Back to Journals » Journal of Pain Research » Volume 18
Transcutaneous Electrical Acupoint Stimulation (TEAS) Facilitates Postoperative Recovery in Day Lung Cancer Surgery: A Randomized Controlled Trial
Authors Wu S ![]() , Lou J, Zou H, Wang W, Zhang Y, Xu Y, Hou X, Wu J
, Lou J, Zou H, Wang W, Zhang Y, Xu Y, Hou X, Wu J ![]()
Received 19 March 2025
Accepted for publication 10 June 2025
Published 17 June 2025 Volume 2025:18 Pages 3017—3026
DOI https://doi.org/10.2147/JPR.S529193
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
Siyin Wu,1,* Jieqiong Lou,2,* Houdong Zou,3,* Wei Wang,1 Yunyun Zhang,1 Yunhua Xu,4 Xumin Hou,2 Jingxiang Wu1
1Department of Anesthesiology, Shanghai Chest Hospital, Shanghai Jiao Tong University, School of Medicine, Shanghai, People’s Republic of China; 2President’s Office, Shanghai Chest Hospital, Shanghai Jiao Tong University, School of Medicine, Shanghai, People’s Republic of China; 3Department of Science and Education, Shanghai Chest Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, People’s Republic of China; 4Department of Shanghai Lung Cancer Center, Shanghai Chest Hospital, Shanghai Jiao Tong University, School of Medicine, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jingxiang Wu, Department of Anesthesiology, Shanghai Chest Hospital, Shanghai Jiao Tong University, School of Medicine, No. 241 West Huaihai Road, Shanghai, People’s Republic of China, Tel +86 18930857186, Email [email protected] Xumin Hou, President’s Office, Shanghai Chest Hospital, Shanghai Jiao Tong University, School of Medicine, Shanghai, People’s Republic of China, Tel +86-021-62821990, Email [email protected]
Background: Day thoracic surgery requires effective analgesia and a rapid recovery. This study evaluated whether Transcutaneous Electrical Acupoint Stimulation (TEAS) reduces postoperative pain and analgesic use in lung cancer surgery.
Methods: In this randomized, sham-controlled trial at a tertiary hospital in Shanghai, 100 patients (18– 70 years old, ASA I–II) who underwent day lung cancer surgery (video-assisted thoracoscopic pulmonary wedge resection) were enrolled. Participants were randomized to receive either TEAS or sham TEAS in the Post-Anesthesia Care Unit. The TEAS group received 30 minutes of stimulation at Hegu (LI4) and Neiguan (PC6), whereas the sham group received electrode placement without stimulation. Primary outcome was pain intensity 24 h after surgery, measured using the visual analog scale (VAS). Secondary outcomes were VAS scores at 1 h and 12 h post-surgery, analgesic consumption, incidence of moderate-to-severe pain (VAS score > 4), incidence of postoperative nausea and vomiting (PONV), Quality of Recovery (QoR-15) scores, and safety events.
Results: The TEAS group had significantly lower VAS scores at 1 hour (0.94 vs 1.84, p = 0.006), 12 hours (2.00 vs 5.40, p < 0.001), and 24 hours (1.72 vs 4.02, p < 0.001). The incidence of moderate-to-severe pain within 12 hours was reduced (12.0% vs 74.0%, p < 0.001). Analgesic consumption was lower in the TEAS group. The QoR-15 scores at 24 h were higher in the TEAS group (130.8 vs 115.9, p < 0.001). No significant differences were observed in PONV, length of hospital stay, or adverse events.
Conclusion: TEAS reduces postoperative pain and analgesic use, improves the recovery quality in lung cancer surgery, and supports its integration into ERAS protocols.
Trial Registration: ChiCTR2200066600. https://www.chictr.org.cn/showproj.html?proj=187035.
Keywords: transcutaneous electrical acupoint stimulation, postoperative pain, day surgery, lung cancer, enhanced recovery after surgery
Introduction
Day thoracic surgery, specifically lung resection procedures aimed at same-day or next-day discharge, aligns with principles of Enhanced Recovery After Surgery (ERAS). ERAS protocols are designed to optimize patient outcomes by minimizing surgical stress and promoting faster recovery. The adoption of day thoracic surgery offers numerous advantages, including a shortened hospital stay, reduced healthcare costs, and improved patient satisfaction.1,2 However, day thoracic surgery presents unique challenges, such as significant postoperative pain and the critical impact on respiratory function, which necessitate more rigorous and effective pain management strategies.3–6 Traditional analgesic methods such as intravenous opioids often require prolonged administration, which is incompatible with the rapid discharge goals of day surgery. Moreover, opioids are associated with adverse effects such as nausea, vomiting, sedation, and respiratory depression, which can hinder recovery. Alternative techniques, such as single-dose nerve blocks, provide limited pain relief and may require additional intervention.4,7,8
Transcutaneous Electrical Acupoint Stimulation (TEAS) has emerged as a promising non-pharmacological analgesic method on labor pain, cancer-related pain, myofascial pain syndrome, and postoperative pain.9–12 TEAS involves the application of electrical stimulation to specific acupoints, such as Hegu (LI14) and Neiguan (PC6), which have been reported to alleviate pain and improve recovery outcomes.13–15 Recent research has shown that electroacupuncture may alleviate pain by blocking central sensitization mediated by the BDNF/TrkB signaling pathway.16 Unlike traditional acupuncture, TEAS is noninvasive, poses no risk of infection or bleeding, and can be easily administered in the Post-Anesthesia Care Unit (PACU) without the need for prolonged intervention.14 Previous studies have demonstrated the efficacy of TEAS in reducing postoperative pain and opioid consumption in various surgical settings.9,17–19 However, its application in daily thoracic surgery remains unexplored. This randomized controlled trial aimed to investigate the efficacy of TEAS in enhancing postoperative recovery and facilitating early discharge of patients undergoing surgery for lung cancer. The primary hypothesis was that TEAS would effectively alleviate postoperative pain and enhance recovery quality, thereby supporting its integration into ERAS protocols for daily thoracic surgery.
Methods
Aim, Design, and Setting
This study was a randomized controlled trial conducted at Shanghai Chest Hospital, Shanghai, China. The study was approved by the Institutional Review Board of Shanghai Chest Hospital (IRB #KS (Y) 23025) and was conducted in accordance with the Nuremberg Code, Declaration of Helsinki, and relevant Chinese regulations. Informed consent was obtained from all participants. This trial was registered in the Chinese Clinical Trial Registry (No. ChiCTR2200066600).
Participants
Eligible patients were scheduled for ambulatory video-assisted thoracoscopic pulmonary wedge resection under general anesthesia, aged 18–70 years, and with ASA of Anesthesiologists grade I or II. The inclusion criteria were normal liver and kidney functions, compliance with treatment and follow-up, and clear communication ability.
Participants were excluded if they had previously undergone surgical intervention along the meridian or had a history of local infection, trauma, or significant scarring at meridian points. Additional exclusion criteria included the presence of upper or lower limb nerve damage, a long history of sedation, use of analgesics or antidepressants, a history of surgery associated with chronic incision pain, pregnancy or breastfeeding, and participation in any similar trial (including the TEAS trial) within 3 months prior to the current trial. Patients who were unable to complete the study plan because of language difficulties, infectious diseases, or other medical histories were also excluded.
Randomization and Blinding
Eligible participants (n=100) were randomly assigned (1:1) to receive either TEAS or sham TEAS upon arrival at the Post-Anesthesia Care Unit (PACU). Randomization was performed using a computer-generated list of random numbers created by an independent third party. A professionally trained anesthesiologist administered the interventions according to a serial number corresponding to the random number table All clinicians and researchers collecting or analyzing the data were blinded to the group assignments. To enhance blinding, the sham TEAS group received electrode patches affixed without electrical stimulation to simulate the sensory experience without actual electrical current. Complete blinding of all subjects was attempted; however, the sensation of electrical stimulation can bring about some perceptual differences, and this difference may affect the interpretation of the result. Nonetheless, considering that the participants’ consciousness level was basically low when they entered the PACU, the weak current intensity might not be detected by the patients. In the event of serious adverse events, the investigator or clinician could re-evaluate the patient’s treatment and provide appropriate relief, leading to withdrawal from the trial.
Anesthetic and Surgical Management
Ultrasound-guided thoracic paravertebral nerve blocks were performed at T4-7 levels. After anesthesia induction, endotracheal intubation was performed, adopting one-lung ventilation and a protective lung ventilation strategy.20 The patients’ core temperature was maintained stable by using 41°C infusion heating and a warm air blower, and the bispectral index (BIS) was maintained between 40–60 throughout the operation. Vasoactive agents were administered to maintain the heart rate and blood pressure within 20% of the baseline values, and 200 mg of sugammadex sodium was administered postoperatively. Sufentanil, propofol, and rocuronium bromide were used for anesthesia induction, whereas propofol, remifentanil, rocuronium bromide, and dexmedetomidine were continuously administered during the operation. Ropivacaine (150 mg) is used for TPVB,21 but postoperative patient-controlled analgesia (PCA) is not routinely applied. No additional postoperative analgesics were administered unless the postoperative VAS(visual analogue scale) score exceeded 4. Paracetamol and oxycodone with acetaminophen tablets or intravenous parecoxib sodium (40 mg) were administered.22 More details can be found in Supplementary Material 1.
Intervention
Upon arrival in the PACU, participants were randomly assigned to the TEAS or Sham groups. Prior to anesthesia induction, all patients were informed about the potential use of TEAS for postoperative pain management and were shown the electrode patches to be applied to specific acupoints, ensuring awareness and minimizing placebo effects.
In the TEAS group, an experienced anesthesiologist administered Transcutaneous Electrical Acupoint Stimulation at the bilateral Hegu (LI14) and Neiguan (PC6) points23 using an acupoint nerve stimulator (Model: HANS-200A; Nanjing Jisheng Medical Technology Co., Ltd.). The device delivered fixed-intensity electrical stimulation at frequencies of 2 hz and 10 hz and a current of 12–20 mA for 30 min.24 Stimulation began immediately upon PACU arrival, while the patients were still under residual anesthesia, ensuring consistency and minimizing the placebo effects.
In the sham TEAS group, electrode patches were affixed to the same acupoints without electrical stimulation for 30 min. The presence of electrode patches and prior briefings created a comparable experience, maintained blinding, and reduced psychological biases.
Administering TEAS during residual anesthesia reduced the likelihood of participants discerning their group based on sensation. TEAS participants might experience numbness and acid distension at acupoints if they become more awake, reinforcing the perception of receiving active treatment. Conversely, sham TEAS participants, despite no active stimulation, might believe that they received TEAS due to the electrode patches and initial briefing, further minimizing placebo-related bias.
TEAS was implemented in accordance with the Standards for Reporting of Controlled Trials in Acupuncture (STRICTA) guidelines to ensure methodological rigor and reproducibility.23
Outcomes
The primary outcome was pain intensity 24 h after surgery, measured using visual analog scale (VAS) scores (0–10).
Secondary outcomes included VAS scores at 1 h and 12 h post-surgery, incidence of moderate to severe pain (VAS >4) in the first 12 h, analgesic consumption, incidence of postoperative nausea and vomiting (PONV) within 1 hour, 1–12 hours, and 12–24 hours post-surgery, Quality of Recovery (QoR-15)25 scores at 24 h post-surgery, length of hospital stay, and safety.
Statistical Analysis
We evaluated the distributions of continuous variables using histograms and QQ plots and checked for normality using the Shapiro–Wilk test. Normally distributed continuous variables were expressed as mean ± standard deviation (SD) and compared using Student’s t-test. Asymmetrically distributed variables were presented as medians (interquartile range [IQR]) and compared using the Mann–Whitney U-test. Categorical variables are expressed as absolute numbers (percentages) and compared using Pearson’s χ2 test with continuity correction or Fisher’s exact test. Mixed linear models were used for repeated measures, considering the treatment group, time, and their interaction as fixed effects with a random intercept for each participant. Estimates were summarized as mean differences (MD) or relative risks (RR) with 95% confidence intervals (CI). A 2-factor repeated measures ANOVA was used to analyze the VAS scores at each time point post-surgery. The Kolmogorov–Smirnov test was used to assess data normality. Statistical significance was set at a 95% confidence limit and p < 0.05. All outcomes were evaluated in the intention-to-treat (ITT) population, which included all subjects in the full analysis set (FAS). Statistical analyses were performed using SPSS version 21 (IBM, Armonk, NY, USA), Stata 14 (StataCorp, TX, USA), and GraphPad Prism (version 7.0, GraphPad Software, USA).
Calculation of Sample Sizes
The sample size was determined based on a 25% reduction in pain scores with a statistical power of 90% and a type I error of 5%. This calculation was based on preliminary data, where patients receiving standard general anesthesia had a mean VAS pain score of 4.05 with a standard deviation of 1.95 in the first 24 h postoperatively. A 25% reduction corresponds to a VAS score decrease of at least 1 point (from 4 to 3), which is considered clinically significant as it transitions pain from moderate to mild levels. To account for the potential loss to follow-up (estimated at approximately 20%), 50 patients per treatment group were included, resulting in a total of 100 participants.
Results
Participant Flow
Between January 5, 2023, and May 28, 2023, 132 patients admitted to the day ward of the Chest Hospital Affiliated to Shanghai Jiao Tong University School of Medicine for minimally invasive lung cancer surgery were screened. Among them, 32 refused to sign an informed consent form or met at least one exclusion criterion. Consequently, 100 eligible patients were selected and randomly assigned to two groups: 50 in the TEAS group and 50 in the control group. All patients successfully completed the final follow-up, with no data loss, except for three patients who were discharged within 24 hours post-surgery and could not be contacted for data collection at the 24-hour mark. All the results were included in the final analysis according to the ITT principle (Figure 1). Baseline demographics and clinical characteristics were well balanced between the two groups (Table 1).
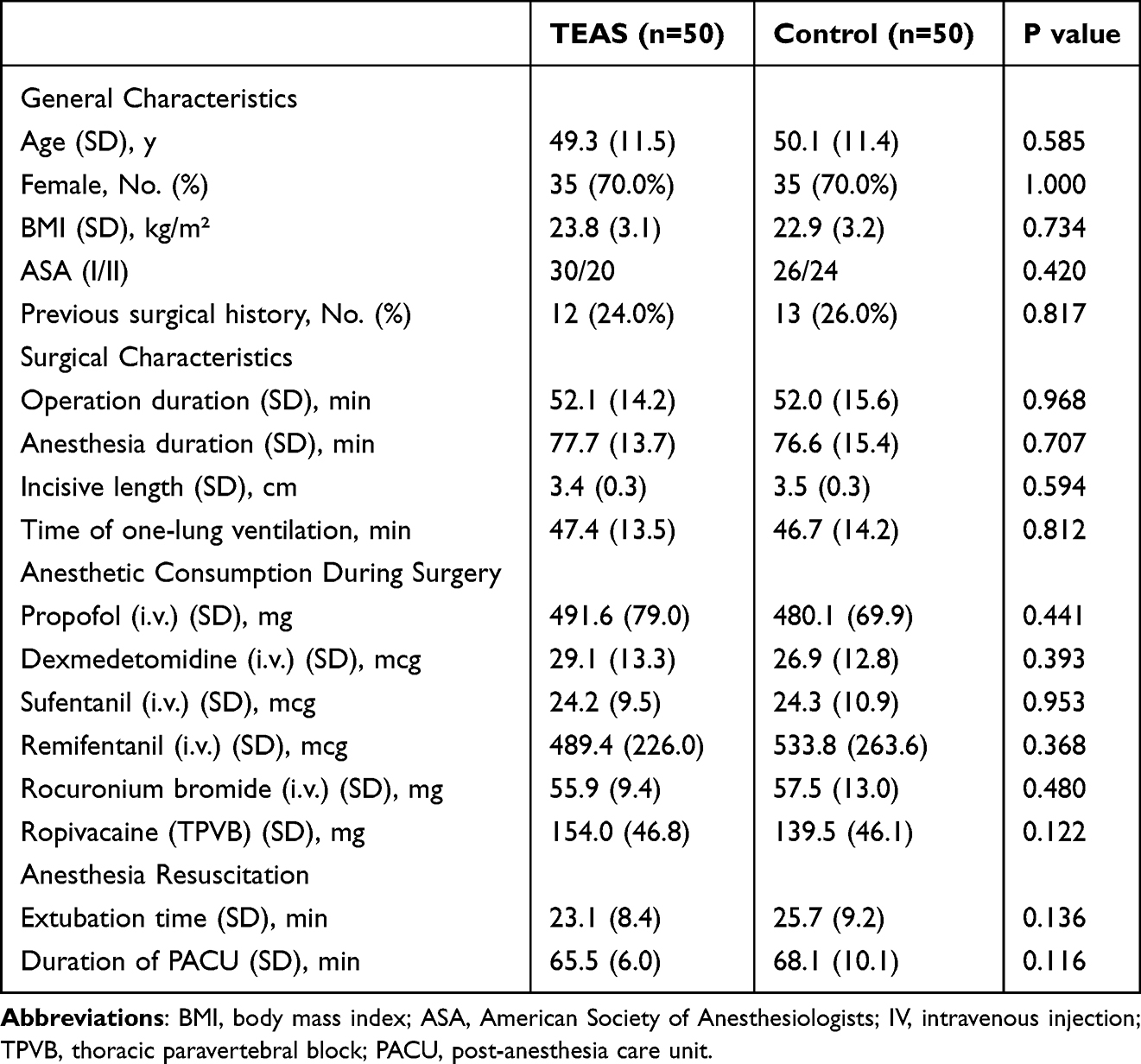 |
Table 1 Baseline Demographics and Clinical Characteristics |
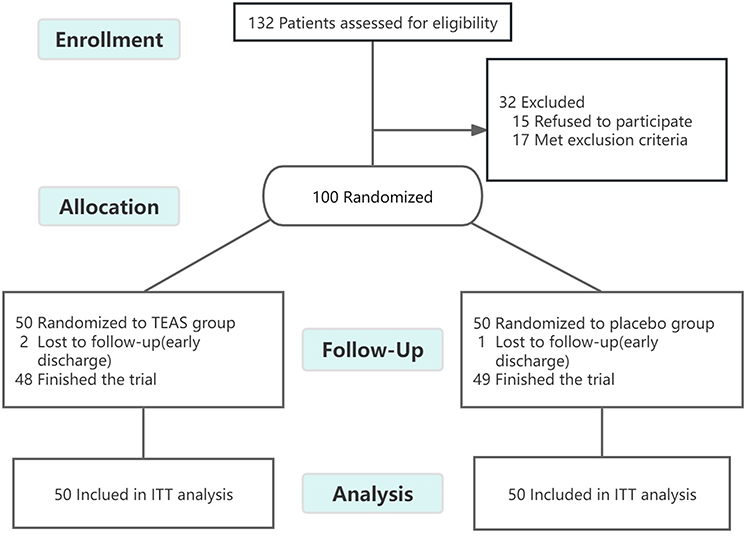 |
Figure 1 CONSORT flow diagram of the study participants. Abbreviation: ITT, intention-to-treat. |
Primary Outcome
The primary outcome of this study was pain intensity 24 hours after surgery, as measured by the VAS score. The VAS score at 24 hours post-surgery was significantly lower in the TEAS group compared to the control group (TEAS 1.7 ± 0.9 vs control 4.0 ± 1.4, p < 0.001) (Table 2).
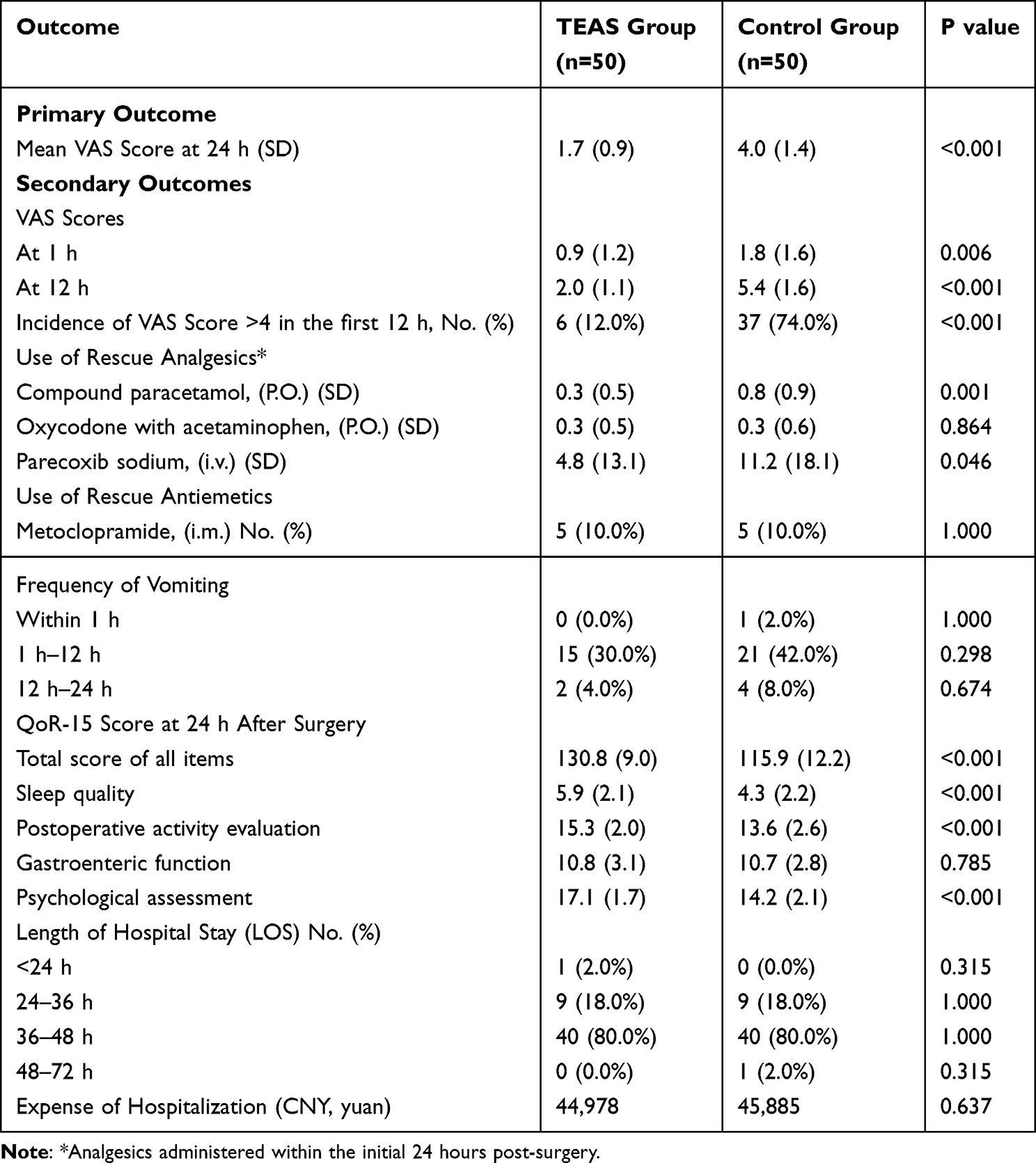 |
Table 2 Primary and Secondary Outcomes of TEAS vs Control in Facilitating Postoperative Recovery in Day Lung Cancer Surgery |
Secondary Outcomes
The level of pain was low in both groups 1 hour after surgery, but the VAS score in the TEAS group was significantly lower than in the control group (TEAS 0.9 ± 1.2 vs control 1.8 ± 1.6, p = 0.006). Similarly, the VAS score at 12 hours after surgery was significantly lower in the TEAS group compared to the control group (TEAS 2.0 ± 1.1 vs control 5.4 ± 1.6, p < 0.001). The pain level was highest 12 h postoperatively, with the prevalence of moderate-to-severe pain (VAS >4) being markedly higher in the control group than in the TEAS group within the first 12 h after surgery (TEAS 12.0% vs control 74.0%, p < 0.001) (Table 2).
In terms of postoperative analgesic use, the dose of oral compound paracetamol in the TEAS group was significantly lower than in the control group (TEAS 0.3 ± 0.5 tablets vs control 0.8 ± 0.9 tablets, p = 0.001). The oral dose of oxycodone with acetaminophen was similar between the TEAS and control groups (TEAS 0.3 ± 0.5 tablets vs control 0.3 ± 0.6 tablets, p = 0.864). The postoperative intravenous parecoxib sodium dose was significantly lower in the TEAS group than in the control group (TEAS 4.8 ± 13.1 mg vs control 11.2 ± 18.1 mg, p = 0.046) (Table 2).
Postoperative vomiting primarily occurred 1–12 hours postoperatively in both groups. Notably, none of the patients in the TEAS group vomited within 1 h after the intervention, whereas one patient in the control group vomited within 1 h. The incidence of vomiting was similar between the TEAS and control group 1–12 hours after surgery. (TEAS group: 15 patients vs control group: 21 patients, p = 0.298). Between 12–24 hours after surgery, the number of patients experiencing vomiting was relatively low, with no significant difference between the two groups (TEAS: 2 patients vs control: 4 patients, p = 0.674). Patients with severe vomiting were administered 10 mg metoclopramide intramuscularly, and there was no significant difference in the number of patients who received metoclopramide between the two groups (TEAS: 5 patients vs control: 5 patients, p = 1.000) (Table 2).
Short-term recovery quality was higher in the TEAS group than in the control group, with the QoR-15 score at 24 h post-surgery being significantly higher in the TEAS group than in the control group (TEAS 130.8 ± 9.0 vs control 115.9 ± 12.2, p < 0.001). Similarly, the scores for sleep quality were higher in the TEAS group (TEAS 5.9 ± 2.1 vs control 4.3 ± 2.2, p < 0.001), indicating that TEAS can remarkably enhance the sleep condition of patients within 24 hours after surgery. The recovery of motor function was better in the TEAS group than in the control group (TEAS 15.3 ± 2.0 vs control 13.6 ± 2.6, p < 0.001). There was no significant difference in gastrointestinal function recovery between the two groups (TEAS 10.8 ± 3.1 vs control 10.7 ± 2.8, p = 0.785). In terms of psychological assessment, the score was significantly higher in the TEAS group (TEAS 17.1 ± 1.7 vs control 14.2 ± 2.1, p < 0.001), indicating lower levels of anxiety and depression in the TEAS group (Table 2).
There were no significant differences in the mean length of hospital stay and hospitalization costs between the two groups. In addition to nausea, vomiting, and postoperative pain, the most common adverse event was dizziness, with a comparable incidence between the two groups (TEAS: 8 patients vs control: 10 patients, p > 0.05). TEAS generally has few and mild adverse reactions, mainly including local skin reactions such as itching and erythema, as well as pain or local discomfort, and none of these adverse reactions were observed. No other serious adverse events were observed during the trial (Table 2).
Discussion
Our results demonstrated that TEAS significantly reduced pain intensity 24 h post-surgery, as evidenced by the lower VAS scores compared to the control group. Additionally, TEAS was associated with a lower incidence of moderate-to-severe pain within the first 12 h after surgery, reduced need for certain analgesics, and improved overall recovery quality as measured by the QoR-15 score. However, there was no significant difference in the incidence of postoperative vomiting, use of oxycodone and acetaminophen, length of hospital stay, or hospitalization expense between the two groups.
This study addressed the critical gap in postoperative pain management in patients undergoing thoracic surgery. To the best of our knowledge, this is the first randomized controlled clinical trial to investigate the use of transcutaneous electrical acupoint stimulation (TEAS) in day thoracic surgery. Chen et al investigated the postoperative analgesic effect of TEAS following conventional minimally invasive lung cancer surgery and documented that VAS scores, opioid consumption, and the incidence of nausea and vomiting were significantly reduced-24–48 hours after surgery in the TEAS group treated with patient-controlled intravenous analgesia (PCIA).26 Due to earlier discharge, the day of lung surgery requires higher demands for postoperative analgesia within 24 h under the premise of ERAS. However, unlike traditional thoracic surgery, it cannot use higher doses of opioid drugs or maintain long-term PCIA.5,27 Therefore, this trial predominantly focused on the effect of short-term TEAS treatment on early postoperative recovery of patients without PCIA.
Our results revealed that the VAS scores of the TEAS and control groups peaked within 24 h after surgery, approximately 12 h postoperatively. In the early postoperative period (1–8 hours), the intensity of pain was relatively low, likely because of the ongoing effect of thoracic paravertebral nerve block.28,29 As the paravertebral block effect gradually waned, inflammation, edema, and nerve injury around the surgical incision peaked 12 h post-surgery, potentially leading to a “rebound pain” phenomenon. The TEAS group showed significantly lower VAS scores at 1, 12, and 24 h postoperatively than did the control group. Additionally, the incidence of moderate-to-severe pain (VAS score >4) within the first 12 h after surgery was significantly lower in the TEAS group than in the sham TEAS group (12.0% vs 74.0%, p < 0.001). These findings indicate that TEAS effectively mitigates postoperative pain within the first 24 h, enhances hospitalization experience, and contributes to postoperative recovery.
Interestingly, while an earlier systematic review corroborated that TEAS can reduce the frequency and dosage of postoperative opioid usage,30,31 there was no significant difference in the oral doses of oxycodone and acetaminophen between the two groups of patients in this trial. Although opioids are recommended for postoperative remedial analgesia, the use of TPVB and requirement for rapid recovery after surgery may have partially reduced the need for opioids, resulting in no significant difference between the two groups.
In addition, our study observed that postoperative vomiting largely occurred 1–12 hours after surgery, which may be related to stimulation of the vagus nerve following the surgical operation and the residual effect of opioids.32,33 Compared with the control group, the incidence of vomiting 1–12 hours after surgery was lower in the TEAS group (30.0% vs 42.0%), but the difference was not statistically significant. Although TEAS has been shown to lower the incidence of postoperative nausea and vomiting14,26,34 a study by Cynthia et al35 reported that neither acupuncture nor TEAS effectively inhibited the gastrointestinal gag reflex. The potential mechanisms by which TEAS alleviates postoperative vomiting (POV) include local inhibition of somatic nerve signals, inhibition of motor efferent (vagus) signals, relaxation responses, and placebo effects.36 However, the effectiveness of these mechanisms may depend on the choice of the stimulation point. In this study, PC 6 and ST 36 were selected as therapeutic targets, consistent with previous studies.35
In contrast, the QoR-15 score was significantly higher in the TEAS group than in the control group (130.8 vs 115.9), suggesting that TEAS can promote early postoperative recovery, which has been corroborated by a large number of previous studies.17,37 Among these, TEAS significantly improved the sleep quality of lung cancer patients undergoing day surgical interventions in the early postoperative period, promoted the recovery of postoperative motor function, and alleviated the stress and anxiety levels of patients in the 24-hour postoperative period. Nevertheless, TEAS did not significantly improve gastrointestinal function during the early postoperative period, suggesting that it cannot significantly inhibit POV. There were no significant differences between the two groups in terms of the mean length of stay and hospitalization costs. In addition to nausea and vomiting, the most common adverse event was dizziness; however, this difference was not statistically significant. Neither group of patients developed postoperative pulmonary complications (PPCs), which is consistent with the findings of other studies.38 In general, our study highlights the safety of TEAS.
Recent advances in multimodal analgesia for day thoracic surgery have emphasized the importance of combining various analgesic techniques to enhance recovery and minimize opioid consumption.39–41 TEAS, as a non-pharmacological intervention, TEAS fits well into this paradigm by providing effective pain relief and improving patient outcomes without side effects associated with opioids. Future research should continue to explore the integration of TEAS with other analgesic modalities to optimize postoperative care during thoracic surgery.
Nonetheless, our trial had some limitations that cannot be overlooked. First, owing to the inherent limitations of trial conditions and techniques, we could not fully blind patients while they were awake, potentially leading to a bias in subjective sensations (numbness and distension elicited by electrical stimulation), although similar previous studies partially circumvented this problem by applying intraoperative electrical stimulation.42 Future resolutions to this challenge may depend on advancements in TEAS instrument design. Second, due to the shorter hospitalization time and faster operation speed of day-ward patients, the treatment duration of TEAS was short in this trial, and its efficacy was mainly assessed within 24 hours after surgery. Consequently, we were unable to comprehensively evaluate the advantages and disadvantages of TEAS during day lung surgery. Nevertheless, based on our results, we posit that a short period of TEAS stimulation contributes to the postoperative recovery after daytime chest surgery. Finally, we employed uniform TEAS stimulation intensities (2 hz and 10 hz, 12–20 mA) to ensure the effectiveness of stimulation. Individualized settings were not considered to prevent patients from easily perceiving whether they received actual TEAS during the testing process, which might have interfered with the accuracy of the results owing to the placebo effects. However, this approach has been adopted in the most recent TEAS-related studies. Further large-sample studies are required to validate our results.
Conclusion
In summary, TEAS serves as an effective nonpharmacological intervention for managing postoperative pain and enhancing recovery quality in patients undergoing lung cancer surgery. Its integration into ERAS protocols perhaps offer significant benefits by reducing pain intensity and analgesic requirements, thereby facilitating a faster and more comfortable recovery. Nevertheless, further multicenter trials are needed to confirm these findings, explore long-term outcomes, and establish standardized protocols for TEAS application in diverse clinical settings.
Abbreviations
ERAS, Enhanced Recovery After Surgery; TEAS, Transcutaneous Electrical Acupoint Stimulation; VAS, Visual Analogue Scale; PACU, Post-Anesthesia Care Unit; PONV, Postoperative Nausea and Vomiting; QoR-15, Quality of Recovery-15; ASA, American Society of Anesthesiologists; PCIA, Patient-Controlled Intravenous Analgesia; TPVB, Thoracic Paravertebral Block; PPCs, Postoperative Pulmonary Complications; ST36, Zusanli (an acupoint); LI4, Hegu (an acupoint); PC6, Neiguan (an acupoint); IRB, Institutional Review Board; ANOVA, Analysis of Variance.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The study was approved by the Institutional Review Board of Shanghai Chest Hospital (IRB #KS (Y) 23025). Informed consent was obtained from all participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Fundamental Research Funds for the Central Universities (YG2024LC10), Shanghai Hospital Association Hospital Management Research Fund (x2022179), and National Natural Science Foundation of China (82373226).
Disclosure
The authors declare that they have no competing interests. This paper has been uploaded to SSRN as a preprint: https://ssrn.com/abstract=4889532.
References
1. Tovar EA, Roethe RA, Weissig MD, Lloyd RE, Patel GR. One-day admission for lung lobectomy: an incidental result of a clinical pathway. Ann Thorac Surg. 1998;65(3):803–806. doi:10.1016/S0003-4975(97)01381-7
2. Kulkarni S, Harsoor SS, Chandrasekar M, et al. Consensus statement on anaesthesia for day care surgeries. Indian J Anaesth. 2017;61(2):110–124. doi:10.4103/ija.IJA_659_16
3. Linden PA, Perry Y, Worrell S, et al. Postoperative day 1 discharge after anatomic lung resection: a society of thoracic surgeons database analysis. J Thorac Cardiovasc Surg. 2020;159(2):667–78.e2. doi:10.1016/j.jtcvs.2019.08.038
4. Towe CW, Thibault DP, Worrell SG, et al. Factors associated with successful postoperative day one discharge after anatomic lung resection. Ann Thorac Surg. 2021;112(1):221–227. doi:10.1016/j.athoracsur.2020.07.059
5. Rae A. Reasons for delayed patient discharge following day surgery: a literature review. Nurs Stand. 2016;31(11):42–51. doi:10.7748/ns.2016.e10292
6. Jiang L, Lei T, Zhou K, Ma H, Che G. Pivotal role of video-assisted thoracoscopic surgery in improving survival outcome of stage I non-small cell lung cancer in day surgery patients. Thorac Cancer. 2021;12(21):2865–2872. doi:10.1111/1759-7714.14145
7. Moorthy A, Eochagáin AN, Dempsey E, et al. Postoperative recovery with continuous erector spinae plane block or video-assisted paravertebral block after minimally invasive thoracic surgery: a prospective, randomised controlled trial. Br J Anaesth. 2023;130(1):e137–e47. doi:10.1016/j.bja.2022.07.051
8. Shen C, Che G. Thoracic day surgery versus thoracic inpatient surgery for treatment of patients with lung cancer: a systematic review and meta-analysis. J Cardiothorac Surg. 2023;18(1):341. doi:10.1186/s13019-023-02462-4
9. Chang XL, Liu XM, An LX, Zheng JY, Zhang K. Effects of transcutaneous electrical acupoint stimulation (TEAS) on postoperative pain in patients undergoing gastric and esophageal ESD surgery: a study protocol for a prospective randomized controlled trial. BMC Complement Med Ther. 2023;23(1):253. doi:10.1186/s12906-023-04075-9
10. Dowswell T, Bedwell C, Lavender T, Neilson JP. Transcutaneous electrical nerve stimulation (TENS) for pain relief in labour. Cochrane Database Syst Rev. 2009;2009(2):Cd007214.
11. Lyu Z, Tian S, Bao G, et al. Transcutaneous electrical acupoint stimulation for cancer-related pain management in patients receiving chronic opioid therapy: a randomized clinical trial. Support Care Cancer. 2023;32(1):16. doi:10.1007/s00520-023-08240-1
12. Galasso A, Urits I, An D, et al. A comprehensive review of the treatment and management of myofascial pain syndrome. Curr Pain Headache Rep. 2020;24(8):43. doi:10.1007/s11916-020-00877-5
13. Qin J, Ye X, Ye C, et al. The effect of transcutaneous electrical acupoint stimulation on high-risk patients with PONV undergoing laparoscopic gynecologic surgery: a randomized controlled trial. J Clin Med. 2023;12(3):1192. doi:10.3390/jcm12031192
14. Chen J, Tu Q, Miao S, Zhou Z, Hu S. Transcutaneous electrical acupoint stimulation for preventing postoperative nausea and vomiting after general anesthesia: a meta-analysis of randomized controlled trials. Int J Surg. 2020;73:57–64. doi:10.1016/j.ijsu.2019.10.036
15. Liu J, Zhang K, Zhang Y, et al. Perioperative transcutaneous electrical acupoint stimulation reduces postoperative pain in patients undergoing thoracoscopic surgery: a randomized controlled trial. Pain Res Manag. 2024;2024:5365456. doi:10.1155/2024/5365456
16. Xue M, Sun YL, Xia YY, Huang ZH, Huang C, Xing GG. Electroacupuncture modulates spinal BDNF/TrκB signaling pathway and ameliorates the sensitization of dorsal horn WDR neurons in spared nerve injury rats. Int J Mol Sci. 2020;21(18):6524. doi:10.3390/ijms21186524
17. Song B, Chang Y, Li Y, Zhu J. Effects of transcutaneous electrical acupoint stimulation on the postoperative sleep quality and pain of patients after video-assisted thoracoscopic surgery: a prospective, randomized controlled trial. Nat Sci Sleep. 2020;12:809–819. doi:10.2147/NSS.S270739
18. Lu Z, Wang Q, Sun X, et al. Transcutaneous electrical acupoint stimulation before surgery reduces chronic pain after mastectomy: a randomized clinical trial. J Clin Anesth. 2021;74:110453. doi:10.1016/j.jclinane.2021.110453
19. Liu LY, Su Y, Wang RR, et al. Transcutaneous electrical acupoint stimulation benefits postoperative pain relief of oocyte retrieval: a randomized controlled trial. J Integr Med. 2024;22(1):32–38. doi:10.1016/j.joim.2024.01.005
20. Goligher EC, Jonkman AH, Dianti J, et al. Clinical strategies for implementing lung and diaphragm-protective ventilation: avoiding insufficient and excessive effort. Intensive Care Med. 2020;46(12):2314–2326. doi:10.1007/s00134-020-06288-9
21. Sandeep B, Huang X, Li Y, Xiong D, Zhu B, Xiao Z. A comparison of regional anesthesia techniques in patients undergoing video-assisted thoracic surgery: a network meta-analysis. Int J Surg. 2022;105:106840. doi:10.1016/j.ijsu.2022.106840
22. Garmi G, Parasol M, Zafran N, Rudin M, Romano S, Salim R. Efficacy of single wound infiltration with bupivacaine and adrenaline during cesarean delivery for reduction of postoperative pain: a randomized clinical trial. JAMA Network Open. 2022;5(11):e2242203. doi:10.1001/jamanetworkopen.2022.42203
23. MacPherson H, Altman DG, Hammerschlag R, et al. Revised STandards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA): extending the CONSORT statement. J Evid Based Med. 2010;3(3):140–155. doi:10.1111/j.1756-5391.2010.01086.x
24. Chen Y, Yao Y, Wu Y, Dai D, Zhao Q, Qiu L. Transcutaneous electric acupoint stimulation alleviates remifentanil-induced hyperalgesia in patients undergoing thyroidectomy: a randomized controlled trial. Int J Clin Exp Med. 2015;8(4):5781–5787.
25. Kleif J, Waage J, Christensen KB, Gögenur I. Systematic review of the QoR-15 score, a patient- reported outcome measure measuring quality of recovery after surgery and anaesthesia. Br J Anaesth. 2018;120(1):28–36. doi:10.1016/j.bja.2017.11.013
26. Chen J, Zhang Y, Li X, et al. Efficacy of transcutaneous electrical acupoint stimulation combined with general anesthesia for sedation and postoperative analgesia in minimally invasive lung cancer surgery: a randomized, double-blind, placebo-controlled trial. Thoracic Cancer. 2020;11(4):928–934. doi:10.1111/1759-7714.13343
27. Ghosh-Dastidar MB, Deshpande RP, Rajagopal K, Andersen D, Marrinan MT. Day surgery unit thoracic surgery: the first UK experience. Eur J Cardiothorac Surg. 2011;39(6):1047–1050. doi:10.1016/j.ejcts.2010.09.032
28. Yeung JH, Gates S, Naidu BV, Wilson MJ, Gao Smith F. Paravertebral block versus thoracic epidural for patients undergoing thoracotomy. Cochrane Database Syst Rev. 2016;2(2):Cd009121. doi:10.1002/14651858.CD009121.pub2
29. Pace MM, Sharma B, Anderson-Dam J, Fleischmann K, Warren L, Stefanovich P. Ultrasound-guided thoracic paravertebral blockade: a retrospective study of the incidence of complications. Anesthesia Analg. 2016;122(4):1186–1191. doi:10.1213/ANE.0000000000001117
30. Meng D, Mao Y, Song QM, et al. Efficacy and Safety of Transcutaneous Electrical Acupoint Stimulation (TEAS) for postoperative pain in laparoscopy: a systematic review and meta-analysis of randomized controlled trials. Evid Based Complement Alternat Med. 2022;2022:9922879. doi:10.1155/2022/9922879
31. Ao L, Shi J, Bai Y, Zhang S, Gan J. Effects of transcutaneous electrical acupoint stimulation on perioperative immune function and postoperative analgesia in patients undergoing radical mastectomy: a randomized controlled trial. Exp Ther Med. 2021;21(3):184. doi:10.3892/etm.2021.9615
32. Apfel CC, Meyer A, Orhan-Sungur M, Jalota L, Whelan RP, Jukar-Rao S. Supplemental intravenous crystalloids for the prevention of postoperative nausea and vomiting: quantitative review. Br J Anaesth. 2012;108(6):893–902. doi:10.1093/bja/aes138
33. Mihara T, Tojo K, Uchimoto K, Morita S, Goto T. Reevaluation of the effectiveness of ramosetron for preventing postoperative nausea and vomiting: a systematic review and meta-analysis. Anesthesia Analg. 2013;117(2):329–339. doi:10.1213/ANE.0b013e31829847a1
34. Liu YY, Duan SE, Cai MX, Zou P, Lai Y, Li YL. Evaluation of transcutaneous electroacupoint stimulation with the train-of-four mode for preventing nausea and vomiting after laparoscopic cholecystectomy. Chin J Integr Med. 2008;14(2):94–97. doi:10.1007/s11655-008-0094-4
35. Diep C, Karibe H, Goddard G, Phan Y, Shubov A. Acupuncture and transcutaneous electrical acupoint stimulation do not suppress gag reflex. Med Acupuncture. 2021;33(5):353–357. doi:10.1089/acu.2021.0008
36. Lee A, Done ML. Stimulation of the wrist acupuncture point P6 for preventing postoperative nausea and vomiting. Cochrane Database Syst Rev. 2004;2004(3):CD003281.
37. Wang D, Shi H, Yang Z, et al. Efficacy and safety of transcutaneous electrical acupoint stimulation for postoperative pain: a meta-analysis of randomized controlled trials. Pain Res Manag. 2022;2022:7570533. doi:10.1155/2022/7570533
38. Lai Y, Wang X, Li P, Li J, Zhou K, Che G. Preoperative peak expiratory flow (PEF) for predicting postoperative pulmonary complications after lung cancer lobectomy: a prospective study with 725 cases. J Thoracic Dis. 2018;10(7):4293–4301. doi:10.21037/jtd.2018.07.02
39. Huang C, Huang Q, Shen Y, Liu K, Wu J. General anaesthesia with double-lumen intubation compared to opioid-sparing strategies with laryngeal mask for thoracoscopic surgery: a randomised trial. Anaesth Crit Care Pain Med. 2022;41(3):101083. doi:10.1016/j.accpm.2022.101083
40. Zheng L, Zhang X, Ma Q, et al. Application of multimodal analgesia combined with opioid-free anesthetics in a non-intubated video-assisted thoracoscopic surgery bullectomy: a case report. Front Surg. 2023;10:1116523. doi:10.3389/fsurg.2023.1116523
41. Rice D, Rodriguez-Restrepo A, Mena G, et al. Matched pairs comparison of an enhanced recovery pathway versus conventional management on opioid exposure and pain control in patients undergoing lung surgery. Ann Surg. 2021;274(6):1099–1106. doi:10.1097/SLA.0000000000003587
42. Liu X, Li S, Wang B, An L, Ren X, Wu H. Intraoperative and postoperative anaesthetic and analgesic effect of multipoint transcutaneous electrical acupuncture stimulation combined with sufentanil anaesthesia in patients undergoing supratentorial craniotomy. Acupuncture Med. 2015;33(4):270–276. doi:10.1136/acupmed-2014-010749
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effect of Multimodal Health Education Combined with the Feedback Method in Perioperative Patients with Lung Cancer: A Randomised Controlled Study
Yuan Z, Gao L, Zheng M, Ye X, Sun S
Patient Preference and Adherence 2023, 17:413-420
Published Date: 16 February 2023
Pain Catastrophizing After Early-Stage Lung Cancer Surgery: The Mediating Effects of Interoceptive Awareness, Negative Attentional Bias, and Social Support
Bian G, Sun X, Chang Q, Liu L, Zhang C
Journal of Pain Research 2026, 19:569494
Published Date: 13 January 2026
Preoperative Transcutaneous Electrical Acupoint Stimulation Alleviates Postoperative Pain and Improves Sleep Quality in Breast Cancer Patients with Preoperative Sleep Disturbance: A Partially Randomized Controlled Trial
Ma C, Xiong H, Fu W, Lv S, Zhang L, Zhao D, Hu C, Wang X, Li W
Journal of Pain Research 2026, 19:619125
Published Date: 10 July 2026