Back to Journals » Journal of Pain Research » Volume 19
Pain Catastrophizing After Early-Stage Lung Cancer Surgery: The Mediating Effects of Interoceptive Awareness, Negative Attentional Bias, and Social Support
Authors Bian G, Sun X, Chang Q ![]() , Liu L, Zhang C
, Liu L, Zhang C
Received 23 September 2025
Accepted for publication 8 January 2026
Published 13 January 2026 Volume 2026:19 569494
DOI https://doi.org/10.2147/JPR.S569494
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jonathan Greenberg
Guanjun Bian,1,2 Xiaoting Sun,2 Qing Chang,1 Lifeng Liu,1 Chunmei Zhang3
1Department of Pulmonary Oncology, Tianjin Medical University Cancer Institute and Hospital, National Clinical Research Center for Cancer, Key Laboratory of Cancer Prevention and Therapy, Tianjin, Tianjin’s Clinical Research Center for Cancer, Tianjin, 300060, People’s Republic of China; 2Graduate School, Tianjin University of Traditional Chinese Medicine, Tianjin, 301617, People’s Republic of China; 3School of Nursing, Tianjin University of Traditional Chinese Medicine, Tianjin, 301617, People’s Republic of China
Correspondence: Chunmei Zhang, School of Nursing, Tianjin University of Traditional Chinese Medicine, 10 Poyanghu Road, West Tuanbo New Town, Jinghai District, Tianjin, 301617, People’s Republic of China, Email [email protected]
Background: Pain Catastrophizing (PC) is a prevalent maladaptive cognitive - affective response after lung cancer surgery, linked to poor outcomes. The mechanisms between sub - acute pain and PC development within 3 months are unclear. Conventional pain management often neglects psychological and social factors related to PC and recovery. According to the biopsychosocial model, multiple factors are associated with PC, but their mediating pathways are not fully understood.Therefore, grounded in the stress and coping theory and the pain threat appraisal theory, first examines the multiple-parallel mediating roles of introspection, negative attentional bias, and social support between pain intensity and PC in early-stage lung cancer patients post - surgery.
Methods: A cross-sectional study recruited 414 early-stage lung cancer patients within 3 months post-surgery from ambulatory care follow-up and day ward treatment at a tertiary hospital from May to August 2025. Questionnaires were used for investigation, and parallel mediation was tested by structural equation modeling.
Results: The average PCS score was 30.49 ± 6.27. PC was positively correlated with pain intensity, interoceptive awareness, and negative attentional bias, and negatively correlated with social support. Interoceptive awareness, negative attentional bias, and social support together accounted for 59.81% of the total effect, with social support having the most prominent effect (31.05%)—substantially larger than interoceptive awareness (5.51%) and negative attentional bias (5.91%).
Conclusion: Post-operative PC levels in early-stage lung cancer patients are moderate to high. Pain intensity is directly and indirectly related to PC. Healthcare professionals are advised to develop a multidimensional, phased, and integrated intervention framework including pain management, cognitive behavioral therapy, and mindfulness training. This approach can effectively reduce PC and support precise prevention and intervention.
Keywords: lung cancer, postoperative pain, pain catastrophizing, interoceptive awareness, negative attention bias, social support, mediating effects
Introduction
Lung cancer is the most prevalent and lethal malignant tumor globally, presenting a significant public-health challenge.1 With growing public-health awareness and advancements in early cancer screening, its incidence has been rising steadily. However, effective management of postoperative pain remains a major clinical obstacle. Although thoracoscopic surgery reduces surgical trauma, about 80% of patients still suffer from varying degrees of postoperative pain. This not only hinders recovery but may also increase the risk of disease recurrence.2 Studies3–5 show that the incidence of postoperative pain among lung cancer patients within three months after surgery is 56–69%, and 15–60% of them may develop chronic pain.
Currently, traditional pain-management strategies primarily focus on pharmacological interventions and pain assessment, neglecting psychological and social factors. This may lead to pain catastrophizing in patients, negatively affecting postoperative recovery.6 Thus, assessing pain catastrophizing levels is of great clinical significance. Pain catastrophizing is a maladaptive cognitive-emotional response, where individuals overstate pain threats, experience more distress, and feel a lack of control.7 Research indicates that 20–35.3% of postoperative lung cancer patients have PCS scores ≥38,8–10 highlighting the clinical significance of assessment.
According to the biopsychosocial model, pain catastrophizing is influenced by multiple interrelated factors including biological mechanisms, psychological states, and social support. Existing evidence suggests that pain intensity,7 interoceptive awareness,11,12 negative attentional bias,13 and perceived social support14 are key factors. Interoceptive awareness is an individual’s ability to detect and regulate internal physiological signals, related to cognitive and behavioral regulation.15 Negative attentional bias is a cognitive tendency to focus on negative stimuli while ignoring neutral or positive information.16
Despite these known factors, the specific mediating pathways among pain intensity, interoceptive awareness, negative attentional bias, and social support in the development of pain catastrophizing remain unexamined in early-stage lung cancer patients. Grounded in Stress and Coping Theory and Pain Threat Interpretation Theory,17,18 this study is among the first to test the multiple parallel mediating roles of these three variables in the pain-catastrophizing relationship. This work addresses a critical gap by simultaneously examining these mechanisms within a single integrated biopsychosocial model.
Therefore, this study puts forward the following two central research questions: (1) Mediation mechanism: Do interoceptive awareness, negative attentional bias, and social support significantly mediate the relationship between pain intensity and pain catastrophizing among patients following early-stage lung cancer surgery? (2) Multiple mediation pathways: Are there multiple parallel mediation pathways through which interoceptive awareness, negative attentional bias, and social support influence the relationship between pain intensity and pain catastrophizing? If so, what is the relative importance of each pathway? Answering these questions will lay a solid theoretical foundation for the prevention of pain catastrophizing and the development of targeted rehabilitation.
Materials and Methods
Study Design
A cross-sectional study design was employed to investigate patients who had undergone early-stage lung cancer surgery and were attending follow-up visits at ambulatory care and day ward treatment of a tertiary grade A specialized hospital in Tianjin from May to August 2025. These individuals were selected as research participants through convenience sampling, and relevant data were collected via face-to-face interviews.
Participants
Eligibility criteria for patients: (1) Diagnosis of lung cancer confirmed by imaging and pathological examinations, and meeting the staging criteria for early-stage lung cancer as defined in the Chinese Medical Association guideline for clinical diagnosis and treatment of lung cancer (2024 Edition);19 (2) Completion of curative lung resection surgery with discharge within 3 months postoperatively; (3) Age ≥ 18 years; (4) Sufficient cognitive and language abilities to understand and complete the questionnaire independently or with minimal assistance; (5) Provision of written informed consent prior to participation. Exclusion criteria: (1) Presence of diagnosed psychiatric disorders or a history of receiving formal psychological or psychiatric treatment; (2) Significant comorbidities involving major organ systems, including severe cardiac, pulmonary, hepatic, or renal dysfunction. Dropout criteria: (1) Missing data exceeding 5% in key scale items or essential clinical records; (2) Evidence of systematic or patterned responding on questionnaires, indicating non-compliance or invalid responses.Based on the sample size estimation method proposed by Kendall,20 which recommends that the sample size should be 10 to 20 times the number of independent variables, this study included 33 independent variables and used a multiplier of 11, resulting in a minimum required sample size of 363. Accounting for a 10% questionnaire invalidity rate and considering clinical feasibility, the final target sample size was set at 414 participants.
Procedure
Four nurses who had received standardized training and possessed clinical experience were selected as study investigators. Two nurses were assigned to the outpatient department and two to the day ward to conduct the questionnaire administration. After obtaining informed consent, patients in the day ward completed the questionnaires at their bedside, while those in the outpatient setting completed them in a quiet waiting area. Investigators delivered standardized verbal instructions to explain the study purpose and questionnaire completion procedures, ensuring that participants completed the questionnaires independently and truthfully. Upon completion, each questionnaire was immediately reviewed on site by the investigator; any missing or incomplete items were identified and addressed with the participant before final submission. Once completeness was confirmed, the questionnaires were collected on the spot. A total of 425 questionnaires were distributed, and 414 valid responses were obtained, yielding an effective response rate of 97.4%. Ethical approval for the study was obtained from Tianjin Medical University Cancer Institute & Hospital (bc20252060), with conduct in strict adherence to Helsinki Declaration guidelines.
Measures
General Information on the Questionnaire
The questionnaire was developed by the research team based on a comprehensive review of relevant literature and expert group discussions. It comprises two sections: general demographic information and disease-related characteristics. Demographic variables include gender, age, marital status, educational attainment, occupation, place of residence, living arrangement, household income, medical payment method, and personality traits. Disease-related variables encompass time since surgery, prior medical history, body mass index (BMI), preoperative pain experience, long-term use of analgesic medications, sleep quality, postoperative treatment regimen, and pathological stage.
Pain Catastrophizing Scale (PCS)
The Pain Catastrophizing Scale (PCS) was developed by Sullivan et al21 in 1995 to assess the tendency of individuals to engage in catastrophic thinking in response to pain. It is currently the most widely used instrument for evaluating pain-related catastrophizing in clinical settings. The scale was specifically designed to measure the severity of pain catastrophizing and comprises 13 items distributed across three subscales: helplessness, magnification, and rumination. Each item is rated on a 5-point Likert scale ranging from 0 (“never”) to 4 (“always”), yielding a total score between 0 and 52. A cutoff score of ≥ 30 has been established as clinically significant,16 indicating the presence of notable pain catastrophizing, with higher scores reflecting greater severity. The Chinese version of the scale was translated and culturally adapted by Yap et al22 in 2008. In this study, the scale demonstrated strong internal consistency, with an overall Cronbach’s α coefficient of 0.864, confirming its reliability and validity.
Pain Assessment Ruler
The Pain Assessment Ruler23,24 integrates three single-dimensional pain scales—the Numerical Rating Scale (NRS), Verbal Descriptor Scale (VDS), and Revised Faces Pain Scale (FPS-R)—as coordinated response options where the NRS serves as the primary quantitative outcome measure for statistical analyses. The VDS and FPS-R function as supplementary visual and verbal anchors to assist patients, particularly older adults, in accurately selecting their NRS score. The NRS employs an 11-point numeric scale ranging from 0 (“no pain”) to 10 (“worst possible pain”), with scores of 0–3 indicating mild pain, 4–6 moderate pain, and 7–10 severe pain. The VDS provides descriptive verbal anchors from “no pain” to “severe pain,” while the FPS-R depicts six facial expressions representing increasing pain levels from “no pain” to “very much pain.” This integrated design ensures simplicity, efficiency, and enhanced accuracy for pain assessment in older adults by facilitating reliable NRS scoring.
The Multidimensional Assessment of Interoceptive Awareness, Version2 (MAIA-2)
In 2018, Mehling et al revised the Multidimensional Assessment of Interoceptive Awareness (MAIA) to develop the second edition (MAIA-2).25 Relative to the original version, MAIA-2 retains eight dimensions and comprises 37 items. It employs a 6-point Likert scale ranging from 0 (“never”) to 5 (“always”), with higher scores indicating greater interoceptive awareness. To improve content coverage and measurement precision, three items were added to the “Not Distracted” dimension and two items to the “Not Worrying” dimension. The Chinese version of the MAIA-2 (MAIA-2C) was translated and culturally adapted in 2022,26 and its psychometric properties were validated in a mainland Chinese population. In this study, the scale demonstrated excellent internal consistency, with an overall Cronbach’s α coefficient of 0.920, confirming its reliability and validity.
The Chinese Attention to Negative Inventory (ANI)
The Attention to Positive and Negative Information Inventory (APNI), developed by Dai Qin et al27, has undergone translation and cultural adaptation to produce a Chinese version. It comprises two subscales: the Positive Information Attention Scale and the Negative Information Attention Scale. The Chinese version of the Negative Information Attention Scale consists of 10 items organized across two dimensions: self and others. It utilizes a 5-point Likert scoring system (ranging from 1 to 5), with total scores varying between 10 and 50; higher scores reflect a stronger negative attentional bias. The subscale demonstrates a Cronbach’s α coefficient of 0.82 and a test-retest reliability coefficient of 0.62. For the Positive Information Attention Scale, the Cronbach’s α coefficient is 0.86, with a test-retest reliability of 0.79. Research indicates that the correlation between the two subscales is low, suggesting good discriminant validity and supporting their independent use in clinical or research settings to assess attentional biases toward positive and negative information. In this study, the Chinese version of the Negative Information Attention Scale was employed for assessment purposes. It exhibited strong internal consistency in the current sample, with an overall Cronbach’s α coefficient of 0.887, confirming its reliability and validity as a measurement tool.
Social Support Rating Scale (SSRS)
The Social Support Rating Scale (SSRS),28 developed by Shuiyuan Xiao at Hunan Medical University in China in 1986, is a widely used instrument designed to assess individuals’ perceived levels of social support. The scale comprises 10 items distributed across three dimensions: objective support (items 2, 6, and 7), subjective support (items 1, 3, 4, and 5), and utilization of support (items 8, 9, and 10). The maximum total score is 66. Scoring is conducted as follows: items 1–4 and 8–10 are rated on a 4-point scale, with responses 1 to 4 assigned scores of 1 to 4, respectively. Item 5 consists of five sub-items (A, B, C, D, and E), each scored from 1 to 4 according to the level of support—from “none” to “full support”—and the sum of these sub-item scores constitutes the total for item 5. For items 6 and 7, a response of “no source” is scored as 0, while endorsement of “the following sources” yields one point per identified source. Higher total scores indicate greater levels of perceived social support. Based on established normative criteria, scores ≤ 22 reflect low social support, scores ranging from 23 to 44 reflect moderate social support, and scores ≥ 45 indicate high social support. In this study, the SSRS demonstrated strong internal consistency, with an overall Cronbach’s α coefficient of 0.836, confirming its reliability and validity as a psychometric tool.
Data Analysis
Data were entered using Microsoft Excel and independently double-entered by two researchers to ensure accuracy. Data analysis was performed with SPSS 26.0 including descriptive statistics of pain catastrophizing (such as mean, standard deviation, etc.) and Pearson correlation analysis to examine the relationships among pain intensity, interoceptive awareness, negative attentional bias, social support, and pain catastrophizing.
A structural equation model (SEM) was subsequently constructed using AMOS 24.0 to test the mediating effects of interoceptive awareness, negative attentional bias, and social support in the relationship between pain intensity and pain catastrophizing. Notably, variables associated with pain catastrophizing (PCS) identified in univariate analysis (eg, marital status, analgesic use, pathological stage) were excluded from the SEM model. This exclusion was because this decision was grounded in the study’s theoretical focus on testing the mediating mechanisms of interoceptive awareness, negative attentional bias, and social support within a biopsychosocial framework. As these three variables constitute the core cognitive-affective processes directly underlying PCS, their inclusion, as primary mediators, enhanced the model’s internal validity and explanatory power. While the omitted demographic and clinical variables may indirectly influence PCS by affecting these core mediators, they were excluded to maintain model parsimony and concentrate analytical power on the hypothesized mediating pathways, which represented the central focus of this research. The significance of indirect effects was evaluated using the Bootstrap method with 5000 resamples at a 95% confidence interval. The statistical significance level was set at α = 0.05.
Results
Result of the Common Method Bias Test
The Harman single-factor test was employed to assess common method bias. All items from the Chinese version of the PCS, the Pain Assessment Scale, MAIA-2, the Chinese version of the ANI, and the SSRS were included in an unrotated exploratory factor analysis for patients who underwent surgery for early-stage lung cancer. The analysis yielded 15 factors with eigenvalues exceeding 1. The first factor accounted for 21.75% of the total variance, which is below the 40% threshold, indicating no significant common method bias in the study.
Descriptives
In the univariate analysis of factors influencing pain catastrophizing in patients after early-stage lung cancer surgery, statistically significant factors included marital status, personality traits, operation time, duration of pain, long-term use of analgesics, sleep quality, the number of days pain restricted daily life or work, treatment methods, and pathological stage (P < 0.05). For details, please refer to Table 1.
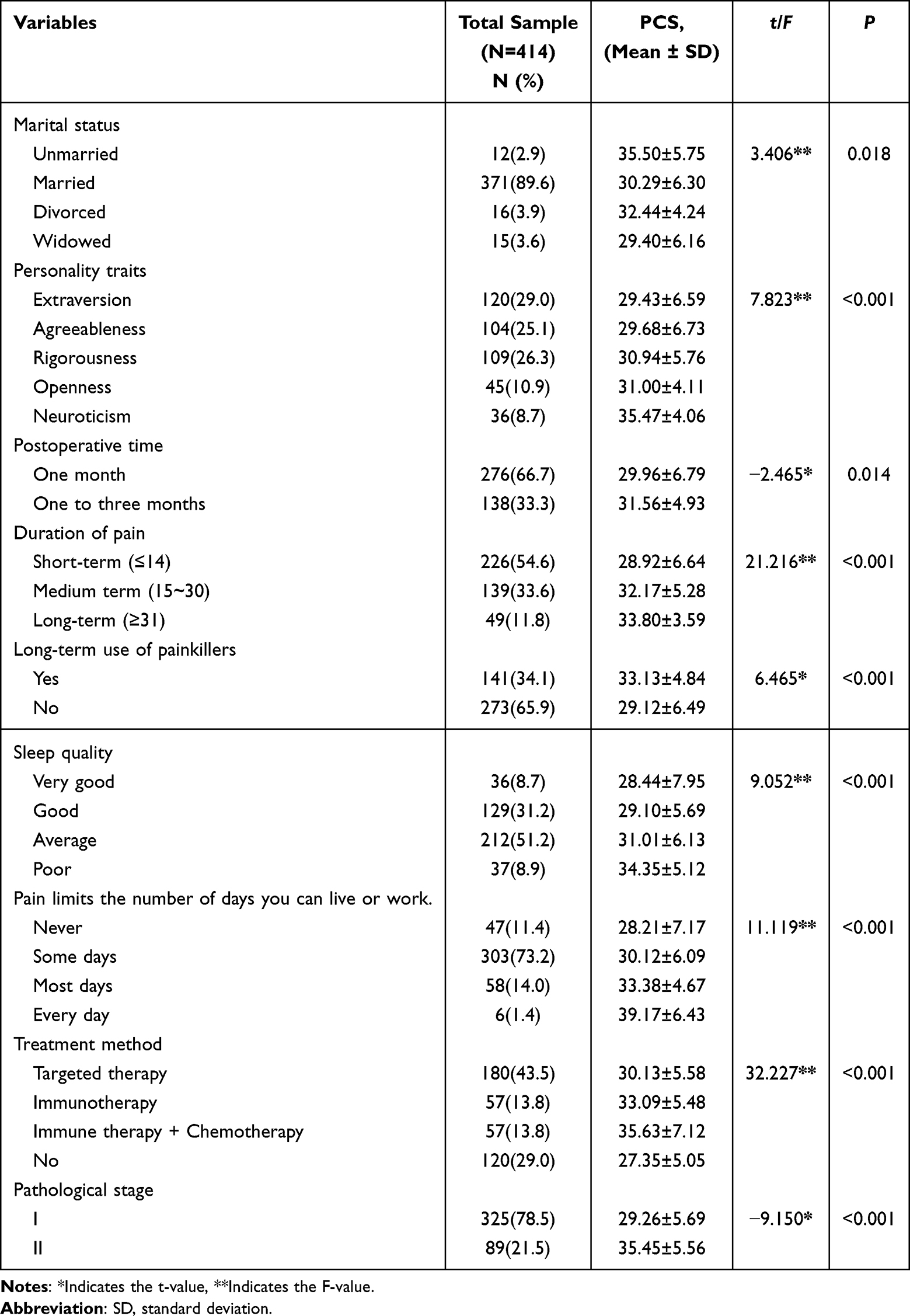 |
Table 1 Univariate Analysis Of Demographic Data Of Patients with Early-Stage Lung Cancer After Surgery |
The mean pain severity score among patients who underwent surgery for early-stage lung cancer was 3.22 ± 1.13, interoceptive awareness was 109.33 ± 5.89, negative attentional bias toward information was 29.24 ± 6.72, and perceived social support was 40.06 ± 6.80. Further details are in Table 2.
 |
Table 2 Pain Severity, Interoceptive Awareness, Negative Attentional Bias, Social Support, and Pain Catastrophizing Scores Among Patients with Early-Stage Lung Cancer After Surgery (n = 414) |
Correlations Analysis
Pain intensity was significantly positively correlated with the total scores of interoceptive awareness, negative attentional bias, and pain catastrophizing (P < 0.001), and significantly negatively correlated with the total score of social support (P < 0.001). The total score of interoceptive awareness was also significantly positively associated with the total scores of negative attentional bias and pain catastrophizing (P < 0.001), and showed a significant negative correlation with the total score of social support (P < 0.001). Furthermore, the total score of negative attentional bias was significantly positively correlated with the total score of pain catastrophizing (P < 0.001), and significantly negatively correlated with the total score of social support (P < 0.001). Lastly, a significant negative correlation was observed between the total score of social support and the total score of pain catastrophizing (P < 0.001), as shown in Table 3.
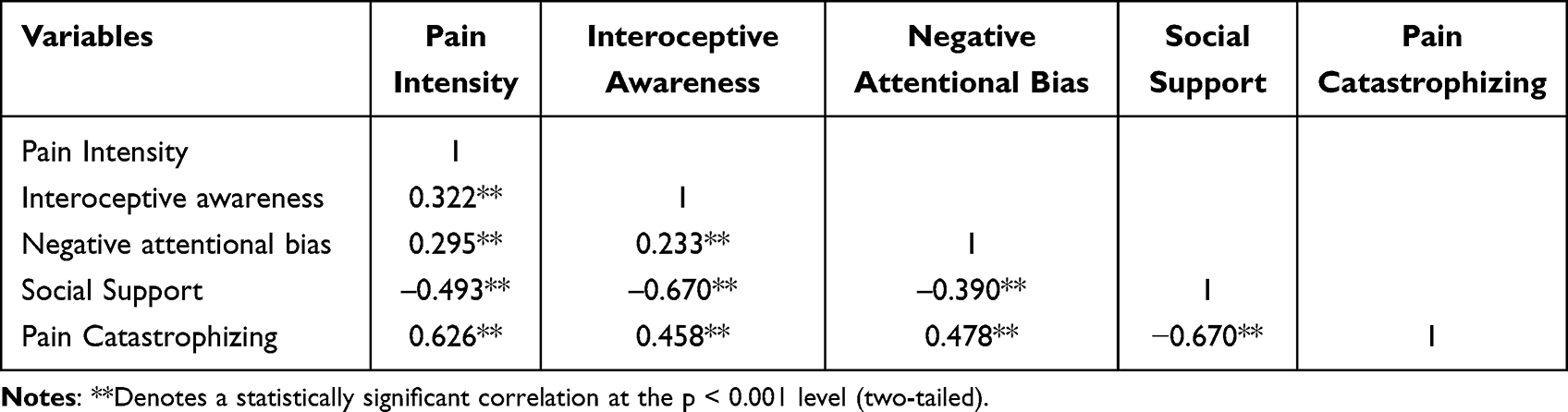 |
Table 3 Correlation Analysis of Pain Intensity, Interoceptive Awareness, Negative Attentional Bias, Social Support, and Pain Catastrophizing in Patients with Early-Stage Lung Cancer After Surgery (n = 414) |
Structural Equation Model (SEM)
A structural equation model was constructed with pain catastrophizing as the dependent variable, pain intensity as the independent variable, and interoceptive awareness, negative attentional bias, and social support as mediating variables (Figure 1). Model fit indices (χ2/df = 2.663, GFI = 0.931, AGFI = 0.896, CFI = 0.945, NFI = 0.916, IFI = 0.946, TLI = 0.926, RMSEA = 0.063, SRMR = 0.056) all fall within acceptable thresholds, indicating good model fit and supporting the adequacy of the proposed model (Table 4). To examine the mediating effects of each pathway, 5,000 bootstrap samples were generated using the non-parametric percentile Bootstrap method, with a 95% confidence interval (Table 5).
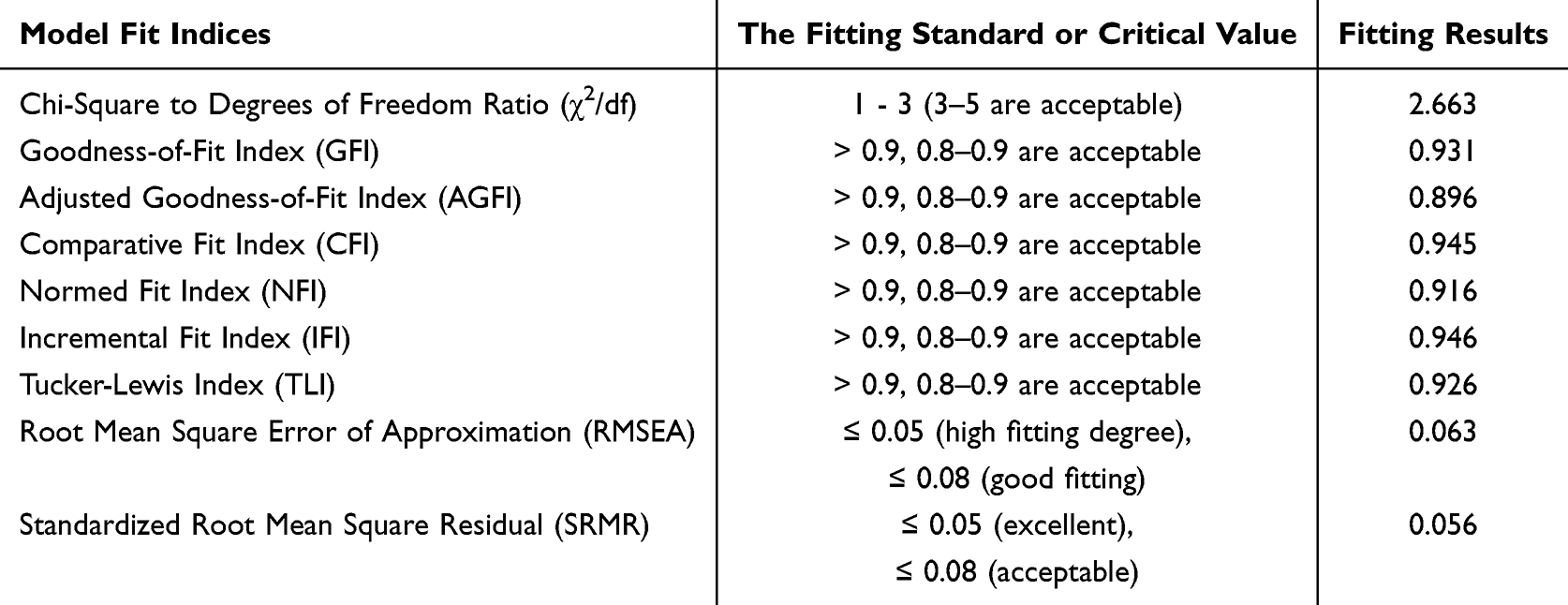 |
Table 4 Model Fit Indices |
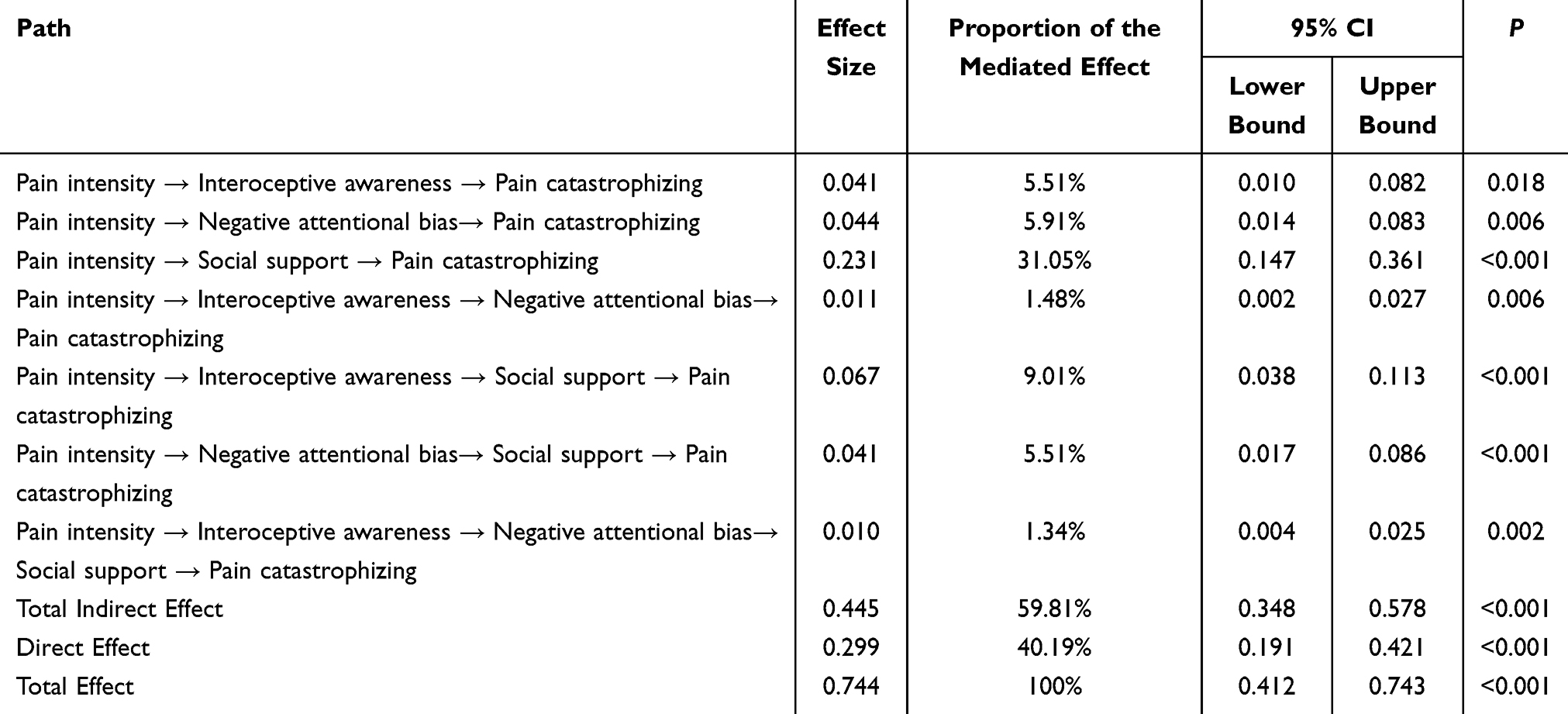 |
Table 5 Standardized Mediating Effects Of Interoceptive Sensitivity, Negative Attentional Bias, and Social Support in The Relationship Between Pain Intensity and Pain Catastrophizing Among Patients with Early-Stage Lung Cancer After Surgery |
 |
Figure 1 Mediating effect model of interoceptive awareness, negative attentional bias, and social support in the relationship between pain intensity and pain catastrophizing among patients with early-stage lung cancer after surgery. |
Discussion
Prevalence and Clinical Profile of Postoperative Pain Catastrophizing
The mean PCS score of 30.49 ± 6.27 slightly exceeds the clinical cutoff (≥30), indicating moderately high pain catastrophizing in early-stage lung cancer patients within three months post-surgery.8–10 The rumination subscale scored highest, reflecting persistent attentional focus on pain that exacerbates psychological distress.7,21 Key risk factors include neurotic personality traits (8.7% of this sample),29 long-term analgesic use (34.1%) indicating suboptimal pain control, and higher pathological stage (21.5% Stage II).6,30 Notably, A PCS score 1–3 months post-surgery that is higher than 1 month post-surgery may be related to prolonged pain, which can trigger anxiety about recovery progress and disease recurrence, exacerbating catastrophic thinking. Given these findings, it is recommended that healthcare providers proactively identify high-risk patients—particularly those with neurotic traits, inadequate pain control, or prolonged pain—and integrate routine assessment of pain catastrophizing into standard clinical care. Moreover, cognitive-behavioral interventions should be implemented to assist patients in identifying and restructuring maladaptive pain-related cognitions, reducing rumination, and promoting active engagement in pain self-management strategies to enhance perceived control and ultimately reduce pain catastrophizing.
Direct Effect of Pain Intensity
Correlation analysis revealed a significant positive association between pain intensity and catastrophizing (r = 0.636, P < 0.001), supporting pain threat interpretation theory18 and consistent with prior research.6,10 High-intensity pain acts as a potent stressor that triggers fear and anxiety, leading patients to misinterpret pain as disease recurrence or deterioration. This creates a self-perpetuating cycle of pain vigilance and hypervigilance that reinforces maladaptive cognitive patterns.7,18 SEM confirmed a significant direct effect (β = 0.299, P < 0.001), with pain intensity accounting for 40.19% of the total effect on catastrophizing. Clinically, elevated pain scores should trigger psychological assessment and integrated non-pharmacological interventions (cognitive restructuring, attentional retraining, pain education) rather than sole reliance on analgesics.
Multiple Mediating Pathways
The analysis revealed significant parallel and sequential mediating pathways. Interoceptive awareness, negative attentional bias, and social support collectively mediated 59.81% of the pain - catastrophizing relationship, highlighting the substantial role of psychosocial processes. Social support was the most prominent mediator (31.05% of the total effect). Higher pain intensity was linked to lower perceived social support, which in turn strongly predicted greater PC. Adequate support provides emotional reassurance and practical resources, enhancing pain coping self - efficacy, whereas its absence can exacerbate feelings of isolation and helplessness.14,31 Interoceptive awareness reflects heightened bodily vigilance that amplifies routine sensations into threats,11,15,32 and it accounted for 5.51% of the total effect. Negative attentional bias represents selective attention to pain - related negative stimuli that consolidates maladaptive cognitive patterns,13,16 and it accounted for 5.91% of the total effect. These factors operate in sequence. Firstly, higher pain intensity leads to increased interoceptive awareness. Secondly, increased interoceptive awareness gives rise to negative attentional bias. Thirdly, negative attentional bias further results in diminished support utilization. Finally, diminished support utilization leads to pain catastrophizing, representing a cascading vulnerability sequence. A sequential pathway (pain intensity→interoceptive awareness/negative attentional bias→reduced social support→catastrophizing) underscores the interplay of biological, psychological, and social factors. This supports a multidimensional clinical framework: combine pain control, cognitive-behavioral therapy(CBT), mindfulness training, and social support enhancement to disrupt cascading maladaptive processes.
Integrated Clinical Implications
These findings advocate for an integrated, multidimensional intervention framework grounded in the biopsychosocial model to address both the direct and mediated pathways to PC: (1) Effective Pain Management: As the foundational element to reduce the primary driver. (2) Social support is the most powerful psychosocial mediator of pain catastrophizing and should therefore be prioritized as highly as pharmacological pain control in clinical practice. Assessing and strengthening patients’ social support networks must become an integral component of routine postoperative care. Social support optimization involves proactively engaging family caregivers, establishing peer support groups, and connecting patients with community resources. (3) Cognitive-behavioral strategies: Target attentional retraining and cognitive restructuring to disrupt rumination. (4) Mindfulness-based interventions: Teach non-judgmental interoceptive awareness (eg, body scanning) to reduce catastrophic misinterpretation. (5) Risk stratification: Prioritize patients with neurotic traits, persistent analgesic requirements, and early postoperative status for intensive psychological support.
Limitations and Future Directions
This study has several limitations. First, the single-center design may introduce selection bias via convenience sampling, thereby limiting generalizability to broader early-stage lung cancer surgery cohorts. Second, reliance on self-report measures risks response biases and subjective inconsistencies, including social desirability and variable interoceptive awareness ratings. Third, potential residual confounding from unmeasured variables—such as preoperative pain trajectories and psychological comorbidities—cannot be fully eliminated. Fourth, the cross-sectional design contributes to common method bias by collecting all data at a single time point, which may artificially inflate correlations and precludes establishing causal relationships or directional effects (eg, pain intensity versus catastrophizing). Finally, heterogeneity due to the 1–3 month postoperative window may obscure critical period-specific recovery patterns. Future research should employ multicenter, longitudinal, or interventional designs to confirm causal pathways and temporal dynamics. Integrating objective measures (eg, physiological indicators, attention bias tasks) with self-reports would enhance robustness.
Conclusions
This study suggests that patients with early lung cancer exhibit moderate-high levels of pain catastrophizing within 3 months post-surgery, with pain intensity showing significant associations with catastrophizing through potential mediators of interoception, negative attentional bias, and social support. These findings generate hypotheses for intervention research, healthcare professionals should consider implementing a multidimensional intervention strategy: awareness-based interventions can regulate introspection, cognitive-behavioral therapy techniques can target negative attentional bias, and family education sessions or patient support groups can enhance social support. Such approaches may mitigate catastrophizing, though interventional studies are needed to test these hypotheses. However, the single-center, cross-sectional design limits generalizability and causal inference; future multi-center, longitudinal, or intervention studies are essential to validate these pathways, test causality, and evaluate intervention effectiveness.
Acknowledgment
We sincerely appreciate the participants for their contributions to the current research. The authors acknowledge the financial support from Tianjin Research Program on Traditional Chinese Medicine and Integrated Chinese-Western Medicine (grants No. 2025020), Tianjin Key Medical Discipline Construction Project (grants No. TJYXZDXK-3-003A), and Research Project Funded by the Tianjin Nursing Association (grants No. tjhlky2025QN16).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Qin N, Ma H, Jin G, et al. Annual progress in epidemiological studies of lung cancer 2022. Chin Med J. 2023;103(14):1068–11. doi:10.3760/cma.j.cn112137-20221123-02448
2. Chinese Society of Oncology. Guidelines for clinical diagnosis and treatment of lung cancer (2024 edition). Chin J Oncol. 2024;46(09):805–843. doi:10.3760/cma.j.cn112152-20240510-00189
3. Tawfic Q, Kumar K, Pirani Z, et al. Prevention of chronic post-surgical pain: the importance of early identification of risk factors. J Anesthesia. 2017;31:424–431. doi:10.1007/s00540-017-2339-x
4. K.h G, Oksholm T, Follestad T, et al. Trajectories of pain in patients undergoing lung cancer surgery: a longitudinal prospective study. J Pain Symptom Manage. 2020;59(4):818–828.e1. doi:10.1016/j.jpainsymman.2019.11.004
5. Wang Q. Changes of myeloid inhibitory cells during the perioperative period of lung cancer and their effects on tumor growth and angiogenesis. Cancer. 2016;10:452–458. doi:10.3781/j.issn.1000-7431.2016.33.041
6. Tuna T, Boz S, V OL, et al. Comparison of the pain sensitivity questionnaire and the pain catastrophizing scale in predicting postoperative pain and pain chronicization after spine surgery. Clin Spine Surg. 2018;31(9):E432–E440. doi:10.1097/BSD.00000000000094
7. Wang S, Lu J, Hao W, et al. Research progress on pain catastrophizing. Chin Clin Nurs. 2023;15(04):252–256. doi:10.3969/j.issn.1674-3768.2023.04.013
8. Prasertsri N, Holden J, Keefe FJ, et al. Repressive coping style: relationships with depression, pain, and pain coping strategies in lung cancer outpatients. Lung Cancer. 2011;71(2):235–240. doi:10.1016/j.lungcan.2010.05.009
9. Dalton JA, Higgins MK, Miller AH, et al. Pain intensity and pain interference in patients with lung cancer: a pilot study of biopsychosocial predictors. Am J Clin Oncol. 2015;38(5):457–464. doi:10.1097/COC.0b013e3182a79009
10. Wang R, Yang L, Zhu X, et al. Analysis of the current situation and influencing factors of pain catastrophizing in patients with lung cancer pain. Guangxi Med J. 2023;45(24):
11. Ferguson RJ, Ahles TA. Private body consciousness, anxiety and pain symptom reports of chronic pain patients. Behav Res Ther. 1998;36(5):527–535. doi:10.1016/s0005-7967(98)00048-5
12. DuBois D, H AS, Lai M-C, et al. Interoception in autism spectrum disorder: a review. Int J Dev Neurosci. 2016;52:104–111. doi:10.1016/j.ijdevneu.2016.05.001
13. Wong WS, Fielding R. Suppression of emotion expression mediates the effects of negative affect on pain catastrophizing: a cross-sectional analysis. Clin J Pain. 2013;29(10):865–872. doi:10.1097/AJP.0b013e31827da3b5
14. Wang Y, Wei S. Analysis of pain catastrophizing and its influencing factors among patients with neuropathic pain. Nurs Res. 2020;34(13):2371–2374. doi:10.12102/j.issn.1009-6493.2020.13.023
15. Locatelli G, Matus A, James R, et al. What is the role of interoception in the symptom experience of people with a chronic condition? A systematic review. Neurosci Biobehav Rev. 2023;148:105142. doi:10.1016/j.neubiorev.2023.105142
16. Booth RW, Sharma D. Attentional control and estimation of the probability of positive and negative events. Cogn Emot. 2020;34(3):553–567. doi:10.1080/02699931.2019.1657382
17. Folkman S. Personal control and stress and coping processes: a theoretical analysis. J Pers Soc Psychol. 1984;46(4):839–852. doi:10.1037/0022-3514.46.4.839
18. Todd J, Sharpe L, Johnson A, et al. Towards a new model of attentional biases in the development, maintenance, and management of pain. Pain. 2015;156(9):1589–1596. doi:10.1097/j.pain.0000000000000214
19. Oncology Society of Chinese Medical Association. Chinese Medical Association guideline for clinical diagnosis and treatment of lung cancer (2024 edition). Zhonghua Zhong Liu Za Zhi. 2024;46(9):805–843. [Chinese]. doi:10.3760/cma.j.cn112152-20240510-00189
20. Kendall MG, Stuart A, Ord JK. Kendall’s advanced theory of statistics. Techno Metrics. 1994;31(1):128. doi:10.2307/2348968
21. Sullivan MJL, Bishop SR, Pivik J. The pain catastrophizing scale: development and validation. Psychol Assess. 1995;7(4):524–532. doi:10.1037/1040-3590.7.4.524
22. Yap JC, Lau J, Chen PP, et al. Validation of the Chinese Pain Catastrophizing Scale (HK-PCS) in patients with chronic pain. Pain Med. 2008;9(2):186–195. doi:10.1111/j.1526-4637.2007.00307.x
23. Cao Y, Liao L, Qin J, et al. A systematic review of assessment tools for acute postoperative pain in adults. J Nurs. 2023;38(07):110–116. doi:10.3870/j.issn.1001-4152.2023.07.110
24. Zhao J. Design and clinical application of the simple pain assessment scale. Nurs Res. 2012;26(31):289. doi:10.3969/j.issn.1009-6493.2012.31.006
25. E MW, Acree M, Stewart A, et al. The Multidimensional Assessment of Interoceptive Awareness, Version 2 (MAIA-2). PLoS One. 2018;13(12):e0208034. doi:10.1371/journal.pone.0208034
26. Teng B, Wang D, Su C, et al. The multidimensional assessment of interoceptive awareness, version 2: translation and psychometric properties of the Chinese Version. Front Psychiatry. 2022;13:970982. doi:10.3389/fpsyt.2022.970982
27. Dai Q, Feng Z, Xu S, et al. Validity and reliability of the Chinese version of the positive and negative information attention scale in a sample of college students. Chin J Mental Health. 2015;29(05):395–400. doi:10.3969/j.issn.1000-6729.2015.05.017
28. Xiao S. Theoretical basis and research application of the “Social support rating scale”. J Clin Psychiatry. 1994;02:98–100.
29. Chang Q. The relationship between the big five personality traits and pain, depression, anxiety and pain catastrophizing in patients with chronic lung cancer. Kunming Med Univ. 2022. doi:10.27202/d.cnki.gkmyc.2022.000869
30. Wu X, Xu T, Cai P, et al. Latent profile analysis of pain catastrophizing in post-operative lung cancer patients. J Pain Res. 2025;18:1735–1745. doi:10.2147/JPR.S507027
31. E GA, Burnsj W, Aranda F, et al. Social support, social undermining and acute clinical pain in women: mediational path ways of negative cognitive appraisal and emotion. J Health Psychol. 2020;25(13–14):2328–2339. doi:10.1177/1359105318796189
32. Oliveira I, Vaz Garrido M, Carvalho H, et al. Sensing the body matters: profiles of interoceptive sensibility in chronic pain adjustment. Pain. 2024;165(2):412–422. doi:10.1097/j.pain.0000000000003032
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Relationship Between Fear Avoidance Belief and Threat Learning in Postoperative Patients After Lung Surgery: An Observational Study
Bao L, Peng C, He J, Sun C, Feng L, Luo Y
Psychology Research and Behavior Management 2023, 16:3259-3267
Published Date: 16 August 2023
Effect of Personality and Pain Catastrophizing on Postoperative Analgesia Following Cesarean Section: A Prospective Cohort Study
Ren Y, Guo Y, Tang J, He L, Li M, Huang X, Lu Q, Sun B, Feng H, Liu H, Du J, Li J
Journal of Pain Research 2024, 17:11-19
Published Date: 3 January 2024
A Randomized Controlled Trial of Clinical Hypnosis as an Opioid-Sparing Adjunct Treatment for Pain Relief in Adults Undergoing Major Oncologic Surgery
Rosenbloom BN, Slepian PM, Azam MA, Aternali A, Birnie KA, Curtis K, Thaker S, Ladak S, Waisman A, Clarke H, Katz J, Weinrib AZ
Journal of Pain Research 2024, 17:45-59
Published Date: 4 January 2024
Therapy-Related Symptoms and Sense of Coherence: The Mediating Role of Social Support and Hope in Lung Cancer Patients Undergoing Chemotherapy
Wang F, Nie A, Liao S, Zhang Z, Su X
Patient Preference and Adherence 2024, 18:2559-2568
Published Date: 13 December 2024
The Chain Mediating Role of Hope and Posttraumatic Growth Between Social Support and Psychological Distress Among Lung Cancer Patients
Huang JG, Xu CH, Shi YM, Jiang J, Huang FM, Xu LL
Cancer Management and Research 2025, 17:1399-1419
Published Date: 16 July 2025