Back to Journals » Cancer Management and Research » Volume 17

Tumor-Associated Autoantibodies Anti-p53 is Associated with Poor Prognosis in Patients with Lung Adenocarcinoma
Authors Jing K, Ouyang L, Cai J, Zheng P, Li G, Wang R
Received 2 July 2025
Accepted for publication 21 October 2025
Published 7 November 2025 Volume 2025:17 Pages 2665—2674
DOI https://doi.org/10.2147/CMAR.S540712
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Harikrishna Nakshatri
Keying Jing, Libo Ouyang, Jun Cai, Peiming Zheng, Gang Li, Rong Wang
Department of Clinical Laboratory, Henan Provincial People’s Hospital, People’s Hospital of Zhengzhou University, Zhengzhou, People’s Republic of China
Correspondence: Rong Wang, Email [email protected]
Purpose: There is a known association between tumor-associated autoantibodies (TAAbs) and lung cancer. TAAbs are currently used in clinical settings for the early detection of lung cancer. However, the relationship between TAAbs profiles and clinical outcomes in lung cancer patients remains incompletely understood. This study aims to investigate the association between TAAbs and survival rates in individuals diagnosed with lung adenocarcinoma.
Patients and Methods: This study enrolled 161 patients diagnosed with lung adenocarcinoma at Henan Province People’s Hospital between January 2020 and December 2022. Levels of TAAbs were measured using a commercial enzyme-linked immunosorbent assay (ELISA) kit. Follow-up data were collected through December 2024. The association between TAAbs levels and disease progression was evaluated using Kaplan–Meier survival analysis and Cox proportional hazards models.
Results: In the univariate analysis, the presence of p53 autoantibodies (anti-p53) and CAGE autoantibodies (anti-CAGE) was associated with an increased risk of reduced progression-free survival (PFS). In the multivariate analysis, anti-p53 remained significantly associated with shorter PFS, while anti-CAGE was not correlated with poor prognosis. The significant association between anti-p53 and worse PFS persisted after adjusting for gender, age, smoking status, pathological stage, and treatment. Kaplan–Meier survival analysis further confirmed that patients positive for anti-p53 had significantly shorter PFS (P = 0.0025).
Conclusion: Tumor-associated autoantibody anti-p53 correlates poor prognosis in lung adenocarcinoma patients, offering novel insights into tumor prognosis.
Keywords: lung adenocarcinoma, autoantibodies associated with lung cancer, prognosis, progression-free survival
Introduction
Lung cancer is the second most prevalent cancer worldwide and leads in both occurrence and fatality among all cancers in China.1,2 A major concern is that lung cancer is frequently diagnosed at advanced stages, which contributes to its high recurrence rate. Recent studies indicate that by 2020, lung adenocarcinoma had emerged as the predominant subtype of lung cancer worldwide. Specifically, among new lung cancer cases, adenocarcinoma accounted for 39% in male patients, surpassing squamous cell carcinoma (25%). In female patients, adenocarcinoma represented 57% of cases, whereas squamous cell carcinoma constituted only 12%.3 Despite its predominance, reliable biomarkers for predicting prognosis in lung adenocarcinoma remain scarce. Therefore, the identification of effective prognostic biomarkers for this disease is critically needed.
Tumor markers have long played a crucial role in cancer detection during its earliest stages.4–8 The detection of lung cancer has benefited from an array of blood biomarkers. Notably, both neuron-specific enolase (NSE) and cytokeratin fragment 21–1 (CYFRA 21–1) have shown significant associations with lung cancer.5,6 However, few biomarkers are currently available for monitoring lung cancer prognosis. Increased CYFRA 21–1 concentrations are associated with decreased overall survival in advanced-stage lung cancer.9 Additionally, a retrospective study demonstrated that high levels of carcinoembryonic antigen (CEA) both before and after surgery independently predict worse outcomes in stage I–III lung adenocarcinoma patients.10 However, the variety of available markers remains relatively limited.
During cancer’s initial development, the body’s immune defenses can detect trace amounts of irregular proteins produced by malignant cells-referred to as tumor-associated antigens (TAAs). These biological markers set off a targeted immunological reaction that prompts the generation of autoantibodies.11 Studies have demonstrated that various types of cancer are associated with specific antibodies targeting TAAs. In lung cancer patients, gene mutations, translocations, or recombination occur early during tumor development. Upon release, these antigens trigger immune recognition, leading to antibody production-specifically tumor-associated autoantibodies (TAAbs).12–14
Although TAAbs have been widely used in lung cancer screening, their potential role in prognosis monitoring remains underexplored. Some studies have suggested a possible association between TAAbs and improved cancer outcomes,15,16 but the evidence remains inconclusive. This study aims to evaluate the prognostic value of TAAbs in the peripheral blood of patients with lung adenocarcinoma.
Materials and Methods
Patients
This retrospective study included 161 lung adenocarcinoma patients from Henan Provincial People’s Hospital (2020–2022). Eligibility required participants to be ≥18 years old with biopsy-confirmed lung adenocarcinoma, as per the National Comprehensive Cancer Network guidelines.17 Participants were not included if they had simultaneous autoimmune disorders or additional primary cancers. Comprehensive patient data, covering gender, age, smoking history, cancer stage, and treatments, were systematically collected from the hospital information management system. Patients were monitored via phone. The follow-up deadline was December 2024 (Figure 1). All study participants provided informed consent. All procedures adhered to pertinent guidelines and laws. The Ethics Board at Henan Provincial People’s Hospital gave the study its consent (202390).
 |
Figure 1 Flow diagram of the screening and enrollment of study patients. |
Serum Collection and Detection of Tumor-Associated Autoantibodies
Prior to TAAbs detection, serum samples were centrifuged and subsequently stored at −80°C in a cryogenic freezer.
In this study, TAAbs detection kits utilizing Enzyme-linked immunosorbent assay (ELISA) (Hangzhou Cancer Probe Biotech, Hangzhou, China). The kit number is CNDA-REG-20153402087. The results of the three batch test kits showed that all were no higher than 3.75 U/mL. Analyzing the specificity, the results showed that the influence of potential interfering substances and cross-reactive substances on the test kit was within ±20.0%. The results of the three batches of test kits showed a good linear relationship within the range of 3.75 to 60 U/mL, with r ≥ 0.9900.
Principle of detection:
The kit contained a total of eight antigens, with streptavidin serving as the primary detecting antigen for background assessment, and the remaining antigens being TAAbs: p53, GAGE7, PGP9.5, CAGE, MAGE A1, SOX2, GBU4-5. The seven antigen proteins were modified with streptomycin biotin and Myc tags for protein expression, purification, coating and detection processes. Following purification, the antigens were indirectly coated onto the solid phase plate through a specific reaction between biotin and streptomycin, after which the diluted serum was applied. The TAAbs present in the serum samples were specifically bound to the antigens on the solid phase plate. This led to the formation of an antigen-antibody-enzyme-labeled antibody complex. With any unbound enzyme-labeled anti-human IgG antibody being subsequently washed away. After reacting with a chromogenic substrate, the absorbance was measured at 450nm using a microplate reader, enabling the calculation of the relative concentration of TAAbs.
Preparations:
① Before the experiment, all reagents were equilibrated to room temperature (18–25°C) and mixed. ② Wash working solution: 10 times of wash solution was diluted 10 times with pure water and prepared into wash working solution, which was stored at 2–8°C. ③ PBS buffer: pH 7.6. ④ Serum sample to be tested: 545 ul of sample diluent was added to a 1.5mL EP tube, and then 5uL of the serum sample to be tested was added to the sample diluent and mixed. ⑤ Enzyme conjugate working Solution: “enzyme conjugate working solution” and “enzyme conjugate diluents” were mixed at a ratio of 1:19 to the desired volume of the experiment and prepared 15 min before use. ⑥ Chromogen: Mix “Chromogen A solution” and “Chromogen B solution” at a ratio of 1:19.
Experimental procedures:
① 200 μL PBS buffer was added to each well, the plate was washed once and pat dry on clean absorbent paper. ② Add 50 μL of quality control, calibrator, loading control and diluted samples to be tested in corresponding microwells, attach the sealing plate membrane and incubate at room temperature for 60 minutes with shaking. ③ Wash plate: shake off the liquid in the hole and pat dry on clean absorbent paper. Two hundred ul of wash working solution was added to each well and then dried. Washing the plate was repeated 3 times and finally patted dry on clean absorbent paper. ④ 50 μL of the diluted enzyme conjugate working solution was added to each well, shaken, affixed to the plate sealing membrane, and incubated for 30 minutes at room temperature with shaking. ⑤ Wash the plate: Repeat the above steps. ⑥ 100 μL of the mixed chromogenic agent was added to each well and incubated at room temperature in the dark with shaking for 15 minutes. About 50 μL of termination solution was added to each well and gently shaken. ⑦ OD values were read using a microplate reader within 30 minutes of the end of the reaction.
Statistical Analysis
This experiment is an exploratory study. Categorical data were summarized using counts and percentages [n (%)], whereas continuous measures were reported as means accompanied by standard deviations (mean ± SD). The value of TAAbs is expressed by the median (IQR). Tumors were staged based on the Union for International Cancer Control’s 8th edition TNM Malignant Tumors Classification,18 the lung cancer patients were categorized into four stages. To evaluate the influence of clinical factors on progression-free survival (PFS) in lung adenocarcinoma cases, we conducted Cox proportional hazards regression analyses. This study has verified the assumptions of the Cox proportional hazards model using the Schoenfeld residuals method, ensuring the reliability of the analysis results. The findings are presented as hazard ratios (HRs) along with their 95% confidence intervals (CIs).
Age was converted from continuous to binary, with 60 years as the cutoff to classify patients as elderly (≥60) or younger. Immunotherapy was defined as any regimen that used PD-1/PD-L1 inhibitor. “Other treatments” were treatment modalities that excluded surgical treatment or immunotherapy.
For assessing the link between TAAbs and lung adenocarcinoma patient outcomes, both unadjusted and adjusted-for-multiple-factors analyses were conducted. The initial crude model did not account for any confounding variables. Subsequently, Model III incorporated adjustments for key factors, including patient demographics (gender, age), smoking history, tumor stage, and treatment protocols. The adjusted I model accounted for only two variables: gender and age. The adjusted II model expanded on this by also factoring in smoking status. The most comprehensive model (Model III) went a step further, incorporating not only demographic and lifestyle factors but also clinical variables such as pathological staging and treatment protocols for lung adenocarcinoma cases.
PFS was calculated as the time between initial disease diagnosis and the first observed disease progression. The Kaplan–Meier (K-M) method was employed to generate the PFS survival curve, with a cut-off for statistical relevance being a p-value below 0.05.
Results
Characterization of the Study Population
This retrospective study enrolled 161 patients with histologically confirmed lung adenocarcinoma, comprising 86 cases with disease progression and 75 progression-free individuals. Table 1 summarizes participant demographics and clinical features. The study included 161 participants, comprising 84 men (52.2%) and 77 women (47.8%), with an average age of 61.5 years (±9.8 years). Sixty-five patients (40.4%) were smokers. For analytical purposes, pathological stages were dichotomized into early-stage (I & II; n = 26, 16.1%) and advanced-stage disease (III & IV; n = 135, 83.9%). Among the 161 patients, the most patients were treated with immunotherapy (n = 93, 57.8%).
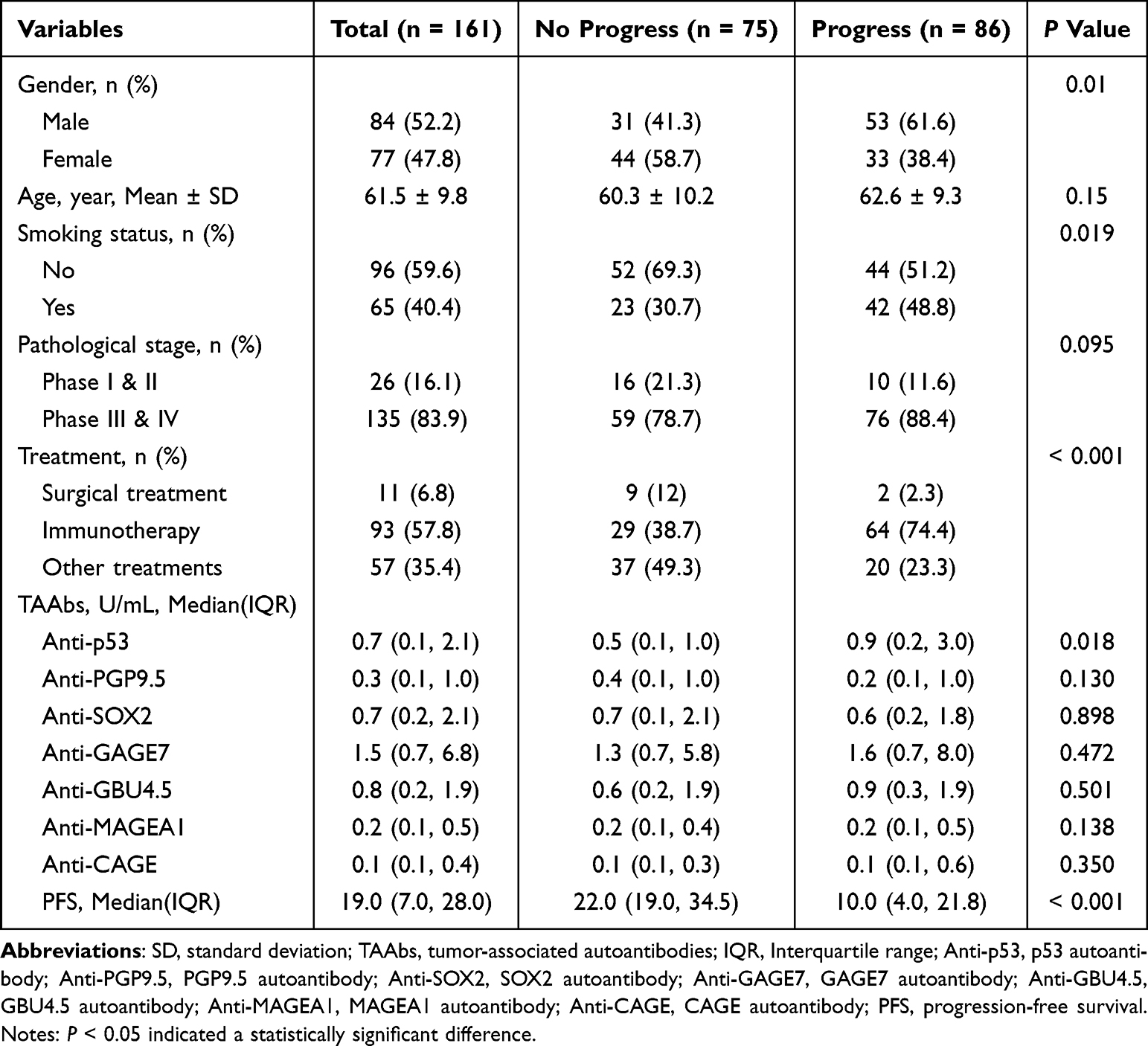 |
Table 1 Demographic and Clinical Characteristics of the Patients with Lung Adenocarcinoma |
Univariate Cox Regression Models of Seven TAAbs in Patients with Lung Adenocarcinoma
Table 2 presents HRs and 95% CIs for factors influencing disease progression in lung adenocarcinoma patients. We observed that female patients had an 41% depressed risk of disease progression compared to male patients (P = 0.019). The univariate analysis of seven lung cancer autoantibodies demonstrated a statistically significant association between anti-p53 levels and disease progression, with each unit increase corresponding to a 9% higher risk (P < 0.001). Mirroring this trend, the data in Table 2 indicated that elevated anti-CAGE levels similarly predicted poorer outcomes, showing a 5% increased risk per unit (P = 0.039). Notably, among the seven antibodies examined in lung adenocarcinoma cases, anti-p53 and anti-CAGE stood out as having distinct prognostic implications.
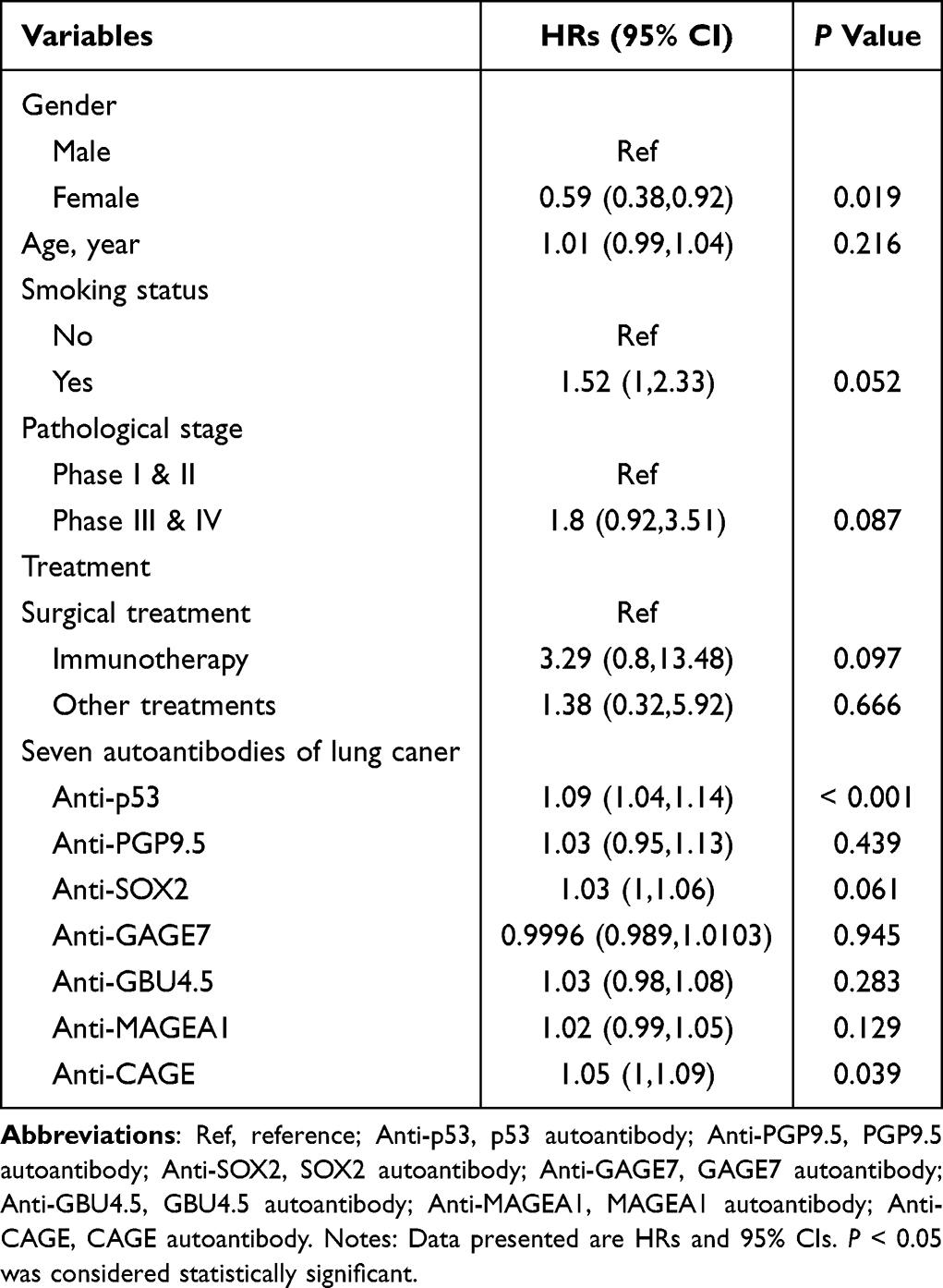 |
Table 2 Univariate Cox Regression Models for Patients with Lung Adenocarcinoma |
Multivariable Cox Regression Models of Anti-p53 in Patients with Lung Adenocarcinoma
The results of the univariate analysis indicated that anti-p53 had an impact on the progression of lung adenocarcinoma patients, with anti-p53 being considered a continuous variable. In the multivariate analysis and survival analysis, anti-p53 was categorized as a categorical variable, with cut-off values selected using X-tile software.19,20 The cut-off value of anti-p53 is 1.0 U/mL. Table 3 displayed the HRs and corresponding 95% CIs for anti-p53 and its association with disease progression in lung adenocarcinoma patients. In the unadjusted model, it was observed that patients with anti-p53 had an 91% increased risk of disease progression compared to patients without anti-p53 (95% CIs: 1.25, 2.93). After adjusted for gender and age, the HR was 1.88 (95% CIs: 1.22, 2.89, P for trend = 0.004). Model II, fine-tuned for gender, age, and smoking habits, exhibited a hazard ratio of 1.88. Finally, after adjusted for gender, age, smoking status, pathological staging and treatments, the HR was 1.91 (95% CIs: 1.23, 2.96, P for trend = 0.004).
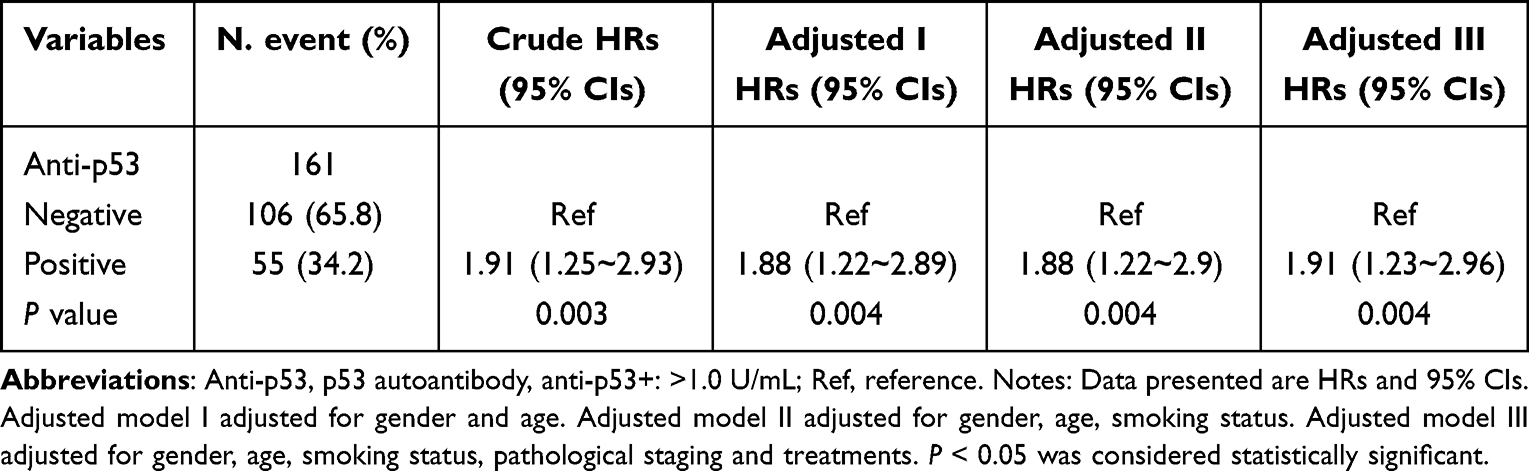 |
Table 3 Multivariable Cox Regression Model for Anti-p53 in Patients with Lung Adenocarcinoma |
Multivariable Cox Regression Models of Anti-CAGE in Patients with Lung Adenocarcinoma
Similar to anti-p53, anti-CAGE was treated as a categorical variable in multivariate analysis.19,20 The cut-off value of anti-CAGE is 10.1 U/mL. Table 4 showed the HRs and 95% CIs for anti-CAGE. In the unadjusted analysis, anti-CAGE-positive patients had a 2.66-fold higher disease progression risk compared to anti-CAGE-negative individuals (95% CIs: 1.15, 6.11, P for trend = 0.022). After adjusted for gender, age, smoking status, pathological staging and treatments, there was no significant difference between them. The HR was 2.07 (95% CIs: 0.88, 4.92, P for trend = 0.097).
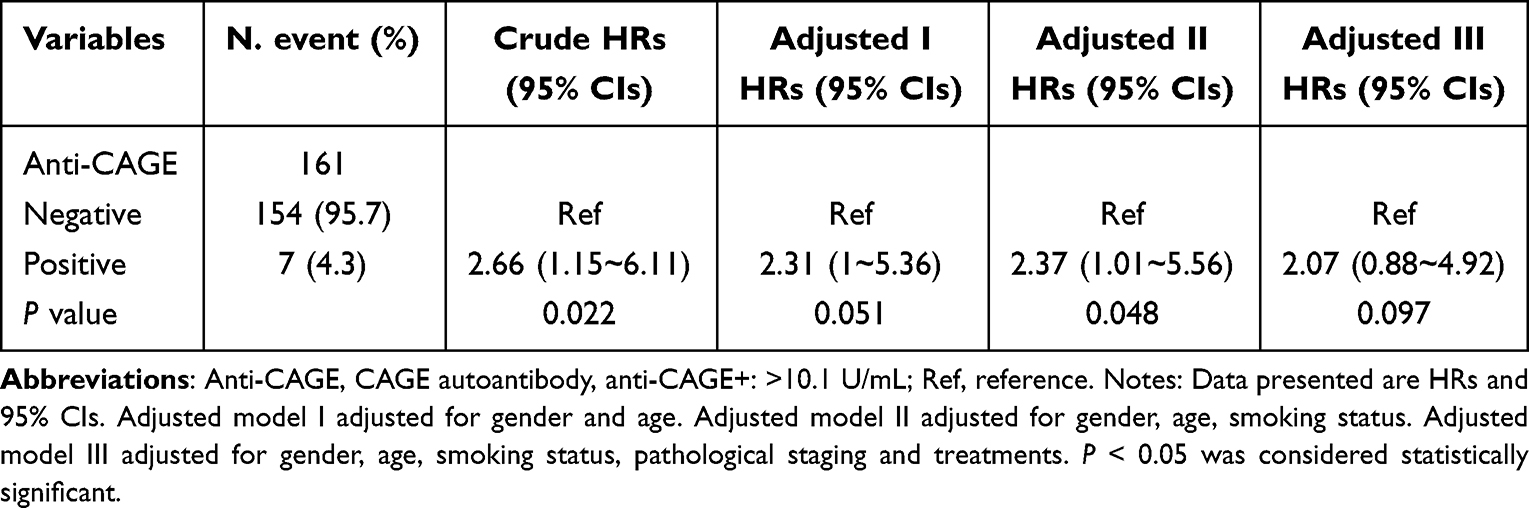 |
Table 4 Multivariable Cox Regression Models for Anti-CAGE in Patients with Lung Adenocarcinoma |
Subgroup Analysis of Anti-p53 in Patients with Lung Adenocarcinoma
To explore whether the link between anti-p53 antibodies and patient outcomes in lung adenocarcinoma remained consistent across different groups, we conducted a stratified analysis. The subgroups were divided by gender, age, smoking history, disease stage, and treatment type (Table 5). This approach allowed us to assess the robustness of the observed associations under varying conditions.
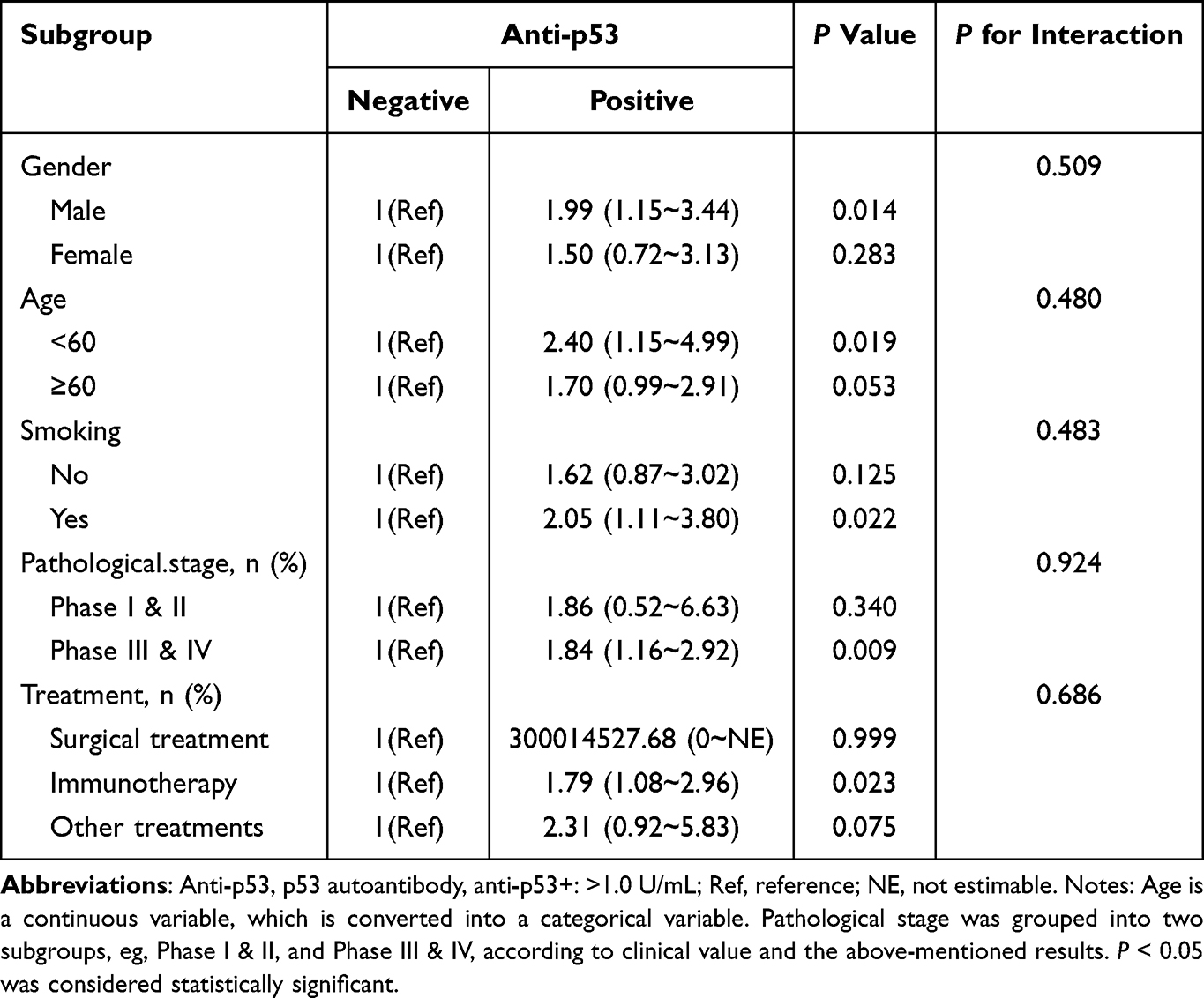 |
Table 5 Anti-p53 Autoantibody Subgroup Analyses |
The study revealed that the relationship between anti-p53 and lung cancer patients’ outcomes held steady across various demographics, including gender, age, smoking history, disease stage, and treatment. The interplay between these factors and the outcomes did not differ significantly. What’s more, the association seemed stronger in males, the younger age group, smokers, and those with more advanced lung adenocarcinoma. Figure 2A showed the results of the forest plot for the anti-p53 subgroup analysis. Overall, the link between anti-p53 antibody and lung cancer outcomes remained consistent regardless of gender, age, smoking history, disease stage, or therapy.
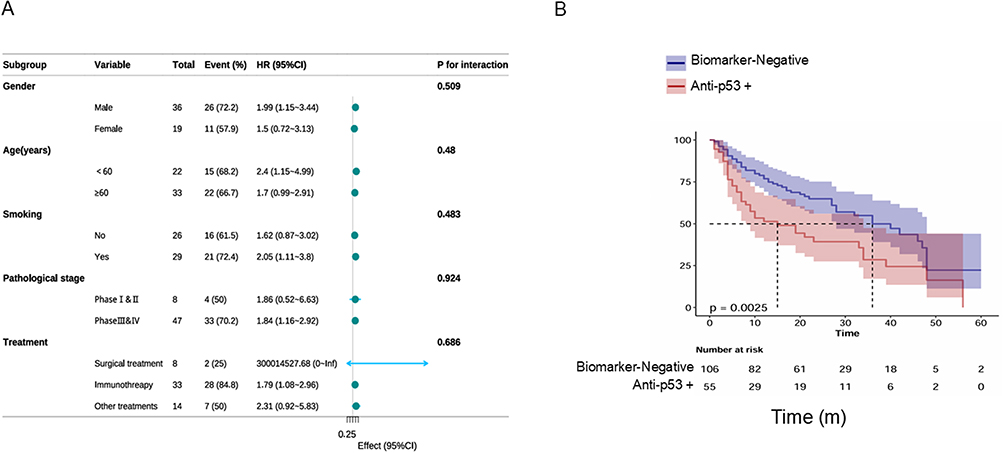 |
Figure 2 (A) The results of the forest plot for the anti-p53 subgroup analysis. (B) Progression-free survival analysis of anti-p53 in patients with lung adenocarcinoma. Abbreviations: Anti-p53, p53 autoantibody; P value < 0.05 indicated a statistically significant difference. |
Analysis of Survival
The associations between the presence of anti-p53 and PFS in lung adenocarcinoma patients were evaluated using K-M curves. The findings were depicted in Figure 2B. Specifically, Figure 2B demonstrated that patients positive for anti-p53 had significantly shorter PFS compare to those without anti-p53 (P = 0.0025). The presence of anti-p53 can predict the poor prognosis of patients.
Discussion
With the increasing incidence and mortality of lung cancer, there is a pressing need to identify reliable biomarkers for predicting tumor development and monitoring prognosis. In this study, we analyzed 161 patients with lung adenocarcinoma and detected the presence of seven TAAbs. Our findings indicate that anti-p53 acts as an independent biomarker of poor prognosis, irrespective of gender, age, smoking status, pathological stage, or treatment modalities. Furthermore, patients positive for anti-p53 exhibited significantly shorter PFS.
As tumors develop and progress, they produce and release unique proteins known as TAAs. These TAAs arise from a variety of mechanisms, including protein overexpression, mutation, misfolding, and dysregulated degradation. The aberrant expression and presentation of these antigens can trigger a humoral immune response, stimulating the immune system to produce specific autoantibodies against TAAs, referred to as TAAbs.21 This study evaluated a panel of seven tumor-associated autoantibodies (TAAbs). Univariate analysis indicated that both anti-p53 and anti-CAGE were statistically significant in predicting the progression of lung adenocarcinoma. However, due to the limited number of anti-CAGE-positive patients, the results for this marker may be subject to potential bias. Furthermore, multivariate analysis showed that anti-CAGE was not statistically significant (P > 0.05) after adjustment for covariates. Therefore, we focused subsequent analyses exclusively on anti-p53.
The tumor suppressor gene product of p53 is one of the earliest discovered tumor suppressor genes and consists of 393 amino acids of transcription factors. Inactivation of p53 protein due to p53 gene mutation is a crucial step in the development of many cancers.22–24 Mutations in the p53 gene not only lead to the loss of its tumor-suppressor function but may also confer gain-of-function oncogenic properties. Concurrently, these alterations can induce the production of specific autoantibodies. For example, in pancreatic cancer, the p53R172H missense mutation modulates the expression of chemokines including CXCL1, contributing to an immunosuppressive tumor microenvironment and reducing the efficacy of immune checkpoint inhibitor therapy.25 Furthermore, p53 mutants often have a longer half-life, resulting in their abnormal accumulation within tumor cells. This accumulation is not only associated with the malignant progression of the tumor but may also trigger the body’s immune system to produce specific autoantibodies.
Numerous studies in recent years have established the significant value of anti-p53 in the early detection of various cancer types. In lung cancer, anti-p53 have been incorporated into clinical screening strategies. Detection of anti-p53 via ELISA, particularly in combination with other tumor-associated antibodies, has been shown to significantly improve the early diagnosis rate of lung cancer. Apart from its value in early cancer screening, the anti-p53 also demonstrates great potential in cancer prognosis assessment. A study investigated the impact of two combined methods anti-p53 expression and preoperative serum carcinoembryonic antigen (S-CEA) testing on the prognosis of colorectal cancer patients. The results showed that the combined method of p53 and S-CEA detection was more effective in evaluating the prognosis of colorectal cancer compared to the traditional combination.26 A recent investigation of a panel of tumor-associated autoantibodies, including anti-p53, anti-CAGE, anti-MAGEA4, anti-GAGE7, anti-UTP14A, anti-IMP2 and anti-PSMC1 7, revealed that patients with these TAAbs exhibited a longer PFS.15 Additionally, another study reported that a panel of five TAAbs targeting anti-p53, anti-BRCA2, anti-HUD, anti-TRIM21, and anti-NY-ESO-1 was linked to a better prognosis and extended PFS.16 The research on non-small cell lung cancer patients linked elevated anti-PGP9.5 and anti-p53 levels to reduced PFS.27 Moreover, an earlier study indicated that the survival rate of TAAbs-positive lung cancer patients was significantly lower compare to negative or low-titer patients at 30-month mark.28 The prognostic value of anti-p53 is closely linked to p53 mutation and functional disruption.29,30 Another research showed that loss of p53 function leads to upregulation of IL-34 gene normally suppressed by p53. This enhances CD36-mediated fatty acid oxidation, promotes M2-type polarization of foam-like tumor-associated macrophages (TAMs), and inhibits CD8⁺ T cell function, ultimately facilitating immune escape. Importantly, blocking the IL-34-CD36 axis can restore anti-tumor immunity and synergize with anti-PD-1 treatment.31 This might partly explain the reason why patients with positive p53 autoantibodies have a poorer prognosis.
TAAbs have emerged as promising biomarkers for monitoring lung cancer prognosis, offering several practical advantages. Firstly, TAAbs are more readily detectable than their corresponding TAAs. Secondly, they demonstrate high stability under routine sample handling and storage conditions, with low pre-analytical requirements and an extended serum half-life. Thirdly, serum-based TAAbs detection-commonly performed via ELISA-is minimally invasive, technically feasible, and highly reproducible. Moreover, TAAbs can often be detected months or even years before radiographic signs become apparent.
However, several limitations must be considered when using TAAbs for prognostic prediction. Firstly, we acknowledge the shortcomings of our study. The study was a single-center study with a small sample size. Secondly, we have only explored the value of TAABS in the prognosis of lung cancer. Further research is needed for other cancer types. Clinically, TAAbs currently have limited application in routine practice. The positive results may not be exclusive to lung cancer, as these antibodies can occur in other benign or malignant conditions. In the future, we will need more experiments to continue exploring.
Conclusion
In summary, this study found that patients with the anti-p53 exhibited shorter PFS. This finding holds significant clinical implications, offering new insights and methods for monitoring the prognosis of lung adenocarcinoma patients. However, the role of the immune response in lung adenocarcinoma patients remains not fully understood. In the future, we will conduct more large-scale and multi-center studies to further explore the mechanisms and effects involved, providing more valuable reference evidence for clinical significance.
Abbreviations
TAAbs, tumor associated-autoantibodies; ELISA, Enzyme-linked immunosorbent assay; anti-p53, p53 autoantibodies; anti-CAGE, CAGE autoantibodies; PFS, progression-free survival; CTCs, circulating tumor cells; ctDNA, circulating tumor DNA; TEPs, tumor educated platelets; NSE, neuron-specific enolase; CYFRA 21-1, cytokeratin fragment 21-1; OS, overall survival; CEA, carcinoembryonic antigen; TAAs, tumor-associated antigens; HRs, hazard ratios; CIs, confidence intervals; K-M, Kaplan-Meier; AUC, area under curve; NSFC, Natural Science Foundation of China.
Data Sharing Statement
All the results are presented in the article. Further inquiries can be directed to the corresponding authors.
Ethics Statement
The study received ethical clearance from Henan Provincial People’s Hospital. (Approval number. 202390). All experiments and procedures were performed according to the Declaration of Helsinki (as revised in 2013).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the National Natural Science Foundation of China (NSFC) (82002210) and the Henan Provincial medical science and technology research project (LHGJ20240098).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–263. doi:10.3322/caac.21834
2. Siegel RL, Miller KD, Wagle NS, Jemal A. Cancer statistics, 2023. CA Cancer J Clin. 2023;73(1):17–48. doi:10.3322/caac.21763
3. Zhang Y, Vaccarella S, Morgan E, et al. Global variations in lung cancer incidence by histological subtype in 2020: a population-based study. Lancet Oncol. 2023;24(11):1206–1218. doi:10.1016/S1470-2045(23)00444-8
4. Mamdani H, Ahmed S, Armstrong S, Mok T, Jalal SI. Blood-based tumor biomarkers in lung cancer for detection and treatment. Transl Lung Cancer Res. 2017;6(6):648–660. doi:10.21037/tlcr.2017.09.03
5. Sun A. Clinical role of serum tumor markers SCC, NSE, CA 125, CA 19-9, and CYFRA 21-1 in patients with lung cancer. Lab Med. 2023;54(6):638–645. doi:10.1093/labmed/lmad020
6. Stieber P, Hasholzner U, Bodenmuller H, et al. CYFRA 21-1. A new marker in lung cancer. Cancer. 1993;72(3):707–713. doi:10.1002/1097-0142(19930801)72:3<707::AID-CNCR2820720313>3.0.CO;2-X
7. Ren S, Zeng G, Yi Y, et al. Combinations of plasma cfDNA concentration, integrity and tumor markers are promising biomarkers for early diagnosis of non-small cell lung cancer. Heliyon. 2023;9(10):e20851. doi:10.1016/j.heliyon.2023.e20851
8. Yang G, Xiao Z, Tang C, Deng Y, Huang H, He Z. Recent advances in biosensor for detection of lung cancer biomarkers. Biosens Bioelectron. 2019;141:111416. doi:10.1016/j.bios.2019.111416
9. Kanaji N, Kadota K, Tadokoro A, et al. Serum CYFRA 21-1 but not vimentin is associated with poor prognosis in advanced lung cancer patients. Open Respir Med J. 2019;13:31–37. doi:10.2174/1874306401913010031
10. Jiao Z, Cao S, Li J, et al. Clinical associations of preoperative and postoperative serum CEA and lung cancer outcome. Front Mol Biosci. 2021;8:686313. doi:10.3389/fmolb.2021.686313
11. Belousov PV. Analysis of the repertoires of circulating autoantibodies’ specificities as a tool for identification of the tumor-associated antigens: current problems and solutions. Biochemistry. 2021;86(10):1225–1242. doi:10.1134/S0006297921100060
12. Tan EM, Zhang J. Autoantibodies to tumor-associated antigens: reporters from the immune system. Immunol Rev. 2008;222:328–340. doi:10.1111/j.1600-065X.2008.00611.x
13. Xu Y, Zhang W, Xia T, et al. Diagnostic value of tumor-associated autoantibodies panel in combination with traditional tumor markers for lung cancer. Front Oncol. 2023;13:1022331. doi:10.3389/fonc.2023.1022331
14. Tan EM. Autoantibodies, autoimmune disease, and the birth of immune diagnostics. J Clin Invest. 2012;122(11):3835–3836. doi:10.1172/JCI66510
15. Zhao J, Wu Y, Yue Y, et al. The development of a tumor-associated autoantibodies panel to predict clinical outcomes for immune checkpoint inhibitor-based treatment in patients with advanced non-small-cell lung cancer. Thorac Cancer. 2023;14(5):497–505. doi:10.1111/1759-7714.14772
16. Zhou J, Zhao J, Jia Q, et al. Peripheral blood autoantibodies against to tumor-associated antigen predict clinical outcome to immune checkpoint inhibitor-based treatment in advanced non-small cell lung cancer. Front Oncol. 2021;11:625578. doi:10.3389/fonc.2021.625578
17. Ettinger DS, Wood DE, Aisner DL, et al. Non-small cell lung cancer, version 3.2022, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2022;20(5):497–530. doi:10.6004/jnccn.2022.0025
18. Detterbeck FC, Boffa DJ, Kim AW, Tanoue LT. The eighth edition lung cancer stage classification. Chest. 2017;151(1):193–203. doi:10.1016/j.chest.2016.10.010
19. Camp RL, Dolled-Filhart M, Rimm DL. X-tile: a new bio-informatics tool for biomarker assessment and outcome-based cut-point optimization. Clin Cancer Res. 2004;10(21):7252–7259. doi:10.1158/1078-0432.CCR-04-0713
20. Pan C, Wang X, Chen W, et al. Reevaluation of glypican-3 as a prognostic marker in HCC using X-tile software. Med Oncol. 2015;32(1):359. doi:10.1007/s12032-014-0359-z
21. Heo CK, Bahk YY, Cho EW. Tumor-associated autoantibodies as diagnostic and prognostic biomarkers. BMB Rep. 2012;45(12):677–685. doi:10.5483/BMBRep.2012.45.12.236
22. Mack U, Ukena D, Montenarh M, Sybrecht GW. Serum anti-p53 antibodies in patients with lung cancer. Oncol Rep. 2000;7(3):669–674. doi:10.3892/or.7.3.669
23. Shimada H, Ochiai T, Nomura F. Japan p53 antibody research g. titration of serum p53 antibodies in 1,085 patients with various types of malignant tumors: a multiinstitutional analysis by the Japan p53 antibody research group. Cancer. 2003;97(3):682–689. doi:10.1002/cncr.11092
24. Gupta S, Silveira DA, Mombach JC, Hashimoto RF. Targeting NSCLC drug resistance: systems biology insights into the MALAT1/miR-145-5p axis and Wip1 in regulating ferroptosis and apoptosis. J R Soc Interface. 2025;22(226):20240852. doi:10.1098/rsif.2024.0852
25. Mahat DB, Kumra H, Castro SA, et al. Mutant p53 exploits enhancers to elevate immunosuppressive chemokine expression and impair immune checkpoint inhibitors in pancreatic cancer. Immunity. 2025;58(7):1688–1705e1689. doi:10.1016/j.immuni.2025.06.005
26. Tong G, Wang Y, Qian H, Tan Z, Shen Y, Li H. The effects of two combined methods of P53 expression and preoperative serum CEA detection on the prognosis of colorectal cancer. Front Oncol. 2025;15:1590836. doi:10.3389/fonc.2025.1590836
27. Chen SS, Li K, Wu J, et al. Stem signatures associated antibodies yield early diagnosis and precise prognosis predication of patients with non-small cell lung cancer. J Cancer Res Clin Oncol. 2021;147(1):223–233. doi:10.1007/s00432-020-03325-4
28. Mattioni M, Soddu S, Prodosmo A, et al. Prognostic role of serum p53 antibodies in lung cancer. BMC Cancer. 2015;15:148. doi:10.1186/s12885-015-1174-4
29. Siolas D, Vucic E, Kurz E, Hajdu C, Bar-Sagi D. Gain-of-function p53(R172H) mutation drives accumulation of neutrophils in pancreatic tumors, promoting resistance to immunotherapy. Cell Rep. 2021;36(8):109578. doi:10.1016/j.celrep.2021.109578
30. Yu J, Ling S, Hong J, et al. TP53/mTORC1-mediated bidirectional regulation of PD-L1 modulates immune evasion in hepatocellular carcinoma. J Immunother Cancer. 2023;11(11):e007479. doi:10.1136/jitc-2023-007479
31. Nian Z, Dou Y, Shen Y, et al. Interleukin-34-orchestrated tumor-associated macrophage reprogramming is required for tumor immune escape driven by p53 inactivation. Immunity. 2024;57(10):2344–2361e2347. doi:10.1016/j.immuni.2024.08.015
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comprehensive Analysis of the E2F Transcription Factor Family in Human Lung Adenocarcinoma
Wang Q, Liu J, Cheang I, Li J, Chen T, Li Y, Yu B
International Journal of General Medicine 2022, 15:5973-5984
Published Date: 2 July 2022
High Expression of DEPDC1B Predicts Poor Prognosis in Lung Adenocarcinoma

Li P, Chen X, Zhou S, Xia X, Wang E, Han R, Zeng D, Fei G, Wang R
Journal of Inflammation Research 2022, 15:4171-4184
Published Date: 23 July 2022
Expression, Clinical Significance, Immune Infiltration, and Regulation Network of miR-3940-5p in Lung Adenocarcinoma Based on Bioinformatic Analysis and Experimental Validation
Lin Z, Huang W, Xie Z, Yi Y, Li Z
International Journal of General Medicine 2022, 15:6451-6464
Published Date: 6 August 2022
Decreased Expression of a Novel lncRNA FAM181A-AS1 is Associated with Poor Prognosis and Immune Infiltration in Lung Adenocarcinoma
Liang W, Lu Y, Pan X, Zeng Y, Zheng W, Li Y, Nie Y, Li D, Wang D
Pharmacogenomics and Personalized Medicine 2022, 15:985-998
Published Date: 2 December 2022
Prognostic Significance of Iron Metabolism Related Genes in Human Lung Adenocarcinoma
Li P, Wu X, Chen P, Gu Z
Cancer Management and Research 2023, 15:203-216
Published Date: 22 February 2023