Back to Journals » Journal of Inflammation Research » Volume 18
Triglyceride-Glucose Index and Neutrophil-to-Lymphocyte Ratio: A Metabolic-Inflammatory Signature for Mortality Prediction in a Multicenter Retrospective Cohort of 1249 Dialysis Patients with Coronary Artery Disease
Authors Li Y, Li P, Tang Q, Jiao T, Gao Y, An S, Jiang H, Cheng H, Yang Z, Zhou J, Sun Y, Yang Y ![]() , Zheng J
, Zheng J ![]()
Received 4 July 2025
Accepted for publication 8 October 2025
Published 15 October 2025 Volume 2025:18 Pages 14203—14215
DOI https://doi.org/10.2147/JIR.S548327
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Rongxue Wu
Yike Li,1,* Peng Li,2,* Qiang Tang,3,* Ting Jiao,4 Yanxiang Gao,5 Shuoyan An,5 Hao Jiang,3 Hui Cheng,6 Zixuan Yang,1 Jiahui Zhou,1 Yuxuan Sun,7 Yining Yang,6 Jingang Zheng1,5
1Department of Cardiology, China-Japan Friendship Hospital (Institute of Clinical Medical Sciences), Chinese Academy of Medical Sciences, Peking Union Medical College, Beijing, People’s Republic of China; 2Department of Cardiology, The Fifth Affiliated Hospital of Xinjiang Medical University, Urumqi, People’s Republic of China; 3Department of Cardiology, Peking University Shougang Hospital, Beijing, People’s Republic of China; 4Department of Cardiology, Xinjiang Medical University affiliated second hospital, Urumqi, People’s Republic of China; 5Department of Cardiology, China-Japan Friendship Hospital, Beijing, People’s Republic of China; 6Department of Cardiology, People’s Hospital of Xinjiang Uygur Autonomous Region, Urumqi, People’s Republic of China; 7Department of Cardiology, Peking University China-Japan Friendship School of Clinical Medicine, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jingang Zheng, Email [email protected] Yining Yang, Email [email protected]
Introduction: Hyperlipidemia, impaired glucose tolerance, and inflammatory status are critical contributors to the progression of coronary artery disease (CAD). Biomarkers associated with these pathways may predict clinical outcomes in dialysis-dependent CAD patients. This study aims to compare conventional lipid profiles, inflammatory markers, and insulin resistance-related indicators to evaluate their associations with mortality and prognostic performance in this high-risk population.
Methods: This multicenter retrospective cohort study included 1249 patients from January 2015 to June 2021. 864 patients were finally included in the analysis. Baseline lipid profiles, inflammatory markers, and insulin resistance-related indicator (the triglyceride-glucose [TyG] index) were analyzed.
Results: Among 864 patients, 252 deaths (29.2%) occurred over three years. Both the TyG index (hazard ratio [95% confidence interval]: 1.22 [1.03– 1.44], p=0.024) and inflammatory marker (neutrophil-to-lymphocyte ratio [NLR]: 1.02 [1.00– 1.04], p=0.038) were independently associated with mortality, whereas lipid profiles showed no significant association. Adding the TyG index or NLR to the Global Registry of Acute Coronary Events (GRACE) score (TyG c-index: 0.644 [0.609– 0.679]; NLR c-index: 0.642 [0.607– 0.677]) or baseline model (TyG c-index: 0.707 [0.676– 0.738]; NLR c-index: 0.705 [0.672– 0.738]) improved predictive performance. The combined model integrating TyG index and NLR demonstrated the highest discriminative ability for mortality prediction (GRACE score c-index: 0.660 [0.625– 0.695]; Baseline model c-index: 0.713 [0.682– 0.744]).
Conclusion: The findings indicate that systemic inflammation and insulin resistance are more significant risk factors for three-year mortality in dialysis-dependent CAD patients than dyslipidemia. This suggests that targeted anti-inflammatory therapies and regulation of glucose-lipid metabolism may offer greater benefits compared to conventional lipid-lowering strategies in this high-risk cohort.
Keywords: dialysis, coronary artery disease, inflammation, triglyceride-glucose index, all-cause mortality
Introduction
Patients undergoing dialysis experience an exceptionally high burden of cardiovascular mortality, with a risk that is 7 to 8 times greater than that of individuals with normal renal function.1 Risk evaluation tools, including the Global Registry of Acute Coronary Events (GRACE) score, are broadly applied in coronary artery disease (CAD) cohorts, yet they often fail to accurately predict the risks of heart attack and mortality in CAD patients on dialysis.2 This limitation highlights the pressing need for novel biomarkers that are specifically tailored to the unique pathophysiology of dialysis-dependent CAD.
Emerging evidence indicates a deviation from traditional cardiovascular risk paradigms in end-stage renal disease (ESRD). Chronic inflammation, driven by the accumulation of uremic toxins and repeated immune activation related to vascular access, accelerates atherosclerosis through endothelial injury and increased plaque vulnerability.3,4 Furthermore, dialysis patients exhibit a “reverse epidemiology” of lipid metabolism, where lower levels of low-density lipoprotein cholesterol (LDLC) paradoxically correlate with increased mortality. This term describes a common paradox in ESRD where the association of traditional risk factors with outcomes is reversed. This phenomenon likely reflects the malnutrition-inflammation complex syndrome rather than providing cardiovascular protection.5,6 Additionally, insulin resistance, as quantified by the triglyceride-glucose (TyG) index, has recently been associated with cardiovascular events in dialysis cohorts, suggesting a role for glucose-lipid dysregulation that is independent of traditional diabetes metrics.7
Current evidence lacks direct comparisons of lipid profiles, inflammatory markers, and the TyG index in predicting mortality among dialysis patients who have CAD, and their interactions under uremic conditions remain inadequately understood. Our multicenter cohort study aims to fill this knowledge gap by examining these biomarkers to improve risk stratification and guide targeted interventions in this high-risk group.
Method
Study Population
Data utilized in this study were derived from the Coronary Revascularization in Patients on Dialysis in China-Retrospective Registry (CRUISE-R, ClinicalTrials.gov entry: NCT05841082). Supplementary Table 1 provides details on the CRUISE-R study design. This national multicenter retrospective study was conducted across 30 medical centers in 12 provinces of China. It involved a total of 1,249 patients who were undergoing regular dialysis and had been diagnosed with CAD through coronary angiography. The study period extended from January 2015 to June 2021. Ethical approval was obtained from the Ethics Committee of the China-Japan Friendship Hospital (2020–112-K71). The ethics committee explicitly waived the requirement for informed consent due to the retrospective analysis. All data were handled in a strictly confidential and anonymized manner. In this particular analysis, we omitted 23 patients with tumors, 136 patients with active infections or autoimmune diseases, 21 patients with abnormal liver function (defined as liver enzyme levels more than three times the normal upper limit), 45 patients lacking routine blood indices, and 50 patients with triglyceride (TG) deficiency. 22 patients with blood glucose deficiency, 28 cases of suspected familial hypertriglyceridemia, with TG levels at or above 5.65 mmol/L (suspected familial hypertriglyceridemia), and 60 patients who were lost to follow-up (Figure 1). The final analysis included 864 participants. Researchers adhered to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement guidelines during the observational study.
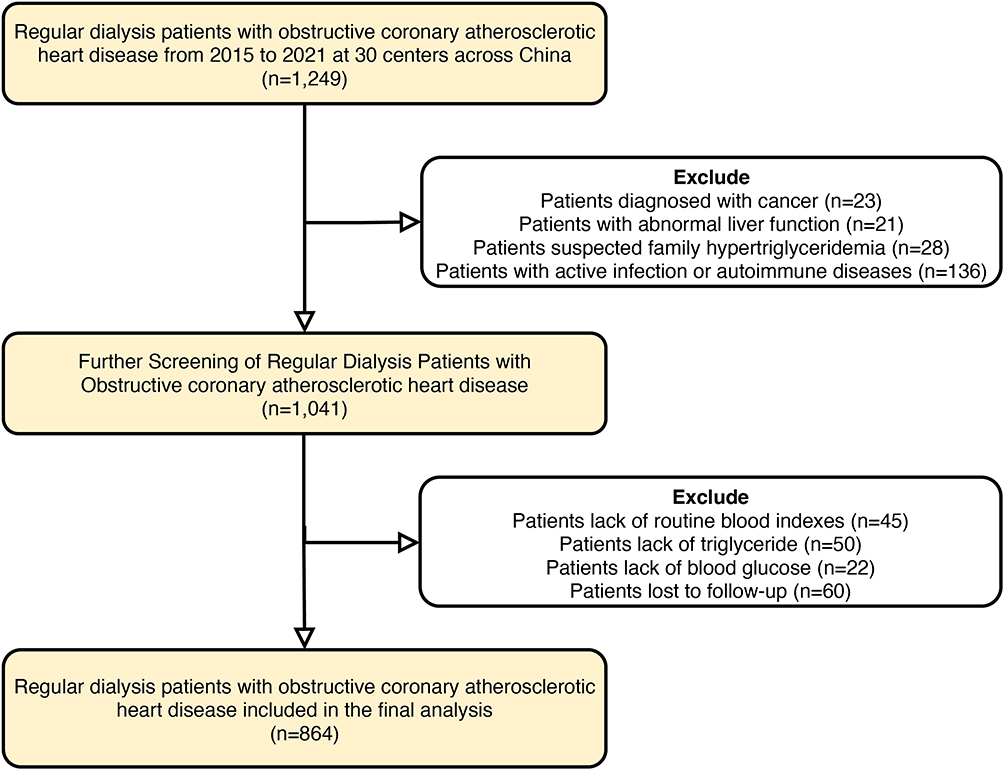 |
Figure 1 Flowchart of the patient inclusion and exclusion. |
Study Definition
In this investigation, trained study coordinators assembled data by examining the medical files of participants, which covered basic information, existing health conditions, heart-related background, heart performance, details of coronary artery disease, therapeutic measures, and significant medical occurrences. Experienced nursing professionals administered outpatient consultations and conducted telephone interviews using standardized forms to evaluate patient survival and clinical outcomes. Standardized follow-up procedure and consistent definitions for clinical endpoints were implemented to ensure uniform assessment of outcome events. In this context, dialysis patients were defined as those undergoing blood or peritoneal dialysis for a minimum of three months. Using values gathered within 24 hours of admission, the TyG index is calculated by first multiplying fasting triglyceride and fasting glucose levels, then dividing the result by 2, and finally taking the natural logarithm of that quotient.
Five inflammatory scores were calculated as follows: The neutrophil-to-lymphocyte ratio (NLR) was determined by dividing the neutrophil count by the lymphocyte count; The platelet-to-lymphocyte ratio (PLR) was calculated by dividing the platelet count by the lymphocyte count; The monocyte-to-lymphocyte ratio (MLR) was obtained by dividing the monocyte count by the lymphocyte count; The systemic immune-inflammation index (SII) was computed as the product of the platelet count and neutrophil count, divided by the lymphocyte count; The systemic immune-inflammation response index (SIIRI) was defined as the product of the neutrophil count, monocyte count, and platelet count, divided by the lymphocyte count.
The following calculations were made for five lipid-derived indices using lipid profiles, including total cholesterol (TC), TG, high-density lipoprotein cholesterol (HDLC), and LDLC collected within the first 24 hours of hospital admission. The atherogenic index of plasma (AIP) was calculated as the logarithm of the ratio of TG to HDLC; The lipoprotein combine index (LCI) was determined by multiplying TC, TG, and LDLC, and then dividing the product by HDLC; Castelli’s index-II (CRIII) was obtained by dividing LDLC by HDLC; The atherogenic index (AI) was calculated as the difference between TC and HDLC, divided by HDLC; The atherogenic combined index (ACI) was computed by multiplying TG by the difference between TC and HDLC, and then dividing the result by HDLC.
Outcomes
The endpoint was defined as mortality from any cause within a three-year period, with follow-up conducted via telephone by trained nursing staff.
Statistical Analysis
To compare the baseline characteristics between the two groups, the Mann–Whitney U-test was utilized for variables with non-normal distributions. For continuous variables that followed a normal distribution, the independent samples t-test was applied. Categorical variables were analyzed using the chi-square test (χ²). A significance level of P < 0.05 was set for two-tailed tests.
To examine the correlation between various scores and endpoint events, the scores were segmented into three tiers according to their tertile distribution, with each tier labeled as T1, T2, and T3. The Log rank test was subsequently utilized to compare the incidence of events among these three groups. Additionally, Cox regression models were employed, with the score initially treated as a continuous variable and subsequently as a categorical variable. The following variables were adjusted in the adjusted multivariate Cox model: age, sex, manifestations of coronary heart disease, systolic and diastolic blood pressure, hypertension, diabetes, atrial fibrillation, cerebrovascular disease, admission treatment method, left main CAD, three-vessel disease, heart rate, active smoking and pharmacological therapies including beta-blocker, statin, dual antiplatelet therapy, angiotensin-converting enzyme inhibitor (ACEI) or angiotensin II receptor blocker (ARB). The relationship between various scores and outcome events was further examined using a restricted cubic spline plot. The model’s precision and optimal cut-off point were assessed using the receiver-operating characteristic (ROC) curves. Calibration curves and Decision Curve Analysis (DCA) were also employed to assess the model’s predictive accuracy. To compare the discrimination of different scores for 3-year all-cause deaths, three metrics were calculated: Harrell’ concordance index, continuous net reclassification improvement (NRI) and integrated discrimination improvement (IDI). All statistical analyses were performed using R software (version 4.5.0).
Results
Characteristics of the Study Population
The study cohort comprised 864 participants, whose mean age was 61.8 years, and the majority (75.2%) were men. Of these, 58.3% were diagnosed with myocardial infarction, 93.5% had hypertension, and 53.8% had diabetes mellitus. Over the three-year follow-up period, 252 patients died from any cause, resulting in an all-cause mortality rate of 29.2%. Compared to survivors, those who experienced outcome events were older and had a higher incidence of myocardial infarction, atrial fibrillation, valvular disease, diabetes, and left main and three-vessel coronary artery disease. Lab tests showed that patients who died from any cause had higher blood glucose, white blood cell, and neutrophil counts when admitted, with no notable differences in blood lipid levels (Table 1).
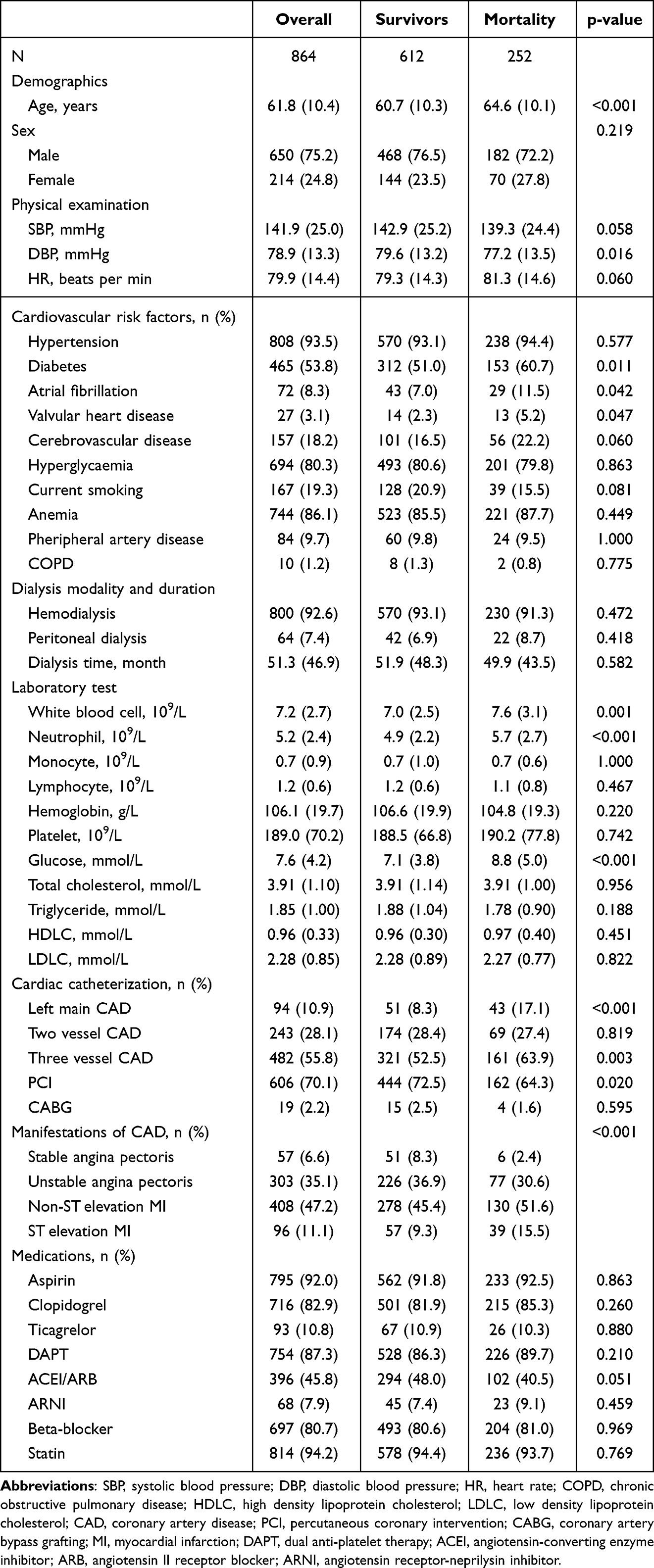 |
Table 1 Population Baseline |
Insulin Resistance, Lipid-Derived Index and Inflammation Score with All-Cause Death
The AUC was calculated to assess the prognostic value of 9 lipid-related indices and 9 inflammatory scores concerning all-cause mortality, with the results displayed in supplementary Figure 1. Notably, the inflammation score (NLR) and the lipid-related index (LDLC) demonstrated superior predictive performance for all-cause mortality (NLR: 0.601; LDLC: 0.521). Subsequently, participants were divided into three strata according to the tertiles of the TyG index, NLR, and LDLC, labeled as T1, T2, and T3. A notable variation in all-cause mortality was detected among individuals classified by the TyG index and NLR, whereas no significant prognostic difference was detected among patients grouped by LDLC levels (Figure 2).
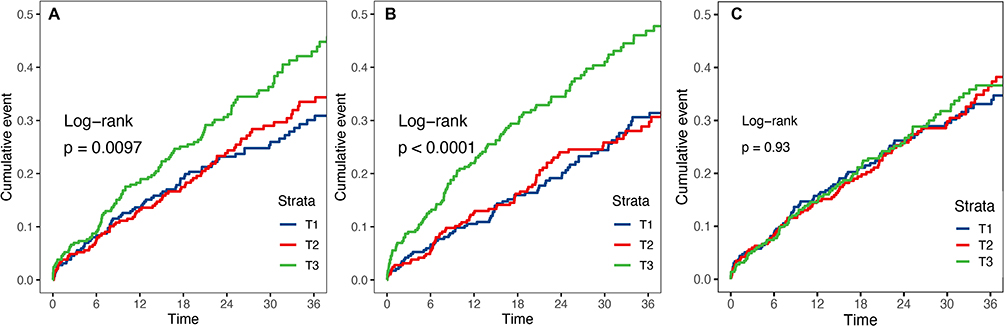 |
Figure 2 Cumulative event rate curves for mortality based on TyG index, NLR, and LDLC. (A) Cumulative event rate curves of TyG index. (B) Cumulative event rate curves of NLR. (C) Cumulative event rate curves of LDLC. Abbreviations: TyG index, triglyceride-glucose index; NLR, neutrophil - lymphocyte ratio; LDLC, low-density lipoprotein cholesterol. |
Correlation of TyG Index and NLR with Three-year Mortality
The results from the Cox proportional hazards models demonstrated that the TyG index is a significant independent risk factor for all-cause mortality (hazard ratio [HR]=1.22, 95% confidence interval [95% CI]:1.03–1.44, p=0.024), after accounting for multiple covariates (Table 2). As a categorical variable, the third tertile had a 40% greater risk of death relative to those in the lowest tertile (HR=1.40, 95% CI:1.01–1.93, p=0.041). NLR also emerged as a significant independent predictor of mortality (when evaluated continuously, HR=1.02, 95% CI:1.00–1.04, p=0.038; when categorized, T3 vs T1, HR=1.57, 95% CI:1.14–2.16, p=0.005). Figure 3 shows the dose-response relationships of TyG and NLR, both as continuous and categorical variables, with all-cause mortality over a 3-year span. The analysis revealed a notable dose-response link between the TyG index and NLR with overall mortality. Notably, the hazard of all-cause mortality escalated significantly once the TyG index exceeded 8.141. A comparable increase in mortality risk was also detected when the NLR value went above 2.207.
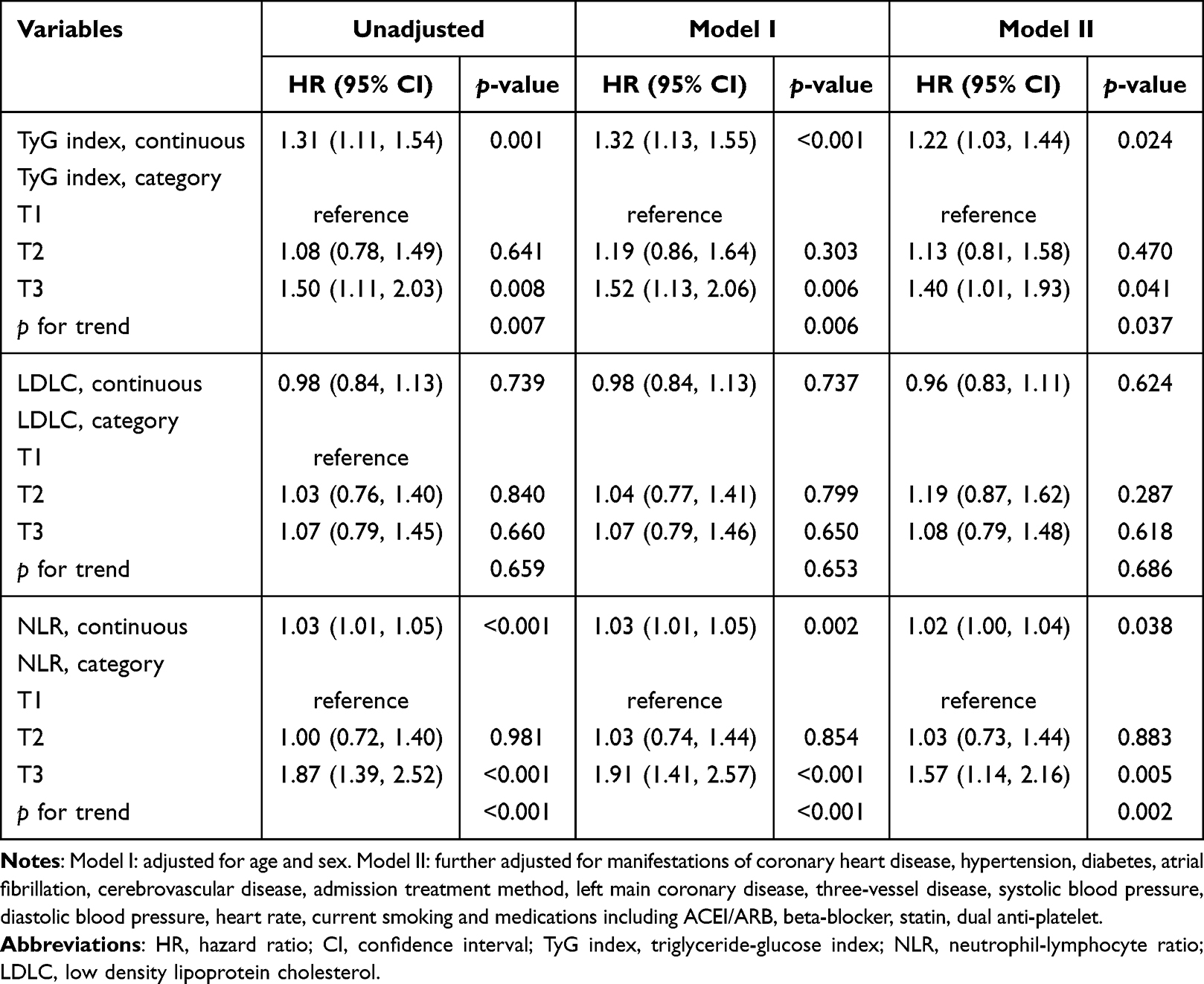 |
Table 2 Association of TyG Index, LDLC and NLR with 3-year All-Cause Mortality |
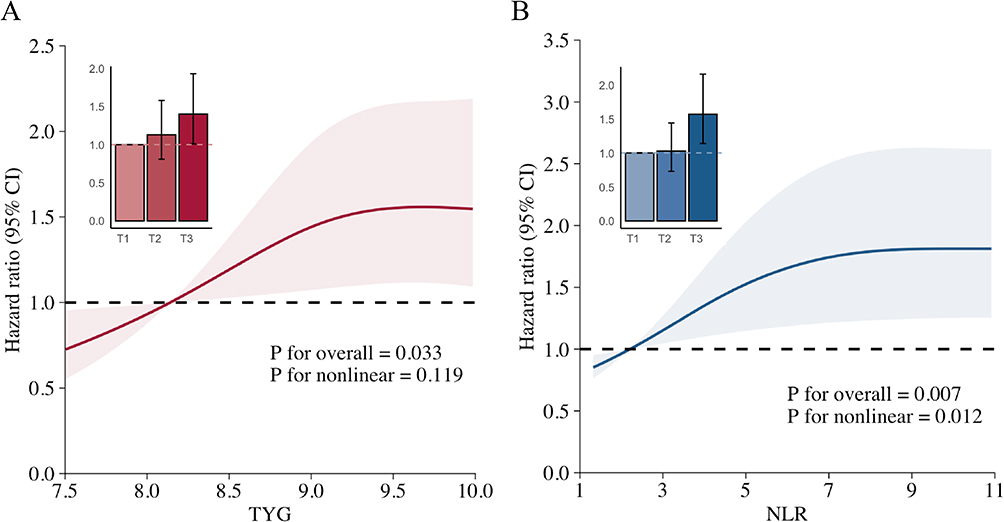 |
Figure 3 Dose - response relationship of TyG index and NLR with 3-year all-cause mortality. (A) The smooth curve fitting diagram of TyG index. (B) The smooth curve fitting diagram of NLR. Abbreviations: TyG index, triglyceride-glucose index; NLR, neutrophil - lymphocyte ratio. |
Predictive Performance of the TyG Index Combined with NLR
Since the TyG index and NLR are both linked to mortality risk, a correlation analysis was conducted, revealing a weak correlation between the two indices (correlation coefficient = 0.080, p = 0.021, Supplementary Figure 2). This weak correlation suggests that the TyG index and NLR likely capture distinct yet complementary pathophysiological pathways, and may have a synergistic effect in predicting prognosis in dialysis patients with CAD. Given these findings, we investigated whether combining the TyG index with NLR could provide superior predictive power for all-cause mortality compared to using each index separately. To determine the most effective thresholds for the TyG index and NLR in predicting all-cause mortality, we utilized ROC curve analysis (see Supplementary Figure 3). The TyG index was found to have an optimal threshold of 8.981, which corresponded to a 66.1% sensitivity and a 52.6% specificity. In the case of NLR, the ideal threshold was set at 4.941, yielding a sensitivity of 48.9% and a specificity of 68.6%. TyG index≥8.981 was classified as high TyG index, otherwise was low TyG index, and NLR was also divided. Reclassification revealed a marked difference in all-cause mortality across the four groups (Supplementary Figure 4). Even after considering multiple factors, individuals with elevated TyG index (HR=1.93, 95% CI:1.32–2.81, p<0.001) or NLR alone (HR=1.87,95% CI:1.21–2.87, p=0.005) had a higher risk of death compared to those with lower levels of both. Moreover, those who had elevated levels of both the TyG index and NLR faced a significantly increased risk of mortality (HR=2.48, 95% CI:1.68–3.66, p<0.001) as shown in Figure 4.
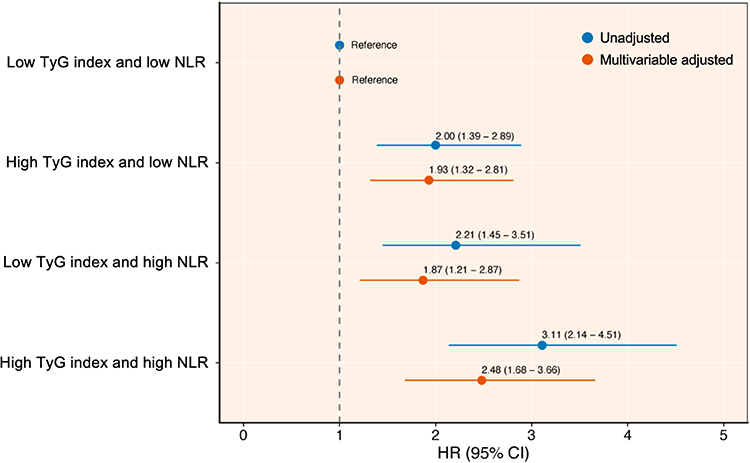 |
Figure 4 Forest plot of all-cause mortality in combination with TyG index and NLR. Multivariable adjusted for Model II in the Cox regression analysis. Abbreviations: TyG index, triglyceride-glucose index; NLR, neutrophil - lymphocyte ratio; HR, hazard ratio; CI, confidence interval. |
When the TyG index and NLR were reclassified into categorical variables based on their optimal thresholds to develop the predictive model, compared with TyG single index, the accuracy of the model can be significantly improved, which is specifically reflected in the increase of c-index (0.606 vs 0.561, p<0.001, Table 3). Compared with NLR alone, the c-index, NRI and IDI of the model were significantly higher (c-index: 0.606 vs 0.574, p<0.001; NRI: 0.190 [0.104–0.266], p<0.001; IDI: 0.020 [0.006–0.036], p<0.001), indicating improved accuracy and reclassification capability. Additionally, the TyG index and NLR, when integrated with GRACE scores or the baseline model, outperformed the original model or the original model paired with a single index (Table 4). Furthermore, both the calibration curves and DCA curves demonstrated that incorporating the TyG index and NLR into the GRACE model or the baseline model enhanced the predictive accuracy (Figure 5).
 |
Table 3 Predictive Performance of Combined TyG Index and NLR |
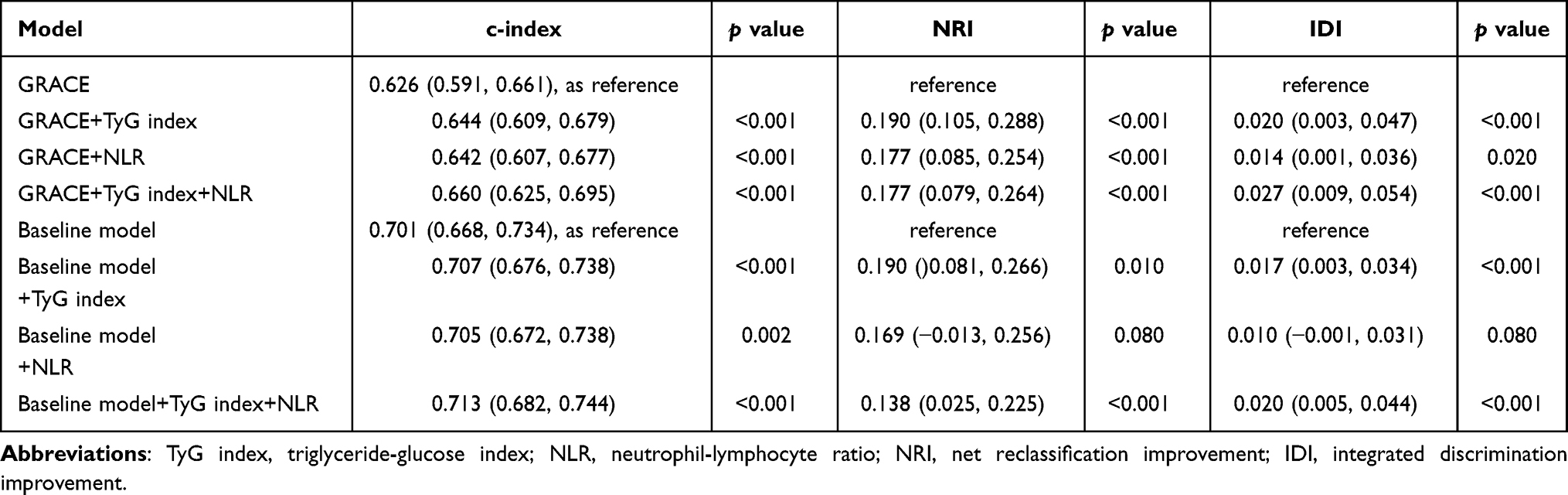 |
Table 4 The Incremental Effects of Incorporating the TyG Index and NLR to GRACE Score and a Baseline Risk Model on Prognostic Prediction |
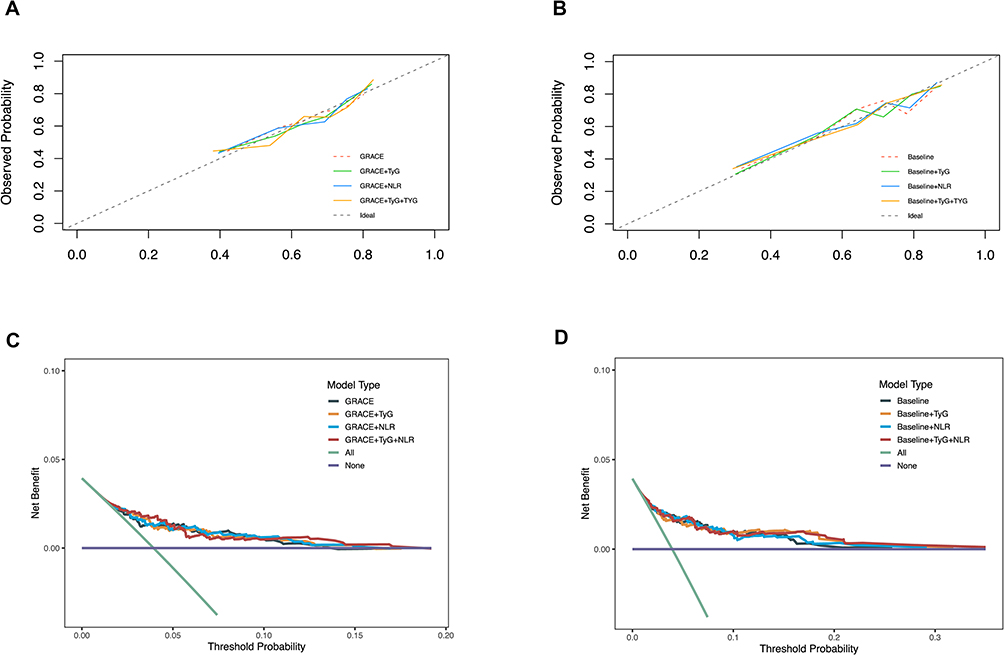 |
Figure 5 Calibration and Decision Curve Analysis (DCA) for the integration of the TyG index and NLR with the GRACE score or the baseline model. (A) Calibration curve of TyG index and NLR with GRACE score. (B) Calibration curve of TyG index and NLR with baseline model. (C) Decision curve of TyG index and NLR with GRACE score. (D) Decision curve of TyG index and NLR with baseline model. Abbreviations: TyG index, triglyceride-glucose index; NLR, neutrophil - lymphocyte ratio; GRACE score, Global Registry of Acute Coronary Events score. |
Subgroup Analysis and Sensitivity Analysis
Further subgroup investigations were conducted to examine how the TyG index and NLR relate to all-cause mortality within different population segments, including age, sex, diabetes mellitus, myocardial infarction, insulin treatment, and dialysis modality (Supplementary Figure 5). Across all subgroups, the results remained relatively consistent, with no significant interactions detected. Similar findings were observed for NLR, except within the dialysis modality subgroup, where a significant interaction was identified (p for interaction=0.031). Notably, only 64 patients were undergoing peritoneal dialysis, and within this cohort, higher NLR levels were tied to greater all-cause mortality risk (HR=1.22, 95% CI:1.07–1.39, p=0.003). However, the findings in the peritoneal dialysis subgroup (n=64 with 22 events) are severely limited by low statistical power and potential model overfitting.
To ensure the conclusions’ robustness, a sensitivity analysis was undertaken. At first, 23 patients who died in the hospital were omitted (Supplementary Table 2). Secondly, we excluded 59 patients with hypoglycemia (blood glucose<3.9mmol/L), 2 patients with leukopenia (neutrophil count <1×109), and 42 patients with lymphocytopenia (lymphocyte count <0.5×109). The analysis ultimately comprised 761 patients (Supplementary Table 3). When assessed in both continuous and categorical formats, the TyG index and NLR were significantly related to 3-year all-cause mortality, after accounting for multiple factors.
Discussion
In this multicenter retrospective cohort study comprising 864 dialysis-dependent patients with CAD, systemic inflammation (NLR: HR=1.02, 95% CI:1.00–1.04, p=0.038) and insulin resistance (TyG index, HR=1.22, 95% CI:1.03–1.44, p=0.024) emerged as predominant predictors of 3-year all-cause mortality, surpassing traditional lipid profiles (LDLC: HR=0.96, 95% CI:0.83–1.11, p=0.624). The joint assessment of the TyG index and NLR outperformed the predictive accuracy of evaluating individual biomarkers. The addition of the TyG index and NLR to the model considerably refined the predictive accuracy of both the GRACE score (c-index: 0.660 vs 0.626, p<0.001) and baseline models (c-index: 0.713 vs 0.701, p<0.001).
Our study provides a unique advance by validating a novel metabolic-inflammatory signature (TyG-NLR) specifically in a high-risk, understudied population: dialysis patients with CAD. This addresses a critical evidence gap, as findings from general ACS cohorts cannot be extrapolated to this unique population. These results challenge traditional cardiovascular risk paradigms in ESRD and are consistent with emerging evidence that underscores the distinct pathophysiology of uremic atherosclerosis.8,9 Our findings build upon previous research by directly comparing lipid, inflammatory, and metabolic biomarkers, while offering mechanistic and clinical insights into risk stratification for this high-risk population.7,10,11
Although lipid-lowering therapies are fundamental in the cardiovascular management of the general population,12,13 emerging clinical data show a disparity between standard lipid metrics and death rates in ESRD patients. In a randomized controlled trial involving hemodialysis patients, rosuvastatin significantly reduced LDLC levels (mean difference: −43 mg/dL) but did not confer a survival benefit.14 A meta-analysis assessing the effects of lipid-lowering treatments on clinical outcomes in chronic kidney disease has verified that statins do not have a significant impact on mortality risk for patients on dialysis.15 Additionally, new findings suggest that ceramide, a specific lipid metabolite, is essential in the advancement of atherosclerosis among those with kidney dysfunction.8 In alignment with these findings, our research did not find a standalone link between LDLC levels and all-cause mortality over three years (HR=0.96, 95% CI:0.83–1.11,p=0.624), indicating that traditional lipid-centric risk stratification may lack clinical significance in this population. Instead, TyG index - a surrogate for adipose tissue insulin resistance - emerged as a robust predictor in ESRD cohorts.7,16 Notably, our TyG index threshold (>8.141) corresponds with the cut-off values identified in non-dialysis CAD populations (8.840–9.037),17,18 suggesting a conserved metabolic risk pathway exacerbated by uremia.
Inflammatory biomarkers, including neutrophil, monocyte, and lymphocyte counts, have traditionally served as indicators of systemic inflammatory status. However, their individual variability can result in false negatives or delayed responses, particularly in chronic conditions. Recent advancements underscore the utility of composite indices derived from routine blood counts, such as the NLR, MLR, and PLR, which offer stable and cost-effective prognostic value for assessing the severity and outcomes of CAD.19–22 In our study comparing the prognostic performance of multiple inflammatory indices, NLR achieved the largest AUC value (0.601). In dialysis patients, NLR is associated with cardiovascular mortality (HR=1.03, 95% CI:1.01–1.05, p=0.002),10 an NLR of 3.5 was identified as the optimal cutoff for predicting death, with patients on dialysis above this threshold having a 1.7-fold increase in mortality.23 Our study further substantiates this evidence by illustrating the independent prognostic significance of NLR for long-term all-cause mortality in dialysis-dependent CAD patients (adjusted HR=1.02, 95% CI:1.00–1.04, p=0.038). Additionally, our identified optimal cutoff (NLR > 4.941) may indicate a higher baseline level of inflammation in dialysis populations with prevalent CAD.24
The elevated inflammatory burden reflected by NLR must be understood within the broader pathophysiological context of ESRD, where endothelial dysfunction emerges as the central orchestrator of cardiovascular disease and mortality. The uremic milieu, characterized by the accumulation of toxins, oxidative stress, and fluid overload, directly inflicts damage upon the vascular endothelium.25 A dysfunctional endothelium, in turn, becomes a prolific source of pro-inflammatory cytokines and adhesion molecules, creating a self-perpetuating cycle of systemic inflammation and immune cell activation that drives atherogenesis and plaque vulnerability.26 As recently highlighted by Prabhahar et al,27 this endothelial-centric inflammatory cascade is a hallmark of renal disease and a key therapeutic target.28
Inflammation and insulin resistance collectively contribute to cardiovascular risk through a complex bidirectional interaction, largely mediated by endothelial dysfunction. Pro-inflammatory signaling pathways, such as JNK/mTOR activation, impair adipose tissue functionality, leading to increased levels of free fatty acids and inflammatory cytokines while decreasing adiponectin, thereby intensifying insulin resistance.29 Conversely, insulin resistance amplifies inflammation via oxidative stress caused by high blood sugar levels and the accumulation of advanced glycation end products. This vicious cycle accelerates endothelial injury and plaque instability.30 Consistent with this paradigm, Cui et al demonstrated that patients with increased TyG index and high-sensitivity C-reactive protein had a 30% greater risk of CAD than those with lower levels of these markers,31 underscoring the synergistic interplay between insulin resistance and inflammation in CVD pathogenesis.
In dialysis populations, where chronic inflammation and insulin resistance are markedly amplified by uremic toxins and metabolic dysregulation,32,33 dual-biomarker models integrating these pathways may offer superior risk stratification. Our study addresses this gap by demonstrating that the combined TyG-NLR model outperforms either biomarker alone in predicting all-cause mortality. Furthermore, integrating TyG index and NLR into the GRACE score (0.660 vs 0.626, p<0.001) or baseline clinical models (0.713 vs 0.701, p<0.001) significantly enhanced predictive performance, with C-index improvements. The TyG-NLR signature offers exceptional clinical practicality. It is derived from routine, low-cost parameters, requiring no specialized assays. This makes it an accessible and immediately implementable tool for risk stratification in global clinical practice, potentially helping to identify high-risk patients for more intensive management.
To explore the mechanistic context of our findings, we hypothesize that the synergy between TyG and NLR reflects a self-reinforcing cycle where uremic milieu-aggravated insulin resistance primes innate immune activation, elevating neutrophil counts and suppressing lymphocytes, which in turn exacerbates metabolic dysfunction through cytokine-mediated impairment of insulin signaling. This entire pathway is both a cause and a consequence of endothelial dysfunction, ultimately culminating in major adverse cardiovascular events. Future studies are warranted to validate this pathophysiological model by: 1) correlating the TyG-NLR signature with direct measures of vascular inflammation and specific inflammatory cytokines in serially collected samples; and 2) investigating in experimental models whether therapeutic modulation of one pathway (eg, using SGLT2 inhibitors to improve metabolism or anti-IL-6 agents to dampen inflammation) elicits concordant changes in the other, ultimately leading to improved outcomes.
Strengths and Limitations
Our study uniquely focuses on the high-risk population of dialysis-dependent patients with CAD, leveraging a nationwide multicenter retrospective cohort spanning 30 Chinese centers to comprehensively evaluate the prognostic relevance of lipid profiles, inflammatory markers, and insulin resistance. By demonstrating the lack of independent association between conventional lipid parameters and 3-year all-cause mortality, we reinforce the paradigm shift away from lipid-centric risk assessment in this population. Crucially, we identified a synergistic prognostic effect of inflammation (NLR) and insulin resistance (TyG index), with their combined model achieving superior discriminative performance. This underscores the clinical utility of integrating routine, cost-effective biomarkers to refine risk stratification in dialysis-complicated CAD.
This study has several limitations that need to be recognized. First, this retrospective study may harbor residual confounding and selection bias. Second, the moderate sample size limits the power for subgroup analyses. Third, the levels of the TyG index and NLR were measured at a single time point upon study enrollment. This retrospective design limits our ability to capture the dynamic changes of these biomarkers over time and to assess their time-dependent association with mortality. Furthermore, our study participants were exclusively recruited from Chinese centers, which may limit the generalizability of our findings to other ethnic populations with differing genetic backgrounds, dietary habits, and healthcare systems. The specific cut-off values of the TyG-NLR signature we identified may require validation in other ethnic cohorts. Finally, while we adjusted for the use of major drug classes (statins, antiplatelet agents, ACEI/ARBs), we lacked data on other anti-inflammatory therapies. Therefore, we cannot fully rule out some unmeasured confounding effects of pharmacotherapy. Further prospective randomized studies are essential to substantiate this conclusion.
Conclusion
In this multicenter cohort of dialysis-dependent CAD patients, systemic inflammation (NLR) and insulin resistance (TyG index) emerged as dominant predictors of 3-year all-cause mortality, while traditional lipid profiles showed no independent prognostic value. The combined TyG-NLR model significantly improved risk stratification beyond GRACE score or baseline model, underscoring the synergistic interplay between metabolic dysregulation and chronic inflammation in this high-risk population.
Our findings advocate for a paradigm shift toward dual-pathway risk assessment. Looking forward, prospective studies are essential to validate these thresholds. Moreover, our results illuminate a compelling therapeutic possibility: the TyG-NLR signature could potentially identify patients for trials with agents that target both metabolism and inflammation (e.g., SGLT2 inhibitors, IL-6 antagonists). Ultimately, interventional research is needed to determine if ameliorating this metabolic-inflammatory axis translates into improved survival.
Data Sharing Statement
The corresponding author Jingang Zheng can supply the relevant data upon reasonable request.
Ethics Approval and Informed Consent
The study adhered to the principles of the Declaration of Helsinki and received approval from the Ethics Committee at China-Japan Friendship Hospital (2020-112-K71). The ethics committee explicitly waived the requirement for informed consent due to the retrospective analysis. All data were handled in a strictly confidential and anonymized manner.
Acknowledgments
The authors thank all study participants and the research staff for their essential contributions to this work.
Funding
Capital’s Founds for Health Improvement and Research (No. 2022-1-4062). Beijing Research Ward Construction Clinical Research Project (2022-YJXBF-04-03). National High Level Hospital Clinical Research Funding (2024-NHLHCRF-YS-01). National Key Clinical Specialty Construction Project (No. 2020-QTL-009).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Writing Group for the CKD Prognosis Consortium, Grams ME, Coresh J, Matsushita K, et al. Estimated glomerular filtration rate, albuminuria, and adverse outcomes: an individual-participant data meta-analysis. JAMA. 2023;330(13):1266–1277. doi:10.1001/jama.2023.17002
2. Gurm HS, Gore JM, Anderson FA, et al. Comparison of acute coronary syndrome in patients receiving versus not receiving chronic dialysis (from the global registry of acute coronary events [GRACE] registry). Am J Cardiol. 2012;109(1):19–25. doi:10.1016/j.amjcard.2011.07.062
3. Kane J, Vos WG, Bosmans LA, et al. Peritoneal dialysis aggravates and accelerates atherosclerosis in Uremic ApoE-/- mice. J Am Heart Assoc. 2024;13(14):e034066. doi:10.1161/JAHA.123.034066
4. Wakamatsu T, Yamamoto S, Yoshida S, Narita I. Indoxyl sulfate-induced macrophage toxicity and therapeutic strategies in uremic atherosclerosis. Toxins. 2024;16(6):254. doi:10.3390/toxins16060254
5. Park J, Ahmadi SF, Streja E, et al. Obesity paradox in end-stage kidney disease patients. Progress Cardiovasc Dis. 2014;56(4):415–425. doi:10.1016/j.pcad.2013.10.005
6. Ebert T, Qureshi AR, Lamina C, et al. Time-dependent lipid profile inversely associates with mortality in hemodialysis patients - independent of inflammation/malnutrition. J Intern Med. 2021;290(4):910–921. doi:10.1111/joim.13291
7. Xie E, Ye Z, Wu Y, et al. The triglyceride-glucose index predicts 1-year major adverse cardiovascular events in end-stage renal disease patients with coronary artery disease. Cardiovasc Diabetol. 2023;22(1):292. doi:10.1186/s12933-023-02028-7
8. Zhang S, Lin H, Wang J, et al. Sensing ceramides by CYSLTR2 and P2RY6 to aggravate atherosclerosis. Nature. 2025.
9. Curaj A, Vanholder R, Loscalzo J, et al. Cardiovascular consequences of uremic metabolites: an overview of the involved signaling pathways. Circ Res. 2024;134(5):592–613. doi:10.1161/CIRCRESAHA.123.324001
10. Turkmen K, Guney I, Yerlikaya FH, Tonbul HZ. The relationship between neutrophil-to-lymphocyte ratio and inflammation in end-stage renal disease patients. Ren Fail. 2012;34(2):155–159. doi:10.3109/0886022X.2011.641514
11. Stompór T, Pasowicz M, Sulłowicz W, et al. An association between coronary artery calcification score, lipid profile, and selected markers of chronic inflammation in ESRD patients treated with peritoneal dialysis. Am J Kidney Dis. 2003;41(1):203–211. doi:10.1053/ajkd.2003.50005
12. Virani SS, Newby LK, Arnold SV, et al. 2023 AHA/ACC/ACCP/ASPC/NLA/PCNA guideline for the management of patients with chronic coronary disease: a report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation. 2023;148(9):e9–119. doi:10.1161/CIR.0000000000001168
13. Byrne RA, Rossello X, Coughlan JJ, et al. 2023 ESC Guidelines for the management of acute coronary syndromes. Eur Heart J. 2023;44(38):3720–3826. doi:10.1093/eurheartj/ehad191
14. Fellström BC, Jardine AG, Schmieder RE, et al. Rosuvastatin and cardiovascular events in patients undergoing hemodialysis. N Engl J Med. 2009;360(14):1395–1407. doi:10.1056/NEJMoa0810177
15. Liao G, Wang X, Li Y, et al. Antidyslipidemia pharmacotherapy in chronic kidney disease: a systematic review and Bayesian Network meta-analysis. Pharmaceutics. 2022;15(1):6. doi:10.3390/pharmaceutics15010006
16. Tuo J, Li Z, Xie L. Association between triglyceride-glucose index and clinical outcomes among patients with chronic kidney disease: a meta-analysis. BMC Nephrol. 2025;26(1):61. doi:10.1186/s12882-025-03984-w
17. Siverio-Morales O, Mora-Fernández C, Hernández-Carballo C, et al. Predictive value of triglyceride-glucose index for the evaluation of coronary artery disease severity and occurrence of major adverse cardiovascular events. Am J Physiol Heart Circ Physiol. 2025;328(1):H14–20. doi:10.1152/ajpheart.00684.2024
18. Ye Z, An S, Gao Y, et al. Association between the triglyceride glucose index and in-hospital and 1-year mortality in patients with chronic kidney disease and coronary artery disease in the intensive care unit. Cardiovasc Diabetol. 2023;22:110. doi:10.1186/s12933-023-01843-2
19. Tudurachi B-S, Anghel L, Tudurachi A, Sascău RA, Stătescu C. Assessment of inflammatory hematological ratios (NLR, PLR, MLR, LMR and monocyte/HDL-cholesterol ratio) in acute myocardial infarction and particularities in young patients. Int J Mol Sci. 2023;24(18):14378. doi:10.3390/ijms241814378
20. Angkananard T, Anothaisintawee T, McEvoy M, Attia J, Thakkinstian A. Neutrophil lymphocyte ratio and cardiovascular disease risk: a systematic review and meta-analysis. Biomed Res Int. 2018;2018:2703518. doi:10.1155/2018/2703518
21. J H, Bian X, Song C, et al. High neutrophil to lymphocyte ratio with type 2 diabetes mellitus predicts poor prognosis in patients undergoing percutaneous coronary intervention: a large-scale cohort study. Cardiovasc Diabetol. 2022;21(1):156. doi:10.1186/s12933-022-01583-9
22. Dziedzic EA, Gąsior JS, Tuzimek A, et al. Investigation of the Associations of Novel Inflammatory Biomarkers-Systemic Inflammatory Index (SII) and Systemic Inflammatory Response Index (SIRI)-With the Severity of Coronary Artery Disease and Acute Coronary Syndrome Occurrence. Int J Mol Sci. 2022;23(17):9553. doi:10.3390/ijms23179553
23. Li H, Lu X, Xiong R, Wang S. High Neutrophil-to-Lymphocyte Ratio Predicts Cardiovascular Mortality in Chronic Hemodialysis Patients. Mediators Inflamm. 2017;2017:9327136. doi:10.1155/2017/9327136
24. Trionfetti F, Marchant V, González-Mateo GT, et al. Novel Aspects of the Immune Response Involved in the Peritoneal Damage in Chronic Kidney Disease Patients under Dialysis. Int J Mol Sci. 2023;24(6):5763. doi:10.3390/ijms24065763
25. Querfeld U, Mak RH, Pries AR. Microvascular disease in chronic kidney disease: the base of the iceberg in cardiovascular comorbidity. Clin Sci (Lond). 2020;134(12):1333–1356. doi:10.1042/CS20200279
26. Jebari-Benslaiman S, Galicia-García U, Larrea-Sebal A, et al. Pathophysiology of Atherosclerosis. Int J Mol Sci. 2022;23(6):3346. doi:10.3390/ijms23063346
27. Prabhahar A, Batta A, Hatwal J, Kumar V, Ramachandran R, Batta A. Endothelial dysfunction in the kidney transplant population: current evidence and management strategies. World J Transplant. 2025;15(1):97458. doi:10.5500/wjt.v15.i1.97458
28. Marrone G, Cornali K, Di Lauro M, et al. Innovative Treatments to Counteract Endothelial Dysfunction in Chronic Kidney Disease Patients. Biomedicines. 2024;12(5):1085. doi:10.3390/biomedicines12051085
29. Aroor AR, McKarns S, DeMarco VG, Guanghong J, Sowers JR. Maladaptive immune and inflammatory pathways lead to cardiovascular insulin resistance. Metabolism. 2013;62(11):1543–1552. doi:10.1016/j.metabol.2013.07.001
30. Poznyak A, Grechko AV, Poggio P, Myasoedova VA, Alfieri V, Orekhov AN. The Diabetes Mellitus–Atherosclerosis Connection: the Role of Lipid and Glucose Metabolism and Chronic Inflammation. Int J Mol Sci. 2020;21(5):1835. doi:10.3390/ijms21051835
31. Cui C, Liu L, Qi Y, et al. Joint association of TyG index and high sensitivity C-reactive protein with cardiovascular disease: a national cohort study. Cardiovasc Diabetol. 2024;23:156. doi:10.1186/s12933-024-02244-9
32. Ebert T, Neytchev O, Witasp A, Kublickiene K, Stenvinkel P, Shiels PG. Inflammation and Oxidative Stress in Chronic Kidney Disease and Dialysis Patients. Antioxid Redox Signal. 2021;35(17):1426–1448. doi:10.1089/ars.2020.8184
33. Lambie M, Bonomini M, Davies SJ, Accili D, Arduini A, Zammit V. Insulin resistance in cardiovascular disease, uremia, and peritoneal dialysis. Trends Endocrinol Metab. 2021;32(9):721–730. doi:10.1016/j.tem.2021.06.001
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Systemic Immune Inflammatory Response Index Can Predict the Clinical Prognosis of Patients with Initially Diagnosed Coronary Artery Disease
Li Y, Bai G, Gao Y, Guo Z, Chen X, Liu T, Li G
Journal of Inflammation Research 2023, 16:5069-5082
Published Date: 2 November 2023
Discordance Between Neutrophil to Lymphocyte Ratio and High Sensitivity C-Reactive Protein to Predict Clinical Events in Patients with Stable Coronary Artery Disease: A Large-Scale Cohort Study
He J, Song C, Zhang R, Yuan S, Li J, Dou K
Journal of Inflammation Research 2023, 16:5439-5450
Published Date: 20 November 2023
Associations Between Estimated Pulse Wave Velocity and Five-Year All-Cause Mortality in Patients with Atherosclerotic Cardiovascular Disease with and without Standard Modifiable Risk Factors: Evidence From NHANES 1999-2016
Li X, Chen Y, Liu B, Ye M, Liu B, Lu L, Guo R
Clinical Epidemiology 2024, 16:367-377
Published Date: 28 May 2024
Inflammatory Gene Signature Identified by Machine Algorithms Reveals Novel Biomarkers of Coronary Artery Disease
Liu X, Zhang Y, Wang Y, Xu Y, Xia W, Liu R, Xu S
Journal of Inflammation Research 2025, 18:2033-2044
Published Date: 10 February 2025
Inflammatory Biomarkers in Coronary Artery Disease: Insights From Mendelian Randomization and Transcriptomics

Xiao Z, Cheng X, Bai Y
Journal of Inflammation Research 2025, 18:3177-3200
Published Date: 4 March 2025