Back to Journals » Journal of Pain Research » Volume 19
Preoperative Transcutaneous Electrical Acupoint Stimulation Alleviates Postoperative Pain and Improves Sleep Quality in Breast Cancer Patients with Preoperative Sleep Disturbance: A Partially Randomized Controlled Trial
Authors Ma C, Xiong H, Fu W, Lv S, Zhang L, Zhao D, Hu C, Wang X, Li W
Received 22 April 2026
Accepted for publication 1 July 2026
Published 10 July 2026 Volume 2026:19 619125
DOI https://doi.org/10.2147/JPR.S619125
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Karina Gritsenko
Can Ma,1,2 Hong Xiong,3 Wenchao Fu,1 Shihua Lv,1 Lijuan Zhang,1,2 Dengming Zhao,1,2 Cong Hu,1 Xiuli Wang,4 Wenzhi Li1,2
1The Key Laboratory of Anesthesiology and Intensive Care Research of Heilongjiang Province, Harbin, Heilongjiang, People’s Republic of China; 2Department of Anesthesiology, Second Affiliated Hospital of Harbin Medical University, Harbin, Heilongjiang, People’s Republic of China; 3The Third People’s Hospital of Chengdu, Chengdu, Sichuan, People’s Republic of China; 4Department of Anesthesiology, The Third Hospital of Hebei Medical University, Shijiazhuang, Hebei, People’s Republic of China
Correspondence: Wenzhi Li, Department of Anesthesiology, Second Affiliated Hospital of Harbin Medical University, No. 246 Xuefu Road, Nangang District, Harbin, Heilongjiang, People’s Republic of China, Tel +86 18045159998, Email [email protected]
Purpose: Preoperative sleep disturbance exacerbates postoperative pain and delays recovery. Transcutaneous electrical acupoint stimulation (TEAS) may alleviate insomnia and pain. This trial evaluated preoperative TEAS on postoperative pain, sleep, and intraoperative hemodynamics in breast cancer patients with preoperative sleep disturbance.
Patients and Methods: Fifty-nine breast cancer patients (aged 37– 70 years) were stratified by Pittsburgh Sleep Quality Index (PSQI): PSQI < 6 were assigned to the non-randomized control group (Group C, n = 26), while patients with PSQI ≥ 6 were randomly allocated (1:1) to the sleep disturbance group (Group S, n = 16) or the TEAS group (Group T, n = 17). TEAS (2/100 Hz, 8– 12 mA, 30 min) was delivered pre-anesthesia at LI4, HT7, and PC6. Pain was assessed via Numerical Rating Scale (NRS) at 4, 24, 48, and 72 h postoperatively. Sleep was measured with Athens Insomnia Scale (AIS). Intraoperative systolic blood pressure variability (sdSBP, cvSBP) was recorded.
Results: In observational comparisons, Group S exhibited elevated NRS scores at 24, 48, and 72 h vs Group C (p < 0.05). TEAS significantly reduced NRS scores across all time points (p < 0.05) and improved AIS scores on postoperative days 1– 2 (p < 0.05). Intraoperative sdSBP and cvSBP were lower in Group T than Group S (9.31 ± 2.73 vs 18.85 ± 6.74; 0.08 ± 0.02 vs 0.16 ± 0.05; p < 0.05). Among non-TEAS patients (Groups C and S), preoperative PSQI positively correlated with postoperative NRS and AIS scores.
Conclusion: Preoperative TEAS significantly attenuates postoperative pain and improves sleep in breast cancer patients with preoperative sleep disturbance, possibly associated with reduced intraoperative blood pressure variability. Preoperative sleep quality may predict postoperative outcomes.
Keywords: transcutaneous electrical acupoint stimulation, postoperative pain, sleep disturbance, breast cancer, autonomic nervous system
Introduction
Postoperative pain remains a significant clinical challenge, with up to 40–60% of surgical patients experiencing moderate to severe pain in the early postoperative period.1 Inadequate pain control not only prolongs hospital stay and delays functional recovery but also increases the risk of chronic postsurgical pain and long-term opioid use.2,3 Breast cancer patients scheduled for elective surgery represent a particularly vulnerable population, facing both surgical trauma and profound psychological distress related to cancer diagnosis and the prospect of mastectomy or breast-conserving surgery.4 According to the latest GLOBOCAN estimates, female breast cancer was the second most common cancer globally in 2022, with approximately 2.3 million new cases and 666,000 deaths, accounting for 11.6% of all cancer cases and 6.9% of all cancer deaths worldwide.5 Identifying effective, low-risk analgesic strategies that complement conventional pharmacotherapy is therefore of considerable clinical importance.
Sleep disorders are highly prevalent among breast cancer patients, with reported rates ranging from 60% to 90%.6,7 Importantly, preoperative sleep disturbance is not merely a benign comorbidity, it actively exacerbates postoperative pain perception through multiple neurobiological mechanisms, including enhanced central sensitization8,9 and sympathetic hyperactivation.10 The bidirectional relationship between sleep and pain is well established: poor sleep amplifies pain perception, while unrelieved pain fragments sleep architecture.10,11 This vicious cycle underscores the need for interventions that can simultaneously address both pain and sleep disturbance in the perioperative setting.
Transcutaneous electrical acupoint stimulation (TEAS), a non-invasive acupuncture modality that delivers electrical current through surface electrodes placed at specific acupoints, has emerged as a promising complementary therapy for pain management11,12 and sleep improvement.13 Systematic reviews and meta-analyses have demonstrated that TEAS significantly reduces postoperative pain scores and decreases cumulative opioid consumption across various surgical procedures.14,15 Despite this evidence, few studies have specifically examined TEAS in breast cancer patients with documented preoperative sleep disturbance—a population at particularly high risk for exacerbated postoperative pain and delayed recovery. Moreover, the potential of preoperative TEAS to stabilize intraoperative hemodynamics and improve postoperative pain outcomes in this high-risk subgroup has not been comprehensively evaluated. Therefore, the present randomized controlled trial was designed to investigate: (1) whether preoperative sleep disturbance is associated with worsened postoperative pain and intraoperative hemodynamic fluctuations in breast cancer patients; and (2) whether a single session of TEAS administered prior to anesthesia can attenuate postoperative pain intensity, improve sleep quality, and reduce sympathetic excitability during surgery.
Materials and Methods
Ethical Approval and Trial Registration
This prospective, partially randomized controlled trial was approved by the Medical Ethics Committee of the Second Affiliated Hospital of Harbin Medical University (approval number: KY2022-193) and conducted in accordance with the ethical principles of the Declaration of Helsinki. The trial was prospectively registered with the Chinese Clinical Trial Registry (http://www.chictr.org.cn/, registration number: ChiCTR2200062959, registration date: 2022–08-25). Written informed consent was obtained from all participants prior to enrollment. The full trial protocol is available from the corresponding author upon reasonable request. Patients and the public were not involved in the design, conduct, reporting, or dissemination plans of this research.
Participants
Patients with histopathologically confirmed breast cancer scheduled for elective surgery at our institution between July and November 2022 were screened for eligibility. Inclusion criteria were: (1) American Society of Anesthesiologists (ASA) physical status I–III; (2) age 18–70 years; (3) normal cognitive function and no communication impairment; and (4) anticipated surgical duration ≥ 30 minutes. Exclusion criteria were: (1) declined participation; (2) development of severe postoperative complications; (3) requirement for intensive care unit admission; (4) presence of cardiac pacemaker or implantable electronic device; (5) severe underlying conditions including cardiovascular, cerebrovascular, hepatic, renal, or hematopoietic diseases; (6) infection or injury at the designated TEAS electrode placement sites; and (7) history of severe neurological or psychiatric disorders. Surgical procedures included breast-conserving surgery with sentinel lymph node biopsy (BCS + SLNB), simple mastectomy with sentinel lymph node biopsy (SM + SLNB), and modified radical mastectomy (MRM), as determined by tumor stage and multidisciplinary team consensus.
Group Allocation and Randomization
On the day prior to surgery, all enrolled patients were assessed for their sleep status over the preceding month using the Chinese version of the Pittsburgh Sleep Quality Index (PSQI), a validated 19-item self-report questionnaire that evaluates seven components of sleep quality (total scores: 0–21, higher scores indicating poorer sleep quality). This instrument has demonstrated good reliability and validity in Chinese cancer populations (Cronbach’s α = 0.82–0.85).16 The full version used in this study is provided as Supplementary Material 1.
This was a partially randomized controlled trial. Patients with PSQI scores < 6 (indicating no clinically significant sleep disturbance) were assigned to the non-randomized reference control group (Group C). Patients with PSQI scores ≥ 6 (indicating poor sleep quality) were randomly allocated in a 1:1 ratio to either the sleep disturbance group (Group S) or the TEAS intervention group (Group T) using a computer-generated random number table Consequently, the primary randomized comparison was between Group S and Group T; comparisons involving Group C versus Groups S or T should be interpreted as observational. Allocation concealment was not feasible due to the physical nature of the TEAS intervention (researchers performing TEAS were necessarily aware of treatment allocation); however, outcome assessors were blinded to group assignment. Randomization was performed by a researcher not involved in patient recruitment, intervention delivery, or outcome assessment.
Sample Size Calculation
Sample size was estimated based on preliminary data from 30 patients (10 per group). Pairwise comparisons between Group C and Group S, and between Group T and Group S, were performed using postoperative Athens Insomnia Scale (AIS) score as the primary outcome. Power analysis conducted using the Power and Sample Size software indicated that 16 patients per group would provide 80% power to detect a clinically meaningful difference in AIS scores with a type I error (α) of 0.05. Postoperative NRS pain intensity was designated as a co-primary outcome of equal clinical importance; however, formal power calculation for NRS was not performed in the preliminary phase due to incomplete data collection. Post-hoc inspection of the final NRS results confirmed that the achieved sample size detected statistically significant between-group differences at all time points. To account for potential dropouts, a total of 72 patients were enrolled.
Anesthesia Protocol
A standardized general anesthesia protocol was applied to all patients. Anesthesia was induced with intravenous propofol (1.5–2.0 mg/kg), sufentanil (0.3–0.5 μg/kg), and cis-atracurium (0.1 mg/kg). Following tracheal intubation, anesthesia was maintained with sevoflurane inhalation (1.0–2.0% end-tidal concentration) and continuous intravenous remifentanil infusion (0.1–0.3 μg/kg/min), titrated to maintain bispectral index (BIS) values between 45 and 60. Intraoperative blood pressure was maintained within 20% of baseline values; ephedrine (5–10 mg intravenous bolus) was administered when systolic blood pressure decreased by more than 20% from baseline. For postoperative analgesia, flurbiprofen axetil (100 mg) was administered intravenously 30 minutes before the end of surgery and subsequently once daily for three consecutive days. No other regional blocks or additional analgesics were administered intraoperatively. All patients received standard perioperative care including prophylactic antiemetics (dexamethasone and granisetron) to prevent postoperative nausea and vomiting.
TEAS Intervention
Patients in Group T received a single 30-minute session of TEAS prior to anesthesia induction. A standardized electrical stimulator (HANS-200A, Nanjing Jisheng Medical Technology Co., Ltd., China) delivered biphasic square waves at alternating frequencies of 2 Hz and 100 Hz (dense-disperse mode), with current intensity individually adjusted to 8–12 mA based on patient tolerance (visible local muscle twitching without discomfort). Four acupoints were selected based on traditional Chinese medicine principles for their established roles in pain modulation and sleep regulation: Hegu (LI4) and Shenmen (HT7) on the left upper limb, and Hegu (LI4) and Neiguan (PC6) on the right upper limb. LI4 is located on the dorsum of the hand, between the first and second metacarpal bones, at the midpoint of the second metacarpal bone on the radial side. HT7 is located at the ulnar end of the transverse crease of the wrist, in the depression between the pisiform bone and the ulna. PC6 is located approximately 2 cun (≈6.7 cm) proximal to the transverse wrist crease, between the tendons of the palmaris longus and flexor carpi radialis muscles. The anatomical locations of these acupoints are illustrated in Figure 1. Electrode placement and stimulation parameters were standardized across all participants in Group T. Patients in Groups C and S did not receive TEAS or sham stimulation.
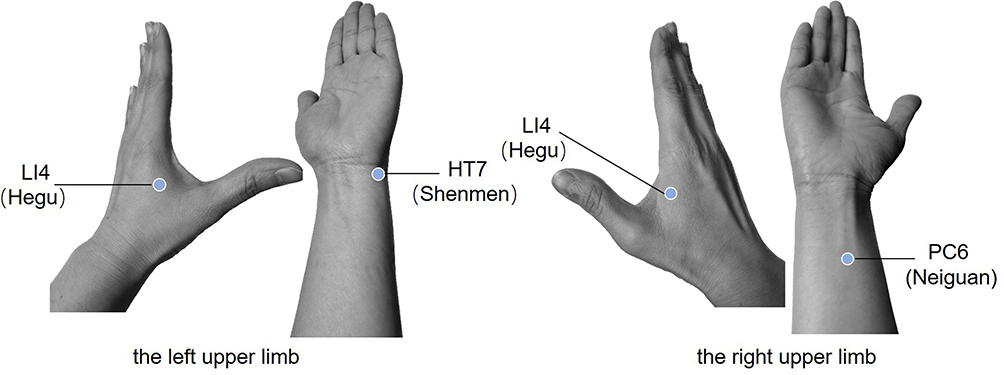 |
Figure 1 Anatomical locations of the acupoints used for transcutaneous electrical acupoint stimulation (TEAS). Notes: LI4 (Hegu) is located on the dorsum of the hand between the first and second metacarpal bones. HT7 (Shenmen) is located at the ulnar end of the transverse wrist crease. PC6 (Neiguan) is located approximately 2 cun proximal to the transverse wrist crease between the tendons of the palmaris longus and flexor carpi radialis muscles. |
Outcome Measures
Primary Outcome: Postoperative Pain Intensity and Sleep Quality
The primary outcome was postoperative pain intensity assessed using the 11-point Numerical Rating Scale (NRS; 0 = no pain, 10 = worst pain imaginable). Pain scores were recorded at rest at four time points: 4, 24, 48, and 72 hours after surgery. The NRS is a well-validated, reliable tool for assessing acute postoperative pain and demonstrates strong correlation with visual analog scales in surgical populations.
Sleep quality was assessed using the Athens Insomnia Scale (AIS), a validated 8-item self-report instrument that evaluates sleep induction, nocturnal awakenings, final awakening, total sleep duration, sleep quality, well-being, functioning capacity, and daytime sleepiness. The AIS has demonstrated good reliability (Cronbach’s α = 0.87–0.90) and validity in both preoperative and postoperative settings, with scores ≥ 6 indicating clinically significant insomnia.17 AIS scores were recorded at four time points: one day before surgery (T0), on the day of surgery (T1), and on the first (T2) and second (T3) postoperative days. Additionally, the number of nocturnal awakenings was documented.
Secondary Outcomes: Intraoperative Hemodynamics and Recovery
Intraoperative hemodynamic stability was assessed using two derived parameters: the standard deviation of systolic blood pressure (sdSBP), which quantifies overall blood pressure variability during surgery; and the coefficient of variation of systolic blood pressure (cvSBP), calculated as sdSBP divided by mean systolic blood pressure, which serves as a normalized index of sympathetic nervous system activity.18,19 Blood pressure measurements were recorded at 5-minute intervals throughout surgery, and sdSBP and cvSBP were computed from all intraoperative readings. Total intraoperative ephedrine consumption was also recorded as an indicator of hemodynamic instability.
Secondary clinical outcomes included: incidence of postoperative nausea and vomiting (PONV) within 24 hours after surgery; preoperative anxiety assessed using the Chinese version of the Self-Rating Anxiety Scale (SAS); heart rate variability (HRV) parameters (LF/HF ratio) derived from preoperative Holter monitoring; and total length of hospital stay. Preoperative risk of PONV was assessed using the Adult Apfel simplified scoring scale.
Data Collection
An outcome assessor blinded to group allocation performed all data collection. Baseline demographic and clinical data including age, body mass index (BMI), history of surgery and chemotherapy, comorbidities, baseline blood pressure and heart rate, intraoperative blood loss, fluid resuscitation volume, and surgical duration were recorded. All postoperative assessments (NRS pain scores, AIS sleep scores, PONV incidence) were conducted by the same blinded assessor to minimize inter-rater variability. No serious adverse events related to TEAS or study procedures were reported during the trial period.
Statistical Analysis
Continuous variables are expressed as mean ± SD and categorical variables as frequencies (%). Normality was assessed using the Kolmogorov–Smirnov test. Between-group comparisons for continuous data were performed using one-way ANOVA with Bonferroni post-hoc correction (normally distributed) or the Kruskal–Wallis test with Dunn’s post-hoc test (non-normally distributed). Categorical variables were compared using Fisher’s exact test, Pearson’s chi-square test, or the Cochran–Mantel–Haenszel test as appropriate.
For longitudinal outcomes (NRS and AIS), two-way repeated-measures ANOVA was employed with Group (C, S, T) as the between-subjects factor and Time as the within-subjects factor. Mauchly’s test was used to assess sphericity; the Greenhouse–Geisser correction was applied when violated. Main effects of Group and Time, as well as the Group × Time interaction, were examined. Bonferroni-corrected pairwise comparisons were performed when the interaction was significant or marginally significant (p < 0.10). Effect sizes were reported as partial eta-squared (η2).
Linear regression analysis was used to examine associations between preoperative PSQI scores and intraoperative hemodynamic parameters (sdSBP, cvSBP) and postoperative outcomes (AIS scores, NRS pain scores). Results are reported as standardized coefficients (β) with 95% confidence intervals (CI), adjusted R2, and two-tailed p values.
Categorical variables were analyzed using Pearson’s chi-square test when expected cell frequencies were ≥ 5, or Fisher’s exact test when expected frequencies were < 5. The exact test used for each comparison is specified in the corresponding table footnote.
A two-tailed p < 0.05 was considered statistically significant. All analyses were performed using SPSS version 22.0 (IBM Corp., Armonk, NY, USA) and GraphPad Prism version 9.5 (GraphPad Software, San Diego, CA, USA).
Results
Patient Enrollment and Disposition
A total of 72 breast cancer patients were screened for eligibility. Eight patients declined participation, and three patients were excluded for not meeting inclusion criteria. Sixty-one patients were enrolled: 26 patients with PSQI < 6 were assigned to the non-randomized control group (Group C), and 35 patients with PSQI ≥ 6 were randomly allocated (1:1) to the sleep disturbance group (Group S, n = 17) or the TEAS intervention group (Group T, n = 18). During the follow-up period, one patient in Group S and one patient in Group T were lost to follow-up due to incomplete postoperative data. Consequently, 59 patients (aged 37–70 years) were included in the final analysis: Group C (n = 26), Group S (n = 16), and Group T (n = 17). The CONSORT flow diagram is provided as Figure 2.
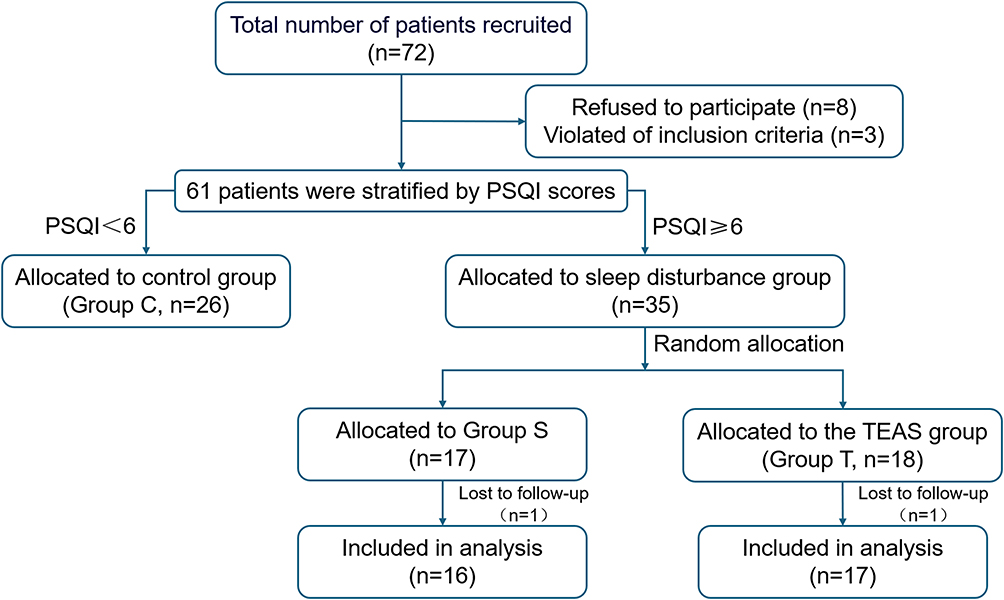 |
Figure 2 CONSORT flow diagram showing patient enrollment, allocation, follow-up, and analysis. |
Baseline Characteristics
Demographic and baseline clinical characteristics of the three groups are summarized in Table 1. There were no statistically significant differences among groups in age, BMI, Apfel PONV risk scores, prevalence of hypertension or diabetes, history of prior surgery or chemotherapy, type of surgical procedure, duration of surgery, preoperative systolic blood pressure, preoperative heart rate, intraoperative blood loss, or fluid resuscitation volume (all p > 0.05). LF/HF ratio from preoperative Holter monitoring also did not differ significantly among groups (p = 0.418).
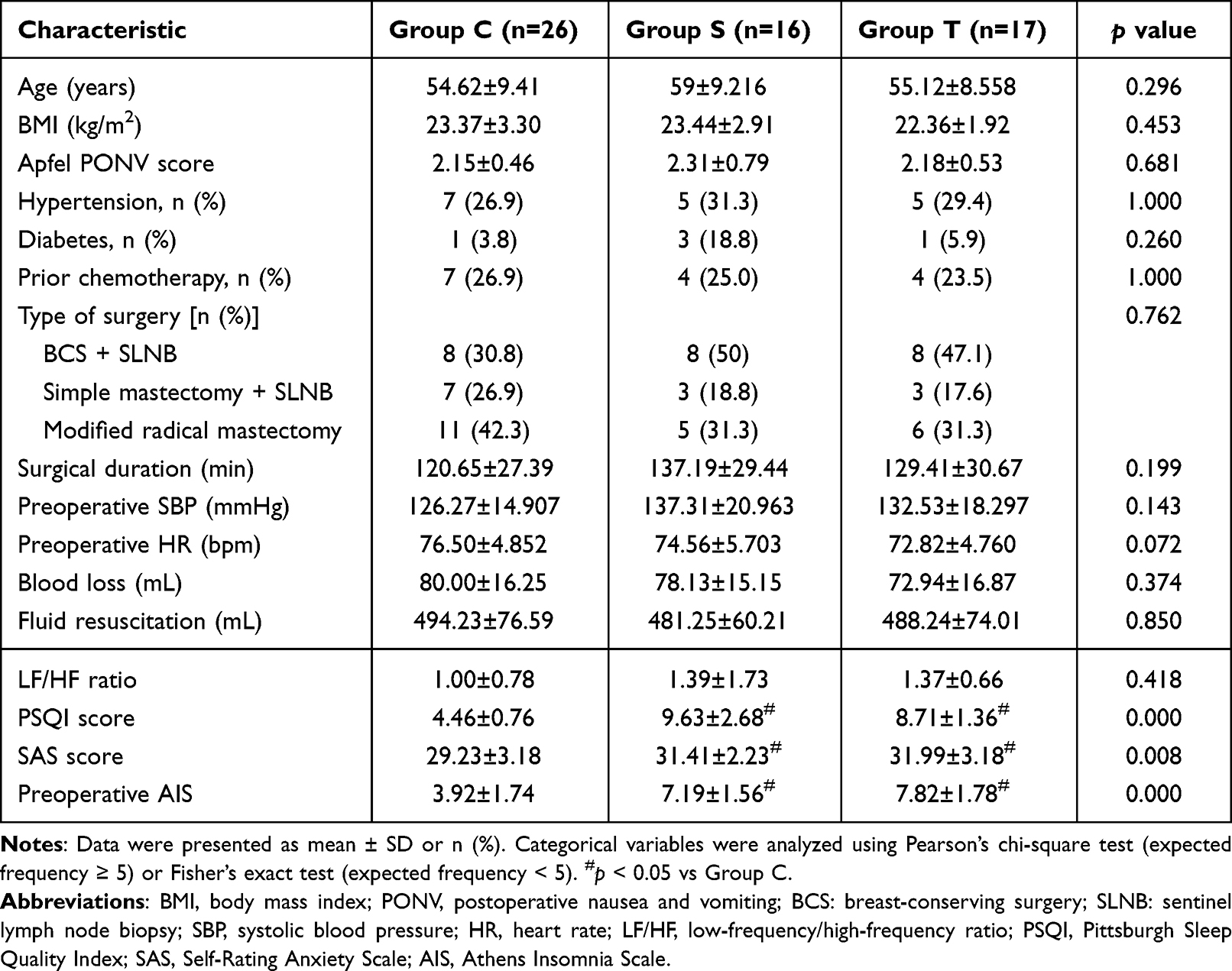 |
Table 1 Baseline Demographic and Clinical Characteristics |
As expected based on group allocation criteria, significant differences were observed in preoperative PSQI scores (Group C: 4.46 ± 0.76; Group S: 9.63 ± 2.68; Group T: 8.71 ± 1.36; p < 0.001), preoperative AIS scores (Group C: 3.92 ± 1.74; Group S: 7.19 ± 1.56; Group T: 7.82 ± 1.78; p < 0.001), and preoperative SAS anxiety scores (Group C: 29.23 ± 3.18; Group S: 31.41 ± 2.23; Group T: 31.99 ± 3.18; p = 0.008). Importantly, there were no significant differences in these baseline sleep and anxiety parameters between Group S and Group T, confirming successful randomization of the sleep-disordered cohort.
Postoperative Pain Outcomes
Postoperative NRS pain scores at rest are presented in Figure 3. In observational comparisons, patients in Group S exhibited significantly higher NRS scores at 24, 48, and 72 hours postoperatively compared with the non-randomized control group (Group C) (p < 0.05 at each time point). TEAS intervention (Group T) significantly reduced NRS pain scores compared with Group S at all postoperative time points (p < 0.05). Notably, pain scores in Group T were comparable to those in Group C across all time points, suggesting that preoperative TEAS effectively normalized postoperative pain perception in patients with baseline sleep disturbance.
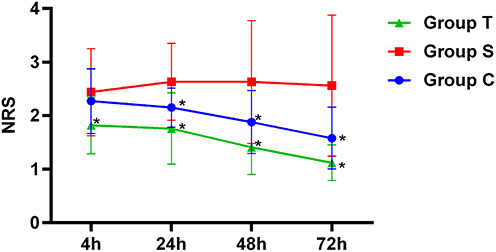 |
Figure 3 Postoperative NRS pain scores at rest. Abbreviations: NRS, numerical rating scale (NRS; 0 = no pain, 10 = worst pain imaginable). Notes: Data were presented as mean ± SD. Two-way repeated-measures ANOVA revealed a significant main effect of Group (p < 0.001) and Time (p < 0.001), and a marginally significant Group × Time interaction (p = 0.075). *p < 0.05 vs Group S (Bonferroni post-hoc test). |
Postoperative Sleep Quality
AIS scores and nocturnal awakening frequency are presented in Figure 4. At baseline (T0), both Group S and Group T had significantly higher AIS scores than Group C (p < 0.05). On the day of surgery (T1), sleep quality was uniformly poor across all three groups, with no significant between-group differences (p > 0.05). However, on postoperative days 1 (T2) and 2 (T3), both Group C and Group T demonstrated significantly greater improvements in AIS scores compared with Group S (p < 0.05). The number of nocturnal awakenings in Group T progressively decreased after surgery, mirroring the trend observed in Group C.
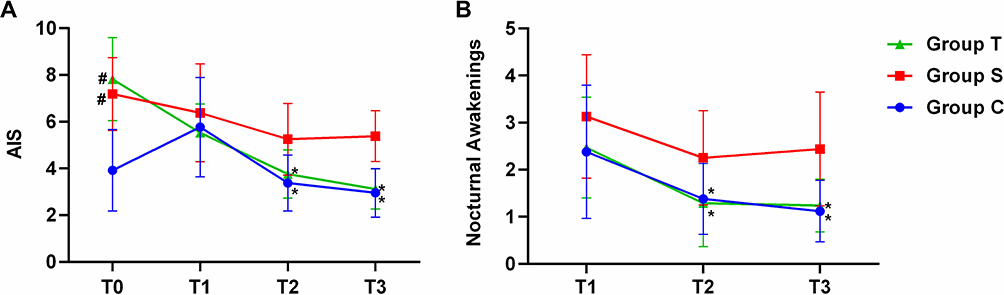 |
Figure 4 Postoperative sleep quality. (A) Athens Insomnia Scale (AIS) scores across the perioperative period in the three groups. T0, baseline; T1, day of surgery; T2, postoperative day 1; T3, postoperative day 2. (B) Number of nocturnal awakenings. Notes: Data were presented as mean ± SD. Two-way repeated-measures ANOVA revealed significant main effects of Group (p < 0.001) and Time (p < 0.001), and a highly significant Group × Time interaction (p < 0.001). #p < 0.05 vs Group C; *p < 0.05 vs Group S (Bonferroni post-hoc test). |
Intraoperative Hemodynamic Parameters
Intraoperative hemodynamic parameters and vasopressor requirements are summarized in Table 2. Both sdSBP and cvSBP were significantly lower in Group C and Group T compared with Group S (p < 0.05). Specifically, mean sdSBP values were: Group C, 12.09 ± 3.56; Group S, 18.85 ± 6.74; Group T, 9.31 ± 2.73 (p < 0.001). Mean cvSBP values were: Group C, 0.10 ± 0.03; Group S, 0.16 ± 0.05; Group T, 0.08 ± 0.02 (p < 0.001). Notably, patients receiving TEAS (Group T) demonstrated the lowest sdSBP and cvSBP values among all groups, even lower than those in Group C. Meanwhile, intraoperative ephedrine consumption was significantly lower in Group C (10.73 ± 6.01 mg) and Group T (11.29 ± 5.15 mg) compared with Group S (16.31 ± 7.26 mg) (p = 0.016).
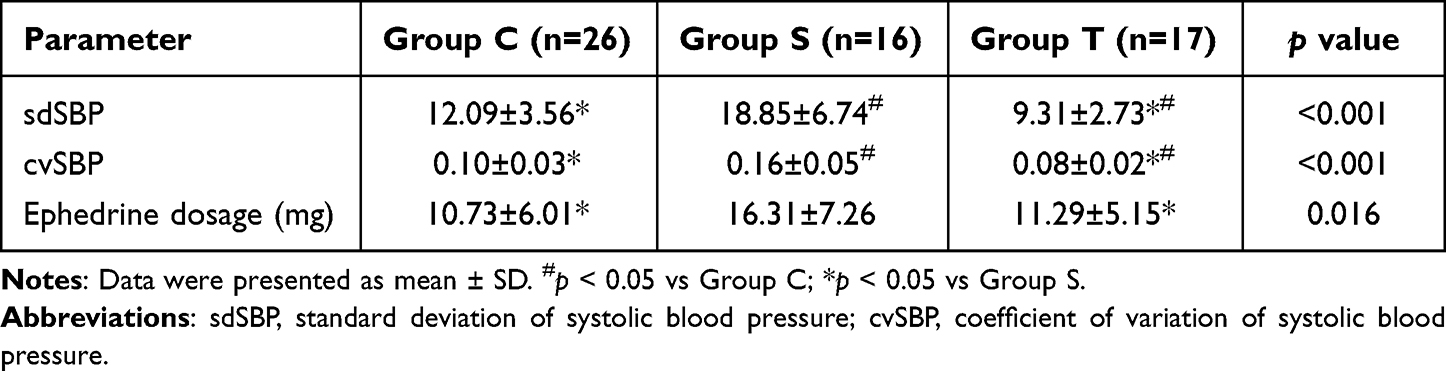 |
Table 2 Intraoperative Hemodynamic Parameters and Vasopressor Use |
Postoperative Nausea, Vomiting, and Length of Stay
The incidence of postoperative nausea and vomiting and length of hospital stay are presented in Table 3. The incidence of nausea within 24 hours postoperatively was 50% (13/26) in Group C, 50% (8/16) in Group S, and 35.3% (6/17) in Group T; the incidence of vomiting was 42.3% (11/26) in Group C, 43.8% (7/16) in Group S, and 35.3% (6/17) in Group T. Although Group T exhibited numerically lower rates of both nausea and vomiting, these differences did not reach statistical significance (p = 0.590 and p = 0.863, respectively). Length of hospital stay was slightly longer in Group S (8.06 ± 2.29 days) compared with Group C (7.27 ± 2.41 days) and Group T (6.82 ± 1.68 days); however, this difference was not statistically significant (p = 0.266).
 |
Table 3 Postoperative Nausea, Vomiting, and Length of Hospital Stay |
Correlations Between Preoperative Sleep Quality and Perioperative Outcomes
Linear regression analysis was performed in the combined non-TEAS cohort (Groups C and S, n = 42) to examine associations between preoperative PSQI scores and perioperative outcomes.
Preoperative PSQI score was significantly and positively associated with intraoperative sdSBP (B = 0.903, 95% CI: 0.355–1.451, β = 0.466, p = 0.002, adjusted R2 = 0.197) and cvSBP (B = 0.007, 95% CI: 0.003–0.011, β = 0.493, p < 0.001, adjusted R2 = 0.224) (Figure 5). This indicates that patients with poorer preoperative sleep quality experienced greater intraoperative blood pressure fluctuations.
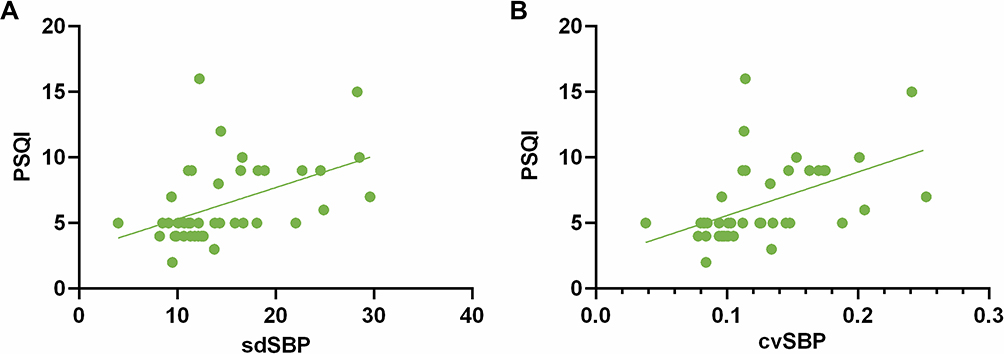 |
Figure 5 Linear regression analysis between preoperative PSQI scores and intraoperative hemodynamic parameters. (A) PSQI scores and sdSBP and (B) PSQI scores and cvSBP in patients not receiving TEAS (Groups C and S combined). Abbreviations: PSQI, Pittsburgh Sleep Quality Index; sdSBP, standard deviation of systolic blood pressure; cvSBP, coefficient of variation of systolic blood pressure. |
Furthermore, preoperative PSQI scores were significantly associated with postoperative AIS scores on day 1 (B = 0.291, 95% CI: 0.152–0.430, β = 0.556, p < 0.001, adjusted R2 = 0.292) and day 2 (B = 0.329, 95% CI: 0.203–0.456, β = 0.639, p < 0.001, adjusted R2 = 0.394) (Figure 6). Similarly, significant positive associations were observed between preoperative PSQI scores and postoperative NRS pain scores at 24 hours (B = 0.080, 95% CI: 0.027–0.134, β = 0.432, p = 0.004, adjusted R2 = 0.166), 48 hours (B = 0.132, 95% CI: 0.047–0.217, β = 0.446, p = 0.003, adjusted R2 = 0.179), and 72 hours (B = 0.176, 95% CI: 0.084–0.268, β = 0.521, p < 0.001, adjusted R2 = 0.253) (Figure 7). These findings suggest that preoperative sleep quality, as quantified by PSQI, may serve as a clinically useful predictor of both postoperative pain intensity and sleep disturbance.
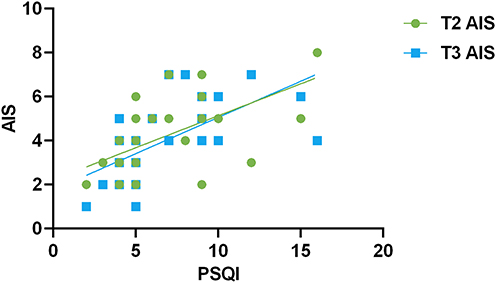 |
Figure 6 Linear regression analysis between preoperative PSQI scores and postoperative AIS scores on days 1 and 2 in patients not receiving TEAS (Groups C and S combined). Abbreviations: PSQI, Pittsburgh Sleep Quality Index; AIS, Athens Insomnia Scale. |
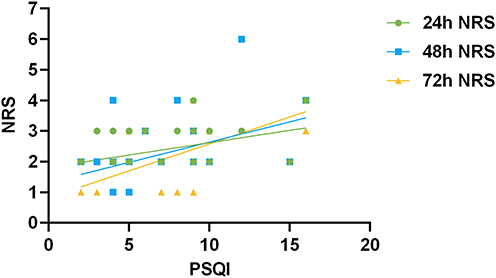 |
Figure 7 Linear regression analysis between preoperative PSQI scores and postoperative NRS pain scores at 24, 48, and 72 hours in patients not receiving TEAS (Groups C and S combined). Abbreviations: PSQI, Pittsburgh Sleep Quality Index; NRS, numerical rating scale. |
Adverse Events
No serious adverse events attributable to TEAS or study procedures were reported during the trial period. All patients tolerated the TEAS intervention well, with no reports of skin irritation, burns, or discomfort requiring discontinuation of stimulation.
Discussion
The principal findings of this partially randomized controlled trial are fourfold. First, preoperative sleep disturbance in breast cancer patients is associated with significantly elevated postoperative pain intensity, poorer postoperative sleep quality, and greater intraoperative hemodynamic instability. Second, a single 30-minute session of TEAS administered prior to anesthesia effectively attenuates postoperative pain, improves postoperative sleep quality, and reduces intraoperative blood pressure variability in patients with documented preoperative sleep disturbance. Third, TEAS reduces cvSBP—a normalized index of blood pressure variability—suggesting that its clinical benefits may be mediated, at least in part, through modulation of autonomic balance. Fourth, preoperative PSQI scores were significantly associated with postoperative pain and sleep quality, highlighting the potential utility of routine preoperative sleep screening for risk stratification and targeted intervention.
Preoperative Sleep Disturbance Exacerbate Postoperative Pain
The observation that patients with preoperative sleep disturbance (Group S) experienced significantly higher postoperative pain scores across all time points aligns with a growing body of evidence linking sleep disruption to enhanced pain sensitivity. Neuroimaging studies have demonstrated that sleep deprivation amplifies activity in pain-related somatosensory cortical regions while simultaneously reducing activity in key pain-modulatory areas including the cingulate gyrus, insular cortex, thalamus, and nucleus accumbens.8 Moreover, sleep loss reduces endogenous opioid production and decreases μ- and δ-opioid receptor binding affinity, effectively impairing the descending pain inhibitory system.9 The positive correlation between preoperative PSQI scores and postoperative NRS pain scores (β = 0.432–0.521) observed in our study provides clinical confirmation of this sleep–pain relationship in the surgical setting. These findings underscore the importance of identifying patients with preoperative poor sleep quality as a high-risk subgroup warranting proactive analgesic intervention.
TEAS Provides Multimodal Analgesic and Sleep-Promoting Effects
TEAS produced clinically meaningful reductions in postoperative pain scores across all assessment time points, with Group T achieving pain levels comparable to those of patients without baseline sleep disturbance (Group C). This analgesic effect is consistent with the known neurobiological mechanisms of acupuncture-related therapies. Mechanistically, TEAS generates action potentials in peripheral afferent nerve fibers,11,20 and electrical signals transmitted to the central nervous system trigger the release of endogenous opioid peptides (β-endorphin, enkephalin, dynorphin), serotonin, and adenosine,12 while concurrently inhibiting spinal nociceptive transmission through gate-control mechanisms.21 The dense-disperse frequency mode (2/100 Hz) employed in our protocol is particularly effective, as 2 Hz stimulation preferentially releases enkephalins and β-endorphin, whereas 100 Hz stimulation promotes dynorphin release.22 A recent review further summarized the comprehensive mechanisms of TEAS in the perioperative period, including regulation of the neuroendocrine network, inhibition of oxidative stress, and modulation of inflammatory responses.23 Furthermore, TEAS has been shown to reduce microglial activation in the spinal cord, thereby attenuating central sensitization and hyperalgesia.24
Beyond its direct analgesic effects, TEAS significantly improved postoperative sleep quality, with Group T demonstrating AIS score trajectories that paralleled those of Group C. This dual benefit on pain and sleep is particularly noteworthy, as effective pain management is known to enhance sleep quality, while improved sleep reciprocally reduces pain perception.25,26 The sleep-promoting mechanisms of TEAS are multifaceted. Acupuncture and related techniques have been shown to activate sleep-regulating brain regions including the hypothalamus,27 and systematic reviews indicate that acupuncture improves both subjective and objective sleep parameters through modulation of neurotransmitters, inflammatory cytokines, the hypothalamic–pituitary–adrenal axis, and melatonin secretion.28 Beyond acupuncture, direct evidence supports TEAS efficacy: a recent pilot RCT found that TEAS significantly improved sleep quality (measured by PSQI) in hypertensive patients with comorbid sleep disorders, with both low- and high-frequency stimulation proving similarly effective.29 Collectively, these findings suggest that TEAS, like acupuncture, promotes sleep through multimodal neuroendocrine and autonomic modulation. The acupoints selected in our study were specifically chosen for their traditional and modern evidence in promoting sleep: HT7 (Shenmen), the Yuan-source point of the Heart meridian, is classically used for calming the Shen (spirit) and treating insomnia; PC6 (Neiguan), the Luo-connecting point of the Pericardium meridian, is renowned for its broad regulatory effects on autonomic function and stress responses; and LI4 (Hegu), the Yuan-source point of the Large Intestine meridian, is a master point for pain modulation and general homeostasis. The convergence of these acupoints provides a rational basis for the observed improvements in both pain and sleep outcomes.
TEAS Is Associated with Reduced Intraoperative Blood Pressure Variability
A novel observation of our study is that preoperative TEAS was associated with significantly reduced intraoperative cvSBP, a normalized index of blood pressure variability.19 Patients with poor sleep quality exhibited elevated cvSBP and sdSBP during surgery, consistent with the known association between sleep deprivation and heightened cardiovascular lability coupled with diminished baroreceptor sensitivity.30 Sleep loss increases daytime catecholamine levels, which likely contributes to intraoperative blood pressure fluctuations. TEAS treatment preoperatively reduced cvSBP in sleep-disordered patients to levels even lower than those observed in control patients, suggesting that TEAS may exert a modulatory effect on autonomic tone that contributes to hemodynamic stability.
The beneficial effects of TEAS observed in this study may be attributed to its capacity to influence autonomic nervous system balance. A 2025 comprehensive review highlighted that TEAS modulates autonomic balance by suppressing excessive sympathetic excitability and restoring parasympathetic tone,23 and a 2023 meta-analysis confirmed that acupuncture significantly increases parasympathetic tone as reflected by improved heart rate variability parameters.31
Mechanistically, these effects are hypothesized to be mediated through central pathways, wherein acupuncture signals are transmitted to the hypothalamus and integrated to regulate autonomic output.32 In the present study, the reduction in cvSBP provides direct clinical evidence that TEAS may attenuates sympathetic hyperactivation during surgery, thereby stabilizing intraoperative hemodynamics. The positive correlation between preoperative PSQI scores and intraoperative sdSBP/cvSBP further supports the concept that poor sleep quality predisposes patients to greater hemodynamic lability during surgical stress.
However, we emphasize that sdSBP and cvSBP are indirect and imperfect markers of autonomic activity. These measures are influenced by multiple perioperative factors, including anesthetic depth, opioid dosing, vasopressor use, surgical stimulation, baseline blood pressure, and anxiety. Our standardized anesthesia protocol mitigates some inter-patient variability, but these hemodynamic parameters cannot definitively establish altered sympathetic tone without direct neurochemical or microneurographic measurements.
Clinical Implications and Predictors
Our findings carry important clinical implications. First, routine preoperative sleep assessment using validated tools such as the PSQI may help identify high-risk patients for postoperative pain and sleep disturbance, facilitating targeted perioperative management. Second, TEAS represents a non-invasive, safe, and low-cost adjunct that can be easily integrated into existing perioperative care pathways without significant additional resource requirements. Importantly, TEAS is not associated with the adverse effects commonly seen with opioid analgesics (respiratory depression, nausea, sedation) or sedative-hypnotics (daytime drowsiness, dependence), making it a particularly attractive option for vulnerable populations such as elderly patients or those with comorbidities. Third, the combination of analgesic, sleep-promoting, and sympatholytic effects positions TEAS as a uniquely multimodal intervention that addresses multiple interrelated aspects of perioperative pathophysiology.
Limitations
Several limitations of this study warrant consideration. First, this study employed a partially randomized design: Group C (PSQI < 6) served as a non-randomized, sleep-healthy reference cohort, whereas the randomized comparison was confined to Group S versus Group T. Consequently, comparisons involving Group C versus Groups S or T are observational and should be interpreted as stratified by baseline sleep status rather than as randomized contrasts. Second, the lack of a sham TEAS group precludes exclusion of placebo effects on subjective outcomes. Although outcome assessor blinding was maintained, participant blinding was not feasible given the physical nature of the intervention. Third, the sample size was relatively small (final n = 59, with approximately 16–26 per group), which may have limited statistical power to detect differences in secondary outcomes; the secondary and exploratory findings should be interpreted as hypothesis-generating rather than confirmatory. Fourth, sleep quality was assessed exclusively using subjective self-report instruments (PSQI and AIS) without objective polysomnography or actigraphy monitoring. Fifth, allocation concealment and participant blinding were not feasible due to the physical nature of the TEAS intervention. Sixth, this study employed a single 30-minute preoperative TEAS session, whereas prior studies have used multiple perioperative sessions with extended postoperative applications.33 Combined with our short follow-up period (pain assessed for 72 h, sleep for 2 days), this design limits evaluation of both the durability and cumulative effects of TEAS; no inference regarding chronic postsurgical pain or longer-term recovery can be drawn. Seventh, the mechanisms underlying TEAS effects were inferred from indirect measures (cvSBP, HRV) rather than direct neurochemical assays (eg, plasma catecholamines, endogenous opioid levels). Finally, this is a unicentric study, which may limit the generalizability of our findings to other institutions, geographic regions, or healthcare settings. Although baseline covariates were balanced across groups, future studies with larger cohorts should perform multivariable analyses to further confirm the independence of these associations.
Conclusion
In conclusion, this partially randomized controlled trial demonstrates that preoperative sleep disturbance is associated with significantly exacerbated postoperative pain, impaired sleep quality, and intraoperative hemodynamic instability in breast cancer patients. A single preoperative TEAS may effectively attenuate postoperative pain, and improve postoperative sleep quality, and is associated with reduced intraoperative blood pressure variability. Furthermore, preoperative sleep quality may serve as a clinically useful predictor of postoperative outcomes, suggesting that routine preoperative sleep screening may facilitate risk stratification and targeted intervention. TEAS represents a safe, non-pharmacologic, and multimodal adjunct that warrants consideration for incorporation into perioperative care pathways for breast cancer patients, particularly those identified as having preoperative sleep disturbance.
Data Sharing Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to ethical and legal restrictions imposed by the informed consent agreement signed by all participants and the ethical approval granted by the Medical Ethics Committee of the Second Affiliated Hospital of Harbin Medical University (approval number: KY2022-193). The informed consent document explicitly states that participants’ personal information will be strictly protected and kept confidential, and that study results will be published without disclosing any personal identifying information. Individual deidentified participant data will not be deposited in public repositories or shared with external researchers. Requests for data access will be considered on a case-by-case basis and require approval from the corresponding author and the institutional ethics committee.
Acknowledgments
The authors thank all the patients who participated in this study and the clinical staff who assisted with data collection.
Funding
This research received no specific grant from any funding agency.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Xu J, Liu X, Zhao J, et al. Comprehensive review on personalized pain assessment and multimodal interventions for postoperative recovery optimization. J Pain Res. 2025;18:2791–14. doi:10.2147/jpr.S516249
2. Glare P, Aubrey KR, Myles PS. Transition from acute to chronic pain after surgery. Lancet. 2019;393(10180):1537–1546. doi:10.1016/s0140-6736(19)30352-6
3. Martinez V, Lehman T, Lavand’homme P, et al. Chronic postsurgical pain: a European survey. Europ J Anaesthesiol. 2024;41(5):351–362. doi:10.1097/eja.0000000000001974
4. Yang C, Liu Y, Xiao B, et al. Evidence summary for the management of sleep disorders after malignant tumor surgery. Front Neurol. 2025;16:1580216. doi:10.3389/fneur.2025.1580216
5. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. Ca a Cancer J Clin. 2024;74(3):229–263. doi:10.3322/caac.21834
6. Lin D, Huang X, Sun Y, et al. Perioperative sleep disorder: a review. Front Med. 2021;8:640416. doi:10.3389/fmed.2021.640416
7. Savard J, Ivers H, Savard MH, et al. Cancer treatments and their side effects are associated with aggravation of insomnia: results of a longitudinal study. Cancer. 2015;121(10):1703–1711. doi:10.1002/cncr.29244
8. Wilson JM, Franqueiro AR, Rosado E, et al. Preoperative decreased physical activity is associated with greater postoperative pain: the mediating role of preoperative sleep disturbance. Support Care Cancer. 2024;32(7):429. doi:10.1007/s00520-024-08625-w
9. Stroemel-Scheder C, Kundermann B, Lautenbacher S. The effects of recovery sleep on pain perception: a systematic review. Neurosci Biobehav Rev. 2020;113:408–425. doi:10.1016/j.neubiorev.2020.03.028
10. Al Haddad N, Costanian C, Zibara V, et al. The association between sleep disturbances and blood pressure variability: a review of the literature. J Clin Sleep Med. 2023;19(8):1533–1544. doi:10.5664/jcsm.10566
11. Kagitani F, Uchida S, Hotta H, et al. Manual acupuncture needle stimulation of the rat hindlimb activates groups I, II, III and IV single afferent nerve fibers in the dorsal spinal roots. Jpn J Physiol. 2005;55(3):149–155. doi:10.2170/jjphysiol.R2120
12. Han JS. Acupuncture: neuropeptide release produced by electrical stimulation of different frequencies. Trends Neurosci. 2003;26(1):17–22. doi:10.1016/s0166-2236(02)00006-1
13. Ning J, An CF, Li LM, et al. Effects of perioperative transcutaneous electrical acupoint stimulation on sleep quality after general anaesthesia: a systematic review and meta-analysis. J College Phys Surg--Pakistan. 2026;36(2):223–232. doi:10.29271/jcpsp.2026.02.223
14. Song B, Chang Y, Li Y, et al. Effects of transcutaneous electrical acupoint stimulation on the postoperative sleep quality and pain of patients after video-assisted thoracoscopic surgery: a prospective, randomized controlled trial. Nat Sci Sleep. 2020;12:809–819. doi:10.2147/nss.S270739
15. Wang J, Lu FF, Ge MM, et al. Transcutaneous electrical acupoint stimulation improves postoperative sleep quality in patients undergoing laparoscopic gastrointestinal tumor surgery: a prospective, randomized controlled trial. Pain Ther. 2023;12(3):707–722. doi:10.1007/s40122-023-00493-2
16. Tsai PS, Wang SY, Wang MY, et al. Psychometric evaluation of the Chinese version of the pittsburgh sleep quality index (CPSQI) in primary insomnia and control subjects. Qual Life Res. 2005;14(8):1943–1952. doi:10.1007/s11136-005-4346-x
17. Soldatos CR, Dikeos DG, Paparrigopoulos TJ. Athens insomnia scale: validation of an instrument based on ICD-10 criteria. J Psychosomatic Res. 2000;48(6):555–560. doi:10.1016/s0022-3999(00)00095-7
18. Parati G, Ochoa JE, Lombardi C, et al. Assessment and management of blood-pressure variability. Nat Rev Cardiol. 2013;10(3):143–155. doi:10.1038/nrcardio.2013.1
19. Schutte AE, Kollias A, Stergiou GS. Blood pressure and its variability: classic and novel measurement techniques. Nat Rev Cardiol. 2022;19(10):643–654. doi:10.1038/s41569-022-00690-0
20. Fan Z, Dou B, Wang J, et al. Effects and mechanisms of acupuncture analgesia mediated by afferent nerves in acupoint microenvironments. Front Neurosci. 2023;17:1239839. doi:10.3389/fnins.2023.1239839
21. Kato Y, Yachi K, Hoshi H, et al. Two distinct neural mechanisms underlying acupuncture analgesia. Front Pain Res. 2022;3:869884. doi:10.3389/fpain.2022.869884
22. Zhang R, Lao L, Ren K, et al. Mechanisms of acupuncture-electroacupuncture on persistent pain. Anesthesiology. 2014;120(2):482–503. doi:10.1097/aln.0000000000000101
23. Jiang X, Li M, Tang Y, et al. Research progress on the mechanism of transcutaneous electrical acupoint stimulation in the perioperative period. Front Neurol. 2025;16:1563681. doi:10.3389/fneur.2025.1563681
24. Lin L, Skakavac N, Lin X, et al. Acupuncture-induced analgesia: the role of microglial inhibition. Cell Transplant. 2016;25(4):621–628. doi:10.3727/096368916x690872
25. Giordano NA, Kent M, Andersen SG, et al. Postoperative pain mediates the association between peripheral nerve blocks and postoperative sleep following lower extremity arthroplasty. Clin J Pain. 2021;37(7):487–493. doi:10.1097/ajp.0000000000000942
26. Niklasson A, Finan PH, Smith MT, et al. The relationship between preoperative sleep disturbance and acute postoperative pain control: a systematic review and meta-analysis. Sleep Med Rev. 2025;79:102014. doi:10.1016/j.smrv.2024.102014
27. Spence DW, Kayumov L, Chen A, et al. Acupuncture increases nocturnal melatonin secretion and reduces insomnia and anxiety: a preliminary report. J Neuropsychiatr Clin Neurosci. 2004;16(1):19–28. doi:10.1176/jnp.16.1.19
28. Zhao FY, Spencer SJ, Kennedy GA, et al. Acupuncture for primary insomnia: effectiveness, safety, mechanisms and recommendations for clinical practice. Sleep Med Rev. 2024;74:101892. doi:10.1016/j.smrv.2023.101892
29. Bao XY, Liu CZ, Qian ZT, et al. Transcutaneous electrical acupoint stimulation for hypertension complicated by anxiety or sleep disorders: a pilot randomized controlled trial. Complementary Ther Med. 2025;89:103138. doi:10.1016/j.ctim.2025.103138
30. Hori A, Su X, Sagasaki S, et al. Sleep deprivation elevates resting and exercise blood pressures and augments pressor response at exercise onset. Med Sci Sports Exercise. 2025;57(5):996–1007. doi:10.1249/mss.0000000000003640
31. Hamvas S, Hegyi P, Kiss S, et al. Acupuncture increases parasympathetic tone, modulating HRV - Systematic review and meta-analysis. Complementary Ther Med. 2023;72:102905. doi:10.1016/j.ctim.2022.102905
32. Zhou X, Zhou J, Zhang F, et al. Key targets of signal transduction neural mechanisms in acupuncture treatment of cardiovascular diseases: hypothalamus and autonomic nervous system. Heliyon. 2024;10(19):e38197. doi:10.1016/j.heliyon.2024.e38197
33. Yan L, Sun B, Zhou M, et al. [Effect of transcutaneous electrical acupoint stimulation on postoperative pain in patients undergoing modified radical mastectomy for breast cancer]. Zhongguo Zhen Jiu. 2025;45(2):162–166. doi:10.13703/j.0255-2930.20240206-k0002
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Transcutaneous Electrical Acupoint Stimulation (TEAS) Facilitates Postoperative Recovery in Day Lung Cancer Surgery: A Randomized Controlled Trial
Wu S, Lou J, Zou H, Wang W, Zhang Y, Xu Y, Hou X, Wu J
Journal of Pain Research 2025, 18:3017-3026
Published Date: 17 June 2025