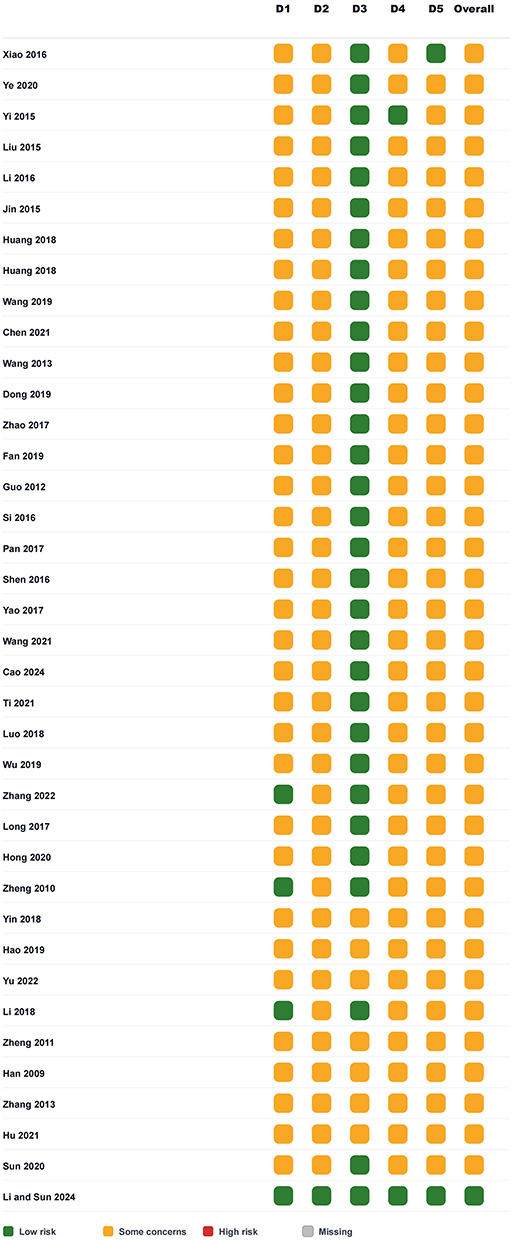 |
Figure 3 Risk of bias assessment for each included study. |
Meta−Analysis Results
Effective Rate
According to the results of a meta−analysis of thirty−five studies. The inclusion of acupuncture increased the overall treatment efficacy rate (RR = 1.14, 95% CI: 1.11–1.18, P < 0.001), with low heterogeneity among the included studies (I2 = 16.6%, P = 0.197) (Figure 4A). In comparisons of different acupuncture techniques, MA demonstrated positive effects (RR = 1.16, 95% CI: 1.12–1.19)(Figure 4B). Subgroup analysis further revealed that acupuncture in combination with CBZ (RR = 1.17, 95% CI: 1.06–1.29) and acupuncture combined with Traditional Chinese Medicine (TCM) (RR = 1.24, 95% CI: 1.11–1.37) both demonstrated higher efficacy rates compared to the respective monotherapies (Figure 4C and D). Sensitivity analyses conducted by sequentially excluding individual studies demonstrated that the pooled effect size remained stable and was not significantly influenced by any single study (eFigure 1).
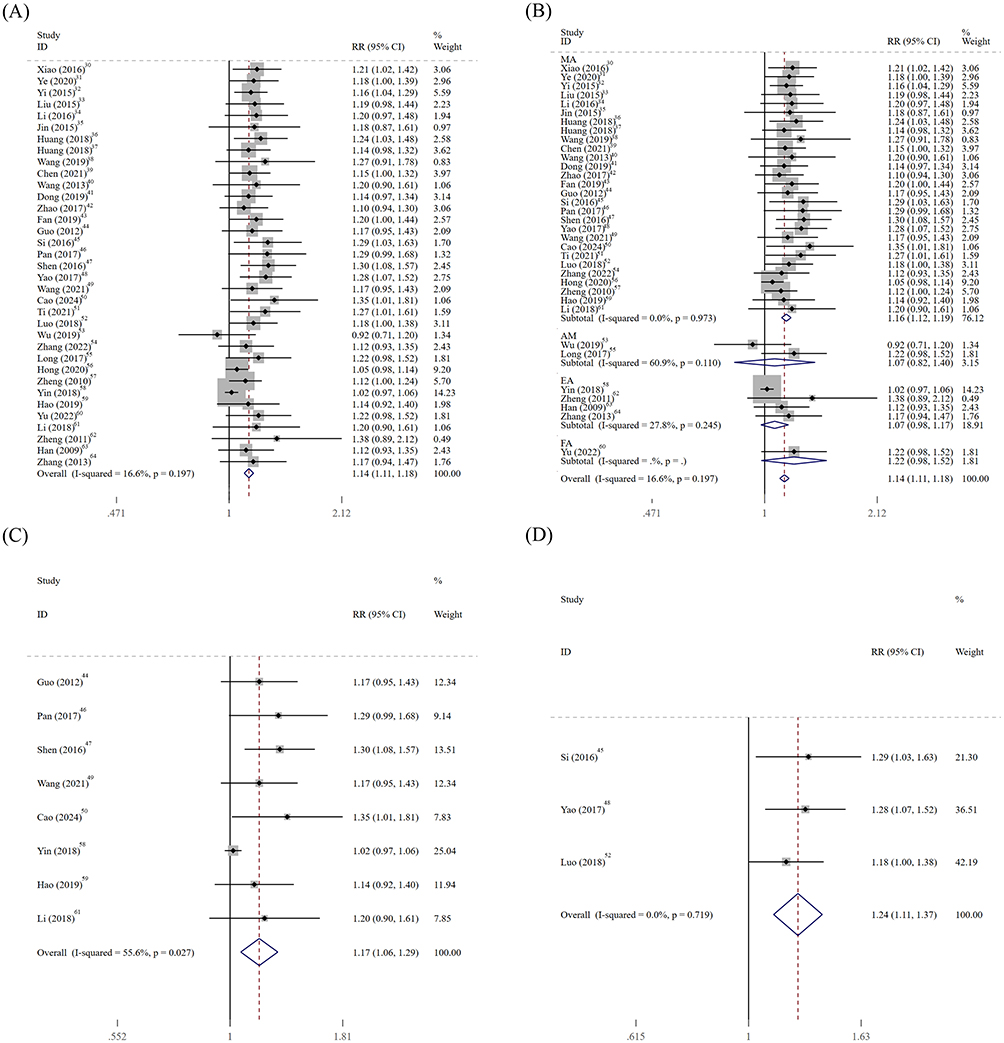 |
Figure 4 Forest plots for the experimental and control groups: Response rate. (A) Overall analysis; (B) Subgroup analysis by acupuncture method; (C) Acupuncture plus CBZ vs CBZ; (D) Acupuncture plus TCM vs TCM. Abbreviations: CBZ, carbamazepine; TCM, traditional Chinese Medicine; MA, manual acupuncture; AM, acupuncture and moxibustion; EA, electroacupuncture; FA, fire acupuncture; CI, confidence interval. |
VAS
Twenty−four studies reported changes in VAS among patients with TN treated with acupuncture. The pooled analysis showed that the VAS reduction in the acupuncture group was greater than that in the control group (SMD = −1.19, 95% CI: −1.62 to −0.76), but between-study heterogeneity was substantial (I2 = 93.6%, P < 0.001) (Figure 5A). Subgroup analysis revealed differences in efficacy among various acupuncture modalities: MA demonstrated significant effects (SMD = −1.22, 95% CI −1.61 to −0.82). Other methods yielded inconclusive results due to high inter−study heterogeneity or inconsistent findings (Figure 5B). Additionally, subgroup analyses of combined therapies revealed that acupuncture combined with TCM (SMD = −1.00, 95% CI −1.52 to −0.48) or in combination with CBZ (SMD = −0.75, 95% CI −1.41 to −0.08) demonstrated greater pain reduction compared to the respective monotherapies (Figure 5C and D).
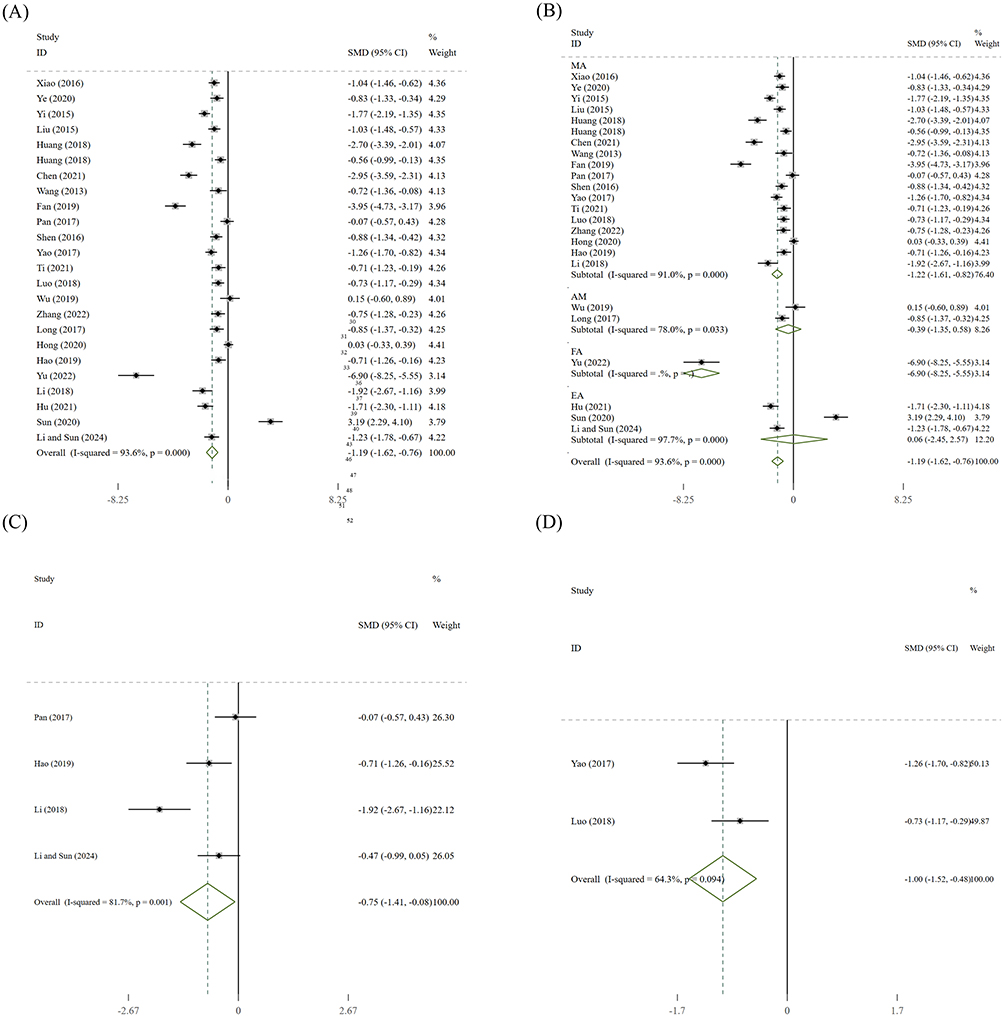 |
Figure 5 Forest plots for the experimental and control groups: Visual Analog Scale (VAS). (A) Overall analysis; (B) Subgroup analysis by acupuncture method; (C) Acupuncture plus CBZ vs CBZ; (D) Acupuncture plus TCM vs TCM. Abbreviations: CBZ, carbamazepine; TCM, traditional Chinese Medicine; MA, manual acupuncture; AM, acupuncture and moxibustion; EA, electroacupuncture; FA, fire acupuncture; CI, confidence interval. |
To explore potential sources of heterogeneity, further subgroup analyses were performed for direct comparison between MA and CBZ and by study year; however, heterogeneity was not reduced (eFigures 2 and 3). Sensitivity analyses showed that the pooled effect size remained stable around −1.19 when any single study was excluded, and no study reversed the direction or statistical significance of the effect (eFigure 4), suggesting that the results were robust.
Frequency of Pain Attacks
Seven studies reported changes in the frequency of pain episodes before and after treatment in patients with TN. Results showed that the acupuncture group had a significantly greater reduction in seizure frequency compared with the control group in reducing seizure frequency (SMD = −1.31,95% CI: −2.18 to −0.44, P< 0.05) (Figure 6). Sensitivity analysis indicated that the pooled result was stable, as the effect direction remained consistently negative after the sequential exclusion of any single study (eFigure 5).
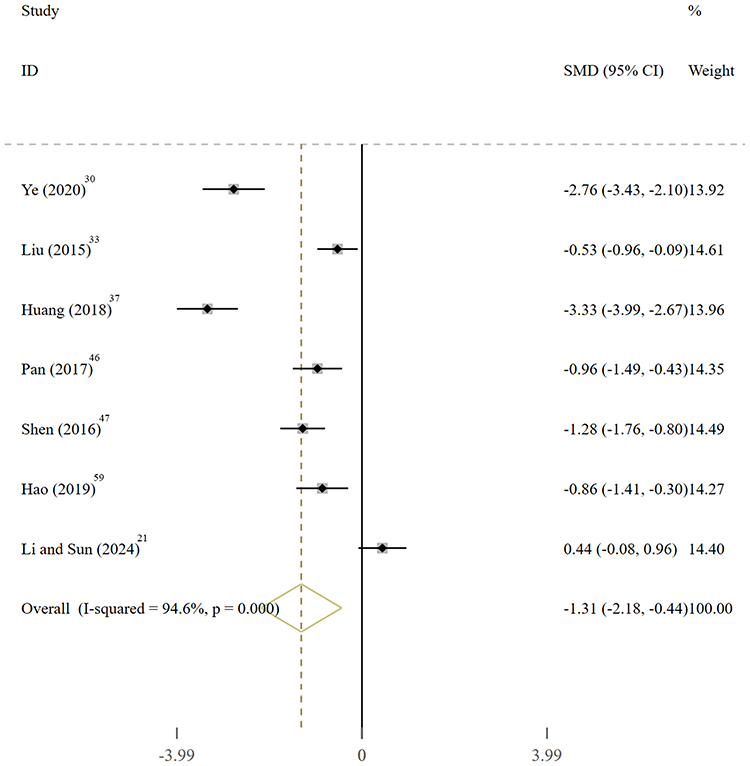 |
Figure 6 Forest plots for the experimental and control groups: Frequency of pain attacks. |
BPI
Three studies investigated the effect of acupuncture treatment on BPI scores for TN. Analysis revealed that the acupuncture group showed a significantly greater reduction in facial pain scores compared to the control group in reducing facial pain scores (SMD = −0.53, 95% CI: −0.96 to −0.09, p < 0.05) and low study heterogeneity (I2 = 46.3%, P = 0.155) (Figure 7A). Analysis of the BPI quality of life scores for acupuncture treatment of TN revealed very high heterogeneity (I2 = 97.0%, P = 0.000, SMD = −2.22, 95% CI: −4.55–0.12), which did not reach statistical significance (Figure 7B). Sensitivity analysis suggested that the BPI facial pain score result was robust, with confidence intervals remaining entirely below zero across all omitted studies (eFigure 6). Concurrently, the BPI quality of life score results was unstable; excluding studies with extreme effect sizes may reverse the direction of the pooled effect size, rendering the current evidence insufficient to support firm conclusions (eFigure 7).
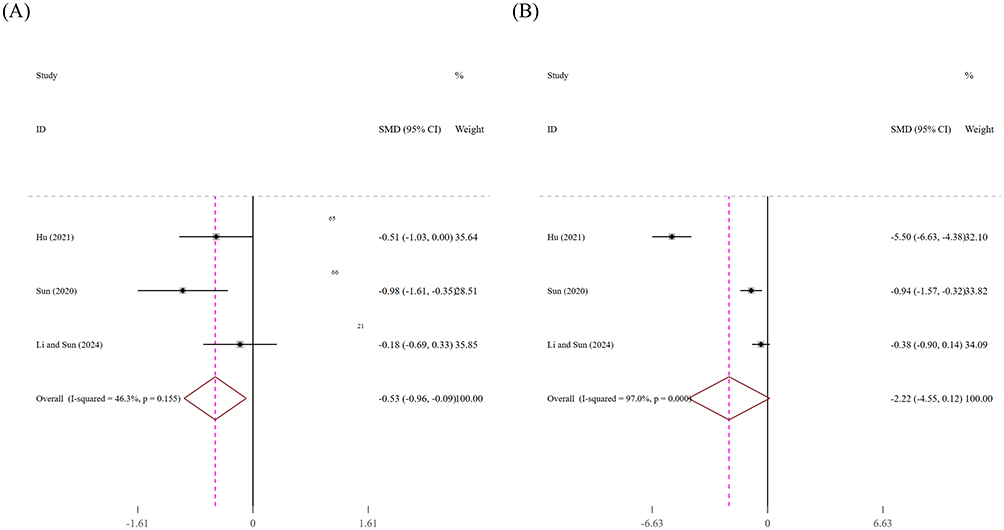 |
Figure 7 Forest plots for the experimental and control groups: Brief Pain Inventory (BPI). (A) Facial pain severity; (B) Pain interference with life. Abbreviation: CI, confidence interval. |
AEs
Thirteen of the studies included in the analysis reported treatment-related AEs. Analysis results indicate that the incidence of AEs in the acupuncture combination therapy group was significantly lower than that in the conventional drug control group primarily receiving CBZ (RR 0.28, 95% CI: 0.16–0.50) (Figure 8). However, given the known high incidence of AEs associated with CBZ, acupuncture is considered safer than drugs such as CBZ; however, this primarily reflects a comparative advantage. Acupuncture−related adverse reactions (9 cases) in 13 studies were predominantly mild, transient local symptoms (such as needle syncope) and neuropsychiatric reactions like drowsiness. In contrast, CBZ-related AEs (82 cases) were more common and relatively more severe, primarily including dizziness, abnormal liver function, rash or exfoliative dermatitis, as well as gastrointestinal symptoms such as nausea and vomiting. In the trials of MA in combination with CBZ, a total of 2 AEs were reported, primarily reflecting the combined effects of both treatment responses. This incidence rate was 71% lower than that observed with CBZ monotherapy; however, this downward trend should be interpreted with caution, as it may be partly attributable to the higher baseline incidence of AEs in the CBZ treatment group. It is worth noting that over one−third of the studies reported only the number of AEs without describing their specific manifestations, further highlighting the need for more comprehensive safety reporting. Detailed information on AEs between the acupuncture and control groups is presented in Table 2.
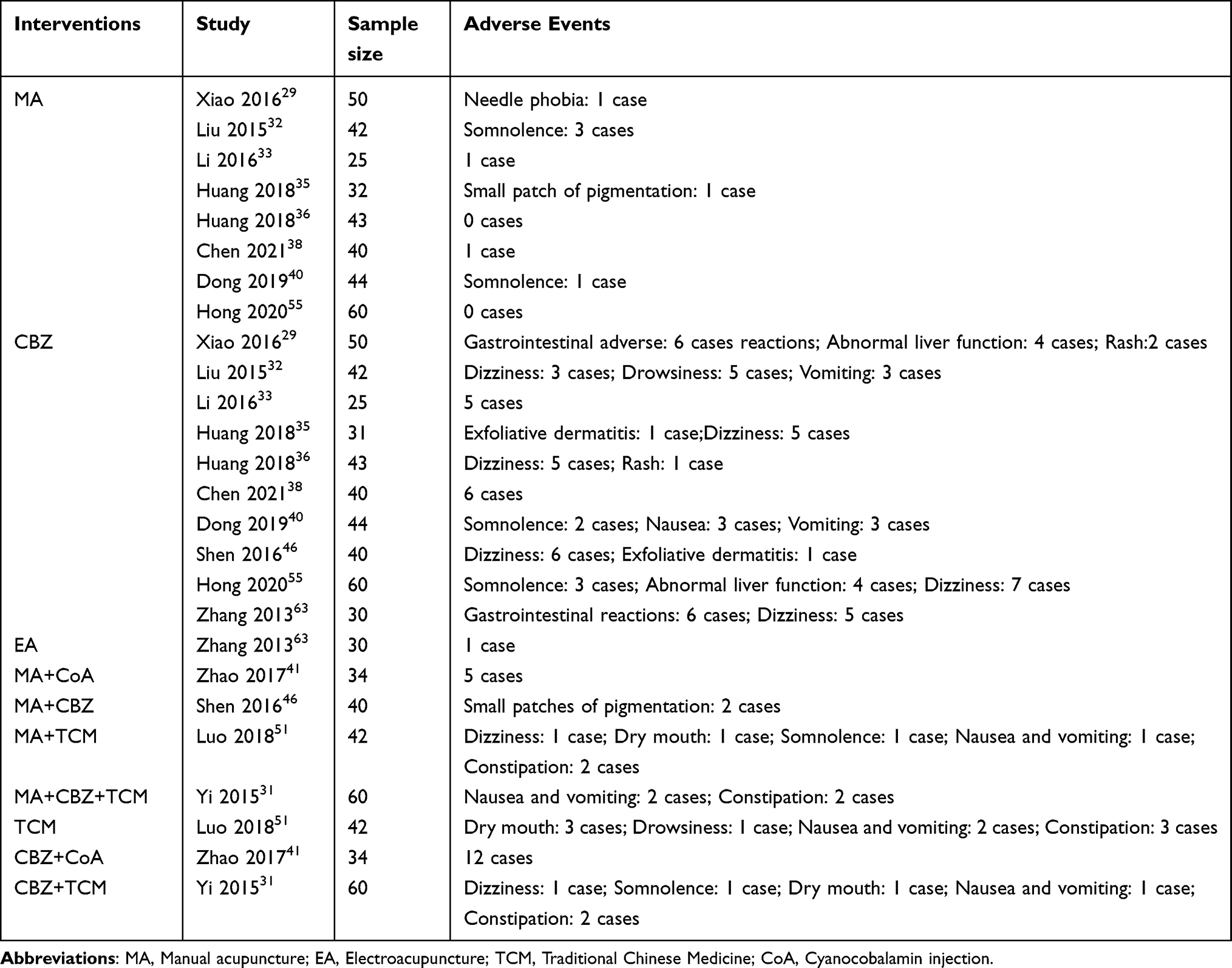 |
Table 2 Adverse Events in Included RCTs |
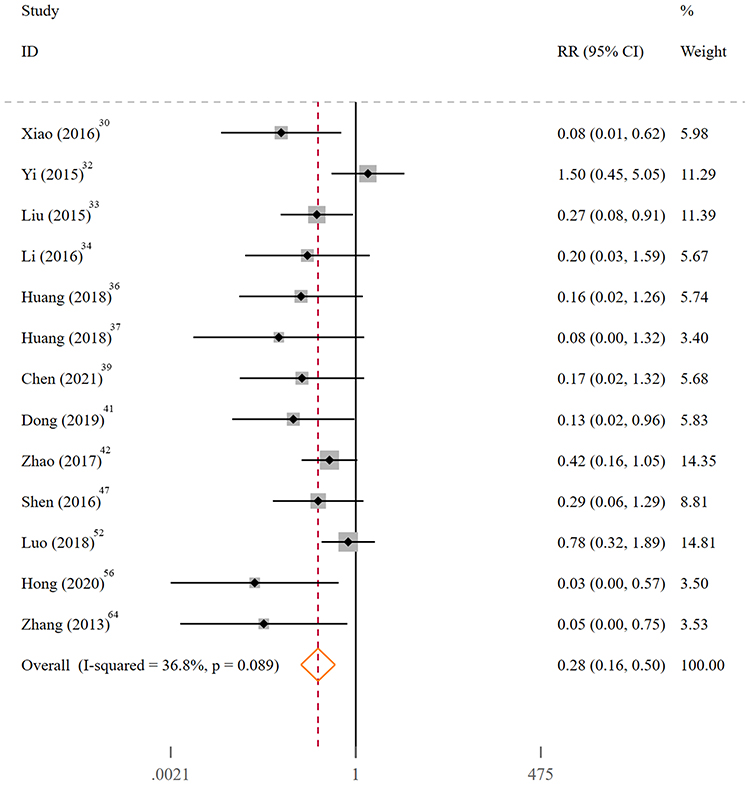 |
Figure 8 Forest plots for the experimental and control groups: adverse events(AEs). Abbreviation: CI, confidence interval. |
Publication Bias
Of the 38 included studies, 37 were published in Chinese, suggesting a risk of publication bias and possible positive selection bias. The Egger test revealed significant small-study effects for both response rate (intercept = 1.74, P < 0.001) and AEs (intercept = −2.59, P = 0.001), but in opposite directions; small studies tended to report greater efficacy and fewer AEs (eFigure 8). The Egger tests for VAS (P = 0.08), BPI quality of life (P = 0.074), BPI facial pain (P = 0.291), and frequency of pain attacks (P = 0.060) were all non-significant. Funnel plots were constructed for outcomes with more than four studies (response rate, VAS, AEs, and frequency of pain attacks). The data points were asymmetrically distributed (eFigure 9), suggesting possible publication bias. Given the small number of studies and limited statistical power, a non-significant Egger’s test does not rule out bias. In summary, publication bias cannot be ruled out, and this bias may result in overestimated efficacy and underestimated adverse event rates.
GRADE Assessment
Direct and indirect evidence was compared using the GRADE approach. The quality of outcome measures ranged from very low to moderate. However, most evidence was rated as very low certainty evidence (Table 3), primarily due to risk of bias, inconsistency, and imprecision.
 |
Table 3 GRADE Summary of Findings |
Discussion
This systematic review offers several novel contributions through its comprehensive integration of recently published evidence. Our study includes 38 RCTs up to December 2025, involving a total of 2836 patients. Notably, the study’s methodological rigor is evidenced by its preregisteration on PROSPERO and strict adherence to PRISMA guidelines. The multidimensions treatment outcomes have been analyzed in this study, including efficacy rates, pain intensity, attack frequency, and safety profile, complemented by comprehensive subgroup analyses, sensitivity testing, and GRADE evidence grading. Quantitative analysis further shows that acupuncture is more effective than CBZ in reducing AEs. However, due to certain methodological limitations, the quality of the evidence is relatively low; therefore, the results should be interpreted with caution.
In terms of therapeutic efficacy, the evidence suggests the effectiveness of acupuncture. First, acupuncture increased the overall treatment response rate (RR = 1.14). Subgroup analysis further revealed that acupuncture combined with either CBZ or TCM demonstrated higher efficacy compared to monotherapy with the respective drugs. Second, acupuncture was associated with a reduction in pain intensity (VAS, SMD = −1.19) and a decrease in the frequency of pain episodes (SMD = −1.31). MA has demonstrated positive effects across all core efficacy indicators, and it was the most frequently evaluated acupuncture modality in the included studies. Additionally, acupuncture was associated with an improvement in the BPI facial pain score.
In terms of safety, the combined treatment regimen incorporating acupuncture was associated with a lower reported overall incidence of AEs compared to the conventional drug therapy group primarily using CBZ. Specifically, adverse reactions directly related to acupuncture itself (such as mild dizziness or localized discomfort) occurred infrequently, are mild in severity, and are often transient. In contrast, monotherapy with CBZ is frequently associated with relatively more common and severe adverse reactions, including dizziness, abnormal liver function, rash, and gastrointestinal symptoms. Notably, when acupuncture is in combination with CBZ, it may be associated with improved efficacy and a lower risk of AEs associated with the latter. Although acupuncture combined with medication may offer potential advantages over monotherapy, the current evidence is of low quality and should be interpreted with caution. Future research urgently needs to employ standardized and rigorous RCTs to further validate the clinical utility of acupuncture in the management of TN.
TN is a neuropathic pain syndrome characterized by sudden, severe, and brief episodes of pain on one side of the face.66 This type of pain not only frequently leads to functional disability and a significant decline in quality of life,67 but also imposes a substantial disease burden. Epidemiological data indicate that its incidence rate can reach 25.33 per 100,000 person−years, with a global annual prevalence of 45.38 per 100,000 and a lifetime prevalence as high as 108.43 per 100,000.68 Correspondingly, TN patients exhibit a significantly elevated risk of sleep disorders, depression, and anxiety, with over one−third exhibiting suicidal tendencies, which are closely correlated with pain intensity.69,70
In response to this clinical challenge, conventional drugs such as CBZ primarily exert their therapeutic effects by acting on sodium channels,71,72 representing a relatively singular mode of action. This study reveals that acupuncture treatment for TN may exert its effects through a multi−target, multi−pathway integrated regulatory mechanism, offering new insights for therapeutic approaches. Current understanding suggests that the pathogenesis of TN involves neurovascular compression, voltage−gated sodium/potassium channel dysfunction, and abnormal restructuring of brain structural and functional connectivity.73–77 It is a multifaceted disorder encompassing peripheral and central sensitization pathways.
In response to this complexity, acupuncture achieves synchronized regulation across multiple systems. At the central level, it not only promotes the release of endogenous opioids, modulates neurotransmitters such as 5−HT and NE, and activates descending inhibitory pathways to directly suppress pain transmission,78,79 but also suppresses neuroinflammation and central sensitization by regulating signaling pathways such as TLR4/NF−κB.80,81 Additionally, acupuncture helps remodel abnormal functional connectivity in brain regions such as the anterior cingulate cortex and insula, thereby reversing pain-related neuroplasticity changes.82,83 At the peripheral level, acupuncture improves the microenvironment at the injury site by increasing local blood flow, clearing inflammatory mediators, and promoting adenosine release. This reduces peripheral sensitization, thereby achieving comprehensive relief of facial pain.84,85
A UK study on TN showed that acupuncture had a slightly higher treatment efficacy rate (86.5%) than MVD (79.3%) and CBZ (71.7%). Among the three treatments, acupuncture also had the lowest side effect incidence (22.7%) and the lowest psychological distress score (53 points). A long-term cost analysis indicated that acupuncture became the most cost-effective option at 65 weeks of treatment, with a total cost of approximately £750 over five years—half that of CBZ and significantly lower than surgery.86 A study by Zhao et al on neuropathic pain, including one three-arm trial and 15 two-arm trials, found that the total weekly treatment costs (including direct and indirect costs) in descending order were as follows: EA (¥1160.60), AM (¥789.95), MA (¥687.18), FA (¥547.75), antiepileptic drugs (¥140.39), and nonsteroidal anti-inflammatory drugs (NSAIDs)(¥100.63).87 Overall, acupuncture may slightly increase short-term direct medical costs for TN. However, it can shorten illness duration, reduce cumulative costs from long-term medication and frequent clinic visits, and decrease reliance on analgesics and psychological well-being.88 Currently, there is a lack of comparative studies on the time of pain relief among different acupuncture modalities, which is a key area for future research.
Unlike previous reviews that primarily compared different single acupuncture therapies, this study focuses on systematically integrating evidence for the combined treatment of acupuncture with conventional medication. This approach further helps clarify its potential value in achieving synergistic clinical effects. From a clinical practice perspective, this value is notable. Evidence indicates that incorporating acupuncture as an adjunct therapy to CBZ or TCM not only enhances treatment efficacy but also reduces the risk of adverse reactions associated with drug therapy alone. Therefore, this combined strategy offers a potential complementary treatment option for TN patients who are intolerant to drug side effects or experience poor therapeutic response.
However, this study also has certain limitations: the methodological quality of the included studies was generally low, with deficiencies in random allocation concealment, implementation of blinding, and reporting. For example, only 4 out of 38 studies adequately described the randomisation process. Due to the lack of pain biomarkers, pain assessment in the included studies relied heavily on non‑blinded subjective outcome measures (eg, VAS score, response rate), which likely led to overestimation of the pooled estimates. In addition, many Chinese clinical trials used unvalidated or study‑specific criteria, and the definition of “response rate” varied across studies, introducing indirectness and bias. The quality of evidence for most outcomes was rated as “low” or “very low,” with insufficient or uncertain evidence for some outcomes and a lack of long−term efficacy assessments. Furthermore, the safety reports are insufficiently comprehensive, and the predominance of Chinese literature may introduce language bias. Therefore, although acupuncture combined with medication shows potential advantages over monotherapy, the strength of the current evidence is limited, and the findings should be interpreted with caution.
Conclusion
Acupuncture combined with medication may improve efficacy and reduce adverse events compared to medication alone for TN, but these findings should be interpreted with caution due to the low certainty of evidence. To translate these findings into clinical practice, future rigorously designed, multicenter RCTs must employ standardized acupuncture protocols, blinded outcome assessment, and longer-term follow-up. Until such evidence is available, clinicians should weigh these potential benefits against the limitations cautiously.
Declaration Section
This study protocol is registered with PROSPERO (registration number: CRD420251269307).
Data Sharing Statement
The data used and/or analyzed in this study may be obtained upon reasonable request to the corresponding author, Rongrong Li.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work will be supported by the Zhejiang Traditional Chinese Medicine Inheritance and Innovation Talent Support Program (2023ZR031) and Young Elite Scientists Sponsorship Program by ZAST.
Disclosure
The author declares that the research, writing, and/or publication of this paper did not receive any financial support.
References
1. Zakrzewska JM, Linskey ME. Trigeminal neuralgia. BMJ. 2015;350:h1238. doi:10.1136/bmj.h1238
2. Araya EI, Claudino RF, Piovesan EJ, Chichorro JG. Trigeminal neuralgia: basic and clinical aspects. Curr Neuropharmacol. 2020;18(2):109–22. doi:10.2174/1570159X17666191010094350
3. De Toledo IP, Conti Réus J, Fernandes M, et al. Prevalence of trigeminal neuralgia: a systematic review. J Am Dent Assoc. 2016;147(7):571–576.e2. doi:10.1016/j.adaj.2016.02.014
4. Mueller D, Obermann M, Yoon MS, et al. Prevalence of trigeminal neuralgia and persistent idiopathic facial pain: a population-based study. Cephalalgia Int J Headache. 2011;31(15):1542–1548. doi:10.1177/0333102411424619
5. Rozen TD. Trigeminal neuralgia and glossopharyngeal neuralgia. Neurol Clin. 2004;22(1):185–206. doi:10.1016/S0733-8619(03)00094-X
6. Loving BA, Oyeniyi JF, Ramanathan S, et al. Outcomes and predictive factors after second stereotactic radiosurgery for refractory trigeminal neuralgia. Clin Transl Radiat Oncol. 2025;53:100969. doi:10.1016/j.ctro.2025.100969
7. Zakrzewska JM, Wu J, Mon-Williams M, Phillips N, Pavitt SH. Evaluating the impact of trigeminal neuralgia. Pain. 2017;158(6):1166–1174. doi:10.1097/j.pain.0000000000000853
8. Wu TH, Hu LY, Lu T, et al. Risk of psychiatric disorders following trigeminal neuralgia: a nationwide population-based retrospective cohort study. J Headache Pain. 2015;16:64. doi:10.1186/s10194-015-0548-y
9. Chang B, Zhu W, Li S. Effects of depression and anxiety on microvascular decompression outcome for trigeminal neuralgia patients. World Neurosurg. 2019;128:e556–e561. doi:10.1016/j.wneu.2019.04.194
10. Cheng J, Long J, Hui X, Lei D, Zhang H. Effects of microvascular decompression on depression and anxiety in trigeminal neuralgia: a prospective cohort study focused on risk factors and prognosis. Clin Neurol Neurosurg. 2017;161:59–64. doi:10.1016/j.clineuro.2017.08.011
11. Ruscheweyh R, Gierthmühlen J, Hedderich DM, Goßrau G, Leis S. [Trigeminal neuralgia: drug therapy: the new German guideline]. Schmerz. 2024;38(4):283–292. German. doi:10.1007/s00482-024-00810-4
12. Allam AK, Sharma H, Larkin MB, Viswanathan A. Trigeminal neuralgia: diagnosis and treatment. Neurol Clin. 2023;41(1):107–121. doi:10.1016/j.ncl.2022.09.001
13. Snel BJ, Cohen SP, Erdine S, et al. 13. Trigeminal neuralgia. Pain Pract. 2025;25(5):e70051. doi:10.1111/papr.70051
14. Di Stefano G, La Cesa S, Truini A, Cruccu G. Natural history and outcome of 200 outpatients with classical trigeminal neuralgia treated with carbamazepine or oxcarbazepine in a tertiary centre for neuropathic pain. J Headache Pain. 2014;15(1):34. doi:10.1186/1129-2377-15-34
15. Ahmadi R, Tronnier VM. [surgical treatment of trigeminal pain]. Der Schmerz. 2024;38(6):441–448. German. doi:10.1007/s00482-024-00835-9
16. Di Carlo DT, Benedetto N, Marani W, Montemurro N, Perrini P. Microvascular decompression for trigeminal neuralgia due to vertebrobasilar artery compression: a systematic review and meta-analysis. Neurosurg Rev. 2022;45(1):285–294. doi:10.1007/s10143-021-01606-1
17. Akdag H, Comert D, Akdur K, Sakarcan A, Seyithanoglu H, Hatiboglu MA. The efficacy of gamma knife radiosurgery in patients with trigeminal neuralgia: the initial experience of the bezmialem vakif university. Neurol India. 2019;67(2):476–480. doi:10.4103/0028-3886.258009
18. Xia L, Zhong J, Zhu J, et al. Effectiveness and safety of microvascular decompression surgery for treatment of trigeminal neuralgia: a systematic review. J Craniofac Surg. 2014;25(4):1413–1417. doi:10.1097/SCS.0000000000000984
19. Guo S, Chao ST, Reuther AM, Barnett GH, Suh JH. Review of the treatment of trigeminal neuralgia with gamma knife radiosurgery. Stereotact Funct Neurosurg. 2008;86(3):135–146. doi:10.1159/000120425
20. Eskandar E, Kumar H, Boini A, et al. The role of radiofrequency ablation in the treatment of trigeminal neuralgia: a narrative review. Cureus. 2023;15(3):e36193. doi:10.7759/cureus.36193
21. Li R, Sun J, Luo K, et al. Electroacupuncture and carbamazepine for patients with trigeminal neuralgia: a randomized,controlled,2 × 2 factorial trial. J Neurol. 2024;271(8):5122–5136. doi:10.1007/s00415-024-12433-x
22. Wei L, Han H, Meng J, Li X, Yao QP. Meta-analysis and sequential analysis of acupuncture compared to carbamazepine in the treatment of trigeminal neuralgia. World J Clin Cases. 2024;12(22):5083–5093. doi:10.12998/wjcc.v12.i22.5083
23. Yin Z, Wang F, Sun M, Zhao L, Liang F. Acupuncture methods for primary trigeminal neuralgia: a systematic review and network meta-analysis of randomized controlled trials. Evid-Based Complement Altern Med. 2022;2022:3178154. doi:10.1155/2022/3178154
24. Liu Y, Wang D, Li S, et al. Treatment of trigeminal neuralgia by acupuncture combined with Chinese medicine from the perspective of modern medicine: a review. Medicine. 2024;103(44):e40318. doi:10.1097/MD.0000000000040318
25. Liao CC, Lin CL, Liao KR, Li JM. Long-term beneficial effects of acupuncture with reduced risk of depression development following trigeminal neuralgia: a nationwide population-based cohort study. Neuropsychiatr Dis Treat. 2020;16:2961–2973. doi:10.2147/NDT.S284857
26. Ang L, Kim HJ, Heo JW, et al. Acupuncture for the treatment of trigeminal neuralgia: a systematic review and meta-analysis. Complement Ther Clin Pract. 2023;52:101763. doi:10.1016/j.ctcp.2023.101763
27. Cochrane handbook for systematic reviews of interventions | cochrane. Available from: https://www.cochrane.org/authors/handbooks-and-manuals/handbook.
28. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n7
29. Xiao F, Xu SZ. Clinical study on Zhuyu Huoluo acupuncture treatment of primary trigeminal neuralgia. China J Chin Med. 2016;31(6):918–921. doi:10.16368/j.issn.1674-8999.2016.06.257
30. Ye QQ. Effect of traditional chinese medicine acupuncture on relieving pain in clinical treatment of primary trigeminal neuralgia. Diet Health. 2020;39:87.
31. Yi JK, Tang ZZ, Ren GS. Clinical value of traditional Chinese medicine combined with acupuncture for treating recurrent trigeminal neuralgia. J Clin Acupunct Moxibust. 2015;31(7):23–26.
32. Liu K. Trigeminal neuralgia parallel randomized controlled study of acupuncture treatment. J Pract Trad Chin Internal Med. 2015;29(6):139–140. doi:10.13729/j.issn.1671-7813.2015.06.63
33. Li KX. Clinical value of acupuncture in the treatment of primary trigeminal neuralgia. Nei Mongol J Trad Chin Med. 2016;35(11):120. doi:10.16040/j.cnki.cn15-1101.2016.11.115
34. Jin ZC, Liu F, Fan X. Clinical efficacy observation on primary trigeminal neuralgia treated with combination of acupuncture with Chinese medicine. J Liaoning Univ Traditional Chin Med. 2015;17(3):92–94. doi:10.13194/j.issn.1673-842x.2015.03.032
35. Huang S. Clinical observation on acupuncture treatment of primary trigeminal neuralgia. Trad Chin Med Rehabilit. 2018;9(10):19–20.
36. Huang FH, Lin LC. Clinical experience of acupuncture treatment of trigeminal neuralgia. Biped Health. 2018;27(19):1–2. doi:10.19589/j.cnki.issn1004-6569.2018.19.001
37. Wang Y. Clinical observation on 30 cases of primary trigeminal neuralgia treated with acupuncture. Yunnan J Trad Chin Med Mater Med. 2019;40(7):94–95.
38. Chen H, He K. Clinical observation on acupuncture for primary trigeminal neuralgia. J Pract Trad Chin Med. 2021;37(3):468–469.
39. Wang LF, Huang LP, Luo Q, Wang X, Chen K. Clinical efficacy observation on primary trigeminal neuralgia with acupuncture. J Clin Acupunct Moxibust. 2013;29(7):28–30.
40. Dong XF. Therapeutic effect of acupuncture on trigeminal neuralgia. Smart Healthc. 2019;5(25):94–95. doi:10.19335/j.cnki.2096-1219.2019.25.040
41. Zhao M, Liu TJ, Li XM. Acupuncture treatment of Qi stagnation and blood stasis type of trigeminal nerve pain. Shaanxi J Trad Chin Med. 2017;38(5):665–667. doi:10.3969/j.issn.1000-7369.2017.05.055
42. Fan SJ. Clinical observation on acupuncture-moxibustion as adjuvant therapy for trigeminal neuralgia in 38 cases. Forum Trad Chin Med. 2019;34(2):41. doi:10.13913/j.cnki.41-1110/r.2019.02.019
43. Guo CH. Acupuncture assisted carbamazepine and doxepin in the treatment of trigeminal neuralgia comparative study. J Pract Trad Chin Internal Med. 2012;26(15):91–92.
44. Si YP. Analysis on the clinical effect of acupuncture combined with medicine in the treatment of primary trigeminal neuralgia. Guangming J Chin Med. 2016;31(11):1615–1617. doi:10.3969/j.issn.1003-8914.2016.11.045
45. Pan ZQ, Fu RY, Lin WM. Clinical study on mind-regulating acupuncture in treating primary trigeminal neuralgia. Shanghai J Acupuncture Moxibustion. 2017;36(9):1069–1073. doi:10.13460/j.issn.1005-0957.2017.09.1069
46. Shen QY. Clinical observation of acupuncture combined with carbamazepine tablets for primary trigeminal neuralgia in 40 cases. Trad Chin Med Res. 2016;29(9):63–65. doi:10.3969/j.issn.1001-6910.2016.09.30
47. Yao FL, Wu JX. Clinical observation of acupuncture combined with Sanfeng Jiejing Formula for primary trigeminal neuralgia. Shaanxi J Trad Chin Med. 2017;38(8):1137–1138. doi:10.3969/j.issn.1000-7369.2017.08.072
48. Wang ZC. Clinical observation on acupuncture combined with carbamazepine in the treatment of trigeminal neuralgia. Chin Med Moder Distance Educ China. 2021;19(11):139–141. doi:10.3969/j.issn.1672-2779.2021.11.052
49. Cao WT. Curative effect of acupuncture at yifeng and xiaguan points on trigeminal neuralgia and influence on pain degree. Smart Healthc. 2024;10(19):74–76. doi:10.19335/j.cnki.2096-1219.2024.19.024
50. Ti YC. Clinical observation on acupuncture for trigeminal neuralgia. Shaanxi J Trad Chin Med. 2021;37(2):32–33. doi:10.3969/j.issn.1000-7156.2021.02.013
51. Luo FQ, Guo XW, Zhang J, Wang SP, Ye L. Analysis of the application of acupoint acupuncture therapy on recurrent trigeminal neuralgia accompanied by anxiety and depression patients. Chin J Gen Pract. 2018;16(8):1361–1363. doi:10.16766/j.cnki.issn.1674-4152.000372
52. Wu JL, Yang H, Mi Y, Song Y, Wang R. Clinical study on warm acupuncture at Xiaguan (ST7) for primary trigeminal neuralgia. Xinjiang J Trad Chin Me. 2019;37(3):34–36.
53. Zhang WW, Tian SY, Tang TT, Li YX. Chicken-claw needling at Xiaguan (ST 7) combined with intradermal needling on negative emotions in primary trigeminal neuralgia of phlegm obstruction and blood stasis: a randomized controlled trial. Chin Acupunct Moxibus. 2022;42(9):999–1003. doi:10.13703/j.0255-2930.20220314-0004
54. Long QM, Huang CH, Gan YT, Wei RP, Du Y. Clinical observation on Shu-acupuncture combined with warm acupuncture for primary trigeminal neuralgia. J Guangxi Univ Chin Med. 2017;20(3):11–13.
55. Hong YB. Clinical observation on liver-soothing and fire-purging acupuncture for primary trigeminal neuralgia of liver-stomach stagnant heat pattern. Acta Chin Med. 2020;35(S1):11.
56. Zheng SH, Wu YJ, Jiao JK, Wei LL, Ren R, Cui X. Clinical study of puncturing point Renyin deeply for trigeminal neuralgia. J Hunan Univ Chin Med. 2010;30(5):71–72. doi:10.3969/j.issn.1674-070X.2010.05.023.070.03
57. Yin YH, Zhou HM. Carbamazepine combining high frequency electroacupuncture therapy for trigeminal neuralgia and its effects on patients’ pain relief and life quality. Int Med Health Guid News. 2018;24(12):1806–1808. doi:10.3760/cma.j.issn.1007-1245.2018.12.016
58. Hao WB, Li YF, Gong SY. Clinical observation on carbamazepine combined with acupuncture for primary trigeminal neuralgia. J Pract Trad Chin Med. 2019;35(2):209–210.
59. Yu T. Clinical control study on filiform fire needle combined with Fuzheng Yangyin decoction in the treatment of trigeminal neuralgia. Chin Med Moder Distance Educ China. 2022;20(22):111–113. doi:10.3969/j.issn.1672-2779.2022.22.041
60. Li YX, Bai ZY, Shao XQ, Liu X. Adjuvant therapies of Co-Q10 and acupuncture in the treatment of TN: comparative analysis on clinical efficacy, oxidative stress, and mitochondrial respiratory proteins. Inform Trad Chin Med. 2018;35(6):62–67. doi:10.19656/j.cnki.1002-2406.180180
61. Zheng JQ, Shi JP. Therapeutic effect of electro-acupuncture on primary trigeminal neuralgia observation. Inner Mongolia J Trad Chin Med. 2011;30(1):62–64. doi:10.3969/j.issn.1006-0979.2011.01.060
62. Han QZ. Clinical observation on electroacupuncture for primary trigeminal neuralgia in 30 cases. J Trad Chin Med Pharm. 2009;15(9):35. doi:10.3969/j.issn.1672-951X.2009.09.020
63. Zhang C. Analysis on curative effect of electric head acupuncture therapy of primary trigeminal neuralgia. Liaoning J Trad Chin Med. 2013;40(6):1214–1215. doi:10.13192/j.ljtcm.2013.06.164.zhangc.050
64. Hu YH, Dong P, Feng XX, Li WW, Wang C. Clinical study of electroacupuncture combined with repetitive transcranial magnetic stimulation in the treatment of primary trigeminal neuralgia. Chin J Geriatr Dent. 2021;19(6):325–330. doi:10.19749/j.cn.cjgd.1672-2973.2021.06.002
65. Sun J, Li RR, Li XY, et al. Therapeutic Observation of Cluster Superficial Needling Combined with Electroacupuncture for Trigeminal Neuralgia. Shanghai J Acupuncture Moxibustion. 2020;39(4):456–461. doi:10.13460/j.issn.1005-0957.2020.04.0456
66. DosSantos MFH, Ramos LR, Bonacchi L, et al. Subcortical neuroimaging signature of painful disorders of the trigeminal nerve: a UK biobank study. J Headache Pain. 2026;27(1):40. doi:10.1186/s10194-026-02271-9
67. Schuster NM, Argoff CE, Barad MJ, et al. Debunking myths in facial pain diagnosis for the pain practitioner. Reg Anesth Pain Med. 2026:rapm–2025–107382. doi:10.1136/rapm-2025-107382
68. Jeong YD, Jo Y, Son Y, et al. Global incidence and prevalence of trigeminal neuralgia, 1945–2024: a systematic review and meta-regression analysis. J Clin Neurol. 2026;22(1):102–112. doi:10.3988/jcn.2025.0433
69. Fishbein NS, Bakhshaie J, Greenberg J. Suicidal ideation and self-injury in trigeminal neuralgia. J Pain Res. 2025;18:2003–2010. doi:10.2147/JPR.S493649
70. Martinelli R, Vannuccini S, Burattini B, et al. Psychological assessment in patients affected by trigeminal neuralgia. A systematic review. Neurosurg Rev. 2025;48(1):414. doi:10.1007/s10143-025-03556-4
71. Siqueira SRDT, Alves B, Malpartida HMG, Teixeira MJ, Siqueira JTT. Abnormal expression of voltage-gated sodium channels Nav1.7, Nav1.3 and Nav1.8 in trigeminal neuralgia. Neuroscience. 2009;164(2):573–577. doi:10.1016/j.neuroscience.2009.08.037
72. Di Stefano G, De Stefano G, Leone C, et al. Real-world effectiveness and tolerability of carbamazepine and oxcarbazepine in 354 patients with trigeminal neuralgia. Eur J Pain. 2021;25(5):1064–1071. doi:10.1002/ejp.1727
73. Hilton DA, Love S, Gradidge T, Coakham HB. Pathological findings associated with trigeminal neuralgia caused by vascular compression. Neurosurgery. 1994;35(2):299–303;discussion303. doi:10.1227/00006123-199408000-00017
74. Xu W, Zhang J, Wang Y, Wang L, Wang X. Changes in the expression of voltage-gated sodium channels Nav1.3, Nav1.7, Nav1.8, and Nav1.9 in rat trigeminal ganglia following chronic constriction injury. Neuroreport. 2016;27(12):929–934. doi:10.1097/WNR.0000000000000632
75. Costa GMF, Rocha LPC, de Siqueira SRDT, Moreira PR, Almeida-Leite CM. No association of polymorphisms in Nav1.7 or nerve growth factor receptor genes with trigeminal neuralgia. Pain Med. 2019;20(7):1362–1369. doi:10.1093/pm/pny191
76. Wang Y, Cao DY, Remeniuk B, Krimmel S, Seminowicz DA, Zhang M. Altered brain structure and function associated with sensory and affective components of classic trigeminal neuralgia. Pain. 2017;158(8):1561–1570. doi:10.1097/j.pain.0000000000000951
77. Zhang Y, Mao Z, Pan L, et al. Frequency-specific alterations in cortical rhythms and functional connectivity in trigeminal neuralgia. Brain Imaging Behav. 2019;13(6):1497–1509. doi:10.1007/s11682-019-00105-8
78. Shi JT, Cao WY, Zhang XN, et al. Local analgesia of electroacupuncture is mediated by the recruitment of neutrophils and released β-endorphins. Pain. 2023;164(9):1965–1975. doi:10.1097/j.pain.0000000000002892
79. Potential mechanisms of acupuncture for neuropathic pain based on somatosensory system - PubMed. Available from: https://pubmed.ncbi.nlm.nih.gov/36203799/.
80. Wang M, Liu W, Ge J, Liu S. The immunomodulatory mechanisms for acupuncture practice. Front Immunol. 2023;14:1147718. doi:10.3389/fimmu.2023.1147718
81. Ma Q. Somatotopic organization of autonomic reflexes by acupuncture. Curr Opin Neurobiol. 2022;76:102602. doi:10.1016/j.conb.2022.102602
82. Cai RL, Shen GM, Wang H, Guan YY. Brain functional connectivity network studies of acupuncture: a systematic review on resting-state fMRI. J Integr Med. 2018;16(1):26–33. doi:10.1016/j.joim.2017.12.002
83. Huang W, Pach D, Napadow V, et al. Characterizing acupuncture stimuli using brain imaging with FMRI--a systematic review and meta-analysis of the literature. PLoS One. 2012;7(4):e32960. doi:10.1371/journal.pone.0032960
84. Li N, Guo Y, Gong Y, et al. The anti-inflammatory actions and mechanisms of acupuncture from acupoint to target organs via neuro-immune regulation. J Inflamm Res. 2021;14:7191–7224. doi:10.2147/JIR.S341581
85. Diao XT, Yao L, Ma JJ, et al. Analgesic action of adenosine A1 receptor involves the dephosphorylation of glycine receptor α1ins subunit in spinal dorsal horn of mice. Neuropharmacology. 2020;176:108219. doi:10.1016/j.neuropharm.2020.108219
86. Edwards JW, Shaw V. Acupuncture in the management of trigeminal neuralgia. Acupunct Med. 2021;39(3):192–199. doi:10.1177/0964528420924042
87. Zhao W, Huang H, Liu K, et al. Acupuncture and moxibustion for peripheral neuropathic pain: a frequentist network meta-analysis and cost-effectiveness evaluation. Evid-Based Compl Altern Med ECAM. 2022;2022:6886465. doi:10.1155/2022/6886465
88. Gao J, Zhao C, Jiang W, Zheng B, He Y. Effect of acupuncture on cognitive function and quality of life in patients with idiopathic trigeminal neuralgia. J Nerv Ment Dis. 2019;207(3):171–174. doi:10.1097/NMD.0000000000000937
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Efficacy and Safety of Acupuncture for Depression-Related Insomnia: Protocol for a Systematic Review and Meta-Analysis
Hu H, Li Z, Cheng Y, Gao H
Journal of Pain Research 2022, 15:1939-1947
Published Date: 13 July 2022
The Efficacy and Safety of Acupuncture for Tinnitus-Associated Insomnia: A Protocol for a Systematic Review and Meta-Analysis
Fan L, Gao Y, Zhou J, Hu H, Gao H
Journal of Pain Research 2022, 15:2957-2965
Published Date: 21 September 2022
The Role of Acupuncture and Its Related Mechanism in Treating Chronic Prostatitis/Chronic Pelvic Pain Syndrome
Wang H, Zhang J, Ma D, Zhao Z
International Journal of General Medicine 2023, 16:4039-4050
Published Date: 6 September 2023
The Effectiveness and Safety of Acupuncture for Mammary Hyperplasia: A Systematic Review and Meta-Analysis
Li J, Zhang D, Hu J, Cui J, Mansoor KM
Journal of Pain Research 2024, 17:1761-1772
Published Date: 17 May 2024
Efficacy of Acupuncture in Patients with Fibromyalgia Syndrome: A Meta-Analysis
Jin L, Zhou Y, Li L, Song F, Zhou Y
Journal of Pain Research 2026, 19:568235
Published Date: 3 February 2026